Embed Size (px)
Citation preview

Page 1 LPFA(NB) 09/2016
Lifestyle Protector Risk New Business
APPLICATION NUMBER/S: Liberty – an Authorised Financial Services Provider Registration number 1957/002788/06
Checklist
The “Client Declaration and Consent” form, signed.
The “Declaration of Health – Living Lifestyle Dependant Protector Benefit” form, signed (if applicable).
The “Replacement Policy Advice Record” form, signed by both the financial adviser and policyholder (if applicable).
The “Self-Certification Declaration” form, signed (if applicable).

Page 2
POLICY INFORMATION
Policy details
Replacement of an existing policy Important Note: Replacement of any insurance may be to the disadvantage of the policyholder. Is this application to replace the whole or any part of your existing insurance with any insurer (whether replacement is to occur immediately or to replace an insurance discontinued within the past four months or within the next four months)? If “Yes”, the financial adviser must discuss and complete the Replacement Policy Advice Record and attach it to this application form.
Yes No
Policy language: English Afrikaans
Source (If not ordinary): Replacement Option Conversion
Group continuation option Member number Signature of policyholder
Lifestyle Protector plan details
REFER TO SIGNED QUOTE. Quote number
Financial adviser details and declaration (This section should be completed by the financial adviser)
(Not required if replacement policy effected as a result of the internet, telephone or direct marketing) I hereby declare that I have requested and recorded the policyholder's responses to the question with regard to replacement and that the policyholder is fully aware of the possible detrimental consequences of the replacement of an insurance policy. I further declare that, irrespective of the client’s response to this replacement question, I explained the following to the policyholder:
• The meaning of replacement, • That a replacement is potentially prejudicial, • The levying/deduction of a termination charge, and • That where a replacement is considered, the client is legally entitled to comprehensive information regarding the consequences of
replacement. Personal reference (internal)
Initials and surname Personal code % Split Liberty code Signature
Debit order details
Account type: Cheque/Current account Savings account Transmission
Debit date
Name of bank Account number
Branch code Branch name
Initial of account holder Surname/Company name
Addresses of policyholder/s
To be completed by the financial adviser: Do you confirm that these are the policyholder’s addresses? Yes No
Correspondence
Postal code
Residential
Postal code
Business
Postal code
Please select if the policyholder would prefer the summary policy document/documentation to be received via email? Yes No
If “Yes”, please confirm policyholder’s email address.
Page 3
FIRST LIFE ASSURED
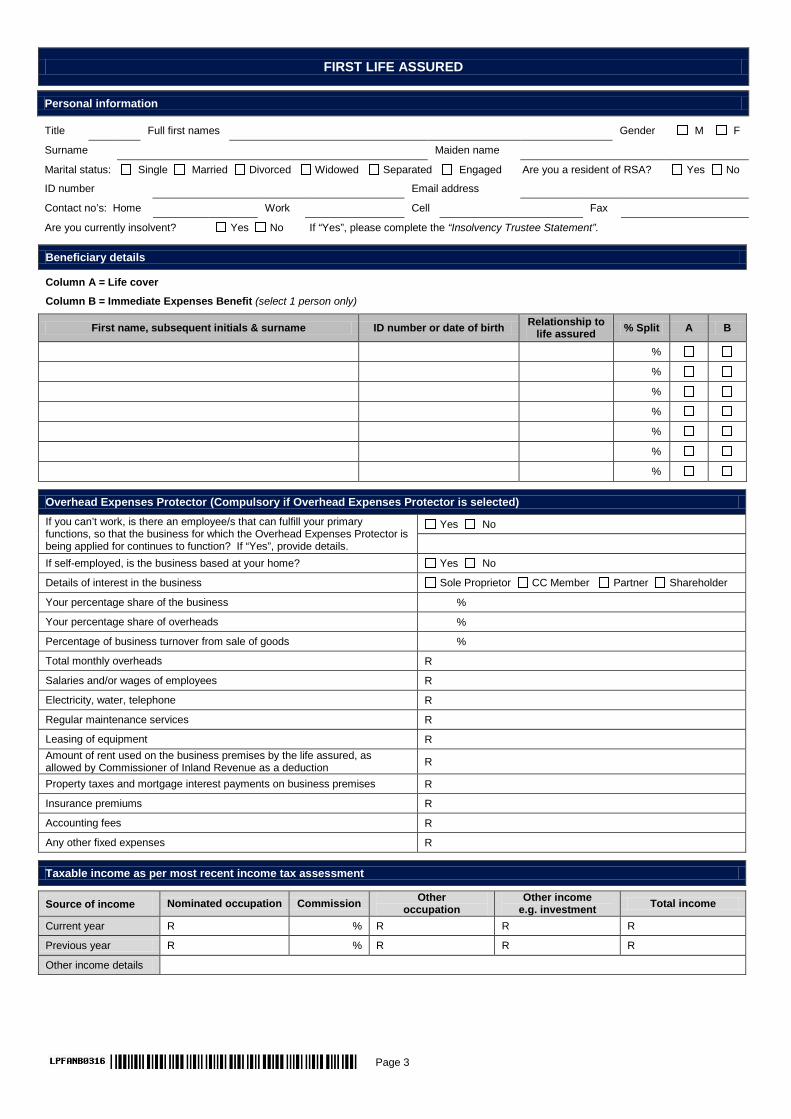
Personal information
Title Full first names Gender M F
Surname Maiden name
Marital status: Single Married Divorced Widowed Separated Engaged Are you a resident of RSA? Yes No
ID number Email address
Contact no’s: Home Work Cell Fax
Are you currently insolvent? Yes No If “Yes”, please complete the “Insolvency Trustee Statement”.
Beneficiary details
Column A = Life cover Column B = Immediate Expenses Benefit (select 1 person only)
First name, subsequent initials & surname ID number or date of birth Relationship to life assured % Split A B
%
%
%
%
%
%
%
Overhead Expenses Protector (Compulsory if Overhead Expenses Protector is selected)
If you can’t work, is there an employee/s that can fulfill your primary functions, so that the business for which the Overhead Expenses Protector is being applied for continues to function? If “Yes”, provide details.
Yes No
If self-employed, is the business based at your home? Yes No Details of interest in the business Sole Proprietor CC Member Partner Shareholder
Your percentage share of the business %
Your percentage share of overheads %
Percentage of business turnover from sale of goods %
Total monthly overheads R
Salaries and/or wages of employees R
Electricity, water, telephone R
Regular maintenance services R
Leasing of equipment R Amount of rent used on the business premises by the life assured, as allowed by Commissioner of Inland Revenue as a deduction R
Property taxes and mortgage interest payments on business premises R
Insurance premiums R
Accounting fees R
Any other fixed expenses R
Taxable income as per most recent income tax assessment
Source of income Nominated occupation Commission Other occupation
Other income e.g. investment Total income
Current year R % R R R
Previous year R % R R R
Other income details

Page 4
Income information for Income Protection benefits (To be completed when applying for Income Protection benefits)
Will you be insuring your Income Protector benefits using your: Pre-tax annual income* or Post-tax annual income** from your nominated occupation? Income amount R Proof of income to be provided at:*** Underwriting stage Claim stage Notes: * Pre-tax annual income
Salaried employees For salaried employees, pre-tax income is defined as the cost to company, earned for the last 12 months. This is the total cost to your employer and includes all benefits associated with employment except for the following: annual bonuses (including 13th cheques), ad-hoc bonuses, leave pay, merit award, share incentive awards, bonus/incentive amount paid to an employee to retain his/her service for a specified period. Self-employed individuals and partnerships Pre-tax income is defined as the share of the average monthly fees (and sales) earned, less the share of cost of sales, less the share of overhead expenses (where fees earned and costs incurred are shared on a pro-rata basis) earned over the last 12 months. Self-employed professionals For professionals that charge a fee for services, pre-tax income equals the average monthly sum of the professional fee and the net income from trading activities, after deducting business overheads expenses earned over the last 12 months.
