Embed Size (px)
Citation preview
Tiirkish Neiirosiirgery 8: 96 - 100, 1998 Berkiiiaii: Liiemiitte-Diicios Disease
Lhermitte-Duclos Disease
LhermiUe-Duclos Hastaligi
M. ZAFER BERKMAN, SAFAK ULUER, TURGUT DERINKÖK
SSK Okmeydani Hospital Department of Neurosurgery, Istanbul, Turkey
Abstract: Lhermitte-Duclos disease is a rare disorder
characterized by a slowly enlarging mass lesion in thecerebellum. A case of histopathologically confirmedLhermitte-Duclos disease is reported and our findings arediscussed.
Key Wards: Cerebellum, displastic gangliocytoma,Lhermitte-Duclos disease
INTRODUCTION
Lhermitte-Duclos disease, first described byLhermitte and Duclos in 1920 (1l), is a disease of
ra rely seen hamartamaous lesion mostly situatedwithin a cerebellar hemisphere, presenting withposterior fossa tumor findings most commonly inyoung and middle age adults (2-4,7,11,12,14,18,23,25).
Since the exact nature of the pathogenesis is notfully understood, different names have been givento this disease in literature. Gangliomatosis,dysplastic gangliocytoma, benign hypertrophy ofcerebellum, diffuse ganglioneuroma of cerebellarcortex, purkinjeoma, hamartoma of the cerebellum,neurocystic blastoma, hamartomablastoma,neurocytoma myelinicum, and gangliocytomamyelinicum diffusum are some of the other namesused for this disease (7,10,19,23,26).
We report a case with histopathologicallyproven dysplastic gangliocytoma in which the
96
Özet: Lhermitte-Duclos hastaligi serebellumda yavasbüyüyen kitle lezyonu ile karakterize patolojidir.Histopatolojik olarak dogrulanmis bir Lhermitte-Ducloshastaligi olgusu bildirilmis ve bulgularimiz tartisilmistir.
Anahtar Sözcükler: Displastik gangliositom, LhermitteDuclos hastaligi, serebellum
patient had undergone an operation with thediagnosis of posterior fossa tumor.
CASE REPORT
The patient was a 24-year-old female,complaining of headache, ataxia, and visualdisturbances in her right eye.
Her medical history revealed that she had 2thyroid operabons, the first four years ago, and thesecond one month ago, af ter which her complaintsbegan.
Neurological examination demonstrated poortandem gait with ataxia and deviation, dismetria,dysdiadochokinesia to the left side and bilateralpapilledema.
Skull x-ray films showed no pathologicalfindings. Computerized tomography (CT) revealeda mass lesi on in the left cerebellar hemisphere

Tiirkish Neiirosiirgen) 8: 96 - 100, 1998
extending to superior vermis leading to distortion inthe brain stern and the 4th ventric1e with the ventral
portion contrast-enhanced and resulting withtriventricular hydracephalus (Figure 1).
Figure 1. Preoperative CT shows a hypodense mass lesionin the left cerebellar hemisphere leading to thedistortion of the 4th ventriele and resulting inthe hydrocephalus and the ventromedial part ofthe lesion a dilated vascular structure.
