Embed Size (px)
Citation preview

ORIGINAL ARTICLE
Less invasive transjugular approach with Fallopian bridgetechnique for facial nerve protection and hearingpreservation in surgery of glomus jugulare tumors
Yoichi Nonaka & Takanori Fukushima & Kentaro Watanabe &
Allan H. Friedman & John T. McElveen Jr. &Calhoun D. Cunningham III & Ali R. Zomorodi
Received: 19 November 2012 /Accepted: 10 March 2013 /Published online: 6 June 2013# Springer-Verlag Berlin Heidelberg 2013
Abstract For the past three decades, surgery of glomus jug-ulare tumors (GJTs) has been characterized by extensive com-bined head and neck, neuro-otologic, and neurosurgicalapproaches. In recent years, the authors have modified theoperative technique to a less invasive approach for preserva-tion of cranial nerves while achieving satisfactory tumor re-section. We evaluated and compared the clinical outcomes ofour current less invasive approach with our previous more
extensive procedures. The clinical records of 39 cases of GJTsurgically treated between 1992 and 2011 were retrospectivelyreviewed. The less invasive transjugular approach with Fallo-pian bridge technique (LI-TJ) was used for the most recentfive cases. The combined transmastoid–transjugular and highcervical (TM-HC) approach was performed in 30 cases, whilefour cases were treated with a transmastoid–transsigmoidapproach with facial nerve translocation. Operative technique,extent of tumor resection, operating time, hospital stay, andmorbidity were examined through the operative records, and acomparison was made between the LI-TJ cases and the moreinvasive cases. No facial nerve palsy was seen in the LI-TJgroup while the TM-HC group demonstrated six cases(17.6 %) of facial palsy (House–Brackmann facial nervefunction grading scale grade II and III). The complication ratewas 0 % in the LI-TJ group and 16.7 % in the more invasivegroup. The mean operative time and hospital stay were shorterin the LI-TJ group (6.4 h and 4.3 days, respectively) comparedwith the more invasive group (10.7 h and 8.0 days, respectively).The LI-TJ approach with Fallopian bridge technique providedadequate tumor resection with cranial preservation and definitiveadvantage over the more extensive approach.
Keywords Facial nerve . Fallopianbridge .Glomus jugularetumor . Jugular bulb . Jugular foramen
Introduction
Glomus jugulare tumors (GJT) are formidable lesions whichcan grow aggressively to damage inner ear structures, involve
Portions of the contents of the paper have been presented at “The 24thAnnual Meeting of Japanese Society for Skull Base Surgery” (Tokyo,Japan, July 11–12, 2012) and at the “Fifth International Cerebrovascularand Skull Base Workshop” (Kiev, Ukraine, September 6–8, 2012).
Y. Nonaka : T. Fukushima :K. Watanabe :A. H. Friedman :A. R. ZomorodiDivision of Neurosurgery, Duke University Medical Center,Box 3807, 1000 Trent Drive 4520 Hosp South, Durham,NC 27710, USA
T. FukushimaCarolina Neuroscience Institute, 4030 Wake Forest Rd suite 115,Raleigh, NC 27612, USA
J. T. McElveen Jr. : C. D. Cunningham IIICarolina Ear & Hearing Clinic, PC, 3100 Duraleigh Road suite300, Raleigh, NC 27612, USA
Y. Nonaka (*)Department of Neurosurgery, Fukushima Takanori Skull BaseCenter, Shin-yurigaoka General Hospital, 255 Furusawa Asao-ku,Kawasaki, Kanagawa 215-0026, Japane-mail: [email protected]
Y. Nonakae-mail: [email protected]
Neurosurg Rev (2013) 36:579–586DOI 10.1007/s10143-013-0482-x

multiple cranial nerves and the carotid artery, or extend into theintracranial and high cervical spaces. These tumors continue topose a significant challenge to skull base surgeons [1, 5, 6, 8,18, 23, 28, 32, 33, 36].
Over the past three decades, the extensive postauricularapproach with facial nerve rerouting and high cervical expo-sure introduced by Fisch has been the basis for GJT surgery[8]. This technique has been recommended by many authorswith some modifications and is advocated as a two-stageoperation in some cases [5, 6, 20, 21, 23].
However, in our experience, the postauricular combinedapproach is too invasive and is associated with significantmorbidity and patient dissatisfaction. Closure of the externalauditory canal (EAC), radical procedures in the inner ear,rerouting of the facial nerve, manipulation of the lower cranialnerves, and high cervical carotid artery exposure all resulted inan unacceptable rate of cranial nerve dysfunction.
