Embed Size (px)
Citation preview

Superficial Back Muscles
By Charles Curtis
Dorsal Wall of the Trunk Upper Limb
• The back forms the entire dorsal wall of the trunk from the cervical to sacral region. The muscles of the back are arranged in superficial and deep layers.
• The superficial back muscles consist of body wall muscles that have been annexed by the upper limb to support the :– scapula (levator scapulae and rhomboids), – ribs (serratus posterior muscles)– humerus (latissimus dorsi).

Dorsal Wall of the TrunkUpper Limb
• In addition, the trapezius supports the scapulothoracic joint.
• These superficial back muscles migrate onto the back and neck superficial to the deep (epaxial or intrinsic) back muscles.
• The deep back muscles attach to the dorsal aspect of the vertebral column.

Match the muscle to the numberRhomboid minor muscleRhomboid major muscleSpine of scapulaUpper fibers of trapezius muscleLigamentum nuchaeLatissimus dorsi musclePosterior lamella of thoracolumbar fasciaMiddle fibers of trapezius muscleLower fibers of trapezius muscleTeres major muscleInfraspinatus muscleTeres minor muscleLevator scapulae muscle
1
2
3 4
56
7
8
9
10
1112
13

1. Latissimus dorsi muscle2. Posterior lamella of thoracolumbar fascia3. Lower fibers of trapezius muscle4. Middle fibers of trapezius muscle5. Upper fibers of trapezius muscle6. Spine of scapula7. Deltoid muscle8. Teres major muscle9. Teres minor muscle10. Acromion of scapula11. Infraspinatus muscle
1
2
3
4
5
6
789
10
11
Extrinsic muscles of back (superficial layer; posterior view). The superficial layer of extrinsic back muscles produces movement of the upper limb and, therefore, is in close proximity to other muscles of the upper limb, such as the rotator cuff, and shoulder.

Dorsal Wall of the TrunkUpper Limb
• The deep back muscles span from the occipital bone to the sacrum in 4 distinct muscle groups.
• From superficial to deep, the groups are the:– spinotransversales, – erector spinae, – transversospinales, and – intersegmental muscles.

12
3
4
5
6
7
8
910
111213
14
1516
17
18
19 20
Extrinsic muscles of back (superficial and intermediate layers; posterior view). The superficial layer of extrinsic back muscles produces movement of the upper limb and, therefore, is in close proximity to other muscles of the upper limb, such as the rotator cuff, and shoulder. The intermediate layer attaches to the vertebral column and ribs and produces elevation and depression of the rib cage.
Identify the items:
Trapezius
The above superficial back muscles act on the upper limb and thoracic body wall.
Superficial back muscles (upper limb). Form the posterior muscular connection of the pectoral girdle to the body wall (vertebral column) and thus control movements of the upper limb and neck.

Trapezius/Levator Scap/Rhomboids Mj and Minor/Lats
Trapezius. Medial attachment.Lateral attachment..Function. Blood supply. Innervation. Motor innervation and proprioceptive innervation
Levator Scap– Superior attachment..– Inferior attachment. – Function. – Blood supply. – Innervation.
• Rhomboid Major– Medial attachment..– Lateral attachment. – Function. – Blood supply. – Innervation.
• Rhomboid Minor– Medial attachment..– Lateral attachment. – Function. – Blood supply. – Innervation.
• Latissimus Dorsi – Medial attachment..– Lateral attachment. – Function. – Blood supply. – Innervation.


Dorsal Scapular Nerve Injury
Clinical

1. C5 spinal nerve2. Brachial plexus upper trunk3. Posterior circumflex humeral artery4. Suprascapular nerve5. Dorsal scapular nerve6. Brachial plexus posterior cord7. Circumflex scapular artery8. Radial nerve9. Dorsal scapular artery10. Axillary nerve
1
2
3
4
4
5
5
67
8
9 10
Brachial plexus (posterior view). In this illustration, the arterial system is ghosted in for reference.

Dorsal Scapular Nerve Injury
• Injury to the dorsal scapular nerve (DSN), which innervates the levator scapula and rhomboid muscles.
• Signs and symptoms. Patients may or may not have pain over the scapular muscles innervated by the DSN. A more common complaint is weakness and fatigue.

Dorsal Scapular Nerve Injury
• Causes. DSN injury is rare in isolation but can occur after acute or repetitive trauma to the neck or shoulder area.– Acute trauma can occur with direct blow or twisting injury of
the neck or shoulder.– Repetitive movements such as weight lifting, throwing sports, or
activities such as washing a car can lead to trauma over time.• Scapula. The DSN is a motor nerve that arises from the C5
spinal nerve root and innervates 3 of the muscles that attach to the medial border of the scapula: The levator scapula, rhomboid major, and rhomboid minor. Paralysis of these muscle results in a winged scapula.

1. Winged scapula
1
Winged scapula (posterior view). The medial border of the right scapula is elevated from paralysis of the rhomboids.
Dorsal Scapular Nerve Injury
• Physical exam. Patient will have decreased or complete loss of scapular adduction and downward rotation. This may lead to a "winged scapula," in which the medial border of the scapula protrudes dorsally and has a wing-like appearance.– Winged scapula is more commonly due to injury of the long thoracic
nerve that innervates the serratus anterior muscle.– Maneuvers to isolate the rhomboid muscles can be performed. The
patient is positioned prone on the physical exam table. The patient's elbow is flexed, and the arm is internally rotated with the hand behind the back (envision the patient reaching into his or her back pocket). The patient is then instructed to raise the hand and arm off of the back against resistance. This will be difficult for the patient if there is denervation of the rhomboid muscles.

Dorsal Scapular Nerve Injury
• Imaging. MR is the imaging method of choice if imaging is clinically indicated. Imaging of the cervical spine and shoulder area in the setting of trauma may be completed.– MR may show fluid signal (neurogenic edema) in the levator
scapula &/or rhomboid muscles in the setting of acute injury.– There may be fatty atrophy of the muscle bodies in the
setting of chronic injury.• Electromyography (EMG). EMG will show denervation
potentials in the rhomboid muscles and levator scapula

Intermediate group back muscles (thoracic body wall).
• Muscles of the intermediate layer of the back attach to the vertebral column and the ribs and play a minor role in elevating and depressing the rib cage.–Serratus Posterior Superior–Serratus Posterior Inferior

Match up the muscle with the numbers on the left side of the body?Serratus posterior inferior muscleLower fibers of trapezius muscleMiddle fibers of trapezius muscleUpper fibers of trapezius muscleLevator scapulae muscleRhomboid minor muscleSerratus posterior superior muscleSupraspinatus muscleSpine of scapulaInfraspinatus muscleTeres minor muscleTeres major muscleSerratus anterior muscleLatissimus dorsi musclePosterior lamella of thoracolumbar fasciaInferior angle of scapulaLigamentum nuchae
12
3 45 6
78
9
10
11
12
13
14
15
16
17
Superficial and deep dissection of neck, trunk, and shoulder (posterior view).
Serratus Posterior Superior
Serratus posterior superior.– Medial attachment. – Lateral attachment.
Function.– Blood supply– Innervation.
Serratus posterior inferior. – Medial attachment. – Lateral attachment.
Function. – Blood supply..– Innervation.

1. Posterior lamella of thoracolumbar fascia2. Middle fibers of trapezius muscle3. Lower fibers of trapezius muscle4. Teres major muscle5. Infraspinatus muscle6. Teres minor muscle7. Levator scapulae muscle8. Rhomboid minor muscle9. Rhomboid major muscle10. Spine of scapula11. Upper fibers of trapezius muscle12. Ligamentum nuchae13. Latissimus dorsi muscle
1
2
3 4
56
7
8
9
10
1112
13
Shoulder, back, and upper limb muscles (posterior view). This prosection is a of the superficial extrinsic muscles of back.

1. Deltoid muscle2. Trapezius muscle3. Teres major muscle4. Latissimus dorsi muscle5. Posterior lamella of thoracolumbar fascia6. Serratus posterior inferior muscle7. Rhomboid minor muscle8. Rhomboid major muscle9. Serratus posterior superior muscle10. Levator scapulae muscle11. Supraspinatus muscle12. Clavicle13. Acromion of scapula14. Teres major muscle15. Teres minor muscle16. Teres minor muscle17. Erector spinae muscles18. Erector spinae muscles19. Infraspinatus muscle20. Infraspinatus muscle
12
3
4
5
6
7
8
910
111213
14
1516
17
18
19 20
Extrinsic muscles of back (superficial and intermediate layers; posterior view). The superficial layer of extrinsic back muscles produces movement of the upper limb and, therefore, is in close proximity to other muscles of the the upper limb, such as the rotator cuff, and shoulder. The intermediate layer attaches to the vertebral column and ribs and produces elevation and depression of the rib cage.
Deep Group of Back Muscles
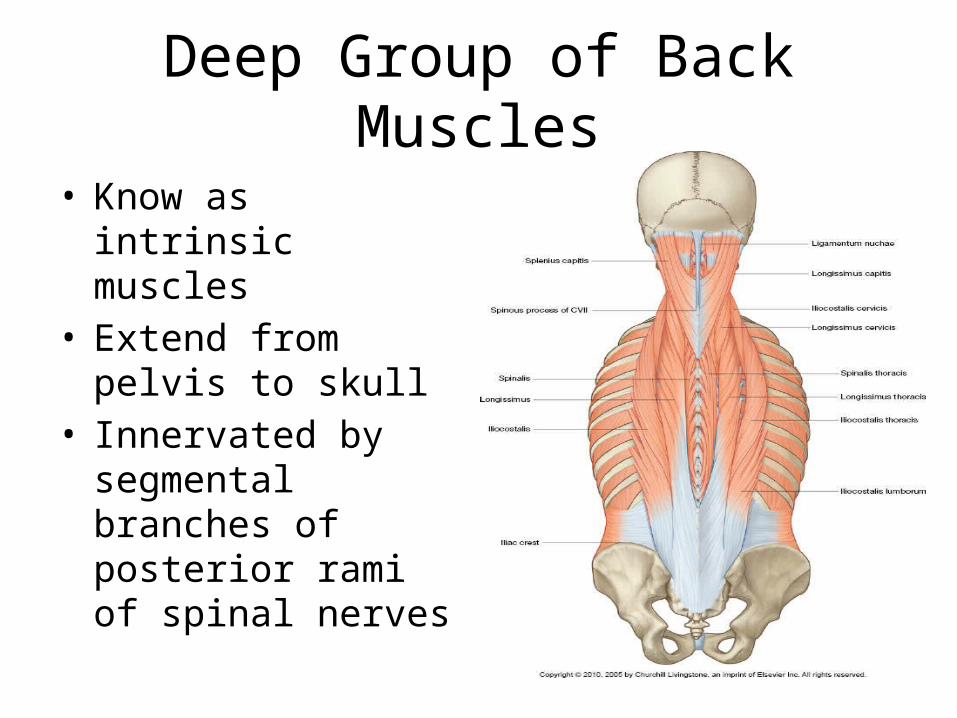
• Know as intrinsic muscles
• Extend from pelvis to skull
• Innervated by segmental branches of posterior rami of spinal nerves

Deep Group Back Muscles/Innervation

Back Muscles
Thoracolumbar fascia
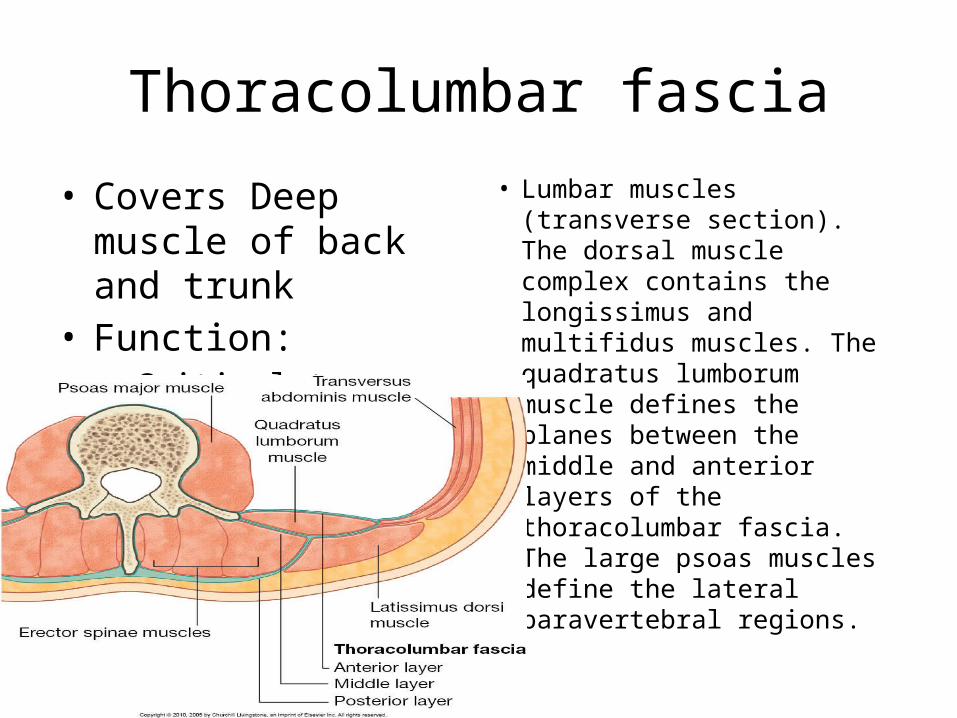
• Covers Deep muscle of back and trunk
• Function:– Critical to overall
organization and integrity of the region
• Lumbar muscles (transverse section). The dorsal muscle complex contains the longissimus and multifidus muscles. The quadratus lumborum muscle defines the planes between the middle and anterior layers of the thoracolumbar fascia. The large psoas muscles define the lateral paravertebral regions.

Deep Group of Muscles
• Spinotransversales Muscles:– Splenius Capitis– Splenius Cervicis
• Erector Spinae Muscle– Iliocostalis Lumborum– Iliocostalis thoracis– Iliocostalis cervicis– Longissimus thoracis– Longissimus cervicis– Longissimus capitis– Spinalis thoracis– Spinalis cervicis– Spinalis capitis

1. Interspinalis muscle2. Iliocostalis muscle3. Latissimus dorsi muscle4. Longissimus muscle5. Multifidus muscle
1
2
3
45
Axial CECT image of thoracolumbar junction. The erector spinae group (e.g., medial multifidus and the lateral iliocostalis muscles) are well defined here.

Deep Group of Muscles
• Transversospinalis Muscle Group– Semispinalis thoracis– Semispinalis cervicis– Semispinalis capitis– Mutifuidus– Rotatores lumborum– Rotatores Thoracis– Rotatores Cervicis
Suboccipital Muscles
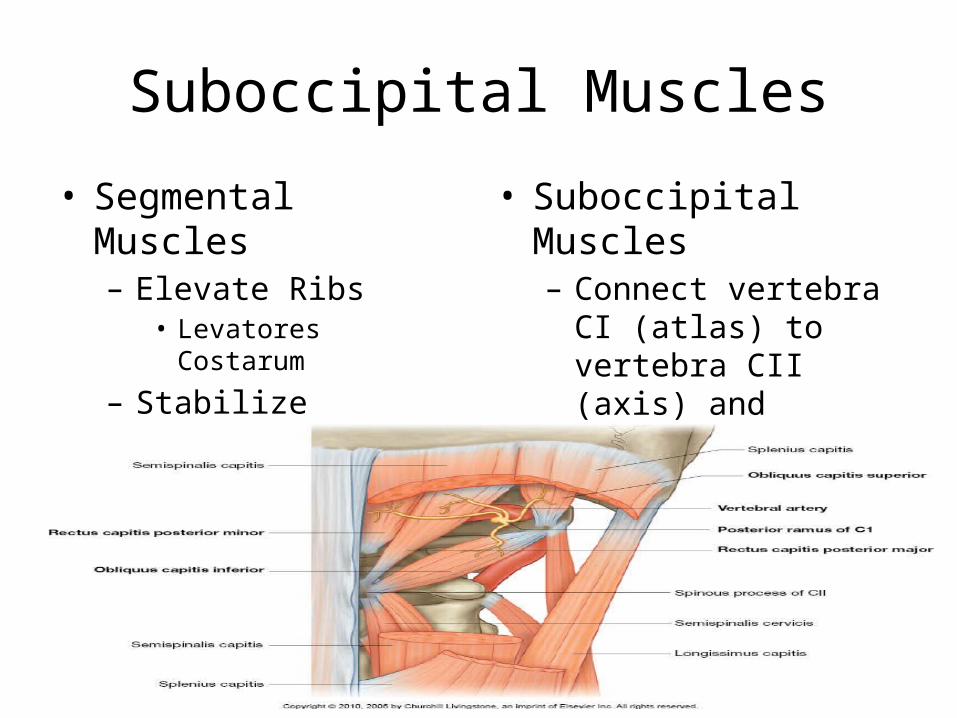
• Segmental Muscles– Elevate Ribs
• Levatores Costarum
– Stabilize Vertebra• Interspinales• Intertransversarii
• Suboccipital Muscles– Connect vertebra CI
(atlas) to vertebra CII (axis) and connect both vertebra to base of skull

Suboccipital Muscles
• Rectus capitis Posterior major– Extend head and rotate to same side
• Rectus capitis posterior minor– Extend head
• Obliquus capitis superior– Extend head and bend to same side
• Obliquus capitis inferior– Rotation of head to same side

Spinal Cord and Meninges
By Charles Curtis
Created by AnatomyOne™ on 04/20/2014

Spinal Cord
• The spinal cord is located within the vertebral canal and transitions from medulla oblongata to spinal cord at the C1 vertebral level.
• The vertebral column grows faster than the spinal cord during development and, therefore, ends at the sacrum in a fetus, the L3-L4 vertebral levels in a newborn, and the L1-L2 vertebral levels in an adult.
• The spinal cord is protected by the segmented vertebral canal, which is flexible yet strong, and solid and spinal meninges.

