Embed Size (px)
Citation preview

Leukemia is characterized by hyperproliferation
of immature white blood cells
white blood cell
Leukemic patientnormal person
red blood cells
hyperproliferation of white blood cells

Wikipedia
To understand leukemia we need to examinedevelopment of the Hematopoietic System
myeloid lymphoid
self renewal
self renewal self renewal
granulocytes

Molecular Cell BiologyLodish et al. Fig. 24.1
Different types of leukemiaaffect different stem cell types and distinct stages intheir development

Chronic myelogenous leukemia (CML)
Annual incidence: 1/100,000 people(~15% of all leukemias)Median age: 30-60 yrs
Median survival: 4 yrs with conventional chemotherapy 6 yrs with aIFN therapy; allogeneic bone marrow transplantation may cure the patient

Chronic myelogenous leukemia (CML)
Arises in a particular bone marrow stem cell =The granulocyte precursor
Gives rise to neutrophils , basophils & megakaryocytes.
Neutrophils-- fight infection by phagocytosisBasophils-- release immune modulators, e.g., histamines, ProstaglandinsPlatelets- cell fragments of megakaryocytes.

Molecular Cell BiologyLodish et al. Fig. 24.1
CML arises in a stem cell that is
a granulocyte precursor

“The findings suggest a causal relationship between the chromosome abnormality observed and chronic granulocytic leukemia.”
Peter Nowell
1960 Nowell and Hungerford find that one copy of chromosome 22 is extremely short in CML patients

Nature 1973 243:290-3
“A new consistent chromosomal abnormality in CML identified by quinacrine fluorescence and Giemsa staining.”
Rowley JD.Janet Rowley in 1998
Upon receiving the Lasker Award

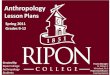
A chromosomal translocation triggers CML
Normal individual
Leukemic patient
Chr. 9
Chr. 22
9; 22 TranslocationThe Philadelphiachromosome

Karyotype courtesy of L. J. Beauregard,Eastern Maine Medical Center
A characteristic karyotype indicates CML

Acute lymphoblastic leukemia (ALL)
Affects precursor of leukocytes(B and T cells)
Ph+ chromosomes in 20% of adult ALL2-5% of childhood ALL
In adults prognosis very poor(Only 35- 40% of adults with ALL survive 2 years) Bone marrow transplant the only long term treatment

Table 4.5 The Biology of Cancer (© Garland Science 2007)
Chromosomal rearrangements are a hallmark of leukemia, being present in 70-90% of cases

Table 4.5 The Biology of Cancer (© Garland Science 2007)
Why is this the case?

Molecular Biology of the Cell Alberts et al
We cannot dedicate all 25,000 genes in the genome
just to make antibodies.
What’s the solution?
Put antibodies together by a mix-and match approach!

Molecular Biology of the Cell Alberts et al
requires rearranging the DNA

Molecular Biology of the Cell Alberts et al
requires rearranging the DNA

Molecular Biology of the Cell Alberts et al
The result:an antibody light chain

Since there are multiple types of each gene segment, there are thousands of possible V-D-J
combinations Each B cell gets a unique
combination

Since there are multiple types of each gene segment, there are thousands of possible V-D-J
combinations Each B cell gets a unique
combination

As we have seen, sometimes this goes wrong, and other genes are juxtaposed to the Ig or TCR genes

Rearrangement mistakes can also juxtapose Other genes with oncogenic consequences

The Philadelphia chromosome translocation fuses the bcr and abl genes
normal individual Leukemic patient
Chr. 9
Chr. 22abl
bcr Bcr-abl
9; 22 Translocationfuses Bcr and Abl
De Klein et al. Nature 300, 765 (1982)Groffen et al. Cell 36, 93 (1984)

Abelson was first identified as the oncogene carried by Abelson leukemia virus,
which causes pre-B cell Lymphoma in mice
Abelson and Rabstein, Cancer Res 30, 2213 (1970)

The v-abl containing
retrovirus was recovered
from a tumor found
in mice infected by
Moloney Leukemia virus

The Cell, G. Cooper, Fig. 15.25
In CML the translocation results in production of a fusion protein that joins
the amino-terminal end of the BCR proteinto most of the Abl protein

In fact, different breakpoints in bcrLead to slightly different Bcr-Abl fusion proteins
That are found in different cancers

Fluorescence In Situ Hybridization (FISH)a tool for diagnosing CML
abl bcr

fusion 9abl/bcr
fusion 22bcr/abl
ablbcr
Fluorescence In Situ Hybridization (FISH)a tool for diagnosing CML
BCR ABL
The current methd: PCR