Over the past 20 years, we have attempted to modify theFisch approach tomake it a smaller less invasive exposure andminimize cranial nerve morbidity. In recent years, we havedeveloped a less invasive transjugular approach with Fallo-pian bridge technique (LI-TJ), which allows tumor resectionwhile preserving hearing and protecting the pars nervosa.
We describe the key aspects of this approach with anatom-ical demonstrations and evaluate its advantages by retrospec-tively reviewing our series of GJT treated over the past 20 years,comparing the clinical outcomes of the new LI-TJ cases withour prior approaches.
Clinical material and methods
Over the past 20 years, between 1992 and 2011, 39 GJTs weresurgically treated by the senior author (T.F.) and the skull baseteam. The clinical records of these patients were retrospec-tively reviewed through operative records, radiological find-ings, and intraoperative videos. Angiography and preopera-tive embolization were routinely used in all cases. Operativetechnique, extent of tumor resection, duration of surgery,hospital stay, blood loss, and morbidity were analyzed. Theresults obtained with the LI-TJ approach were compared withour prior more extensive approaches using the Student t test todetect any significant difference (P<0.05).
Surgical approaches used
The postauricular combined transmastoid–transjugular andhigh cervical (TM-HC) approach was used for tumors withextension into the high cervical region in 30 cases. The trans-mastoid–transsigmoid (TM-TS) approach with anterior trans-location of the facial nerve was used in four cases where thetumor was located in the jugular foramen, and intradural space,with minimal high cervical involvement. The LI-TJ approach
with Fallopian bridge technique was performed for our mostrecent five cases.
Evolution of less invasive surgical technique
Over the initial 10 years of our experience, we modified theFisch technique. First, wemoved away from performing a two-stage operation. Second, we abandoned the large S-shapedincision for a small postauricular C-shaped incision. Third, inpatients with functional hearing, we did not close the externalauditory canal. Fourth, we stopped performing extensive neckdissection in favor of a limited high cervical exposure.
In four cases of small to large tumors with minimalextension to the high cervical region, we performed a trans-mastoid–transsigmoid–transjugular approach with anteriortranslocation of the Fallopian segment of the facial nerve[10, 23]. We recognized that even though we used the lessinvasive transmastoid and high cervical approach, we expe-rienced significant morbidity with facial weakness, hearingloss, and lower cranial nerve dysfunction. In addition, of the30 patients in the combined TM-HC group, there were fivecases (16.7 %) of wound infection and CSF leak. In order todecrease these complications, after extensive anatomicstudy, we have developed a much less invasive transmastoid,infralabyrinthine, transjugular approach with preservation ofthe Fallopian canal.
Description of the LI-TJ approach and Fallopian bridgetechnique
The patient is positioned in a supine position with headsupported on an ENT pillow. A standard retroauricular C-shaped incision is made. An extended mastoidectomy isperformed with total skeletonization of the sigmoid sinus,exposing both the retrosigmoid and presigmoid dura. Max-imum shaving of the labyrinth and Fallopian canal, and fullexposure of the jugular dome are done next. A thin layer ofcortical bone (egg shell) is left to cover the entire Fallopiansegment of the facial nerve from the genu to the stylomastoidforamen, creating the “Fallopian bridge” (Fig. 1a). The mas-toid tip is maximally skeletonized, the digastric groove isremoved, and infrajugular drilling is carried down into theoccipital condyle until the hypoglossal canal is exposed.
Extended facial recess exposure and skeletonizationof the inferior tympanic ring
After creation of the Fallopian bridge, further bone removalfrom the facial recess exposes the tumor in the inner ear andthe hypotympanum area [2, 24, 30, 34, 35]. This allowsidentification and preservation of the annulus of the tympan-ic membrane. While protecting the thin wall of the externalauditory canal, the inferior bony tympanic ring is maximally
580 Neurosurg Rev (2013) 36:579–586

drilled away. This removes the base of the styloid processand exposes the vertical C7 segment of the internal carotidartery which is located anterior to the jugular bulb [22]. Atthis point, the viewing angle of the microscope can bemanipulated, allowing the surgeon full visualization of thejugular structures, the vertical carotid artery, and the hearingapparatus, looking from above or below the Fallopian bridge.
