Embed Size (px)
Citation preview



Lecture Notes: Tropical Medicine

This book is dedicated to Dr Dion Bell, author
and later editor of the first four editions of this
book, a gifted teacher of tropical medicine,
and an inspiration to generations of doctors
working in the tropics.

Lecture Notes
Tropical Medicine
EDITED BY
Geoff GillProfessor of International MedicineLiverpool School of Tropical MedicineLiverpool, UK
Nick BeechingSenior Lecturer in Infectious DiseaseLiverpool School of Tropical MedicineLiverpool, UK
Sixth Edition
A John Wiley & Sons, Ltd., Publication

This edition first published 2009, © 2009 by Blackwell Publishing LtdPrevious editions: 1981, 1985, 1990, 1995, 2004
Blackwell Publishing was acquired by John Wiley & Sons in February 2007. Blackwell’s publishing program has been merged with Wiley’s global Scientific, Technical and Medical business to form Wiley-Blackwell.
Registered office: John Wiley & Sons Ltd, The Atrium, Southern Gate, Chichester, West Sussex, PO19 8SQ , UK
Editorial offices: 9600 Garsington Road, Oxford, OX4 2DQ , UK The Atrium, Southern Gate, Chichester, West Sussex, PO19 8SQ , UK 111 River Street, Hoboken, NJ 07030-5774, USA
For details of our global editorial offices, for customer services and for information about how to apply for permission to reuse the copyright material in this book please see our website at www.wiley.com/wiley-blackwell
The right of the author to be identified as the author of this work has been asserted in accordance with the Copyright, Designs and Patents Act 1988.
All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in any form or by any means, electronic, mechanical, photocopying, recording or otherwise, except as permitted by the UK Copyright, Designs and Patents Act 1988, without the prior permission of the publisher.
Wiley also publishes its books in a variety of electronic formats. Some content that appears in print may not be available in electronic books.
Designations used by companies to distinguish their products are often claimed as trademarks. All brand names and product names used in this book are trade names, service marks, trademarks or registered trademarks of their respective owners. The publisher is not associated with any product or vendor mentioned in this book. This publication is designed to provide accurate and authoritative information in regard to the subject matter covered. It is sold on the understanding that the publisher is not engaged in rendering professional services. If professional advice or other expert assistance is required, the services of a competent professional should be sought.
Library of Congress Cataloging-in-Publication Data
Lecture notes. Tropical medicine. — 6th ed. / [edited by] Geoff Gill, Nick Beeching. p. ; cm. Rev. ed. of: Lecture notes on tropical medicine. 5th ed. 2004. Includes bibliographical references and index. ISBN 978-1-4051-8048-1 1. Tropical medicine. I. Gill, Geoffrey V. II. Beeching, N. III. Lecture notes on tropical medicine. IV. Title: Tropical medicine. [DNLM: 1. Tropical Medicine. WC 680 L471 2009]RC961.L42 2009616.9’883 —dc22 2008042562
ISBN: 978-1-4051-8048-1
A catalogue record for this book is available from the British Library.
Set in 8/12 pt Stone Serif by Charon Tec Ltd (A Macmillan Company), Chennai, IndiaPrinted in Singapore
1 2009
Contributors, vii
Preface, ix
List of Abbreviations, x
New Drug Names, xiii
Part 1: A General Approach to Syndromes/Symptom Complexes
1 Gastrointestinal presentations 3
2 Respiratory presentations 11
3 Neurological presentations 17
4 Febrile presentations 26
5 Dermatological presentations 32
6 The patient with anaemia 36
7 A syndromic approach to sexually
transmitted infections 40
8 Splenomegaly in the tropics 49
Part 2: Major Tropical Infections
9 Malaria 55
10 Visceral leishmaniasis 73
11 Cutaneous leishmaniasis 80
12 Tuberculosis 85
13 HIV infection and disease in the tropics 101
14 Onchocerciasis, filariasis and loiasis 133
15 African trypanosomiasis 148
16 South American trypanosomiasis—
Chagas’ disease 155
17 Schistosomiasis 158
18 Leprosy 171
Part 3: Other Tropical Diseases
Gastrointestinal
19 Amoebiasis 185
20 Bacillary dysentery 192
21 Cholera 195
22 Giardiasis and other intestinal protozoal
infections 199
23 Intestinal cestode infections (tapeworms)
including cysticercosis 204
24 Soil-transmitted helminths 208
25 Viral hepatitis 215
26 Liver and intestinal flukes 226
27 Hydatid disease 229
Respiratory
28 Pneumonia 233
29 Lung flukes 241
30 Tropical pulmonary eosinophilia 244
Neurological
31 Pyogenic meningitis 246
32 Cryptococcal meningitis 254
33 Encephalitis 256
34 Acute flaccid paralysis 261
35 Spastic paralysis 264
36 Rabies 267
37 Tetanus 272
Fever
38 Brucellosis 275
39 Typhoid and paratyphoid fevers 280
40 Arboviruses 287
41 Viral haemorrhagic fevers 289
42 Dengue and yellow fever 296
43 Relapsing fevers 301
44 Rickettsial infections 304
45 Leptospirosis 306
46 Melioidosis 309
Miscellaneous
47 Tropical ulcer 311
48 Buruli ulcer 313
49 Myiasis 316
50 Cutaneous larva migrans 318
51 Scabies and lice 320
52 Strongyloidiasis 322
v
Contents

53 Guinea worm infection (dracunculiasis) 326
54 Histoplasmosis 328
55 Other fungal infections 330
56 Haemoglobinopathies and red cell
enzymopathies 333
57 Haematinic deficiencies 338
58 Bites and stings 342
59 Non-communicable diseases 347
60 Refugee health 365
61 Syndromes of malnutrition 373
Index 380
Contents
vi

Imelda Bates Senior Lecturer, Liverpool School of
Tropical Medicine, Pembroke Place, Liverpool
L3 5QA
Chapters 6, 8, 56, 57
Nick Beeching Senior Lecturer, Liverpool
School of Tropical Medicine, Pembroke Place,
Liverpool L3 5QA; Clinical Lead, Tropical &
Infectious Disease Unit, Royal Liverpool
University Hospital, Liverpool L7 8XP
Chapters 1, 5, 18, 25, 29, 31, 38, 53
Tom Blanchard Honorary Senior Lecturer in
Infection & Immunity, University of Liverpool;
Honorary Fellow, Liverpool School of Tropical
Medicine; Consultant in Infectious Diseases &
Tropical Medicine, North Manchester General
Hospital, Delaunays Rd, Manchester M8 5RB
Chapter 4
Martin Dedicoat Chief Specialist Physician,
Polokwane Mankweng Hospital Complex,
Polokwane, Limpopo 0700, South Africa
Chapter 13
Tom Doherty Senior Lecturer, London School
of Hygiene & Tropical Medicine, London
WC1E 7HT; Consultant Physician, Hospital
for Tropical Diseases, Mortimer Market Centre,
Capper Street, London WC1E 6AU
Chapter 61
Neil French Director, Karonga Prevention Study,
Box 46, Chilumba, Malawi; Reader in
Infectious Disease Epidemiology, London
School of Hygiene & Tropical Medicine,
London WC1E 7HT
Chapters 2, 28, 30
Geoff Gill Professor, Liverpool School of Tropical
Medicine, Pembroke Place, Liverpool L3 5QA;
and Honorary Consultant Physician, Aintree
University Hospital, Liverpool L9 1AE
Chapters 44, 47, 49–52, 54, 59
Stephen Gordon Senior Lecturer, Liverpool
School of Tropical Medicine, Pembroke Place,
Liverpool L3 5QA
Chapters 2, 28, 30
Rachel Kneen Consultant Paediatric Neurologist,
Alder Hey Children’s NHS Foundation Trust,
Alder Hey, Liverpool L12 2AP
Chapters 3, 33, 34
David Lalloo Clinical Director and Reader,
Liverpool School of Tropical Medicine,
Pembroke Place, Liverpool L3 5QA
Chapters 15, 16, 32, 37, 46, 55, 58
Diana Lockwood Professor, London School of
Hygiene & Tropical Medicine, London WC1E
7HT; Consultant Physician and Leprologist,
Hospital for Tropical Diseases, Mortimer Market
Centre, Capper Street, London WC1E 6AU
Chapter 18
Alastair Miller Honorary Fellow, Liverpool
School of Tropical Medicine; Consultant
Physician, Tropical & Infectious Disease Unit,
Royal Liverpool University Hospital, Liverpool
L7 8XP
Chapter 45
Malcolm Molyneux Professor, Liverpool
School of Tropical Medicine, Pembroke Place,
Liverpool L3 5QA
Chapter 9
vii
Contributors