Magnetic resonance imaging (MRI)demonstrated a lesion on the lateral side of the left
cerebellar hemisphere, nonhomogenous iso /hypointense in Tl weighted, hyperintense in T2weighted sections; exc1uding the peripheral vascularstructures, the parenchyma of the lesion was notcontrast-enhanced and its contours were not well
defined; the lesion compressed the rastral brain stemand the 4th ventric1e. There seemed a dila ted
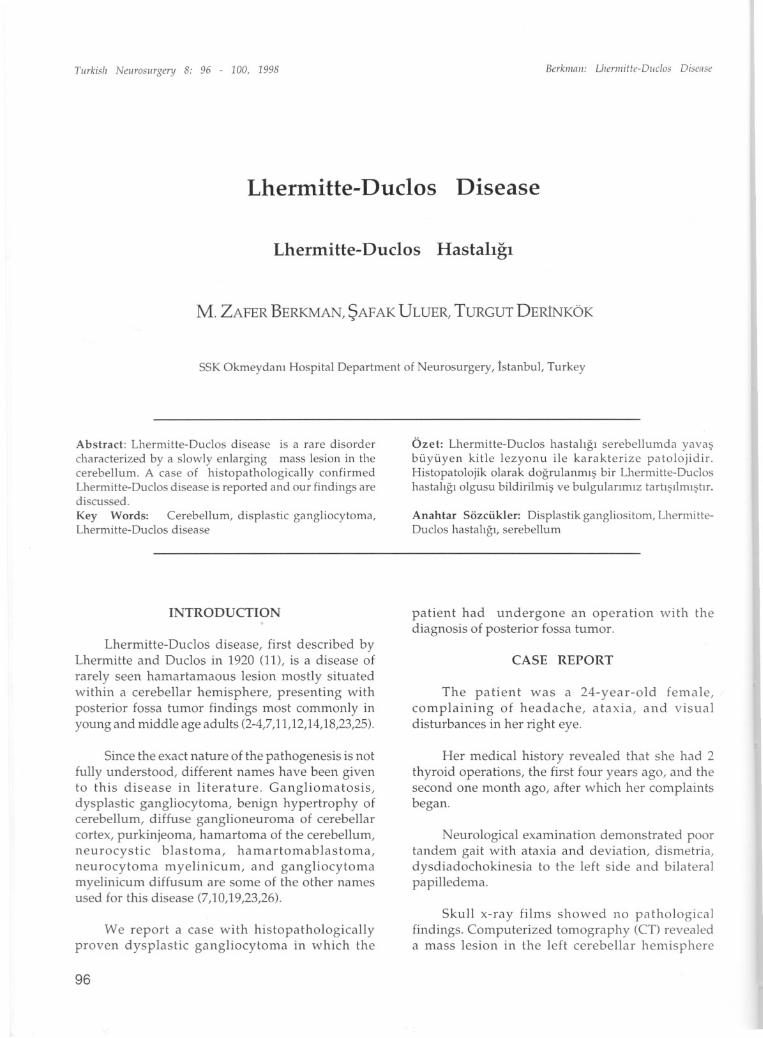
vascular structure on ventromedial part of the lesion;triventricu1ar hydrocephalus and a syringomyeliccavity measuring 15x7x7 mm in size extendingbetween C2-C3 levels could be seen (Figure 2).Vertebral angiography revealed a left cerebellarvenous angioma in the left inferior cerebellar region,in which radially located veins converged upwardsand drained into a broad venous structure
(Figure 3).
During surgery, at sitting position, suboccipitalcraniectomy and CL-C2-C3 laminectomy wereperformed. When dura was opened the enlarged leftcerebellar hemisphere was encountered. Just 1 cmbeneath the cortical surface, the tumoral tissue,
Berkiiinii: Uieniiille-Oiic/os Disen:,t'
Figure 2 a and b. MR! shows a lesion on the left cerebellarhemisphere localized laterally, hyperintense noncontrast enhanced and compressing theupperbrain stern and the 4th ventriele; and inthe ventromedial part of the lesion a dilatedvascular structure, triventricular hydrocephaly,and syringomyelic cavity extending between C2C3level.
occupying fully 1/3 lateral part of the cerebellarhemisphere, grayish in color, nonhaemorrhagic butinc1uding small vascular malformations and partlyaspiratable was found and totally excised. Thevenous angioma ventral to the tumor remaineduntouched. Then, applying a myelotomy, at C3 levelthe syringomyelic cavity was connected to thesubarachnoid space by placing a shunt connectar inbetween. Torkildsen shunting procedure was
97
Tiirkish Nelll'Oslirgery 8: 96 - 100, 1998
Figure 3. Vertebral angiography shows a cerebellar venousangioma in the left inferior cerebellar regionwhere radially extending veins convergeupwards and drain into a broad venousstructure.
performed for hydrocephaly and the dura was closedby duraplasty.