For self-employed individuals, partnerships and professionals that provide proof of their income at the inception or reinstatement of the Income Protector benefit and whenever the sum assured is increased, Liberty will allow an increase to the pre-tax income by an amount of up to 20% of your share of monthly business expenses that will continue to be incurred in your personal capacity after a disability or permanent impairment event occurs. Expenses that are insured under any other insurance benefit that aims to cover business expenses on your disability may not be included. Personal expenses that are not related to business activities may not be included. Expenses that will not continue in your personal capacity after a disability or permanent impairment event occurs may not be included.
Pre-tax income excludes passive income that is not related to the income being generated for the occupation being insured e.g. dividends, rental income etc.
** Post-tax annual income Post-tax income is the pre-tax income defined above less the tax payable on taxable income receivable on account of the life assured’s
employment, or any services rendered by the life assured.
*** If proof of income is provided upfront at underwriting stage, proof of income will not be a requirement at claim stage.
Medical tests at your convenience
May Liberty contact you directly if additional medical information is required? Yes No Would you like a Liberty nurse to visit you to obtain medical requirements? Yes No If “Yes”, can you please specify the physical address where you would like to be consulted? Address Postal code
Contact number Alternate contact number Preferred time of contact: Morning 08:00-12:00 Afternoon 12:00-17:00 Any time
Medical attendant/s details
Please give the details of a doctor to who reasons for a health loading or results of blood tests including an HIV test may be sent.
Initials Surname Tel no. No. of years as a patient of this doctor
Address of doctor
Postal code
Height and weight details
Height (m) Weight (kg)
Underwriting (Only complete if you did not select tele-underwriting)
If any question is answered “Yes”, details must be given in the table supplied: Have you ever had trouble with, or disorders/disease of: 1. Your heart or circulation? Yes No 1.1 Angina 1.2 Angioplasty/Stent 1.3 Coronary artery bypass graft/CABG 1.4 Chest pain 1.5 Cholesterol raised 1.6 Coronary heart disease 1.7 Heart attack/Myocardial infarction 1.8 Heart murmur 1.9 Hypertension 1.10 Rheumatic fever 1.11 Varicose veins 1.12 Other conditions
2. Your lungs or other breathing problems (excluding colds, influenza)? Yes No 2.1 Asthma 2.2 Bronchitis 2.3 Persistent cough 2.4 Pneumonia 2.5 Tuberculosis 2.6 Other conditions
Page 5
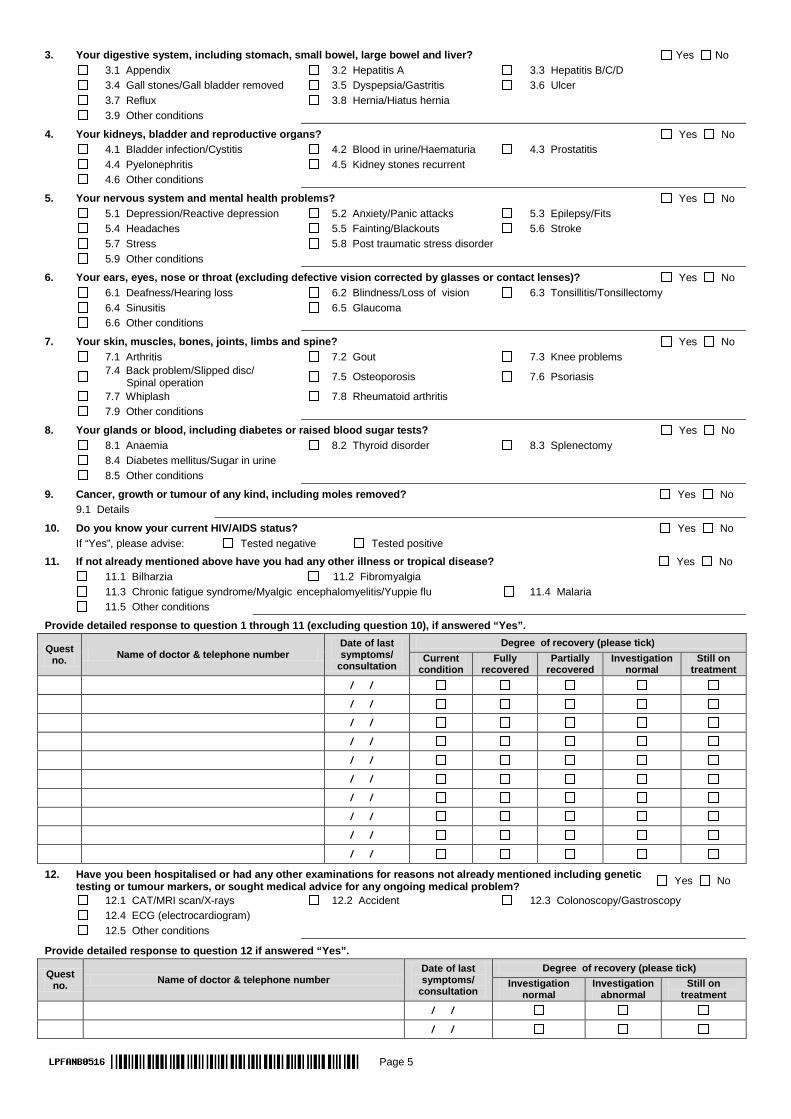
3. Your digestive system, including stomach, small bowel, large bowel and liver? Yes No 3.1 Appendix 3.2 Hepatitis A 3.3 Hepatitis B/C/D 3.4 Gall stones/Gall bladder removed 3.5 Dyspepsia/Gastritis 3.6 Ulcer 3.7 Reflux 3.8 Hernia/Hiatus hernia 3.9 Other conditions
4. Your kidneys, bladder and reproductive organs? Yes No 4.1 Bladder infection/Cystitis 4.2 Blood in urine/Haematuria 4.3 Prostatitis 4.4 Pyelonephritis 4.5 Kidney stones recurrent 4.6 Other conditions
5. Your nervous system and mental health problems? Yes No 5.1 Depression/Reactive depression 5.2 Anxiety/Panic attacks 5.3 Epilepsy/Fits 5.4 Headaches 5.5 Fainting/Blackouts 5.6 Stroke 5.7 Stress 5.8 Post traumatic stress disorder 5.9 Other conditions
6. Your ears, eyes, nose or throat (excluding defective vision corrected by glasses or contact lenses)? Yes No 6.1 Deafness/Hearing loss 6.2 Blindness/Loss of vision 6.3 Tonsillitis/Tonsillectomy 6.4 Sinusitis 6.5 Glaucoma 6.6 Other conditions
7. Your skin, muscles, bones, joints, limbs and spine? Yes No 7.1 Arthritis 7.2 Gout 7.3 Knee problems
7.4 Back problem/Slipped disc/ Spinal operation 7.5 Osteoporosis 7.6 Psoriasis
7.7 Whiplash 7.8 Rheumatoid arthritis 7.9 Other conditions
8. Your glands or blood, including diabetes or raised blood sugar tests? Yes No 8.1 Anaemia 8.2 Thyroid disorder 8.3 Splenectomy 8.4 Diabetes mellitus/Sugar in urine 8.5 Other conditions
9. Cancer, growth or tumour of any kind, including moles removed? Yes No 9.1 Details
10. Do you know your current HIV/AIDS status? Yes No If “Yes”, please advise: Tested negative Tested positive
11. If not already mentioned above have you had any other illness or tropical disease? Yes No 11.1 Bilharzia 11.2 Fibromyalgia 11.3 Chronic fatigue syndrome/Myalgic encephalomyelitis/Yuppie flu 11.4 Malaria 11.5 Other conditions
Provide detailed response to question 1 through 11 (excluding question 10), if answered “Yes”.