In amajority ofGJTs, the retrofacial air cell space is filledwithtumor. Resection of the tumor from this suprajugular area mustbe done with extreme caution to prevent damage to the posteriorsemicircular canal and the basal turn of the cochlea. Additionally,care must be used while resecting tumor from around the internalcarotid artery (ICA) to prevent damage to the crossing ninthnerve or the arterial adventitia. Transsigmoid and transjugularexposure facilitates resection of the major tumor mass. Thedissection plane between the tumor and the medial wall of thejugular bulb is established proximally in the sigmoid sinus, inorder to preserve the lower cranial nerves (Fig. 1b). In cases ofintradural extension, maximum effort is used to preserve ana-tomical continuity of the lower cranial nerves, unless the patientpresents with lower cranial nerve deficits.
Tumor extension into the internal jugular vein can be removedwith dissectors, ring curettes, and tumor forceps because thisportion of the tumor is not adherent to the endothelial surface(Fig. 2a–e). As the tumor is removed from the intraluminal space,bleedingwill be encountered from remaining feeding vessels andthe inferior petrosal sinus. These are controlled with the standardtechniques of cautery, bone wax, and Surgicel.
Results
Table 1 summarizes the clinical features of our cases. TheFisch classificationwas used to classify these lesions (Table 2).
Thirty of the 39 cases were resected with the combined TM-HC with or without the transotic approach. Four cases weretreated with a TM-TJ approach with facial nerve translocation.Most recently, five cases were treated with the LI-TJ Fallopianbridge technique.
Using our prior more invasive approaches, 24 out of 34patients had gross total resection (70.5 %), 5 cases had neartotal resection (14.7 %), and 5 cases (14.7 %) had subtotalresection. In our five LI-TJ cases, three (60 %) had GTR,and two patients (40 %) had near total resection. The extentof tumor resection was similar in the two groups.
There was no mortality in this series. Non-neurologicaloperative complications including CSF leaks and wound infec-tions were seen in 16.7 % in the more invasive surgery group.There were no CSF leaks or wound infections in the LI-TJgroup.
Facial nerve outcome
No postoperative facial nerve weakness or palsies were seenin the LI-TJ group. The more invasive group (TM-HC orTM-TS) had six cases of new facial palsy (17.6 %; House–Brackmann facial nerve function grading scale grade II andIII) [13]. In these cases, the facial nerve was either reroutedor translocated anteriorly. Nerve reconstruction using a suralnerve or greater auricular nerve was performed in threecases with preexisting severe facial nerve palsy.
Hearing preservation
Postoperative hearing function was preserved at the preop-erative level in all cases of the LI-TJ approach. The transoticapproach was applied in seven cases in the TM-HC group.Six of these patients lost hearing as a result of the approach.
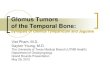
Fig. 1 a The schematic illustration demonstrates final exposure of theFallopian bridge technique. Vertical portions of the carotid artery andjugular bulb are exposed under the Fallopian bridge. The sigmoid sinus isskeletonized all the way down to the jugular bulb. Transcondylar drilling
is performed until the hypoglossal canal is exposed. b Cadaveric studydemonstrates final picture of this approach after tumor removal. Thesigmoid sinus and inner wall of the jugular bulb were removed to exposelower cranial nerves (CNIX, X, and XI) at the jugular foramen
Neurosurg Rev (2013) 36:579–586 581

In addition, three patients had worsening of their preopera-tive deficits. In all, 26 % of patients in the more invasivegroup had worsening hearing or deafness as a result of thesurgery.
LCN function
Of the five cases in the LI-TJ group, two patients had preex-isting lower cranial nerve (LCN) difficulty, and no new defi-cits occurred in this group. In the more invasive group, sixpatients (17.6 %) developed new swallowing disturbance orvocal cord paralysis, while five patients (14.7 %) had wors-ening of their preoperative CNIX or X deficits.
In the more invasive surgery group, there were two patientswith new deficits and two patients with worsening dysfunctionof CNXI. Additionally, there were two new CNXII deficits inthis group. There were no new deficits or worsening of CNXIor XII function in the LI-TJ group.
