Embed Size (px)
Citation preview
ASHRAE1791 Tullie Circle, NE • Atlanta, Georgia 30329-2305404-636-8400 • fax: 404-321-5478 • www.ashrae.org
ASHRAE Position Document onLegionellosis
Approved by ASHRAE Board of DirectorsJune 25, 1998
Reaffirmed by ASHRAE Technology CouncilJanuary 25, 2012
ExpiresJanuary 25, 2015
The ASHRAE Position Paper on Legionellosis was developed by the Society's Legionellosis Position Paper Committee (listed below) under the direction of the Environmental Health Committee.
Linden E . Witherell, Esq., PE ., M.PH . Environmental Health Services Burlington, VT
Richard A. Charles, PE . G&B Consulting Engineers San Francisco, CA
Legionellosis Position Paper and Statement Committee
1998 Revision
Amanda K. Meitz, Chair Nalco Diversified Technologies, Inc. Chagrin Falls, OH
James M. Barbaree, Ph .D . Auburn University Auburn, AL
Robert F Breiman, M.D . Centers for Disease Control and Prevention Atlanta, GA
J . Donald Millar, M.D. Don Millar & Associates Atlanta, GA
Brian G. Shelton, M.PH . PathCon Laboratories Norcross, GA
Laurance S. Staples L.S . Staples Company Prairie Village, KS
© 1998 ASHRAE (www.ashrae.org). For personal use only. Additional reproduction, distribution, or transmission in either print or digital form is not permitted without ASHRAE’s prior written permission.
HISTORY OF REVISION/REAFFIRMATION/WITHDRAWAL DATES
The following summarizes this document’s revision, reaffirmation, or withdrawal dates:
6/25/1998—BOD approves revision to Position Document titled Legionellosis
1/25/2012—Technology Council approves reaffirmation of Position Document titledLegionellosis
Note: ASHRAE’s Technology Council and the cognizant committee recommend revision,reaffirmation, or withdrawal every 30 months.
Note: ASHRAE position documents are approved by the Board of Directors and express the views of the Societyon a specific issue. The purpose of these documents is to provide objective, authoritative background informationto persons interested in issues within ASHRAE’s expertise, particularly in areas where such information will behelpful in drafting sound public policy. A related purpose is also to serve as an educational tool clarifyingASHRAE’s position for its members and professionals, in general, advancing the arts and sciences of HVAC&R.
© 1998 ASHRAE (www.ashrae.org). For personal use only. Additional reproduction, distribution, or transmission in either print or digital form is not permitted without ASHRAE’s prior written permission.

Table of Contents
Legionellosis
Position Statement . and Position Paper
Legionellosis Position Statement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
1 .0 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
2.0 Background . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
3.0 The Disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
3.1 Causative Agent . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
3.2 Disease Description . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
3.2.1Legionellosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
3.2 .2 Pontiac Fever . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
4.0 Transmission Factors and Prevention . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
4 .1 Reservoirs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
4.2 Amplifiers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
4.3 Aerosolization . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
4.4 Transmission . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
4.5 Susceptible Hosts . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
4.5 .1 Susceptibility Factors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
5.0 Preventative Strategies and Monitoring . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
6.0 Safety Precautions for Decontamination Procedures . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
7.0 Emergency Decontamination for Legionella . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
7.1 Cooling Systems . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
7.2 Potable Systems . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
8.0 Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
9.0 Citations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
© 1998 ASHRAE (www.ashrae.org). For personal use only. Additional reproduction, distribution, or transmission in either print or digital form is not permitted without ASHRAE’s prior written permission.
4
Legionellosis Position Statement
In accordance with the American Society of Heating, Refrigerating and Air-Conditioning Engineers' (ASHRAE) sole objective to advance the arts and sciences of heating, refrigeration, air conditioning and ventilation, and their allied arts and sciences and related human factors, for the benefit of the public, the Society provides and updates a series of Position Statements and Position Papers on topics that are of concern to ASHRAE members and the general public .
Based on the scientific, medical, and engineering literature available to date, ASHRAE concludes the following:
l . Legionellae occur naturally in lakes and streams. They may be transported through potable water distribution lines and then may be aerosolized into the atmosphere. Outbreaks of individual cases of legionellosis have been traced to cooling towers and evaporative condensers, potable water services, and components, such as water heaters, showers, faucets, whirlpool baths respiratory therapy equipment, and decorative fountains .
2 . The mere presence of Legionella in water or on a fixture or device is not sufficient to cause disease . For disease to develop, individuals must inhale sufficient numbers of virulent organisms to overwhelm their natural resistance . Variations in virulence of organisms and susceptibility of people exist.
3 . Design and good operations, maintenance, and housekeeping procedures that prevent amplification and dissemination of Legionella should be formulated and implemented before systems are operated . These procedures should be continued rigidly thereafter. Although using these practices will not guarantee that a system or individual component will be free of legionellae, they should reduce the chance of heavy colonization with these bacteria .
4 . Currently, the most reliable method of testing for the presence of viable legionellae in a system is by culturing for these organisms . No "non-legionellae" surrogate tests are available, and there is currently no correlation between total bacterial counts and legionellae concentrations . The results of single tests must be interpreted cautiously as the concentration of Legionella in a water system can increase substantially over a few days . Attention should be paid to sample handling and laboratory quality control so that the number reported reflects the number present at the time of sampling,
5. The efficacy of a specific biocide treatment in controlling legionellae can only be determined by testing specifically for the presence of legionellae in the field under actual working conditions. Laboratory trials must not be relied on exclusively as the sole proof of the efficacy of a biocide . Biocides can be health and safety hazards and must be handled in accordance with specifications on labels and material safety data sheets.
ASHRAE will continue to collect and analyze new information on the control of Legionella and disseminate this information to its members and to the general public . The Society also will maintain liaison between other professional organizations and government agencies such as the Centers for Disease Control and Prevention and the U.S . Environmental Protection Agency. ASHRAE will continue to encourage and support specific research in the control of Legionella .
© 1998 ASHRAE (www.ashrae.org). For personal use only. Additional reproduction, distribution, or transmission in either print or digital form is not permitted without ASHRAE’s prior written permission.
succumbing to the disease may be higher among particularly vulnerable people .
Legionellosis is an illness that has two distinct clinical forms . The most serious form is a pneumonia illness that is commonly referred to as Legionnaires' disease. Generally, in epidemic settings, the proportion of people who contract the disease is 5% or less ;' however, risk factors such as age, smoking, underlying disease, and compromised immunity play a major role in susceptibility. The incubation period is 2 to 10 days, and treatment with erythromycin with or without rifampin is usually effective. Fatality rates in outbreaks have averaged about 15% . Early diagnosis and treatment (possibly including hospitalization) will reduce the chance of fatality, although the chance of
Legionnaires' disease quickly gained public attention with the outbreak that occurred in the summer of 1976
1 .0 Introduction Control of indoor environments for the-well-being of occupants is one of the ASHRAE's founding principles :
"The Society is organized and operated for the exclusive purpose of advancing the arts and sciences of heating, refrigeration, air conditioning, and ventilation, and the allied arts and sciences and related human factors for the benefit of the general public, as defined in the Certificate of Consolidation. To fulfill its role, the Society shall recognize the effect of its technology on the environment and natural resources to protect the welfare of posterity." (ASHRAE Bylaws, Article I, Section 1 .3)
Consistent with this responsibility, the following is the Society's position on legionellosis.