1. Dura mater2. T1 spinal nerve3. Dorsal root ganglion4. Foramen magnum
1
2
3
4 4
Vertebral column (coronal section; posterior view).

1. Cranial dura mater2. Transverse sinus3. Spinal dura mater4. Posterior cutaneous nerve5. Vertebral canal6. Greater occipital nerve
12
3
4
5
6
Dissection of trunk showing dorsal rami (posterior view).

Spinal Cord• The spinal cord is the postcranial part of the central nervous
system (CNS) and consists of approximately 100 million neurons and 500 million glial cells.
• It sits in the vertebral canal, where it is surrounded and protected by the meninges (dura mater, arachnoid mater, and pia mater).
• Spinal nerves transport sensory input from the body to the spinal cord, which processes these messages and sends appropriate motor responses to muscles and glands by way of spinal nerves.
• The spinal cord consists of white matter (nervous tissue consisting of myelinated axons) and gray matter (nervous tissue consisting of cell bodies and synapses).
• The spinal cord begins at the foramen magnum and ends at the L1-L2 vertebral level as the conus medullaris.

1. Central spinal cord canal2. Cervicomedullary junction3. Obex4. Nucleus gracilis5. Spinal cord6. Subarachnoid space7. Dura mater8. Epidural fat9. Nuchal ligament10. Dens11. C1 vertebra12. Spinous process of C613. Intervertebral disc
1
2
34
5
6
7
8
910
11
12
13
Cervical spinal cord (sagittal section; medial view). The central spinal cord canal is contiguous with the obex, the inferior point of the fourth ventricle. The transition from obex to central canal of the spinal cord is marked by the dorsal "bump" of the nucleus gracilis, which is easily seen on sagittal T2 MR scans through the craniocervical junction.

1. Spinal cord2. Posterior longitudinal ligament3. Dura4. Arachnoid5. Subarachnoid space6. Subdural space (potential space)7. Dura8. Arachnoid9. Extradural fat
1
2
3
4
56
7
8
9
Thoracic level of vertebral canal (sagittal section; medial view). This illustration shows the relationship of the central cord and the surrounding meninges within the vertebral canal. The thick dura defines the intra- and extradural compartments. The extradural compartment contains primarily fat and veins. The arachnoid mater is closely adherent to the inner dura, creating the potential subdural space. The subarachnoid space contains cerebrospinal fluid (CSF), which surrounds the spinal cord, and is continuous with intracranial subarachnoid CSF cisterns. The pia mater is closely adherent to the surface of the cord.

1. Cerebellum2. Cerebrum3. Spinal cord4. Spinal dura mater5. Cranial dura mater
1
2
3
4
5
Section of head and trunk (midsagittal section).

Spinal Cord
Spinal cord segments. The spinal cord is segmentally organized and consists of the following 31 segments:
– 8 cervical spinal cord segments corresponding to the 8 cervical spinal nerves. (only 7 cervical vertebrae)
– 12 thoracic spinal cord segments corresponding to the 12 thoracic spinal nerves.
– 5 lumbar spinal cord segments corresponding to the 5 lumbar spinal nerves.
– 5 sacral spinal cord segments corresponding to the 5 sacral spinal nerves.
– 1 coccygeal spinal cord segment corresponding to the lone coccygeal spinal nerve.
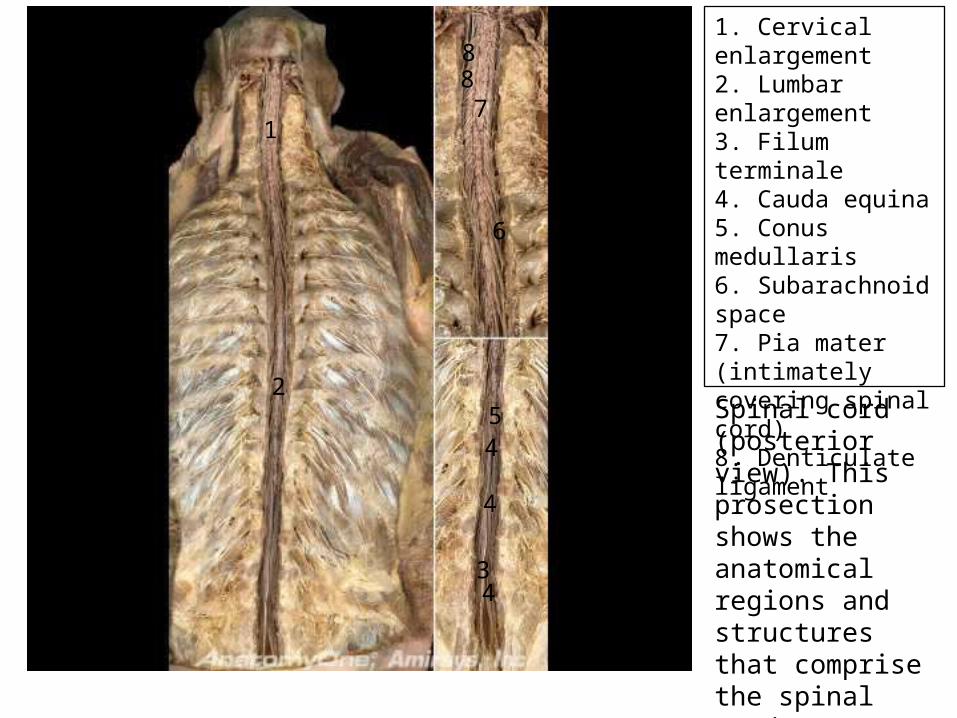
1. Cervical enlargement2. Lumbar enlargement3. Filum terminale4. Cauda equina5. Conus medullaris6. Subarachnoid space7. Pia mater (intimately covering spinal cord)8. Denticulate ligament
1
2
34
4
45
6
7
88
Spinal cord (posterior view). This prosection shows the anatomical regions and structures that comprise the spinal cord.
Spinal Cord
• The spinal cord is surrounded and protected by 3 meningeal layers within the vertebral canal called the:– Dura mater, – Arachnoid mater, and – Pia mater.
• Dura mater. Forms a protective dense fibrous connective tissue sheath around the spinal cord. Dura mater lines the internal surface of the skull and vertebral canal and terminates at the S2 vertebral level, where it forms the coccygeal ligament surrounding pial filum terminale.

Dura Mater
– Dural sleeves of spinal nerves. The dura also evaginates into each intervertebral foramen and becomes continuous with the epineurium around each spinal nerve. Nerve roots within the subarachnoid space lack dura mater and, therefore, are more fragile than spinal nerves.
– Epidural space. The region superficial to the dura mater between the dura mater and the vertebral canal.• An anesthetic agent injected into the epidural space
anesthetizes the spinal nerve roots exiting the vertebral canal in that region. Epidural blocks are particularly useful for procedures involving the pelvis and perineum, such as during childbirth.

1. Dentate ligament2. Dorsal root3. Dura mater4. Arachnoid mater5. Conus medullaris6. Cauda equina7. Filum terminale8. T12 spinal nerve
12
3
4
5
6
6
7
8
Caudal end of spinal cord (sagittal section; posterior view).
Spinal Cord• Subdural space. The potential space located between the dura and
arachnoid mater.
– Arachnoid mater. Forms the intermediate meningeal layer deep to the dura mater. It is attached to the underlying pia mater by numerous cellular extensions called arachnoid trabeculae. The arachnoid trabeculae look like spider webs and receive the name "arachnoid" from its root word for spider.• Subarachnoid space. The space between the arachnoid mater and
pia mater. It contains cerebrospinal fluid (CSF), which suspends the brain, spinal cord, and nerve roots, as well as the arteries and veins that supply the spinal cord.– Lumbar puncture to obtain CSF. The spinal cord terminates in an adult at
the L1–L2 vertebral levels, whereas the subarachnoid space containing CSF extends to the S2 vertebral level. Therefore, CSF can be obtained inferior to the L2 vertebral level without danger of injuring the spinal cord.
Spinal Cord• Dural sac. Region of the subarachnoid space between
the conus medullaris (L1 vertebral level) and beginning of the coccygeal ligament (S2 vertebral level). It contains the cauda equina and filum terminale suspended within CSF.
– Pia mater. The deepest meningeal layer composed of 1-2 layers of epithelial cells that form an inseparable lining around the spinal cord surface. It contains a small plexus of blood vessels.

Spinal Cord• Denticulate ligaments. Located in the coronal plane as a series
of sawtooth projections of the pia mater that separate the ventral and dorsal rootlets of the spinal nerves. The ligaments anchor the spinal cord to the surrounding arachnoid and dura mater. The denticulate ligaments maintain a centralized location for the spinal cord within the subarachnoid space.
• Filum terminale. An inferior extension of pia mater beyond the conus medullaris that anchors the spinal cord to the coccyx in the vertebral canal.– In utero, the spinal cord extends the entire length of the vertebral canal.
However, as development progresses and the vertebrae grow at a faster rate, the spinal cord withdraws superiorly and the sleeve of pia mater that originally surrounded the spinal cord in the caudal region of the vertebral canal collapses upon itself resulting in the formation of the filum terminale.

1. Dural nerve root sleeve2. Dura mater3. Arachnoid mater4. Subarachnoid space5. Pia mater (on spinal cord)6. Epidural fat7. Subdural (potential) space8. Spinal cord9. Anterior spinal artery
1
2
3
45
6
7 8
9
Spinal cord and meninges (cutaway illustration; oblique view). This illustration shows the meningeal layers and their relationships to adjacent regional structures.

Spinal Cord
– Innervation of spinal dura mater. Recurrent meningeal nerves from each spinal nerve segment along the vertebral canal provide general sensory innervation to the spinal cord dura mater.• The function of the sensory innervation is somewhat
unclear; however, it is commonly accepted that sensory neurons in the dura mater supply pain receptors involved in referred pain characteristic of spinal disorders and become irritated when the meninges are inflamed as in meningitis

Paralysis (Quadriplegia, Paraplegia)
By Charles Curtis

Paralysis (Quadriplegia, Paraplegia)
• Complete loss or impairment of motor function of both lower extremities (paraplegia) or all 4 extremities (quadriplegia or tetraplegia)
• Signs and symptoms. Patients may complain of slowly or rapidly progressive loss of motor function in the extremities. Patients may also have acute loss of motor function following a traumatic event, stroke, or neurosurgical procedure.– Patients may describe weakness or complete inability to move
portions of their bodies. Depending on the pathologic process, sensation may be preserved, impaired, or completely lost.

1. Fracture-dislocation2. Cord contusions
1
1
2
2
Sagittal T2WI MR of cervical spine with fracture. This image shows a severe fracture-dislocation at C5-C6 with spinal cord compression and contusions.

Paralysis (Quadriplegia, Paraplegia)• Causes. The list of causes of paralysis is
long, and it is categorized below.– Trauma. – Extrinsic.
• Examples include spinal disc extrusions, spinal stenosis, tumors, abscess, metastatic disease, and hematomas among others.
– Ischemia/Infarct.– Inflammatory. There are multiple
syndromes that may result in demyelination within the brain or spinal cord.• multiple sclerosis and acute inflammatory
demyelinating polyradiculoneuropathy (also called Guillain-Barré syndrome).
• Myasthenia gravis is also an autoimmune disorder causing weakness or paralysis, but the neuromuscular junctions are affected rather than the axons or nerves.
– Infectious. Botulism – Congenital. – Neoplastic.
– Metabolic/Toxic. Deficiencies of vitamin B12 due to malabsorption or abnormal metabolism, copper deficiency, and nitrous oxide toxicity can lead to spinal cord degeneration causing weakness or paralysis.
– Other. The following 2 causes do not fall into any of the above categories:• Amyotrophic lateral sclerosis (ALS) is selective
degeneration of somatic motor neurons of the brainstem/spinal cord and large pyramidal neurons of motor cortex. ALS results in progressive loss of motor function to complete paralysis of unknown etiology.
• Syringomyelia is cystic expansion of the spinal cord due to multiple causes resulting in loss of sensory function followed by loss of motor function.
– Muscular dystrophy. Unlike the above causes, muscular dystrophy is a group of disorders that do not affect the nervous system. These disorders are characterized by progressive destruction of skeletal muscle
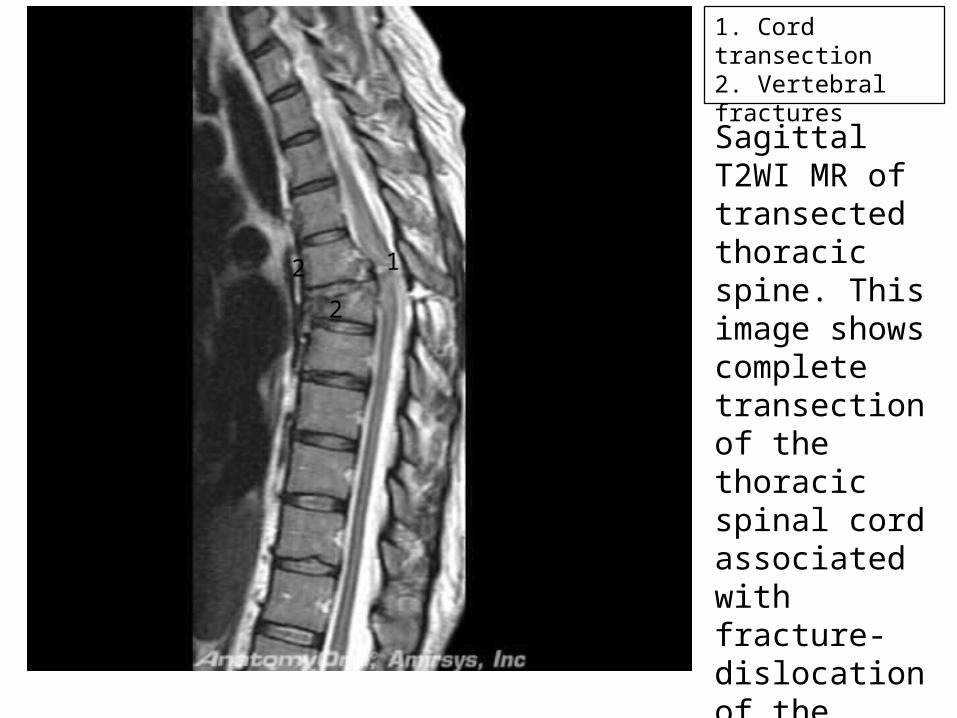
1. Cord transection2. Vertebral fractures
12
2
Sagittal T2WI MR of transected thoracic spine. This image shows complete transection of the thoracic spinal cord associated with fracture-dislocation of the adjacent vertebral levels.

Spinal Cord
• The spinal cord possesses the following external landmarks:– Anterior median fissure. Groove that separates the ventral
1/2s of the spinal cord and extends down the anterior surface of the spinal cord.
– Posterior median sulcus. Groove that separates the dorsal 1/2s of the spinal cord and extends down the posterior surface of the spinal cord.
– Posterolateral sulcus. Bilaterally located grooves along the posterolateral surface of the spinal cord that serve as the location where the dorsal rootlets of spinal nerves enter the spinal cord.

1. C5 spinal cord level2. T7 spinal cord level3. L1 spinal cord level4. S3 spinal cord level5. Lateral horn6. Central canal7. White matter8. Dorsal median sulcus9. Ventral median fissure10. Dorsal horn11. Ventral horn
1
2
3
4
5
6
7
8
9
10
10
11
11
Spinal cord (transverse sections). Contrast the ratio and amount of gray to white mater for each of the regions (cervical, thoracic, lumbar, and sacral).

Spinal Cord
• The spinal cord possesses white matter surrounding gray matter with a central canal.– White matter. Consists of vertical columns of axonal
tracts that surround a central core of gray matter. The white color is a result of the myelin that surround the axons.• Axonal tracts are organized to perform similar functions.
Ascending axonal tracts transport afferent information from dorsal horn gray matter to the brain. Conversely, descending axonal tracts conduct efferent information from the brain to neurons in the ventral horn gray matter.

