Embed Size (px)
Citation preview



List of Papers
This thesis is based on the following papers, which are referred to in the text by their Roman numerals.
I Pettersson U.S., Henriksnäs J., Jansson L. (2009) Reversal of high pancreatic islet and white adipose tissue blood flow in type 2 diabetic GK rats by administration of the 3-adrenoceptor inhibitor SR-59230A. Am J Physiol Endocrinol Metab, 297(2):E490-4
II Pettersson U.S., Sandberg M., Jansson L. Two-week treat-ment with the 3-adrenoceptor antagonist SR59230A norma-lizes the increased pancreatic islet blood flow in type 2 diabet-ic GK rats. Submitted
III Pettersson U.S., Christoffersson G., Massena S., Ahl D., Jans-son L., Henriksnäs J., Phillipson M. (2011) Increased recruit-ment but impaired function of leukocytes during inflammation in mouse models of type 1 and type 2 diabetes. PLoS One. 6(7):e22480
IV Pettersson U.S., Waldén T.B., Carlsson P-O., Jansson L., Phillipson M. Female C57Bl/6 Mice are Protected against High-Fat Diet-Induced Signs of Metabolic Syndrome due to Anti-inflammatory Actions in Visceral Adipose Tissue. Submitted
Reprints were made with permission from the respective publishers.

Supervisors: Mia Phillipson, Docent Integrative physiology, Department of Medical Cell Biology Uppsala University Leif Jansson, Professor Department of Medical Cell Biology Uppsala University Johanna Henriksnäs, PhD Department of Medical Cell Biology Uppsala University Opponent: Mikael Rydén, Docent Department of Medicine Karolinska Institute Members of the examining committee: Lennart Lindbom, Professor, Karolinska Institute Christian Berne, Professor, Uppsala University Anders Tengholm, Docent, Uppsala University

Contents
Introduction ..................................................................................................... 9 The adipose tissue ...................................................................................... 9 The islets of Langerhans .......................................................................... 11 Diabetes mellitus ...................................................................................... 12 The immune system and inflammation .................................................... 13
Inflammation in obesity and type 2 diabetes ....................................... 14 Adipose tissue macrophage subtypes in obesity .................................. 15
The sympathetic nervous system .............................................................. 15 Gender aspects of type 2 diabetes ............................................................ 16
Aims .............................................................................................................. 18
Methodology ................................................................................................. 19 Animals (study I-IV) ................................................................................ 19
Rats (study I and II) ............................................................................. 19 Mice (study III and IV) ........................................................................ 19
Blood measurements ................................................................................ 20 Plasma glucose measurements (study I-IV) ......................................... 20 Glucose tolerance test (study II, III and IV) ........................................ 20 Serum concentration measurements (study I-IV) ................................ 20
Blood flow measurements (study I, II and IV) ......................................... 20 Leukocyte recruitment in vivo (study III) ................................................. 22 Bacterial clearance and phagocytosis (study III) ...................................... 23 Islet isolation and islet function (study I, II and IV) ................................ 23 Macrophage staining (study III-IV) ......................................................... 24 Gene expression (study I and IV) ............................................................. 24 Statistical analysis (study I-IV) ................................................................ 25
Study design .................................................................................................. 26 Study I ...................................................................................................... 26 Study II ..................................................................................................... 26 Study III ................................................................................................... 27 Study IV ................................................................................................... 27
Results and Comments .................................................................................. 28 Study I ...................................................................................................... 28 Study II ..................................................................................................... 29

Study III ................................................................................................... 30 Study IV ................................................................................................... 34
Discussion ..................................................................................................... 36 Of mice and men ...................................................................................... 36 Islet blood flow in relation to endocrine function .................................... 37 Autonomic innervation of islets and adipose tissue ................................. 38 Leukocytes and hyperglycemia ................................................................ 39 Adipose tissue inflammation .................................................................... 41 Does gender matter? ................................................................................. 43
Conclusions ................................................................................................... 44
Future perspectives ....................................................................................... 45
Populärvetenskaplig sammanfattning ........................................................... 46 Bakgrund .................................................................................................. 46 Delarbete I och II ...................................................................................... 46 Delarbete III ............................................................................................. 47 Delarbete IV ............................................................................................. 47
Acknowledgements ....................................................................................... 49
References ..................................................................................................... 52

