Embed Size (px)
Citation preview

Lecture 2: Labour & its problems
Dr.Nassrin Malik Aubead

Objectives
-Describe the principles of labour.
-Describe in outline the most common lie , fetal presentations and positions.
-Describe the principles of inducing labour
-Describe how the physiological state of the fetus may be monitored during
labour
-Describe, in principle, how delivery may be facilitated by intervention.
-Describe the processes which normally limit maternal blood loss after birth.
-Describe the causes of post partum haemorrhage

Progress of labour is depend on three variables (3 P):-
1-The powers, i.e.the efficiency of uterine contractions.
2-The passages,i.e, the uterus, cervix, and the bony pelvis.
3-The passenger, i.e.,the fetus( with particular respect to the size ,
presentation, and position ).





Pelvic outlet

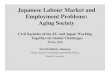
The Passenger
• The size and presentation of the fetus is critical in labour. The
orientation of the head of the fetus when entering the pelvis (in a cephalic
delivery) is variable and as such the head diameter of the fetus varies in
different positions.


0

Attitude
13.5

Presentation : refers to the part of the fetus that is lowermost within the
maternal pelvis like normal presentation (vertex)
Malpresentation (Abnormal presentations ) :any presentation other than the
vertex and therefore includes brow , face, breech ,shoulder, compound
presentations and cord presentation.

Position: Refers to the relation ship between the dominator of the fetal presenting part relative to the maternal pelvis land marks.
Dominator

also known as extended breech) presentation with
extension of the legs
breech presentation with flexion of the legs
What are the incidence & risk factors for breech presentation?
The majority of persistent breech presentations recognized antenatally
are delivered by Caesarean section to avoid fetal risks. However there is
still a place for the vaginal delivery of a breech presentation(e.g
maternal choice and the failure to detect breech presentation until very
late in labour).
Why vaginal beech delivery is risky?

Assessment of Progress of labour
PARTOGRAM is a graphical information about the progress of labour in which the
salient information about the fetal wellbeing, maternal well-being and the
progress of labour are recorded into a chart.
Partogram helps to identify at an early stage those women whose labour is slow.


Failure to progress in labour may be due to:
• Inadequate Power
– Insufficient uterine contraction
• Inadequate Passage
– Abnormal bony pelvis
– Rigid perineum
• Abnormalities of the Passenger
– Fetus too big
– Abnormal fetal presentation (malpresentation) e.g breech, brow, face.
– Abnormal fetal position (malposition) e.g occiput posterior.

Indications
MATERNAL
• Preeclampsia, eclampsia
•PROM, Chorioamnionitis.
•Prolonged pregnancy(usually
offered after 41 completed weeks) -
•Unexplained antepartum
haemorrhage.
•Medical conditions: Intrahepatic
cholestasis of pregnancy.
•Deteriorating maternal illness: DM,
Heart ds, Renal ds,Chr. HT etc.
•Social’ reasons.
FETAL
• IUFD
• Fetal anomaly
incompatible with life
• Severe IUGR
• Rh-isoimmunisation
•Twin pregnancy continuing beyond 38
weeks.
• Macrosomia
The principles of inducing labour