Quest no. Name of doctor & telephone number
Date of last symptoms/
consultation
Degree of recovery (please tick) Current
condition Fully
recovered Partially
recovered Investigation
normal Still on
treatment / / / / / / / / / / / / / / / / / / / /
12. Have you been hospitalised or had any other examinations for reasons not already mentioned including genetic testing or tumour markers, or sought medical advice for any ongoing medical problem? Yes No
12.1 CAT/MRI scan/X-rays 12.2 Accident 12.3 Colonoscopy/Gastroscopy 12.4 ECG (electrocardiogram) 12.5 Other conditions
Provide detailed response to question 12 if answered “Yes”.
Quest no. Name of doctor & telephone number
Date of last symptoms/
consultation
Degree of recovery (please tick) Investigation
normal Investigation
abnormal Still on
treatment / / / /

Page 6
13. Do you intend consulting a medical professional in the next 8 weeks, for any medical examinations or for conditions or symptoms not already disclosed, or is any future surgery planned? Yes No
13.1 Details
Provide detailed response to question 13 if answered “Yes”.
Quest no. Name of doctor & telephone number
Date of last symptoms/
consultation
Degree of recovery (please tick) Current
condition Fully
recovered Partially
recovered Investigation
normal Still on
treatment / / / / / / / /
14. Have you ever taken any recreational drugs including cannabis (dagga), cocaine, ecstasy, anabolic steroids, etc.? Yes No
14.1 Type of drugs
15. Has a proposal/application for life, health, dread disease, disability or functional impairment assurance ever been declined, deferred or accepted with certain provisions e.g. a higher premium, or with exclusions? Yes No
15.1 Details
16. Have you been medically boarded or have you submitted claims for disability or 3rd party benefits or have you been off work for a continuous period of more than a month in the last 3 years (excluding maternity leave)? Yes No
16.1 Details
17. Family history Do any of your relatives (mother, father, sister, brother) have or have they had any of the following medical conditions?
Yes No
Relationship with relative Age of diagnosis <45 ≥45 <45 ≥45 <45 ≥45 <45 ≥45 <45 ≥45 Current age/age at death Blood pressure/hypertension Cancer - breast Cancer - colon Cancer - ovarian Cancer - prostate Coronary artery disease (angina/thrombosis/ heart attack)
Diabetes/high blood sugar Haemophilia Haemochromatosis Huntington’s chorea Mental disorders/bipolar/schizophrenia/suicide Natural causes/old age Polycystic kidney disease Porphyria Cholesterol raised Stroke/Cerebro vascular accident Visual disorders/Retinitis Pigmentosa
18. For female applicants Any disorder of the female organs (breasts, ovaries, uterus) or any abnormality of pregnancy or confinement, dense breast tissue, lumps or cysts in the breasts or ovaries, hysterectomy, mammograms, pap smear?
Yes No
18.1 Conditions 18.2 Are you pregnant? Yes No If “Yes”, how many weeks? Provide detailed response to question 18 if answered “Yes”.
Name of doctor & telephone number Date of last symptoms/
consultation
Degree of recovery (please tick) Current
condition Fully
recovered Partially
recovered Investigation
normal Still on
treatment / / / / / / / /

Page 7
19. Avocations (sport, hobbies and pastimes) Have you participated in, do you currently participate in, or do you intend participating in any hazardous activity, hobby or pastime where there is a possible risk of accident or injury?
Yes No
19.1 Big game hunting 19.2 Aviation 19.3 Motor racing 19.4 Power boat racing 19.5 Parachuting/Skydiving 19.6 Underwater diving 19.7 Mountaineering/ Rock climbing 19.8 Other activities
Provide detailed response to question 19 if answered “Yes”.
Avocation Period and level of participation
Current Intends to Last 3 years More than 3 years ago
20. Have you ever been involved or implicated in any criminal activities or proceedings (excluding speeding fines)? If “Yes”, please provide details. Yes No
20.1 Details
Habits details
Non drinker Yes No If “No”, please complete alcohol consumption question.
