Embed Size (px)
Citation preview

1
Kitch Drutchas Wagner Valitutti & Sherbrook2379 Woodlake Drive, Suite 400
Okemos, Michigan 48864517.381.7192
www.kitch.com
Detroit Lansing Mt. Clemens Marquette Toledo Chicago
LEADINGAGE MICHIGAN
SNF REGULATORY DAY
September 17, 2014
Kitch Drutchas Wagner Valitutti & Sherbrook2379 Woodlake Drive, Suite 400
Okemos, Michigan 48864517.381.7192
www.kitch.com
CMS UPDATES

2
S&C: 14-18 NH
March 28, 2014o Chapter 7 of the State Operations Manual (SOM) has been revised
to incorporate the following provisions of Section 6111 of the Patient
Protection and Affordable Care Act (the Affordable Care Act):
• Independent IDR: An independent informal dispute resolution process
will be available when a civil money penalty (CMP) is imposed.
• Escrow: After an independent IDR, CMP funds will be collected and
placed in escrow pending completion of any formal appeal.
• 50 Percent Reduction: A CMP may be reduced by 50 percent in certain
cases of prompt correction for self-reported non-compliance.
• Use of CMP Funds: A portion of the CMP attributable to Medicare may
be used for programs for the protection or benefit of nursing home
residents.
S&C: 14-18 NH
March 28, 2014o Reminder of Survey Process Timeframes: Reiterates the
requirements for enforcement action timelines when immediate
jeopardy exists and when immediate jeopardy does not exist.
(Chapter 7 of the SOM at sections 7300 thru 7320).
• The plan of correction for the deficiencies should be deferred until a
revisit to verify that the removal of the immediate jeopardy has been
completed.
• The notice of the Immediate Jeopardy to the provider must be
delivered no later than two days of the end of the survey. If official
notification of all deficiencies, i.e., Form CMS-2567, was not given
on the second day, a completed Form CMS-2567 must be sent to
the entity on the tenth working day.
S&C: 14-19 NH
April 11, 2014
An interim report that discusses the
history of the National Partnership to
Improve Dementia Care, summarizes
activities to date, provides reasons for
early progress and outlines next steps for
future Partnership efforts.

3
S&C: 14-30 NH
May 16, 2014
oAs part of the 2010 Affordable Care Act, CMS is
soliciting proposals for a grant opportunity in which
Federal CMP Funds will be utilized to support and
further expand the National Partnership to Improve
Dementia Care in Nursing Homes.
o A total of $500,000 for FY2014-2015 will be
available for a three year period of performance.
Funding will be awarded in 12 month budget
periods.
S&C: 14-20 NH
April 18, 2014o CMS adjusted the number of designated slots and candidates so
States can resume selecting and replacing nursing homes for
SFF designation.
• Now re-building the program by a gradual increase in the number of SFF
slots from its reduced base.
• Later, will also introduce additional methods to address persistently poor
quality in nursing homes.
• Phase in period: States may have the option to start selecting SFFs
immediately or phase in the total to meet the required number by July 2014.
• Continuation of Program Changes: CMS and States will continue with the
Programmatic and Operational Adjustment by conducting the 18 month “last
chance” onsite survey and reviewing the progress of all facilities that have
been on the SFF list for more than 12 months.
S&C: 14-21 LSC
April 18, 2014
Proposed rule that would amend the current fire safety
standards for Medicare- and Medicaid-participating
providers and suppliers. This proposed rule would adopt
the 2012 edition of the Life Safety Code (LSC), National
Fire Protection Association, (NFPA) 101.

4
S&C: 14-33 NH
May 20, 2014o CMS published final rule CMS-3267-F in which CMS
implemented reforms in Medicare regulations that are
identified as unnecessary, obsolete, or excessively
burdensome on health care providers and beneficiaries
o Nursing home and LTC (Automatic Sprinkler Systems):
The rule permits a temporary extension of the automatic
sprinkler system installation due date under limited
circumstances
S&C: 14-29 LSC
May 16, 2014
Provides the procedures to apply for approval of a
request for an extension of time by a qualifying long
term care facility that has not met the August 13, 2013
deadline for the installation of a complete automatic
sprinkler system throughout the facility.
S&C: 14-22 NH
April 18, 2014o Currently developing two distinct focused survey processes to
assess dementia care and Minimum Data Set, Version 3.0 (MDS
3.0) coding practices in nursing homes.
o CMS is planning to pilot these survey types beginning in 2014.
The intent of the dementia care focused survey is to document
dementia care practices in nursing homes. The intent of the
MDS focused survey is to document MDS 3.0 coding practices
and associated care planning in facilities.
o This training will be mandatory for those State Survey Agency
(SA) staff conducting reviews as well as one manager or trainer
within the SA.
• Surveyor Implications: Deficient practices noted during the survey will
result in relevant citations.

