Embed Size (px)
Citation preview

1JClin Pathol 1994;47:512-514
Limb ischaemia after intra-arterial injection ofTemazepam gel: Histology of nine cases
T J Dodd, R N Scott, K R Woodbum, J J Going
AbstractAims-To record the histopathologicalfindings associated with intra-arterialinjection ofTemazepam gel by nine drugmisusers.Methods-Standard histological exami-nation and immunocytochemistry forendothelial markers (factor VIII relatedantigen, Ulex europaeus lectin) werecarried out.Results-Intra-arterial injection of Tem-azepam gel may cause severe vascularinjury and lead to amputation of fingersor limbs. Histological changes includemyocyte necrosis, interstitial oedema,extensive arterial, venous, and capillarythrombosis, and sometimes vasculitis,endothelial swelling, and denudation.Conclusions-Inadvertent injection ofTemazepam gel into arteries may causecatastrophic ischaemic damage, possiblyas a result of toxic effects on endothelialcelis.
(T Clin Pathol 1994;47:512-514)
Ischaemic necrosis of limbs, leading in somecases to major amputations following intra-arterial injection of "solid gel" Temazepamhas been reported from several centres in theUnited Kingdoml4 (figs 1 and 2). In responseto previous misuse of Temazepam by injec-tion a new "solid gel" formulation replaced"liquid fill" capsules,5 but hopes that this for-mulation would curtail abuse have beendashed.6 Heating the capsule contents withwater gives a viscous but injectable product. Asimilar vascular syndrome has succeededintra-arterial "liquid fill" injection,6 but itseems to be more frequently associated withthe gel formulation.
Cases and methodsSeventeen people were admitted to GlasgowRoyal Infirmary after intra-arterial injection of"solid gel" Temazepam during 1991-1992.Of these, 15 had severe reactions. Elevenrequired multiple fasciotomies for the relief ofacute compartment syndromes. Rhabdo-myolysis was common, and four patients
Department ofPathology, GlasgowRoyal Infirmary,Castle Street, GlasgowG4 OSFT J DoddJ J GoingDepartment ofVascular SurgeryRN ScottK R WoodburnCorrespondence to:Dr J J GoingAccepted for publication25 November 1993
Figure 1 Toxicity of intra-arterial Temazepam (case 9).These gangrenous fingers were subsequently amputated.
Figure 2 Ischaemic left leg (case 1). The pallor andmottling are characteristic. High above-knee amputationwas required. Note myoglobinuria.
512
on Novem
ber 2, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.47.6.512 on 1 June 1994. D
ownloaded from

Limb ischaemia after intra-arterial injection of Temazepam gel
Clinical and histological details ofpatients studied
Case No Agelsex Clinical events Histology
1 33 M Left above-knee Arterial and venous thrombosis;amputation intravascular foreign material; necrosis,
vasculitis2 31 M Above-elbow Arterial and venous thrombosis; necrosis;
amputation of arm vasculitis3 23 M Fasciotomy Arterial and venous thrombosis; vasculitis
Amputation of toes4 25 M Fasciotomy-calf Arteriolitis; viable muscle5 30 M Fasciotomy, Arterial and venous thrombosis; necrosis;
renal failure vasculitisno amputations
6 20 F Fasciotomy, Arterial and venous thrombosisno amputations
7 22 M Fasciotomy-calf Fibrin thrombi; necrosis8 29 M Fasciotomy-calf Intravascular foreign material, no necrosis
or vasculitis9 28 M Fasciotomy No necrosis or vasculitis
right forearm
I.D. ,^
.SF6 w ,
-- f. f *I
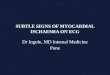
Figure 3 Arterial thrombosis (case 1). Even at this low power there is a suggestion ofendothelial swelling.
Figure 4 Venous thrombosis (case 1).
required haemodialysis for acute renal failure.Three required surgical amputations, includ-ing one above-knee and one above-elbow;others had auto-amputated fingers. Tissuewas available for histological examinationfrom nine cases and included two amputationspecimens and muscle biopsy specimensobtained at fasciotomy.
Standard haematoxylin and eosin sectionswere examined in all cases, and immunocyto-chemistry and lectin binding for endothelialcells was also performed (factor VIII relatedantigen, Ulex europaeus lectin). Tissues werefixed in neutral buffered formalin beforeexamination in view of the history of intra-venous drug misuse in all cases.
Examination of the two amputation speci-mens did not include postoperative angiogra-phy, but dissection of the arterial tree wasextended into the hand and foot respectively,and multiple cross sections of the dissectedvessels were examined at 5 mm intervals.Representative vascular and muscle blockswere processed for histology (11 from thearm, 20 from the leg). All biopsy specimens(which ranged from 10 to 30 mm in length)were completely processed for histologicalassessment.
Histological findings and clinical back-ground are summarised in the table. Cardinalhistological features were profound interstitialoedema, arterial and venous thrombosis, capil-lary thrombosis and very variable degrees ofmyocyte necrosis (figs 3-5). In five cases therewas evidence of vasculitis (fig 5), usually mildbut occasionally pronounced. Endothelial cellswelling was occasionally obvious (fig 6).Complete but focal denudation of endothe-lium was identified in case 1 (fig 7). Sparseexogenous material (in two cases) was of min-eral and plant origin. Gel embolism was notidentifiable histologically.
DiscussionThe catastrophic vascular syndrome associ-ated with intra-arterial injection of Temazepamgel is more severe than the powder embolismexperienced by injecting drug misusers, andsimple embolism seems unlikely to be res-ponsible. Temazepam is toxic to vessels.Intravenous injection of a parenteral prepara-tion (0.5-1 mg/kg) caused moderate or severepain in 22 of 62 patients, and of 11 patientsexamined 14 days later, nine had antecubitalvein thrombosis.7 Severe complications havebeen described following intra-arterial injec-tion of the liquid preparation.8 Launchburyand colleagues have stated that it was impossi-ble to formulate a parenteral preparation ofTemazepam which did not cause unaccept-able venous damage.9
Endothelial damage is perhaps the mostplausible explanation for the syndrome.Endothelial swelling identified in some casesis consistent with this. Abnormal permeabilityof injured vessels could account for the pro-nounced oedema often seen, and more severeloss of endothelial function for vascular
513
on Novem
ber 2, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.47.6.512 on 1 June 1994. D
ownloaded from