Alcohol consumption: Spirits in tots Amount per week
Beer cider in cans/Bottles Amount per week
Wine in glasses Amount per week
Note: 1 bottle of spirits = 21 tots, 1 bottle of wine = 6 glasses. Have you ever received advice to reduce or discontinue alcohol consumption, or have you ever been charged with drunken driving? If “Yes”, please provide details. Yes No
Have you smoked or used tobacco products in the last 6 months? Yes No If a smoker, please indicate number per day: Cigarettes Cigars Pipe
Have you ever received advice to reduce or discontinue tobacco use? If “Yes”, please provide details. Yes No
Highest educational qualification
No matric Matric Technicon diploma Teachers college
diploma Undergraduate university degree Post-graduate
qualification
Occupation details
Self employed, fee based? Yes No Nominated Occupation
Other occupation Employer/Company name
Industry
Please indicate percentage of time spent in all duties: Admin % Supervisory % Manual % Travel %
Is there any hazard associated with your occupation e.g. mining, asbestos, handling of explosives, working at heights etc.? If “Yes”, please provide details: Yes No
Do you travel beyond the RSA borders in the course of your duties? If “Yes”, please specify countries, nature of duties and type of responsibilities. Yes No
Page 8
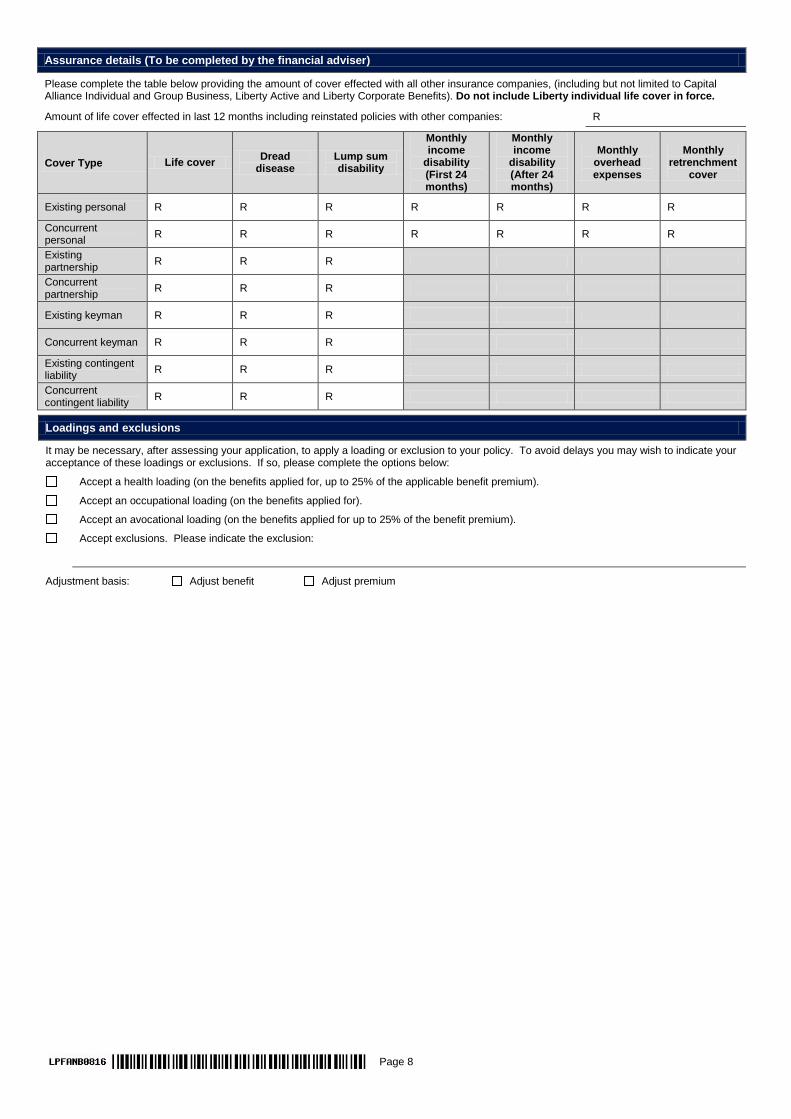
Assurance details (To be completed by the financial adviser)
Please complete the table below providing the amount of cover effected with all other insurance companies, (including but not limited to Capital Alliance Individual and Group Business, Liberty Active and Liberty Corporate Benefits). Do not include Liberty individual life cover in force.
Amount of life cover effected in last 12 months including reinstated policies with other companies: R
Cover Type Life cover Dread disease
Lump sum disability
Monthly income
disability (First 24 months)
Monthly income
disability (After 24 months)
Monthly overhead expenses
Monthly retrenchment
cover
Existing personal R R R R R R R Concurrent personal R R R R R R R Existing partnership R R R
Concurrent partnership R R R
Existing keyman R R R
Concurrent keyman R R R
Existing contingent liability R R R
Concurrent contingent liability R R R
Loadings and exclusions
It may be necessary, after assessing your application, to apply a loading or exclusion to your policy. To avoid delays you may wish to indicate your acceptance of these loadings or exclusions. If so, please complete the options below:
Accept a health loading (on the benefits applied for, up to 25% of the applicable benefit premium).
Accept an occupational loading (on the benefits applied for).
Accept an avocational loading (on the benefits applied for up to 25% of the benefit premium).
Accept exclusions. Please indicate the exclusion:
Adjustment basis: Adjust benefit Adjust premium

Page 9
SECOND/SPOUSE LIFE ASSURED
Personal information
Title Full first names Gender M F
Surname Maiden name
Marital status: Single Married Divorced Widowed Separated Engaged Are you a resident of RSA? Yes No
ID number Email address
Contact no’s: Home Work Cell Fax
Are you currently insolvent? Yes No If “Yes”, please complete the “Insolvency Trustee Statement”.
Beneficiary details
Column A = Life cover Column B = Immediate Expenses Benefit (select 1 person only)
First name, subsequent initials & surname ID number or date of birth Relationship to life assured % Split A B
%
%
%
%
%
%
%
Overhead Expenses Protector (Compulsory if Overhead Expenses Protector is selected)
If you can’t work, is there an employee/s that can fulfill your primary functions, so that the business for which the Overhead Expenses Protector is being applied for continues to function? If “Yes”, provide details.
Yes No
If self-employed, is the business based at your home? Yes No Details of interest in the business Sole Proprietor CC Member Partner Shareholder
Your percentage share of the business %
Your percentage share of overheads %
Percentage of business turnover from sale of goods %
Total monthly overheads R
Salaries and/or wages of employees R
Electricity, water, telephone R
Regular maintenance services R
Leasing of equipment R Amount of rent used on the business premises by the life assured, as allowed by Commissioner of Inland Revenue as a deduction R
Property taxes and mortgage interest payments on business premises R
Insurance premiums R
Accounting fees R
Any other fixed expenses R
Taxable income as per most recent income tax assessment
Source of income Nominated occupation Commission Other occupation
Other income e.g. investment Total income
Current year R % R R R
Previous year R % R R R
Other income details

Page 10
Income information for Income Protection benefits (To be completed when applying for Income Protection benefits)
Will you be insuring your Income Protector benefits using your: Pre-tax annual income* or Post-tax annual income** from your nominated occupation? Income amount R Proof of income to be provided at:*** Underwriting stage Claim stage Notes: * Pre-tax annual income
Salaried employees For salaried employees, pre-tax income is defined as the cost to company, earned for the last 12 months. This is the total cost to your employer and includes all benefits associated with employment, except for the following: annual bonuses (including 13th cheques), ad-hoc bonuses, leave pay, merit award, share incentive awards, bonus/incentive amount paid to an employee to retain his/her service for a specified period. Self-employed individuals and partnerships Pre-tax income is defined as the share of the average monthly fees (and sales) earned, less the share of cost of sales, less the share of overhead expenses (where fees earned and costs incurred are shared on a pro-rata basis) earned over the last 12 months. Self-employed professionals For professionals that charge a fee for services, pre-tax income equals the average monthly sum of the professional fee and the net income from trading activities, after deducting business overheads expenses earned over the last 12 months.
For self-employed individuals, partnerships and professionals that provide proof of their income at the inception or reinstatement of the Income Protector benefit and whenever the sum assured is increased, Liberty will allow an increase to the pre-tax income by an amount of up to 20% of your share of monthly business expenses that will continue to be incurred in your personal capacity after a disability or permanent impairment event occurs. Expenses that are insured under any other insurance benefit that aims to cover business expenses on your disability may not be included. Personal expenses that are not related to business activities may not be included. Expenses that will not continue in your personal capacity after a disability or permanent impairment event occurs may not be included.
Pre-tax income excludes passive income that is not related to the income being generated for the occupation being insured e.g. dividends, rental income etc.
** Post-tax annual income Post-tax income is the pre-tax income defined above less the tax payable on taxable income receivable on account of the life assured’s
employment, or any services rendered by the life assured.
