Embed Size (px)
Citation preview
Linking Multiple Administrative Data Sets to Measure Outcomes for Behavioral Health
Services
Oklahoma Department of Mental Health and Substance Abuse Services
Tracy Leeper, Grant Projects Manager
Funded by CSAT
Focused on Administrative Data
All Adults Who Receive SA
Treatment Services in a Given Year
Two Year Pre & Post Follow-Up Periods
Determine Costs Associated with Outcomes
Outcomes Substance Abuse Treatment Outcomes Monitoring System
Administrative Data
Ongoing & Sustainable
Empirically-Based & Objective
Less Resource Intensive
Longitudinal
Flexible for Populations & Time Frames
Unobtrusive
No Direct Measures for Certain IndicatorsNo Direct Measures for Certain Indicators Little Drug Use InformationLittle Drug Use Information
Level of Functioning or SymptomotologyLevel of Functioning or Symptomotology
Indirect MeasuresIndirect Measures Look at Contribution to Society Versus Cost to
Society
Employed, Paying Taxes
Decrease in Jail and Inpatient Days
Administrative Data
Sources of Data
DMHSAS - State-funded AOD & Mental Health
DPS – DUI Convictions
DOC – Incarcerations, Probation & Parole
OTC – Household Income
OESC – Wage & Unemployment Benefits
Sources of Data
OSDH - Mortality Data
OHCA – Medicaid Claims
OSBI – Arrests/Dispositions
DHS – TANF, Food Stamps, Child Welfare
Legislation
Interagency Pilot Projects
Quid Pro Quo
Good Ol’ Boy Approach
Getting “Buy-In”
Leave Plenty of Time for:Executing Agreements
After Administrative “OK,” Still Need MIS Staff Buy-InDiscussionsWorking Out DetailsMust Have a Working Relationship with Other
Agencies’ MIS Staff
Getting “Buy-In”
Confidentiality Concerns
42 CFR
HIPAA
Interagency Agreement
IRB Approval
42 Codified Federal Regulation (CFR)
Medical Emergencies Research Activities Audit and Evaluation Activities
Subchapter A, Part 2Confidentiality of Alcohol and Drug
Abuse Patient RecordsSubpart D – Disclosures without Patient Consent
Health Insurance Portability and Accountability Act of 1996 (HIPAA)
C. General Risk. (§ 164.506)Covered entities would be able to use or disclose an individual’s protected health information without authorization for treatment, payment, and health care operations.
B. Definitions. (§160.103 and § 164.504)16. Health Care Operations.- Conducting quality assessment and improving activities, including evaluating outcomes, and developing clinical
guidelines.
Interagency Agreement
I. Purpose
II. Effective Dates
III. Confidentiality
IV. Transfer of Data
V. Specify Persons Working with Data
VI. Modification or Amendment
VII. Signatures
Data SecurityHandling and Storage
Receive Data In A Variety Of Ways
Tapes, CDs, Disks, FTP, E-Mail
Dedicated File Server
Limited Users
Secure Location
Separate Identifiers and Outcome Data
Cleaning & Preparing the Data(Good News, Bad News)
Data Sets Are Not Well Documented
Many Variables Are Defined Differently
Data Formats Change Periodically (i.e.,
Constantly)
Cleaning & Preparing the Data(Good News, Bad News)
Recode the Variables
01/01/1999 vs. 01-01-99
vs. 990101
Unduplicate the Records
Allow for Aliases
Format Names
Exact (All-Or-Nothing)
Probabilistic
Combination of the Two
Overlap Procedure (PPE)
Linking The Data
Methods:
Block by Sex and DOB Components
Sex & Month & Year
Sex & Day & Year
Sex & Month & Day
Assign Weights to All Identifying
Variables
Linking The Data
Positive & Negative Weights
Jaro, Matthew. Statistics in Medicine, Vol. 14, 491-498
(1995).
Determine Threshold of Likelihood
Gray Area – Manual Inspection
Matching Algorithm Changes Depending on
Available Variables
Weighting The Data
Perfect Match = 69 pts.
SSN (all digits) = 22.55
SSN (8 digits) = 14.51 pts.
SSN (7 digits) = 6.07 pts.
Weighting The Data
or -2.38 pts.
Last or Maiden Name = 9.58 or –3.62 pts.
First Name = 6.69 or –3.27 pts.
