Embed Size (px)
Citation preview

Left Anterior Descending Artery OcclusionSecondary to Blunt Chest Trauma Diagnosedby Comprehensive Echocardiography andCoronary Angiography
Lin Sun, MD,1 Zhi-an Li, MD,1 Ying Zhao, MD,1 Jiancheng Han, MD,1 Michael Y. Henein, MD2
1 Department of Ultrasound, Beijing Anzhen Hospital, Capital Medical University, Beijing 100029, China2 Heart Centre and Department of Public Health and Clinical Medicine, Umea University, Sweden
Received 5 December 2010; accepted 10 February 2012
ABSTRACT: Blunt chest trauma can cause serious
complications, but coronary artery occlusion is rare.
In a 19-year-old man, 40 days after a motorcycle acci-
dent, comprehensive echocardiography detected left
anterior descending artery occlusion and left ventricu-
lar dysfunction, which was confirmed by coronary
angiography and ventriculography. Echocardiography
was also able to confirm restored left anterior
descending artery flow and improved left ventricular
function after coronary artery bypass grafting. VVC 2012
Wiley Periodicals, Inc. J Clin Ultrasound 40:370–374,2012; Published online in Wiley Online Library
(wileyonlinelibrary.com). DOI: 10.1002/jcu.21907
Keywords: coronary artery; occlusion; blunt chest
trauma; echocardiography
Coronary artery occlusion secondary to bluntchest trauma is rare but can be fatal and is
often overlooked. It affects mainly the left ante-rior descending artery (LAD) and can lead toacute myocardial infarction.1–4 We report such arare case to emphasize the role of comprehensiveechocardiographic examination in diagnosingLAD occlusion and its consequences.
CASE REPORT
A 19-year-old man without cardiovascular riskfactors suffered from severe chest pain after a
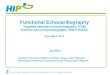
motorcycle accident. However, his vital signswere stable. An early clinical assessment afterthe accident in a local hospital showed normalchest X-ray. Because of the absence of obviousskeletal injury, the patient’s symptoms were over-looked for 40 days. Subsequently, the patient wasadmitted to our hospital because of recurrent ret-rosternal chest pain and tightness. Cardiacenzymes (creatine phosphokinase with its muscleband form) were in the normal range. A 12-leadelectrocardiogram (ECG) showed marked ST seg-ment changes, pathological Q waves in I, augu-mented vector left (aVL), V2–V4 leads, right bun-dle branch block, and left posterior fascicularblock (Figure 1). Two- and three-dimensionalechocardiography showed akinetic myocardialsegments subtended by the LAD, including asmall apical aneurysm and an overall left ventric-ular (LV) ejection fraction of 33%, without peri-cardial effusion. It also revealed an interruptionof LAD course 4 mm from its origin and noobvious coronary artery aneurysm. Color Dopplershowed retrograde, low-velocity, blood flow rightafter the obliterated LAD segment, while no flowsignal could be detected at the middle-distal seg-ments. On the basis of these echocardiographicfindings, the diagnosis of LAD artery occlusionsecondary to blunt chest trauma was made. Coro-nary angiography confirmed total occlusion of theproximal LAD (Figure 2) with collaterals origi-nating from the ostia of LAD, right coronary ar-tery and left circumflex artery, and LAD coronarydissection immediately after the occluded partwith its middle segment involved, as shown by
Correspondence to: Z. Li
' 2012 Wiley Periodicals, Inc.
370 JOURNAL OF CLINICAL ULTRASOUND
Case Report

FIGURE 1. The electrocardiogram demonstrating ST segment changes with pathological Q waves in I, aVL, V2 through V4, right bundle branch
block, and left posterior fascicular block.
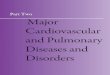
FIGURE 2. Transthoracic two- and three-dimensional echocardiography showing an interruption of left anterior descending coronary artery (LAD)
course at its proximal part (arrow) (A, B). Color Doppler showing obliterated LAD lumen at its proximal part (arrows) followed with retrograde
flow (in blue color) (C). Coronary angiography revealing a total occlusion in the proximal LAD (arrow) (D). AO, aorta.
CORONARY ARTERY OCCLUSION AFTER BLUNT TRAUMA
VOL. 40, NO. 6, JULY/AUGUST 2012 371