Tim O’Dempsey Senior Lecturer, Liverpool
School of Tropical Medicine, Pembroke Place,
Liverpool L3 5QA
Chapters 10, 11, 14, 19, 20, 22–24, 26, 27,
43, 48, 60
Chris Parry Senior Lecturer, Department of
Medical Microbiology and Genitourinary
Medicine, University of Liverpool, Duncan
Building, Liverpool L69 3GA
Chapter 39
Paul Shears Consultant Microbiologist, Sheffield
Teaching Hospitals NHS Foundation Trust,
Sheffield S10 2JF
Chapter 21
Rebecca Sinfield Clinical Lecturer, Child and
Reproductive Health, Liverpool School of
Tropical Medicine, Pembroke Place, Liverpool
L3 5QA
Chapter 61
Tom Solomon Professor, Division of Neurological
Science, University of Liverpool, Liverpool L9 7LJ
Chapters 3, 33–36, 40–42
Bertie Squire Reader, Liverpool School of
Tropical Medicine, Pembroke Place, Liverpool
L3 5QA
Chapters 12, 17
Miriam Taegtmeyer Senior Lecturer, Liverpool
School of Tropical Medicine, Pembroke Place,
Liverpool L3 5QA
Chapters 7, 13
Maureen Wilkinson Consultant Psychiatrist,
Cheshire and Wirral Partnership NHS
Foundation Trust, Countess of Chester Health
Park, Chester CH2 1BQ
Chapter 59
Contributors
viii

The first edition of Lecture Notes in Tropical
Medicine was published in 1981, conceived and
entirely written by Dr Dion Bell of the Liverpool
School of Tropical Medicine. It rapidly became
a highly successful ‘classic’ due to its practical,
authoritative and entertaining style. The next
two editions continued as single author books,
but by the time of the fourth edition in 1994,
the spectrum of tropical disease had consider-
ably expanded—HIV/AIDS in particular had
become a major health problem. In view of this,
other authors from the Liverpool School became
involved to cover specific topics.
Dion Bell was one of the greatest tropical physi-
cians and teachers of his time, and it has been a
privilege for us to take over editorship of this book
following his retirement and sadly his subsequent
death. In the fifth edition, we continued the proc-
ess of multi-authorship, though all contributors
were either staff of the Liverpool School of Tropical
Medicine or teachers on the Liverpool DTM&H
course. We also introduced syndromic chapters on
fever, splenomegaly, skin problems, etc., as well as
new chapters on the emerging problems of non-
communicable diseases and refugee health.
In this, the sixth edition, all chapters have
been updated, and a new chapter on nutritional
syndromes has been added, and a section on
mental health has been included in the chapter
on non-communicable diseases. We continue
to use bullet points, tables and boxes, and lists
of recommended reading, including websites.
We say goodbye in this edition to three valued
retiring authors Professor Charlie Gilks, Dr Fred
Nye, and Dr George Wyatt and welcome to our
team Dr Tom Doherty, Dr Rebecca Sinfield and
Dr Maureen Wilkinson.
As well as continuing the style and philoso-
phy of Lecture Notes in Tropical Medicine begun by
Dr Dion Bell 28 years ago, we have also continued
the same financial arrangements with the pub-
lishers. No author or editor of the book has ever
accepted payment and all royalties are paid to the
Liverpool School and used to award medical stu-
dent bursaries for elective periods in the tropics.
We hope that this new edition is useful to both
students and practitioners of tropical medicine. As
always, we welcome any comments and criticisms.
Geoff Gill
Nick Beeching
Liverpool, UK
ix
Preface

x
AAFB acid- and alcohol-fast bacilli
Ab antibody
ABC abacavir
ACE angiotensin-converting enzyme
ACR adequate clinical response
ADLA acute dermatolymphangioadenitis
AFB acid-fast bacilli
AFL acute filarial lymphangitis
Ag antigen
AgB antigen B
AIDP acute inflammatory demyelinating
polyneuropathy
AIDS acquired immune deficiency syndrome
ALA amoebic liver abscess
ALB albendazole
AMAN acute motor axonal neuropathy
APOC African Programme for Onchocerciasis
Control
ARC AIDS-related complex
ARI annual risk of infection
ART antiretroviral therapy
ARV antiretroviral drug
AZT zidovudine
BB borderline leprosy
BCG bacille Calmette–Guérin
b.d. twice daily
BI bacterial index
BL borderline lepromatous leprosy
BMI body mass index
BP blood pressure
b.p.m. beats per minute
BT borderline tuberculoid leprosy
cAMP cyclic adenosine monophosphate
CATT card agglutination test for trypanosomes
CBT cognitive behaviour therapy
CCHF Crimean–Congo haemorrhagic fever
ComDT Community directed treatment with
ivermectin
CFT complement fixation test
CHE complex humanitarian emergency
CHK chikungunya virus
CIATT card indirect agglutination test for
trypanosomes
CL cutaneous leishmaniasis
CM cryptococcal meningitis
CMI cell-mediated immunity
CMR crude mortality rate
CMV cytomegalovirus
CNS central nervous system
COPD chronic obstructive pulmonary disease
CRP C-reactive protein
CSF cerebrospinal fluid
CT computerized tomography
CTC community based therapeutic care
CTF Colorado tick fever
CVP central venous pressure
CXR chest x-ray
DAT direct agglutination test
d4T stavudine
DCL diffuse cutaneous leishmaniasis
ddi didanosine
DD5 double diffusion test for arc 5
DEN dengue virus
DDS 4,4-diaminodiphenylsulphone
DDT dichlorodiphenyl-trichloroethane
DEC diethylcarbamazine citrate
DF dengue fever
DHF dengue haemorrhagic fever
DHFR dihydrofolate reductase
DHPS dihydropteroate synthetase
DIC disseminated intravascular coagulation
DKA diabetic ketoacidosis
DOT directly observed therapy
DOTS directly observed short course therapy
DSS dengue shock syndrome
DTH delayed-type hypersensitivity
List of Abbreviations