*** If proof of income is provided upfront at underwriting stage, proof of income will not be a requirement at claim stage.
Medical tests at your convenience
May Liberty contact you directly if additional medical information is required? Yes No Would you like a Liberty nurse to visit you to obtain medical requirements? Yes No If “Yes”, can you please specify the physical address where you would like to be consulted? Address
Postal code
Contact number Alternate contact number Preferred time of contact: Morning 08:00-12:00 Afternoon 12:00-17:00 Any time
Medical attendant/s details
Please give the details of a doctor to who reasons for a health loading or results of blood tests including an HIV test may be sent.
Initials Surname Tel no. No. of years as a patient of this doctor
Address of doctor
Postal code
Height and weight details
Height (m) Weight (kg)
Underwriting (Only complete if you did not select tele-underwriting)
If any question is answered “Yes”, details must be given in the table supplied: Have you ever had trouble with, or disorders / disease of: 1. Your heart or circulation? Yes No 1.1 Angina 1.2 Angioplasty/Stent 1.3 Coronary artery bypass graft/CABG 1.4 Chest pain 1.5 Cholesterol raised 1.6 Coronary heart disease 1.7 Heart attack/Myocardial infarction 1.8 Heart murmur 1.9 Hypertension 1.10 Rheumatic fever 1.11 Varicose veins 1.12 Other conditions
2. Your lungs or other breathing problems (excluding colds, influenza)? Yes No 2.1 Asthma 2.2 Bronchitis 2.3 Persistent cough 2.4 Pneumonia 2.5 Tuberculosis 2.6 Other conditions
Page 11
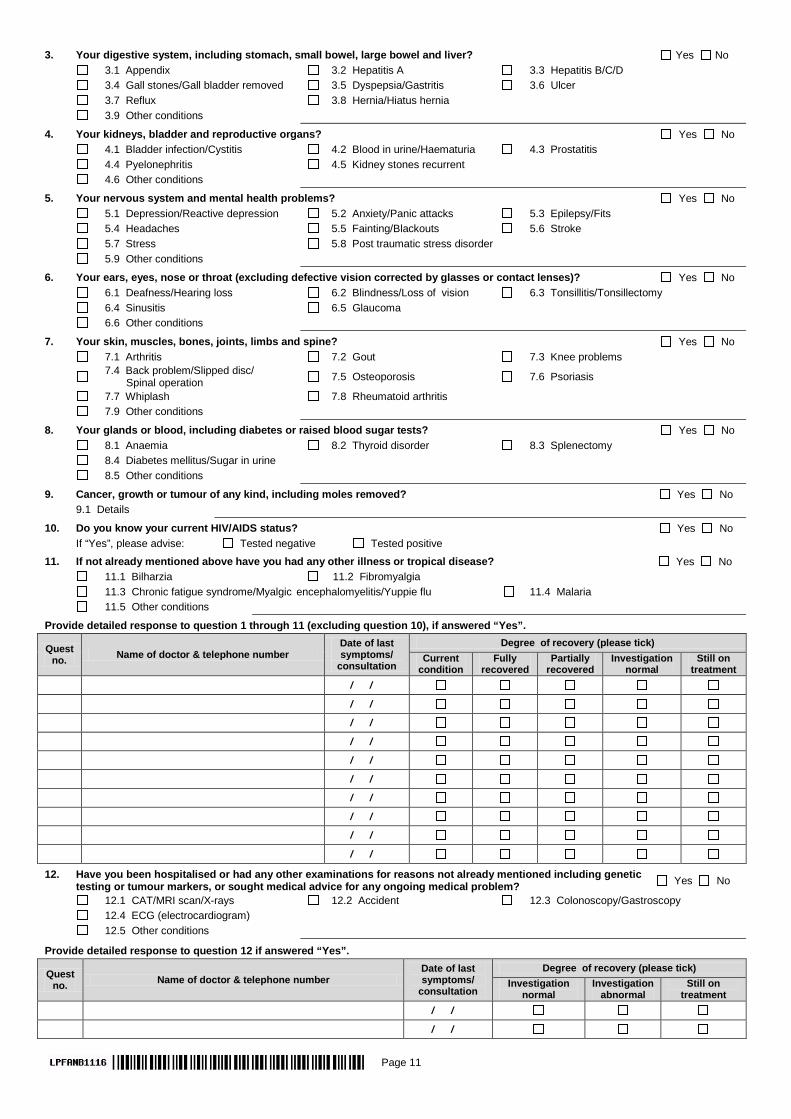
3. Your digestive system, including stomach, small bowel, large bowel and liver? Yes No 3.1 Appendix 3.2 Hepatitis A 3.3 Hepatitis B/C/D 3.4 Gall stones/Gall bladder removed 3.5 Dyspepsia/Gastritis 3.6 Ulcer 3.7 Reflux 3.8 Hernia/Hiatus hernia 3.9 Other conditions
4. Your kidneys, bladder and reproductive organs? Yes No 4.1 Bladder infection/Cystitis 4.2 Blood in urine/Haematuria 4.3 Prostatitis 4.4 Pyelonephritis 4.5 Kidney stones recurrent 4.6 Other conditions
5. Your nervous system and mental health problems? Yes No 5.1 Depression/Reactive depression 5.2 Anxiety/Panic attacks 5.3 Epilepsy/Fits 5.4 Headaches 5.5 Fainting/Blackouts 5.6 Stroke 5.7 Stress 5.8 Post traumatic stress disorder 5.9 Other conditions
6. Your ears, eyes, nose or throat (excluding defective vision corrected by glasses or contact lenses)? Yes No 6.1 Deafness/Hearing loss 6.2 Blindness/Loss of vision 6.3 Tonsillitis/Tonsillectomy 6.4 Sinusitis 6.5 Glaucoma 6.6 Other conditions
7. Your skin, muscles, bones, joints, limbs and spine? Yes No 7.1 Arthritis 7.2 Gout 7.3 Knee problems
7.4 Back problem/Slipped disc/ Spinal operation 7.5 Osteoporosis 7.6 Psoriasis
7.7 Whiplash 7.8 Rheumatoid arthritis 7.9 Other conditions
8. Your glands or blood, including diabetes or raised blood sugar tests? Yes No 8.1 Anaemia 8.2 Thyroid disorder 8.3 Splenectomy 8.4 Diabetes mellitus/Sugar in urine 8.5 Other conditions
9. Cancer, growth or tumour of any kind, including moles removed? Yes No 9.1 Details
10. Do you know your current HIV/AIDS status? Yes No If “Yes”, please advise: Tested negative Tested positive
11. If not already mentioned above have you had any other illness or tropical disease? Yes No 11.1 Bilharzia 11.2 Fibromyalgia 11.3 Chronic fatigue syndrome/Myalgic encephalomyelitis/Yuppie flu 11.4 Malaria 11.5 Other conditions
Provide detailed response to question 1 through 11 (excluding question 10), if answered “Yes”.