2.0 Background A presidential ad hoc committee was appointed in Sep-tember 1980 to evaluate Legionnaires' disease. Members of ASHRAE as well as consultants from industry, private practice, government, and academic institutions, having scientific, medical, or engineering expertise on Iegionellosis, were appointed to the committee.
The work of this ad hoc committee resulted in : (1) a Position Statement that delineated the nature of the problem and discussed possible approaches for its solutions, and (2) a two-part Position Paper that presented basic information known at that time about the disease and its causative agents ; a discussion of environmental, energy, and economic implications of the disease; and recommendations for future action . This paper is the second update and condensation of these previous documents .
3.0 The Disease
Leqionellosis Position Paper
The other clinical illness,' Pontiac fever, is a flu-like illness without pneumonia. In contrast to Legionnaires' disease, most of those who are exposed develop illness within 48 to 72 hours and most recover without antibiotic therapy.2.3
3 .1 Causative Agent
Legionellosis is caused byLegionella, a type of bacteria discovered in 1977 . These microbes measure about 0.3 pm by 2 Nm. When microorganisms grow their numbers increase . Individual cells repeatedly divide with new cells dividing again and again. The result can be millions of cells after a few hours or days . Legionella do not grow on ordinary laboratory media, but grow best when supplemented with L-cysteine, soluble iron and near a pH of 6.9 .4 In spite of the strict nutritional requirements in the laboratory, these organisms are found in a wide variety of fresh waters ,s~ 6 and are found commonly in lakes and streams. Several investigators have reported nutritional relationships between legionellae and other bacteria,? algae," and protozoa .9~'o
For epidemiologic purposes, further characterization of organisms, such as Legionella pneumophila serogroup 1, can be done using monoclonal antibodies," multilocus enzyme assay (MEA),'2 ribotyping,'3 restriction fragment length polymorphism (RFLP),'4 random amplified polymorphic DNA (RAPD),'S and pulsed-field-gel electrophoresis (PFGE)'6 procedures . These techniques are commonly called "finger printing", and can be used to correlate the specific Legionella strain from an infected patient with an environmental source."
Legionella pneumophila can grow in tap water at 25°C to 42°C (77°F to 108°F) with an optimal temperature for growth of 37°C (98.6°F) .'e Growth can also occur outside this range, but the environment becomes more hostile the further from the optimal.
Currently, there are more than 35 species with numerous serogroups within some species . To date, roughly one-half have been associated with disease .
3 .2 Disease Description
3 .2 .1 Leqionellosis
© 1998 ASHRAE (www.ashrae.org). For personal use only. Additional reproduction, distribution, or transmission in either print or digital form is not permitted without ASHRAE’s prior written permission.
Sincelhe Philadelphia outbreak, additional outbreaks and numerous sporadic cases of legionellosis have been reported . About 1,400 cases are officially reported annually to the CDC, and about 500 are confirmed. A study of people hospitalized with pneumonia calculated that 11,000 cases of legionellosis occur annually in the United States . This calculation is thought to be an underestimate . Estimates as high as 100,000 cases annually in the U.S . have been sug-gested, although the scientific basis for these esti-mates is not clear. Serologic surveys indicate that many people in the general population have antibodies to legionellae in their blood. This suggests that large numbers of people may have been exposed and pos-sibly infected with legionellae.23.2' While most of the earlier outbreaks were traced to aerosols contaminated with these organisms from either cooling towers or evaporative condensers '21, zs, 27, za, as other outbreaks have been traced to potable water services and components, such as water heaters, showers, faucets, whirlpool baths,3o, 3'' 32. 33' 34 respiratory therapy equipment '31 decorative fountains '36,31 and an ultrasonic mister sometimes used in grocery stores .38
Water is the reservoir for legionellae in the envir-onment . Many lakes and streams have been found to harbor legionellae.'S~'6 Theoretically, the ultimate method for preventing human infections of legionellosis would be to completely eliminate or eradicate legionellae from the environment; however, this is impossible because of the ubiquitousness of legionellae in water in the outdoor environment . Factors that influence survival in natural reservoirs include temperature, pH, available nutrients, and existing microbiota . Control in natural reservoirs is probably outside the scope of epidemiology and medicine and certainly outside the scope of building management practices.
6
among conventioneers attending the meeting of the Pennsylvania Division of the American Legion in Philadelphia.'9 Because of the size and seventy of the outbreak, federal, state, and local health authorities launched the largest cooperative investigation in history (before 1980) to determine the cause of the outbreak .
People who developed illness did so between 2 and 10 days after they had attended meetings in the convention center's hotel. High fever, chills, headaches, and muscle aches and pains were the initial symptoms . Some people had dry coughs, chest pains, shortness of breath, mental confusion, vomiting, and diarrhea . All eventually developed pneumonia . Ultimately, 34 of the 221 people who became ill died . No person-to-person spread was documented in this outbreak or any others . Careful epidemiologic investigation eliminated a multitude of possible sources . Air was implicated as the probable pathway of infection. It was shown statistically that patients had spent a significantly longer period of time in the lobby of the convention center's hotel than those who remained healthy.
Examination of sera and tissue specimens from some previously unsolved outbreaks that had been stored at the Centers for Disease Control and Prevention (CDC) in Atlanta, Georgia, and elsewhere revealed that outbreaks of this disease had occurred earlier. The earliest case so far documented occurred in a soldier who had an unidentified pneumonia in 1947 when he was at Fort Bragg, North Carolina .20 The earliest outbreak (three or more cases from -the same source) of legionellosis appears to have occurred in a meat packing plant in 1957.2'
3.2 .2 Pontiac Fever
The first documented outbreak of Pontiac fever occurred in 1968 in Pontiac, Michigan ." Ninety-five percent of .the employees at the Oakland County Health Department developed illness, which generally lasted 2 to 3 days and consisted of fever, headache, and generalized muscle aching . All of the 144 people who became ill recovered. Ultimately, Legionella pneumophila serogroup 1 bacteria were isolated from condensate water collected from the drip pan of an evaporative condenser located in the building's basement .41 In subsequent outbreaks of Pontiac fever Legionella pneumophila," L. anisa,'2 L. feeleii,3 and L. mcdadeii43 were implicated as the causative agents .