5
S&C: 14-24 ALL
May 2, 2014o Section 2008D is being revised to conform more clearly to the
governing regulation at 42 CFR 489.13.
o Survey Process after Denial of Initial Application: Section 2005
has been revised to reflect the following: an applicant who is
denied certification (CMS), based on a finding of substantial
noncompliance from the initial survey, may reapply for
certification.
• However, the applicant may submit no more than two reapplications
for certification in connection with one enrollment application, and
no more than six months may elapse between the date of the CMS
Regional Office’s (RO’s) first denial and the RO’s receipt of the
second reapplication. Applicants who reapply for certification must
undergo a subsequent survey.
S&C: 14-24 ALL
May 2, 2014o Applicants subject to the Life Safety Code – if the applicant
was in substantial compliance with the LSC on the initial
survey, at SA or AO discretion compliance with the LSC does
not have to be reassessed.
o Various SOM sections, including Sections 2053, 2777, 2779,
3005 and 3008 have been revised to update provisions
concerning Medicaid.
o Assigning Medicaid-only CMS Certification numbers (CCNs)
within the classification system, including in the Automated
Survey Process Environment (ASPEN).
o Multiple provisions of the SOM related to accreditation have
been clarified.
S&C: 14-25 NH
May 16, 2014
oThe guidance under Tag F441, Infection
Control, Preventing Spread of
Infection/Indirect Transmission has been
revised.
oSingle-Use Device Guidance: Nursing
homes may purchase reprocessed single-
use devices when these devices are
reprocessed by an entity or a third party
reprocessor that is registered with the FDA.

6
S&C: 14-28 NH
May 9, 2014
A notice of proposed rule-making (NPRM)
regarding Nursing Home Civil Monetary
Penalties was published on May 6, 2014,
which provides clarification of statutory
requirements under Section 6111 of the
Affordable Care Act regarding the approval
and use of Civil Money Penalties (CMPs)
imposed CMS against nursing facilities.
S&C: 14-34 NH
May 20, 2014• Guidance for SNFs and NFs: Use pasteurized shell eggs or liquid
pasteurized eggs to eliminate the risk of residents contracting Salmonella
Enteritidis (SE).
• In accordance with (CDC) and (FDA) standards, SNFs and NFs should not
prepare nor serve soft-cooked, undercooked or sunny-side up eggs from
unpasteurized eggs.
• Surveyors implications: Will look for signed health release agreements
between the resident (or the resident’s representative) and the facility that
acknowledges the resident’s acceptance of the risk of eating undercooked
unpasteurized eggs are not permitted.
– Surveyors can cite this as deficiencies at F371 if fail to comply. Determination of
the appropriate scope and severity shall be based upon the actual or potential
negative resident outcomes in accordance with guidance given at F371.
S&C: 14-35 ALL
May 20, 2014o A “Non-IJ High” category for prioritizing
complaint allegations has been added to Section
5075 of the State Operations Manual (SOM) for
non-long term care (non-LTC).
o It applies to all substantial allegations of
noncompliance (except for immediate jeopardy
(IJ) allegations), and requires a SA complaint
investigation.