514~~~~~~~~~~~~~~~~~~~~~~~~Dodd,Scott, Woodburn, Going
1k.~~~~~~~~~~~~~~~~~~~~.A ~ ~ ~ ~
is..........
Figure 5 Interstitial oedema, inflammation, and myocyte necrosis (case 1.the largest vessel is also infiltrated by inflammatory cells.
i It
'2-47
o I
'A~~~~~~~~~~~~.II,
1I4I1
V
r. .4(;
thrombosis. Thus two potent ischaemicmechanisms (increased compartment pres-sure and vascular thrombosis) potentiallycontribute to a myocyte necrosis that is some-times severe. It is not clear why the solid-gelTemazepam preparation should apparentlycause more problems than the liquid-filledcapsules. Launchbury has pointed out that themacrogol vehicle is water soluble butTemazepam itself is highly insoluble, and~,would be expected to form an insoluble pre-cipitate when heated with water.9 Perhaps thischange of state is responsible for the apparentPotentiation of toxicity under these circum-stances. The vasculitis may reflect non-specific damage.The possibility of such a mechanism, and
theseverity of the toxicity following intra-arte-f). The wall of rial injection, leads us to wonder about the
possible effects of Temazepam solid-gel cap-sule abuse on the pulmonary vasculature fol-lowing intravenous injection. PrecipitatedTemazepam might be retained in, and dam-age, pulmonary vessels. Death has followedintravenous injection of crushed Temazepamtablets suspended in water; in that case thepulmonary vasculature contained embolisedforeign material, but its nature was not estab-lished.'I0
If endothelial injury is indeed the major*pathogenetic mechanism of this severe
adverse reaction, then it may be appropriatefor therapeutic interventions to be directedtowards modifying endothelial cell function.This strategy was used by Nott and col-leagues,4 and may have been beneficial.
We thank Mr JG Pollock, Mr DP Leiberman, and Mr DGGilmour for permission to report patients under their care.
Figure 6 Thrombosed vessel showing pronounced swelling and vacuolation of endothelialcells (case 1; (fex europaeus lectin).
*'....
4m
a'~~~~~~~~~~~~~~~~~~~-
.w
P-41; I
'AIIL-.-40.rl,: owI
I''aIAW.
Figure 7 Partial loss of endothelial lining in a venule (case 1; Ulex europaeus lectin).
1 Blair SD, Holcombe C, Coombes EN, O'Malley MCK. Legischaemia secondary to non-medical injection ofTemazepam. Lancer 1991;338:1393-4.
2 Scott RN, Wooburn KR, Reid DB, Maraj E, Going ii,Gihmour DG, et al. Intrs-arterial Temazepam. BMJ1992;304: 1630.
3 Adisheshah M, Jones DA, Round JM. Intrs-arterialTemazepam. BMJ 1992;304:1630.
4 Nont DM, Chandrasekar R, Enabi L, Greany M, BakrxanA, Harris PL. Intra-arterial injection of Temazepam indrug abusers. EurJ7 Vascular Surg 1993;7:87-9.
5 Drake J, Freedman PS, Hawkins BC, Horth CE,Launchbury AP, Whateley-Smith C. Comparative phar-macodynamics of Temazepam Geithix and liquid-filledsoft gelatin capsules.J_7Clin Pharm Ther 1991;16:345-51.
6 Ruben SM, Morrison CL. Temazepam misuse in a group ofinjecting drug users. BrJAddict 1992;87: 1387-92.
7 Hudson MM, Edmonda M, Watkins S. Misuse ofTemazepam. BMJ 1991;303:993.
8 Halliday NJ, Dundee JW, Carlisle RJT, Moore J,McCafferty JF, Woolfson AD. Experiences with IV
¶Temazepam. BrJAnaesth 1986;58:810P-lIIP.9Launchbury AP, Drake J Saeger H. Mfisuse of
Temazepam. BMJ 1992;305:252-3.10 Vella EJ, Edwards CW. Death from pulmonary microem-
bolisation after intravenous injection of Temazepam.BMJ 1993;307:26.
514
.4 i.
*.,. p
lk
.;sF
....4p.
on Novem
ber 2, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.47.6.512 on 1 June 1994. D
ownloaded from







![[XLS] · Web viewTintura Yumel Gel caléndula Gel cantharis Gel fucus Gel hamamelis Gel sulphur Gel thuja Gel bálsamo para contusiones Gel sepia Gel ledum Gel de graphites Gel de](https://img.pdfslide.net/doc/110x75/5ac4a6697f8b9a220b8ced85/xls-viewtintura-yumel-gel-calndula-gel-cantharis-gel-fucus-gel-hamamelis-gel-sulphur.jpg)