Spinal Cord• The amount of white matter increases at each successive
higher spinal cord segment. Conversely, it decreases at each lower spinal cord segment.
• Cervical spinal cord levels have more white matter compared to thoracic, lumbar, and sacral levels due to the high number of ascending and descending fibers coming from and going to their destined spinal cord levels.
• The sacral spinal cord has the least amount of white matter because most ascending fibers are located superior to the sacral region and most descending fibers have ended at their destined spinal cord level superior to the sacral level.
Spinal Cord
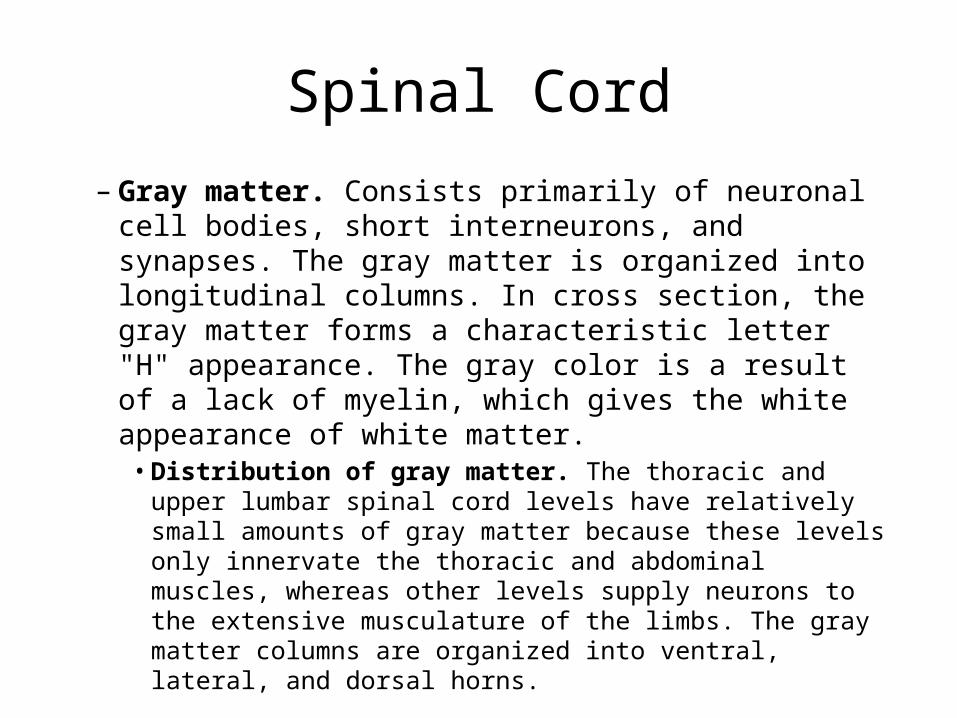
– Gray matter. Consists primarily of neuronal cell bodies, short interneurons, and synapses. The gray matter is organized into longitudinal columns. In cross section, the gray matter forms a characteristic letter "H" appearance. The gray color is a result of a lack of myelin, which gives the white appearance of white matter.• Distribution of gray matter. The thoracic and upper lumbar
spinal cord levels have relatively small amounts of gray matter because these levels only innervate the thoracic and abdominal muscles, whereas other levels supply neurons to the extensive musculature of the limbs. The gray matter columns are organized into ventral, lateral, and dorsal horns.
Clinical Question
• Question: A 1st-year radiology resident is looking through axial spine MR images. Identify the most likely characteristics she uses to distinguish cervical spinal cord levels from the other spinal cord levels.– Smallest amount of white matter and high amount of gray
matter– Highest amount of white matter and small amount of gray
matter– Smallest amount of white matter and small amount of gray
matter– Highest amount of white matter and high amount of gray
matter

Spinal Cord• Ventral horn. Contains the cells bodies for motor neurons whose
axons exit the ventral root to innervate the deep back (epaxial) muscles via dorsal rami and the body wall and limb (hypaxial) muscles via ventral rami. Along its length, a spinal cord ventral horn is not uniform and possesses enlargements in the cervical and lumbosacral regions.– Cervical spinal enlargement. Ventral horn gray matter in the C5-T1 spinal
cord segments contain a large number of motor neuron cell bodies that give rise to axons forming the brachial plexus, which innervates upper limb muscles. It is this increased number of cell bodies in the ventral horn that results in the swelling of the cervical spinal cord.
– Lumbosacral spinal enlargement. Ventral horn gray matter in the L2-S3 spinal cord segments contains a large number of motor neuron cell bodies that give rise to axons forming the lumbosacral plexus, which innervates lower limb muscles. It is this increased number of cell bodies in the ventral horn that results in the swelling of the lumbosacral spinal cord.

Horns of Spinal Cord

Spinal Cord• Lateral horn. Contains the cell bodies for preganglionic autonomic
motor neurons and is only seen in some regions of the spinal cord.– Sympathetic. Preganglionic sympathetic neurons originate only in the lateral
horns of the T1-L2 spinal cord levels.– Parasympathetic. Preganglionic parasympathetic neurons originate only in the
lateral horns of the S2-S4 spinal cord levels. Due to the large ventral horns that result in the lumbosacral enlargements, it may be difficult to distinguish the lateral horns in the sacral spinal cord levels.
• Dorsal horn. Receives sensory neurons entering the spinal cord via the dorsal roots. It also contains the cell bodies of interneurons that communicate with motor neurons in the ventral horn or ascend up tracts in the white matter.
– Central canal. Located within the middle of the gray matter as an adult remnant of the neural tube. It generally does not contain CSF and has no clinical significance.

1. Junction of dural sleeve and spinal nerve perineurium2. Dura mater3. Epidural fat4. Arachnoid mater5. Dural nerve root sleeve6. Subdural space7. Denticulate ligament8. Spinal cord and pia mater9. Arachnoid trabeculae10. Epidural fat
1
2 3
4
5
6
78
9910
Thoracic spinal cord and spinal nerves (transverse section; superior view). The nerve root sleeves are directly contiguous with the dura mater, which joins the peripheral nerve epineurium lateral to the neural foramen. Arachnoid mater lines the root sleeves. The web-like tissue within the subarachnoid space represents the inner arachnoid trabeculae (septum posticum). The denticulate ligaments arise between the dorsal and ventral spinal nerve roots and anchor the spinal cord laterally to the dura mater of the thecal sac.

Spinal Cord Arterial Supply

Clinical Question
• A 34-year-old man presents with back pain and minimal lower extremity weakness with paresthesias. MR imaging reveals a subdural hemorrhage in the middle-to-lower thoracic canal suggestive of a dissecting aneurysm arising from the artery of Adamkiewicz. Identify the space where blood is pooling in this patient.– Between the arachnoid mater and pia mater– Between the pia mater and spinal cord– Between the vertebral bone and dura mater– Between the dura mater and arachnoid mater– Within the central canal
Spinal Cord Veins/Meninges

Spinal Cord
• The vertebral canal is longer than the spinal cord in adults due to their unequal growth during fetal development.– Example. A C4 vertebral fracture could potentially have a bone
fragment press against the C4 spinal cord segment. However, a patient with a T11 vertebral fracture could potentially have a bone fragment that would press against the L1 spinal cord segment. Spinal cord levels and vertebral levels do not always necessarily correspond to each other in the horizontal plan
• Filum terminale. A delicate filament of pia mater that extends from the conus medullaris to the dural sac at the S2 vertebral level. It assists in tethering the spinal cord inferiorly.

Conus Medullaris
• Conus medullaris is the most caudal portion of the spinal cord containing sacral spinal cord levels. However, as a result of this unequal growth, the sacral spinal cord levels are located at the L1-L2 vertebral levels.– Cauda equina. The collection of dorsal and ventral roots in the
inferior region of the vertebral canal. The spinal cord ends at the L1-L2 vertebral levels, but the dorsal and ventral roots continue inferiorly down the vertebral canal to exit the intervertebral foramina at their appropriate vertebral levels.• For example, the S3 sacral nerve roots arise from the S3 spinal cord
level. However, the S3 spinal cord level is located at the L2 vertebral level and descends as part of the cauda equina to exit the vertebral canal via the S3 sacral foramina

1. L3 nerve root2. Dura3. L4 dural root sleeve and nerve4. L4 pedicle5. Filum terminale6. Arachnoid7. Cauda equina8. Conus medullaris
1
2
3
4
5
6
7
8
Cauda equina (coronal section; posterior view). This illustration demonstrates the relationship between dura mater and nerve roots. Note that the nerve root and sleeve exit the spinal canal just under the pedicle of the same numbered level.

Clinical Question
• A 35-year-old construction worker presents to the emergency department after falling from a 10-foot ladder onto his back. Radiographic imaging reveals a dislocated bone fragment pressing upon the underlying S1 level of the spinal cord. Identify the vertebral level most likely fractured.
• S1 vertebra• C1 vertebra• L1 vertebra• T1 vertebra

1. Ventral roots of cauda equina2. Dorsal roots of cauda equina3. Conus tip
11
223
Axial T2 MR images at L1 foraminal level. This image demonstrates the tip of the conus medullaris and cauda equina. At this level, the ventral and dorsal nerve roots of the cauda equina are separately positioned ventrally and dorsally, respectively, within the thecal sac.

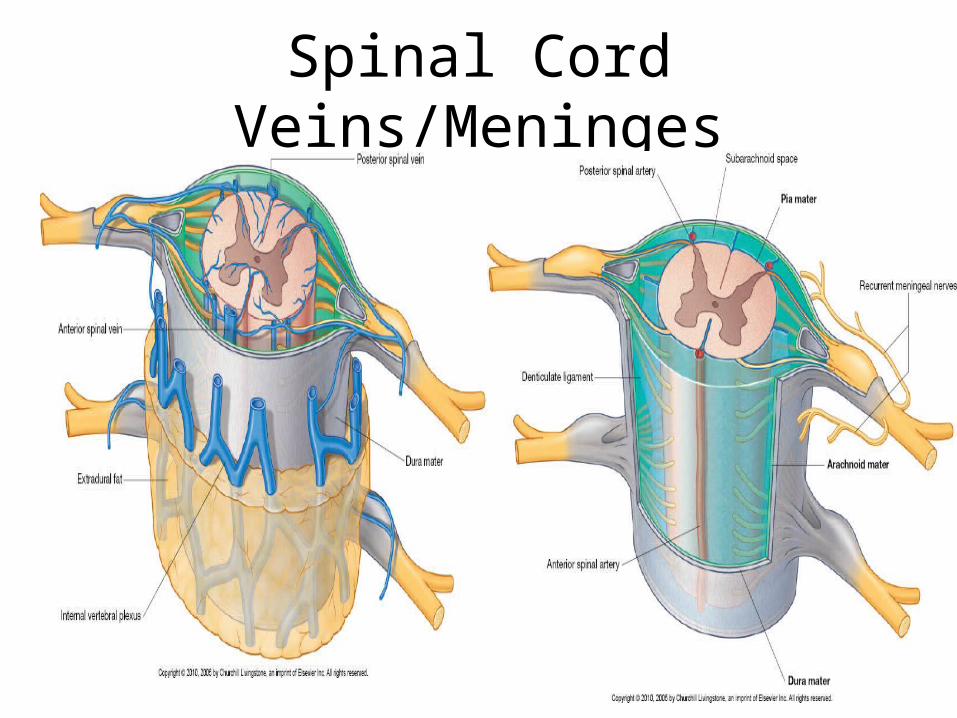
Spinal Cord Arterial Supply• The spinal cord receives arterial supply from the anterior spinal
artery and 2 posterior spinal arteries, which arise intracranially from the vertebral arteries.
• Anterior and posterior spinal arteries are joined segmentally by medullary arteries and radicular arteries, which arise from the ascending cervical artery, deep cervical artery, vertebral artery, posterior intercostal artery, lumbar artery, and lateral sacral artery.
• The veins of the spinal cord include the spinal veins, anterior medullary veins, posterior medullary veins, deep cervical vein, vertebral vein, posterior intercostal veins, lumbar veins, and lateral sacral veins.
• These veins drain into the large venous plexuses within the vertebral canal.
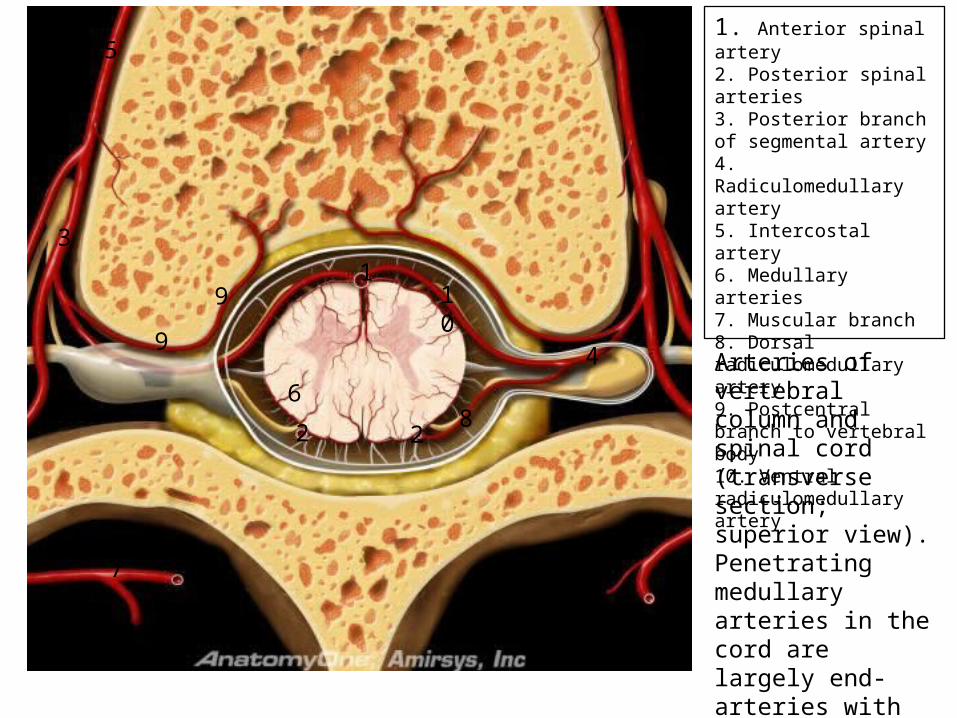
1. Anterior spinal artery2. Posterior spinal arteries3. Posterior branch of segmental artery4. Radiculomedullary artery5. Intercostal artery6. Medullary arteries7. Muscular branch8. Dorsal radiculomedullary artery9. Postcentral branch to vertebral body10. Ventral radiculomedullary artery
1
2 2
3
4
5
6
7
8
9
9
10
Arteries of vertebral column and spinal cord (transverse section; superior view). Penetrating medullary arteries in the cord are largely end-arteries with few collaterals. The cord "watershed" zone is at the central gray matter.
Spinal Cord Arterial Supply
• Great anterior segmental medullary artery (of Adamkiewicz). The largest anterior segmental medullary artery supplying the spinal cord.
• It reinforces arterial supply to the lower 2/3rds (thoracolumbar region) of the spinal cord.
• Most of the time it arises from the left side between T12 and L1.
• However, it may also arise anywhere between T7 and L4.

Spinal Nerves
By Charles Curtis

Spinal Nerves• Spinal nerves are the functional components of the postcranial
peripheral nervous system. • Spinal nerves travel from the spinal cord of the central nervous system
to the somites of the body wall and lateral mesoderms of the limbs. • The typical spinal nerve consists of motor (efferent) fibers that arise
from cell bodies located in the spinal cord and of sensory (afferent) fibers that arise from cell bodies located in the dorsal root ganglion of the spinal nerve itself.
• Immediately after the motor and sensory fibers merge to form a spinal nerve, the spinal nerve divides into a ventral ramus and a dorsal ramus.
• The dorsal rami segmentally innervate deep back muscles (motor) and the skin of the back (sensory).
• The ventral rami distribute to the hypaxial muscles of the myotome, including the limbs, and the overlying parts of the dermatome.
Spinal Cord

1. Dorsal primary rami2. Multifidus muscle3. Semispinalis muscle
1
1
1
2
3
Epaxial (trunk) muscles (posterior view). Dorsal rami segmentally innervated the skin of the back in a dermatomal pattern and innervated the deep back muscles, such as the erector spinae and transversospinalis muscles. Dorsal rami do not innervate the limbs or face.

1. Dorsal primary rami2. Greater occipital nerve (dorsal ramus of C2)3. Dura mater surrounding spinal cord4. Superior cluneal nerve (dorsal rami in gluteal region)
1
1
1
2
3
4
Dissection of trunk showing dorsal rami (posterior rami). Dorsal rami segmentally innervated the skin of the back in a dermatomal pattern and innervated the deep back muscles, such as the erector spinae and transversospinalis muscles. Dorsal rami do not innervate the limbs or face.
Spinal Nerves
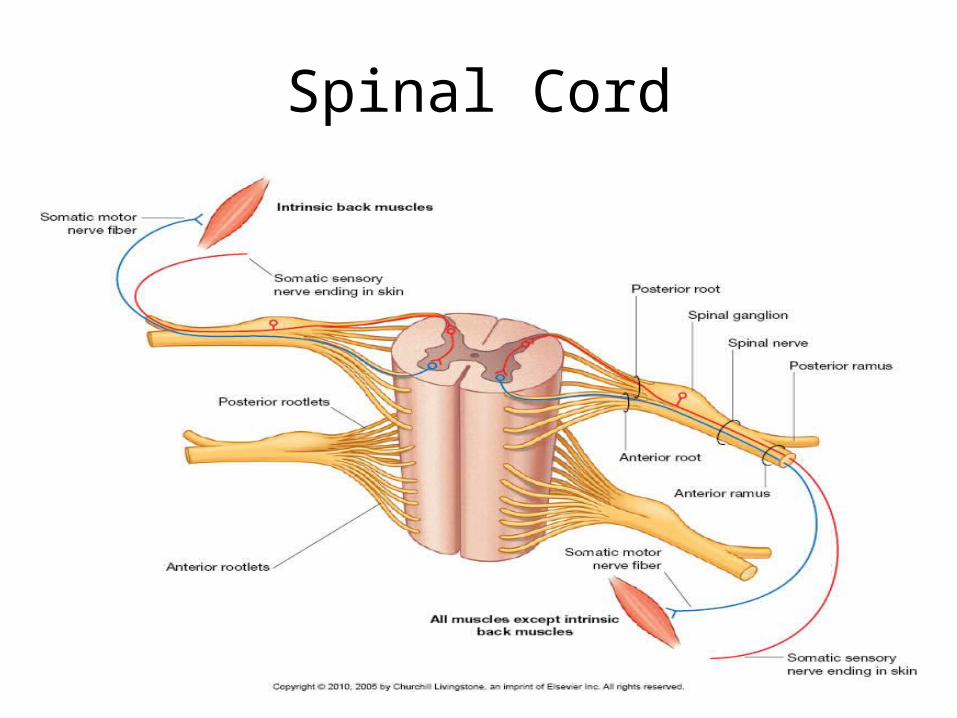
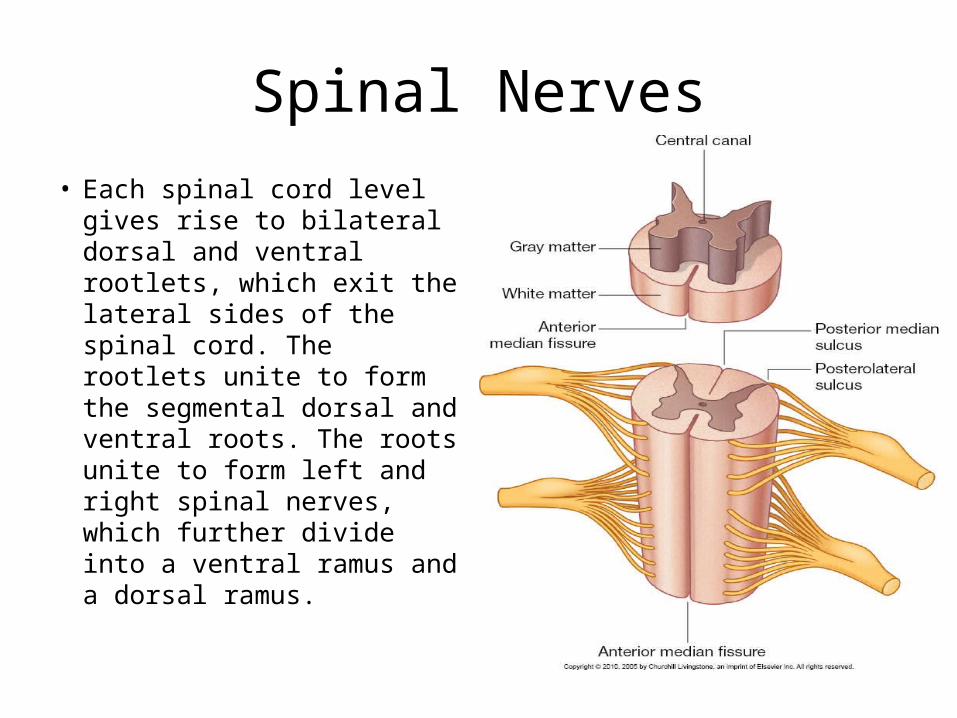
• Each spinal cord level gives rise to bilateral dorsal and ventral rootlets, which exit the lateral sides of the spinal cord. The rootlets unite to form the segmental dorsal and ventral roots. The roots unite to form left and right spinal nerves, which further divide into a ventral ramus and a dorsal ramus.