Quest no. Name of doctor & telephone number
Date of last symptoms/
consultation
Degree of recovery (please tick) Current
condition Fully
recovered Partially
recovered Investigation
normal Still on
treatment / / / / / / / / / / / / / / / / / / / /
12. Have you been hospitalised or had any other examinations for reasons not already mentioned including genetic testing or tumour markers, or sought medical advice for any ongoing medical problem? Yes No
12.1 CAT/MRI scan/X-rays 12.2 Accident 12.3 Colonoscopy/Gastroscopy 12.4 ECG (electrocardiogram) 12.5 Other conditions
Provide detailed response to question 12 if answered “Yes”.
Quest no. Name of doctor & telephone number
Date of last symptoms/
consultation
Degree of recovery (please tick) Investigation
normal Investigation
abnormal Still on
treatment / / / /

Page 12
13. Do you intend consulting a medical professional in the next 8 weeks, for any medical examinations or for conditions or symptoms not already disclosed, or is any future surgery planned? Yes No
13.1 Details
Provide detailed response to question 13 if answered “Yes”.
Quest no. Name of doctor & telephone number
Date of last symptoms/
consultation
Degree of recovery (please tick) Current
condition Fully
recovered Partially
recovered Investigation
normal Still on
treatment / / / / / / / /
14. Have you ever taken any recreational drugs including cannabis (dagga), cocaine, ecstasy, anabolic steroids, etc.? Yes No
14.1 Type of drugs
15. Has a proposal/application for life, health, dread disease, disability or functional impairment assurance ever been declined, deferred or accepted with certain provisions e.g. a higher premium, or with exclusions? Yes No
15.1 Details
16. Have you been medically boarded or have you submitted claims for disability or 3rd party benefits or have you been off work for a continuous period of more than a month in the last 3 years (excluding maternity leave)? Yes No
16.1 Details
17. Family history Do any of your relatives (mother, father, sister, brother) have or have they had any of the following medical conditions?
Yes No
Relationship with relative Age of diagnosis <45 ≥45 <45 ≥45 <45 ≥45 <45 ≥45 <45 ≥45 Current age/age at death Blood pressure/hypertension Cancer - breast Cancer - colon Cancer - ovarian Cancer - prostate Coronary artery disease (angina/thrombosis/ heart attack)
Diabetes/high blood sugar Haemophilia Haemochromatosis Huntington’s chorea Mental disorders/bipolar/schizophrenia/suicide Natural causes/old age Polycystic kidney disease Porphyria Cholesterol raised Stroke/Cerebro vascular accident Visual disorders/Retinitis Pigmentosa
18. For female applicants Any disorder of the female organs (breasts, ovaries, uterus) or any abnormality of pregnancy or confinement, dense breast tissue, lumps or cysts in the breasts or ovaries, hysterectomy, mammograms, pap smear?
Yes No
18.1 Conditions 18.2 Are you pregnant? Yes No If “Yes”, how many weeks?
Provide detailed response to question 18 if answered “Yes”.
Name of doctor & telephone number Date of last symptoms/
consultation
Degree of recovery (please tick) Current
condition Fully
recovered Partially
recovered Investigation
normal Still on
treatment / / / / / / / /
Page 13
19. Avocations (sport, hobbies and pastimes) Have you participated in, do you currently participate in, or do you intend participating in any hazardous activity, hobby or pastime where there is a possible risk of accident or injury?
Yes No
19.1 Big game hunting 19.2 Aviation 19.3 Motor racing 19.4 Power boat racing 19.5 Parachuting/Skydiving 19.6 Underwater diving 19.7 Mountaineering/ Rock climbing 19.8 Other activities
Provide detailed response to question 19 if answered “Yes”.
Avocation Period and level of participation
Current Intends to Last 3 years More than 3 years ago
20. Have you ever been involved or implicated in any criminal activities or proceedings (excluding speeding fines)? If “Yes”, please provide details. Yes No
20.1 Details
Habits details
Non drinker Yes No If “No”, please complete alcohol consumption question.
Alcohol consumption: Spirits in tots Amount per week
Beer cider in cans/Bottles Amount per week
Wine in glasses Amount per week
Note: 1 bottle of spirits = 21 tots, 1 bottle of wine = 6 glasses. Have you ever received advice to reduce or discontinue alcohol consumption, or have you ever been charged with drunken driving? If “Yes”, please provide details. Yes No
Have you smoked or used tobacco products in the last 6 months? Yes No If a smoker, please indicate number per day: Cigarettes Cigars Pipe
Have you ever received advice to reduce or discontinue tobacco use? If “Yes”, please provide details. Yes No
Highest educational qualification
No matric Matric Technicon diploma Teachers college
diploma Undergraduate university degree Post-graduate
qualification
Occupation details
Self employed, fee based? Yes No Nominated occupation
Other occupation Employer/Company name
Industry
Please indicate percentage of time spent in all duties: Admin % Supervisory % Manual % Travel %
Is there any hazard associated with your occupation e.g. mining, asbestos, handling of explosives, working at heights etc.? If “Yes”, please provide details: Yes No
Do you travel beyond the RSA borders in the course of your duties? If “Yes”, please specify countries, nature of duties and type of responsibilities. Yes No
Page 14
Assurance details (To be completed by the financial adviser)
Please complete the table below providing the amount of cover effected with all other insurance companies, (including but not limited to Capital Alliance Individual and Group Business, Liberty Active and Liberty Corporate Benefits). Do not include Liberty individual life cover in force.
Amount of life cover effected in last 12 months including reinstated policies with other companies: R
Cover Type Life cover Dread disease
Lump sum disability
Monthly income
disability (First 24 months)
Monthly income
disability (After 24 months)
Monthly overhead expenses
Monthly retrenchment
cover
Existing personal R R R R R R R Concurrent personal R R R R R R R Existing partnership R R R
Concurrent partnership R R R
Existing keyman R R R
Concurrent keyman R R R
Existing contingent liability R R R
Concurrent contingent liability R R R
Loadings and exclusions
It may be necessary, after assessing your application, to apply a loading or exclusion to your policy. To avoid delays you may wish to indicate your acceptance of these loadings or exclusions. If so, please complete the options below:
Accept a health loading (on the benefits applied for, up to 25% of the applicable benefit premium).
Accept an occupational loading (on the benefits applied for).
Accept an avocational loading (on the benefits applied for up to 25% of the benefit premium).
Accept exclusions. Please indicate the exclusion:
Adjustment basis: Adjust benefit Adjust premium
CHILD LIFE ASSURED
Child lives (Maximum number of children per benefit is 16)
Column A = Child Living Lifestyle Column B = Hospitalisation Lifestyle Enhancer Column C = EduCator
Please indicate the institution type (in column C) P = Public I = Independent
Assured Full first names Surname ID Number Date of birth A B C Gender M F
Child 1 / /
Child 2 / /
Child 3 / /
Child 4 / /
Child 5 / /
Child 6 / /
Child 7 / /
Child 8 / /
Should the number of children per benefit exceed 8, please insert page with additional child lives. Note: Addendum needs to be signed by all relevant parties.

Page 15
POLICYHOLDER
Policyholder details (Only the policyholder can act on the policy and make changes to the policy)
Company/Trust name Company registration number
Insurable interest/Reason for assurance
Company/Employer owned policy? Yes No If “Yes”, do you wish to claim an s11(w)(ii) deduction on the premium? Yes No
Tax Status of policyholder: Tax-exempt body Tax paying body Tax paying trust
Non-tax paying trust Company/Close Corporation Natural person
Is the entity organised, incorporated or resident for tax purposes outside of South Africa and/or does a foreign person/entity have an equity interest in or exercise control over the entity? If “Yes”, please complete the “Self-Certification Declaration for an Entity” form.