Operating time, blood loss, and hospital stay
Table 3 summarizes the operating time, estimated blood loss,and hospital stay in the LI-TJ group and the TM-HC group.These data were available for all 5 LI-TJ cases (case no. 35–39)and 21 of the TM-HC cases (case no. 1, 2, 4–7, 9, 11, 13–18,21, 24, 26–28, 32, and 33) that could have been applied the LI-
Fig. 2 a Coronal MRIsdemonstrating a glomusjugulare tumor in the rightjugular foramen withextracranial expansion throughthe jugular bulb. bIntraoperative photodemonstrates exposure of theright side jugular bulb and itsvicinity through a transmastoiddrilling using the Fallopianbridge technique. The tumorfilled the jugular bulb and stuckout from its upper wall. c–eAfter opening the jugular bulb,the intraluminal component ofthe tumor can be pulled outwithout difficulty
582 Neurosurg Rev (2013) 36:579–586

TJ approach with retrospective analysis. The mean operatingtime was 6.44 h (range, 4.5–8.8) in the LI-TJ group and 10.63 h(range, 7.3–17.7) in the TM-HC group (P=0.0174).
The mean blood loss was 260 cc (range, 50–400) in theLI-TJ group and 512 cc (range, 100–1,000) in the TM-HCgroup (P=0.0607). The mean hospital stay was 4.3 days
Table 1 Clinical summary of patients with glomus jugulare tumors
Case no. Age/sex Fischclassification
Previoussurgery
Surgicalapproach
Extent oftumorremoval
Postoperative cranial nerve deficits Non-neurologicalcomplications
VII VIII IX X XI XII
1 30/F C1De2 TM-HC GTR +* +, #
2 50/M C3De2 TM-HC GTR + +* +*
3 65/F C4De2 TM-HC GTR +*, # +*
4 64/F C1De2 TM-HC GTR +*
5 31/F C1De2 TM-HC GTR
6 55/M C1De2 TM-HC GTR +*
7 53/M C1De1 + TM GTR +* +* +* +*
8 28/F C2De2 TM-HC NTR +* +* Wound infection
9 44/M C3De2 TM-TS GTR +*, #
10 54/F C3De2Di2 TM-HC GTR +* W W W Wound infection
11 68/F C2De2 TM-HC NTR +*
12 33/F C4De2 + TM-HC GTR +*
13 28/F C2De2 TM-HC GTR + +* +* +*
14 50/M C3De2 TM-HC NTR + +* +
15 42/M C2De2 TM-HC STR + +* + W
16 23/F C2De2 TM-HC GTR W + CSF leak, wound infection
17 25/F C1De2Di1 TM-HC NTR +*
18 53/F C2De2 TM-HC GTR W + + +
19 35/F C4De2 TM-HC GTR +*, # + CSFleak, otitis media
20 47/F C3De2Di1 TM-HC NTR + W + + +
21 42/F C2De2Di1 TM-HC GTR W W W
22 42/M C2De2 TM-HC GTR +
23 44/F C2De2Di2 TM-HC GTR +* + +* +*
24 34/M C2De2 TM-HC GTR +* + +
25 58/F C2De2 TM-HC GTR
26 43/F C1De2 + TM-TS STR +* +*
27 30/F C2De2 TM-HC GTR
28 37/F C2De2 TM-HC STR + +*
29 36/M C2De2 TM-HC GTR W +* +* CSF leak, infection
30 54/F C4De2Di1 TM-HC STR W +*
31 27/M C3De2Di2 + TM-TS GTR +*
32 49/F C2De2 TM-HC STR +*
33 41/F C2De2 TM-HC GTR +* +* +* +*
34 57/M C3De2 TM-HC GTR +* +* +* +* +*
35 58/M C1De2 LI-TJ NTR +*
36 56/F C1De2 LI-TJ NTR +* +* +* +*
37 65/F C1De2 LI-TJ GTR
38 43/M C1De2 + LI-TJ GTR +* +* +*
39 52/F C2De2 LI-TJ GTR
CSF cerebrospinal fluid, GTR gross total resection, LI-TJ less invasive transjugular, NTR near total resection, STR subtotal resection, TMtransmastoid, TM-HC combined transmastoid transjugular and high cervical, TM-TS transmastoid–transsigmoid, W preexist deficit worsened, +new deficit, +* preexisting deficit, # nerve reconstruction was performed
Neurosurg Rev (2013) 36:579–586 583

(range, 3–6 days) in the LI-TJ group and 8.0 days (range, 4–12 days) in the TM-HC group (P=0.0012). This highlightsthe significant advantage of the less invasive LI-TJ approachwith Fallopian bridge technique.