4.0 Transmission Factors and Prevention
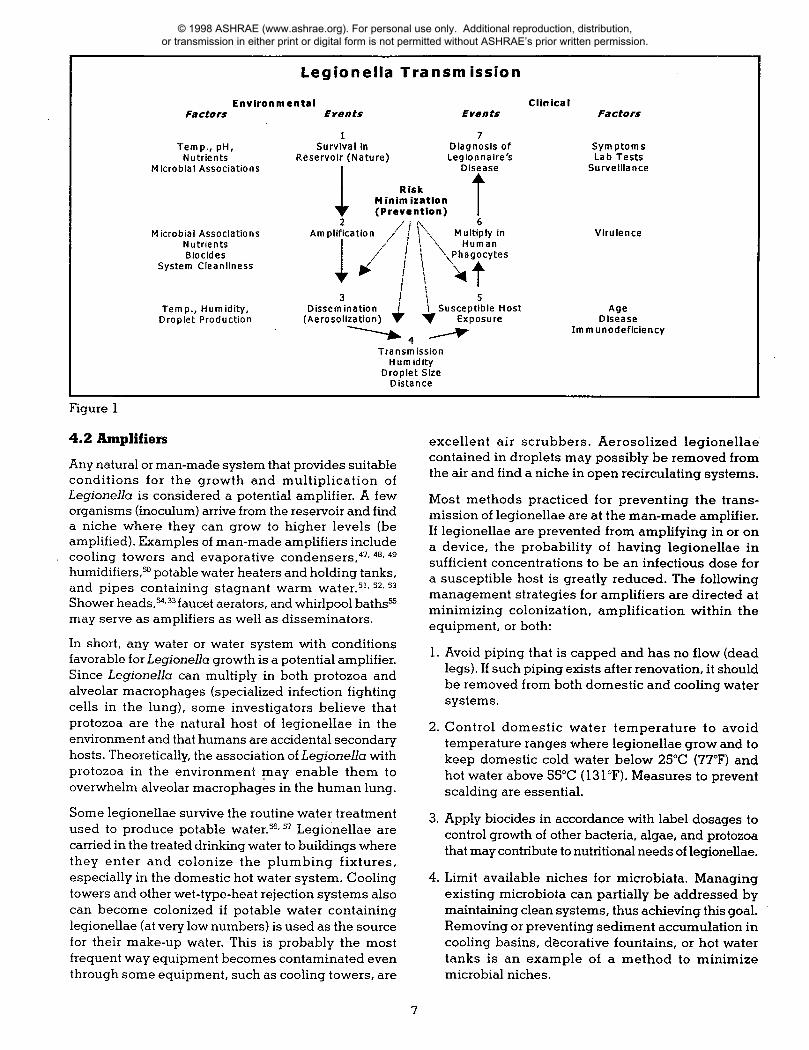
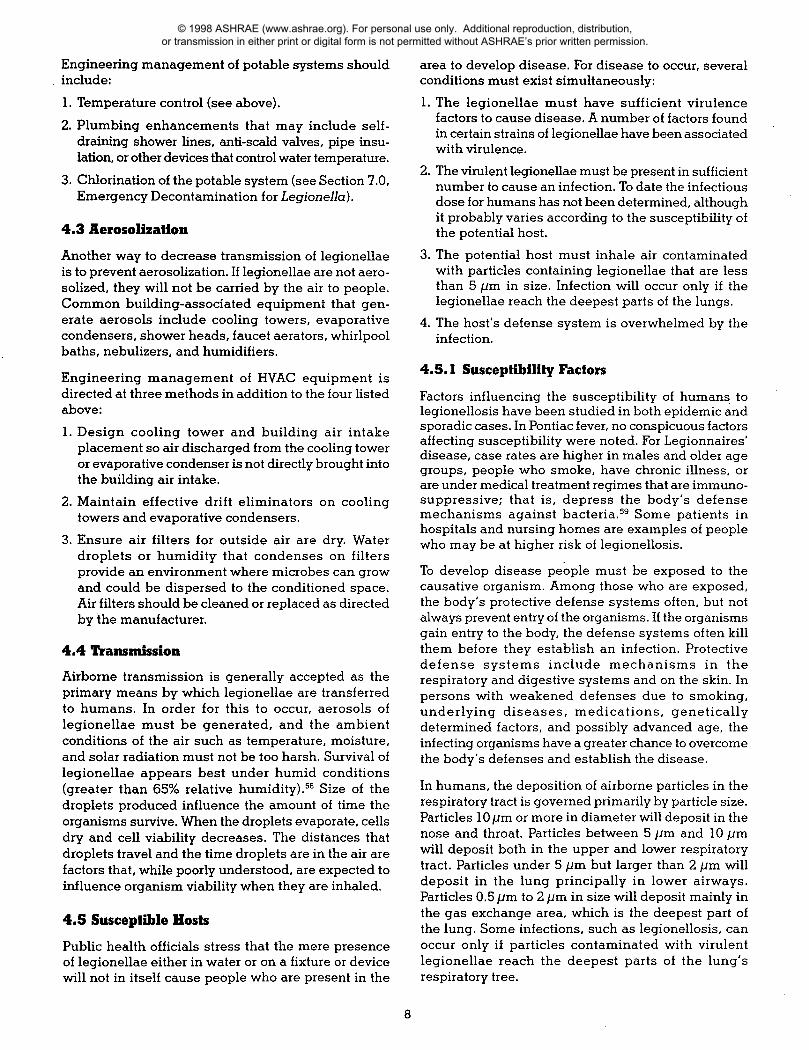
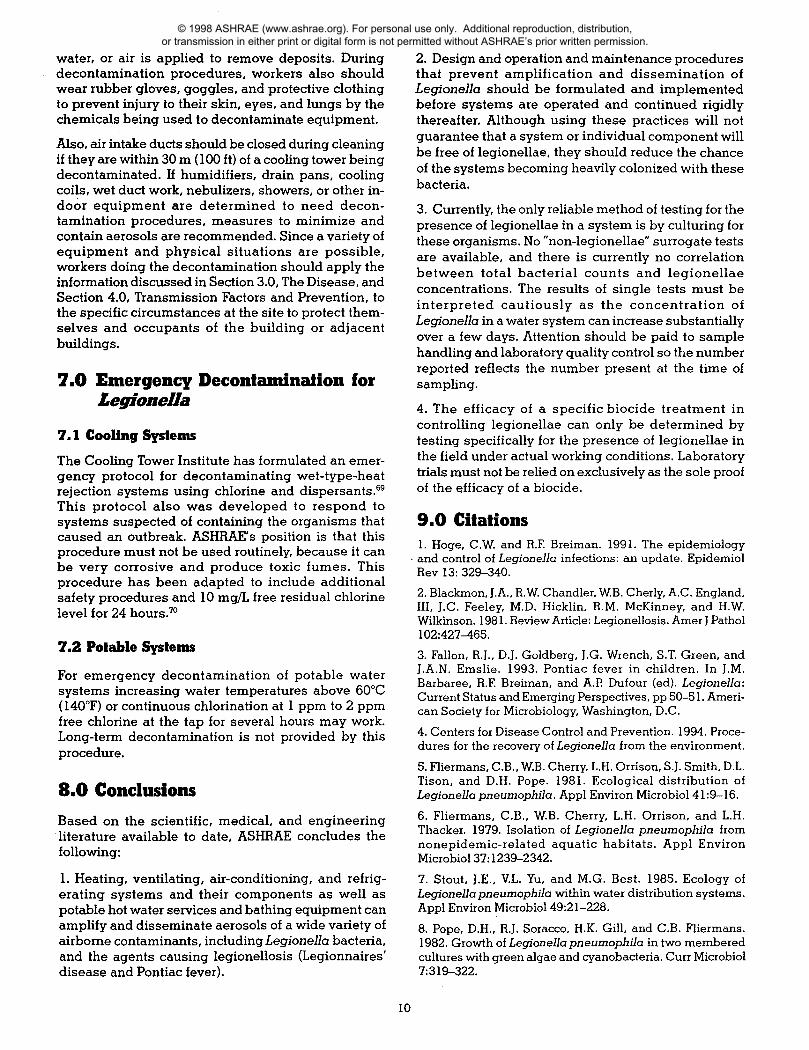
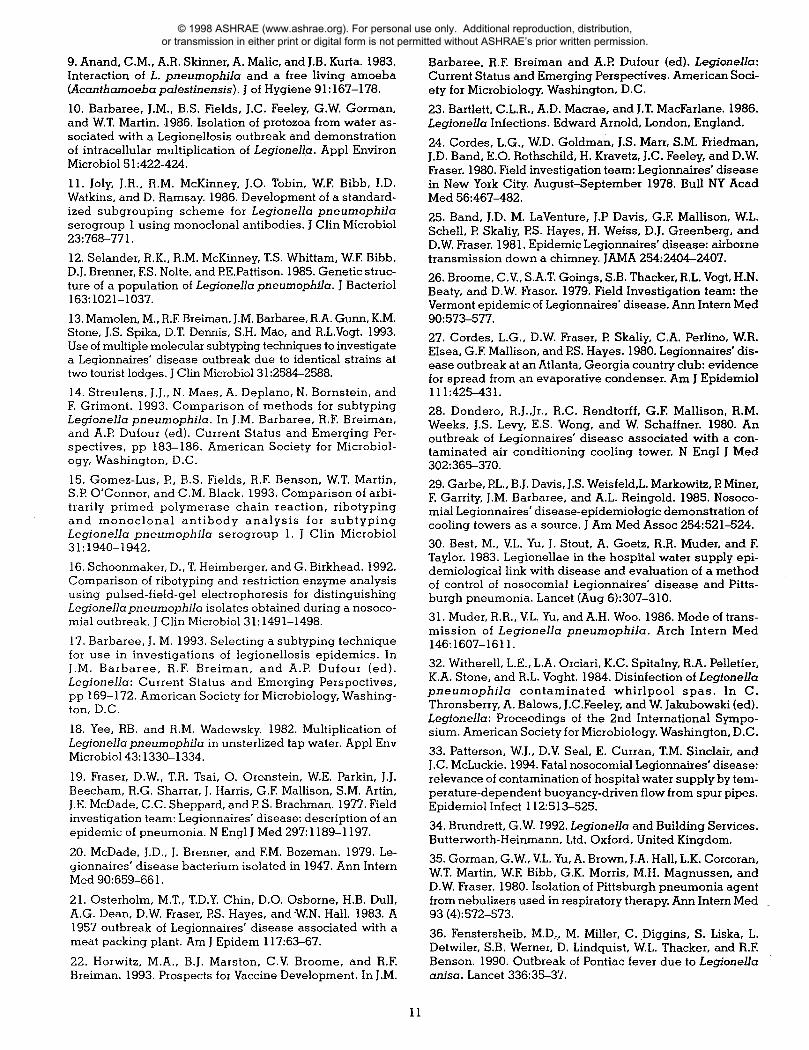
Prior to developing actual disease, a number of events must occur. Some of these events can be influenced by good engineering and maintenance practices. These events and prevention opportunities are out-lined in Figure 1 .'4 The first event is generally outside the scope of building engineering and management practices . Events 2 to 4 can be influenced by engineering design and maintenance procedures . Later events are influenced by individuals' health care practices.
The most effective control for most diseases including legionellosis is preventing transmission at as many points as possible in the diseases' chain of transmission . The rationale for this is that if one preventative measure fails, others will be present and act as fail-safe mechanisms . With this philosophy in mind, each step for possible transmission of Legionella are presented and possible intervention strategies discussed . General concepts are presented so that readers may develop an understanding of the types of conditions that may allow amplification and transmission of Legionella .
4.1 Reservoirs
© 1998 ASHRAE (www.ashrae.org). For personal use only. Additional reproduction, distribution, or transmission in either print or digital form is not permitted without ASHRAE’s prior written permission.
Environmental Factors Events Events
1 7 Temp., pH, Survival in Diagnosis of Nutrients Reservoir (Nature) Legionnaire's
Microbial Associations Disease
Risk Minimization (Prevention) T
.' Microbial Associations Amplification Multiply in
Nutrients Human Blocides ~'".\Phagocytes
System Cleanliness
3 Temp., Humidity, Dissemination I Susceptible Host Droplet Production (Aerosolization) VF '~ Exposure
0
Transmission Humidity
Droplet Size Distance
Age Disease
Immunodeficiency
Some legionellae survive the routine water treatment used to produce potable water .56, -97 Legionellae are carried in the treated drinking water to buildings where they enter and colonize the plumbing fixtures, especially in the domestic hot water system . Cooling towers and other wet-type-heat rejection systems also can become colonized if potable water containing legionellae (at very low numbers) is used as the source for their make-up water. This is probably the most frequent way equipment becomes contaminated even through some equipment, such as cooling towers, are
4. Limit available niches for microbiata . Managing existing microbiota can partially be addressed by maintaining clean systems, thus achieving this goal . Removing or preventing sediment accumulation in cooling basins, decorative fountains, or hot water tanks is an example of a method to minimize microbial niches.
Legionella Transmission
Clinical Factors
Symptoms Lab Tests
Surveillance
Virulence
Figure 1
4.2 Amplifiers
Any natural or man-made system that provides suitable conditions for the growth and multiplication of Legionella is considered a potential amplifier. A few organisms (inoculum) arrive from the reservoir and find a niche where they can grow to higher levels (be amplified) . Examples of man-made amplifiers include cooling towers and evaporative condensers '47, 411 . 49