Yes No
Policyholder 1
Title Full first names
Surname Maiden name
Marital status: Single Married Divorced Widowed Separated Engaged Gender M F
Email address Date of birth / /
ID/passport number Country of issue
Contact no’s: Home Work Cell Fax
Are you a resident of RSA? Yes No Income tax number
Are you currently insolvent? Yes No If “Yes”, please complete the “Insolvency Trustee Statement”.
Are you a foreign citizen and/or have dual nationality and/or are you resident for tax purposes anywhere other than South Africa? If “Yes”, please complete the “Self-Certification Declaration for an Individual” form. Yes No
Policyholder 2
Title Full first names
Surname Maiden name
Marital status: Single Married Divorced Widowed Separated Engaged Gender M F
Email address Date of birth / /
ID/passport number Country of issue
Contact no’s: Home Work Cell Fax
Are you a resident of RSA? Yes No Income tax number
Are you currently insolvent? Yes No If “Yes”, please complete the “Insolvency Trustee Statement”.
Are you a foreign citizen and/or have dual nationality and/or are you resident for tax purposes anywhere other than South Africa? If “Yes”, please complete the “Self-Certification Declaration for an Individual” form. Yes No
Policyholder 3
Title Full first names
Surname Maiden name
Marital status: Single Married Divorced Widowed Separated Engaged Gender M F
Email address Date of birth / /
ID/passport number Country of issue
Contact no’s: Home Work Cell Fax
Are you a resident of RSA? Yes No Income tax number
Are you currently insolvent? Yes No If “Yes”, please complete the “Insolvency Trustee Statement”.
Are you a foreign citizen and/or have dual nationality and/or are you resident for tax purposes anywhere other than South Africa? If “Yes”, please complete the “Self-Certification Declaration for an Individual” form. Yes No

Page 16
Policyholder 4
Title Full first names
Surname Maiden name
Marital status: Single Married Divorced Widowed Separated Engaged Gender M F
Email address Date of birth / /
ID/passport number Country of issue
Contact no’s: Home Work Cell Fax
Are you a resident of RSA? Yes No Income tax number
Are you currently insolvent? Yes No If “Yes”, please complete the “Insolvency Trustee Statement”.
Are you a foreign citizen and/or have dual nationality and/or are you resident for tax purposes anywhere other than South Africa? If “Yes”, please complete the “Self-Certification Declaration for an Individual” form. Yes No
Policyholder 5
Title Full first names
Surname Maiden name
Marital status: Single Married Divorced Widowed Separated Engaged Gender M F
Email address Date of birth / /
ID/passport number Country of issue
Contact no’s: Home Work Cell Fax
Are you a resident of RSA? Yes No Income tax number
Are you currently insolvent? Yes No If “Yes”, please complete the “Insolvency Trustee Statement”.
Are you a foreign citizen and/or have dual nationality and/or are you resident for tax purposes anywhere other than South Africa? If “Yes”, please complete the “Self-Certification Declaration for an Individual” form. Yes No
Signatures
Signed at on / /
First life assured/Policyholder Second/Spouse life assured
Policyholder (if different from first life assured) Policyholder 2
Policyholder 3 Policyholder 4
Policyholder 5 Signature of payer life/account holder (if different from policyholder)
DECLARATION OF HEALTH LIVING LIFESTYLE DEPENDANT PROTECTOR BENEFIT
Page 17
POLICY NUMBER
1. If Living Lifestyle Dependant Protector benefit has been applied for, please complete this form using a black pen once you have read and understood the contents on this form.
2. Please fax/email ONLY this page to any one of the following entry points: • Fax: +27 (0)11 408 4235/4533 • Email: [email protected]
Assured First name & initials Relationship Surname if different to life assured Date of birth ID Number
Spouse / /
Child dependant / /
Child dependant / /
Child dependant / /
The definition of child and spouse are as follows: • “Child” means the life assured’s own child, legally adopted child or stepchild. The child must be unmarried. • “Spouse” includes the person you are legally married to either by civil or customary law, by civil union, by Asiatic religion or the person whom
you are in the same sex or heterosexual cohabiting relationship with. I, the life assured declare that the following statements are true and correct and will form part of my application for the Living Lifestyle Dependant Protector benefit. • That my spouse or child dependant(s) mentioned above meet the definition of “Spouse” and/or “Child” as defined above.
• Neither my spouse nor child dependant(s) suffers from, have ever been diagnosed with or have been investigated for genetic or congenital abnormalities, nor are any of them expecting to be tested for such abnormalities in future.
• Neither my spouse nor child dependant(s) has ever made an application to any life assurer or medical aid where the application was declined, deferred or accepted on special medical terms.
• Neither my spouse nor child dependant(s) are currently experiencing any symptoms which may prompt them to seek medical advice within the next six months, nor do my spouse or child dependant(s) currently receive regular medical care (including the use of chronic medication) for any medical condition.
• Neither my spouse nor child dependant(s) have ever submitted any claim to Liberty or any other Life Office.
• There are no other circumstances not mentioned above which may predispose my spouse or child dependant(s) to hospitalisation, surgical procedures or other medical treatment.
Furthermore, I, the life assured understand:
That no claim will be admitted on the Living Lifestyle Dependant Protector benefit where in the opinion of Liberty’s Chief Medical Officer (CMO) the condition was present at the inception of the benefit or where the condition is in any way related to conditions which are diagnosed before the inception of the benefit.
Signature of policyholder (owner) Date
Signature of first life assured Date
Signature of second/spouse life assured Date
Signature of payer Date
CLIENT DECLARATION AND CONSENT
Page 18
Policy number:
1. Please complete this form using a black pen once you have read and understood the contents on this form. 2. Please fax/email both pages to any one of the following entry points:
• Fax: +27 (0)11 408 4171 • Email: [email protected] Your personal information We need to collect and process some of your personal information in terms of various laws to provide products or services to you. As this information
forms the basis of our assessment and terms we offer you, it must be correct, complete and up to date. If any information you give us is wrong,
incomplete or outdated, we may cancel your policy or decline a future claim. We will comply with all relevant regulations in dealing with your
information and keep it secure and confidential at all times.
In terms of the Protection of Personal Information Act we are required to:
• Keep your information secure, confidential and only for as long as required.
• Only process information as permitted by law.
• Provide you with access to update or rectify any of your information.
• Notify you if any of your information has been compromised Authorisation to share and process information You hereby authorise us, our financial advisers and our service providers, as long as required and potentially after your death, to:
• Collect any personal, medical, financial and other information about you directly from all available internal and external sources (including specifically your medical scheme and/or pathology laboratory);
• For external sources, you agree that this authorisation is considered a legally binding personal instruction to the parties concerned to provide
any relevant information requested directly to us; and
• Process and share this information internally and externally only as required in order to assess risks, provide terms, service your product, consider claims and conduct research.