Discussion
Development of less invasive surgical approaches for GJTs
In 1969, House proposed an extended facial recess approach toexpose the hypotympanum, which provided access to the JBwhile conserving the EAC [12]. Farrior demonstrated an ante-rior hypotympanic approach which effectively cured or con-trolled small GJTs in selected patients with the preservation ofthe facial nerve and hearing [7]. Fisch described the infratem-poral fossa approach at the end of 1970s which was an exten-sive and invasive method that became a standard surgicaltechnique for GJTs [8]. Since then, modified techniques andless invasive approaches were described in the literature withtailored exposures depending on tumor size and extension [6,17, 19–21, 23, 25, 29, 37].
Rerouting or translocation of the facial nerve invariablycaused moderate to severe facial nerve deficits. Martin andPrades reported selective application of the infralabyrinthineapproach without facial nerve mobilization for localizedtumors without involvement of the medial aspect of the ICA[27]. Maniglia described the inferior mastoidectomy–hypo-tympanic approach for the removal of smaller GJTs [26].Jackson first introduced the technique of facial nerve protec-tion by bony coverage in the infratympanic extended facialrecess approach (IEFR) [16]. The IEFR was presented as aconservative procedure with very specific indications andlimitations. The “Fallopian bridge technique” was first used
by Pensak and Jackler for smaller tumors with no erosion ofthe EAC and no extension anterosuperior to the carotid genu[15, 31]. In the majority of their cases, satisfactory exposure ofthe region of the jugular fossa could be provided withoutfacial nerve rerouting with favorable result.
Our technique is similar to the jugular foramen approachdescribed by Inserra et al. and the transmastoid infralabyrinthineapproach described by Gjuric and Bilic, differing in the extent ofskin incision [11, 14]. A postauricular C-shaped incision pro-vides enough exposure of the mastoid and its vicinity. Bobra etal. proposed the infralabyrinthine approach and the pre- andretrofacial approaches with or without closure of the EAC,whichallowed removal of any size of GJT without rerouting of thefacial nerve [3, 4]. With these techniques, good facial nerveoutcomes have been reported in patients with GJTs. The LI-TJapproach is a combination and modification of these previouslyreported approaches and concepts which can be performedthrough the standard retroauricular C-shaped incision.
Preservation of LCNs
The other major management issue with GJTs is the preserva-tion of the LCN function. Unless the patient presents with
Table 2 Fisch classification ofglomus tumors Class Description
A Tumors confined to the tympanum and arising from the promontory, without evidence of bone erosion
B Tumors involving the tympanum, with or without mastoid involvement but always arising from thehypotympanic region; the cortical bone over the jugular bulb must be intact
C Tumors eroding the bone over the jugular bulb; the tumor may extend into and destroy the bone of theinfralabyrinthine and apical compartments of the temporal bone
C1 Tumors involving the foramen caroticum
C2 Tumors involving the vertical segment of the carotid canal
C3 Tumors involving the horizontal segment of the carotid canal
C4 Tumors extending to the ipsilateral foramen lacerum and cavernous sinus
D Tumors with intracranial extension
De1 Tumors with intracranial extradural extension of up to 2 cm
De2 Tumors with intracranial extradural extension of more than 2 cm
Di1 Tumors with intracranial intradural extension of up to 2 cm
Di2 Tumors with intracranial intradural extension of more than 2 cm
D3 Tumors with inoperable intracranial extension
Table 3 Operating time, blood loss, and hospital stay
LI-TJ approacha TM-HC approachb P value
Operating time (h) 6.44 (4.47–8.75) 10.63 (7.28–17.7) 0.0174
Blood loss (cc) 260 (50–400) 512 (100–1,000) 0.0607
Hospital stay (days) 4.3 (3–6) 8.0 (4–12) 0.0012
a Data analysis of case numbers 35–39b Data analysis of case numbers 1, 2, 4–7, 9, 11, 13–18, 21, 24, 26–28,32, and 33
584 Neurosurg Rev (2013) 36:579–586

compensated severe preexisting LCN deficits, our prior expe-rience has convinced us that worsening or a new deficit ofLCNs substantially diminishes the patient’s quality of life.Meticulous care must be used to preserve the LCNs in theintradural, pars nervosa, and high cervical regions. We had nocases of worsening LCN function in our patients who had theLI-TJ approach.
In our series, two third of the GJTs were soft, separabletumors which compressed the pars nervosa. One third of thetumors were fibrous and firm tumors with invasion of the parsnervosa. In the latter instance, it is best to leave remnants oftumor along the cranial nerves or ICA. Any remnants of tumorfragments along the internal carotid artery or the pars nervosacan be observed with radiographic surveillance for many yearswithout symptomatic progression. Symptomatic progressionor significant growth of these remnants should be treated witha second operation or radiosurgery.