xi
DTM&H diploma in tropical medicine and
hygiene
DTP diptheria, tetanus and pertussis
EBV Epstein–Barr virus
ECG electrocardiogram
EEE eastern equine encephalitis
EEG electroencephalography
EFV efavirenz
EIA enzyme immunoassay
EITB enzyme-linked immunoelectrotransfer blot
ELISA enzyme-linked immunoabsorbent assay
EMF endomyocardial fibrosis
ENL erythema nodosum leprosum
EPI extended programme of immunization
ERCP endoscopic retrograde
cholangiopancreatography
ESR erythrocyte sedimentation rate
ETF early treatment failure
FAR fever–arthralgia–rash
FBC full blood count
FCPD fibrocalculous pancreatic diabetes
FES fasciola excretory–secretory
FEV1 forced expiratory volume in 1 second
FGM female genital mutilation
FGT formol gel test
FTC emtricitabine
FUO fever of unknown origin
FVC forced vital capacity
G6PD glucose-6-phosphate dehydrogenase
GABA γ-aminobutyric acid
GAELF Global Alliance for the Elimination of
Lymphatic Filariasis
GAVI Global Alliance for Vaccines and
Immunization
GBS Guillain-Barré syndrome
GCS Glasgow coma score
GDP gross domestic product
GTT glucose tolerance test
HAART highly active antiretroviral therapy
HAV hepatitis A virus
HbA adult haemoglobin
HbF fetal haemoglobin
HbS sickle haemoglobin
HBeAg hepatitis B ‘e’ antigen
HBIg hepatitis B immunoglobulin
HBsAg hepatitis B surface antigen
HBV hepatitis B virus
HCC hepatocellular carcinoma
HCV hepatitis C virus
HDCV human diploid cell vaccine
HDV hepatitis D virus
HEV hepatitis E virus
HFRS haemorrhagic fever with renal
syndrome
Hib Haemophilus influenzae type b
HIV human immunodeficiency virus
HLA human leucocyte antigen
HNK hyperosmolar non-ketotic coma
HPV human papilloma virus
HTLV-1 human T lymphotrophic virus type 1
HUS haemolytic uraemic syndrome
ICT immunochromatographic card test
IDP internally displaced person
IFAT indirect fluorescent antibody test
IFN interferon
Ig immunoglobulin
IGRA interferon gamma release assays
IL interleukin
i.m. intramuscular
IMAI Integrated Management of Adult Illness
strategy
IMCI Integrated Management of Childhood
Illness strategy
INR international normalized ratio
IPT intermittent presumptive therapy
IRD immune reconstitution disease
IRIS immune reconstitution inflammatory
syndrome
i.v. intravenous
IVDU intravenous drug use
IVM ivermectin
JEV Japanese encephalitis virus
KS Kaposi’s sarcoma
LACV La Crosse virus
LBRF louse-borne relapsing fever
LED light emitting diode
LF lymphatic filariasis
LL lepromatous leprosy
LP lumbar puncture
LR leishmaniasis recidivans
LRTI lower respiratory tract infection
LTF late treatment failure
MAEC minianion exchange column technique
MAT microscopic agglutination test
List of Abbreviations

xii
MCH mean corpuscular haemoglobin
MCHC mean corpuscular haemoglobin
concentration
MCL mucocutaneous leishmaniasis
MCV mean corpuscular volume
MDR multidrug resistant
MDT multidrug therapy
Mf/mL microfilariae per millilitre
MHCT microhaematocrit
ML mucosal leishmaniasis
MMDM malnutrition-modulated diabetes
mellitus
MOTT mycobacteria other than tuberculosis
MRDM malnutrition-related diabetes mellitus
MRI magnetic resonance imaging
MSF Médecins sans frontières
MTB Mycobacterium tuberculosis
MTCT mother to child transmission
MUAC mid-upper arm circumference
MVE Murray Valley encephalitis
NCD non-communicable disease
NGO non-governmental organizations
NK natural killer
NNN Novy, MacNeal and Nicolle’s medium
NNRTI non nucleoside reverse transcriptase
inhibitor
NRTI nucleoside reverse transcriptase inhibitor
NSAID non-steroidal anti-inflammatory drug
NTS non-typhi Salmonella
NVP nevirapine
OCP Onchocerciasis Control Programme
OEPA Onchocerciasis Elimination Program for
the Americas
OLM ocular larva migrans
ONN o’nyong nyong virus
ORS oral rehydration solution
ORT oral rehydration therapy
OTF outpatient treatment facility
OTP outpatient therapeutic programme
PAS periodic acid–Schiff
PCECV purified primary chick embryo cell vaccine
PCP Pneumocystis jirovecii (formerly P carinii)
pneumonia
PCR polymerase chain reaction
PCV packed cell volume
PDEV purified duck embryo vaccine
PE pre-erythrocytic
PEG pegylated
PI protease inhibitors
PID pelvic inflammatory disease
PF peak flow
PGL persistent generalized lymphadenopathy
PHC primary health clinic
PKDL post-kala-azar dermal leishmaniasis
PML progressive multifocal leucoencephalopathy
PMTCT prevention of mother to child
transmission
PPD purified protein derivatives
PTSD post traumatic stress disorder
PUO pyrexia of unknown origin
PVCV purified vero cell vaccine
PVRV purified Vero cell vaccine
QBC quantitative buffy coat
q.d.s. four times a day
QTc corrected QT interval (electrocardiographic)
RAPLOA rapid assessment procedures for loiasis
RDT rapid diagnostic test
RIG rabies immune globulin
r.p.m. revolutions per minute
RR respiratory rate
RRV Ross River virus
RUTF ready to use therapeutic food
RVF Rift Valley fever
SACD subacute combined degeneration of the
spinal cord
SAM severe acute malnutrition
SAT standard agglutination test
SFP selective feeding programme
SLE systemic lupus erythematosus
SLE St Louis encephalitis
SMB suckling mouse brain
SP sulfadoxine–pyrimethamine
STD sexually transmitted disease
STI sexually transmitted infection
TB tuberculosis
TBE tick-borne encephalitis
TBRF tick-borne relapsing fever
TCBS thiosulphate citrate bile salt sucrose
TDF tenofovir
t.d.s. three times daily
TFC therapeutic feeding centre
TIF thiomersal, iodine and formol
TNF tumour necrosis factor
TPE tropical pulmonary eosinophilia
List of Abbreviations

xiii
TT tuberculoid leprosy
U&E urea and electrolytes
UFM under-fives mortality
UN United Nations
UNICEF United Nations Children’s Fund
UTI urinary tract infection
VCT voluntary counselling and testing
VEE Venezuelan equine encephalitis
VHF viral haemorrhagic fever
VIMTO vascular, infectious, metabolic, tumours
trauma and toxins, other
VL visceral leishmaniasis
VLM visceral larva migrans
W/H weight-for-height index
WBC white blood cell count
WBCT20 20-min whole blood clotting test
WHO World Health Organization
WNV West Nile virus
XDR extremely drug resistant
YF yellow fever
New Drug Names
New Old
aciclovir acyclovir
amoxicillin amoxycillin
anthelmintic antihelminthic
beclometasone beclomethasone
chlorphenamine chlorphenyramine
hydroxycarbamide hydroxyurea
lidocaine lignocaine
nonoxinol ‘9’ non-oxynol 9
phenobarbital phenobarbitone
sulfamethoxazole sulphamethoxazole
tiabendazole thiabendazole
thioacetazone thiacetazone
List of Abbreviations

Part 1
A General Approach to Syndromes/Symptom Complexes


3
Lecture Notes: Tropical Medicine, 6th edition. By G.V. Gill and N.J. Beeching. Published 2009 by Blackwell Publishing, ISBN: 978-1-4051-8048-1.
Chapter 1
Gastrointestinal presentations
The most important gastrointestinal presentation
in the tropics is diarrhoea, and the majority of
this chapter is devoted to this problem. However,
other presentations of gastrointestinal disease are
discussed first.
Dysphagia
Significant recent-onset dysphagia should always
raise the possibility of oesophageal carcinoma.
This malignancy is particularly common in cer-
tain parts of the tropics, for example, some areas
of Central and East Africa. Oesophageal can-
didiasis (AIDS-related) is also a common cause
of tropical dysphagia. In South America, the
mega-oesophagus of Chagas’ disease should be
considered. Finally, peptic strictures, corrosive
chemical ingestion and foreign bodies (fish bones
especially in some areas) may also be important
causes of impaired swallowing.
Haematemesis
In all areas of the world, an upper gastrointestinal
haemorrhage can be caused by peptic ulceration,
gastritis, oesophagitis and gastric or oesophageal
carcinoma. Gastritis, gastric erosions and gastric
ulcers may be drug related, for example, corti-
costeroids and non-steroidal anti-inflammatory
drugs (NSAIDs). Helicobacter pylori is recognized
globally as a major cause of gastric and duode-
nal inflammation and/or ulceration. Oesophageal
varices may be a particularly common cause of
haematemesis in many tropical areas—at least
25% of all cases in some series. The underlying
liver disease can be the late result of chronic viral
hepatitis or schistosomal hepatic fibrosis.
Abdominal pain
In ‘western’ populations, severe abdominal pain
can result from appendicitis, mesenteric adeni-
tis, perforated peptic ulcers, biliary colic, chole-
cystitis and intestinal obstruction (commonly
because of adhesions or malignancy). This list is
far from exhaustive, but serves to demonstrate
that the spectrum of causes in the tropics is much
wider. The following ‘exotic’ causes of acute severe
abdominal pain may need to be considered.● Abdominal tuberculosis (TB)● Typhoid (including typhoid perforation)● Hydatid cyst rupture● Amoebic colitis (including perforation)● Amoebic liver abscess (which may rupture)● Intestinal obstruction caused by Ascaris
lumbricoides● Ectopic ascariasis (e.g. biliary and/or pancreatic
obstruction)