Middle Initial = 3.65 pts.
Date of Birth = 6.22 pts.
Weighting The Data
Data SecurityHandling and Storage
Determine What Type of Results
You Want Before You Start What Type of Analysis Do the Data Allow?
What Do the Stakeholders Want?
What Type of Data Structure Do You Need?
Large Data SetsNeed Lots of Hard Drive Space & Memory
Need Appropriate Software
Treatment Completers: “Planned Discharge” & more than 5 units of Service
Treatment Non-completers: No “Planned Discharge” & more than 5 units of Service
Minimally Treated: 5 or fewer units of Service
Detox Only: Detoxification Services Only
Work Closely with Participating Agencies –
Disclose Results To Them
Think of Political Ramifications
for All Agencies Involved
Explicitly State What You Want the
Audience to Get from the Results
Disseminating The Results
Allow Much More Time Than You Think At Each Step
Be Flexible – Willing to Start Over Or Live With It
Meet With Other MIS Staff
Be Willing to Evolve With Technology and Experience
Lessons Learned Along The Way
Managed Care vs. Traditional System
Mental Health Court Involvement
PACT/ACT Clients
Persons with Co-Occurring
Special Interest Groups
Case-Mix Analysis
Cost Analysis
Interstate Cooperative Study
Parity – Race, Gender, Geography
