Embed Size (px)
Citation preview
Define common nonpain symptoms
experienced by hospice and palliative
care patients
Relate underlying mechanisms of these
issues
Discuss assessment of these symptoms
Describe treatment strategies, both
pharmacologic and nonpharmacologic
1. Fatigue 2. Pain 3. Anorexia 4. Drowsiness 5. Difficulty
concentrating 6. Feeling sad 7. Dyspnea 8. Agitation 9. Worrying 10. Cough
11. Nervousness
12. Constipation
13. Irritability
14. Edema arms/legs
15. Insomnia
16. Weight loss
17. Dry mouth
18. Dysphagia
19. Skin changes
20. Nausea
J Kutner, et al Symptom Burden at the End of Life JPSM 2001
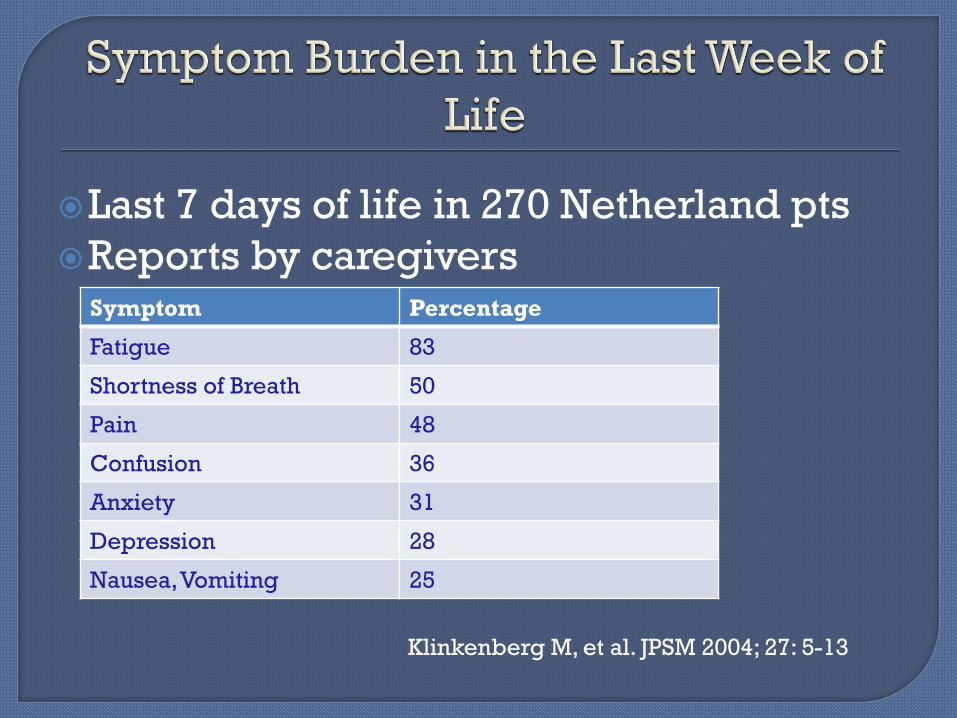
Last 7 days of life in 270 Netherland pts
Reports by caregivers
Symptom Percentage
Fatigue 83
Shortness of Breath 50
Pain 48
Confusion 36
Anxiety 31
Depression 28
Nausea, Vomiting 25
Klinkenberg M, et al. JPSM 2004; 27: 5-13
Meta-analysis for 5 diseases: Cancer, Heart Disease, Renal Disease, HIV,
COPD Despite multiple methodologies, pattern
emerged: • 11 Symptoms affected both cancer and noncancer
patients
• Pain, Depression, Anxiety, Confusion, Fatigue, Breathlessness, Insomnia, Nausea, Constipation, Diarrhea, Anorexia
• >50% had Pain, Fatigue, Breathlessness
Solano J et al. JPSM 2006; 31(1):58-69
Symptoms were assessed at 2 weeks, 2
months, 4 months
Avg age: 50s, male, caucasian
Dx: Respiratory, Sepsis/MOSF, GI
At 4 months, 11.5% “no symptoms”
Top symptoms: Weakness, Fatigue,
Insomnia, Pain, Dyspnea, Diarrhea,
Anorexia, Nausea/Vomiting, Fever,
Constipation
Choi J et al. JPSM 2014; 47(2):257-270
Approach that improves the quality of life of patients and their families facing life-threatening illness, through the prevention and relief of suffering by means of early identification and impeccable assessment and treatment of pain and other problems, physical, psychosocial, and spiritual.
http://www.who.int/cancer/palliative/definition/en

1. Fatigue 2. Pain 3. Anorexia 4. Drowsiness 5. Difficulty
concentrating 6. Feeling sad 7. Dyspnea 8. Agitation 9. Worrying 10. Cough
11. Nervousness
12. Constipation
13. Irritability
14. Edema arms/legs
15. Insomnia
16. Weight loss
17. Dry mouth
18. Dysphagia
19. Skin changes
20. Nausea
J Kutner, et al Symptom Burden at the End of Life JPSM 2001
Dyspnea very distressing symptom: Definition: “a subjective experience of