Chapter 1 Gastrointestinal presentations
4
● Sickle cell crisis● Splenic rupture● Hyperinfection syndrome of strongyloidiasis.
Malabsorption
Malabsorption can be a feature of infection with
Giardia lamblia, Strongyloides stercoralis, intestinal
TB, as well as AIDS. Perhaps the most common
cause, however, is the temporary lactase-defi-
cient situation that may occur after any signifi-
cant acute infective diarrhoeal illness. Milk and
milk products may need to be avoided, although
yoghurt is usually tolerated, because of its high
bacterial lactase content.
Tropical sprue
A particularly well-described form of tropical
malabsorption is ‘tropical sprue’. This occurs pre-
dominantly in India and South East Asia, as well
as in the Caribbean and Central America. Patients
develop non-bloody diarrhoea (sometimes steator-
rhoea) often with abdominal bloating and signifi-
cant weight loss. There may be a history of initial
acute diarrhoeal illness, which is thought to be
the precipitant (although the exact mechanism is
unknown). Duodenal biopsy, as well as biochemi-
cal features of malabsorption, typically shows par-
tial villous atrophy. The illness can be prolonged
and debilitating. Traditional treatment with tetra-
cycline (for associated bacterial small bowel over-
growth) and folic acid is often highly effective.
Diarrhoea
Diarrhoeal illness is one of the most important
causes of morbidity and mortality in the tropics,
causing over six million deaths per year, and is
clearly linked with poor hygiene and contamina-
tion of water and food. A wide variety of viral, bac-
terial and parasitic pathogens have been implicated
in the pathogenesis of diarrhoea, but it is impossible
and unnecessary to test for all these in individual
cases. Systematic review of epidemiological, clinical
and host factors usually enables a sensible work-
ing aetiological diagnosis to be established. The
working diagnosis can be used to decide whether
specific investigation should be performed, or to
direct empirical antimicrobial therapy in the minor-
ity of cases in which it is required. The mainstay of
management of diarrhoeal illness is the assessment
and maintenance of adequate hydration and elec-
trolyte balance, irrespective of the aetiology, as well
as the introduction of control measures in an epi-
demic setting to prevent further cases.
History
It is essential to establish that both the doctor
and the patient are talking about the same thing,
especially if interpreters are being used to take
the clinical history. A useful working definition
of diarrhoea is the passage of three or more loose
or watery bowel motions in 24 h. The distinction
between soft and loose diarrhoea is more difficult,
but bowel motions can be described as diarrhoeal,
when they assume the shape of the collecting con-
tainer. This definition works with acute diarrhoeal
illness but is less satisfactory with chronic diar-
rhoeal illness related to malabsorption in which
bulky, sticky soft bowel motions are abnormal but
may not be fluid enough to move around in the
container. Key features in the history are the pres-
ence or absence of visible blood in the stool (dys-
entery), the presence and degree of abdominal
pain, the presence of tenesmus and the presence of
fever. The duration of illness is important—chronic
diarrhoea can usefully be defined as diarrhoea last-
ing more than 14 days, although a more precise
definition (especially in the context of an immuno-
compromised host) is the passage of three or more
loose or watery stools a day for 28 days or more.
In the historical assessment of fluid balance, the
volume and frequency of faecal loss should be esti-
mated together with the frequency and approxi-
mate volume of any vomiting. The amount of
fluid intake should be checked, as should the fre-
quency of urinary output during the last 24 h.
The epidemiological setting is important. Illness
in close family contacts should be ascertained, and
enquiry should be made about whether the patient
has attended any functions or eaten unusual foods
in the preceding 48–72 h. If so, have any other

Gastrointestinal presentations Chapter 1
5
guests had similar illness? Point source outbreaks
can be caused by toxin-mediated food poisoning
in which case vomiting is often a predominant
feature and incubation periods are usually shorter
than 24 h. This may be difficult to distinguish from
outbreaks of norovirus infection in which vom-
iting is a predominant feature and contacts are
readily infected. Unusual systemic pathogens (e.g.
anthrax of the gut) or non-infectious poisoning
caused by adulterated or contaminated food prod-
ucts must always be considered. Bacterial patho-
gens causing small or large bowel diarrhoea usually
have intermediate incubation periods of 12–72 h.
More detailed food histories are not otherwise very
helpful, except in the case of expatriates who have
unwisely overindulged in very spicy foods (‘tasting
the chilli twice’) or who have recently arrived in
the tropics (traveller’s diarrhoea). Diarrhoea devel-
oping in patients who are already hospitalized sug-
gests a nosocomial or antibiotic-associated cause,
while outbreaks of diarrhoeal illness in a refugee
or camp setting imply specific infections such as
shigellosis or cholera (see later) (Fig. 1.1).
Other illness
Diarrhoea can be a prominent feature of many sys-
temic illnesses, including malaria, pneumonia and
enteric fever, especially in children, and evaluation
of the patient should exclude these as potential
causes. Surgical and other intra-abdominal condi-
tions may mimic gastroenteritis, as can inflamma-
tory bowel disease. In older or immobile patients,
constipation with overflow diarrhoea must be
excluded. Alcohol and drugs frequently cause diar-
rhoea with or without nausea and vomiting.
Host factors
Conditions that cause hypochlorhydria (e.g. gastric
surgery, H2 antagonists and proton pump inhibi-
tors) reduce the gastric acid barrier to many bacterial
pathogens, so a smaller infective dose is required.
Patients with established cardiovascular or renal
disease are less likely to tolerate dehydration, as are
those on diuretics and patients with poorly con-
trolled diabetes. Pre-existing large bowel problems
such as inflammatory bowel disease predispose to
complications of dysenteric infections such as toxic
megacolon, signs of which may be partly masked
by concurrent steroid therapy. Bowel tumours can
produce diarrhoea with or without blood or weight
loss. Small bowel problems, including lymphoma,
can cause prolonged diarrhoea. Immunosuppression
of the patient, particularly by HIV, predisposes to
increased invasiveness (local and systemic) of bac-
terial pathogens such as non-typhoidal Salmonella,
increased recurrence of such pathogens and chronic
diarrhoea caused by a variety of protozoa.
Examination
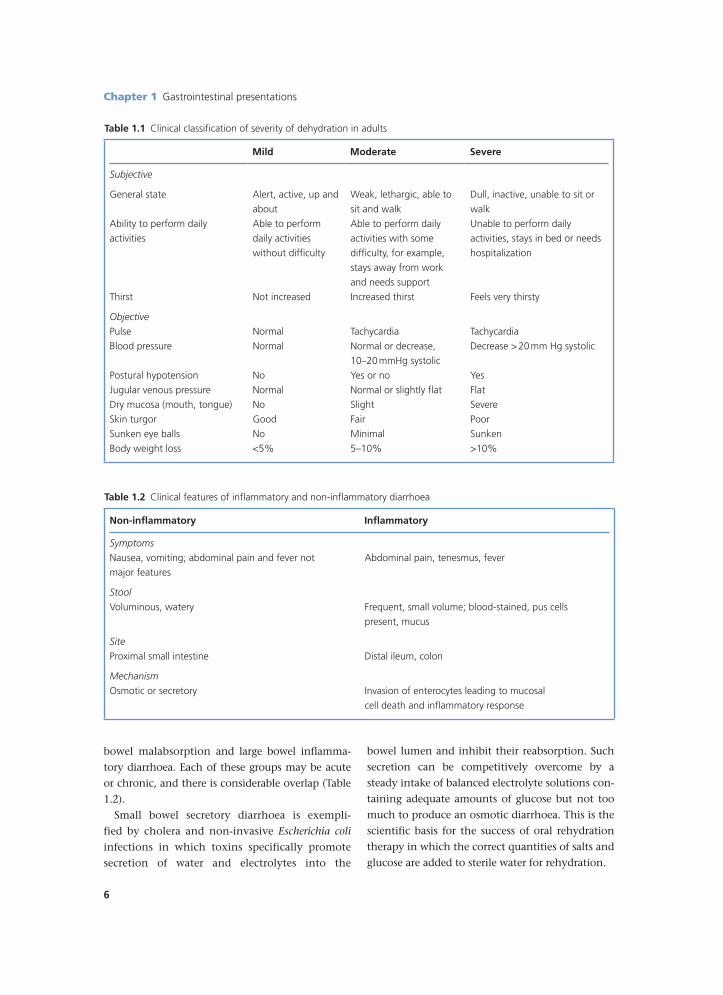
General examination must include assessment
of the state of hydration. This is more difficult
to quantify clinically in adults than in children,
but key features are summarized in Table 1.1.
Measurement of any postural drop in blood pres-
sure (BP) is particularly useful. Rectal examination
should be performed, except in obvious cases of
cholera, and is particularly important in older
patients who are more likely to have non-infec-
tious bowel problems. Systemic causes of diar-
rhoea and signs of immunosuppression (e.g. zoster
scars and oral candidiasis) should be sought out.
Clinical syndromes of diarrhoea
Apart from acute toxin-mediated food poison-
ing, diarrhoeal illness can be broadly classi-
fied into small bowel secretory diarrhoea, small Figure 1.1 Though it looks like urine, this is the `ricewater’ stool from a patient with cholera.
Chapter 1 Gastrointestinal presentations
6
bowel malabsorption and large bowel inflamma-
tory diarrhoea. Each of these groups may be acute
or chronic, and there is considerable overlap (Table
1.2).
Small bowel secretory diarrhoea is exempli-
fied by cholera and non-invasive Escherichia coli
infections in which toxins specifically promote
secretion of water and electrolytes into the
bowel lumen and inhibit their reabsorption. Such
secretion can be competitively overcome by a
steady intake of balanced electrolyte solutions con-
taining adequate amounts of glucose but not too
much to produce an osmotic diarrhoea. This is the
scientific basis for the success of oral rehydration
therapy in which the correct quantities of salts and
glucose are added to sterile water for rehydration.
Table 1.1 Clinical classification of severity of dehydration in adults
Mild Moderate Severe
Subjective
General state Alert, active, up and
about
Weak, lethargic, able to
sit and walk
Dull, inactive, unable to sit or
walk
Ability to perform daily
activities
Able to perform
daily activities
without difficulty
Able to perform daily
activities with some
difficulty, for example,
stays away from work
and needs support
Unable to perform daily
activities, stays in bed or needs
hospitalization
Thirst Not increased Increased thirst Feels very thirsty
Objective
Pulse Normal Tachycardia Tachycardia
Blood pressure Normal Normal or decrease,
10–20 mmHg systolic
Decrease > 20 mm Hg systolic
Postural hypotension No Yes or no Yes
Jugular venous pressure Normal Normal or slightly flat Flat
Dry mucosa (mouth, tongue) No Slight Severe
Skin turgor Good Fair Poor
Sunken eye balls No Minimal Sunken
Body weight loss <5% 5–10% >10%
Table 1.2 Clinical features of inflammatory and non-inflammatory diarrhoea
Non-inflammatory Inflammatory
Symptoms
Nausea, vomiting; abdominal pain and fever not Abdominal pain, tenesmus, fever
major features
Stool
Voluminous, watery Frequent, small volume; blood-stained, pus cells
present, mucus
Site
Proximal small intestine Distal ileum, colon
Mechanism
Osmotic or secretory Invasion of enterocytes leading to mucosal
cell death and inflammatory response