Additional Uses
EVALUATING OUTCOMES OF CLIENTS RECEIVING BOTH SUBSTANCE ABUSE AND
MENTAL HEALTH TREATMENT
Oklahoma Department of Mental Health
and Substance Abuse ServicesBecki Moore and Tracy Leeper
To determine whether outcomes for clients with
dual treatment differ from those of clients receiving
mental health or substance abuse treatment only
To demonstrate the feasibility and utility of using
administrative data for different populations and
outcomes
Purpose
Methods
Study GroupThree Cohorts
mental health treatmentsubstance abuse treatmentdual treatment
Adults, 18 years of age or older, admitted to treatment during FY97 (N=28,104)
Administrative Data
Two-year Pre- and Post-Treatment Study Periods
Methods
Sources of Data
DMHSAS - State-funded SA & MH
OSDH - Mortality
DOC - Incarcerations, Probation &
Parole
OSBI - Arrests
OESC - Wages
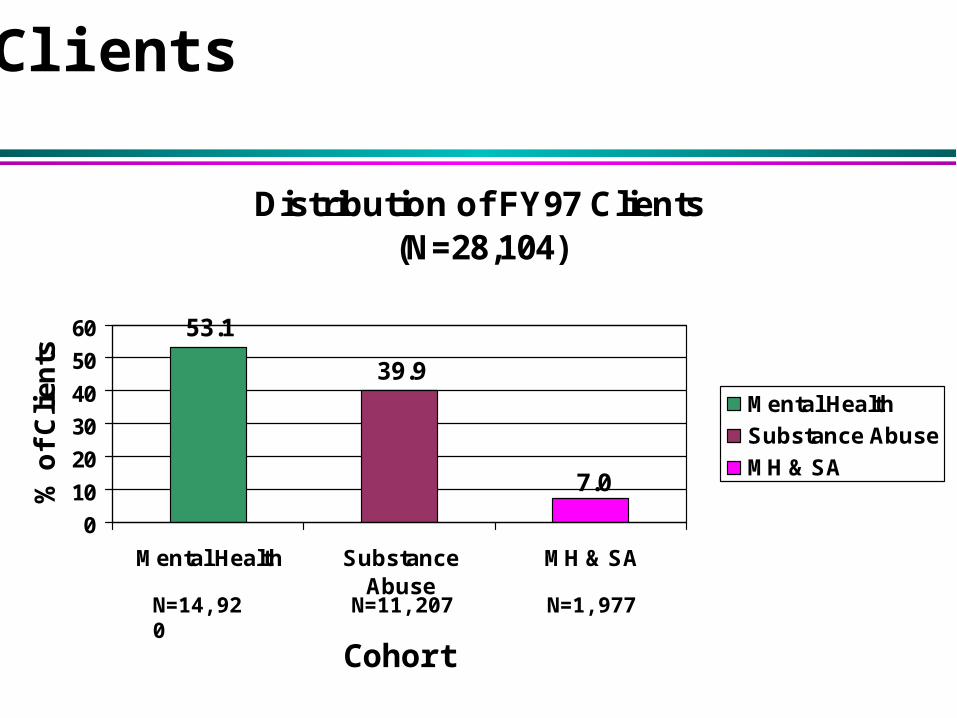
Distribution of FY97 Clients (N=28,104)
53.1
39.9
7.0
0
10
20
30
40
50
60
Mental Health SubstanceAbuse
MH & SA
% o
f C
lien
ts
Mental Health
Substance Abuse
MH & SA
N=14,920 N=11,207 N=1,977
Clients
Cohort
Clients
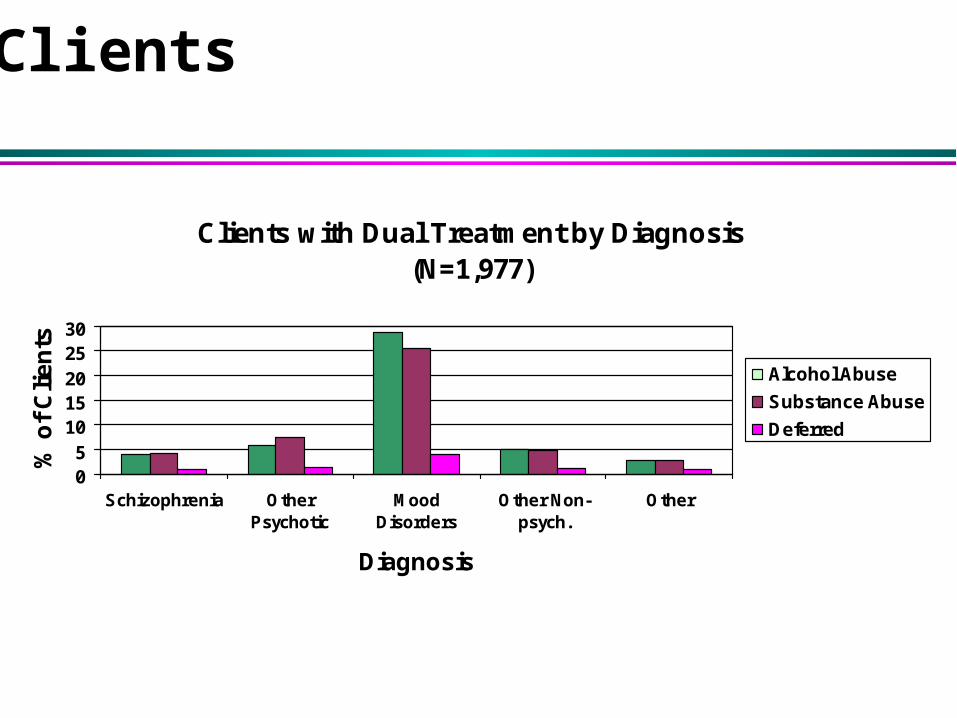
Clients with Dual Treatment by Diagnosis(N=1,977)
05
1015202530
Schizophrenia OtherPsychotic
MoodDisorders
Other Non-psych.