breathing discomfort that consists of qualitatively distinct sensations varying in intensity. The experience derives from interactions among multiple physiological, psychological, social, and environmental factors.”
94% COPD patients experience dyspnea in last year of life
Mahler D, Selecky P,Harrod C et al, Chest 2010; 137 (3): 674-691
Complex interaction of mechanical and
chemical receptors, specific nerve fibers,
vagus nerve—peripheral mechanism
Central nervous system: nucleus tractis
solitaris (medulla) , thalamus,
somatosensory cortex and insular cortex,
additional connection to the limbic
system
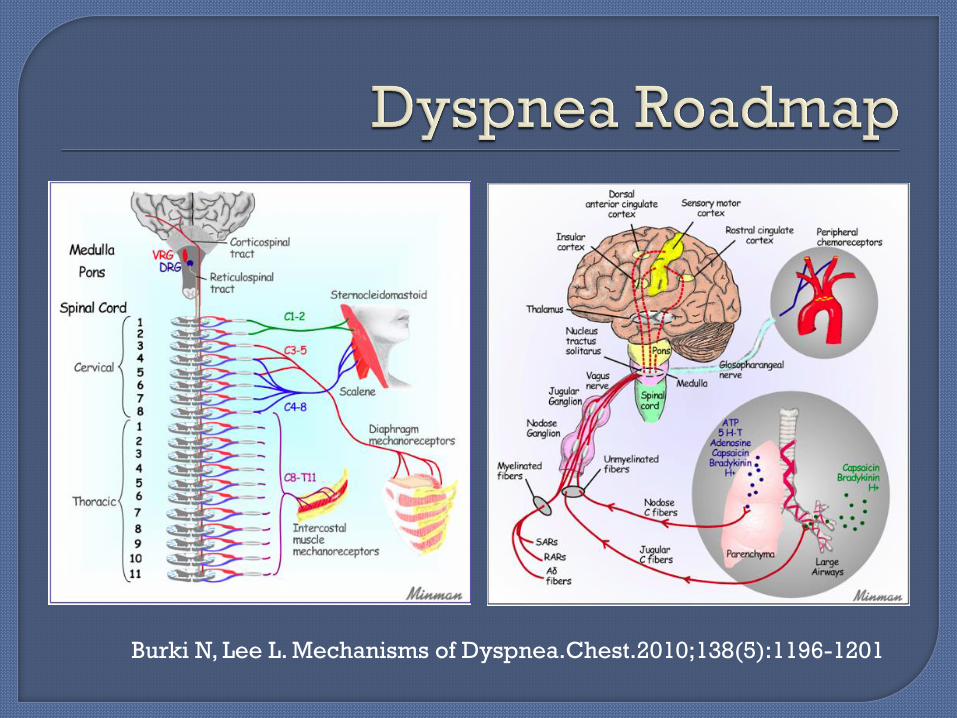
Burki N, Lee L. Mechanisms of Dyspnea.Chest.2010;138(5):1196-1201
Chemical Abnormalities • Hypercapnia, hypoxemia
Increased Work of Breathing • Mechanoreceptors, stretch receptors
Neuromechanical Dissociation • “Mismatch” between the brain’s desire for
respiratory effort and afferent feedback
Assessment:
Multiple tools
Simplest: 1-10 point scale versus four
level descriptor • None (0-1) Mild (2-4) Moderate (5-7) Severe (8-10)
Like pain, dyspnea is subjective, must
believe patient’s report
Wysham N, Miriosky B, Currow D J Pain Symptom Manage 2015;
Assessment:
Multiple tools
Modified Borg
Baseline Dyspnea Index
Medical Research Council scale
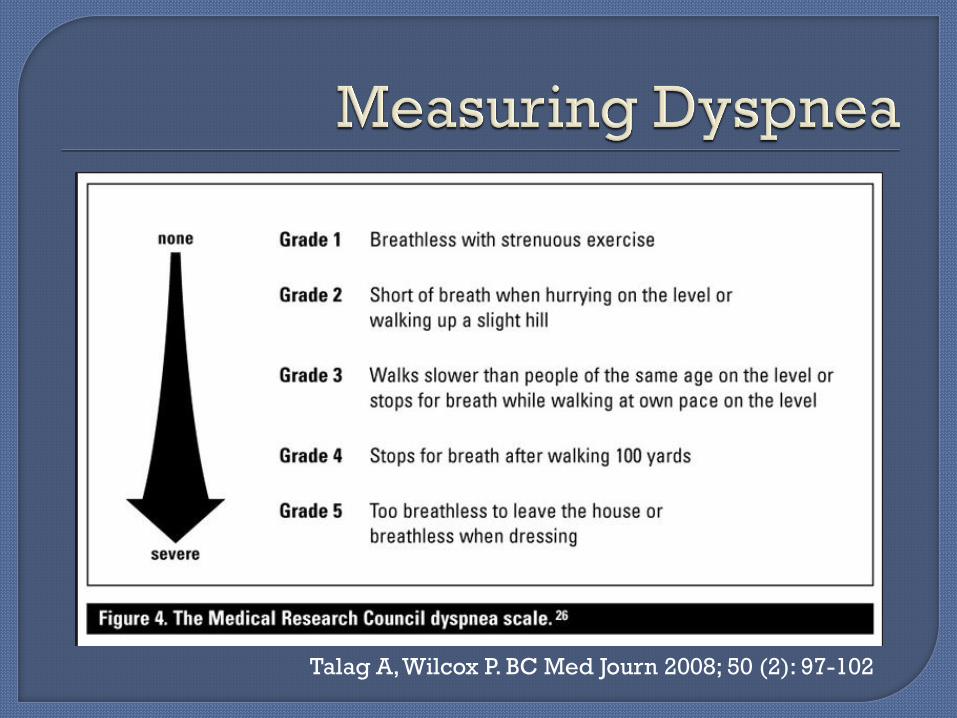
Talag A, Wilcox P. BC Med Journ 2008; 50 (2): 97-102
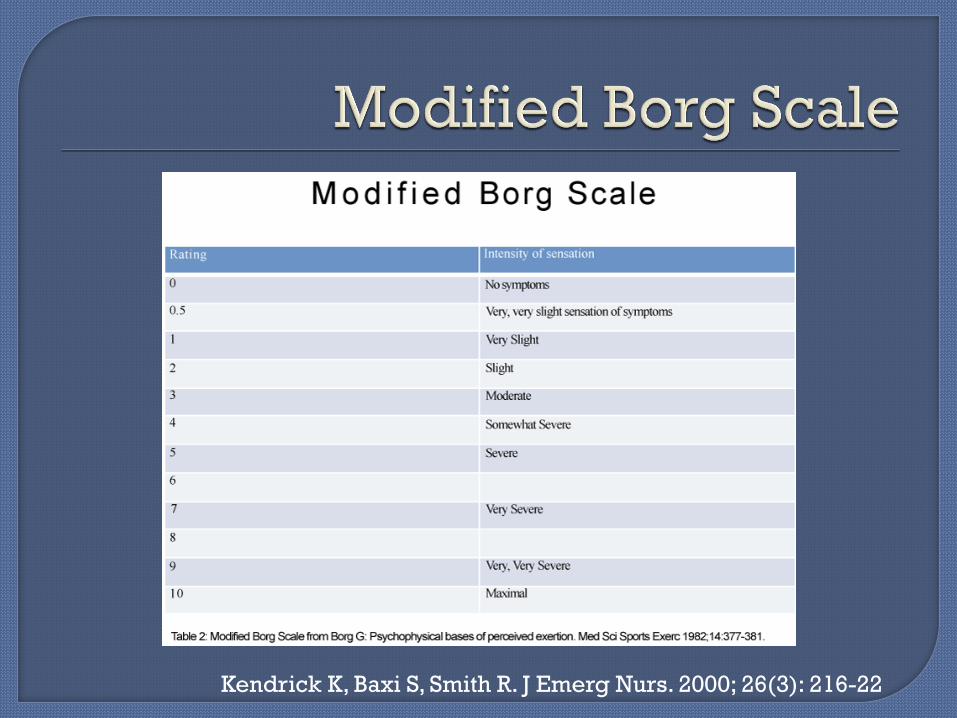
Kendrick K, Baxi S, Smith R. J Emerg Nurs. 2000; 26(3): 216-22
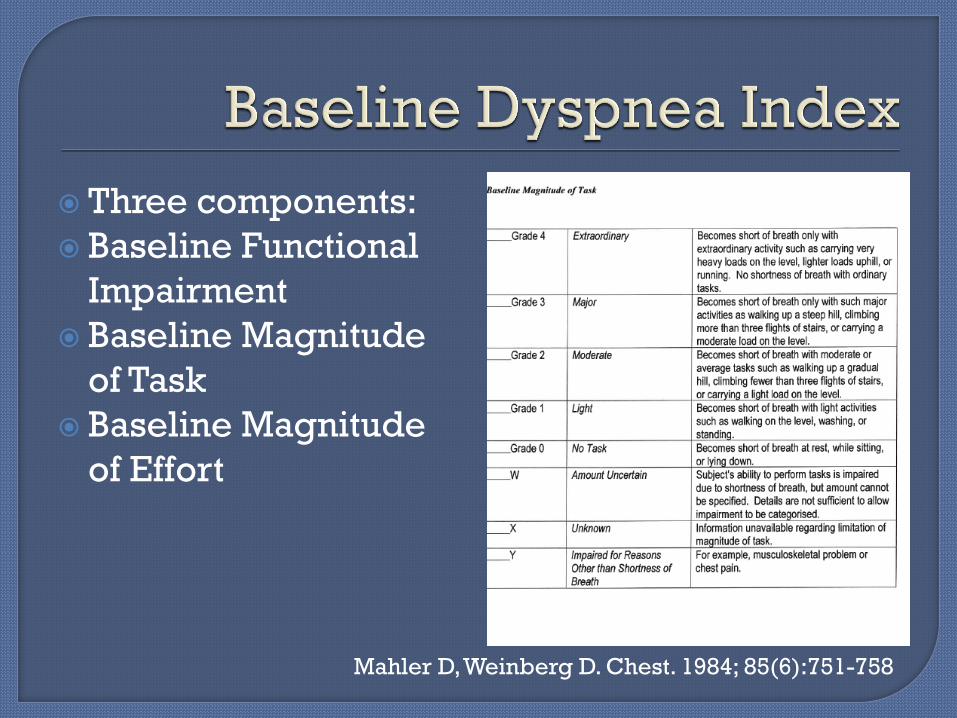
Three components:
Baseline Functional
Impairment
Baseline Magnitude
of Task
Baseline Magnitude
of Effort
Mahler D, Weinberg D. Chest. 1984; 85(6):751-758
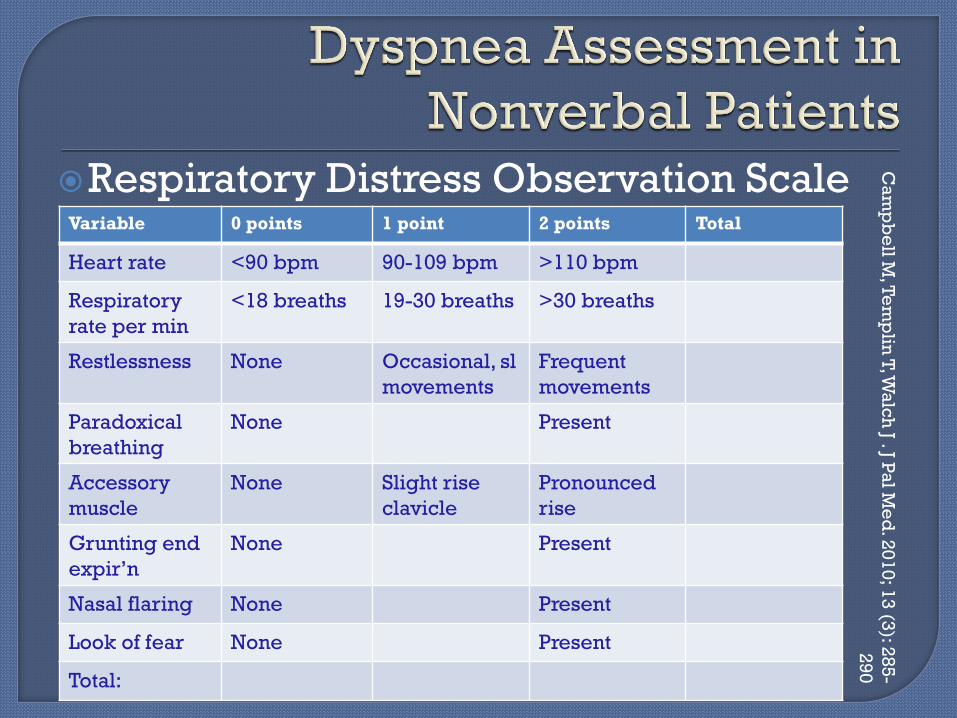
Respiratory Distress Observation Scale
Variable 0 points 1 point 2 points Total
Heart rate <90 bpm 90-109 bpm >110 bpm
Respiratory
rate per min
<18 breaths 19-30 breaths >30 breaths
Restlessness None Occasional, sl
movements
Frequent
movements
Paradoxical
breathing
None Present
Accessory
muscle
None Slight rise
clavicle
Pronounced
rise
Grunting end
expir’n
None Present
Nasal flaring None Present
Look of fear None Present
Total:
Ca
mp
be
ll M, T
em
plin
T, W
alc
h J . J P
al M
ed
. 20
10
; 13
(3): 2
85
-
29
0

Treatment of choice: • Morphine and other opiates
Oxygen • ? True efficacy
Anxiolytics • Increased incidence of GAD in pts with lung dz
Bronchodilators Diuretics CPAP or BiPAP Treat the underlying cause!