Gastrointestinal presentations Chapter 1
7
Malabsorption is a common complication
of infectious diarrhoea in the tropics, as many
races have relatively low disaccharidase activity
in the small bowel enterocytes. Disruption of
‘normal’ bowel activity readily leads to failure
to break down sugars and a moderately pro-
longed lactose intolerance. This is particularly
common after infections that cause flattening of
the small bowel mucosa (such as giardiasis and
cryptosporidiosis). Large bowel diarrhoea is usu-
ally caused by direct invasion of the bowel by
pathogens such as Entamoeba histolytica, bacteria
such as Campylobacter species or Clostridium dif-
ficile after antibiotic therapy. Other parasites such
as Schistosoma mansoni can also cause prolonged
large bowel diarrhoea. In heavy Trichuris trichiura
infections, oedema of the rectal mucosa together
with continued efforts to defaecate resulting from
tenesmus can lead to rectal prolapse. A summary
of the major pathogens in inflammatory and non-
inflammatory diarrhoea is shown in Table 1.3.
Investigations
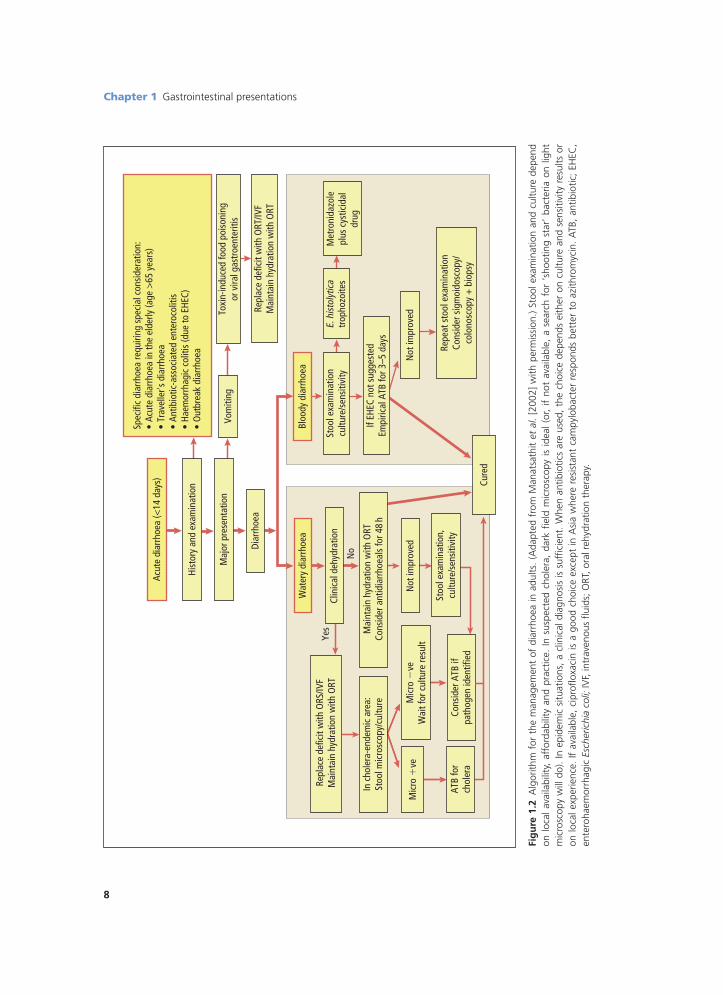
A useful algorithmic approach to individual
patient diagnosis and management is shown in
Figure 1.2. In most tropical settings, microbio-
logical investigation proves impossible or very
Table 1.3 Pathogens in inflammatory and non-inflammatory diarrhoea
Inflammatory Non-inflammatory
VirusesNil Rotavirus
Adenovirus 40/41
Astrovirus
Norovirus (Norwalk agent)
Calicivirus
Small round structureless virus
Coronavirus
Torovirus
Bredavirus
Picobirnavirus
BacteriaEnteroinvasive Escherichia coli (EIEC) Enterotoxigenic E. coli (ETEC)
Enterohaemorrhagic E. coli (EHEC), for example, 0157 Enteropathogenic E. coli (EPEC)
Enteroaggregative E. coli (EAggEC) Vibrio cholerae
Aeromonas hydrophila Vibrio parahaemolyticus
Campylobacter spp. Campylobacter spp.
Salmonella spp. Salmonella spp.
Shigella spp. Plesiomonas shigelloides
Yersinia enterocolitica Bacillus cereus
Clostridium difficile Clostridium perfringens
ProtozoaEntamoeba histolytica Cryptosporidium spp.
Balantidium coli Giardia intestinalis
Cyclospora cayetanensis
Isospora belli
Microsporidia (e.g. Enterocytozoon bieneusi)
HelminthsSchistosoma spp. Strongyloides stercoralis
Chapter 1 Gastrointestinal presentations
8
Fig
ure
1.2
Alg
orith
m f
or t
he m
anag
emen
t of
dia
rrho
ea in
adu
lts.
(Ada
pted
fro
m M
anat
sath
it et
al.
[200
2] w
ith p
erm
issi
on.)
Stoo
l exa
min
atio
n an
d cu
lture
dep
end
on l
ocal
ava
ilabi
lity,
aff
orda
bilit
y an
d pr
actic
e. I
n su
spec
ted
chol
era,
dar
k fie
ld m
icro
scop
y is
ide
al (
or,
if no
t av
aila
ble,
a s
earc
h fo
r ‘s
hoot
ing
star
’ ba
cter
ia o
n lig
ht
mic
rosc
opy
will
do)
. In
epi
dem
ic s
ituat
ions
, a
clin
ical
dia
gnos
is is
suf
ficie
nt.
Whe
n an
tibio
tics
are
used
, th
e ch
oice
dep
ends
eith
er o
n cu
lture
and
sen
sitiv
ity r
esul
ts o
r on
loca
l exp
erie
nce.
If a
vaila
ble,
cip
roflo
xaci
n is
a g
ood
choi
ce e
xcep
t in
Asi
a w
here
res
ista
nt c
ampy
loba
cter
res
pond
s be
tter
to
azith
rom
ycin
. A
TB,
antib
iotic
; EH
EC,
ente
roha
emor
rhag
ic E
sche
richi
a co
li; IV
F, in
trav
enou
s flu
ids;
ORT
, ora
l reh
ydra
tion
ther
apy.
Acut
e di
arrh
oea
(<14
day
s)
Hist
ory
and
exam
inat
ion
Maj
or p
rese
ntat
ion
Diar
rhoe
a
Spec
ific
diar
rhoe
a re
quiri
ng s
peci
al c
onsi
dera
tion:
• Ac
ute
diar
rhoe
a in
the
elde
rly (a
ge >
65 y
ears
)•
Trav
elle
r's d
iarr
hoea
• An
tibio
tic-a
ssoc
iate
d en
tero
colit
is•
Haem
orrh
agic
col
itis
(due
to E
HEC)
• O
utbr
eak
diar
rhoe
a
Vom
iting
Toxi
n-in
duce
d fo
od p
oiso
ning
or v
iral g
astr
oent
eriti
s
Repl
ace
defic
it w
ith O
RT/IV
FM
aint
ain
hydr
atio
n w
ith O
RT
Wat
ery
diar
rhoe
aBl
oody
dia
rrho
ea
Clin
ical
deh
ydra
tion
Rep
lace
def
icit
with
ORS
/IVF
Mai
ntai
n hy
drat
ion
with
ORT
In c
hole
ra-e
ndem
ic a
rea:
Stoo
l mic
rosc
opy/
cultu
re M
aint
ain
hydr
atio
n w
ith O
RT C
onsi
der a
ntid
iarr
hoea
ls fo
r 48
h
Mic
ro �
veM
icro
�ve
Wai
t for
cul
ture
resu
ltN
ot im
prov
ed
ATB
for
chol
era
Cons
ider
ATB
ifpa
thog
en id
entif
ied
Stoo
l exa
min
atio
n,cu
lture
/sen
sitiv
ity
Cure
d
Stoo
l exa
min
atio
ncu
lture
/sen
sitiv
ityM
etro
nida
zole
plus
cys
ticid
aldr
ug
If EH
EC n
ot s
ugge
sted
Empi
rical
ATB
for 3
–5 d
ays
Not
impr
oved
Repe
at s
tool
exa
min
atio
nCo
nsid
er s
igm
oido
scop
y/co
lono
scop
y +
bio
psy
Yes
No
trop
hozo
ites
E. h
isto
lytic
a