humidifiers,s° potable water heaters and holding tanks, and pipes containing stagnant warm water .51, -92, 53
Shower heads,14~33faucet aerators, and whirlpool baths may serve as amplifiers as well as disseminators.
In short, any water or water system with conditions favorable for Legionella growth is a potential amplifier. Since Legionella can multiply in both protozoa and alveolar macrophages (specialized infection fighting cells in the lung), some investigators believe that protozoa are the natural host of legionellae in the environment and that humans are accidental secondary hosts. Theoretically, the association of Legionella with protozoa in the environment may enable them to overwhelm alveolar macrophages in the human lung .
excellent air scrubbers. Aerosolized legionellae contained in droplets may possibly be removed from the air and find a niche in open recirculating systems .
Most methods practiced for preventing the trans-mission of legionellae are at the man-made amplifier. If legionellae are prevented from amplifying in or on a device, the probability of having legionellae in sufficient concentrations to be an infectious dose for a susceptible host is greatly reduced. The following management strategies for amplifiers are directed at minimizing colonization, amplification within the equipment, or both :
Avoid piping that is capped and has no flow (dead legs). If such piping exists after renovation, it should be removed from both domestic and cooling water systems.
2. Control domestic water temperature to avoid temperature ranges where legionellae grow and to keep domestic cold water below 25°C (77°F) and hot water above 55°C (131°F) . Measures to prevent scalding are essential.
3. Apply biocides in accordance with label dosages to control growth of other bacteria, algae, and protozoa that may contribute to nutritional needs of legionellae.
© 1998 ASHRAE (www.ashrae.org). For personal use only. Additional reproduction, distribution, or transmission in either print or digital form is not permitted without ASHRAE’s prior written permission.
In humans, the deposition of airborne particles in the respiratory tract is governed primarily by particle size . Particles 10pm or more in diameter will deposit in the nose and throat . Particles between 5 pm and 10 Nm will deposit both in the upper and lower respiratory tract. Particles under 5 jim but larger than 2 Nm will deposit in the lung principally in lower airways. Particles 0.5 Nm to 2 pm in size will deposit mainly in the gas exchange area, which is the deepest part of the lung . Some infections, such as legionellosis, can occur only if particles contaminated with virulent legionellae reach the deepest parts of the lung's respiratory tree .
Public health officials stress that the mere presence of legionellae either in water or on a fixture or device will not in itself cause people who are present in the
Engineering management of potable systems should include:
1 . Temperature control (see above) .
2. Plumbing enhancements that may include self-draining shower lines, anti-scald valves, pipe insu-lation, or other devices that control water temperature.