Nerve Roots
• Roots are paired and carry either motor or sensory fibers, but not both.
• Ventral and dorsal roots are separated within the vertebral canal by the denticulate ligaments.
• The vertebral canal is longer than the spinal cord in adults due to unequal growth during fetal development. Consequently, nerve roots follow an oblique course from superior to inferior.
• At the intervertebral foramen, roots unite to form the spinal nerve trunk.

Nerve Roots– Ventral root. Contains motor (efferent) fibers from lateral and
ventral horn nerve cell bodies that emerge as rootlets from the ventrolateral aspect of the spinal cord. These efferent fibers carry motor impulses from the spinal cord to the skeletal muscles of the myotome and to the migrating neural crest cells that form the postganglionic autonomic neurons.
– Dorsal root. Contains sensory (afferent) fibers that join the spinal cord as rootlets through the dorsolateral sulcus to enter the dorsal horn of the spinal cord. These afferent fibers carry sensory information from body tissues, such as skin and organs, to the spinal cord.• Dorsal root ganglion. A swelling in the dorsal root that houses the cell
bodies of all sensory neurons entering the spinal cord for that specific body segment.

1. Sympathetic ganglion2. Intercostal nerve3. Ventral ramus4. Dorsal ramus5. Ventral root6. Dorsal root7. Dorsal root ganglion8. Gray and white rami communicantes9. Thoracic vertebral body10. Dorsal horn of gray mater11. Ventral horn of gray mater12. Lateral horn of gray mater13. Spinal nerve trunk14. Subarachnoid space15. Arachnoid trabeculae16. Spinous process17. Transverse process18. Epidural fat19. Dura mater20. Arachnoid mater21. Denticulate ligament
1
2
3
4
5
6
7
88
9
10
1112 13
14
15
16
17
18
1920
21
Spinal cord and spinal nerve (transverse section; superior view). This illustration depicts the dorsal and ventral nerve roots arising from the dorsolateral and ventrolateral sulci, respectively, and are separated by the denticulate ligaments. The roots form a spinal nerve trunk, which then gives rise to ventral and dorsal primary rami. The ventral ramus supplies ventral musculature and skin while the dorsal ramus is smaller and supplies deep back muscles and overlying skin.

Cauda Equina
• Cauda equina. In adults, the spinal cord extends within the vertebral canal from the foramen magnum to approximately the level of the L1-L2 vertebrae. – At this level, the ventral and dorsal nerve roots associated
with more inferior vertebral levels branch from the spinal cord and descend in the vertebral canal in a pattern that resembles a horse's tail (cauda equina).• The cauda equina floats in cerebrospinal fluid (CSF); therefore, a
needle introduced into the subarachnoid space inferior to the L2 vertebral level will displace roots with little possibility of damage to them or the spinal cord

1. Spinal cord levels2. C1 vertebral level3. T12 vertebral level4. C1 spinal nerve exiting superior to C1 vertebra5. C8 spinal nerve exiting inferior to C7 vertebra6. T1 spinal nerve exiting inferior to T1 vertebra7. Cauda equina8. T12 spinal nerve exiting inferior to T12 vertebra9. T12 spinal cord level10. S1 vertebral level11. S1 spinal nerve12. S1 spinal cord level
1 2
3
4
56
7
8
9
1011
12
Spinal cord and spinal nerves (coronal section of vertebral canal; posterior view). In the neck, cervical spinal nerves exit superior to their associated vertebra. Inferior to the cervical region, each spinal nerve from the thoracic, lumbar, and sacral spinal cord segments exits inferior to its associated vertebra. The adult spinal cord terminates at the L1 vertebral level. Observe the differences in vertebral, spinal cord, and spinal nerve levels in the caudal regions of the vertebral column.

Spinal Nerve Roots by Region
• The spinal roots unite in or near the intervertebral foramen to form a spinal nerve. The 31 pairs of spinal nerves formed by the dorsal and ventral roots are organized as follows:– 8 cervical spinal nerves. The first 7 cervical spinal nerves, C1–C7,
exit the vertebral canal superior to each respective cervical vertebra. The last cervical nerve, C8, exits inferior to C7.
– 12 thoracic spinal nerves. Exit inferior to the 12 thoracic vertebrae.
– 5 lumbar spinal nerves. Exit inferior to the 5 lumbar vertebrae.– 5 sacral spinal nerves. Exit inferiorly through the dorsal sacral
foramina of the sacrum.– 1 coccyx spinal nerve. Exits by the coccyx bone.

1. Intercostal nerves2. Sciatic nerve3. L4 spinal nerve exiting at L4-5 level4. T12 spinal nerve exiting at T12-L1 level5. C8 spinal nerve exiting inferior to C7 vertebra6. C1 spinal nerve exiting superior to C1 vertebra7. T1 spinal nerve exiting inferior to T1 vertebra8. Brachial plexus9. Lumbosacral plexuses10. L1 spinal nerve11. C5 spinal nerve12. C7 spinal nerve13. T4 spinal nerve14. T10 spinal nerve15. C6 spinal nerve
1
2
3
4
5
6
78
9
10
1112
13
14
15
Spinal nerve roots (coronal section; anterior view). The C1 root exits between the occiput and C1, while the C8 root exits at the C7-T1 level. Thoracic and lumbar roots exit below their respective pedicles. Each segmental spinal nerve transports sensory information from its associated dermatome. For example, the C6 spinal nerve carries all sensory neurons from the C6 dermatome covering the lateral forearm and thumb.
Brachial Plexus Injury
• Damage inflicted on the brachial plexus, a group of nerves that supplies the shoulder, arm, and hand.

Brachial Plexus Injury
• Signs and symptoms. Brachial plexus injury results in pain and paralysis in a distribution that depends on the specific nerves affected. Patients may have a limp arm with lack of muscle control and loss of feeling in the arm, wrist, &/or hand. Common clinical profiles include:

Brachial Plexus Injury
– Erb palsy. Upper brachial plexus injury resulting in a limp arm that hangs at the side of the body. The forearm is extended at the elbow and pronated. The arm cannot be raised, and the forearm cannot be flexed or supinated. This injury pattern results from a direct blow to the neck/shoulder area or from a birth traction injury.
– Klumpke palsy. Lower brachial plexus injury resulting in a claw hand deformity where the forearm is supinated and the wrist and fingers are flexed. This injury pattern results from sudden pulling on an arm that is abducted. An example would be a person who falls from a tree and grasps a branch to break the fall.
Brachial Plexus Injury
• Causes. Typically, a brachial plexus injury is the result of excessive stretching. This may cause rupture of the nerve along its course in the neck &/or shoulder area or avulsion of the nerve root from the spinal cord.– Birth complication. Often, the stretching injury happens during
birth if the shoulder becomes impacted in the birth canal (shoulder dystocia).
– Trauma. Traumatic causes of brachial plexus injury can occur while playing sports, during falls from a significant height, or in a motor vehicle accident. In such cases, direct impact to the side of the neck and shoulder can cause violent stretching. Gunshot and knife wounds can transect nerves in the brachial plexus.

Brachial Plexus Injury• Physical exam. Patient has paralysis (on exam) and loss of sensation in
a nerve distribution correlating to the specific location of nerve disruption.
• Procedures. Diagnosis confirmation may be made by electromyography (EMG), which is a technique for evaluating and recording muscle electrical activity. Findings of muscle denervation will be evident on EMG, but it may take 5-7 days after the injury for EMG to be positive.
• Imaging. MR is the imaging method of choice for diagnosing brachial plexus injury. If the nerve root has been pulled off of the spinal cord (avulsed), then a cerebral spinal fluid (CSF)-filled sac-like outpouching may extend from the dural sac of the spinal cord. The outpouching will contain no nerve root. In a stretch injury without avulsion, the nerve roots may be thick and irregular or thin and stretched but intact.– CT can also be used to evaluate for brachial plexus injury, but bright contrast
must first be injected into the spinal canal. This procedure is called CT myelography and may be used if the patient has a contraindication for MR

Spinal Nerve Roots

Dermatomes of the body. Dermatomes are a region of skin where all sensory neurons contained within that area travel to the same spinal nerve level. For example, sensory neurons arising from the lateral part of the forearm and hand eventually terminate in the dorsal root of the C6 spinal nerve.

Spinal Nerves Sub division
• Immediately distal to the intervertebral foramen, each spinal nerve divides into a ventral ramus and a dorsal ramus.– Ventral ramus. Segmentally provides innervation of the skin and
hypaxial muscles of the anterolateral aspects of the torso and limbs. Ventral rami of spinal nerves from the cervical, lumbar, and sacral regions of the spinal cord form nerve plexuses en route to their dermatome and myotome targets. They are known as the cervical plexus, brachial plexus, lumbar plexus, and sacral plexus.
– Dorsal ramus. Segmentally provides sensory innervation from the skin of the back and upper gluteal region, and motor innervation to the deep (epaxial) muscles of the back, such as the erector spinae and transversospinalis muscles. Dorsal rami do not contribute innervation to the limbs or face.

1. Ventral rootlets2. Spinal nerve3. Dorsal rootlets4. Dorsal root ganglion5. Ventral horn6. Dorsal horn7. Spinal cord within vertebral canal8. Spinous process9. Intervertebral foramen10. Pia mater, arachnoid mater, and dura mater
1
2
33 4
567
8
9
10
10
10
Step dissection of vertebral column, spinal nerves, spinal meninges, and spinal cord (oblique view).

1. Sensory portion of dorsal ramus (posterior cutaneous nerve)2. Dorsal ramus3. Motor portion of dorsal ramus in erector spinae muscle4. Ventral ramus5. Lateral cutaneous nerve6. Anterior cutaneous nerve7. Ventral root8. Dorsal root ganglion and dorsal root9. Sympathetic ganglion10. Spinal nerve
1
2
3
4
5
6
78 8
9
10
Thoracic region (transverse section). This illustration demonstrates spinal roots, nerves, and rami. The dorsal rami give rise to motor innervation to deep back muscles (i.e., erector spinae muscles) as well as the skin of the back (posterior cutaneous nerves).

1. Cauda equina2. Ventral primary ramus3. Dorsal primary ramus4. Deep vertebral muscles (erector spinae)5. Ventral root6. Intervertebral foramen7. Dorsal root ganglion1 2
3
4
56 7
Lumbar muscles (transverse section). Dorsal rami segmentally innervate the skin of the back in a dermatomal pattern and innervate the deep back muscles, such as the erector spinae and transversospinalis muscles.

1. Uncinate process2. Intervertebral foramen3. Zygapophyseal joint4. Intervertebral disc5. Vertebral body, posterior margin6. Pedicle7. Pedicle8. Exiting spinal nerve roots9. Vertebral body10. Segmental vessels
1
2
3
4
5
6
7
8
8
9
1010
Cervical vertebrae and spinal nerves (sagittal section). Observe exiting spinal nerves within lower part of intervertebral foramen. Neural foramina are oriented anterolaterally (compare with thoracic and lumbar regions). Anterior boundary of neural foramen include uncinate process, intervertebral disc and vertebral body from inferior to superior. Pedicles form superior and inferior boundaries. Posterior boundary is the facet joint complex.

1. Exiting spinal nerve2. Intervertebral foramen3. Zygapophyseal joint4. Intervertebral disc5. Pedicle6. Inferior articular process7. Superior articular process8. Vertebral body9. Anterior longitudinal ligament10. Posterior longitudinal ligament
1
2
3
4
5
67
8
9
10
Intervertebral discs (sagittal section). This illustration shows thoracic vertebrae and spinal nerves. The exiting nerve is positioned superiorly bounded by the vertebral body anteriorly, pedicle above and zygapophyseal (facet) joint posteriorly. Facet joints are oriented in near coronal plane in thoracic spine.

1. L4 vertebral body2. Pedicle3. Inferior articular process4. Zygapophyseal joint5. L5 vertebral body6. S1 vertebral body7. Anterior longitudinal ligament8. Nucleus pulposus9. Annulus fibrosus10. Exiting L4 spinal nerve11. Segmental artery and vein12. Pars interarticularis13. Superior articular process14. Posterior longitudinal ligament15. Exiting S1 spinal nerve
1
2
34
5
6
7
8
9
10
1111
12
13
14
15
Lumbar vertebrae and spinal nerves (sagittal section). Observe position of exiting nerves within the superior aspect of the intervertebral foramen. The segmental vessels are located inferior to the exiting nerve. Intervertebral foramina are bounded anteriorly by dorsal vertebral body above and intervertebral disc below, pedicle above and zygapophyseal (facet) joint and ligamentum flavum posteriorly. The lumbar vertebral bodies are large, with a large intervening intervertebral disc. The pedicles are directed posteriorly, giving rise to large superior and inferior articular facets.

1. Conus medullaris2. Filum terminale3. Cauda equina4. Dura mater5. L4 spinal nerve6. S1 spinal nerve7. L2 spinal nerve8. Sacrum9. Transverse process of L410. Transverse process of L211. Pedicle of L3
1
2
3
4
5
6
7
8
9
10
11
Cauda equina (coronal section; posterior view). This illustration demonstrates the distal thoracic spinal cord and nerve roots of the cauda equina. Note that the cord ends in a diamond-shaped point, the conus medullaris. Lumbar nerve roots exit the thecal sac just under the pedicles of their same-numbered vertebral segments.

1. Filum terminale2. Conus medullaris3. Dura mater4. Cauda equina5. Spinal cord6. Nerve root
1
2
3
4
5
6
Thoracolumbar junction (sagittal view). This illustration demonstrates the conus medullaris and cauda equina. The cauda equina is a collection of nerve roots inferior to the L1 vertebral level where spinal cord ends.
Clinical Questions (True/False)
• 1. The peripheral nervous system includes cranial nerves.
• 2. The peripheral
nervous system consists of 43 pairs of nerves and their branches.
• 3. Myotome is a term referring to a skeletal muscle group innervated by motor neuron axons from a given spinal nerve.
• 4. The sacral plexus is found deep within the shoulder.
• 5. Skeletal muscles are somatic effectors.

Clinical Questions
• 6. Autonomic effectors require two efferent neurons.
• 7. Each spinal nerve
attaches to the spinal cord via two short roots.
• 8. The parasympathetic division is the dominant controller of the body at rest.
9. Sympathetic preganglionic neurons begin within the brain.

Clinical Questions• 10. The peripheral nervous system contains only efferent
nerves. • 11. Even though there are only seven cervical vertebra, this
region generates eight cranial nerves. • 12. The nerves emerging from the lower lumbar and sacral
regions branch from a structure called the cauda equina, not the spinal cord itself.

Chapter 2
Surface Anatomy

Surface Anatomy
• Locate muscle groups• Test peripheral nerves• Identify vertebral column level• Locate organs

What do you notice???