7
S&C: 14-36 ALL
May 30, 2014o If State Survey Agencies (SAs) or Accrediting Organizations (AOs) identify
any of the breaches of generally accepted infection control standards listed
below, they should refer them to appropriate State authorities for public
health assessment and management:
– Using the same needle for more than one individual;
– Using the same (pre-filled/manufactured/insulin or any other) syringe, pen or
injection device for more than one individual;
– Re-using a needle or syringe which has already been used to administer
medication to an individual to subsequently enter a medication container (e.g.,
vial, bag), and then using contents from that medication container for another
individual;
– Using the same lancing/fingerstick device for more than one individual, even if
the lancet is changed.
S&C: 14-37 NH
May 30, 2014
– F161 - Assurance of Financial Security
– F202 - Documentation for Transfer and Discharge
– F208 - Admission Policy
– F221 - Physical Restraints
– F278 - Accuracy of
Assessment/Coordination/Certification/Penalty
for Falsification
– F281 - Services Provided Meet Professional
Standards of Quality
– F286 - Maintaining 15 Months of Resident Assessments (Use)
– F332 - Medication Errors/Free of Medication Errors of 5% or Greater
– F333 - Medication Errors/Residents are Free of
Significant Medication Errors
– F371 – Sanitary Conditions
– F387 - Frequency of Physician Visits/Timeliness
of Visits
– F388 - Personal Visits by the Physician
– F390 - Physician Delegation of Tasks in SNFs/Performance of Physician Tasks in NFs
– F425 - Pharmacy Services
– F428 - Drug Regimen Review
– F431 - Service Consultation/Labeling of Drugs
and Biologicals/Storage of Drugs and
Biologicals
– F441 - Infection Control
– F492 - Compliance with Federal, State and
local laws and Professional Standards
– F514 - Clinical Records
– F516 - Resident Identifiable
Information/Safeguard against loss, destruction, or unauthorized use
o Revision of the Interpretive Guidelines and, where appropriate,
Investigative Protocols for the following F Tags to incorporate S&C
policy memos issued from October 2003 through May 2014:
S&C: 14-37 NH
May 30, 2014
o Revisions to SOM Chapter 4: Section 4132.1E
Waiver of Program Prohibition has been revised to
incorporate information consistent with CFR
483.151(c)(1).
o Section 4542.2 State Agency (SA) Expenses for
Training of SA Personnel has been revised to include
Association of Health Facility Survey Agencies
(AHFSA) to the list of annual meetings.

8
S&C: 14-42 NH
August 25, 2014
o Announcement of the release of a free
learning tool on Building Respect for LGBT
Older Adults.
o The learning tool addresses the needs and
rights of older LGBT adults in long term care
(LTC) and is presented in six online training
modules.
S&C: 14-43 NH
August 25, 2014
o Completion of MDS 3.0 Discharge Assessments for
Transfer from Medicare- and/or Medicaid-Certified
Beds to Non-Certified Beds
o Reinforcing the requirement for MDS 3.0 Discharge
assessments to be completed when a resident
transfers from a Medicare- and/or Medicaid-certified
bed to a non-certified bed.
CY2015 PROPOSED
PHYSICIAN FEE SCHEDULE

9
CY2015 Proposed Physician
Fee Schedule• https://www.federalregister.gov/articles/20
14/07/11/2014-15948/medicare-program-
revisions-to-payment-policies-under-the-
physician-fee-schedule-clinical-laboratory
CY2015 Proposed Physician
Fee Schedule• Last year, CMS finalized a separate
payment for a chronic care management
(CCM) code, outside of a face-to-face visit,
for managing the care of Medicare
patients with two or more chronic
conditions beginning in 2015.
• Now CMS is proposing details relating to
the implementation of this new code,
including payment rates.
CY2015 Proposed Physician
Fee Schedule• CMS is proposing a new process for
establishing PFS payment rates that will
be more transparent and allow for greater
public input prior to payment rates being
set.
• Under the proposed process, payment
changes will go through notice and
comment rulemaking before being
adopted beginning for 2016.

10
CY2015 Proposed Physician
Fee Schedule• The proposed rule sets forth changes for
quality reporting programs including, the
Physician Quality Reporting System
(PQRS), Medicare Shared Savings
Program, and Medicare Electronic Health
Record (EHR) Incentive Program, as well
as changes to the Physician Compare tool
on the Medicare.gov website.
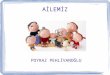
CY2015 Proposed Physician
Fee Schedule• CMS proposes a drop in the current
conversion factor (CF) of $35.8228 down to
$35.7977.
• The Protecting Access to Medicare Act of 2014
(PAMA) replaced the 24 percent reduction in
the PFS with a 0.5 percent update through the
end of this year; however, the law provides a 0
percent update for services furnished on or
after January 1, 2015 through March 31, 2015.
CodeTotal 2015
RVUs
2015
Payment
Rate
(CF=35.79
97)
Total 2014
RVUs
2014
Payment
Rate
(CF=35.82
28)
Percentage
Change
2014-2015
99304 2.57 $92.01 2.61 $93.5 -0.01%
99305 3.67 $131.38 3.72 $133.26 -0.0141%
99306 4.69 $167.9 4.71 $168.73 -0.0049%
99307 1.24 $44.39 1.25 $44.78 -0.0086%
99308 1.94 $69.45 1.93 $69.14 0.0045%
99309 2.56 $91.65 2.54 $90.99 0.01%
99310 3.8 $136.04 3.78 $135.41 0.0046%
99315 2.05 $73.39 2.05 $73.44 -0.0006%
99316 2.96 $105.97 2.94 $105.32 0.0062%
99318 2.7 $96.66 2.69 $96.36 0.0031%
% = (new-old)/old
Estimates for Skilled Nursing Facility Services*
*AMDA