Abelson kinase
• A fatty-acid modified and actin-binding
non-receptor tyrosine kinase
SH3F G
SH2
kinase
Actin-bindin
gMyristate

Abelson kinase
The front end looks a lot like Src!!
SH3F G
SH2
kinase
Actin-bindin
gMyristate

Oncogenic versions of Abelson
F GGag
Abl
v-ablSH3
F G
SH2
kinase
Actin-bindin
g
F GBcr
Bcr-Abl

What’s changed??
F GGag
Abl
v-ablSH3
F G
SH2
kinase
Actin-bindin
g
F GBcr
Bcr-Abl

Remember this?Src is normally inactive due tointramolecular inhibition

Nagar et al.Cell 112:859 (2003)
The structure of Abl reveals a novel mode of intramolecular inhibition

Harrison Cell 112, 737 (2003)
Src and AblDistinct yet analogous modes of regulation

Harrison Cell 112, 737 (2003)
A multistep mechanism for activating Src

Harrison Cell 112, 737 (2003)
A proposed mechanism for activating Abl

But what does Abl normally do?

Insights from the mouse model
• abl mutant mice are viable but runted and have a shortened lifespan They also have problems with: male fertility B cell maturation osteoblasts and bone formation
• Truncation of C-terminus leaving an intact kinase has same phenotype as the null mutant

Insights from the mouse model
• abl mutant mice are viable but runted and have a shortened lifespan They also have problems with: male fertility B cell maturation osteoblasts and bone formation
• Truncation of C-terminus leaving an intact kinase has same phenotype as the null mutant
Why so mild??

Abelson has a twin brother
SH3F G
SH2 kinaseActin-bindin
g
F G
89% 94% 27%34%
Abl
Arg

Are Abl and Arg redundant?• arg mutant mice have behavioral defects
(Arg is expressed in the brain at high levels)

Are Abl and Arg redundant?• arg mutant mice have behavioral defects
(Arg is expressed in the brain at high levels)
• abl; arg double mutants have defects in neural tube
Wild-type abl; arg

Focal adhesion proteins are phosphorylated by Abl (mediator of integrin signaling)

Abl phosphorylates regulators of the actin cytoskeleton

Of course it’s even more complicatedThan that!
Bradley and Koleske jcs.biologists.org/cgi/content/ full/122/19/3441/FIG3

Abl can also directly regulate
Cytoskeletal eventsUsing its
C-terminal region to bundle actin filaments
and Link them
to microtubules

But does this all help usunderstand and treat leukemia?
white blood cell
Leukemic patientnormal person
red blood cells
hyperproliferation of white blood cells

BCR-Abl
Cytoskeleton/adhesion defects
SG2
M
1GG0
Apoptosis
Stem cell turnover
Proliferation & differentiation
BCR-Abl affects multiple cell functions
Adapted from Jörgensen, 2001. Hem. Onc.

Abl may play roles in the nucleus in response to DNA damage
•ATM can phosphorylate Ablin response to DNA damage
•Abl may stabilize p53
Van Etten, TICB 9 179-186

To understand this, we must start by learning
more about the clinical progression of
CMLChronic phase
Median 5–6 years
stabilization
Accelerated phase
Median duration6–9 months
Blast crisis
Median survival3–6 months
Advanced phases
Provided by: Gleevec.com

Blast crisis is thought to involve additional
genetic changes that are only beginning
to be characterizedSuggested events:
•Mutations in p53
•MSI2/HOXA9 fusion protein
•AML1/EVI-1 fusion protein
•Ras mutations•Deletion of the Ikaros transcription factor

Therapy for CML: how do you evaluatewhether a drug is
working?
Hematologic Response Cytogenetic Response
– Complete: – Major:Normal peripheral blood count Complete: 0% Ph+
No immature cells Partial 1-35% Ph+
– Minor: 36%–95% Ph+
Modified from Gleevec.com

Therapeutic Options for CML
• Allogeneic stem cell transplantation (SCT)
• Interferon-alpha (IFN-)–based treatments
• Chemotherapy with hydroxyurea, busulfan
• Gleevec™ (imatinib mesylate, = STI571)
From Gleevec.com

Data of the Italian Cooperative Study group on Chronic Myeloid Leukemia. Blood 1998:92 1541–1548
Until recently interferon-alpha treatmentWas the gold-standard in CML
Even though its mechanism of action IS STILL NOT UNDERSTOOD
IFN=interferon-alpha, CHT= conventional chemotherapy