METHODS OF INDUCTION
Breast/nipple stimulation
Sexual intercourse
Membrane stripping
Amniotomy or ARM
Acupuncture/acupressure
Balloon catheters
Lamineria tents
Synthetic osmotic dilators
" Herbs, evening primrose oil
" Homeopathic prep
" Enemas
" Castor oil
" Oxytocin
" Prostaglandins –
PGE2,Misoprostol
" Relaxin
" Nitric oxide donors
" mifepristone
CHEMICAL NONHORMONAL NATURAL
MECHANICAL HORMONAL
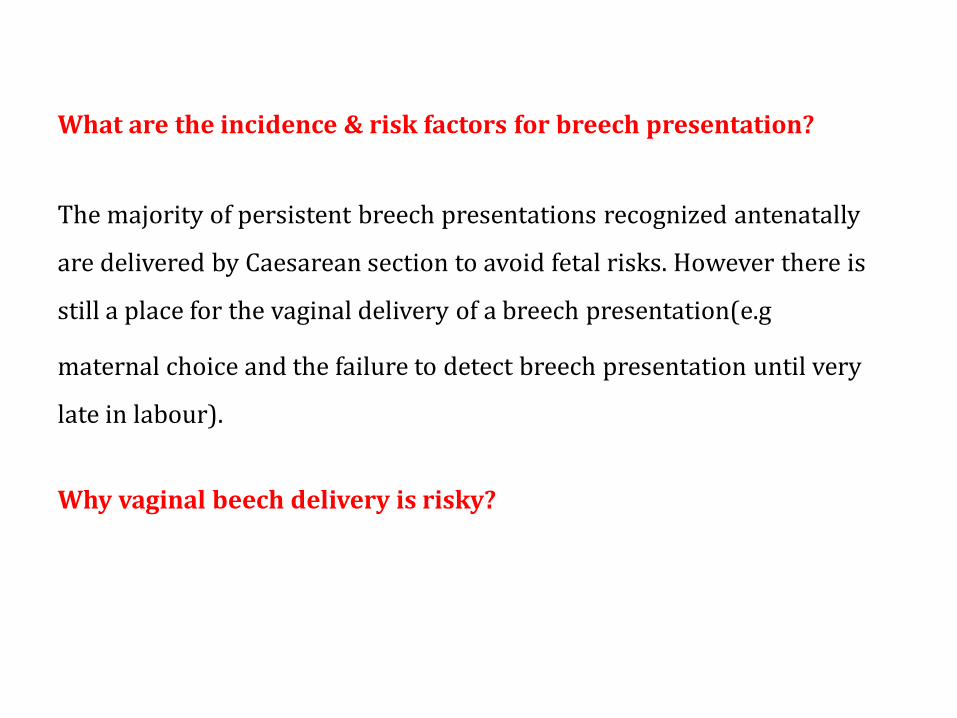
Monitoring the physiological state of the fetus during labour:
During labour fetal heart rate can be assessed using either:
External monitoring by:
- A Pinard stethoscope .
- A handheld Doppler ultrasound.
- Continuous external electronic fetal
monitoring (EFM) using CTG.
or
Internal monitoring by :
Fetal Scalp Electrode
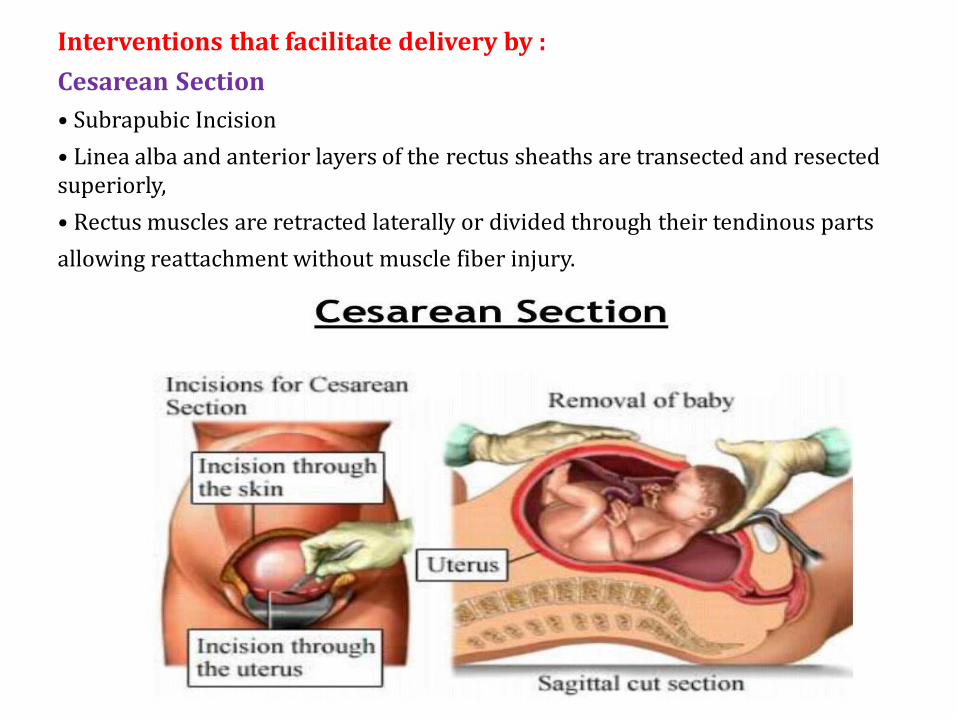
Interventions that facilitate delivery by :
Cesarean Section
• Subrapubic Incision
• Linea alba and anterior layers of the rectus sheaths are transected and resected superiorly,
• Rectus muscles are retracted laterally or divided through their tendinous parts
allowing reattachment without muscle fiber injury.