Surface Anatomy
• Lateral View (Sagittal Plane):– Primary Curvature
• Thoracic• Sacral• coccygeal
– Secondary Curvatures• Cervical • Lumbar

Skeletal Landmarks
• Non Vertebral:– External Occipital
Protuberance– Scapular– Iliac Crest
• Vertebral Spinous Process
Inferior End Spinal Cord
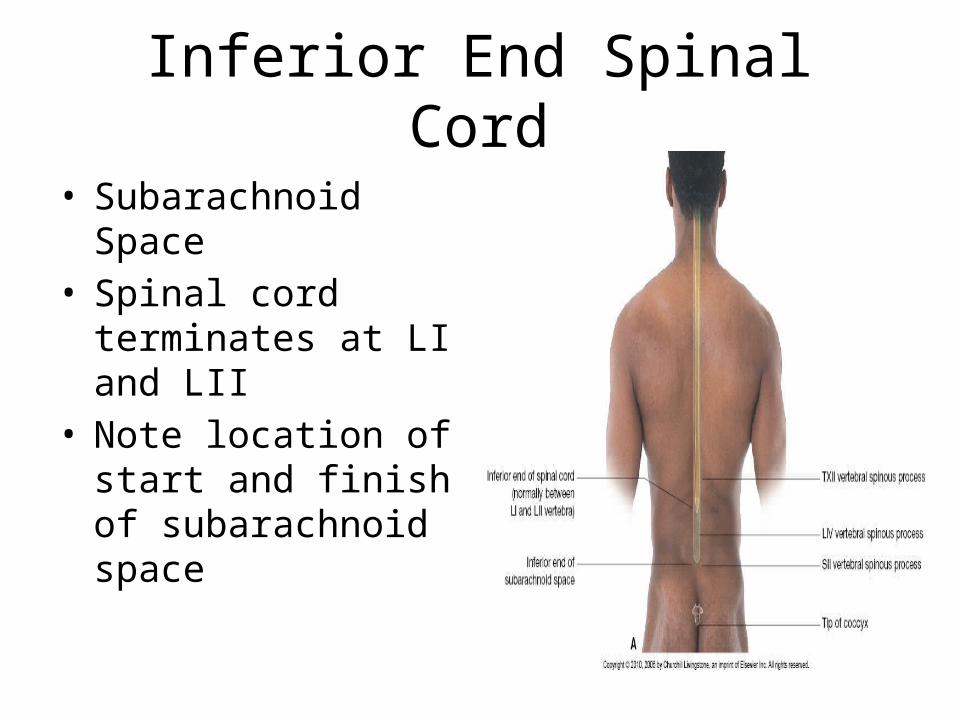
• Subarachnoid Space• Spinal cord terminates
at LI and LII• Note location of start
and finish of subarachnoid space

Identify Major Muscle Groups
Chapter 3Thorax
Charles Curtis
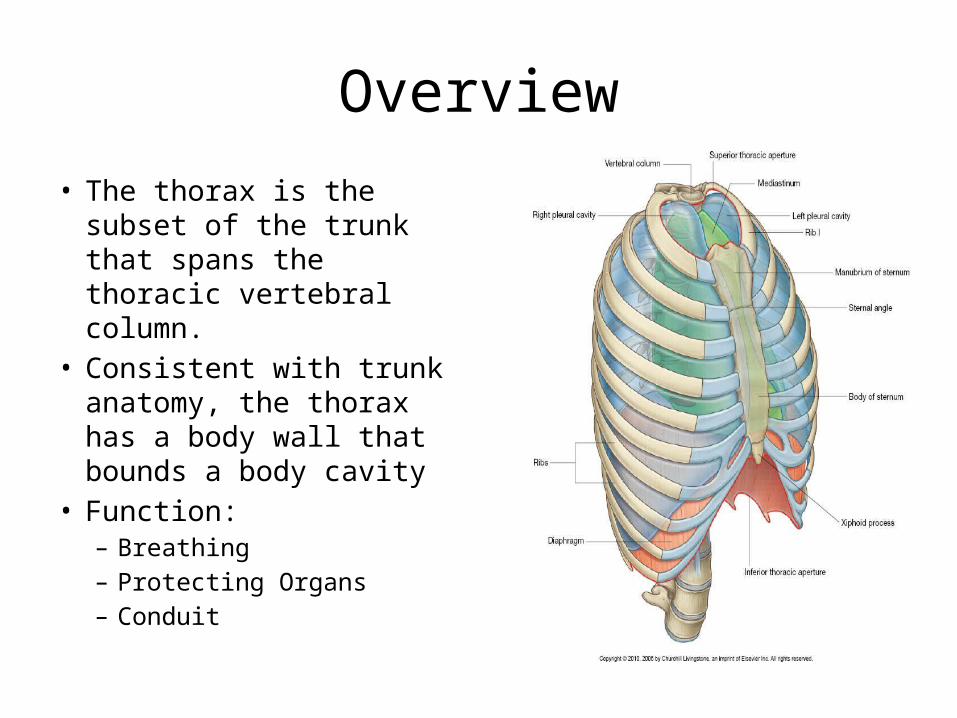
Overview
• The thorax is the subset of the trunk that spans the thoracic vertebral column.
• Consistent with trunk anatomy, the thorax has a body wall that bounds a body cavity
• Function: – Breathing– Protecting Organs– Conduit

Overview
• It differs from the other trunk regions (i.e., neck, abdomen, and pelvis) in that the costal skeletal elements of the body wall do not get incorporated into the vertebrae but instead become the ribs of the thoracic cage. – The wall is composed of dorsal epaxial muscles,
the vertebral extensors, and ventral hypaxial muscles that are segmentally separated by the ribs.

Overview Cont
– The true musculoskeletal wall of the thorax (the limb and head muscles that migrate onto the thorax are not true body wall muscles) is invested in fascia, an external investing (deep) fascia superficial to the musculoskeletal wall, and an internal investing (endothoracic) fascia deep to the musculoskeletal wall. • Superficial to the external investing fascia is the
subcutaneous layer and skin. • Deep to the internal investing fascia is the extraserosal layer
and parietal serosa.
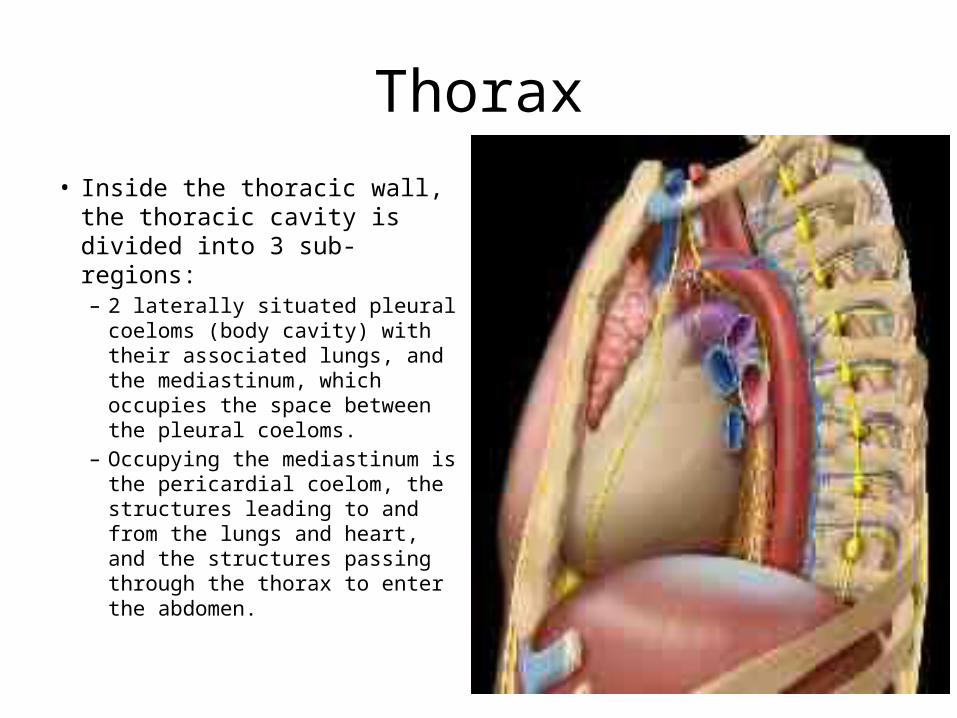
Thorax• Inside the thoracic wall, the
thoracic cavity is divided into 3 sub-regions: – 2 laterally situated pleural
coeloms (body cavity) with their associated lungs, and the mediastinum, which occupies the space between the pleural coeloms.
– Occupying the mediastinum is the pericardial coelom, the structures leading to and from the lungs and heart, and the structures passing through the thorax to enter the abdomen.

Thorax


Overview• The outermost (supracostal)
muscles of the lateral body wall, of both the neck and thorax, are annexed by the scapula to suspend it from the thoracic and cervical skeleton.
• As a result of this relationship with the upper limb, the musculofascial anatomy of the thorax is more complex than that of the abdomen.
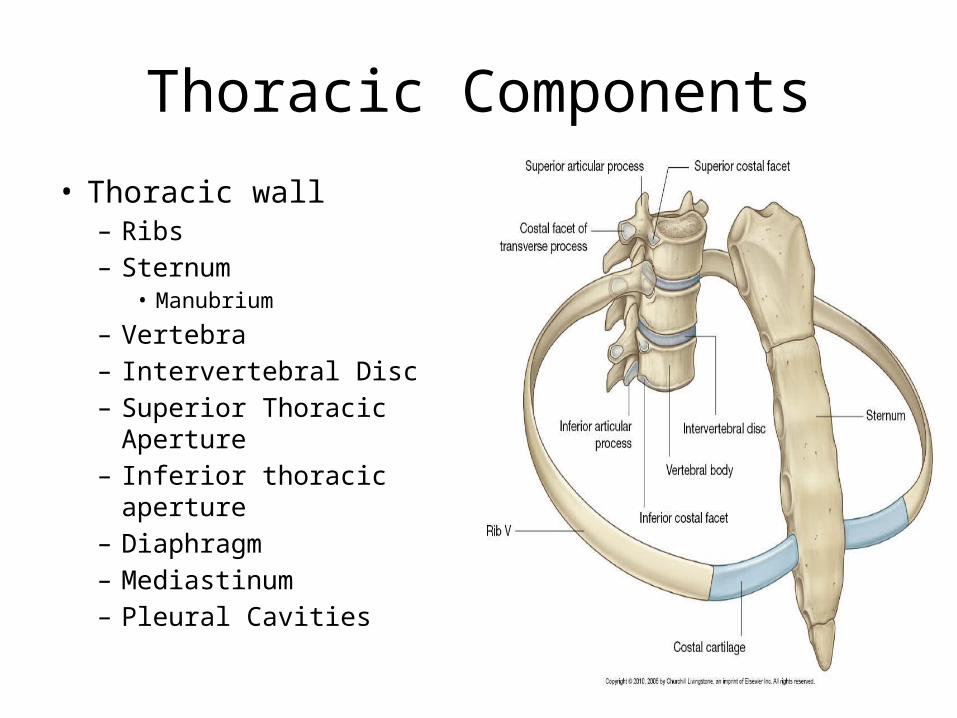
Thoracic Components
• Thoracic wall– Ribs– Sternum
• Manubrium
– Vertebra– Intervertebral Disc– Superior Thoracic Aperture– Inferior thoracic aperture– Diaphragm– Mediastinum– Pleural Cavities

Thoracic Components

Lungs and Bronchial Tree
By Charles Curtis
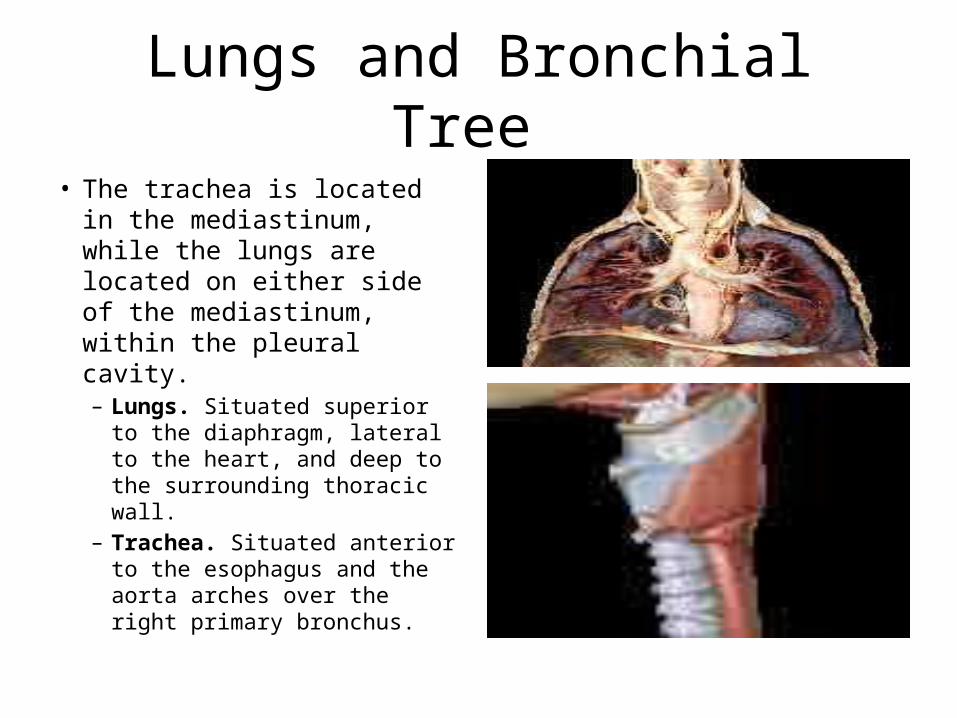
Lungs and Bronchial Tree
• The trachea is located in the mediastinum, while the lungs are located on either side of the mediastinum, within the pleural cavity.– Lungs. Situated superior to
the diaphragm, lateral to the heart, and deep to the surrounding thoracic wall.
– Trachea. Situated anterior to the esophagus and the aorta arches over the right primary bronchus.

Lungs• The lungs are paired organs of respiration. The right lung
is larger than the left and has 3 lobes, whereas the left has only 2.– Anatomic features. Include the following:
• Apex. • Base. • Surfaces. The lungs have the following 3 surfaces:
– Costal surface. – Mediastinal surface.– Diaphragmatic surface..
• Borders. The lungs have the following 3 borders:– Anterior border..– Inferior border. – Posterior border.
• Hilum. • Pulmonary ligament• Bronchopulmonary segments.

1. Left base2. Right costal surface3. Right inferior border4. Left anterior border5. Cardiac notch of left anterior border6. Right apex
1
2
3
4
5
6
Lungs (anterior view). This illustration depicts the surface anatomy of the anterior lungs. The shape of each lung resembles that of a 1/2 cone. The lung surface anatomy is characterized by an apex, a base, 2 surfaces, and 3 borders. The apices represent the highest extent of the lungs. The anterior borders separate the anterior costal surfaces from the mediastinal (medial) surfaces. Note the arcuate morphology of the inferior aspect of the left anterior border, the cardiac notch. The costal surfaces are adjacent to the chest wall. The inferior borders separate the costal surfaces from the bases.

1. Lung apices2. Left lung3. Right lung4. Chest wall5. Mediastinum
1 1
22
33
3
444
5
Lungs in situ (anterior view). This illustration depicts the anatomy of the anterior lungs. The lungs are surrounded by the pleura and the skeletal and soft tissue structures of the chest wall. The 2 lungs are located on either side of the mediastinum. Each lung is freely mobile within its surrounding pleural space and is attached to the mediastinum at the hilum and pulmonary ligament. The lung apices project above the medial clavicles and anterior 1st ribs and course towards the roots of the neck. The right lung has 3 lobes and is larger than the left lung. The left lung has 2 lobes.

Right Lung• Right lung. Located in the right pleural cavity. It possesses 3 lobes, which
are separated by horizontal and oblique fissures. The right lung is larger, shorter, and wider than the left lung because the heart takes up more room on the left, and the diaphragm is higher on the right side.– Lobes. The right lung is divided into the following 3 lobes:
• Superior lobe. Forms the anterior and superior portions of the right lung.• Middle lobe. Forms the anterior and inferior portions of the right lung. The middle lobe
is the smallest lobe of the right lung and is wedge-shaped. Note that the left lung does not have a middle lobe but has a lingula instead.
• Inferior lobe. Forms the posterior and inferior portions of the right lung.
– Fissures. Invaginations of visceral pleura between the lobes of the lung. The right lung has the following 2 fissures:• Horizontal fissure. Located between the superior and middle lobes.• Oblique fissure. Located between the middle and inferior lobes.
– Contact impressions. Indentations on the lung from the azygos vein, heart, and esophagus. They can be identified on the embalmed lung of a cadaver but are not seen during surgery or on fresh lungs.

1. Posterior segment2. Anterior segment3. Apical segment4. Apical segment5. Posterior segment6. Superior segment7. Posterior basilar segment8. Lateral basilar segment9. Posterior basilar segment10. Medial segment11. Medial basilar segment12. Lateral basilar segment13. Lateral segment14. Anterior basilar segment15. Lateral segment
1
2
34
5
6
7
89
10
11
12
13
14
15
Right lung (anterior and posterior views). This illustration demonstrates bronchopulmonary segments. Here, the lung segments of each lobe are color-coded to correspond to the segmental bronchial origins.
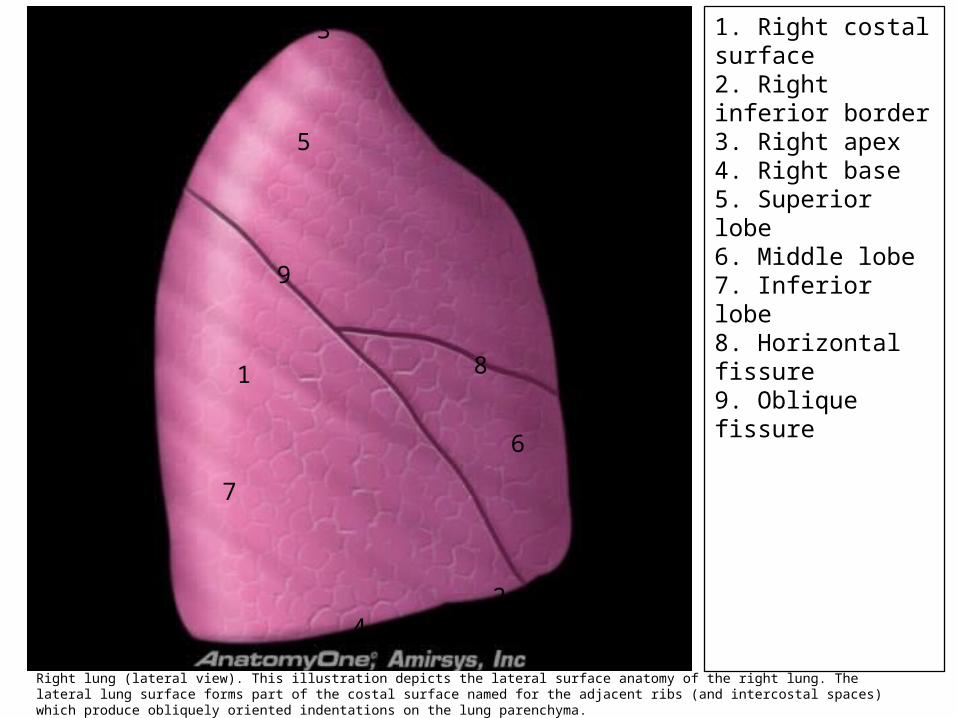
1. Right costal surface2. Right inferior border3. Right apex4. Right base5. Superior lobe6. Middle lobe7. Inferior lobe8. Horizontal fissure9. Oblique fissure
1
2
3
4
5
6
7
8
9
Right lung (lateral view). This illustration depicts the lateral surface anatomy of the right lung. The lateral lung surface forms part of the costal surface named for the adjacent ribs (and intercostal spaces) which produce obliquely oriented indentations on the lung parenchyma.