11
Watching Paint Dry
More exciting than this presentation?
CMS FINALIZES FISCAL YEAR 2015
PAYMENT AND POLICY CHANGES
FOR MEDICARE SKILLED NURSING
FACILITIES
CMS-1605-F
CMS-1605-F
• Projects a 2% increase, or $750 million, in
Medicare payments to skilled nursing
facilities (SNFs) in fiscal year (FY) 2015.
• The estimated increase reflects a 2.5%
market basket update, reduced by a 0.5
percentage point multifactor productivity
adjustment required by law.

12
CMS-1605-F
• CMS will use the new OMB delineations to
identify a provider’s urban or rural status
for rate purposes, the fact sheet said. “In
an effort to mitigate the potential negative
wage index impacts for some providers of
the revised OMB delineations," CMS is
implementing a one-year transition by
using a 50-50 blend of the current and
new OMB delineations in FY 2015.
MEDICAID: FINANCIAL CHARACTERISTICS
OF APPROVED APPLICANTS AND
METHODS USED TO REDUCE ASSETS TO
QUALIFY FOR NURSING HOME COVERAGE
GAO-14-473

13
GAO-14-473
• Fourteen percent of Medicaid nursing
home applicants had over $100,000 in
total resources.
• 41% of applicants had total resources—
both countable and not countable as part
of financial eligibility determination—of
$2,500 or less.
• 44% had between $2,501 and $100,000 in
total resources.
GAO-14-473
• median total resources for all approved
applicants was $7,660, which was less
than the median net worth of elderly
households in the United States.
GAO-14-473
• “Although Congress has acted multiple
times to address financial eligibility
requirements for Medicaid coverage of
nursing home care, methods exist through
which individuals, sometimes with the help
of attorneys, can reduce their assets and
qualify for Medicaid…”

14
NURSING FACILITIES' COMPLIANCE WITH
FEDERAL REGULATIONS FOR REPORTING
ALLEGATIONS OF ABUSE OR NEGLECT
OEI-07-13-00010
OEI-07-13-00010
• 85 percent of nursing facilities reported at
least one allegation of abuse or neglect to
OIG in 2012.
• 76 percent of nursing facilities maintained
policies that address Federal regulations
for reporting both allegations of abuse or
neglect and investigation results.
OEI-07-13-00010
• 61 percent of nursing facilities had
documentation supporting the facilities'
compliance with both Federal regulations
under Section 1150B of the Social
Security Act.
• 53 percent of allegations of abuse or
neglect and the subsequent investigation
results were reported, as Federally
required.

15
OEI-07-13-00010
• “We recommend that CMS ensure that
nursing facilities: (1) maintain policies
related to reporting allegations of abuse or
neglect;
• (2) notify covered individuals of their
obligation to report reasonable suspicions
of crimes; and
OEI-07-13-00010
• (3) report allegations of abuse or neglect
and investigation results in a timely
manner and to the appropriate individuals,
as required.
• CMS concurred with all three.
HEALTH CARE FRAUD AND ABUSE
CONTROL PROGRAM
ANNUAL REPORT FOR FISCAL YEAR 2013

16
HCFAC Annual Report for
Fiscal Year 2013• During Fiscal Year (FY) 2013, the Federal
government won or negotiated over $2.6
billion in health care fraud judgments and
settlements.
• It attained additional administrative
impositions in health care fraud cases and
proceedings.
HCFAC Annual Report for
Fiscal Year 2013• FY 2013, approximately $4.3 billion was
deposited with the Department of the
Treasury and the Centers for Medicare &
Medicaid Services (CMS), transferred to
other Federal agencies administering
health care programs, or paid to private
persons during the fiscal year.
HCFAC Annual Report for
Fiscal Year 2013• Of this $4.3 billion, the Medicare Trust Funds
received transfers of approximately $2.85
billion during this period.
• $576 million in Federal Medicaid money was
similarly transferred separately to the
Treasury.
• The HCFAC account has returned over $25.9
billion to the Medicare Trust Funds since the
inception of the Program in 1997.