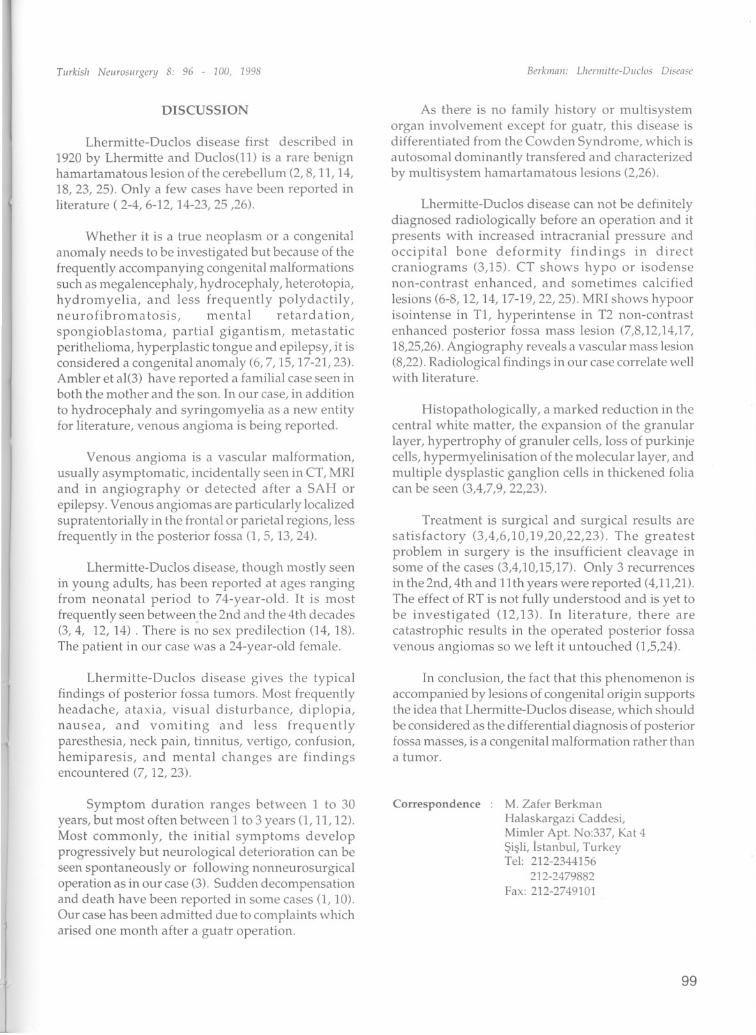
Histopathological examination revealedproliferated ganglion cells in the fibrillar stromai andvenous and arterial proliferated vascular formationsin the cerebellar tissue samples. No morphologicalfinding designating malignancy was observed.Diagnosis was confirmed dysplastic gangliocytomaand AVM ( Figure 4).
Figure 4. Histopathological fea tures of the lesionillustrating proliferated mature ganglion cells infibrillar stroma. H&Ex40.
98
Berkiiinii: L/ieniiifte-Diiclos Disease
She was well after the operation.
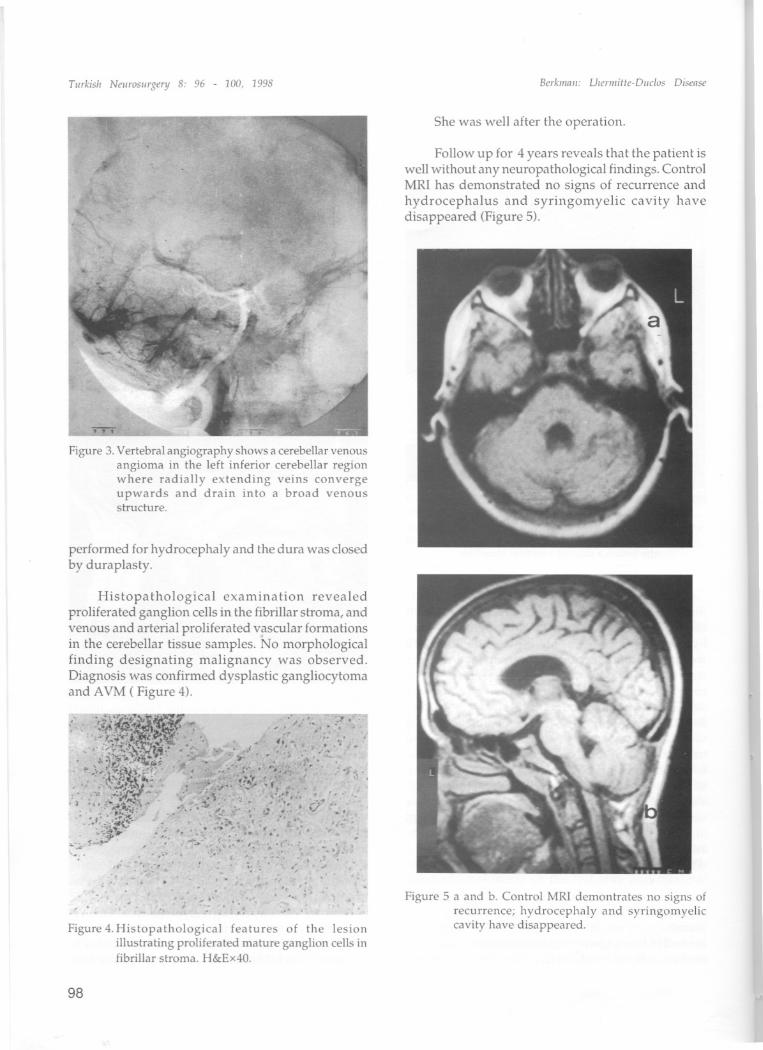
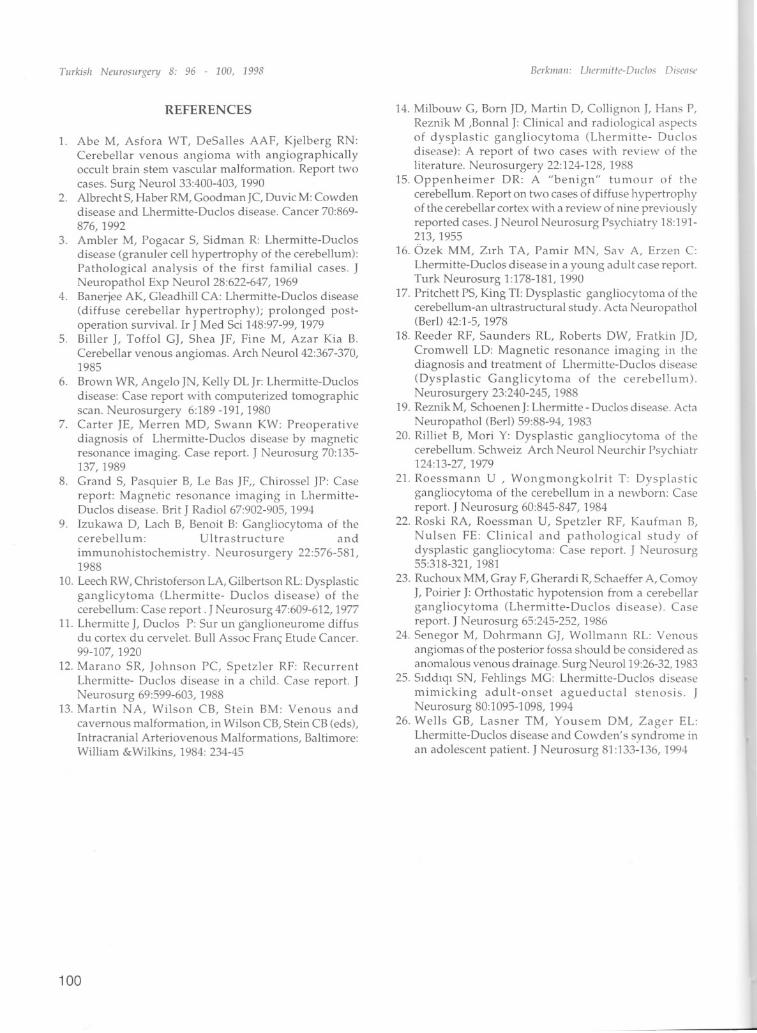
Follow up for 4 years reveals that the patient iswell without any neuropathological findings. ControlMRI has demonstrated no signs of recurrence andhydrocephalus and syringomyelic cavity havedisappeared (Figure 5).
Figure 5 a and b. Control MR! demontrates no signs ofrecurrence; hydrocephaly and syringomyeliccavity have disappeared.
Tiirkis'i Neiirosiirgery 8: 96 - 100, 1998
DISCUSSION
Lhermitte-Ouclos disease first described in
1920 by Lhermitte and Duclos(11) is a rare benignhamartamatous lesion of the cerebellum (2, 8, ll, 14,18,23, 25). Only a few cases have been reported inliterature ( 2-4, 6-12, 14-23, 25 ,26).
Whether it is a true neoplasm or a congenitalanomaly needs to be investigated but because of thefrequently accompanying congenital ma1formationssuch as megalencephaly, hydrocephaly, heterotopia,hydromyelia, and less frequently polydactily,neurofibromatosis, mental retardation,spongioblastoma, partial gigantism, metastaticperithelioma, hyperplastic tongue and epilepsy, it isconsidered a congenital anomaly (6,7, 15, 17-21,23).Ambler et a1(3) have reported a familial case seen inboth the mother and the son. In our case, in additionto hydrocephaly and syringomyelia as a new entityfor literature, venous angioma is being reported.