Abbreviations
ANOVA Analysis of variance between groups ATM Adipose tissue macrophages BAT Brown adipose tissue BMI Body mass index CD4 Cluster of differentiation 4 CD8 Cluster of differentiation 8 CT values Threshold cycle values ELISA Enzyme-linked immunosorbent assay Foxp3 Forkhead box P3 GK rat Goto-Kakizaki rat GTT Glucose tolerance test HFD High-fat diet IL-1 Interleukin-1 IL-6 Interleukin-6 IL-8 Interleukin-8 IL-10 Interleukin-10 LPS Lipopolysaccharides M1 Classical macrophages M2 Resident macrophages MCP-1 Monocyte chemotactic protein-1 MGL-1 Macrophage galactose-type C-type lectin-1 MIP-2 Macrophage inflammatory protein -2 mKC Murine keratinocyte-derived chemokine MPO Myeloperoxidase NETs Neutrophil extracellular traps NF- B Nuclear factor kappa-light-chain-enhancer of activated B-cells PBS Phosphate buffered saline ROS Reactive oxygen species SEM Standard error of the mean SVF Stromal vascular fraction TNF- Tumor necrosis factor- Treg Regulatory T-lymphocyte WAT White adipose tissue WF rat Wistar-Furth rat WHO World Health Organization


9
Introduction
During evolution organisms have developed mechanisms for storage of energy to be used when food is scarce. A modern life style in the Western world during the 21st century is characterized by an almost unlimited food supply, a sedentary job and decreased physical activity. These factors pro-mote weight gain and contribute to the obesity epidemic. The World Health Organization (WHO) estimated that there were 1.5 billion overweight adults in 2008, of which 200 million men and nearly 300 million women were ob-ese [1]. Obesity is associated with several other conditions including cardi-ovascular diseases, type 2 diabetes mellitus, and hypertension all of which increase the risk for premature death, and this associated morbidity also im-pose a great economic burden on society [2,3,4].
The adipose tissue Adipose tissue used to be considered only as a more or less inert reservoir of triglycerides which subsequently can be broken down into free fatty acids and glycerol to provide fuel for metabolism. However, it has more recently been recognized to also constitute the largest endocrine organ in the body, with an important role in general metabolism [5,6,7]. Adipose tissue can traditionally be divided into white adipose tissue (WAT) and brown adipose tissue (BAT). From a functional and anatomical point of view, WAT can be further subdivided into subcutaneous and intra-abdominal WAT. Subcutane-ous adipose tissue depots are located directly beneath the skin in the hypo-dermis and are represented by inguinal and interscapular fat in the present studies, whereas intra-abdominal adipose tissue are found within the perito-neal cavity and constitutes e.g. the perirenal, pancreatic, sternal, gonadal, and retroperitoneal fat [8]. Visceral adipose tissue is the part of the intra-abdominal depots which is drained by the portal vein [9].
WAT is composed of adipocytes, with a size of ~50-200 µms depending on their triglyceride stores, and a stromal vascular fraction (SVF). The latter consists of e.g. resident macrophages, endothelial cells, fibroblasts, pre-adipocytes, and various blood cells [10] (Figure 1.). The adipose tissue un-dergoes constant remodeling due to maturation of pre-adipocytes, balance between triglyceride storage and lipolysis, and angiogenesis.

10
BAT is located in the interscapular region in rodents and is also found, though less abundantly, in the neck and upper-chest regions of humans [11,12,13,14]. BAT is more related to muscle tissue than to WAT [14] and contains smaller multivacuolar adipocytes compared to WAT. It is well vas-cularized and contains abundant mitochondria. The main function of BAT is suggested to be thermogenesis, in which the adipocytes release heat [14,15].
The endocrine function of adipose tissue is mediated through release of several metabolically active factors, referred to collectively as adipokines [16]. They consist of growth factors as well as cytokines, i.e. small proteins mediating signaling between cells. Several adipokines are released locally as well as systemically, thereby regulating or modulating many processes re-lated to metabolism, energy storage, inflammation, immune function, and vascular homeostasis [17,18,19,20] (Table 1).
In obesity, usually defined as a body mass index (BMI) >30, adipose tis-sue expands by increasing the adipocyte cell mass, which can occur either by increased number (hyperplasia) and/or size (hypertrophy) of cells. However, the number of adipocytes is relatively constant during life and it is mainly the accumulation of triglycerides in the individual cells that enlarges the adipose tissue in an individual [21] (Figure 1.). Expansion of adipose tissue influences WAT microcirculation since adipose tissue growth per se creates hypoxia which stimulates angiogenesis [22].
Obesity is strongly correlated with several other conditions including type 2 diabetes, since the adipose tissue is a major contributor to the insulin resis-tance present in this disease [2,3,4].
Figure 1. Schematic illustration of adipose tissue in the normal and obese state, including adipocytes, vascular network, and infiltrating immune cells. Normal adi-pose tissue is enriched with the anti-inflammatory adipokine adiponectin, whereas adipose tissue in obesity is enriched with pro-inflammatory cytokines, e.g. resistin and IL-6. Illustration modified from the original by J. Hübinette.