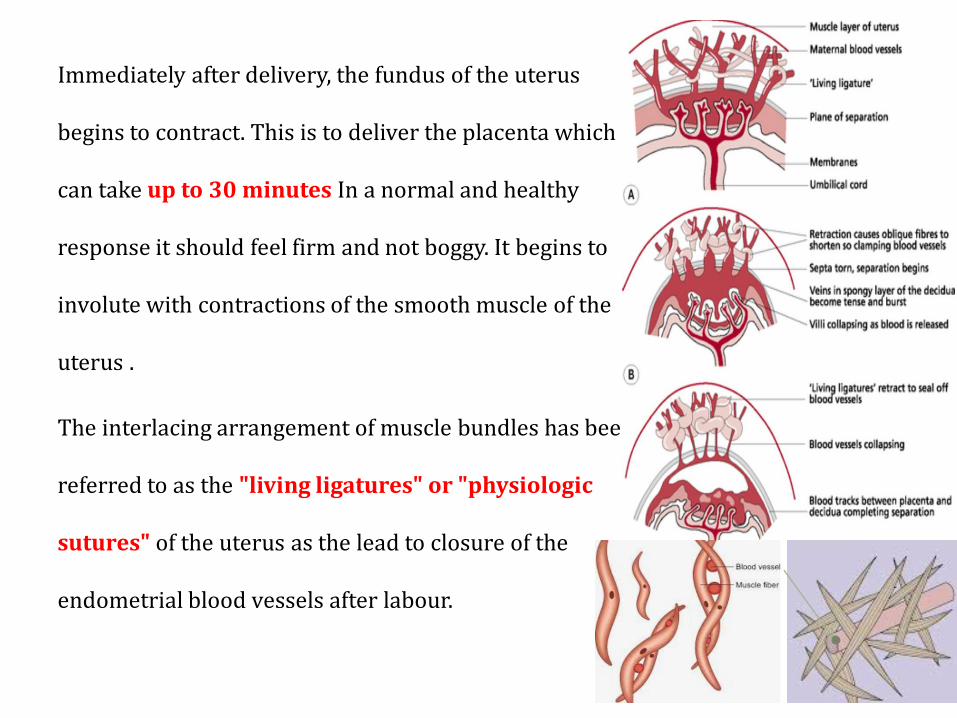
Immediately after delivery, the fundus of the uterus
begins to contract. This is to deliver the placenta which
can take up to 30 minutes In a normal and healthy
response it should feel firm and not boggy. It begins to
involute with contractions of the smooth muscle of the
uterus .
The interlacing arrangement of muscle bundles has been
referred to as the "living ligatures" or "physiologic
sutures" of the uterus as the lead to closure of the
endometrial blood vessels after labour.