Facial nerve and hearing function
We have been using the combined TM-HC approach for GJTswhich resulted in significant incidence of facial nerve palsy(17.6 %) and hearing deficits (26 %). We have avoided totalrerouting of the facial nerve in favor of a slight anteriortranslocation of the nerve. Nonetheless, we noticed significantincidence of facial nerve weakness with our technique. In aprevious publication, we reported a 26.7 % incidence ofpostoperative facial nerve palsy, half of which were permanentin the surgery for GJTs resected via TM-HC approach [9, 23].We had no cases of facial nerve palsy in our LI-TJ group.
In addition, we found significant decreases in total operat-ing time and hospital length of stay with the LI-TJ approach.While this approach is not appropriate for certain very exten-sive giant tumors, retrospective analysis of the radiologic find-ings and operative records demonstrated that 21 out of our 30(70 %) TM-HC cases could have been treated with the LI-TJapproach with elimination of the high cervical exposure.
Conclusions
Increasingly, publications advocate the tailored surgical approachto GJTs depending on the presenting symptoms, tumor size, andextent of the tumor. Except for cases with extensive and infiltra-tive large tumors, a giant mass, or preexisting deficits, the ma-jority of GJTs should be treated with the primary priority beingpreservation of cranial nerves and the carotid system.
Although our case numbers are still small, our experiencewith the LI-TJ approach with Fallopian bridge technique dem-onstrated that radical resection can be achieved while preservingfacial nerve function and the audiologic structures. Operatingtime and hospital stay all favored the LI-TJ approach over theTM-HC approach.
Acknowledgments The authors wish to thank to Elizabeth Howe,Kimberly Peterkin, and Lori Radcliffe for providing the follow-upstudies and examinations.
Conflict of interest The authors report no conflict of interestconcerning the materials or methods used in this study or the findingsspecified in this paper.
References
1. Al-Mefty O, Teixeria A (2002) Complex tumors of the glomusjugulare tumors: criteria, treatment, and outcome. J Neurosurg97:1356–1366
2. Bejjani GK, Sullivan B, Salas-Lopez E et al (1998) Surgicalanatomy of the infratemporal fossa: the styloid diaphragm revis-ited. Neurosurgery 43:842–852
3. Borba LA, Ale-Bark S, London C (2004) Surgical treatment ofglomus jugulare tumors without rerouting of the facial nerve: aninfralabyrinthine approach. Neurosurg Focus 17:E8
4. Borba LA, Araujo JC, de Oliveria JG et al (2010) Surgical managementof glomus jugulare tumors: a proposal of approach selection based ontumor relationships with the facial nerve. J Neurosurg 112:88–98
5. Brackmann DE, Kinney S, Fu K (1987) Glomus tumor: diagnosisand management. Head Neck Surg 9:306–311
6. Day JD, Tschabitscher M, Apuzzo ML, Koos WT, Matula C (1996)The jugular foramen. In: Day JD (ed) Microsurgical dissection of thecranial base. Churchill Livingstone, New York, pp 135–139
7. Farrior JB (1984) Anterior hypotympanic approach for glomustumor of the infratemporal fossa. Laryngoscope 94:1016–1021
8. Fisch U (1978) Infratemporal fossa approach for extensive tumors ofthe temporal bone and base of the skull. J Laryngol Otol 92:949–967
9. Fukushima T, Couldwell WT (2007) In author reply: the combinedtransmastoid retro- and infralabyrinthine transjugular transcondy-lar transtubercular high cervical approach for resection of glomusjugulare tumors. Neurosurgery 61:E1340
10. Fukushima T, Nonaka Y (2010) Postauricular transmastoid “posteriorITFA”. In: Fukushima T, Nonaka Y (eds) Fukushima manual of skullbase dissection, 3rd edn. AF-Neurovideo, Raleigh, pp 188–201
11. Gjuric M, Bilic M (2009) Transmastoid-infralabyrinthine tailoredsurgery of jugular paragangliomas. Skull Base 19:75–82
12. House W (1969) Management of glomus tumors. Arch Otolaryngol89:170–178, Panel discussion (McCabe BF, Rosenwasser H, HouseW, Witten RM, Hamberger CA)
13. House JW, Brackmann DE (1985) Facial nerve grading system.Otolaryngol Head Neck Surg 93:146–147