Other
Diagnosis
% o
f C
lie
nts
Alcohol Abuse
Substance Abuse
Deferred
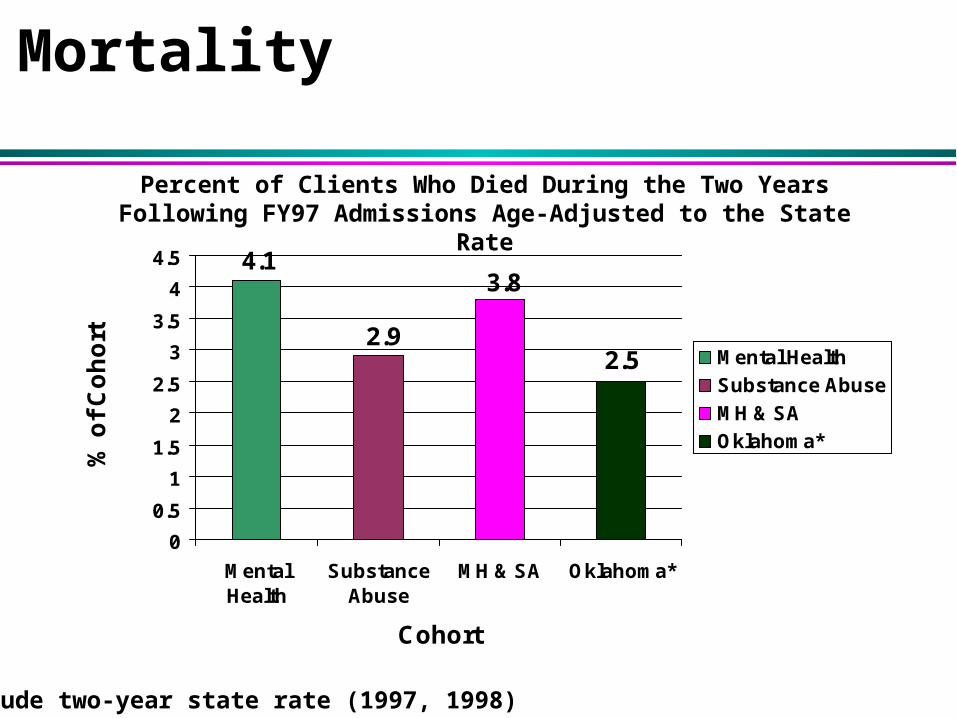
Mortality
2.5
3.8
2.9
4.1
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
MentalHealth
SubstanceAbuse
MH & SA Oklahoma*
Cohort
% o
f C
oh
ort
Mental Health
Substance Abuse
MH & SA
Oklahoma*
* Crude two-year state rate (1997, 1998)
Percent of Clients Who Died During the Two Years Following FY97 Admissions Age-Adjusted to the State Rate
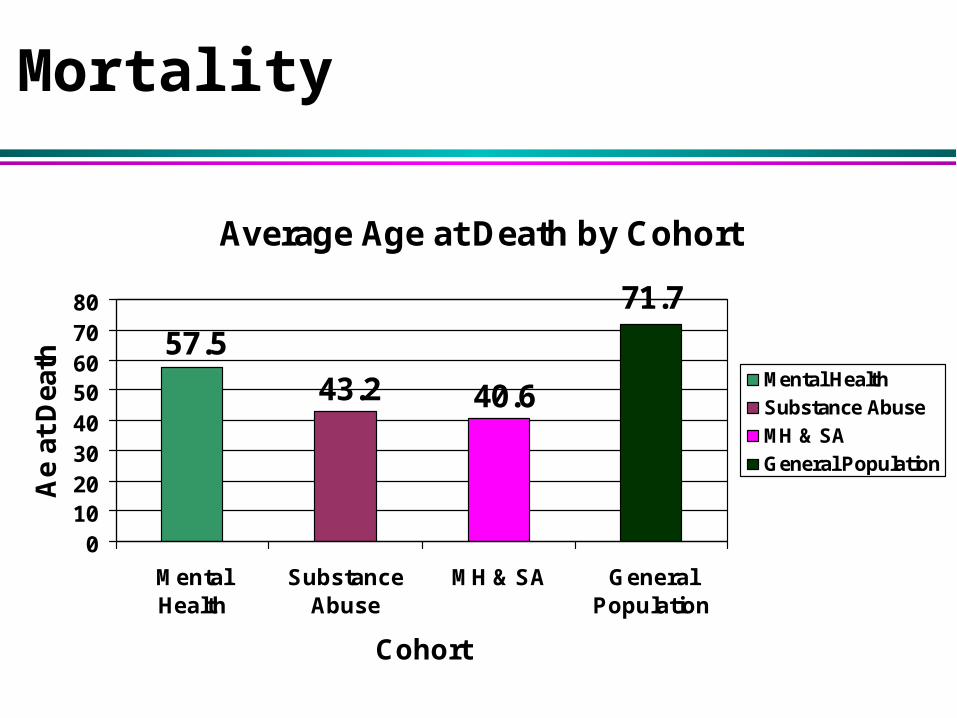
Average Age at Death by Cohort
71.7
40.6
57.5
43.2