17
HCFAC Annual Report for
Fiscal Year 2013• In FY 2013, the Department of Justice
(DOJ) opened 1,013 new criminal health
care fraud investigations involving 1,910
potential defendants.
• Federal prosecutors had 2,041 health care
fraud criminal investigations pending,
involving 3,535 potential defendants, and
filed criminal charges in 480 cases
involving 843 defendants.
HCFAC Annual Report for
Fiscal Year 2013• 718 defendants were convicted of health
care fraud-related crimes during the year.
• FY 2013, DOJ opened 1,083 new civil
health care fraud investigations and had
1,079 civil health care fraud matters
pending at the end of the fiscal year.
HCFAC Annual Report for
Fiscal Year 2013• In FY 2013, Federal Bureau of
Investigation (FBI) health care fraud
investigations resulted in the operational
disruption of 425 criminal fraud
organizations and the dismantlement of
the criminal hierarchy of more than 115
criminal enterprises engaged in health
care fraud.

18
HCFAC Annual Report for
Fiscal Year 2013• In FY 2013, HHS’ Office of Inspector General
(HHS-OIG) investigations resulted in 849
criminal actions against individuals or entities
that engaged in crimes related to Medicare and
Medicaid; and 458 civil actions, which include
false claims and unjust-enrichment lawsuits filed
in Federal district court, civil monetary penalties
(CMP) settlements, and administrative
recoveries related to provider self-disclosure
matters.
HCFAC Annual Report for
Fiscal Year 2013• HHS-OIG also excluded 3,214 individuals
and entities.
NINETY DEFENDANTS CHARGED IN
NATIONWIDE MEDICARE FRAUD
STRIKE FORCE OPERATIONS
DOJ Press Release: May 13, 2014

19
DOJ Press Release: May 13,
2014• A multi-state Medicare Fraud Strike Force
takedown has resulted in charges against
90 individuals for their alleged participation
in Medicare fraud schemes involving
approximately $260 million in false billings.
DOJ Press Release: May 13,
2014• The defendants, including 27 doctors, nurses,
and other medical professionals, are charged
with various health care fraud-related crimes,
including conspiracy to commit health care
fraud, anti-kickback violations, and money
laundering.
• A total of 50 defendants were charged in Miami,
FL; 11 were charged in Houston, TX; eight in
Los Angeles, CA; seven in Detroit, MI; seven in
Tampa, FL; and seven were charged in
Brooklyn, NY.
DOJ Release: May 13, 2014
• Defendants allegedly participated in schemes to
submit claims to Medicare for treatments that
were medically unnecessary and often never
provided. Specifically, court documents allege
patient recruiters, Medicare beneficiaries, and
other co-conspirators were paid cash kickbacks
in return for supplying beneficiary information to
providers, so the providers could then submit
fraudulent bills to Medicare.

20
MEDICARE CONTRACTORS NEED
MORE OVERSIGHT, GUIDANCE TO
CURB DUPLICATIVE AUDITS
(GAO-14-474)
(GAO-14-474)
• In a report issued August 13, the
Government Accountability Office (GAO)
states that the Centers for Medicare &
Medicaid Services (CMS) needs to
improve its oversight of and guidance to
Medicare contractors to avoid duplicative
postpayment claims reviews that are
administratively burdensome to providers.
(GAO-14-474)
• CMS also should standardize the requirements
for corresponding with providers during the
postpayment claims review process across the
four contractor types—Medicare Administrative
Contractors (MACs), Zone Program Integrity
Contractors (ZPIC), Recovery Audit Contractors
(RACs), and the Comprehensive Error Rate
Testing (CERT) contractors—and then regularly
assess compliance with those requirements,
GAO said.