14. Inserra MM, Pfister M, Jackler RK (2004) Anatomy involved inthe jugular foramen approach for jugulotympanic paragangliomaresection. Neurosurg Focus 17:E6
15. Jackler RK (1996) Jugular foramen. In: Jackler RK (ed) Atlas ofneurotology and skull base surgery. Mosby, St. Louis, pp 131–156
16. Jackson CG (1993) The infratympanic extended facial recess ap-proach for anteriorly extensive middle ear disease: a conservationtechnique. Laryngoscope 103:451–454
17. Jackson CG, Cueva RA, Thedinger BA, Glasscock ME 3rd (1990)Conservation surgery for glomus jugulare tumors: the value of earlydiagnosis. Laryngoscope 100:1031–1036
18. Jackson CG, Glasscock ME 3rd, Nissen AJ, Schwaber MK (1982)Glomus tumor surgery: the approach, results, and problems.Otolaryngol Clin North Am 15:897–916
19. Jackson CG, Haynes DS, Walker PA et al (1996) Hearing conserva-tion in surgery for glomus jugulare tumors. Am J Otol 17:425–437
20. Kaylie DM, Wittkopf JE, Coppit G, Warren FM 3rd, NettervilleJL, Jackson CG (2006) Revision lateral skull base surgery. OtolNeurotol 27:225–233
Neurosurg Rev (2013) 36:579–586 585

21. Leonetti JP, Brackmann DE, Prass RL (1989) Improved preserva-tion of facial nerve function in the infratemporal approach to theskull base. Otolaryngol Head Neck Surg 101:74–78
22. Leonetti JP, Smith PG, Linthicum FH (1990) The petrous carotidartery: anatomic relationships in skull base surgery. OtolaryngolHead Neck Surg 102:3–12
23. Liu JK, Sameshima T, Gottfried ON, Couldwell WT, Fukushima T(2006) The combined transmastoid retro- and infralabyrinthine trans-jugular transcondylar transtubercular high cervical approach for resectionof glomus jugulare tumors. Neurosurgery 59:ONS115–ONS125
24. Lustig LR, Jackler RK (1996) The variable relationship betweenthe lower cranial nerves and jugular foramen tumors: implicationsfor neural preservation. Am J Otol 17:658–668
25. Makek M, Franklin DJ, Zhao JC, Fisch U (1990) Neural infiltra-tion of glomus temporale tumors. Am J Otol 11:1–5
26. Maniglia AJ, Sprecher RC, Megerian CA, Lanzieri C (1992) Inferiormastoidectomy–hypotympanic approach for surgical removal of glo-mus jugulare tumors: an anatomical and radiologic study emphasiz-ing distances between critical structures. Laryngoscope 102:407–414
27. Martin C, Prades JM (1992) Removal of selected infralabyrinthinelesions without facial nervemobilization. Skull Base Surg 2:220–226
28. Michael LM II, Robertson JH (2004) Glomus jugulare tumors: historicaloverview of the management of this disease. Neurosurg Focus 17:E1
29. Oghalai JS, Leung MK, Jackler RK, McDermott MW (2004)Transjugular craniotomy for the management of jugular foramentumors with intracranial extension. Otol Neurotol 25:570–579
30. Ozveren MF, Ture U, Ozek MM, Pamir MN (2003) Anatomiclandmarks of the glossopharyngeal nerve: a microsurgical anatom-ic study. Neurosurgery 52:1400–1410
31. Pensak ML, Jackler RK (1997) Removal of jugular foramen tumors:the fallopian bridge technique. Otolaryngol Head Neck Surg117:586–591
32. Patel SJ, Sekhar LN, Cass SP, Hirsch BE (1994) Combinedapproaches for resection of extensive glomus jugulare tumors. Areview of 12 cases. J Neurosurg 80:1026–1038
33. Pellet W, Cannoni M, Pech A (1988) The widened transcochlearapproach to jugular foramen tumors. J Neurosurg 69:887–894
34. Rhoton AL Jr (2000) Jugular foramen. Neurosurgery 47:S267–S28535. Rhoton AL Jr (2000) The temporal bone and transtemporal
approaches. Neurosurgery 47:S211–S26536. Sanna M, De Donato G, Piazza P, Falcioni M (2006) Revision
glomus tumor surgery. Otolaryngol Clin North Am 39:763–78237. Satar B, Yazar F, Ceyhan A, Arsian HH, Aydin S (2009) Analysis
of jugular foramen exposure in the fallopian bridge technique.Skull Base 19:203–207
Comments
Luis A. B. Borba, Curitiba, BrazilJean G. de Oliveira, São Paulo, Brazil
We read with great interest the article entitled “Less invasive transjugularapproach with fallopian-bridge for facial nerve protection and hearing pres-ervation in surgery of glomus jugulare tumors” by Nonaka et al.