Drug of choice
Start with morphine 2.5 to 5 mg doses
Doses are lower than pain doses
Use prn dosing, watch for pattern
Add long acting opiates when dosing
evident—still need “rescue” doses
Oral/IV/SQ
Nebulized opiates not as effective as oral
per Cochrane
Does it help?
Oxygen versus medically provided air
showed similar improvement in dyspnea
symptoms in diverse palliative care
population. (O2 slightly better in AM).
?Stimulation of trigeminal nerve?
Oxygen saturation not followed.
Recommendation: use O2 for dyspnea
scores over 7/10 and consider for 4-6/10 Abernathy A et al. Lancet.2010;376:784-793
Does it help?
Cochrane review:
Oxygen versus air in patients with COPD
who were mildly hypoxemic or nonhypoxic
(not true candidates for oxygen)
Mild reduction of breathlessness in
patients who received O2 for symptoms.
“Palliative Oxygen” Uronis H McCrory D etal. Cochrane Database of Systematic
Reviews 2011. Iss 6. Article CD 0006429
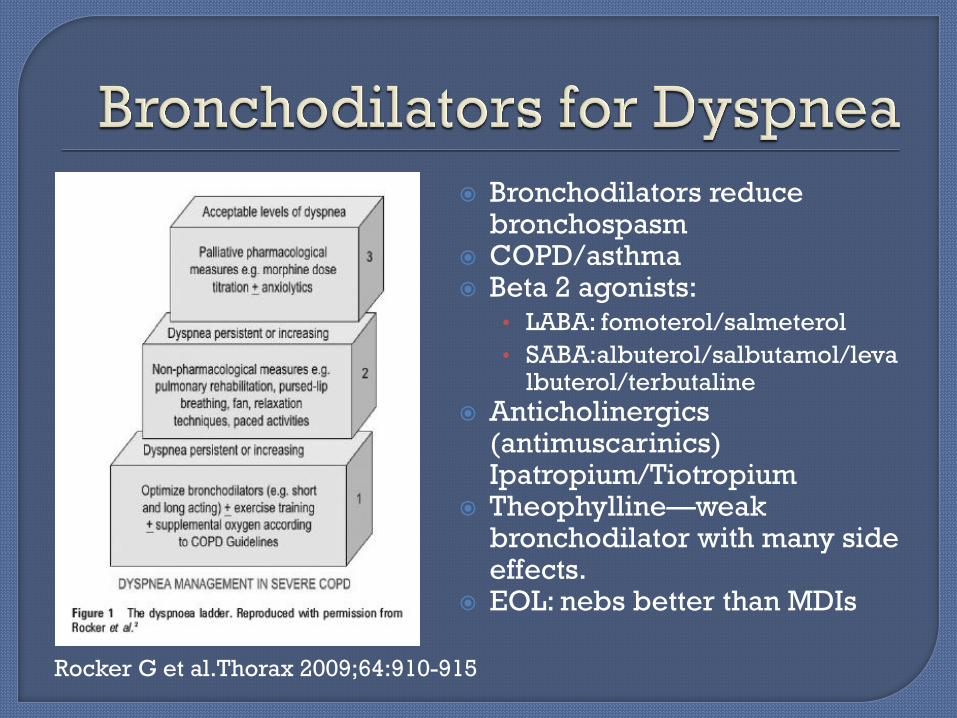
Bronchodilators reduce bronchospasm
COPD/asthma Beta 2 agonists:
• LABA: fomoterol/salmeterol
• SABA:albuterol/salbutamol/levalbuterol/terbutaline
Anticholinergics (antimuscarinics) Ipatropium/Tiotropium
Theophylline—weak bronchodilator with many side effects.
EOL: nebs better than MDIs
Rocker G et al.Thorax 2009;64:910-915
Benzodiazepines are not first line for dyspnea
They treat the anxiety associated with dyspnea
Lorazepam 0.5-1 mg po q 1 hour then schedule q 4-6h
if pattern
Midazolam 0.5 mg IV q 15 min consider infusion if
ongoing anxiety
Diazepam 2-5 mg q 6-8 hrs
Clonazepam 0.25 mg – 2 mg q 12 hrs
Thomas J, Von Gunten C. J Supportive Oncology.2003;1(1):23-34
Increasing numbers of patients come to
hospice on NIV:
Literature supports use of CPAP and
BiPAP for dyspnea in COPD,some cardiac
diseases.
Issues with corneal drying, mask
discomfort, pulling mask off in delirium
Mahler D et al. Chest Consensus statement.2010;137(3):674-691
Diuretics—for volume overload
Steroids—inflammation,
Chlorpromazine--anxiolytic
Thoracentesis—for pleural effusions
Nonpharmacological: Pursed lip breathing in COPD Relaxation techniques Clear line of sight Increasing exercise tolerance in palliative
care patients Fans blowing on facial area Adjust position
• Sit the patient up
• “good lung up”
• Tripod breathing
• Bucket-handle breathing
Integrative Treatments for Dyspnea: • Acupuncture—improved SOB on Borg and 6 minute
walk
14 of 20 pts. Sx improvement peaked at 90 minutes lasted up to 6 hours (8/20 pts resistant to trad tx)
• Acupressure—less dyspnea (VAS) compared to placebo over 6 weeks
• Relaxation techniques—improvement during the session vs. controls, no lasting effects.