3. Chlorination of the potable system (see Section 7.0, Emergency Decontamination for Legionella).
4.3 Aerosolization
Another way to decrease transmission of legionellae is to prevent aerosolization . If legionellae are not aero-solized, they will not be carried by the air to people . Common building-associated equipment that gen-erate aerosols include cooling towers, evaporative condensers, shower heads, faucet aerators, whirlpool baths, nebulizers, and humidifiers .
Engineering management of HVAC equipment is directed at three methods in addition to the four listed above:
1 . Design cooling tower and building air intake placement so air discharged from the cooling tower or evaporative condenser is not directly brought into the building air intake .
2. Maintain effective drift eliminators on cooling towers and evaporative condensers .
3. Ensure air filters for outside air are dry. Water droplets or humidity that condenses on filters provide an environment where microbes can grow and could be dispersed to the conditioned space . Air filters should be cleaned or replaced as directed by the manufacturer.
4.4 Transmission
Airborne transmission is generally accepted as the primary means by which legionellae are transferred to humans. In order for this to occur, aerosols of legionellae must be generated, and the ambient conditions of the air such as temperature, moisture, and solar radiation must not be too harsh. Survival of legionellae appears best under humid conditions (greater than 65% relative humidity) ." Size of the droplets produced influence the amount of time the organisms survive. When the droplets evaporate, cells dry and cell viability decreases. The distances that droplets travel and the time droplets are in the air are factors that, while poorly understood, are expected to influence organism viability when they are inhaled.
4.5 Susceptible Hosts
area to develop disease. For disease to occur, several conditions must exist simultaneously :
1 . The legionellae must have sufficient virulence factors to cause disease. A number of factors found in certain strains of legionellae have been associated with virulence.
2. The virulent legionellae must be present in sufficient number to cause an infection. To date the infectious dose for humans has not been determined, although it probably varies according to the susceptibility of the potential host .
3 . The potential host must inhale air contaminated with particles containing legionellae that are less than 5 pm in size . Infection will occur only if the legionellae reach the deepest parts of the lungs.
4. The host's defense system is overwhelmed by the infection.
4.5.1 Susceptibility Factors
Factors influencing the susceptibility of humans to legionellosis have been studied in both epidemic and sporadic cases . In Pontiac fever, no conspicuous factors affecting susceptibility were noted. For Legionnaires' disease, case rates are higher in males and older age groups, people who smoke, have chronic illness, or are under medical treatment regimes that are immuno-suppressive; that is, depress the body's defense mechanisms against bacteria." Some patients in hospitals and nursing homes are examples of people who may be at higher risk of legionellosis .
To develop disease people must be exposed to the causative organism . Among those who are exposed, the body's protective defense systems often, but not always prevent entry of the organisms. If the organisms gain entry to the body, the defense systems often kill them before they establish an infection. Protective defense systems include mechanisms in the respiratory and digestive systems and on the skin . In persons with weakened defenses due to smoking, underlying diseases, medications, genetically determined factors, and possibly advanced age, the infecting organisms have a greater chance to overcome the body's defenses and establish the disease.
© 1998 ASHRAE (www.ashrae.org). For personal use only. Additional reproduction, distribution, or transmission in either print or digital form is not permitted without ASHRAE’s prior written permission.

Workers conducting cleaning operations that are expected to produce aerosols are advised to wear a half-face respirator mask equipped with a cartridge filter that has a HEPA filter or "Type H" high efficiency rating . Filters capable of filtering aerosols, mists, particulates, radionucleotides, and asbestos should also be capable of removing Legionella and provide protection . Wearing the respirator mask is particularly advisable during cleaning if high-pressure steam,
There is not enough information available to adopt a position on what is a "safe" or "unsafe" number of legionellae or how long that number would be valid for an individual dynamic system, Some cases of legionellosis indicate that a low number of legionellae was sufficient to cause illness . In other analyses, higher numbers of legionellae have not been correlated with disease. Directing research efforts at
9
The upper part of the respiratory tract has a ciliated mucosal lining . Mucus is excreted around the particles that are deposited . Movement of the cilia of the respiratory tract expel the particles continuously in a wave-like motion ; however, these mechanisms can be slowed or stopped by smoking or other forms of air pollution, by certain immunosuppressive drugs, and by some forms of illness. These predisposing conditions, called risk factors, increase the chance of individuals becoming infected with legionellae.
Although infectious dose responses have been determined for some laboratory animals '60 the infectious dose for humans has not been determined . A reasonable assumption is that individuals who have more risk factors should become infected with lower doses than individuals who have few or no risk factors.
Because contamination of some potable waters with legionellae have been documented, concern has been expressed that legionellosis could be contracted by drinking contaminated water, especially if it should be aspirated into the lungs ." On rare occasions Legionnaire's disease may have occurred through aspiration in hospitalized patients with in-dwelling nasogastric tubes .12,61
5.0 Preventative Strategies and Monitoring
Good preventative maintenance is very important in the efficient operation of cooling towers and other evaporative equipment." Preventive maintenance includes having effective drift eliminators, periodically cleaning the system if appropriate, maintaining mechanical components in working order, and having a water treatment program including a biocide. Note that most water treatment programs are designed to minimize scale, corrosion, and biofouling and not to control legionellae.
An estimated 25% to 40% of the 200,000 cooling towers employed on HVAC applications in the U.S . are neither well maintained (broken or missing drift eliminators, unbalanced fans, sludge in basins, and biofilm attached to surfaces) nor treated with biocides . Untreated systems have been correlated with an outbreak of legioneliosis.65 Such conditions are not conducive to efficient system operation (biofouling may reduce heat exchanger efficiency) or to the reducing the risk of legionellosis transmission .
both numbers and virulent characteristics necessary for disease is recommended.
Culturing for Legionella may be appropriate if carried out for a specific purpose, such as tracing the source of an infection, evaluating the potential amplifier or transmission sources at a facility, verifying the effectiveness of a water treatment protocol, verifying that decontamination procedures have been effective, or in health care facilities caring for patients with exceedingly high risk of developing Legionnaire's disease, such as organ transplant recipients or other high risk people .
Routine culturing or samples from building water systems for Legionella has limitations . The presence of the organism is not directly equated to the risk of infection, and the organism has been found without being associated with cases of disease . A number of factors, other than the concentration of organisms in a sample, influence the risk of illness following exposure. Factors include strain virulence, host susceptibility, and how efficiently the organisms are aerosolized to the small particle size required to reach the deep portion of the human lung . Conversely, lack of detection of the organism from a sample does not mean that the potential amplifier sampled will never be colonized. Variations in culture procedures among different labs can lead to different results . Additionally, use of fluorescent antibody or gene probes can result in different values from culture techniques for the same samples so interpretation of the data is important.
Periodic or routine monitoring is never an effective program if done in the absence of a maintenance program . MORE EMPHASIS SHOULD BE PLACED ON CLEAN EQUIPMENT IN EXCELLENT REPAIR THAN ON PERIODIC TESTING WITH CONCURRENT SYSTEM NEGLECT Refer to Section 4.2, Amplifiers, and Section 4.3, Aerosolization, for specific measures to manage amplifiers and aerosols .