Venous angioma is a vascular ma1formation,usually asymptomatic, incidentally seen in CT, MRIand in angiography or detected af ter a SAH orepilepsy. Venous angiomas are particularly localizedsupratentorially in the frontal or pari etairegions, lessfrequently in the posterior fossa (1,5, 13,24).
Lhermitte-Ouclos disease, though mostly seenin young adults, has been reported at ages rangingfrom neonatal period to 74-year-old. it is mostfrequently seen between the 2nd and the 4th decades(3,4, 12, 14) . There is no sex predilection (14, 18).The patient in our case was a 24-year-old female.
Lhermitte-Ouclos disease gives the typicalfindings of posterior fossa tumorso Most frequentlyheadache, ataxia, visual disturbance, diplopia,nausea, and vomiting and less frequentlyparesthesia, neck pain, tinnitus, vertigo, confusion,hemiparesis, and mental changes are findingsencountered (7, 12,23).
Berkiiiiiii: Llieniiilte-Diic1os Diseiise
As there is no family history or multisystemorgan involvement except for guatr, this disease isdifferentiated from the Cowden Syndrome, which isautosomal dominantiy transfered and characterizedby multisystem hamartamatous lesions (2,26).
Lhermitte-Ouclos disease can not be definitelydiagnosed radiologically before an operation and itpresents with increased intracranial pressure andoccipital bone deformity findings in directcraniograms (3,15). CT shows hypo or isodensenon-contrast enhanced, and sometimes calcifiedlesions (6-8, 12, 14, 17-19,22,25). MRI shows hypoorisointense in Tl, hyperintense in T2 non-contrastenhanced posterior fossa mass lesion (7,8,12,14,17,18,25,26).Angiography reveals a vascular mass lesion(8,22).Radiological findings in our case correlate wellwith literature.
Histopathologically, a marked reduction in thecentral white matter, the expansion of the granularlayer, hypertrophy of granuler cells, loss of purkinjecells, hypermyelinisation of the molecular layer, andmultiple dysplastic ganglion cells in thickened foliacan be seen (3,4,7,9,22,23).
Treatment is surgical and surgical results aresatisfactory (3,4,6,10,19,20,22,23). The greatestproblem in surgery is the insufficient cleavage insome of the cases (3,4,10,15,17). Only 3 recurrencesin the 2nd, 4th and 11th years were reported (4,11,21).The effect of RT is not fully understood and is yet tobe investigated (12,13). In literature, there arecatastrophic results in the operated posterior fossavenous angiomas so we left it untouched (1,5,24).
In conclusion, the fact that this phenomenon isaccompanied by lesions of congenital origin supportsthe idea that Lhermitte-Ouclos disease, which shouldbe considered as the differential diagnosis of posteriorfossa masses, is a congenital malformation rather thana tumoT.
Symptom duration ranges between 1 to 30years, but most often between 1 to 3 years (1, ll, 12).Most commonly, the initial symptoms developprogressively but neurological deterioration can beseen spontaneously or following nonneurosurgicaloperation as in our case (3). Sudden decompensationand death have been reported in some cases (1, 10).Our case has been admitted due to complaints whicharised one month after a guatr operation.
Correspondence M. Zafer Berkman
Halaskargazi Caddesi,Mimler Apt. No:337, Kat 4Sisli, Istanbul, TurkeyTel: 212-2344156
212-2479882Fax: 212-2749101
99
Tiirkish Neiirvsiirgery 8: 96 - 100, 1998
REFERENCES
1. Abe M, Asfora WT, DeSalles AAF, Kjelberg RN:Cerebellar venous angioma with angiographicallyoccult brain stem vascular malformation. Report twocases. Surg NeuroI33:400-403, 1990
2. Albrecht S, Haber RM, Goodman JC, Duvic M: Cowdendisease and Lhermitte-Duclos disease. Cancer 70:869
876, 1992
3. Ambler M, Pogacar S, Sidman R: Lhermitte-Duclosdisease (granuler cel! hypertrophy of the cerebel!um):Pathological analysis of the first familial cases. JNeuropathol Exp NeuroI28:622-647, 1969
4. Banerjee AK, Gleadhil! CA: Lhermitte-Duclos disease(diffuse cerebellar hypertrophy); prolonged postoperation survival. Ir J Med Sci 148:97-99, 1979