• Nurse Practitioner led initiatives: improvement in “worst breathlessness score” and “distress from breathlessness”
Pan C, Morrison S, et al. JPSM 2000; 20 (5): 374-387
Agitation and delirium are common at end
of life
Delirium is a continuum from hypoactive
delirium to hyperactive delirium
Up to 88% patients experience delirium in
final days
Not all “agitation” is delirium
Families experience significant distress
watching their loved one
Survivors of delirium report distressing sx
Disturbance in attention (reduced ability to direct, focus, sustain attention) and awareness
Change in cognition that is not better accounted for by dementia
Disturbance is acute/subacute onset (hours to days) and tends to fluctuate
Evidence that disturbance is caused by general medical condition, medication, intoxicating substance or combination
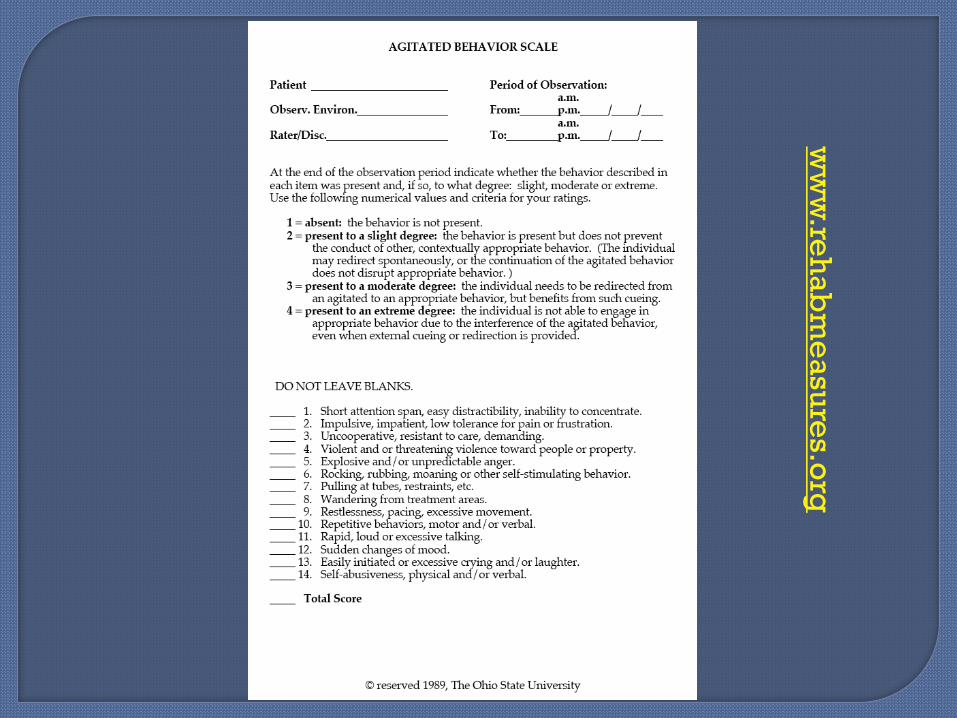
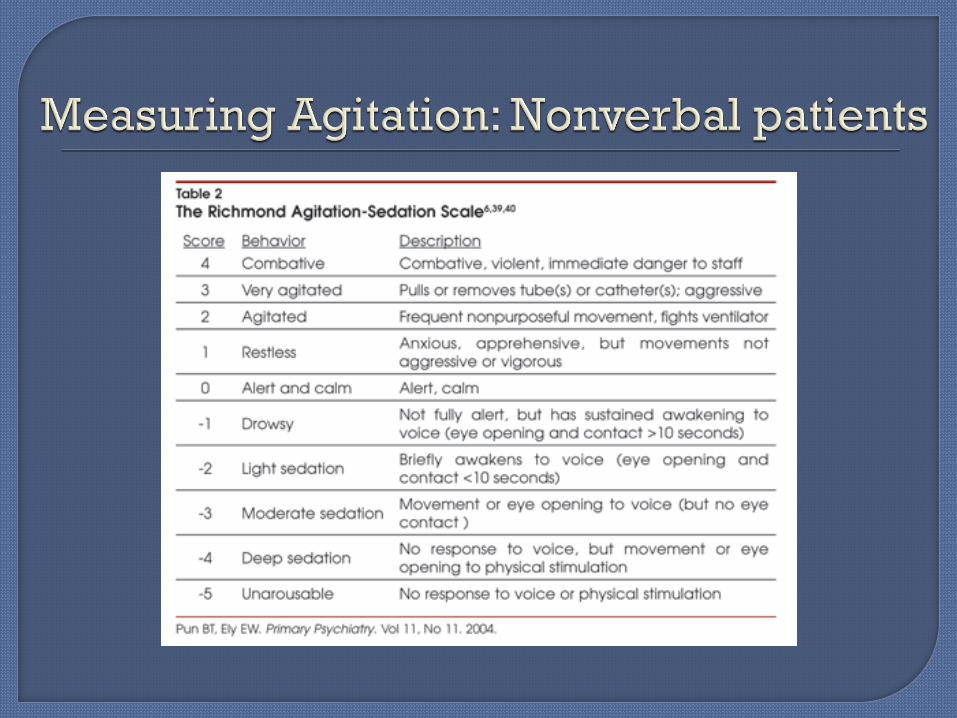
Multiple tools for assessment
MDAS—10 item scale
DRS-98-R 16 items, requires expertise
Confusion Assessment Method-Simple • CAM-S—4 item
LeGrand. JPSM. 2012;44(4):583-594
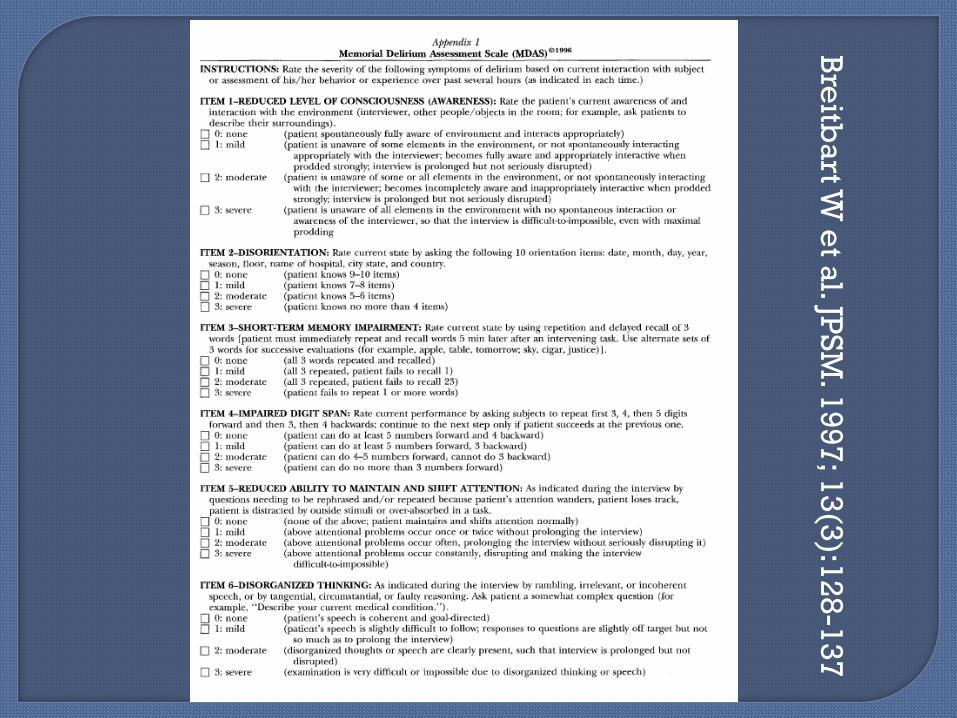
Bre
itba
rt W e
t al. JP
SM
. 19
97
; 13
(3):1
28
-13
7
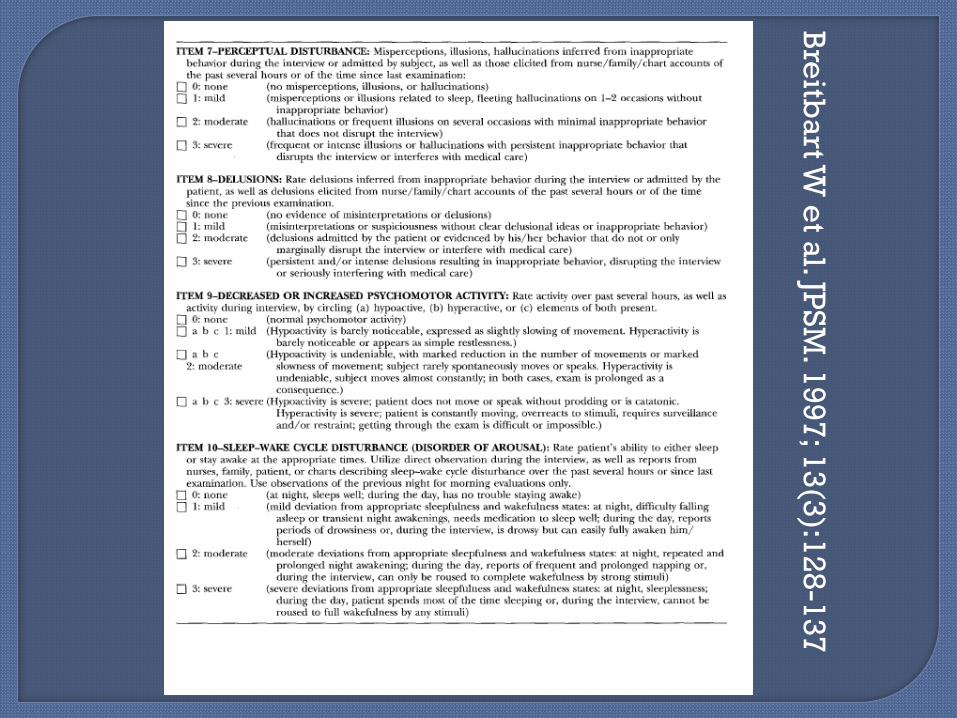
Bre
itba
rt W e
t al. JP
SM
. 19
97
; 13
(3):1
28
-13
7
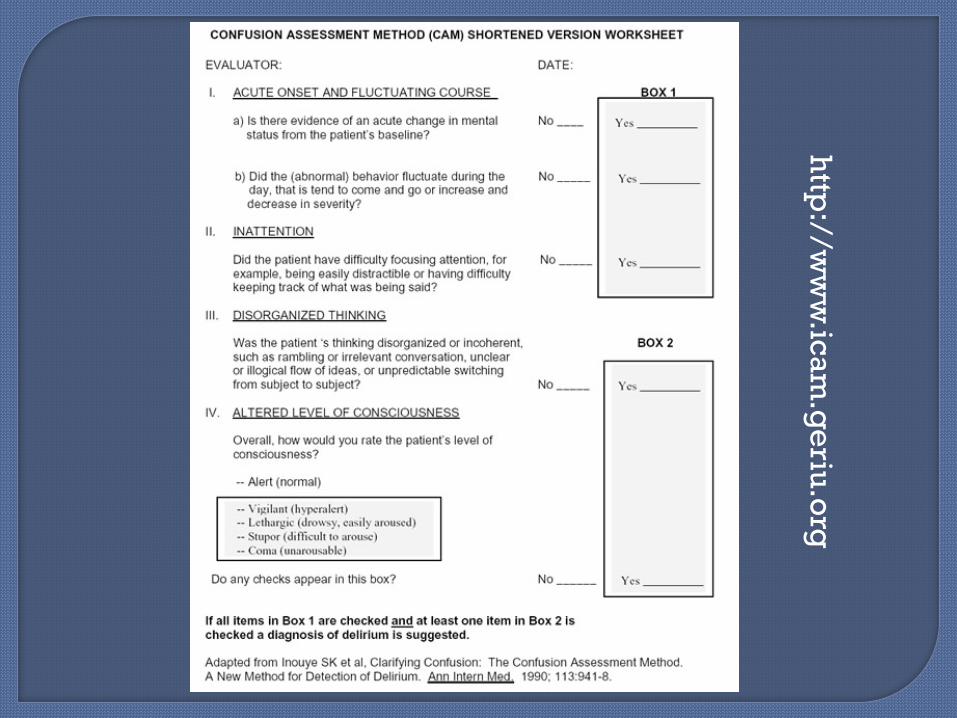
http
://ww
w.ic
am
.ge
riu.o
rg
Neurotransmitter imbalance: decreased
acetylcholine and increased dopamine,
changes to GABA, glutamate, serotonin
Inflammatory cytokines that impact
neurotransmitters
Changes in intraneuronal signals
affecting neurotransmitters
LeGrand. JPSM. 2012;44(4):583-594
Infectious Withdrawal Acute metabolic Trauma CNS pathology Hypoxia Deficiencies Endocrine disease Acute vascular Toxins/Medications Heavy Metals
Drugs, dehydration Electrolytes, environment Lungs, low O2,lack of sleep Infection, infarction,
iatrogenic Retention urine/feces, renal
failure, restraints Injury, intoxication UTI, unfamiliar environment Metabolic, metastases,
medications Subdural,supratentorial
Delirium:
• Opiates
• Benzodiazepines
• Anticholinergic agents
• Steroids
Agitation:
• Stimulants
Agitation “lookalike: • Neuroleptic-----consider akathisia!**
Durkin E, Probolus A,Kayden.Akathisia#282 J Pal Med.2014;17(9):1064-1065
Up to 50% delirium is reversible
More likely in medications, infections,
electrolyte abnormalities
Less likely if previous delirium, hypoxia
or profound metabolic encephalopathy
Dementia a strong risk factor for delirium
in elderly, recovery poor, elevated
mortality rate for delirium superimposed
on dementia
Bush S, Kanji S et al. JPSM. 2014; 48(2):231-248
Determine goals of care
Review medications—any changes?
Consider “common” causes: fecal
impaction, urinary retention, infection
(UTI),dehydration, opiate induced
neurotoxicity
Treat the underlying cause
Often unclear etiology
Haloperidol most commonly used • Quetiapine in Parkinsons/Plus patients

Other antipsychotics • Chlorpromazine—hypotension, anticholinergic
• Atypicals are nonsuperior to haloperidol
Benzodiazepines • Alcohol or GABA receptor withdrawal
• Add to antipsychotic if akathisia/EPS occurs
Valproate (IV) • If antipsychotics ineffective
• Severe agitation/disinhibition
Stern R, Celano C et al.Prim Care Companion to J Clin Psych 2010; 12 (1): PCC.09r00938
Under investigation:
Melatonin
Modafinil
Gabapentin
Consideration of anti-inflammatory meds
due to cytokine involvement