6.0 Safety Precautions for Decontamination Procedures
Although poorly documented in the literature, it must be stressed that several workers who have either serviced or cleaned wet-type-heat rejection equipment and other aerosol producing devices have experienced either Legionnaires' disease or Pontiac fevers' But, in another study increased risk for cooling system maintenance workers was not observed . 68
© 1998 ASHRAE (www.ashrae.org). For personal use only. Additional reproduction, distribution, or transmission in either print or digital form is not permitted without ASHRAE’s prior written permission.
1 . Heating, ventilating, air-conditioning, and refrig-erating systems and their components as well as potable hot water services and bathing equipment can amplify and disseminate aerosols of a wide variety of airborne contaminants, including Legionella bacteria, and the agents causing legionellosis (Legionnaires' disease and Pontiac fever) .
7 . Stout, J.E ., VL . Yu, and M.G . Best . 1985 . Ecology of Leqionella pneumophila within water distribution systems . Appl Environ Microbio149 :21-228 .
8 . Pope, D.H ., R.J . Soracco, H.K . Gill, and C .B . Fliermans . 1982 . Growth of Legionella pneumophila in two membered cultures with green algae and cyanobacteria . Curr Microbiol 7:319-322 .
10
water, or air is applied to remove deposits . During decontamination procedures, workers also should wear rubber gloves, goggles, and protective clothing to prevent injury to their skin, eyes, and lungs by the chemicals being used to decontaminate equipment.
Also, air intake ducts should be closed during cleaning if they are within 30 m (100 ft) of a cooling tower being decontaminated . If humidifiers, drain pans, cooling coils, wet duct work, nebulizers, showers, or other in-door equipment are determined to need decon-tamination procedures, measures to minimize and contain aerosols are recommended. Since a variety of equipment and physical situations are possible, workers doing the decontamination should apply the information discussed in Section 3.0, The Disease, and Section 4.0, Transmission Factors and Prevention, to the specific circumstances at the site to protect them-selves and occupants of the building or adjacent buildings.
7.0 Emergency Decontamination for Legionella
7.1 Cooling Systems
The Cooling Tower Institute has formulated an emer-gency protocol for decontaminating wet-type-heat rejection systems using chlorine and dispersants .s9 This protocol also was developed to respond to systems suspected of containing the organisms that caused an outbreak . ASHRAE's position is that this procedure must not be used routinely, because it can be very corrosive and produce toxic fumes. This procedure has been adapted to include additional safety procedures and 10 mg/L free residual chlorine level for 24 hours.'°
7.2 Potable Systems
For emergency decontamination of potable water systems increasing water temperatures above 60°C (140°F) or continuous chlorination at 1 ppm to 2 ppm free chlorine at the tap for several hours may work. Long-term decontamination is not provided by this procedure.
8.0 Conclusions Based on the scientific, medical, and engineering literature available to date, ASHR.AE concludes the following:
2. Design and operation and maintenance procedures that prevent amplification and dissemination of Legionella should be formulated and implemented before systems are operated and continued rigidly thereafter. Although using these practices will not guarantee that a system or individual component will be free of legionellae, they should reduce the chance of the systems becoming heavily colonized with these bacteria .
3. Currently, the only reliable method of testing for the presence of legionellae in a system is by culturing for these organisms . No "non-legionellae" surrogate tests are available, and there is currently no correlation between total bacterial counts and legionellae concentrations . The results of single tests must be interpreted cautiously as the concentration of Legionella in a water system can increase substantially over a few days . Attention should be paid to sample handling and laboratory quality control so the number reported reflects the number present at the time of sampling .
4. The efficacy of a specific biocide treatment in controlling legionellae can only be determined by testing specifically for the presence of legionellae in the field under actual working conditions . Laboratory trials must not be relied on exclusively as the sole proof of the efficacy of a biocide.
9.0 Citations 1 . Hoge, C.W and R.F Breiman. 1991 . The epidemiology and control of Legionella infections : an update . Epidemiol Rev 13 : 329-340 .
2 . Blackmon, J.A ., R . W. Chandler, W B. Cherly, A.C . England, III, J.C . Feeley, M.D . Hicklin, R.M . McKinney, and H.W. Wilkinson . 1981 . Review Article : Legionellosis . Amer J Pathol 102:427-465.
3 . Fallon, R.j ., D .J . Goldberg, J.G . Wrench, S.T. Green, and J .A.N . Emslie . 1993 . Pontiac fever in children . In J.M . Barbaree, R.F Breiman, and A.P Dufour (ed) . Legionella : Current Status and Emerging Perspectives, pp 50-51 . Ameri-can Society for Microbiology, Washington, D.C .
4 . Centers for Disease Control and Prevention . 1994 . Proce-dures for the recovery of Legionella from the environment .
5 . Fliermans, C.B ., W .B . Cherry, L.H . Orrison, S.J. Smith, D.L . Tison, and D.H . Pope . 1981 . Ecological distribution of Leqionella pneumophila . Appl Environ Microbio141 :9-16 .
6 . Fliermans, C.B ., W .B . Cherry, L.H . Orrison, and L.H . Thacker. 1979 . Isolation of Leqionella pneumophila from nonepidemic-related aquatic habitats . Appl Environ Microbio137:1239-2342 .
© 1998 ASHRAE (www.ashrae.org). For personal use only. Additional reproduction, distribution, or transmission in either print or digital form is not permitted without ASHRAE’s prior written permission.
Barbaree, R.F Breiman and A.P Dufour (ed) . Legionella : Current Status and Emerging Perspectives . American Soci-ety for Microbiology, Washington, D.C .
23 . Bartlett, C.L.R ., A.D . Macrae, and J.T. MacFarlane . 1986 . Legionella Infections . Edward Arnold, London, England .
24 . Cordes, L.G ., W .D. Goldman, J.S . Marr, S.M . Friedman, J.D . Band, E.O . Rothschild, H . Kravetz, J.C . Feeley, and D.W Fraser. 1980 . Field investigation team : Legionnaires' disease in New York City. August-September 1978 . Bull NY Acad Med 56:467-482 .
25 . Band, J.D . M . LaVenture, J.P Davis, G.F Mallison, W .L . Schell, P Skaliy, PS . Hayes, H . Weiss, D.J . Greenberg, and D.W Fraser. 1981 . Epidemic Legionnaires' disease : airborne transmission down a chimney. JAMA 254:2404-2407.
26 . Broome, C.V, S .A.T. Goings, S.B . Thacker, R.L . Vogt, H.N. Beaty, and D .W Fraser. 1979. Field Investigation team : the Vermont epidemic of Legionnaires' disease . Ann Intern Med 90:573-577 .
27 . Cordes, L.G., D.W Fraser, P Skaliy, C.A . Perlino, WR. Elsea, G.F Mallison, and PS . Hayes . 1980 . Legionnaires' dis-ease outbreak at an Atlanta, Georgia country club : evidence for spread from an evaporative condenser. Am J Epidemiol 111 :425-431 .
28 . Dondero, R.J .,1r., R.C . Rendtorff, G.F Mallison, R.M . Weeks, J.S . Levy, E.S . Wong, and W. Schaffner . 1980 . An outbreak of Legionnaires' disease associated with a con-taminated air conditioning cooling tower. N Engl J Med 302:365-370 .
29. Garbe, PL., B.J . Davis, J.S . Weisfeld,L . Markowitz, E Miner, F Garrity, J.M . Barbaree, and A.L. Reingold . 1985 . Nosoco-mial Legionnaires' disease-epidemiologic demonstration of cooling towers as a source . J Am Med Assoc 254:52124.