1. Azygos vein indentation2. Superior vena cava indentation3. Esophagus indentation4. Right cardiac indentation5. Right posterior border6. Right medial surface7. Right anterior border
1
2
3
4
5
6
7
Right lung (medial view). This illustration depicts the surface anatomy of the medial right lung. The mediastinal surface is concave and exhibits indentations produced by adjacent mediastinal structures, including vessels and organs. The right cardiac indentation is produced predominantly by the right atrium. The anterior border separates the mediastinal surface from the costal surface. The right hilum is located centrally on the mediastinal surface.

Left Lung• Left lung. Located in the left pleural cavity. The left lung is smaller
than the right lung and has only 2 lobes separated by an oblique fissure.– Superior lobe. Forms the anterior and superior portions of the left lung.
• Lingula. A tongue-like extension of the superior lobe of the left lung over the heart. The lingula serves as the homologue to the middle lobe of the right lung and has 2 distinct bronchopulmonary segments (superior and inferior).
• Cardiac notch. Concave gap on the medial side of the superior lobe, where the heart lies.
– Inferior lobe. Forms the posterior and inferior portions of the left lung.– Oblique fissure. An oblique invagination of visceral pleura located
between the superior and inferior lobes.The oblique fissure of the left lung is more vertical than the oblique fissure of the right lung.
– Contact impressions. Indentations on the lung from the aortic arch, heart, and descending aorta. They can be identified on the embalmed lung of a cadaver but are not seen during surgery or on fresh lungs

1. Left cardiac indentation2. Aortic arch indentation3. Esophagus indentation4. Left lung base5. Left anterior border6. Descending aorta indentation
1
2
3
4
5
6
Left lung (medial view). This illustration depicts the surface anatomy of the medial left lung. The mediastinal surface exhibits indentations produced by adjacent mediastinal structures. The left cardiac indentation is predominantly produced by the left ventricle. The descending aorta indents the left lower lobe and correlates with visualization of the retrocardiac descending aorta on frontal chest radiographs.

1. Left costal surface2. Left apex3. Left inferior border4. Left base5. Superior lobe6. Inferior lobe7. Oblique fissure8. Lingula9. Cardiac notch
1
2
34
5
6
7
8
9
Left lung (lateral view). This illustration depicts the lateral surface anatomy of the left lung. The lateral surface forms part of the costal surface. The inferior border separates the costal surface from the base.

1. Middle lobe2. Superior lobe3. Superior lobe4. Inferior lobe5. Inferior lobe
1
1
2 3
45
Lungs (anterior view). This prosection shows the right lung as being larger, shorter, and wider than the left lung; the heart takes up more "room" on the left side.
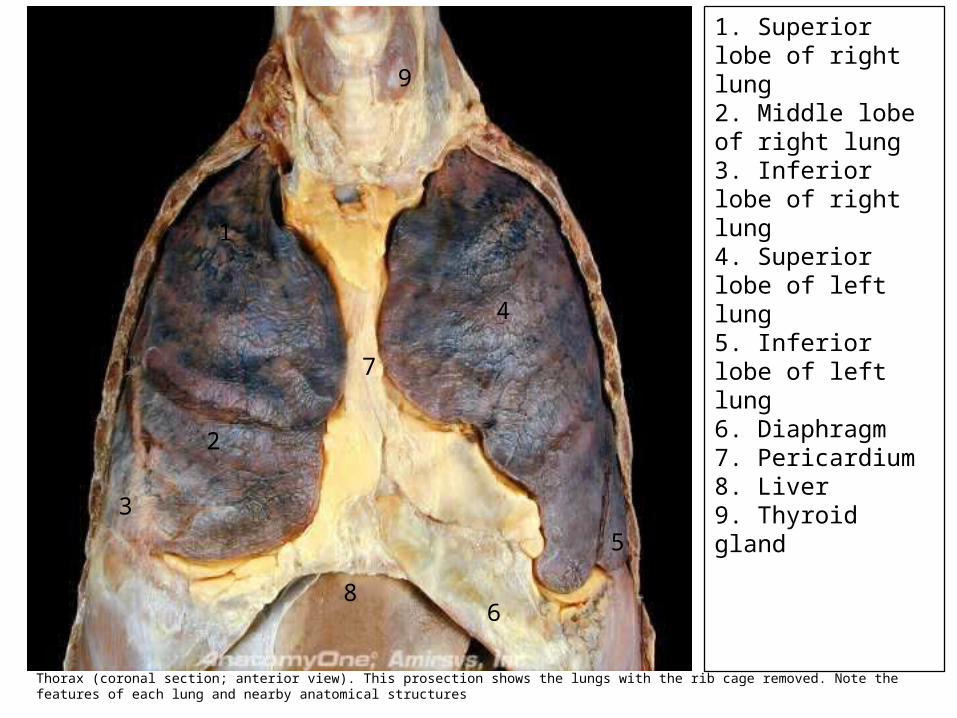
1. Superior lobe of right lung2. Middle lobe of right lung3. Inferior lobe of right lung4. Superior lobe of left lung5. Inferior lobe of left lung6. Diaphragm7. Pericardium8. Liver9. Thyroid gland
1
2
3
4
5
6
7
8
9
Thorax (coronal section; anterior view). This prosection shows the lungs with the rib cage removed. Note the features of each lung and nearby anatomical structures

1. Pulmonary vein2. Right main bronchus3. Middle lobe4. Inferior lobe5. Left pulmonary artery6. Lobar bronchus7. Inferior lobe8. Superior lobe9. Lingula
111112
34
56
7
8
9
Lungs (medial view of each lung). Note the structures located in the hilum.

1. Anterior segment2. Apicoposterior segment3. Apicoposterior segment4. Superior segment of left lower lobe5. Posterior basilar segment6. Anteromedial basilar segment7. Lateral basilar segment8. Posterior basilar segment9. Inferior lingular segment10. Superior lingular segment
1
23
4
5
6
77
8
9
10
Left lung (anterior and posterior views). This illustration demonstrates bronchopulmonary segments. Here, the lung segments of each lobe are color-coded to correspond to the segmental bronchial origins.

Bronchial Tree• The bronchial tree is a series of tubes that transport air to and from the lungs. It
consists of the trachea, bronchi, and bronchioles.– Trachea. Referred to as the windpipe. It is the superiormost portion of the bronchial tree.
The trachea transports air from the larynx to the carina and consists of 16-20 flexible C-shaped hyaline cartilage rings. The trachea is about 10-12 cm (4-5 inches) long and 2.5 cm (1 inch) in diameter.• Carina. Appears as a raised ridge of cartilage tissue in the sagittal plane and marks the bifurcation
of the left and right primary bronchi at the level of the sternal angle (T4-T5 vertebral level). The carina is extremely sensitive, and substances touching it will trigger a cough reflex.
– Bronchi. Cartilaginous tubes that carry air from the trachea to the microscopic bronchioles.• Primary bronchi. Located immediately inferior to the trachea. There are 2 primary bronchi: 1
traveling to the left lung and 1 to the right lung. The primary bronchi contain cartilage that holds the tubes open.– Right primary (main) bronchus. Travels from the trachea to the right lung. The right primary bronchus is larger,
shorter, and more vertical than the left and is thus a likely end point for inhaled objects, although inhaled objects may lodge anywhere in the proximal bronchial tree. The azygos vein arches over the right primary bronchus and joins with the superior vena cava.
– Left primary (main) bronchus. Travels from the trachea to the left lung. The left primary bronchus is more horizontally positioned than the right.
• Secondary (lobar) bronchi. Branch from the primary bronchi and supply each individual lobe. There are 2 left lobar bronchi and 3 right lobar bronchi.
• Tertiary (segmental) bronchi. Branch from the secondary bronchi and supply the bronchopulmonary segments.

1. Trachea2. Primary bronchus3. Lobar (secondary) bronchus4. Segmental (tertiary) bronchus5. Right lung6. Right primary bronchus7. Azygos vein8. Pulmonary veins9. Aorta10. Left common carotid artery11. Esophagus12. Central tendon of diaphragm13. Diaphragm14. Vagus nerve (CN X)
1
23
45
67
88
9
10
11
12
13
14 14
Thorax with bronchial tree and diaphragm (coronal section; anterior view). This dissection shows the relationship between the bronchial tree and the lungs.

1. Left superior pulmonary vein2. Left inferior pulmonary vein3. Left pulmonary artery4. Left main bronchus5. Inferior pulmonary ligament6. Mediastinal pleural reflection
1
2
3
4
5
6
6
Left hilum (medial view). This illustration shows the location of the left hilum on the mid portion of the mediastinal lung surface. The left bronchus is situated posteriorly within the mid hilum. The pulmonary artery is located above the hyparterial left bronchus. The superior and inferior pulmonary veins are located anterior and inferior to the left bronchus respectively.

1. Right pulmonary ligament2. Right inferior pulmonary vein3. Right superior pulmonary vein4. Right pulmonary artery branches5. Right bronchi6. Mediastinal pleural reflection
1
2
3
4
45
6
6 Right hilum (medial view). This illustration shows the central location of the hilum on the mediastinal lung surface and the location of the hilar structures. The upper hilum contains the superior pulmonary vein, right pulmonary artery and right bronchi (from anterior to posterior). The inferior pulmonary vein is located inferiorly. Normal hilar lymph nodes are depicted in green.

1. Intrapulmonary lymph node2. Perivascular lymphatics3. Peribronchial lymphatics4. Intrapulmonary lymph nodes5. Subpleural lymphatics6. Hilar lymph node
122
3
44
5
6
Lymphatic network of the lungs (coronal section). The pulmonary lymphatics are found along bronchi, vessels, and in the subpleural connective tissue. Collecting lymphatics also course within the pulmonary connective tissue septa. The lymphatic network becomes organized as small intrapulmonary lymph nodes that typically occur at the bifurcations of large airways.

Pleural Effusion
• The presence of fluid in the pleural space.
• Signs and symptoms. The patient's presentation may vary from entirely asymptomatic to severely dyspneic, or with symptoms related to the type of effusion (i.e., fever and cough with a purulent effusion from pneumonia).
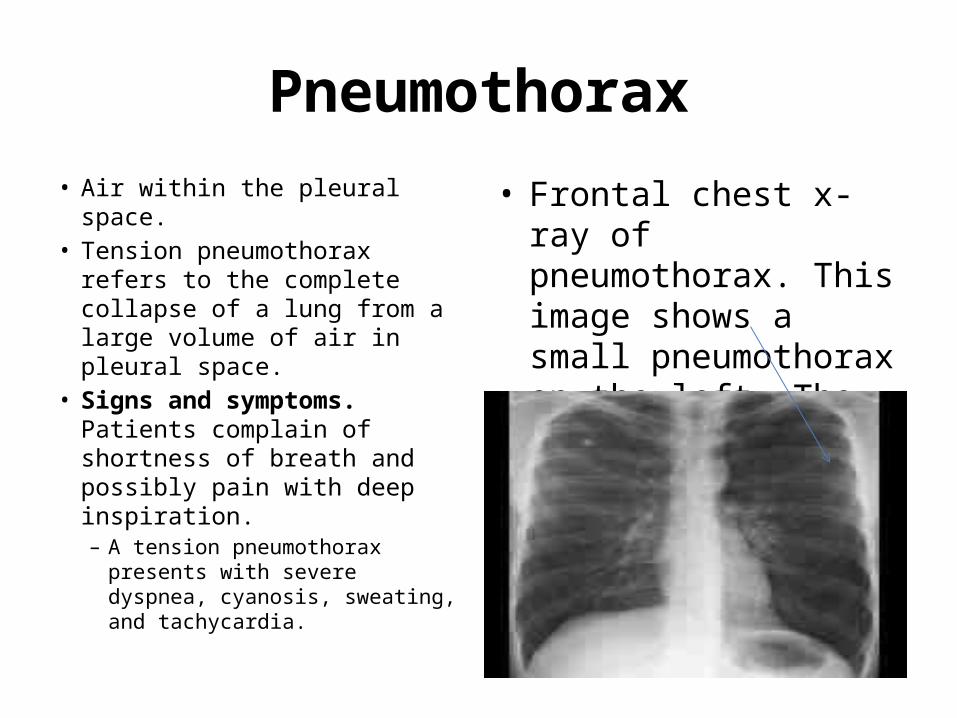
Pneumothorax• Air within the pleural space.• Tension pneumothorax refers
to the complete collapse of a lung from a large volume of air in pleural space.
• Signs and symptoms. Patients complain of shortness of breath and possibly pain with deep inspiration.– A tension pneumothorax
presents with severe dyspnea, cyanosis, sweating, and tachycardia.
• Frontal chest x-ray of pneumothorax. This image shows a small pneumothorax on the left. The visceral pleural line is displaced medially, parallel to the chest wall.

Lung Microstructures• Air travels through a series of microscopic tubes until it eventually reaches the alveoli,
where gas exchange occurs. This region of microscopic tubing is called the acinus.– Terminal bronchioles. The terminal portion of the conducting zone of the respiratory system.
The terminal bronchioles are made of smooth muscle and can be identified under a microscope because they do not contain hyaline cartilage.
– Respiratory bronchioles. Branch from the terminal bronchioles and are the 1st structure in the respiratory zone of the bronchial tree. The alveoli project from their walls.
– Alveolar ducts. Branch from the respiratory bronchioles and lead into the alveolar sacs and alveoli.
– Alveolar sacs. Each consists of 2 or more alveoli that share a common opening.– Alveoli. Serve as the location for gas exchange. There are approximately 300 million alveoli in
the lungs. The alveoli possess elastic walls enabling them to recoil and change shape according to oxygen and carbon dioxide demand. The following cells form the alveolar walls:• Type I alveolar cells (pneumocytes). Simple squamous epithelial cells that are specialized for gas
exchange. These cells are very thin and lay adjacent to the pulmonary capillaries.• Type II alveolar cells (pneumocytes). Interspersed among the type I cells. The type II alveolar cells
secrete surfactant, which is a mixture of phospholipids and lipoproteins that decrease the surface tension within the alveoli.
• Alveolar macrophages (dust cells). Wandering phagocytes that remove debris from the alveoli.
– Respiratory membrane. Located at the junction of an alveolus and a pulmonary capillary. Gas exchange occurs here.
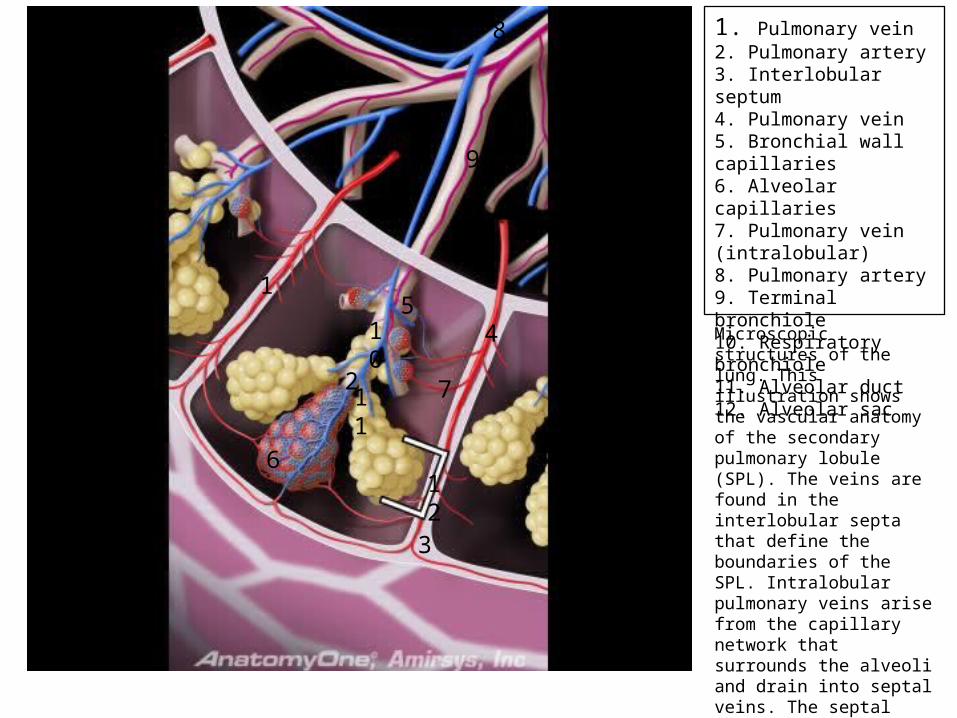
1. Pulmonary vein2. Pulmonary artery3. Interlobular septum4. Pulmonary vein5. Bronchial wall capillaries6. Alveolar capillaries7. Pulmonary vein (intralobular)8. Pulmonary artery9. Terminal bronchiole10. Respiratory bronchiole11. Alveolar duct12. Alveolar sac1
2
3
45
6
7
8
9
10
11
12
Microscopic structures of the lung. This illustration shows the vascular anatomy of the secondary pulmonary lobule (SPL). The veins are found in the interlobular septa that define the boundaries of the SPL. Intralobular pulmonary veins arise from the capillary network that surrounds the alveoli and drain into septal veins. The septal pulmonary veins drain more than one SPL. The pulmonary veins also drain the subendothelial capillary network of the airway walls and the visceral pleura.

1. Alveoli and alveolar ducts2. Bronchus (large airway)3. Bronchus (medium airway)4. Junction of terminal and respiratory bronchioles5. Terminal bronchiole6. Respiratory bronchiole (small airway)
11
1
2
3
45
6
Telescoping airway. This illustration depicts the decreasing size of the different airway types and the structural changes of the airway wall with a decreasing number and size of cartilage plates. Cartilage plates are present in large and medium-size airways but gradually become smaller and less numerous in the medium bronchi. The walls of the small airways (bronchioles) do not contain cartilage. Distal clusters of alveoli and alveolar sacs form acini, the pulmonary functional unit of gas exchange. The acinus is defined as the airways, vessels, and supporting structures distal to a terminal bronchiole.