Bush S, Kanji S et al. JPSM. 2014; 48(2):231-248
Environmental approaches
Reduce stimulation: noise, excessive light
or dark, fewer visitors
No restraints
Orientation board
Re-set sleep-wake cycle, reduce daytime
napping, daytime light, quiet at nighttime
Hearing aids, eyeglasses, dentures
Bush S, Kanji S et al. JPSM. 2014; 48(2):231-248
Music therapy—literature points to relief
of anxiety/some improvement in
agitation in postoperative hip patients
Aromatherapy—used to reduce anxiety
in post operative patients in PACU.
McCaffrey R, Locsin R. Holistic Nursing Practice.2006;20(5):218-224
Common in patients with advanced illness, and at end of life--up to 70%
Constipation is multifactorial. US: more than 2.5 Million physician visits
per year related to constipation In elderly, over 50% using laxatives
regularly Laxative use in US: $821 Million OTC More commonly reported in women
(21% vs. 8% men--NHANES 1989)
Constipation definition: At least 12 weeks with 2 or more
symptoms: Straining >25% time Sensation incomplete evacuation >25% Lumpy/hard stools >25% Anorectal blockage Manual maneuvers to remove stool Less than 3 stools/week
Loose stools are not present without
laxatives
Insufficient criteria for irritable bowel
syndrome
Criteria designed by International
Congress of Gastroenterology
Not specifically designed for palliative
care patients
Infrequent difficult passage of small, hard
stools
Difficulty to defecate at will
Straining
Sensation of incomplete evacuation
Associated hemorrhoids, fissures, fecal
impaction, pain
Decreased quality of life
Librach S, Bouvette M. J Pain Sympt Manage. 2010; 40 (5): 761-773
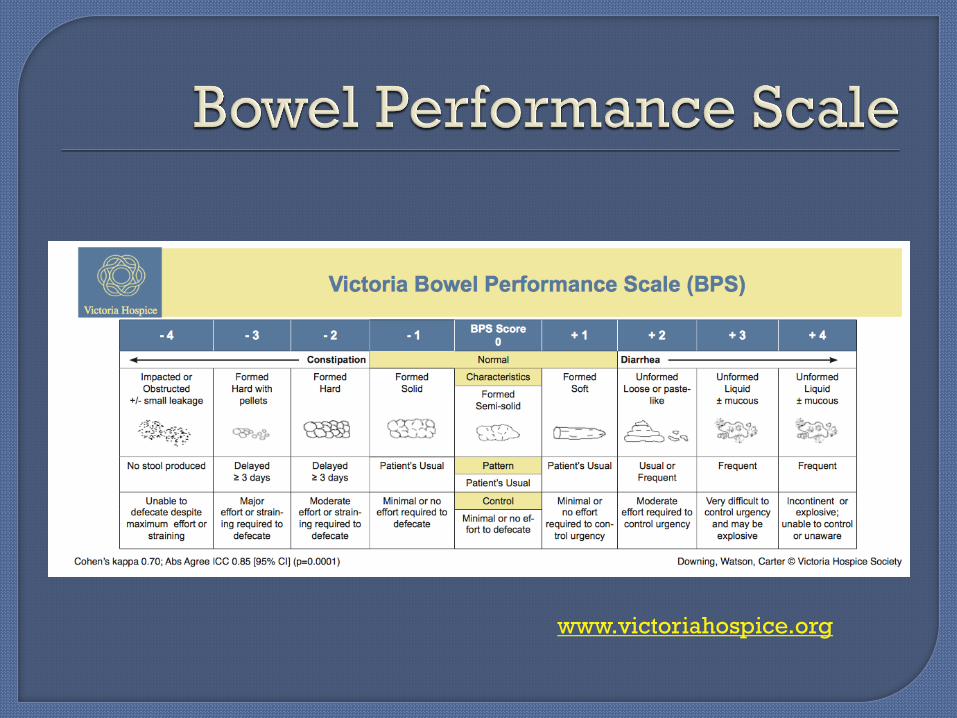
Ask patient to describe usual bowel patterns prior to illness versus now
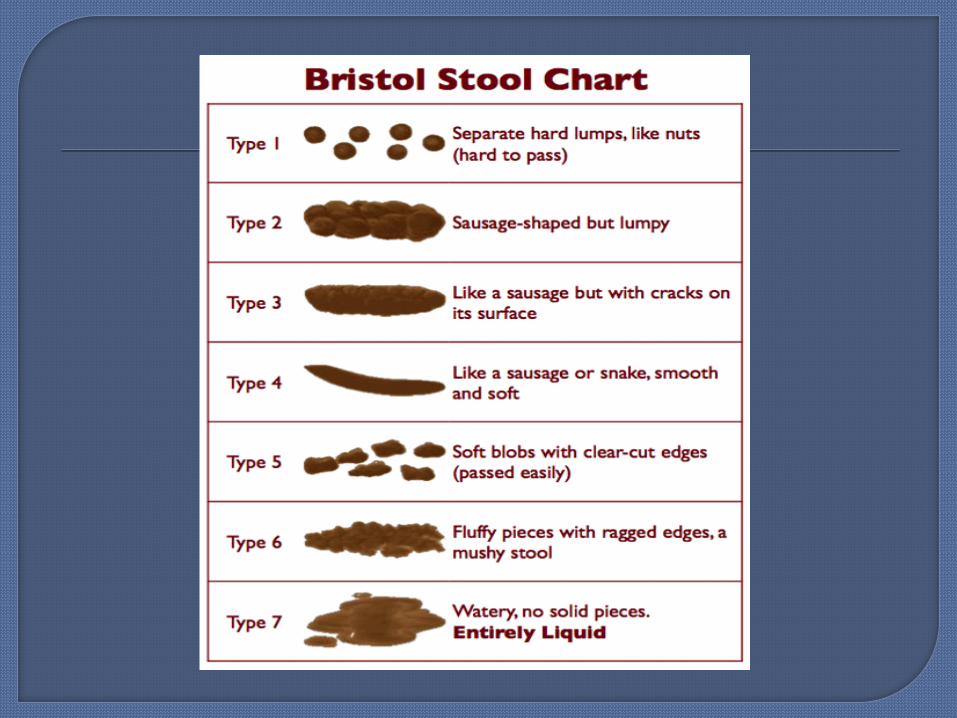
Frequency Character of stools incl blood, mucous,
color, hardness Bloating, flatus Diarrhea? Tenesmus Need for help with elimination (manual
or enema)
Medications: opiates, antacids, antiemetics antiepileptics, antidepressants
Metabolic: dehydration, hypercalcemia, hypothyroidism, uremia
Weakness/fatigue: myopathy Neurological: Cerebral tumors, spinal cord
disease, autonomic dysfunction Anorexia: reduced fluid/food/low fiber Pain of defecation: tenesmus, bone pain, cancer Environmental/cultural: privacy,burden Mobility: bedbound, deconditioning,slow to
toilet, depression, sedation
Librach S, Bouvette M. J Pain Sympt Manage. 2010; 40 (5): 761-773
Physical exam is essential!
Abdominal examination: • Distension, bowel sounds, masses, tenderness
• Tympany versus ascitic fluid
Rectal exam often helpful: • Tone
• Masses at anus, in rectum
• Presence and quality of stool in vault
• Hemorrhoids, fissure, fistula, lesions
• Lots of lubricant, go slowly and gently
Increase fluids
Increased activity (even getting upright)
Toileting strategies--take advantage of
gastro-colic reflex (within 20 minutes of
eating)
Are there barriers to having a BM? (no
assistance with ambulating/transferring
to bedside commode, fear of soiled
diaper)
Attempt to select/substitute less
constipating drugs (eg. Calcium channel
blockers--another class)
Consider lab work: calcium, TSH
Abdominal flat plate: Constipation score
0-3 in all 4 quadrants. More than a “7”
calls for aggressive therapy
Opiates are BIG culprits in constipation at end of life:
Tolerance develops to sedation, nausea, itching, but NOT TO EFFECT OF SLOWING TRANSIT TIME IN COLON!!!
Fiber, which is helpful in general