30 . Best, M., VL . Yu, J . Stout, A . Goetz, R.R . Muder, and F Taylor. 1983 . Legionellae in the hospital water supply epi-demiological link with disease and evaluation of a method of control of nosocomial Legionnaires' disease and Pitts-burgh pneumonia . Lancet (Aug 6):307-310 .
31 . Muder, R.R ., VL . Yu, and A.H . Woo . 1986 . Mode of trans-mission of Legionella pneumophila . Arch Intern Med 146:1607-1611 .
32 . Witherell, L.E ., L.A . Orciari, K.C . Spitalny, R.A . Pelletier, K.A . Stone, and R.L . Voght . 1984 . Disinfection of Legionella pneumophila contaminated whirlpool spas . In C . Thronsberry, A. Balows, J.C.Feeley, and W Jakubowski (ed) . Legionella : Proceedings of the 2nd International Sympo-sium . American Society for Microbiology. Washington, D.C .
33 . Patterson, W.J ., D.V Seal, E . Curran, T.M . Sinclair, and J.C . McLuckie . 1994 . Fatal nosocomial Legionnaires' disease : relevance of contamination of hospital water supply by tem-perature-dependent buoyancy-driven flow from spur pipes . Epidemiol Infect 112:513-525 .
34 . Brundrett, G.W. 1992 . Leqionella and Building Services . Butterworth-Heinmann, Ltd . Oxford, United Kingdom .
35 . Gorman, G.W, V .L . Yu, A . Brown, J.A . Hall, L.K. Corcoran, W .T. Martin, W .F Bibb, G.K . Morris, M.H . Magnussen, and D.W Fraser. 1980. Isolation of Pittsburgh pneumonia agent from nebulizers used in respiratory therapy. Ann Intern Med . 93 (4):572-573.
36 . Fenstersheib, M.D; M. Miller, C. Diggins, S. Liska, L . Detwiler, S.B . Werner, D . Lindquist, VJL. Thacker, and R.F Benson . 1990 . Outbreak of Pontiac fever due to Legionello anisa . Lancet 336:3-37.
21 . Osterholm, M.T., T.D.Y Chin, D.O . Osborne, H.B . Dull, A.G . Dean, D.W. Fraser, PS . Hayes, and WN. Hall . 1983 . A 1957 outbreak of Legionnaires' disease associated with a meat packing plant . Am J Epidem 117:63-67 .
22 . Horwitz, M.A ., B .J . Marston, C .V Broome, and R.F Breiman . 1993. Prospects for Vaccine Development . In J.M .
11
9 . Anand, C .M ., A.R . Skinner, A . Malic, and J.B . Kurta . 1983 . Interaction of L. pneumophila and a free living amoeba (.4canthamoeba palestinensis) . J of Hygiene 91 :167-178 .
10 . Barbaree, J.M ., B.S . Fields, J .C . Feeley, G.W Gorman, and W.T. Martin . 1986 . Isolation of protozoa from water as-sociated with a Legionellosis outbreak and demonstration of intracellular multiplication of Legionella . Appl Environ Microbio151 :422-424 .
11 . Joly, J.R ., R.M . McKinney, J.O . Tobin, W.F Bibb, I.D . Watkins, and D. Ramsay. 1986 . Development of a standard-ized subgrouping scheme for Leqionella pneumophila serogroup 1 using monoclonal antibodies . J Clin Microbiol 23:768-771 .
12 . Selander, R.K ., R.M . McKinney, T.S . Whittam, W F Bibb, D.J . Brenner, FS . Nolte, and EE.Pattison . 1985 . Genetic struc-ture of a population of Legionella pneumophila . J Bacteriol 163:1021-1037 .
13 . Mamolen, M., R.F Breiman, J.M . Barbaree, R.A . Gunn, K.M . Stone, J .S . Spika, D.T. Dennis, S.H . Mao, and R.L.Vogt . 1993 . Use of multiple molecular subtyping techniques to investigate a Legionnaires' disease outbreak due to identical strains at two tourist lodges . J Clin Microbio131 :2584-2588 .
14 . Streulens, J .J ., N . Maes, A. Deplano, N . Bornstein, and F. Grimont . 1993 . Comparison of methods for subtyping Legionella pneumophila . In J.M . Barbaree, R.F Breiman, and A.P Dufour (ed) . Current Status and Emerging Per-spectives, pp 183-186 . American Society for Microbiol-ogy, Washington, D .C .
15 . Gomez-Lus, P, B.S . Fields, R.F Benson, W.T. Martin, S.P O'Connor, and C .M . Black . 1993 . Comparison of arbi-trarily primed polymerase chain reaction, ribotyping and monoclonal antibody analysis for subtyping Legionella pneumophila serogroup 1 . J Clin Microbiol 31 :1940-1942 .
16 . Schoonmaker, D., T. Heimberger, and G. Birkhead . 1992 . Comparison of ribotyping and restriction enzyme analysis using pulsed-field-gel electrophoresis for distinguishing Legion ella pneumophila isolates obtained during a nosoco-mial outbreak . J Clin Microbio131 :1491-1498 .
17 . Barbaree, J . M . 1993 . Selecting a subtyping technique for use in investigations of legionellosis epidemics . In J .M . Barbaree, R .F. Breiman, and A .P Dufour (ed) . Legionella : Current Status and Emerging Perspectives, pp 169-172 . American Society for Microbiology, Washing-ton, D.C .
18 . Yee, RB . and R.M. Wadowsky. 1982 . Multiplication of Legionella pneumophila in unsterlized tap water. Appl Env Microbio143 :1330-1334 .
19 . Fraser, D .W., T.R . Tsai, O. Orenstein, W.E . Parkin, J .J . Beecham, R.G . Sharrar, J . Harris, G.F Mallison, S.M . Artin, J .E . McDade, C .C . Sheppard, and P S . Brachman. 1977 . Field investigation team : Legionnaires' disease : description of an epidemic of pneumonia . N Engl J Med 297:1189-1197 .
20 . McDade, J.D ., J . Brenner, and FM. Bozeman . 1979 . Le-gionnaires' disease bacterium isolated in 1947 . Ann Intern Med 90:659-661 .
© 1998 ASHRAE (www.ashrae.org). For personal use only. Additional reproduction, distribution, or transmission in either print or digital form is not permitted without ASHRAE’s prior written permission.
37. Hady, W G., R.C . Mullen, C.S . Mintz, B.G. Shelton, R.S . Hopkins, and G.L . Daikos . 1993. Outbreaks of Legionnaires' disease linked to a decorative fountain . Am J Epidemiol 138:555-562 .
38 . Mahoney, FJ., C.W Hoge, T.A. Farley, J.M . Barbaree, R.F Breiman, R.F Benson, and L.M . McFarland . 1992. Communitywide outbreak of Legionnaires' disease associ-ated with a grocery store mist machine . J Infect Disease 165:736-739 .
39 . Glick, T.H ., M.G . Gregg, B . Berman, G. Mallison, W.W Rhodes, and I . Kassanoff. 1978 . Pontiac fever: an epidemic of unknown etiology in a health department . 1 . Clinical and epidemiologic aspects . Am J Epidemiol 107 : 149-160 .
40 . Kaufmann, A.K ., J .E . McDade, C.M . Patton, J.V Bennett, P Skaliy, J.C . Feeley, D .C . Anderson, M.E . Potter, V .F. Newhouse, M.B . Gregg, and PS. Brachman . 1981 . Pontiac fever : demonstration of its mode of transmission . Am J Epidemiol 114:33774.