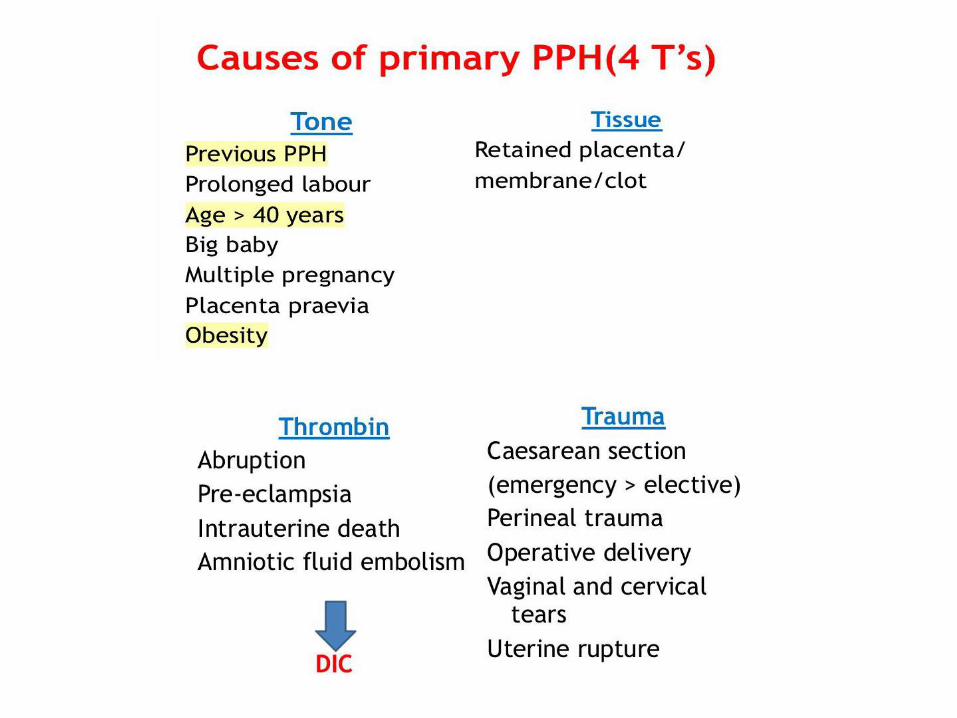
Postpartum haemrrhage
• Primary PPH – blood loss of 500ml or more within 24hours of
delivery.
• Secondary PPH – significant blood loss between 24 hours and 6
weeks after birth.
Why do we care?
Obstetric haemorrhage – more than 1000ml Very rapidly lead to maternal death.
Major obstetric haemorrhage is defined as blood loss ≥2,500 ml, or requiring a blood transfusion ≥5 units red cells or treatment for coagulopathy
Causes of secondary PPH:
-Uterine infection – (known as endometritis).
- Infection of the vaginal or cervical tears.
-Retained placental fragments or tissue
-Abnormal involution of the placental site (inadequate closure and sloughing of
the spiral arteries at the placental attachment site).
-Uterine fibroid, endometrial polyp.
-Undiagnosed cervical carcinoma.
-Blood diseases.
-Trophoblastic disease (very rare).

Puerperial Pyrexia
- A clinical sign that merits careful investigation.
- A temperature of 38 C° more on any 2 occasion in the first 10 days after delivery
excluding the first 24 hr.
CAUSES:
1. Urinary tract infection
2. Genital tract infection
3. Breast infection (mastitis, abscess)
4. Deep vein thrombosis or pulmonary embolism
5. Respiratory infection
6. Other non-obstetrics causes
7. Surgical wounds e.g. C.S














![Syllabus for€¦ · 1.4 Agricultural Management- Concept, Recent trends and Problems. [15] II Agriculture Labour and Efficiency 2.1 Problems of Agriculture Labour 2.2 Impact of Mechanization](https://img.pdfslide.net/doc/110x75/5faf3a0f38c02e20f1613cb5/syllabus-for-14-agricultural-management-concept-recent-trends-and-problems-15.jpg)