population, may not be helpful at end of
life…..it does not directly impact colonic
transit time
Requires that patient take in lots of fluids,
otherwise…..BRICKS
Stimulants Anthracene: Senna Diphenylmethane: Bisacodyl Induce peristalsis Colonic bacteria convert senna to active
form Risk of cramping 6-12 hours to work (suppository 15-60 min)
Stool softeners Dioctyl sodium sulfosuccinate “Docusate”
Decreases surface tension Water enters stool more easily 1-3 days to see an effect BUT literature doesn’t support docusate plus
senna vs senna alone
Lubricants Mineral Oil Lubricates passage 1-3 days to work Risk of aspiration Causes rectal seepage Interferes with absorption of some meds Not considered first line strategy
Osmotic agents: Lactulose, mannitol, sorbitol, Polyethylene
glycol Draw water into stools primarily in small
intestine PolyEthyleneGlycol requires large volumes
water (17 gms in 250 mls liquid) 1-3 days to work Can cause gassiness and bloating
Osmotic agents: Magnesium and phosphate salts Milk of Magnesia, Magnesium citrate Increase intestinal water secretion, stimulate
peristalsis 1-6 hours til effect Use with caution in renal impairment Can cause electrolyte imbalances
Suppositories Local stimulation Glycerin 38% success in 1 hour Bisacodyl (dulcolax)--induces peristalsis
in 15-60 minutes—must touch bowel wall 66% success in 1 hour
Enemas Arachis/olive oil—”retention” lubricants Sorbitol--osmotic Sodium docusate--softening Sodium phosphate--peristalsis Saline--8 l warmed Pure tap water versus phosphate
enemas--concern re: electrolyte shifts Soap and water: irritates rectal mucosa Milk and Molasses--osmotic
Suspected obstruction--NO BULK AGENTS! Softeners
Fecal impaction--may need disimpaction + fecal softening: glycerin, arachis, olive oil
Soft feces in rectum: stimulant No feces in rectum: stimulant
Metoclopramide as a prokinetic agent--more upper GI tract (do not use in obstruction)
Erythromycin and other macrolides
initiate motor complexes in small bowel
Methylnaltrexone (naloxone derivative) a selective opioid antagonist at bowel receptors
Subcutaneous 8-12 mg injection based upon weight <84 lb or >251 lb use 0.15 mg/kg Reduce dose by 50% CrCl < 30
ml/min Laxation within 30 minutes for >30%
pts Use in laxative failure for patient on
opiate regimen

Prokinetic Amitiza (lubiprostone) 24 mcg oral twice a day For chronic idiopathic constipation Chloride channel activator, increases
intestinal fluid secretion, increases motility.
High co-pay for insurance companies Weight gain, chest pain, other side effects
Prokinetic
Linzess (Linaclotide)
Indications: Irritable Bowel Syndrome with
constipation or Chronic Idiopathic Constipation
Guanylate Cyclase-C agonist: moves chloride
and bicarbonate into intestines
Dose: 145 mg once daily for CIC, 290 mg once
daily for IBS with C
Side effects: diarrhea, abdominal pain, N,V,
GERD

Naloxegol (Movantik)
Oral medication binds to opiate
receptors in bowel, 25 mg increased BMs
for patient on opiates.
Side effects: abdominal pain, diarrhea,
nausea and vomiting, gas.
May reduce dose to 12.5
Multiple drug interactions! Antibiotics,
antifungals, grapefruit
Prokinetic
Prucalopride Serotonin receptor agonist. Works similarly to
tegaserod, which was associated with cardiac
events
Tegaserod is selective 5-HT4 agonist, available
only to women less than 55 with IBS-C or CIC
Colchicine—side effect of diarrhea at certain
doses.