Function of Lungs
• The primary purpose of the lungs is to facilitate gas exchange. The trachea and associated bronchial tree are simply transporters. No gas exchange occurs until air reaches the alveoli, where oxygen diffuses from the alveolus to the pulmonary capillary (for body cells) and carbon dioxide diffuses from the pulmonary capillary to the alveoli (to be exhaled).
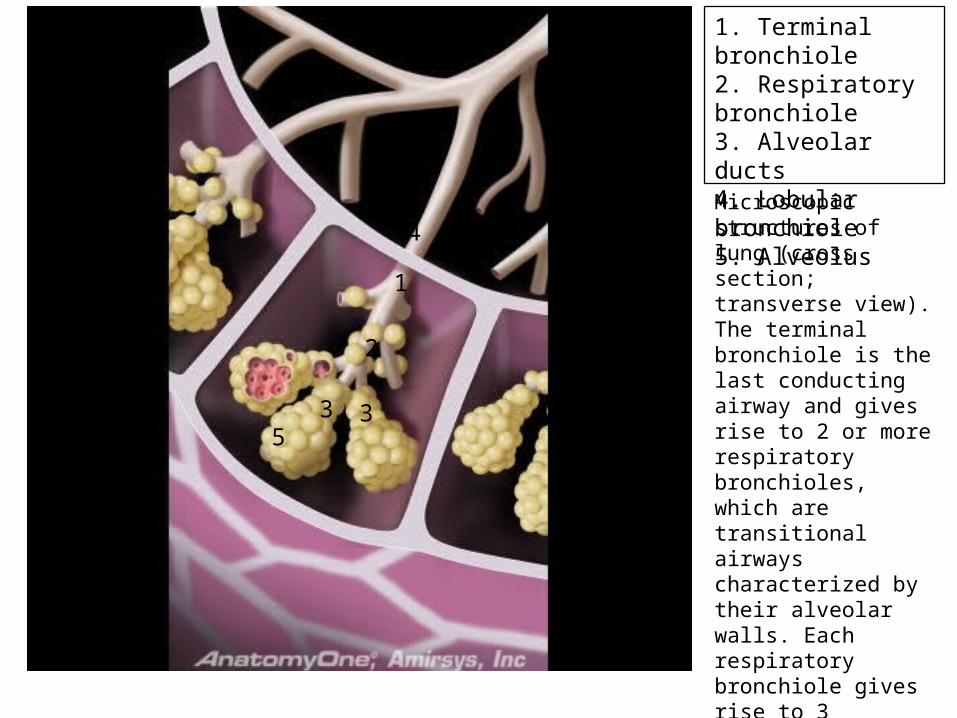
1. Terminal bronchiole2. Respiratory bronchiole3. Alveolar ducts4. Lobular bronchiole5. Alveolus
1
2
33
4
5
Microscopic structures of lung (cross section; transverse view). The terminal bronchiole is the last conducting airway and gives rise to 2 or more respiratory bronchioles, which are transitional airways characterized by their alveolar walls. Each respiratory bronchiole gives rise to 3 alveolar ducts which are airways lined by alveoli. The alveolar ducts terminate in alveolar sacs and alveoli.

1. Capillaries2. Alveolus3. Type 2 pneumocyte4. Alveolar macrophage5. Type 1 pneumocytes6. Tight cell junction
1
1
1
2 3
4
5
5
6
Microscopic structure of alveoli. The alveolar-capillary interface is the principal site of respiration where the alveoli come in contact with the rich capillary network of the lung. Inspired oxygen is delivered to the capillaries and carbon dioxide is delivered to the airway. The type 1 pneumocyte is a flat cell with tight cell junctions that lines the alveolar surface. The tight cell junctions prevent permeability of fluid into the alveolar space. The type 2 pneumocyte is a larger polygonal cell that produces surfactant and processes circulating vasoactive substances. The alveolar macrophage is a migratory cell that forms part of the defense mechanisms of the lung.

Structural Patterns of the Thorax
By Charles Curtis
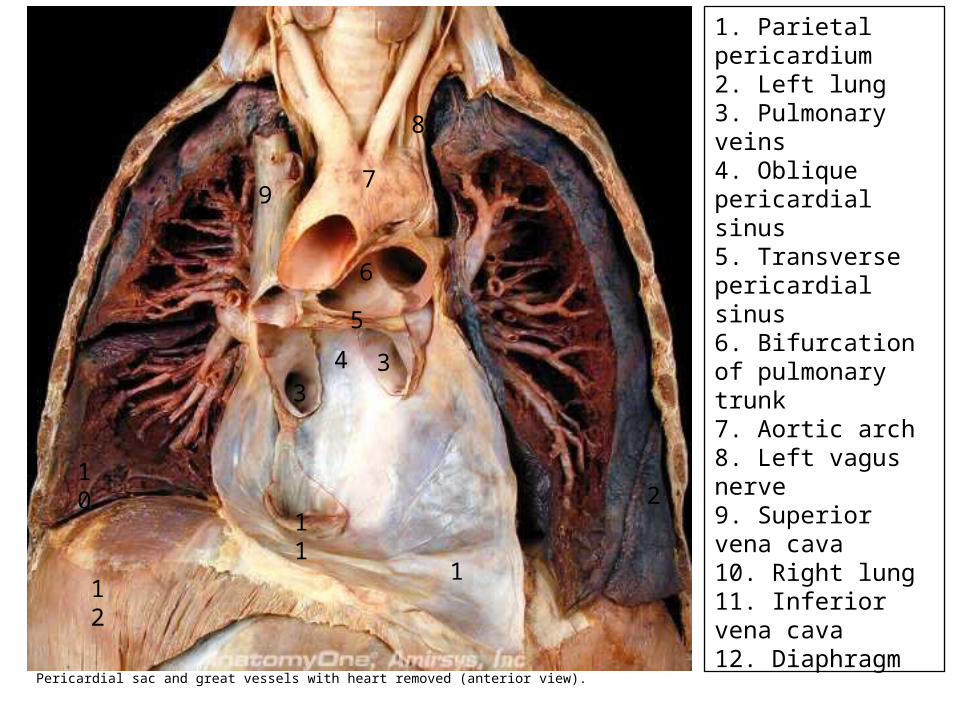
1. Parietal pericardium2. Left lung3. Pulmonary veins4. Oblique pericardial sinus5. Transverse pericardial sinus6. Bifurcation of pulmonary trunk7. Aortic arch8. Left vagus nerve9. Superior vena cava10. Right lung11. Inferior vena cava12. Diaphragm
1
2
33
4
5
6
7
8
9
10
11
12
Pericardial sac and great vessels with heart removed (anterior view).
Thoracic Region
• The thoracic region is that part of the trunk which spans the thoracic vertebral column. The anatomy of the thorax can be clearly explained if you understand 5 types of structural patterns: 1. Trunk body wall patterns, 2. fascial patterns, 3. neurovascular patterns, 4. coelomic patterns (body cavities), 5. and patterns that define the relationship of the limb
and the thoracic body wall.

Thoracic Body Wall
• 4-layered lateral muscle wall. The lateral wall consists of 4 layers. The outer layer is annexed by the limb to support it from the trunk, and the deeper layers form the intercostal muscles.

Thoracic Body Wall
• 4 Layers:• Supracostal or outermost layer. The serratus anterior, rhomboideus major,
rhomboideus minor, and pectoralis minor muscles comprise this layer. These body wall muscles are annexed by the limb to suspend the scapula from the axial skeleton.
• External layer. The external intercostal muscle forms the external muscle layer and is the outer layer of the 3 intercostal layers.
• Middle layer. The internal intercostal muscle forms the middle muscle layer.• Internal layer. This layer is composed of the following named muscles: The
transversus thoracis, innermost intercostal, and subcostal. The diaphragm is also part of this layer as it is peeled away from the internal aspect of the muscle wall during the development of the lungs.
– Subvertebral musculature. The longus colli muscle is the subvertebral muscle of the thorax. It is only present in the upper aspect and then disappears.

1. Vein2. Artery3. Nerve4. Collateral branches of vessels and nerve5. Internal muscle layer6. Middle muscle layer7. External muscle layer8. Internal investing fascia9. Parietal pleura10. Visceral pleura11. Lung12. Rib13. Subcutaneous layer
123
444
5
6
7
8
9
10
11
12
13
Intercostal space (anterolateral view). This illustration shows the topography of neurovascular bundle in body wall. Of note, the neurovascular anatomy of the body wall forms an intercostal VAN (from superior to inferior vein, artery, and nerve) that runs between the middle and internal muscle layers of the lateral thoracic wall.

Relationship between thorax and upper limb
• Limb muscles on thoracic wall. The pectoralis major and latissimus dorsi muscles expand back onto the body wall to cover the true body wall muscles and create an additional muscle plane in the thorax.

1. Ventral muscle (sternalis)2. Subvertebral muscle (longus colli)3. Supracostal layer of lateral wall (serratus posterior superior, rhomboids, serratus anterior, pectoralis minor)4. 3 layers of intercostal muscles (external intercostal, internal intercostal, and innermost intercostal)5. Epaxial muscles6. Limb muscle in brown
1
2
33
3
34
5
6
Muscles of thoracic region (transverse section; superior view). Note that the body wall muscles are deep to the limb muscles (brown) in the upper thorax.

Fascial patterns of thoracic wall
• The pattern is as follows:– Superficial to true body wall musculature. The tissue planes
superficial to the true body wall muscles are (from superficial to deep):• Skin. Epidermis and dermis covering the body.• Subcutaneous layer. Adipose to loose connective tissue layer supporting
the skin and binding it loosely to the limb and external investing fascia.• Limb fascial envelope and limb muscles. As the limb muscles migrate
back onto the body wall, they carry with them a unique fascial plane that invests these muscles and forms an additional fascial envelope superficial to the external investing fascia of the body wall.
• External investing fascia. Dense irregular connective tissue forming the external investment of the true thoracic body wall muscles. This fascia is in contact with the outermost muscles

Fascial patterns of thoracic wall
– Deep to true body wall musculature. (from superficial to deep):• Internal investing fascia. Dense irregular connective
tissue forming the internal investment of the true body wall muscles.• Extraserosal layer. Adipose to loose connective tissue
layer supporting the parietal pleura and binding it loosely to the internal investing fascia.• Parietal pleura. Simple squamous epithelium lining the
thoracic cavity.
Neurovascular patterns of thoracic wall
• Vascular pattern to body wall. The blood supply and drainage of the thoracic wall has the following structural pattern:
• Posterior supply vessel. The aorta runs vertically down the posterior aspect of the thorax.
• Anterior supply vessels. The paired internal thoracic arteries run vertically down the anterior aspect of the the thoracic wall.
• Collateral vessels. Posterior intercostal arteries arise segmentally from the aorta and course anteriorly through the lateral wall. Anterior intercostal arteries arise from the internal thoracic arteries and course posteriorly through the lateral wall. Anterior and posterior intercostal arteries meet and form collateral circuits that link the anterior and posterior blood supply.
• Venous pattern. The veins have the same pattern as the arteries with slight variations. The names of the veins are the same as the arteries (internal thoracic vein, posterior intercostal veins, and anterior intercostal veins) with the exception that the drainage in the posterior wall is via the azygos system of veins.

1. Aorta2. Posterior intercostal arteries3. Internal thoracic artery4. Anterior intercostal arteries1
2
22
2
3
4444
Arterial supply of trunk wall (lateral view). Note the anterior (internal thoracic artery) and posterior (aorta) supply arteries with collateral connections (anterior and posterior intercostal arteries).

Neurovascular patterns of thoracic wall
– Vascular pattern to thoracic viscera. Small branches of the aorta supply the heart, lungs, and esophagus.
– Nervous pattern. The nerves arise as the segmental spinal nerves of the thorax and course with the vessels.• Ventral rami of spinal nerves. Run segmentally with the collateral vessels
as the intercostal nerves and supply the hypaxial muscles of the thorax.• Dorsal rami of spinal nerves. Arise segmentally and course into the epaxial
muscles in the back of the body wall.• Splanchnic nerves. Autonomic fibers course via splanchnic nerves through
the mediastinum to supply the viscera of the thorax.
– Relation of vessels and nerves to muscles. The intercostal nerves and vessels run as a neurovascular bundle in the intercostal spaces of the thoracic wall. They are located between the middle and internal layer of the 4-layered muscle wall.

Body Cavities of the thoracic cavity
• Pleural coeloms. The mesothelial sac that surrounds and protects the lungs.
• Parietal pleura. The part of the mesothelial sac that lines the thoracic cavity.• Visceral pleura. The part of the mesothelial sac that covers the lungs.• Pleural cavity. The small space between the parietal and visceral pleura that
contains a small amount of serous fluid and provides for the frictionless movement of the lungs in the body cavity.
• Pericardial coelom. The mesothelial sac that surrounds and protects the heart.
• Parietal pericardium. The part of the mesothelial sac that lines the fibrous pericardium.
• Visceral pericardium. The part of the mesothelial sac that covers the heart.• Pericardial cavity. The small space between the parietal and visceral
pericardium that contains a small amount of serous fluid and provides for the frictionless movement of the heart within the pericardial sac.

1. Subvertebral muscle2. Ventral muscles3. Lateral outermost muscle4. Lateral external muscle5. Lateral middle muscle6. Lateral internal muscles
12
3
4
5
66
6
Pattern of body wall muscles in thorax and abdomen (anterior view). Each part of the pattern is represented by a distinct color.
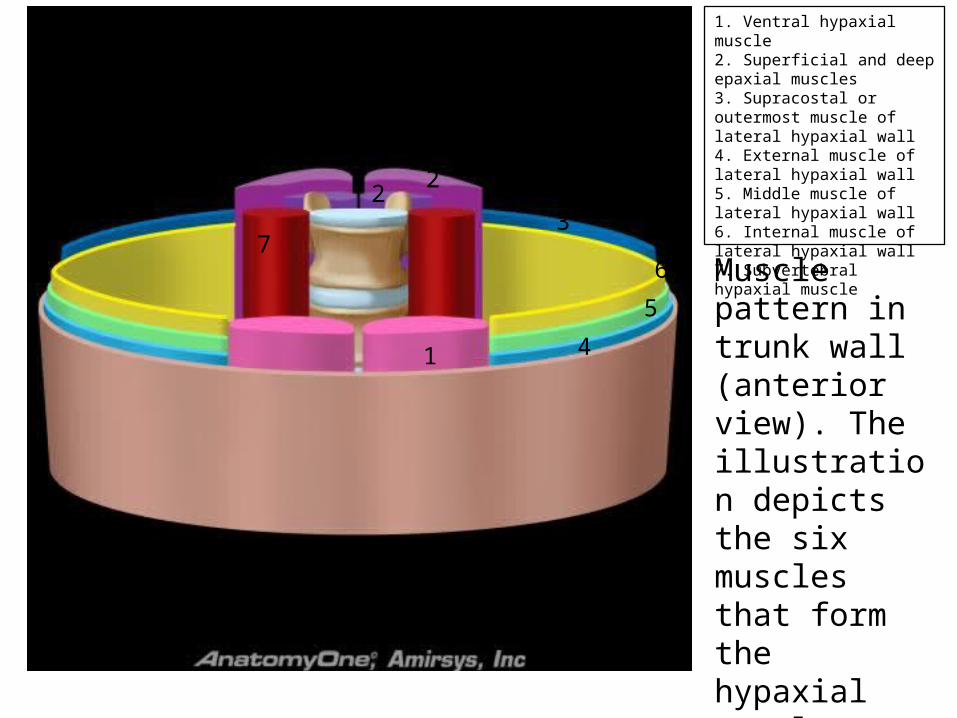
1. Ventral hypaxial muscle2. Superficial and deep epaxial muscles3. Supracostal or outermost muscle of lateral hypaxial wall4. External muscle of lateral hypaxial wall5. Middle muscle of lateral hypaxial wall6. Internal muscle of lateral hypaxial wall7. Subvertebral hypaxial muscle
1
22
3
4
5
67
Muscle pattern in trunk wall (anterior view). The illustration depicts the six muscles that form the hypaxial muscle pattern of the trunk wall, each in a distinct color.
Thoracic Coeloms (Body Cavities)
By Charles Curtis

Body Cavities
• The lungs and heart are enveloped by the pleural sac and pericardial sac, respectively.– Pleural sac. A serous membrane surrounding each
lung and lining the thoracic cavity. The pleural sacs occupy a large portion of the thoracic cavity and are positioned on either side of the heart. Each pleural sac contains an outer parietal layer and an inner visceral layer, which join together at the hilum as the visceral layer reflects from the lung onto the thoracic wall as the parietal layer.