Gastrointestinal presentations Chapter 1
9
limited. Microscopic inspection of faeces for leuco-
cytes, suggestive of invasive pathogens in the large
bowel, is commonly advocated but is of question-
able time-effectiveness compared with macro-
scopic inspection of faeces for blood (and smell)
when resources are limited. However, cholera
vibrios may be observed with their characteristic
‘shooting star’ motility even without dark ground
facilities, and this is very useful when culture is
not available. Investigations for faecal parasites
should be limited to specific settings (e.g. chronic
diarrhoea complicating HIV) and are almost never
indicated in nosocomial diarrhoea. Fresh stool
microscopy for active trophozoites should only
be requested when amoebic dysentery is truly sus-
pected. Blanket requests for faecal microscopy for
‘ova, cysts and parasites’ on all patients are a waste
of time in most settings. Such requesting patterns
overload laboratories, demoralize their staff and
lead to reports of questionable quality with little
effect on clinical management decisions.
In an outbreak setting, full microbiological
identification of the pathogen and assessment
of the antimicrobial resistance patterns are very
helpful, and it should be pursued even if outside
assistance is required. In sporadic cases, detailed
microbiological tests may be inappropriate, but
clinicians need to be aware of the local antibi-
otic sensitivities of organisms such as Shigella,
Salmonella and Campylobacter if they are to use
empirical antimicrobial therapy in a responsible
and effective manner. Other investigations, such
as serum electrolytes, peripheral white cell count
and blood cultures, are performed in a hospital
setting but again may not be available routinely.
Management
Detailed management of individual pathogens is
beyond the scope of this chapter. The key is the
correction of fluid and electrolyte imbalance.
Severely dehydrated patients need rapid intrave-
nous replacement of fluid loss, preferably using
a physiologically balanced electrolyte solution
such as Ringer’s solution (see Chapter 21, p. 197).
Large volumes of dextrose solution can be dan-
gerous. Intravenous fluid can be supplemented
and rapidly replaced by oral rehydration, which
is more successful if small volumes of fluid are
taken steadily rather than large volumes at a time.
Specific World Health Organization (WHO) oral
rehydration solution (ORS) is ideal, but the water
in which it is dissolved must be clean and safe to
drink—preferably by prior boiling and cooling.
Alternative oral rehydration therapy mixtures can
also be used for adults, and food, including milk
products, is usually reintroduced as early as possi-
ble after initial resuscitation of children. Fluid bal-
ance should be carefully monitored, and a cholera
bed is useful for less mobile patients with profuse
diarrhoea. The fluid faeces can then be collected
through a hole in the middle of the bed directly
into a measuring bucket. If a large-bore disposable
Foley’s urinary catheter is available, this can be
inserted into the rectum when diarrhoea is pro-
fuse and watery (e.g. in cholera), removing the
need for frequent evacuation, and allowing accu-
rate measurement of faecal losses by volume.
Antidiarrhoeal agents such as codeine or lop-
eramide should be avoided in patients with acute
invasive or large bowel disease and should not
be used in young children. Antiemetics should
be used sparingly and again avoided in young
children. Zinc supplementation is beneficial for
children, but the roles of probiotics and use of
lactose-free feeds are less clear. Empirical or spe-
cific antimicrobial treatment should be reserved
for specific situations such as proven amoebiasis,
prolonged severe infection in a vulnerable host
or in outbreak settings—for example cholera or
shigellosis. Chronic diarrhoea presents a different
challenge and patients with HIV-related diarrhoea
often progress through successive therapeutic
trials of co-trimoxazole, metronidazole, fluo-
roquinolones, albendazole or nitazoxanide. Such
patients may need ‘hospital at home’ support
including provision of adequate antidiarrhoeal
medications.
In a refugee camp outbreak setting, logisti-
cal support must be requested at an early stage
for detailed epidemiological investigation, triage
and treatment facilities, as well as provision of an
adequate water supply, rehydration solutions and
latrines (Chapter 60).