01020304050607080
MentalHealth
SubstanceAbuse
MH & SA GeneralPopulation
Cohort
Ae
at D
eath
Mental Health
Substance Abuse
MH & SA
General Population
Mortality
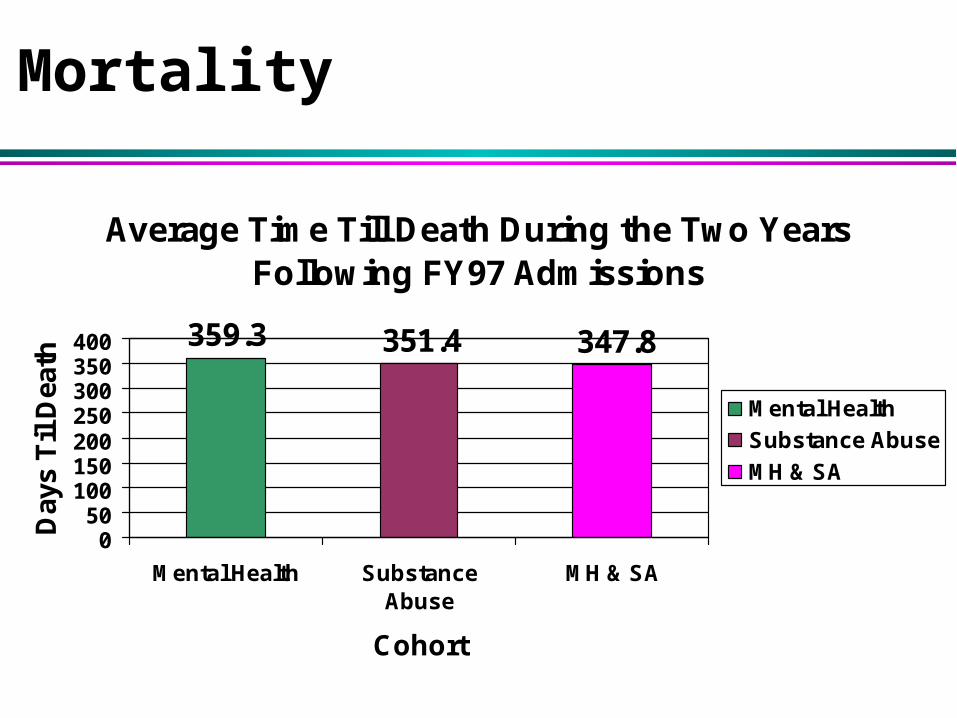
Average Time Till Death During the Two Years Following FY97 Admissions
351.4359.3 347.8
050
100150200250300350400
Mental Health SubstanceAbuse
MH & SA
Cohort
Day
s T
il D
eath
Mental Health
Substance Abuse
MH & SA
Mortality
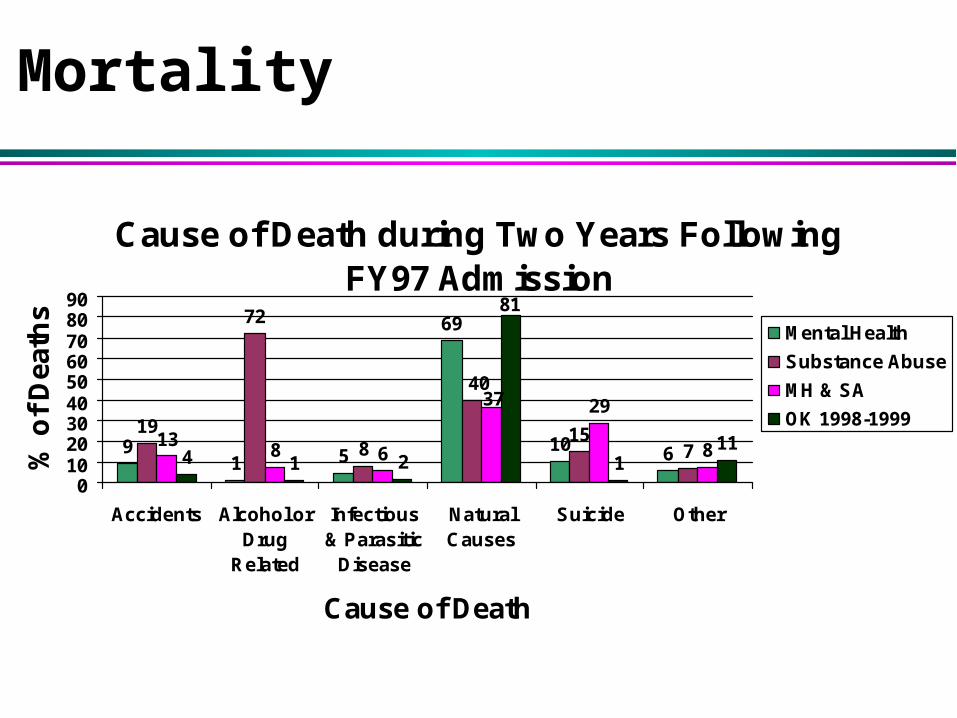
Cause of Death during Two Years Following FY97 Admission
91 5
69
10 6
19
72
815
78 6
29