Pleural Sac
• Pleural Sac:• Parietal pleura. The parietal pleura is assigned the
following names based on the structures that it lines:– Costal parietal pleura. Lines the internal surface of the
sternum, ribs, costal cartilages, and intercostal spaces.– Diaphragmatic parietal pleura. Lines the superior surface of
the diaphragm.– Cervical parietal pleura (pleural cupula, dome of pleura).
Dome of pleura that bulges up into the neck, forming a cup-shaped dome over the apex of the lung. This pleura extends superior to rib 1 into the root of the neck.
– Mediastinal parietal pleura. Lines the lateral surface of the mediastinum, where it primarily covers the lateral aspect of the pericardial sac.
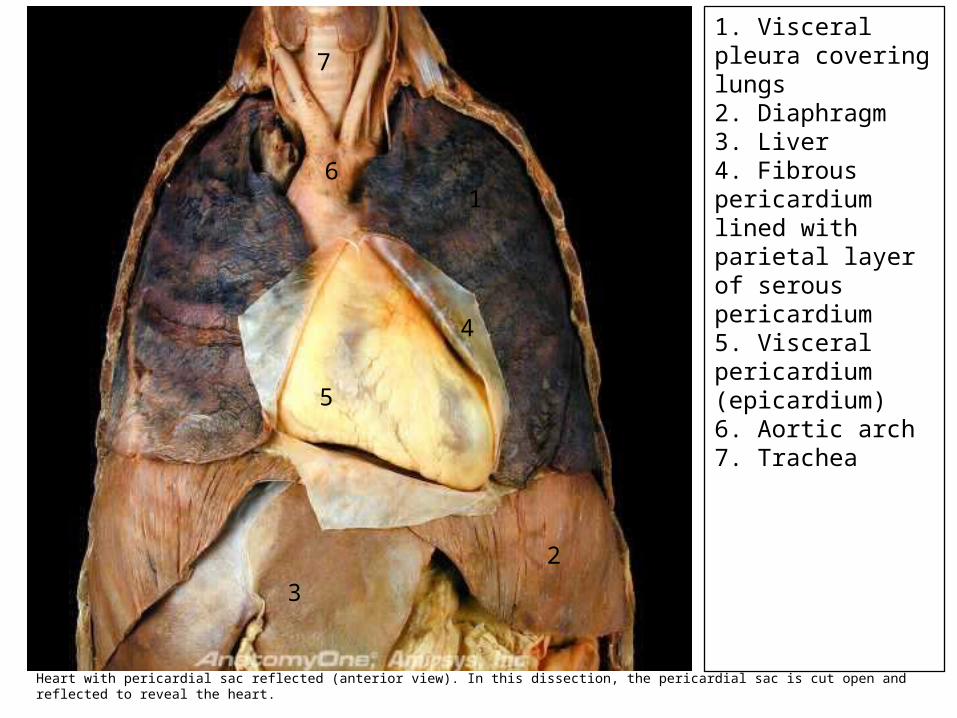
1. Visceral pleura covering lungs2. Diaphragm3. Liver4. Fibrous pericardium lined with parietal layer of serous pericardium5. Visceral pericardium (epicardium)6. Aortic arch7. Trachea
1
2
3
4
5
6
7
Heart with pericardial sac reflected (anterior view). In this dissection, the pericardial sac is cut open and reflected to reveal the heart.

1. Heart2. Left lung3. Superior vena cava4. Proximal aortic arch5. Pulmonary trunk6. Double-layered fibrous and parietal pericardium7. Costodiaphragmatic recess8. Cervical parietal pleura9. Costal parietal pleura10. Diaphragmatic parietal pleura11. Pleural space12. Diaphragm13. Visceral pericardium14. Visceral pleura15. Parietal pericardium, fibrous pericardium, parietal pleura
1
2
3
4
5
6
7
8
9
1011
12
13
1414
14
151515
Mediastinum (coronal section; anterior view). This illustration depicts the coronal anatomy of the mid portion of the mediastinum and shows that it contains the heart (seen in cross section) and portions of the great vessels. The mediastinum is located centrally within the chest between the lungs and pleural surfaces. The inferior boundary of the mediastinum is the diaphragm. The mediastinum extends superiorly to the thoracic inlet.

• Also in the Parietal Pleural:• Pulmonary ligament. • Visceral (pulmonary) pleura. • Pleural space. • Pleural fluid. • Pleural recesses.
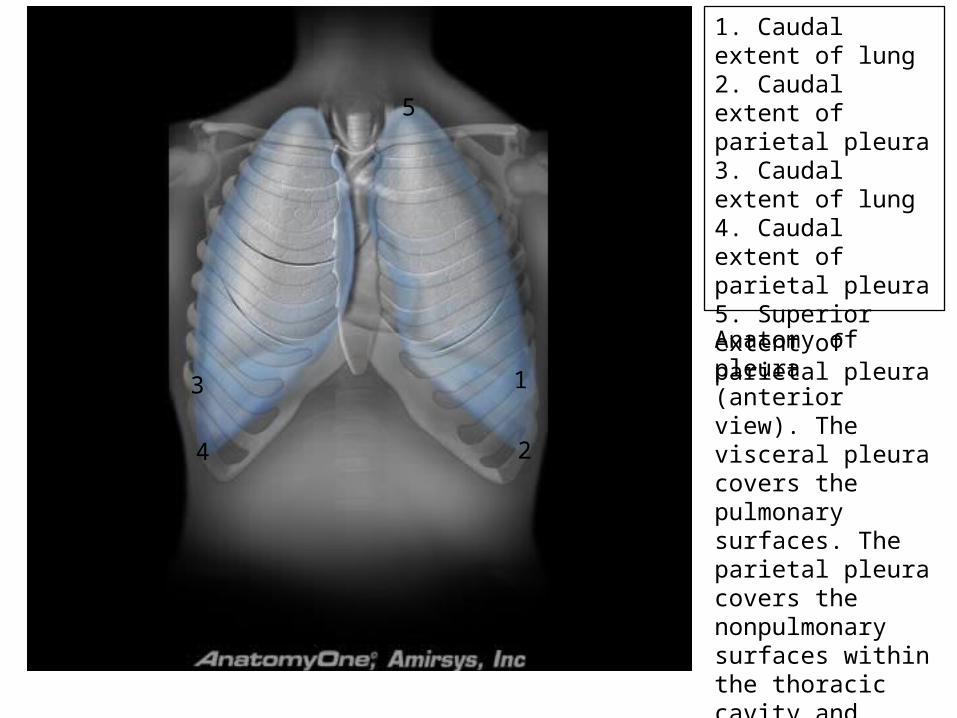
1. Caudal extent of lung2. Caudal extent of parietal pleura3. Caudal extent of lung4. Caudal extent of parietal pleura5. Superior extent of parietal pleura
1
2
3
4
5
Anatomy of pleura (anterior view). The visceral pleura covers the pulmonary surfaces. The parietal pleura covers the nonpulmonary surfaces within the thoracic cavity and extends more caudally than the lungs.

Pleural Recesses
– In the Pleural Recesses:– Costodiaphragmatic recess. Occurs where the costal parietal
pleura and the diaphragmatic parietal pleura come in contact. This recess is located at the inferior limit of the pleural sac.
– Costomediastinal recess. Occurs where the costal parietal pleura and the mediastinal parietal pleura come in contact. This recess is located anteriorly near the midline.

1. Caudal extent of lung2. Caudal extent of lung3. Costodiaphragmatic recess4. Costodiaphragmatic recess5. Costal pleura6. Diaphragmatic parietal pleura7. Mediastinal parietal pleura8. Mediastinal parietal pleura9. Cervical parietal pleura10. Visceral pleura
12
34
5
5
6
78
910
Distribution of pleura (coronal section; anterior view). The visceral pleura covers the surfaces of both lungs and forms interlobar fissures. The parietal pleura lines both thoracic cavities and may be designated by its location as costal, diaphragmatic, or mediastinal pleurae. Inferiorly, the parietal pleura extends deeply into the costodiaphragmatic recesses, where the costal and diaphragmatic pleurae are in apposition.

1. Thoracic vertebral body2. Sternum3. Pulmonary trunk4. Thymus5. Descending aorta6. Superior vena cava7. Subcarinal lymph nodes8. Right main bronchus9. Mediastinal fat10. Root of the lung
1
2
3
4
5
6
78
9
10
Mediastinum at level of pulmonary trunk (transverse section; superior view). The mediastinum is located in the middle of the thorax between the lungs and pleural surfaces. It contains several organs, vascular structures, the esophagus, the central tracheobronchial tree, lymph nodes, nerves, and mediastinal fat.
Pericardial Sac– Pericardial sac (pericardium). Encircling the heart. The
loosely fitting, strong superficial part of this sac is the fibrous pericardium, anchor the heart to the diaphragm. Deep to the fibrous pericardium is the serous pericardium that surrounds the heart and lines the fibrous pericardium.• Fibrous pericardium. • Parietal pericardium. Thin outer layer of the serous pericardial sac• Visceral pericardium (mesothelial layer of epicardium). Forms the
outer layer of the heart• Pericardial cavity. Located between the parietal and visceral layers
of the serous pericardium. • Pericardial sinuses. Located at the junctions of the parietal
pericardium and visceral pericardium.– Oblique pericardial sinus. – Transverse pericardial sinus.

1. Fibrous pericardium2. Serous parietal pericardium3. Serous visceral pericardium4. Pericardial cavity
12
3
4
Pericardium (sagittal view).
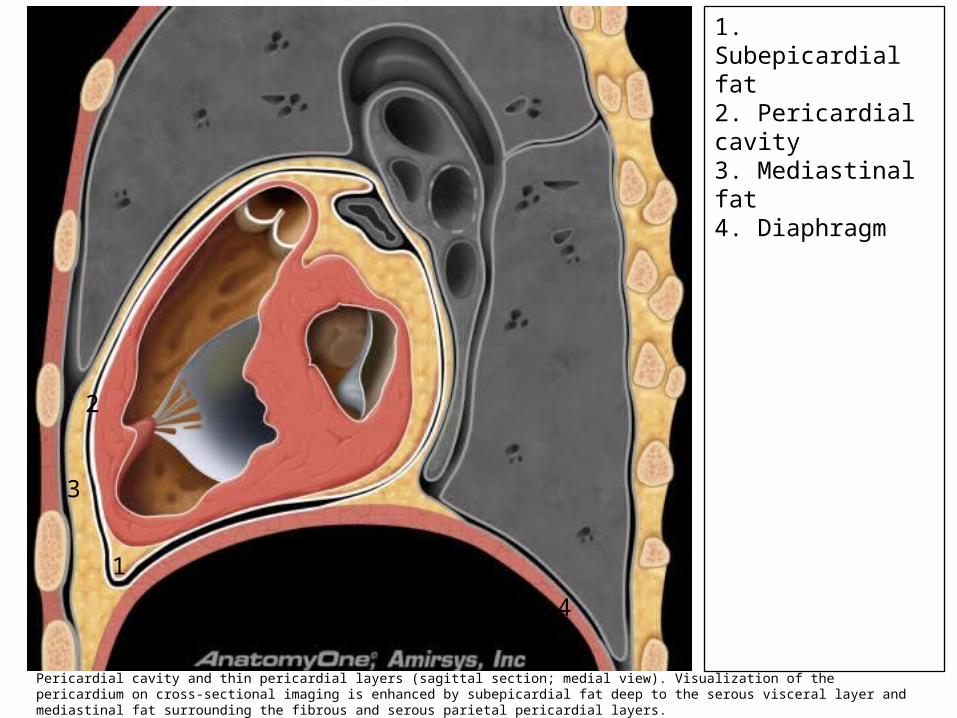
1. Subepicardial fat2. Pericardial cavity3. Mediastinal fat4. Diaphragm
1
2
3
4
Pericardial cavity and thin pericardial layers (sagittal section; medial view). Visualization of the pericardium on cross-sectional imaging is enhanced by subepicardial fat deep to the serous visceral layer and mediastinal fat surrounding the fibrous and serous parietal pericardial layers.

1. Descending aorta2. Peripheral nerve3. Thoracic vertebral body4. Intercostal artery5. Sympathetic trunk and ganglia
1
23
4
5
5
Left thoracic paravertebral region (anterolateral view). The paravertebral region contains vascular structures, fat, lymph nodes, lymphatics, and nerves. The peripheral nerves course through the paravertebral region as they exit the neural foramen. The sympathetic trunk and ganglia are oriented along the length of the paravertebral region.

Arteries• The pleura and pericardium
receive arterial supply from the following arteries and branches:– Parietal pleura. Supplied by the
intercostal arteries, internal thoracic arteries, and musculophrenic arteries.
– Visceral pleura. Supplied by the bronchial arteries.
– Pericardium. Supplied by the pericardiacophrenic arteries, musculophrenic arteries, bronchial arteries, esophageal arteries, and superior phrenic arteries.

1. Aortic hiatus2. Diaphragm3. Right diaphragmatic crus4. Ascending aorta5. Brachiocephalic artery6. Right internal mammary artery7. Left common carotid artery8. Left subclavian artery9. Aortic arch10. Left intercostal arteries11. Right common carotid artery12. Right subclavian artery13. Descending aorta
11
2
3
4
56
7
8
9
10
10
10
1112
13
Thoracic aorta and its branches (anterior view). The aorta has 3 major portions: Ascending aorta, aortic arch, and descending aorta. The ascending aorta courses superiorly and toward the left. The aortic arch curves over the left tracheobronchial angle. The 1st branch of the aortic arch is the brachiocephalic artery followed by the left common carotid and left subclavian arteries. These vessels supply the upper thorax, upper extremities and the head and neck. The brachiocephalic artery gives rise to the right common carotid and right subclavian arteries. The subclavian arteries give rise to the bianterior internal mammary arteries that supply the anterior chest wall and to bilateral vertebral arteries.

1. Aortic arch2. Left internal jugular vein3. Left vagus nerve4. Left recurrent laryngeal nerve5. Left recurrent laryngeal nerve6. Right vagus nerve
1
2
3
4
5
6
Left recurrent laryngeal nerve (lateral view). The left recurrent laryngeal nerve is a branch of the left vagus nerve; it follows an arcuate course under the aortic arch and continues superiorly along the trachea to supply the larynx.

Veins
• Blood from the pleura and pericardium drain through the following veins:– Parietal pleura. Drained by
the intercostal veins.– Visceral pleura. Drained by
the pulmonary veins.– Pericardium. Drained by the
pericardiacophrenic veins and the azygos system of veins (azygos vein, hemiazygos vein, and accessory hemiazygos vein).

1. Superior vena cava2. Azygos arch3. Right subclavian vein4. Left subclavian vein5. Right jugular vein6. Left jugular vein7. Inferior vena cava8. Right intercostal veins9. Left superior intercostal vein10. Accessory hemiazygos vein11. Hemiazygos vein12. Azygos vein13. Right superior intercostal vein
12
3 45 6
7
8
8
8
9
10
11
12
13
Thoracic systemic veins (anterior view). The superior vena cava is formed by the anastomosis of the right and left brachiocephalic veins which in turn are formed by the anastomosis of the jugular and subclavian veins. The chest wall is drained by intercostal veins that course along the undersurface of the ribs and drain into the azygos vein on the right and the hemiazygos and accessory hemiazygos veins on the left. Venous anastomoses connect the azygos and hemiazygos veins. The 1st 3 left intercostal veins drain into the left superior intercostal vein that courses along the lateral aspect of the aortic arch to drain into the posterior aspect of the left brachiocephalic vein. The right superior intercostal vein, shown posterior to the superior vena cava and right brachiocephalic vein, receives the 2nd, 3rd, and 4th right intercostal veins.

Lymph • Lymph from the pleura and
pericardium drain into the right lymphatic duct and thoracic duct.– Visceral pleura. Lymph from the lung
and visceral pleura drains into the subpleural (superficial) lymphatic plexus and ultimately into the bronchopulmonary lymph nodes and tracheobronchial lymph nodes.• Bronchomediastinal lymph trunks. Drain
lymph from the mediastinum and pleura. Lymph from these trunks empties into the right lymphatic duct and the thoracic duct.
– Pericardium. Lymph from the pericardium drains into the transverse mediastinal lymph nodes, prepericardial lymph nodes, tracheobronchial lymph nodes, lateral pericardial lymph nodes, and other regional lymph nodes.• Bronchomediastinal lymph trunks. Drain
lymph from the mediastinum and pleura. Lymph from these trunks empties into the right lymphatic duct and the thoracic duct.

1. Thoracic duct2. Paratracheal nodes3. Tracheobronchial nodes4. Diaphragmatic nodes5. Left gastric nodes
1
2
3
4
5
Tracheobronchial lymph nodes (coronal section; anterior view). Lymphatic drainage from the upper part of the esophagus is usually to the paratracheal and posterior mediastinal nodes, while the distal esophagus drains to the diaphragmatic, celiac, and left gastric nodes; however, there is considerable overlap. The tracheobronchial nodes lie near the carina and may be responsible for the formation of traction diverticula when they become fibrosed, usually as a result of tuberculosis or histoplasmosis.

Neurological• The pleura and pericardium receive innervation from
the autonomic and somatic nervous systems.– Parietal pleura. Innervated by the somatic sensory nerves,
including the intercostal nerves and phrenic nerves. The parietal pleura has many pain fibers and can sense pain.• Costal parietal pleura. Innervated by somatic afferent fibers
from the intercostal nerves.• Mediastinal parietal pleura. Innervated by somatic afferent
fibers from the phrenic nerves.• Diaphragmatic parietal pleura. Innervated by somatic afferent
fibers from the phrenic nerves.• Cervical parietal pleura. Innervated by somatic afferent fibers
from the intercostal nerves.
– .

Neurological– Visceral pleura. Receives autonomic innervation from the
parasympathetic and sympathetic nervous systems. The visceral pleura has no pain fibers.• Parasympathetic innervation. Provided by the vagus nerve (CN X), which
originates in the medulla oblongata.– Pulmonary plexuses. Contain cell bodies of postsynaptic parasympathetic neurons.
• Sympathetic innervation. Provided by the sympathetic fibers of the sympathetic trunks.– Paravertebral sympathetic ganglia. Contain the cell bodies of postsynaptic sympathetic
neurons.
– Fibrous and parietal pericardium. Receives somatic sensory innervation by the phrenic nerve (C3-C5) as the nerve passes through the pericardium on its way to the diaphragm.
– Visceral pericardium. The visceral pericardium receives innervation from CN X and the sympathetic splanchnic nerves from the sympathetic trunks

1. Right phrenic nerve2. Right phrenic nerve3. Right vagus nerve4. Right vagus nerve5. Esophagus6. Intercostal nerve7. Intercostal vein8. Azygos vein9. Superior vena cava10. Sympathetic trunk11. Sympathetic chain12. Diaphragm
1
2
3
4
5
6
7
8 9
10
11
12
Mediastinum (lateral view; right side). Note the intercostal nerves and veins.





