STI571
Gleevec blocks the ATP binding site of the kinase domain

Abl’sKinaseDomainIn complexWith theinhibitorGleevac
Kuriyan lab website

0
Months Since Start of Treatment
Chronic Phase CML1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.0
1 2 3 4 5 6 7 8 9 10
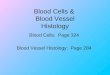
Fraction of patientsthat responded
Major cytogenetic response
Complete cytogeneticresponse
Data: Novartis Pharmaceuticals Corporation
QuickTime™ and aTIFF (Uncompressed) decompressorare needed to see this picture.
Gleevec™: in chronic phase CML

0
Months Since Start of Treatment
Chronic Phase CML1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.0
1 2 3 4 5 6 7 8 9 10
Fraction of patientsthat responded
Major cytogenetic response
Complete cytogeneticresponse
Data: Novartis Pharmaceuticals Corporation
QuickTime™ and aTIFF (Uncompressed) decompressorare needed to see this picture.
This is an awesome drug!Most patients survive
10+ years

Drug was discontinued for adverse events
in 1% of patients in chronic phase,
2% in accelerated phase,
and 5% in blast crisis
Of course there are side effects...

$40,000-50,000 per year!!
And the cost.....

“We now know of over 30 different mutations that can cause BCR-ABL to become resistant to imatinib,” says Dr. Charles Sawyers of UCLA’s Jonsson Cancer Center. In patientswith newly diagnosed disease, we are seeing resistance to imatinib in about 4%of patients per year. The further the disease has progressed before initiating imatinib treatment, the greater the chances are that resistance will arise.”
Unfortunately, natural selection is a powerful process

About 17% of all patients develop resistance in 5 years
Unfortunately, natural selection is a powerful process
Science 331: 1542-44 March 25 2011

A possible solution: a new generation of kinase inhibitors thatStill inhibit Gleevec-resistant tumors
Inject Luciferase-expressing tumor cells
Science 2004 305:399-401
aka Dasatinib

Dasatinib FDA approved for patients with relapses
Inject Luciferase-expressing tumor cells
NCI Cancer Bulletin October 5, 2006
aka Dasatinib

Dasatinib FDA approved for patients with relapsesNCI Cancer Bulletin October 5, 2006
Leads to 73% progression free survival for 3 years

Dasatinib FDA approved for patients with relapses
NCI Cancer Bulletin October 5, 2006
Phase II trials suggest Dasatinib effective in Blast-CrisisPatients with Gleevec-resistant tumors
NCI Cancer Bulletin May 2 2007
Phase II trials suggest Dasatinib effective in ALL patientswith Gleevec-resistant tumors
NCI Cancer Bulletin May 29 2007

This is becoming a general approach
Science 331: 1542-44 March 25 2011

How much do you think that costs?

For CML Add another $70,000/year!

Gleevec also has promise in other tumors
e.g., Gastrointestinal Stromal Tumors90% of malignant GISTs harbor a mutation in c-kit leading to KIT receptor autophosphorylation and ligand-independent activation
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
http://www.answers.com/topic/gist-2-jpg-1

Gleevec also has promise in other tumors
e.g., Gastrointestinal Stromal Tumors90% of malignant GISTs harbor a mutation in c-kit leading to KIT receptor autophosphorylation and ligand-independent activation
Does not respond to chemotherapy (<10% response)Only can be effectively treated if the entire tumorCan be removed surgicallyWithout this median survival 1-2 yrs

Report from the FDAApproval Summary: Imatinib Mesylate in the Treatmentof Metastatic and/or Unresectable MalignantGastrointestinal Stromal TumorsDagher et al. Clinical Cancer Research3034 3034–3038, October 2002
With Gleevec treatment ~50% of patients respondTumors shrink in size
and disease symptoms are greatly reduced
QuickTime™ and aTIFF (Uncompressed) decompressorare needed to see this picture.

April 17, 2008Gleevec treatment also reduces risk or recurrence
After surgical removal of GISTs
97% of patients treated with Gleevec had no recurrence after 1 yearVersus 83% of those receiving placebo
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.

GISTGleevecxtends median survival
from 15 months to 5 years

But.....Long term outcome ?
Many patients who initially respond developsecondary resistance to Gleevec and relapse
Cause: second site mutations in c-kit!

GISTLong term outcome ?
Many patients who initially respond developsecondary resistance to Gleevec and relapse
Cause: second site mutations in c-kit!
Approach: Develop new drugs targeted against c-kit
e.g., AMG706, SU11248
Current Oncology Reports (2005) 7: 293-299

An alternate approach: broader spectrum inhibitors that hit multiple targets
Sunitinib: targets Abl/PDGF Receptor, Src,and VEGF Receptor
NCI Cancer Bulletin Oct. 31 2006
FDA approved afterPhase III clinical trial reveal efficacy in GIST patients whoseTumors are resistant to GleevecQuickTime™ and a
TIFF (Uncompressed) decompressorare needed to see this picture.
George Demetri, MD