84 1 2 111
40
13
37
81
0102030405060708090
Accidents Alcohol orDrug
Related
Infectious& Parasitic
Disease
NaturalCauses
Suicide Other
Cause of Death
% o
f D
eath
s
Mental Health
Substance Abuse
MH & SA
OK 1998-1999
Mortality
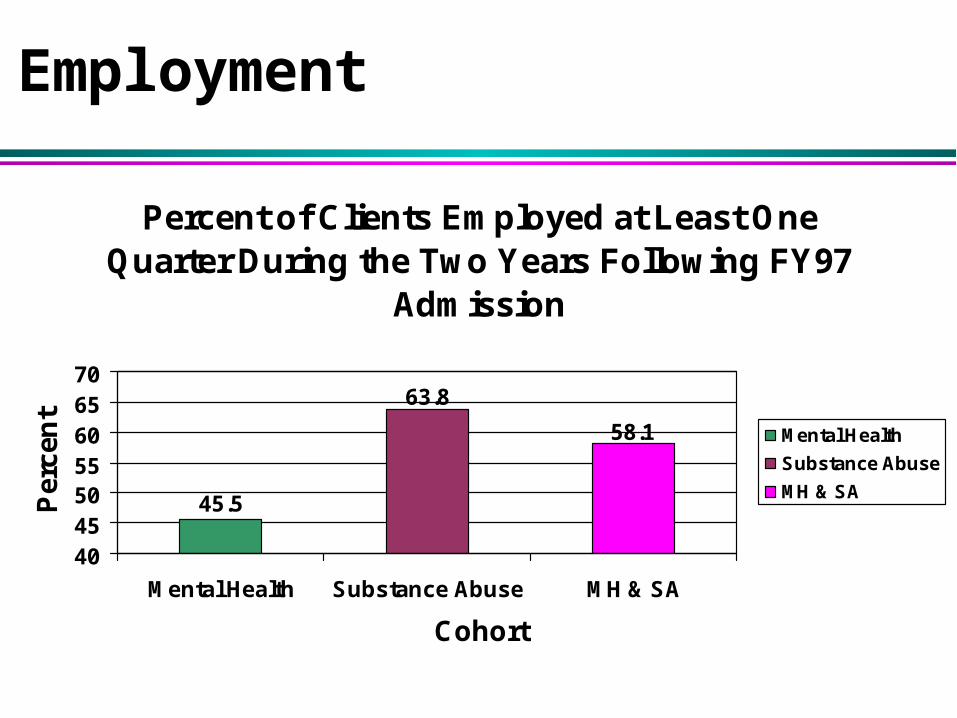
Percent of Clients Employed at Least One Quarter During the Two Years Following FY97
Admission
45.5
63.8
58.1
40455055606570
Mental Health Substance Abuse MH & SA
Cohort
Per
cen
t
Mental Health
Substance Abuse
MH & SA
Employment
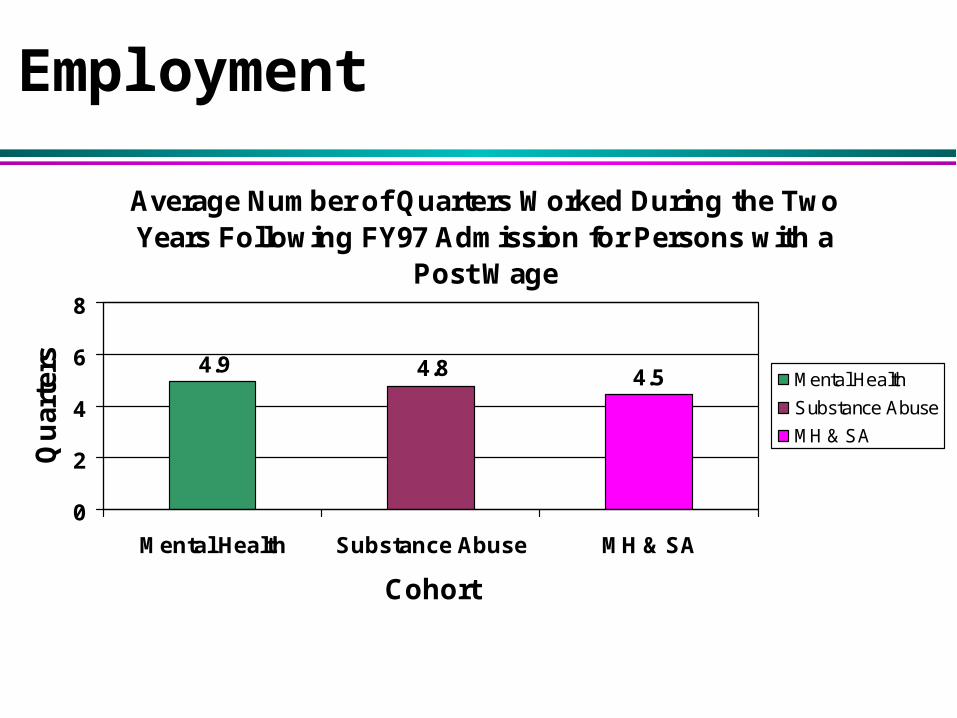