Chapter 1 Gastrointestinal presentations
10
Further reading
Al-Abri SA, Beeching NJ, Nye FJ. Traveller’s diarrhoea.
Lancet Infect Dis 2005; 5: 349–360. [Overview
of aetiology, epidemiology, management and
prevention of this common problem for
travellers.]
Elliott EJ. Acute gastroenteritis in children. BMJ
2007; 334: 35–40. [Concise evidence based
review, very practical and useful.]
Hart CA. Introduction to acute infective diar-
rhoea. In: Cook GC, Zumla A, eds. Manson’s
Tropical Diseases, 21st edn. London: Elsevier
Science, 2003: 907–913. [Good overview with
references of both adult and paediatric diar-
rhoea causes and effects.]
Manatsathit S, DuPont H, Farthing M et al.
Guideline for the management of acute diar-
rhoea in adults. J Gastroenterol Hepatol 2002;
17 (Suppl): S54–S71. [Superb working party
report produced by acknowledged experts from
Thailand, India and Africa as well as ‘west-
ern’ authorities. Detailed definitions, practical
approaches and many references.]
Thomas PD et al. Guidelines for the investigation
of chronic diarrhoea, 2nd edition. Gut 2003; 52:
1–15. [British guidelines for assessment of both
infectious and non-infectious causes of chronic
diarrhoea.]
WHO. Handbook IMCI Integrated Management
of Childhood Illness. WHO 2005. Chapter 8
Diarrhoea—assessment and management of
diarrhoea in children in tropical settings pages
25–31. [Summary of WHO guidelines for use
at clinic level. Full manual and other IMCI
and nutrition-related resources freely down-
loadable from WHO child and adolescent
health development website http://www.who.
int/child_adolescent_health/topics/en/]
WHO. Implementing the New Recommendations on
the Clinical Management of Diarrhoea. Guidelines
for Policy Makers and Programme Managers. WHO
2006. [Summary of new recommendations for
use of the 2003 low osmolarity ORS mixture
and zinc supplementation, plus programme
guidance.]
WHO. The Treatment of Diarrhoea. A Manual for
Physicians and Other Senior Health Workers,
4th edn. WHO 2005. [Comprehensive review
with algorithms for assessment and manage-
ment of children and adolescents in particular,
appropriate for resource poor settings.]
11
Lecture Notes: Tropical Medicine, 6th edition. By G.V. Gill and N.J. Beeching. Published 2009 by Blackwell Publishing, ISBN: 978-1-4051-8048-1.
Chapter 2
Respiratory presentations
Disorders of the respiratory tract are the most
important cause of ill health in human popula-
tions around the world. The normal physiologi-
cal functioning of the respiratory tract exposes it
to prolonged and intimate contact with the exter-
nal environment, leading to a steady exposure to
airborne pollutants and pathogens with disease-
causing potential.
Infectious diseases dominate acute respiratory
illness in the tropics in all age groups; acute viral
and bacterial infections in childhood, and tubercu-
losis and bacterial pneumonia in adults. The enor-
mous global burden of respiratory impairment
due to chronic obstructive pulmonary disease
(COPD) has recently been described and shown to
be worst in South Africa and China, where the dis-
ease is mainly caused by the exposure to tobacco
smoke in men and by indoor air pollution from
cooking with biomass fuel in women. Global con-
cern regarding the health effects of tobacco smoke
has now resulted in important international trea-
ties to limit tobacco products.
Assessment
History
The predominant symptoms of respiratory illness
are breathlessness, cough and chest pain. Symptom
duration and the concurrence of fever are useful
discriminators—common presentations in adults
and children are summarized in Table 2.1.
Breathlessness
Shortness of breath should be characterized by
duration, progression and whether it is constant
or intermittent. Orthopnoea (breathlessness when
lying flat) suggests a cardiac cause or a structural
abnormality of the thoracic cage. Nocturnal dys-
pnoea is a feature of asthma and obstructive air-
ways disease.
The effort required to precipitate breathlessness
provides a good gauge of the level of respiratory
impairment. Breathlessness at rest or inability of
a young child to feed indicates severe restriction.
Shortness of breath in an adult should be quanti-
fied in terms of tasks completed or failed, or dis-
tance walked.
Cough
Cough is a reflex from any part of the vagal sup-
ply and a conscious act. Therefore, discriminating
between causes of cough can be difficult. Cough
may be productive or non-productive, but a ‘pro-
ductive’ cough is often evidence of pulmonary
infection.
The quantity of sputum produced may provide
diagnostic information about COPD or bron-
chiectasis. The expectoration of mucopurulent

Chapter 2 Respiratory presentations
12
material is an indicator of neutrophil activity and
infection.
Haemoptysis is often an indicator of seri-
ous underlying pathology, but it is important to
establish that blood is being coughed and not
coming from the upper airway or enteric tract.
Tuberculosis, bronchiectasis and neoplasia are
primary concerns.
Extreme paroxysms of coughing in a child,
particularly in association with the characteristic
whoop, indicates a diagnosis of whooping cough.
A ‘barking’ cough with inspiratory stridor is the
hallmark of laryngotracheobronchitis—croup.
Chest pain
Complaints of chest pain should be assessed for
their association with breathing and coughing.
Pain derived from the pleura will be noticeable
on breathing and is lateralized. Tracheal pain has
a tearing or burning quality and is felt retroster-
nally, particularly on coughing.
Respiratory history
In addition to the presenting symptoms, it is
important to enquire about● tobacco smoking (quantify in pack years);● occupation—identify occupationally related
symptoms and exposures including asbestos,
inhaled proteins and fumes;
● risk factors for HIV infection and contact with
tuberculosis cases, particularly in children failing
to thrive.
Non-respiratory illness
Non-respiratory illness may present with pre-
dominantly respiratory symptoms. Breathlessness
is a feature of metabolic acidosis which may be
caused by diabetic ketoacidosis, poisoning, severe
sepsis or renal failure. Chronic breathing difficul-
ties are a feature of anaemia and thyroid disease.
Alteration of breathing pattern and breathless-
ness can occur with neurological injury, during
the early stages of tetanus and botulism and fol-
lowing envenomation.
Examination in respiratory cases
A respiratory examination is used to test hypoth-
eses generated by the history. The signs elicited
are rarely diagnostic in isolation.
The general condition of an individual provides
clues to a diagnosis. In particular, cachexia, or fail-
ure to thrive in a young child, will indicate malnu-
trition or chronic underlying illness. Oral thrush,
skin rashes and old herpes zoster scars are highly
suspicious of HIV infection, heightening the possi-
bility of pneumococcal pneumonia or tuberculosis.
Tachypnoea (rapid breathing) can be a feature
of any respiratory illness. In the context of an
Table 2.1 Shortness of breath in adults and children
Sudden (hours) Acute (days) Chronic (weeks, months)
Adults
Pneumothorax Pneumonia Tuberculosis
Pulmonary embolus Bronchitis COPD
Asthma Lung abscess Kaposi’s sarcoma
Acute left ventricular failure Lung cancer
Allergic alveolitis Heart failure
Pulmonary eosinophilia Silicosis/asbestosis
Children
Pneumothorax Pneumonia Tuberculosis
Inhaled foreign body Bronchitis Heart failure
Asthma