First of all, we congratulate the authors for the results.In January 2010, we published our series of glomus jugulare tumors
which divides these tumors into four types (see reference 1 at the endof this comment). The technique described by Nonaka et al. is extreme-ly similar to our type B tumors.
Those classified as type A are tumors located in the jugular with orwithout intradural or neck extension but receive blood supply onlyfrom branches of the external carotid artery. For this type of tumors, werecommend the infralabyrinthine retrofacial approach without openingthe external auditory meatus and exposure of facial nerve. Hearing andfacial nerve function is preserved.
Type B tumors have a similar extension of the type A, but with bloodsupply also from the ICA, which requires a different approach. For typeB, a facial nerve is kept in its canal, and the tumor is removed anteriorlyand posteriorly to the facial canal. The control of carotid tympanicbranches from the ICA is crucial to remove the tumor. The externalauditory meatus and structures of the middle ear are not removed. In thistype, facial nerve function and hearing are preserved as well.
Some glomus jugulare tumors can grow anteriorly, encasing the ICAfrom the carotid canal to the cavernous sinus. For this situation, a moreanterior and superior approach is required. In the type C approach, theexternal auditory meatus and middle ear structures are removed to exposethe whole extension of the ICA in the petrous bone. In this approach, thefacial nerve is kept in place preserving its function. However, the hearing islost.
Glomus jugulare tumors can reach a very large size, sometimes debut-ing with facial nerve palsy, or the nerve can be totally encased andinfiltrated by the tumor. In this situation, we perform a type D approach.In this approach, the facial nerve is transposed for a new position in theparotid gland or decompressed, or even a nerve graft harvest using thegreat auricular nerve. A total petrosectomy is performed in these cases.
Some aspects are decisive in jugular foramen tumor (see references1 and 2 at the end of this comment):
(a) The preoperative evaluation must assess the hearing, facial, andlower cranial nerve functions.
(b) During the opening, begin to prepare the closure. That meansthat regional flaps with posterior temporal and sternocleidomastoidmuscles must be prepared to be used for closure.
(c) The blood supply of the tumor is paramount for the surgicaldecision-making process.
(d) In order to preserve the lower cranial nerve function, the anteriorwall of the jugular bulb must be preserved. Excessive coagulation inthis location must be avoided. The use of fibrin glue helps to stopvenous bleeding that originated from the inferior petrosal sinus, con-dylar vein, and anterior jugular branches.
(e) The extension of the surgical approach must be tailored case bycase. In several situations when we had planned a less aggressive boneremoval, we had to change during the surgery.
Finally, the authors should be congratulated by presenting theirexperience in dealing with glomus jugulars tumors.
References1. Borba LA, Araujo JC, de Oliveira JG, Filho MG, Moro MS,
Tirapelli LF, et al (2010) Surgical management of glomus jugulare tumors:a proposal for approach selection based on tumor relationships with thefacial nerve. J Neurosurg 112(1):88–98. PubMed PMID: 19425885.
2. Borba LA, Ale-Bark S, London C (2004) Surgical treatment ofglomus jugulare tumors without rerouting of the facial nerve: aninfralabyrinthine approach. Neurosurg Focus. 2004 17(2):E8. PubMedPMID: 15329023.
Giannantonio Spena, Brescia, ItalyThe paper by Nonaka et al. is well written and widely analyzes a
very specific and particular aspect of the surgical approach to thetumors of the glomus jugulare. This skull base team has an extendedexperience in treating these very complex tumors, and their attitude isfor sure to be shared since the goal to remove the tumor while limitingmorbidity is nowadays a must. As they stated, this approach hasalready been adopted by Jackler (Atlas of Skull Base and Neurotology,2008), but the use they do of it is clearly commendable.
Still, one point that must be emphasized is that such a dedicatedteam reached these results in a very long time span, demonstrating thededication and knowledge it needs to face these tumors.
The paper merits to be read by a large audience, and we hope thatthe readers not only will learn more about surgical techniques but alsowill be aware about the necessity to gradually approach this complexsurgery and pathology.
586 Neurosurg Rev (2013) 36:579–586