Neuropathy and myopathy are theoretical side
effects.
Gastrografin—iodinated contrast agent
Trial in Italy showed success in 45% cancer
patients with constipation
Neostigmine—acetylcholinesterase inhibitor
reduces intestinal atony (myasthenia gravis)
But bronchoconstriction, bradycardia
Prunes and coffee Rhubarb Cascara Ginger root Licorice root Irish Moss Cayenne Dandelion root Chamomile
Foods:
Papaya
Hot peppers
In some patients with Irritable Bowel
Syndrome Issue: everyone’s bowel problems may be
different
Different organisms used: Lactobacillus and
Bifidobacterium
Different endpoints
Studies underwritten by commercial interests
Delphi technique used
Safety profiles are favorable—can’t hurt!
Stool softeners the primary strategy for
hemorrhoids, anal fissures, and stercoral
ulcers
Herpes of perineum may need
aggressive treatment--aciclovir,
famciclovir, but if resistant/unable po--
cidofovir or foscarnet
Nausea/vomiting Delirium Terminal
restlessness Urinary retention Diarrhea
Presents with nausea, vomiting, intestinal colic
Stools vary from constipation for feces and
flatus to overflow diarrhea
Rule out fecal impaction.
Abdominal Xrays
Stop bulk agents
Stop prokinetics in complete obstruction
Steroids early until you are certain
One of the most distressful symptoms
Usually multifactorial
Common in cancer patients, as well as
end stage renal disease and hepatic
failure
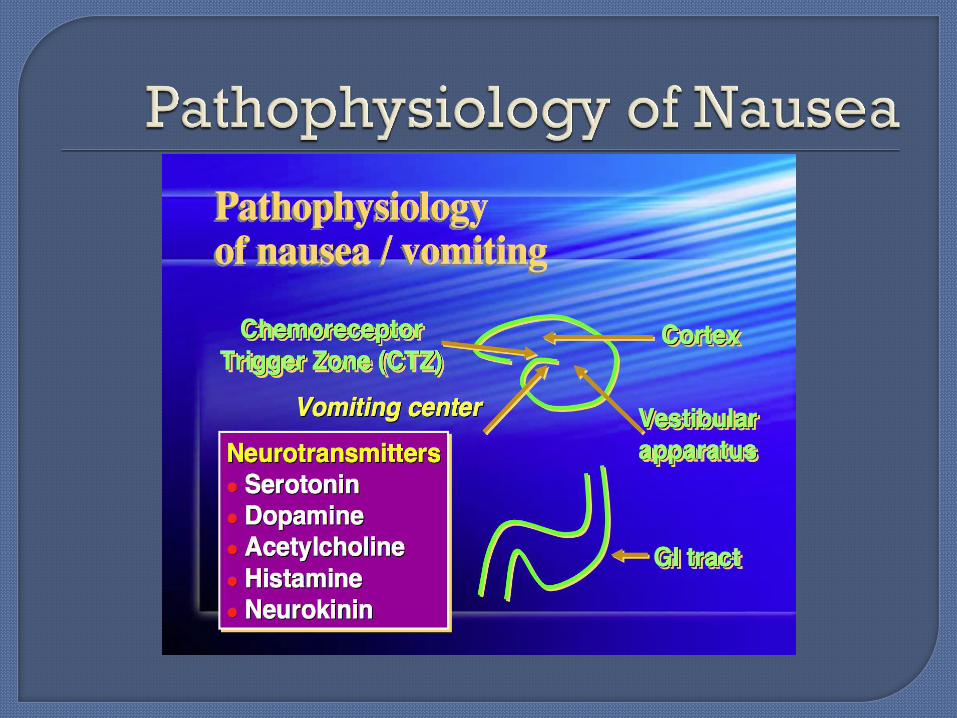
Five areas of interest in treating nausea:
peripheral, vestibular tract,
chemoreceptor trigger zone, cerebral
cortex, vomiting center (midbrain)
Nausea intensity (0-10), duration
Aggravating or activating factors
qUality of life disturbances from N,V
Symptoms accompanying nausea and
vomiting
Emetic episodes per 24 hours
Alleviating factors
Dahlin C, Lynch M, et al Anesth Clin N Amer. 2006;24:39-60
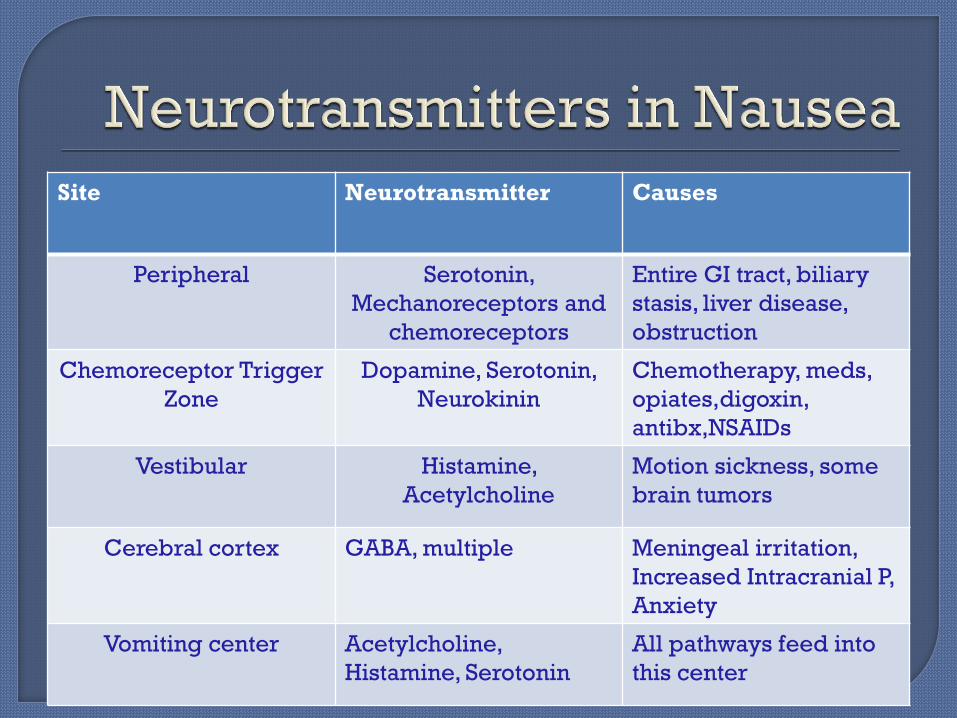
Site Neurotransmitter Causes
Peripheral Serotonin,
Mechanoreceptors and
chemoreceptors
Entire GI tract, biliary
stasis, liver disease,
obstruction
Chemoreceptor Trigger
Zone
Dopamine, Serotonin,
Neurokinin
Chemotherapy, meds,
opiates,digoxin,
antibx,NSAIDs
Vestibular Histamine,
Acetylcholine
Motion sickness, some
brain tumors
Cerebral cortex GABA, multiple Meningeal irritation,
Increased Intracranial P,
Anxiety
Vomiting center Acetylcholine,
Histamine, Serotonin
All pathways feed into
this center
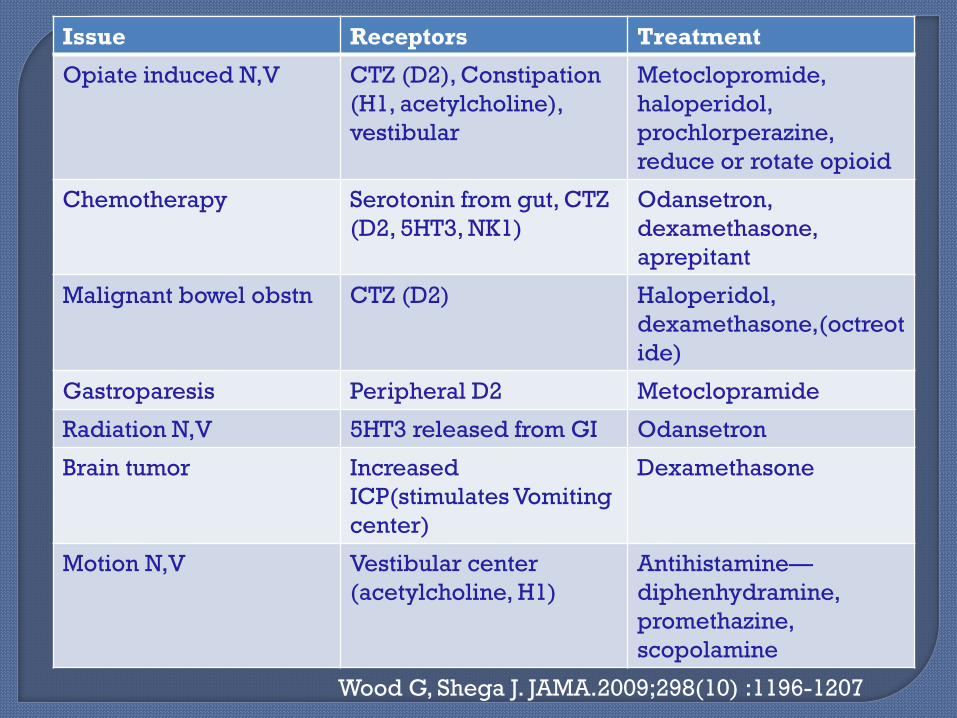