Respiratory presentations Chapter 2
13
acute presentation, rates in adults above 30/min
suggest severe disease particularly in association
with systolic blood pressure below 90 mmHg
and/or a tachycardia in excess of 120 beats per
minute. The criteria for tachypnoea in childhood
are very different from adults. It is diagnosed
only if the respiratory rate is over 60/min before
the age of 2 months, over 50/min from 2 to 12
months, over 40/min from 1 to 5 years and over
30/min (as for adults) over the age of 5 years.
Cyanosis should be looked for in the oral
mucosa but is a difficult sign in pigmented
people. When present it indicates at least 10%
desaturation of haemoglobin and the need for
supplemental oxygen. Pulse oximetry is becom-
ing increasingly widespread and provides more
reliable information.
Altered consciousness and confusion
usually indicate severe acute disease and can
necessitate specific management to protect the
airway. Meningism can be found with severe
pneumonia, with or without pneumococcal
meningitis.
Percussion of the chest will identify a large
pleural effusion (dull note). Lobar consolidation
is common in pneumonia or tuberculosis and can
be diagnosed on the basis of bronchial breathing.
Many patients present with non-specific signs or
scanty chest signs. In these cases, a suggestive
history should lead to further investigation as a
normal chest examination does not exclude sig-
nificant pathology.
Investigation of respiratory disease
Chest X-ray
Limited resources must be carefully rationed in
order to optimally investigate respiratory patients
in the tropics. In particular, a chest X-ray should
be used to extend the examination in difficult
cases and not simply to confirm diagnosis made
confidently on auscultation. Patients with severe
acute respiratory illness or those who fail to
respond to therapy including smear-negative cases
of chronic cough are the ones most frequently
requiring a chest X-ray.
Sputum/respiratory secretions
Sputum examination is essential in the manage-
ment of suspected TB (see Chapter 12) and is of
less value in other cases. Ziehl–Neelsen stain-
ing for mycobacteria and Gram staining for
bacteria are the most common investigations.
Occasionally, an unstained wet preparation of
sputum examined under low power may be
useful for identifying Strongyloides, paragonim-
iasis or fungal elements. Cytology for malig-
nant cells can also be performed on sputum but
requires a skilled pathologist. Other sputum tests
include direct immunofluorescence for viruses
and Pneumocystis jirovecii, antigen detection for
pneumococci and molecular techniques for sev-
eral organisms including tuberculosis, but these
methods are not resource-efficient in developing
countries.
Sputum must be from the lower respiratory
tract and a macroscopic mucopurulent appear-
ance makes this probable. Microscopic sputum
quality assessment is described in Chapter 28.
Sputum samples are best collected in the open air
(outside) to limit the hazard of cross-infection.
When sputum cannot be produced, placing the
patient in a head down position or simple chest
physiotherapy (drumming) for 2–3 min will help.
Lung aspiration increases the diagnostic yield in
young children with lung consolidation. A nee-
dle and syringe primed with 1 mL normal saline
or sterile water is passed into the consolidated
tissue through the thoracic wall and aspirated.
The aspirated material can be smeared onto
slides for examination and injected into liquid
culture media. In young children when sputum is
difficult to collect, gastric washings may be con-
sidered for the investigation of possible tubercu-
losis (mycobacteria are gastric acid resistant).
Blood cultures
Blood cultures are a valuable investigation in all
febrile patients. Recovery of a pathogen allows
confident treatment and is frequently the inves-
tigation by which an unusual cause of pneumo-
nia is established, for example, Salmonella typhi,

Chapter 2 Respiratory presentations
14
Cryptococcus spp, Burkholderia pseudomallei (melio-
idosis), Rhodococcus equi.
Pleural fluid
Sampling of pleural fluid is simple to perform and
should be considered for most effusions, as the
management of simple effusion and empyema is
different. Fluid is aspirated by using a needle and
syringe, avoiding the neurovascular bundle at the
inferior margin of each rib. Occasionally, this fails
because pleural fluid is loculated and has formed
a thick empyema or the chest findings result from
chronic pleural scarring. Protein measurements
may be helpful in confirming an effusion to be a
transudate—a protein level below 30 g/dL and an
absence of inflammatory cells.
Lung function testing
Although lung function can now be measured
using hand-held technology and stored on a lap-
top computer, this is not yet widely used. Now
that asthma prevalence is increasing and COPD is
recognized as a significant burden of chronic dis-
ease in Africa, this may change.
Common presentations
In general, respiratory presentations in the
general medical clinic tend to fall into a small
number of syndromes.
Acute breathlessness and fever in a small child
Lower respiratory tract infection (LRTI) is a lead-
ing killer of children. Consequently, the early
assessment and management of this syndrome is
a core component of the Integrated Management
of Childhood Illness (IMCI) strategy promoted
by the WHO. Vaccination against pneumococcal
and Haemophilus infection are also global
priorities.
Simple assessment at the primary care level
using features of rapid breathing and subcostal
recession (chest indrawing) of a child with fever
and cough is used to distinguish children with an
LRTI who require antibiotics and possible hospital
admission, from those with an upper respiratory
tract infection (see Figure 28.1). Early initiation
of therapy is essential for a good outcome.
Although many LRTIs are initiated by viral
infections, amongst which respiratory syncytial
virus, parainfluenza, adenovirus and measles are
important, super-added bacterial infections are fre-
quent. Streptococcus pneumoniae and Haemophilus
influenzae type b are common. The presentation
of tuberculosis in infants is often occult.
Acute breathlessness, cough and fever in adults
Acute bacterial pneumonia is the principal diag-
nostic consideration, and the diagnosis and
management of this is covered in Chapter 28.
Non-infectious causes become more prevalent in
older adults.
Chronic cough and malaise
Most chronic respiratory problems present
in this way. It is important to exclude or
confirm tuberculosis which represents a seri-
ous public health threat but is readily treat-
able (Chapter 12). A small number of conditions
are specific to the tropics and may need to be
considered under the right epidemiological
circumstances: paragonimiasis in South East
Asia and restricted areas of West Africa (Chapter
29); endemic mycoses in South and Central
America (Chapter 54); and pulmonary compli-
cations of schistosomiasis in endemic regions
(Chapter 17). The incidence of tobacco smoking
associated lung cancer is increasing in developing
countries.
Breathlessness and wheeze
Asthma is an increasingly important problem
in the tropics, particularly in urban centres. The

Respiratory presentations Chapter 2
15
expiratory wheeze or whistling associated with
lower airways obstruction must be differentiated
from inspiratory phase stridor, which indicates
upper airway obstruction. The presence of parox-
ysmal or diurnal cough, breathlessness and wheeze
preferably supported by variation in peak flow
measurements reliably indicates airways obstruc-
tion. An important differential diagnosis of asthma
is tropical pulmonary eosinophilia (Chapter 30).
Although the symptoms are identical, a high
peripheral eosinophil count above 1 � 109/L, dem-
onstration of microfilaria in blood and clinical
response to filaricides support the diagnosis.
Pleural effusion
Symptoms associated with pleural effusions can
be of short or long duration depending on the
nature of the underlying problems, but large effu-
sions are straightforward to find on examination.
Pleural fluid should be sampled as described ear-
lier. In HIV endemic regions, TB is the most com-
mon cause of pleural effusion. Parapneumonic
effusions, empyema or tuberculous effusions
should be suggested by the history. Malignant
effusions must be considered when an infective
aetiology is not readily apparent. Effusions may
indicate extrapulmonary or systemic problems
(Table 2.2).
Respiratory disease in the HIV-infected adults
Respiratory problems head the list of conditions
leading to hospital admission of HIV-infected
adults (Table 2.3). Bacterial (particularly pneu-
mococcal) pneumonia is strongly associated with
HIV infection. It has a similar predictive value for
HIV infection in adults to herpes zoster—around
90% in eastern and southern Africa. HIV infection
Table 2.2 Causes of pleural effusion
Common Infrequent Rare
● Tuberculosis ● Neoplasia ● Thoracic duct damage● Parapneumonic – Lung carcinoma ● Pancreatitis● Empyema – Kaposis’s sarcoma ● Haemorrhagic fever● Heart failure – Burkitt’s lymphoma ● Filariasis
– Mesothelioma ● Hypothyroidism● Constrictive pericarditis
Table 2.3 Respiratory problems complicating HIV infection
Common Infrequent
● Bacterial pneumonia ● Pneumocystis jirovecii pneumoniaa
● Tuberculosis ● Rhodococcus equi infection● Acute bronchitis ● Nocardiasis● Sinusitis ● Lymphoid interstitial pneumonitisb
● Bronchiectasis ● Lymphoma● Pulmonary cryptococcosis ● Pulmonary hypertension● Pulmonary Kaposi’s sarcoma ● Penicillinosisc
● Melioidosisc
● Invasive mycosesd
aCommon in children under 1 year old.bCommon in children.cSouth East Asia.dSouth and Central America.





