pooling and slow clearance of contrast media.Other coronary arteries were fairly normal(Figure 3). Ventriculography revealed a small ap-ical aneurysm. However, our efforts of revascu-larization by percutaneous coronary intervention(PCI) failed. Therefore, the patient underwentoff-pump coronary artery bypass grafting. A leftinternal mammary artery graft to the LAD and asaphenous vein graft to the first diagonal branchfor maximum revascularization were performed.Postoperative transthoracic echocardiogramdemonstrated reestablished LAD flow at its mid-dle-distal segments and no obvious stenosis(Figure 4). In addition, LV ejection fraction roseto 41%.
DISCUSSION
Blunt chest trauma can cause serious complica-tions such as pneumothorax, cardiac contusion,
ventricular rupture, acute aortic tear, and coro-nary artery occlusion with myocardial infarc-tion.1,2 Various traumatic events can cause suchinjuries. Motorcycle accident is the second mostcommon cause of blunt chest trauma.2,3 Themechanism behind coronary occlusion may bemechanical compression, intimal tear, vascularspasm, dissection, thrombus formation, or evenvessel rupture. The most common coronary ar-tery involved is the LAD,1–4 probably because ofits anatomic position, being close to the anteriorchest wall. In our patient, the initial LAD lesionmay have been long-distance traumatic dissec-tion, which may have led to proximal occlusion.
In view of the common presentation of chestpain and the rarity of coronary injury followingnonpenetrating chest trauma, the diagnosis is of-ten missed. Our patient was one of those unfortu-nates who suffered a delayed diagnosis of a proxi-mal LAD occlusion, anterior infarction, and LV
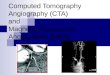
FIGURE 3. Coronary angiographic findings. (A) Collaterals originating from the ostia of the LAD (thick arrows) and left circumflex artery (LCX)
(thin arrows). (B) Coronary dissection right after the occluded part with middle left anterior descending coronary artery (LAD) involved as shown
by contrast medium pooling (thick arrow), and collateral filling from the distal LAD (thin arrow). (C) Normal right coronary artery (RCA). (D) A
collateral from the posterior descending branch of RCA to LAD.
SUN ET AL
372 JOURNAL OF CLINICAL ULTRASOUND

dysfunction. The diagnostic protocol of patientssubjected to blunt chest trauma is not welldefined; however, it conventionally involves car-diac enzymes, ECG monitoring, and echocardiog-raphy.2,4 Cardiac troponin I is a sensitive bio-marker of cardiac injury and may be elevated inmyocardial contusion or traumatic coronaryinjury.5,6 However, the diagnostic period of car-diac troponin I is generally up to 10 days. Ourpatient was admitted to our hospital 40 daysafter the trauma; hence, troponin assessmentwas not indicated. An acute myocardial infarc-tion pattern on ECG, and regional motionabnormalities and ventricular dysfunction onconventional echocardiogram, may suggestmyocardial infarction and lead to further investi-gations such as coronary angiography andintravascular ultrasound. In our patient, a com-prehensive echocardiogram played a unique rolein directing his management plan toward a LADlesion, which was confirmed by angiography. To
our knowledge, this is the first case in whichtransthoracic echocardiography diagnosed coro-nary occlusion secondary to blunt chest trauma.
Moreover, in patients with elevated cardiacbiomarkers levels and ECG abnormalities, car-diac contusion, stress-induced cardiomyopathy,myocarditis, pericardial effusion, and coronarydisease induced by Kawasaki disease may mimictraumatic acute myocardial infarction due to cor-onary artery injury.2,4–8 Comprehensive echocar-diography as performed in our patient, togetherwith coronary angiography, may provide the dif-ferential diagnosis. In addition, before furthertreatment, a MRI or dobutamine stress echocar-diography provides useful data for the clinicianin identifying viable myocardium and decidingwhether the patient should undergo revasculari-zation.9 In the present case, as coronary angiog-raphy demonstrated single-vessel lesion andcollateral LAD filling, chest pain suggestedmyocardial ischemia in the infarction area.
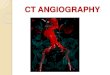
FIGURE 4. Transthoracic color and pulsed Doppler imaging showing changes of left anterior descending coronary artery (LAD) flow at its middle-
distal segments before and after coronary artery bypass surgery. (A) LAD flow not found at the middle-distal segments, even with lowest flow
velocity scale, before operation (arrow). (B) Antegrade and retrograde LAD flow (arrows) near the anastomosis being established along the ante-
rior interventricular groove after operation. (C) Positive frequency spectrum of antegrade LAD flow distal to the anastomosis. (D) Negative Doppler
frequency spectrum of retrograde LAD flow proximal to the anastomosis. LV, left ventricle.
CORONARY ARTERY OCCLUSION AFTER BLUNT TRAUMA
VOL. 40, NO. 6, JULY/AUGUST 2012 373