5. Biller L Toffol GL Shea JF, Fine M, Azar Kia B.
Cerebel!ar venous angiomas. Arch NeuroI42:367-370,1985
6. Brown WR, Angelo JN, Kelly OL Jr: Lhermitte-Duclosdisease: Case report with computerized tomographicscan. Neurosurgery 6:189 -191, 1980
7. Carter JE, Merren MD, Swann KW: Preoperativediagnosis of Lhermitte-Duclos disease by magneticresonance imaging. Case report. J Neurosurg 70:135137, 1989
8. Grand S, Pasquier B, Le Bas JF" Chirossel JP: Casereport: Magnetic resonance imaging in LhermitteDuclos disease. Brit J Radiol 67:902-905, 1994
9. Izukawa D, Lach B, Benoit B: Gangliocytoma of thecerebellum: Ultrastructure and
immunohistochemistry. Neurosurgery 22:576-581,1988
10. Leech RW, Christoferson LA, Gilbertson RL: Dysplasticganglicytoma (Lhermitte- Duclos disease) of thecerebellum: Case report. J Neurosurg 47:609-612, 1977
11. Lhermitte J, Duclos P: Sur un ganglioneurome diffusdu cortex du cervelet. Bull Assoc Franç Etude Cancer.99-107, 1920
12. Marano SR, Johnson PC, Spetzler RF: RecurrentLhermitte- Duclos disease in a child. Case report. JNeurosurg 69:599-603, 1988
13. Martin NA, Wilson CB, Stein BM: Venous andcavernous malformation, in Wilson CB, Stein CB (eds),Intracranial Arteriovenous Malformations, Baltimore:William &Wilkins, 1984: 234-45
100
Berkiiinii: L/iel'lllifle-DIlc/os Disease
14. Milbouw G, Bom JD, Martin D, Collignon J, Hans P,Reznik M ,Bonn al J: Clinical and radiological aspectsof dysplastic gangliocytoma (Lhermitte- Duclosdisease): A report of two cases with review of theliterature. Neurosurgery 22:124-128, 1988
15.0ppenheimer DR: A "benign" tumour of thecerebellum. Report on two cases of diffuse hypertrophyof the cerebellar cortex with a review of nine previouslyreported cases. J Neurol Neurosurg Psychiatry 18:19'1213, 1955
16. Özek MM, Zirh TA, Pamir MN, Sav A, Erzen c:Lhermitte-Duclos disease in a young adult case report.Turk Neurosurg 1:178-181, 1990
17. Pritchett PS, King Tl: Dysplastic gangliocytoma of thecerebellum-an ultrastructural study. Acta Neuropathol(Berl) 42:1-5, 1978
18. Reeder RF, Saunders RL, Roberts DW, Fratkin JD,
Cromwell LO: Magnetic resonance imaging in thediagnosis and treatment of Lhermitte-Duclos disease(Dysplastic Ganglicytoma of the cerebellum).Neurosurgery 23:240-245, 1988
19. Reznik M, Schoenen J: Lhermitte - Duclos disease. Acta
Neuropathol (BerI) 59:88-94, 198320. Rilliet B, Mori Y: Dysplastic gangliocytoma of the
cerebellum. Schweiz Arch Neurol Neurchir Psychiatr124:13-27, 1979
21. Roessmann U , Wongmongkolrit T: Dysplasticgangliocytoma of the cerebellum in a newbom: Casereport. J Neurosurg 60:845-847, 1984
22. Roski RA, Roessman U, Spetzler RF, Kaufman B,Nulsen FE: Clinical and pathological study ofdysplastic gangliocytoma: Case report. J Neurosurg55:318-321, 1981
23. RllChoux MM, Gray F, Gherardi R, Schaeffer A, Com oyJ, Poirier J: Orthostatic hypotension from a cerebellargangliocytoma (Lhermitte-Duclos disease). Casereport. J Neiirosurg 65:245-252, 1986
24. Senegor M, Dohrmann GL Wollmann RL: Venülisangiomas of the posterior fossa should be considered asanomalous venous drainage. Surg NeiiroI19:26-32, 1983
25. Siddiqi SN, Fehlings MG: Lhermitte-Diiclos diseasemimicking adult-onset agiieductal stenosis. JNeurosurg 80:1095-1098, 1994
26. Wells GB, Lasner TM, Yousem DM, Zager EL:Lhermitte-Diiclos disease and Cowden's syndrome in
an adolescent patient. J Neurosurg 81:133~ 136, 199-l





