Average Number of Quarters Worked During the Two Years Following FY97 Admission for Persons with a
Post Wage
4.54.84.9
0
2
4
6
8
Mental Health Substance Abuse MH & SA
Cohort
Qu
arte
rs
Mental Health
Substance Abuse
MH & SA
Employment
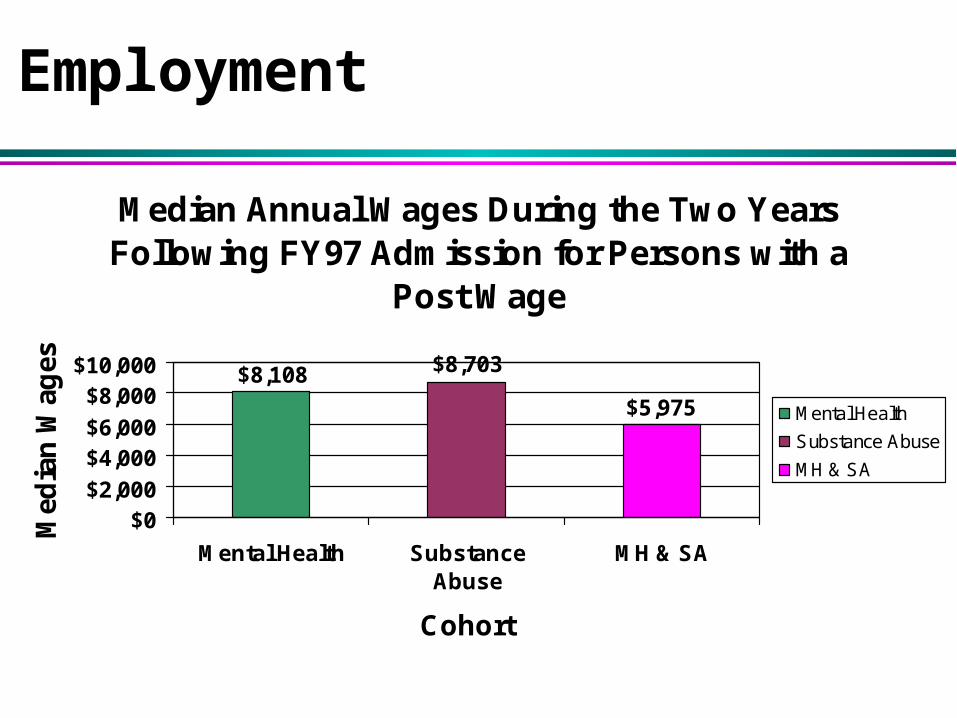
Median Annual Wages During the Two Years Following FY97 Admission for Persons with a
Post Wage
$5,975
$8,703$8,108
$0$2,000
$4,000$6,000
$8,000$10,000
Mental Health SubstanceAbuse
MH & SA
Cohort
Med
ian
Wag
es
Mental Health
Substance Abuse
MH & SA
Employment





