41 . Friedman, S., K . Spitalmy, J . Barbaree, Y Faur, and R . McKinney. 1987 . Pontiac fever outbreak associated with a cooling tower. Am J Public Health 77:56&$71 .
42 . Fields, B.S ., J.M . Barbaree, G.N . Sanden, and WE, Morrill . 1990 . Virulence of Leqionella anisa strain associated with Pontiac fever : an evaluation using protozoan, cell culture and guinea pig models . Infect Immun 58:3139142 .
43 . Herwaldt, L.A ., G.W Gorman, T. McGrath, S . Toma, B . Brake, A.W Hightower, J . Jones, A.L . Reingold, PA . Boxer, P Tang, C .W. Moss, H .W. Wilkinson, D.J . Brenner, A.G . Steigerwalt, and C.V Broome . 1984 . A new Legionella spe-cies, Legionella feleii species nova, causes Pontiac fever in an automobile plant. Ann Intern Med 100:333-338 .
44 . Barbaree, J.M . 1991 . Controlling Legionella in cooling towers . ASHRAE J 33:(6)38-42 .
45 . Dutka, B.J ., K. Walsh, E Ewan, . A. El-Shaarawi, and R.S . Tobin . 1983. Environmental distribution patterns of Legionella in central Canada and longevity studies . National Water Re-search Institute manuscript no . 69-AMD-5-83-BID . Canada Centre for Inland Waters, Burlington, Ontario, Canada .
46 . Tison, D.L . and R.J . Seidler. 1983 . Legionella in aquatic habitats in the Mount Saint Helen's blast zone . Curr Microbio19:345-348 .
47 . Shelton, B ., D . Flanders, and G. Morris . 1994 . Legionnaires' disease outbreaks and cooling towers with amplified Legionella concentrations . Current Microbio128:359-363 .
48 . Witherell, L.E ., L.F Novick, K.M . Stone, R.W Duncan, L.A . Orciari, S .J . Kappel, and D.A . Jilson . 1986 . Legionella in cooling towers . J Env Health 49 (3):134-139 .
49 . Broadbent, C.R . 1997. Water Treatment . Mechanical En-gineering Services Application Manual . Australian Institute of Refrigeration, Air-Conditioning and Heating .
50 . Tyndall, R.L ., E.S . Lehman, EX Bowman, D.K . Milton, and J .M . Barbaree . 1995 . Home humidifiers as a potential source of exposure to microbial pathogens, endotoxins, and allergens . Indoor Air 5:171-178 .
51 . Patterson, W.J ., D .V Seal, E . Curran, T.M . Sinclair, and J.C . McLuckie . 1994. Fatal nosocomial Legionnaires' disease : relevance of contamination of hospital water supply by tem-perature-dependent buoyancy-driven flow from spur pipes . Epidemiol Infect 112:513-525 .
52 . Freije, M.R. 1996. Legionella Control in Health Care Fa-cilities . A Guide for Minimizing Risk. HC Information Re-sources, Inc ., Indianapolis, IN .
53 . Chartered Institution of Building Services Engineers . 1991 . Minimizing the Risk of Legionnaires' Disease . Tech-nical Memoranda 13 . London, England .
54. Breiman, R.F, B.S . Fields, G.N . Sanden, L . Volmer, A . Meir, and J.S . Spika. 1990 . Association of shower use with Legionnaires' disease : possible role of amoebae . JAMA 263 (21):2924-2926 . 55 . Jernigan, D.B ., J. Hofmann, M.S . Cetron, C.A. Genese, J.E Nuorti, B.S . Fields, R.F Benson, R.J . Carter, EH . Edelstein, J.C . Gurrero, S.M . Paul, H.B . Lipman, and R.FBreiman . 1996. Out-break of Legionnaires' disease among cruise ship passengers exposed to a contaminated whirlpool spa. Lancet 347:49500 .
56 . Shands, J ., J . Ho, R . Meyer, G. Gorman, G. Mallison, S . Finegold, and D . Fraser. 1985 . Potable water as a source of Legionnaires' disease. JAMA 253:1412-1416 . 57 . States, S.J ., L.F Conley, J.M . Kuchta, B.M . Oleck, M.J . Lipovich, R.S . Wolford, R.M . Wadowsky, A.M . McNamara, J.L . Sykora, G. Keleti, R.B . Yee . 1987 . Survival and multipli-cation of Legionella pneumophila in municipal drinking water systems . Appl Env Microbiol 53:979-986 . 58 . Berendt, R.F 1980 . Survival of Legionella pneumophila in aerosols : effect of relative humidity. J Infect Dis 141 :689 . 59 . Broome, C .V 1983 . Current issues in epidemiology of Legionellosis . In C . Hornsberry, A. Balows, J .C . Feeley, and W. Jakubowski (ed) . Legionella : Proceedings of the 2nd In-ternational Symposium . American Society of Microbiology. Washington, D.C . 60 . Brendt, R.F, H.W Young, R.G. Allen, and G.L. Knutsen. 1980 . Dose response of guinea pigs experimentally infected with aerosols of Legionella pneumophila . J Infect Dis 141:689 . 61 . Yu, VL . 1993 . Could Aspiration be the major mode of transmission for Legionella? Am J Med 95:13-15 . 62 . Blatt . S .P, M.D . Parkinson, E . Pace, P Hoffman, D. Dolan, P Lauderdale, R . Zajac, and G.Melcher. 1993 . Nosocomial Legionnaires' disease : aspiration as a primary mode of dis-ease acquisition . Am J Med 95:(7)16.
63 . Venezia, R.A ., M.D . Agresta, E.M . Hanley, K . Urquhart, and D . Schoonmaker. 1994 . Nosocomial legionellosis asso-ciated with aspiration of nasoqastric feedings diluted in tap water. Infec Control Hosp Epidermiol 15:529-533 . 64 . American Society of Heating, Refrigerating and Air-Con-ditioning Engineers . 1996. Systems and Equipment Hand-book 33b .10-13 . Atlanta, GA .
65 . Mitchell, P, A . Chereshsky, AT Haskell, and M.A . Briesman . 1991 . Legionellosis in New Zealand : first recorded outbreak . New Zealand Med J 104:915--916 .
66 . OSHA . Section 11 Chapter 7 Legionnaires' Disease .
67 . Fraser, D.W., D.C . Beubner, D.L . Hill, and D.K . Gilliam . 1979 . Nonpneumonic, short-incubation-period Legionellosis (Pontiac fever) in men who cleaned a steam turbine con-denser. Science 205:690-691 . 68 . Goldman, W .D . and J.S . Marr . 1980 . Are air-conditioning maintenance personnel at increased risk of legionellosis? Appl Env Microbio140 : 114-116 .
69 . Cooling Tower Institute . 1980 . Suggested protocol for emergency cleaning of cooling towers and related equip-ment suspected of infection by Legionnaires' disease bac-teria (pneumophila) . Houston, TX .
70 . Tablan, O.C ., L .J . Anderson, N.H . Arden, R.F Breiman, J.C . Butler, M.M . McNeil, and the Hospital Infection Control Practices Advisory Committee . 1994 . Guideline for preven-tion of nosocomial pneumonia . Part 1 . Issues on prevention of nosocomial pneumonia . Am M Infect Control 22:247-292 .
12
© 1998 ASHRAE (www.ashrae.org). For personal use only. Additional reproduction, distribution, or transmission in either print or digital form is not permitted without ASHRAE’s prior written permission.