Therefore, revascularization was decided withoutMRI scan or dobutamine stress echo, whichallowed a shortened hospital stay and limited ex-penditure at the patient’s request.
The management of myocardial infarction fromblunt trauma remains controversial, but usuallyincludes PCI with or without stent implantation,and coronary artery bypass grafting.1,5,6 PCI maybe preferable because it allows rapid revasculari-zation of the culprit vessel and is minimally inva-sive.1,3 Coronary artery bypass grafting has beendemonstrated to have good early and late out-come, but is not appropriate in the setting ofmultiple trauma due to the substantial risk ofbleeding.10–12 Unfortunately, our efforts to per-form PCI failed in our patient. In view of the sin-gle vessel lesion, collaterals to infarction are foundin coronary angiography, and recurrent chestpain, an off-pump coronary artery bypass graftingwith left internal mammary artery to LAD, andsaphenous vein graft to the first diagonal branchwere implemented for complete revascularization.The results were reestablished LAD flow andimproved LV function, which could also beassessed by comprehensive echocardiography.
In conclusion, coronary occlusion secondary toblunt chest trauma involves a significant risk ofmorbidity and mortality and should be includedas a differential diagnosis for posttraumatic chestpain. Early diagnosis and treatment are veryimportant. Noninvasive imaging techniques likecomprehensive echocardiography, or invasivetechniques like angiography, may help establishthe correct diagnosis.
REFERENCES
1. Tsai TN, Yang SP, Tsao TP, et al. Delayed diagnosisof post-traumatic acute myocardial infarction com-
plicated by congestive heart failure. J Emerg Med2005;29:429.
2. Guldner GT, Schilling TD. Coronary arteryocclusion following blunt chest trauma: a casereport and review of the literature. CJEM2005;7:118.
3. Christensen MD, Nielsen PE, Sleight P. Priorblunt chest trauma may be a cause of single vesselcoronary disease; hypothesis and review. Int J Car-diol 2006;108:1.
4. Goel SS, Harvey JE, Penn M, et al. Images in car-diovascular medicine. Left anterior descendingcoronary artery occlusion secondary to blunt chesttrauma. Circulation 2009;119:1975.
5. Jackson L, Stewart A. Best evidence topic report.Use of troponin for the diagnosis of myocardialcontusion after blunt chest trauma. Emerg Med J2005;22:193.
6. Wu AH. Interpretation of high sensitivity cardiactroponin I results: reference to biological variabili-ty in patients who present to the emergency roomwith chest pain: case report series. Clin Chim Acta2009;401:170.
7. Ryu JK, Kim KS, Lee JB, et al. Coronary arterystenting in a patient with angina pectoris causedby coronary artery dissection after blunt chesttrauma [letter]. Int J Cardiol 2007;114:e89.
8. Jesuraj ML, Mukerjee D, Jesuraj AV, et al. Coro-nary artery ectasia in a patient with myocardialinfarction. Cardiovasc J Afr 2011;22:36.
9. Elhendy A, Bax JJ, Poldermans D. Dobutaminestress myocardial perfusion imaging in coronaryartery disease. J Nucl Med 2002;43:1634.
10. Di Donato M, Frigiola A, Benhamouda M, et al.Safety and efficacy of surgical ventricular restora-tion in unstable patients with recent anterior myo-cardial infarction. Circulation 2004;110:II169.
11. Nan YY, Chang JP, Lu MS, et al. Mediastinalhematoma and left main dissection followingblunt chest trauma. Eur J Cardiothorac Surg2007;31:320.
12. Korach A, Hunter CT, Lazar HL, et al. OPCAB foracute LAD dissection due to blunt chest trauma.Ann Thorac Surg 2006;82:312.
SUN ET AL
374 JOURNAL OF CLINICAL ULTRASOUND