21
ENFORCEMENT ACTIONS
• 08-22-2014
• After it self-disclosed conduct to OIG, Rolling
Hills H.C., Inc. and Fountain Lake Health and
Rehab, Inc. (Rolling Hills and Fountain Lake),
Arkansas, agreed to pay $117,748.32 for
allegedly violating the Civil Monetary Penalties
Law. OIG alleged that Rolling Hills and Fountain
Lake employed two individuals that it knew or
should have known were excluded from
participation in Federal health care programs.
• 08-24-2014
• After it self-disclosed conduct to OIG, the
City of Baytown, Texas, agreed to pay
$29,431.43 for allegedly violating the Civil
Monetary Penalties Law. OIG alleged that
the City of Baytown employed an
individual that it knew or should have
known was excluded from participation in
Federal health care programs.

22
• 08-24-2014
• Rock Rapids Health Centre (RRHC), a skilled nursing
facility located in Iowa, entered into a settlement
agreement with the Office of Inspector General (OIG) for
the Department of Health and Human Services, effective
August 24, 2014. The settlement resolves allegations
that RRHC employed an individual who was excluded
from participating in any Federal health care programs.
The excluded individual provided items and services to
RRHC patients that were billed to Federal health care
programs.
2015 Winter Forecast
Better than this presentation?
CASE LAW

23
Foundation Health Services,
Inc.• Foundation Health Services, Inc. (FHS), its
affiliated nursing facilities, and its president
and chief executive officer Richard Daspit,
Sr., have agreed to pay $750,000 to the
United States and the State of Maryland to
resolve allegations that they submitted false
claims for payment to Medicaid and Medicare
for materially substandard and/or worthless
skilled nursing facility services.
Foundation Health Services,
Inc.• The settlement resolves allegations that
between 2006 and 2010, some of the skilled
nursing services provided at several nursing
facilities managed by FHS were materially
substandard and/or worthless.
• As a result of these failures of care, some
residents allegedly suffered from falls, fractures,
head injuries; malnutrition; dehydration;
pressure sores and infections.
Foundation Health Services,
Inc.• FHS failed to (a) follow appropriate fall protocols; (b)
follow appropriate pressure ulcer and infection control
protocols; (c) properly administer medications to avoid
medication errors; (d) appropriately provide for activities
of daily living including bathing, monitoring, feeding and
supervising for some residents; (e) provide appropriate
mental health treatment; (f) answer call lights promptly;
(g) employ a sufficient number and skill-level of nursing
staff to adequately care for the residents; and (h) provide
a habitable living environment, adequate equipment and
needed capital expenditures.

24
United States ex rel. Absher v.
Momence Meadows Nursing Ctr, Inc.
• On August 20, 2014, the Seventh Circuit
overturned a $9 million jury verdict and
cast doubt on the efforts to pursue similar
cases in which a business allegedly
provides services of diminished, but still
some, value.
United States ex rel. Absher v.
Momence Meadows Nursing Ctr, Inc.
• In 2004, former nurses of the facility, filed
a qui tam (or whistleblower) complaint
alleging that the facility defrauded the
government by providing substandard
services to the patients while seeking
reimbursement for patient care of higher
value. While still under seal, the complaint
was amended multiple times through
2009.
United States ex rel. Absher v.
Momence Meadows Nursing Ctr, Inc.
• The government declined to intervene and
the district court unsealed the complaint.
• The relators went forward with the case.
• The relators presented evidence of a host
of shortcomings and noncompliance at
Momence relating to infection control,
cleanliness, food and water temperature,
administration, patient care, and others
issues.

25
United States ex rel. Absher v.
Momence Meadows Nursing Ctr, Inc.
• The jury ruled in favor of the relators,
finding over 1,700 false claims and
awarding compensatory damages over $3
million and fines of over $19 million.
• With treble damages—resulted in an
award of over $9 million. The court
separately vacated the fines imposed by
the jury based on the Eighth Amendment’s
Excessive Fines clause.
United States ex rel. Absher v.
Momence Meadows Nursing Ctr, Inc.
• The worthless services theory—adopted
by the Second, Eighth, and Ninth
Circuits—allows a qui tam relator to bring
claims for violations of the FCA premised
on the theory that the defendant received
reimbursement for products or services
that were worthless.
United States ex rel. Absher v.
Momence Meadows Nursing Ctr, Inc.
• In Absher, the district court had instructed
the jury that “[s]ervices can be worthless,
and the claims for those services can, for
that reason be false, even if the nursing
facility in fact provided some services to
the patient.
• To find the services worthless, you do not
need to find that the patient received no
services at all.”