Notes:
• “Potentially relevant information” includes information about your lifestyle, financial status, health, occupation and hobbies amongst others
and spans a variety of potential sources, but specifically includes claims records from medical schemes, results of pathology and other blood
tests conducted and details on prescription drug usage.
• “Personal Information” includes race, gender, nationality, marital status, age, physical or mental health, disability, language, education, identity number, telephone number, email, postal address, biometric information, and financial, criminal or employment history as defined in the
Protection of Personal Information Act.
• “We” refers to Liberty Holdings Limited and all its subsidiaries.

Page 19
Your signature below is a confirmation that you have read, understood and agreed to the terms in this “Client Declaration and Consent”.
Please complete all details below for your applicable role:
Role
Liberty can share your Personal Information:
Signature Date Within the Liberty Group for marketing purposes and special offers?
With registered banks for marketing purposes and special offers?
With certain specially selected third parties for marketing purposes only?
First life assured/ Policyholder
Yes No Yes No Yes No
Full name ID/Registration no.
Second/Spouse life assured
Yes No Yes No Yes No
Full name ID/Registration no.
Policyholder (if different from first life assured)
Yes No Yes No Yes No
Full name ID/Registration no.
Policyholder 2 Yes No Yes No Yes No
Full name ID/Registration no.
Policyholder 3 Yes No Yes No Yes No
Full name ID/Registration no.
Policyholder 4 Yes No Yes No Yes No
Full name ID/Registration no.
Policyholder 5 Yes No Yes No Yes No
Full name ID/Registration no.
Payer life/ account holder (if different from policyholder)
Yes No Yes No Yes No
Full name ID/Registration no. If you in the future change your mind about any of the above please notify Liberty through your financial adviser or directly at 0860 456 789 or [email protected].
Do not sign blank or incomplete application forms. In order to avoid any claim being repudiated due to “Non-Disclosure” it is vital that all risks (medical, financial, occupation, hobbies, or legal) are fully disclosed to ensure full underwriting assessment, so the appropriate
decision on your application can be made. Please note that in the event of any modification of this form Liberty will regard this application as being invalid.
REPLACEMENT POLICY ADVICE RECORD (RPAR)
Page 20
To be completed in consultation with your representative – please note that this does not serve as a cancellation of the replaced policy; you must advise the insurer in writing about the cancellation of a policy. Name and surname of policyholder
ID number of policyholder (or registration number in the case of juristic persons)
Name and surname of representative
Full name of FSP (Brokerage or Insurer) FSP number
New policy: Type of policy: Investment or risk Policy or application number Insurer
Policy being replaced: Type of policy: Investment or risk Policy or application number Insurer
1. REASONS WHY REPLACEMENT MAY NOT BE ADVISABLE If you do replace any policy, we want to ensure that you make an informed choice. Please mark with an ‘X’ in each block below to indicate that the following information has been carefully discussed with you by your representative:
You will pay some charges and fees twice (e.g. commission, underwriting expenses & other initial charges levied by the insurer) – initially on the existing policy and once again on the new policy.
You may pay higher premiums for risk (or a bigger part of the premium) on the new policy because you are older now or your health situation might have changed.
Your new policy may not have the same life cover or premium guarantees as the existing policy. Check the period for which the life cover or other cover amounts are guaranteed before the insurer is entitled to change your premiums or reduce or remove cover.
Your new policy may have more exclusions, restrictions or waiting periods particularly if your health has deteriorated. Your new policy may not have the same investment performance guarantees as the existing policy (if applicable) The amount of money that you can withdraw under the new policy may be less (if applicable). A new policy will usually have more
legal restrictions on access within the first 5 years.
You may lose the tax advantage of your existing policy (if applicable). The surrender value or paid up value of your existing policy may be as low as 60% of the policy value before the change, and could
even be less than premiums paid in since unrecovered initial expenses must first be deducted. Check what charges you will be paying on termination of the old policy and see whether the advantages of the new policy will make up for any such charges.
The investment risk under the new policy may be higher. Remember that the past performance of a fund or asset manager of a fund is not necessarily an indication of future performance.
The representative informed you whether the existing/terminated policy could be amended to provide similar benefits to the replacement policy.
If such amendment is/was possible, your representative discussed with you why it is appropriate that the terminated policy be replaced by the replacement policy.
2. TO BE COMPLETED IF THE NEW BUSINESS WAS EFFECTED VIA ELECTRONIC BUSINESS Was the replacement policy effected as a result of the: Internet Telephone Direct marketing Please indicate the date, time of the phone call/negotiation and (if applicable) reference number:
Date Time Reference
3. DECLARATION (Signatures compulsory unless the replacement policy was effected as a result of the internet, telephone or direct marketing.) REPRESENTATIVE POLICYHOLDER
I confirm that I have taken all reasonable steps to confirm that the information in this Replacement Policy Advice Records (RPAR) is true and correct. I confirm that in pursuance of my advice to the policyholder to replace the policy(ies) mentioned in this RPAR, I have fully discharged my duties as set out in section 8 (d) of the General Code of Conduct for Authorised Financial Services Providers and their Representatives (the Code) and have retained a record of such advice as required by section 3 of the said Code.
I confirm that the representative has fully explained the consequences of the replacement of the policy(ies) mentioned in this Replacement Policy Advice Record and I understand the consequences of such replacement(s).
Contact telephone number and/or email address:
Signature Signature
Name Name
Date Date

Page 21
COMPARISON OF POLICY BEING REPLACED WITH NEW POLICY: Please ensure that you fully understand the following comparison of the conditions and benefits of your existing policy and the recommended new policy. Your representative must complete all the required information.
POLICY DETAILS EXISTING POLICY/IES RECOMMENDED NEW POLICY/IES Insurance company
Policy number
Age of life assured at inception date Type of policy (e.g. life cover, investment, pension)
1. Fees and charges (R/%) 2. Premium (R) (state whether annual, quarterly, monthly or single) R R R R R R
3. Material difference in the investment risk (conservative/moderate/aggressive)
4. Impact of age or health changes on the premium
5. Any special terms and conditions
6. Term/Initial term of policy
7. Exclusions of liability
8. Waiting period for claims (months)
9. Penalties for cancelling the product (R/%) 10. Are the penalties and charges greater than 15% of fund value? Yes No
11. Loadings and excesses (R/%)
12. Restrictions of benefits 13. To what extent are the funds readily realisable?
14. Which benefit/cover will be lost or changed? R R R R R R 15. Any vested rights or guarantees which will be lost?
16. If you were the representative on the old product, any incentive, commission received
17. Tax implications 18. Why is the replacement product more suitable to the client's needs?
REPRESENTATIVE: I declare that this Replacement Policy Advice Record is an accurate and complete record of the advice and recommendations given to the policyholder.
Name Surname Date Signature
MANAGER:
Name Surname Date Signature
POLICYHOLDER: I declare that this Replacement Policy Advice Record is an accurate and complete record of the advice and recommendations given to me by the representative. I declare that I have read and understand the advice given in this Replacement Policy Advice Record. NB: You may, by law, not be requested to sign this form unless it has been fully completed.
Name Surname Date Signature





