Issue Receptors Treatment
Opiate induced N,V CTZ (D2), Constipation
(H1, acetylcholine),
vestibular
Metoclopromide,
haloperidol,
prochlorperazine,
reduce or rotate opioid
Chemotherapy Serotonin from gut, CTZ
(D2, 5HT3, NK1)
Odansetron,
dexamethasone,
aprepitant
Malignant bowel obstn CTZ (D2) Haloperidol,
dexamethasone,(octreot
ide)
Gastroparesis Peripheral D2 Metoclopramide
Radiation N,V 5HT3 released from GI Odansetron
Brain tumor Increased
ICP(stimulates Vomiting
center)
Dexamethasone
Motion N,V Vestibular center
(acetylcholine, H1)
Antihistamine—
diphenhydramine,
promethazine,
scopolamine
Wood G, Shega J. JAMA.2009;298(10) :1196-1207
Can be determined in many patients
Medications
Metabolic (including dehydration)
Infections
Gastric Slowing
Constipation
Anxiety
Motion
Attempt to reverse if possible
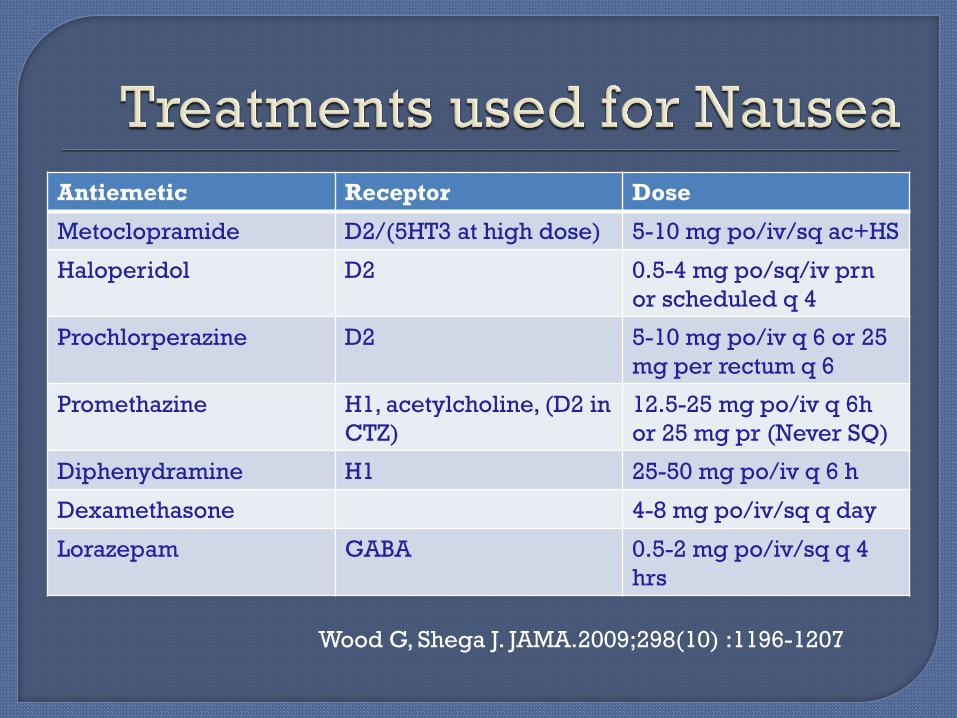
Antiemetic Receptor Dose
Metoclopramide D2/(5HT3 at high dose) 5-10 mg po/iv/sq ac+HS
Haloperidol D2 0.5-4 mg po/sq/iv prn
or scheduled q 4
Prochlorperazine D2 5-10 mg po/iv q 6 or 25
mg per rectum q 6
Promethazine H1, acetylcholine, (D2 in
CTZ)
12.5-25 mg po/iv q 6h
or 25 mg pr (Never SQ)
Diphenydramine H1 25-50 mg po/iv q 6 h
Dexamethasone 4-8 mg po/iv/sq q day
Lorazepam GABA 0.5-2 mg po/iv/sq q 4
hrs
Wood G, Shega J. JAMA.2009;298(10) :1196-1207
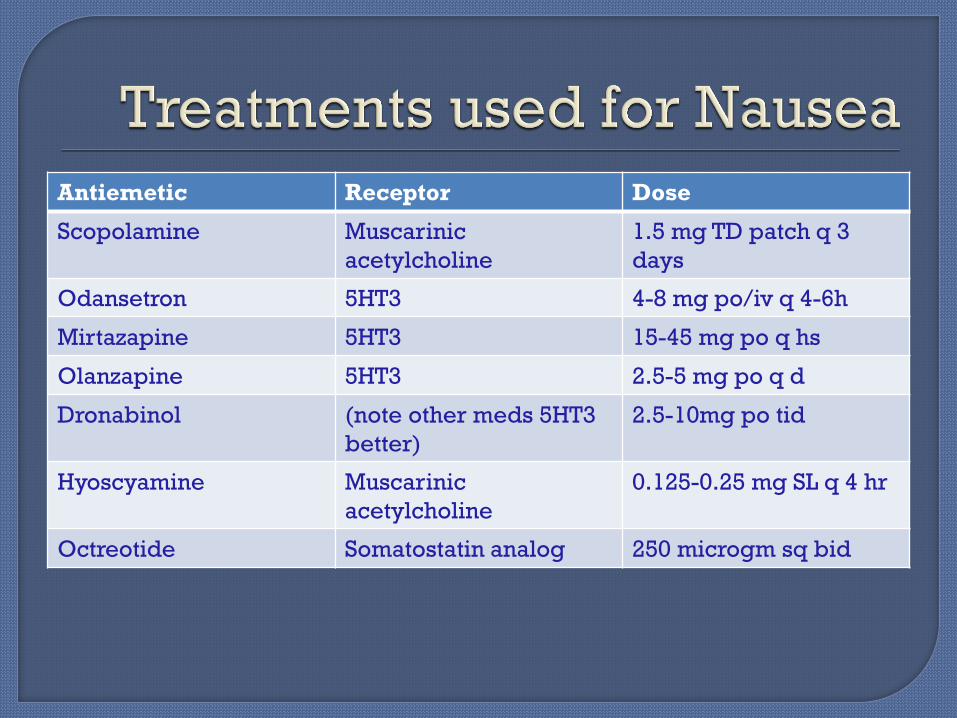
Antiemetic Receptor Dose
Scopolamine Muscarinic
acetylcholine
1.5 mg TD patch q 3
days
Odansetron 5HT3 4-8 mg po/iv q 4-6h
Mirtazapine 5HT3 15-45 mg po q hs
Olanzapine 5HT3 2.5-5 mg po q d
Dronabinol (note other meds 5HT3
better)
2.5-10mg po tid
Hyoscyamine Muscarinic
acetylcholine
0.125-0.25 mg SL q 4 hr
Octreotide Somatostatin analog 250 microgm sq bid
Look at medication list—any recent additions?
Consider drug interactions Streamline medications Consider hydration Treat underlying cause if possible Aim treatment at possible pathway for
nausea Haloperidol remains the most used drug May require multiple antiemetics

Small frequent meals Bland nonspicy food Fluids
Integrative: Accupressure to P6 helpful in nausea,
vomiting Accupuncture less so Ginger and B6 are helpful in pregnancy
(CTZ)
Management relies on good assessment,
use of tools
Understanding underlying mechanisms
help in developing a strategy
Streamline medications to reduce
interactions and additional symptoms!
Symptoms often have nonpharmacologic
interventions as well.
Be anticipatory/proactive