26
United States ex rel. Absher v.
Momence Meadows Nursing Ctr, Inc.
• Seventh Circuit rejected the district court’s
instruction.
• For the worthless services theory to apply, the
“performance of the service [must be] so
deficient that for all practical purposes it is the
equivalent of no performance at all.”
• “[i]t is not enough to offer evidence that the
defendant provided services that are worth
some amount less than the services paid for.
That is, a ‘diminished value’ of services theory
does not satisfy this standard.”
United States ex rel. Absher v.
Momence Meadows Nursing Ctr, Inc.
• “services that are ‘worth less’ are not
‘worthless.’”
PROPOSED NURSING HOME
ADMINISTRATOR RULES

27
Proposed Nursing Home
Administrator Rules• National Association of Long Term Care
Administrator Boards (NAB), has member
organizations in 50 states and the District
of Columbia.
• NAB is encouraging its member
0rganizations to move toward requiring a
minimum of a bachelor’s degree as a
condition for licensure as a nursing home
administrator.
Proposed Nursing Home
Administrator Rules• The NAB has taken this position because practice as a
nursing home administrator has become more
complex and requires, at a minimum, the education
and training consistent with a bachelor’s degree.
• 28 states that require a bachelor’s degree for licensure
as a nursing home administrator.
• 45 states that require applicants pass the NAB
national licensing examination.
• 28 states that require applicants pass a state licensing
examination.
Proposed Nursing Home
Administrator Rules• MCL 333.17309 would require a statutory
amendment to allow the Department to
require a Bachelor’s degree.
• The proposed rules will clarify the
continuing education requirements for
nursing home administrators in Michigan,
which are comparable to the requirements
established by the other states in the
Great Lakes region.

28
Proposed Nursing Home
Administrator Rules• Have been employed as a chief executive or
administrative officer at a Michigan-licensed
hospital for not less than 5 of the 7 years
immediately preceding the date of applying for a
nursing home administrator license, as provided
in MCL 333.17309(3) of the code.
• Pass the national nursing home administrators
licensing examination and the Michigan nursing
home administrators licensing examination.
BENEFICIARY AND FAMILY-
CENTERED CARE (BFCC) QIO
CONTACTOR FOR MICHIGAN
KEPRO
KEPRO
• The new QIN-QIO contract is part of an effort by
CMS to re-structure its QIO program that
historically combined Medicare beneficiary quality
of care case reviews, discharge/discontinuation of
service appeals and quality improvement services
at a single organization in each state or territory.
Under the new structure, beneficiary quality of
care case reviews and appeals have been
separated from quality improvement services and
cannot be administered by the same organization.

29
KEPRO
• Beginning Aug. 1, 2014, KEPRO, based in
Ohio, will handle Medicare quality of care
case reviews, discharge/discontinuation of
service and other related review services
for Michigan, Minnesota and Wisconsin.
KEPRO
• Hospital Discharge QIO Request for
Review
– If you believe you are not medically ready to
go home from the hospital
– If you have a legitimate medical reason to
continue receiving a medical service
– If you have not received clear discharge
instructions
KEPRO
• Other Medicare QIO Requests for
Review
– You may request a QIO review if you disagree
with the decision of skilled nursing facility,
comprehensive outpatient rehabilitation
facility, home health agency, or hospice to
discharge you.

30
KEPRO
• Quality of Care Complaints
• If you believe you are not receiving the care you
need, you have the right to file a quality of care
complaint. Some common complaints include:
– Wrong medication
– Unnecessary surgery or diagnostic testing
– Inadequate care or misdiagnosis by any
Medicare hospital or doctor
– Early discharge from a health care facility
KEPRO
• To complete a Medicare Consumer QIO
Request for Review or file a complaint:
Contact KEPRO toll-free at 1-855-408-
8557. TTY 1-855-843-4776.
• www.keproqio.com.
LEADINGAGE MICHIGAN
SNF REGULATORY DAY
September 17, 2014
Kitch Drutchas Wagner Valitutti & Sherbrook2379 Woodlake Drive, Suite 400
Okemos, Michigan 48864517.381.7192
www.kitch.com


















![[SNF] NyanKoi_cp04](https://img.pdfslide.net/doc/110x75/568bf1191a28ab893391f463/snf-nyankoicp04.jpg)








![HHAR-LEADINGAGE NY-FINAL.ppt [Read-Only]](https://img.pdfslide.net/doc/110x75/617fa0b28043407fc520780d/hhar-leadingage-ny-finalppt-read-only.jpg)