11
Table 1. Source and function of some adipokines in rodents
Adipokine Primary source Function
Adiponectin Adipocytes Anti-inflammatory, insulin-sensitizer [7]Resistin Adipocytes Promotes insulin resistance through release of TNF-
and IL-6 from macrophages [23]Leptin Adipocytes Appetite and metabolism control [6]IL-6 Adipocytes, SVF Inflammation [24]TNF- Adipocytes, SVF Inflammation, antagonist of insulin signaling [5] MCP-1 Adipocytes, SVF Monocyte recruitment [25]IL-6 = interleukin-6, TNF- = tumor necrosis factor- , MCP-1 = monocyte chemotactic protein-1 SVF = stromal vascular fraction.
The islets of Langerhans Insulin producing -cells are situated within the islets of Langerhans in the pancreas. Rodent islets are 100-400 µm in diameter and are scattered throughout the parenchyma. The vast majority of islet cells are -cells, which are mainly located in the islet core, whereas the islet mantle consists of other hormone-producing cells, such as -, -, and pancreatic polypep-tide cells. Apart from the hormone-producing cells the islet also contains nerves, endothelial cells, fibroblasts, macrophages, and dendritic cells [26].
Insulin is released from the -cells in response to glucose and is the only hormone able to decrease plasma glucose levels. When released to the circu-lation, insulin achieves this effect by increasing the glucose uptake in target cells in peripheral tissues and inhibiting hepatic glucose production.
In order to register changes in plasma glucose concentrations and release insulin in appropriate quantities, the endocrine islets depend on a dense ca-pillary network and high blood perfusion (Figure 2.).
The islets constitute only 1-2% of the total pancreas, but receive a blood supply which corresponds to ~10% of the whole pancreatic blood perfusion [27,28]. Blood flow is controlled by metabolic and islet endothelium-derived substances such as glucose, endothelin-1, adenosine, and nitric oxide, as well as the autonomic nervous system [29,30]. Interestingly, the islet blood flow seems to be selectively increased early during the course of impaired glucose tolerance and overt type 2 diabetes [31].

12
Figure 2. Confocal image of islet vascular network with two arteriols and a venole. Vessels are stained by intra-arterial injection of fluorescently labeled CD31 monoc-lonal antibody in anesthetized mouse. Arrows indicate direction of blood flow. The original image is kindly provided by G. Christoffersson.
Diabetes mellitus The inability to decrease elevated plasma glucose concentrations results in diabetes mellitus. Even though it is a heterogeneous disease, it is usually divided into two major forms. Type 1 diabetes is caused by a selective de-struction of the insulin-producing -cells in the islets. This results in a com-plete insulin deficiency requiring lifelong treatment with insulin. Type 2 diabetes constitutes 90% of all cases of diabetes in the Western world and is characterized by an inadequate insulin production due to a defective
-cell function, often associated with peripheral insulin resistance. The -cell defect develops gradually with an initial compensation for the increased demand of insulin, which later fails due to glucotoxiticity caused by hyper-glycemia, as well as lipotoxiticity and amyloid formation within the islet [32]. The insulin resistance is usually due to a post-receptor defect and can be associated with either hypo- or hyperinsulinemia. The hyperglycemia in type 2 diabetes is mainly caused by the insulin resistance, leading to im-paired glucose uptake in skeletal muscle and fat [33], as well as a decreased suppression of the hepatic gluconeogenesis and glycogenolysis, which re-sults in increased glucose output from the liver and elevated plasma glucose levels [34]. Both environmental factors and genomic regions have been iden-tified as markers for increased risk for developing diabetes [35,36].
Type 2 diabetes in humans is also associated with several other conditions such as obesity, hypertension, and dyslipidemia [2]. When occurring togeth-er this is often referred to as the metabolic syndrome [37]. However, the

13
existence of the metabolic syndrome is a matter of some debate [38] and is mostly used in human studies.
Despite the fact that both types of diabetes can be treated, many of the pa-tients eventually develop endothelial dysfunction probably due to prolonged hyperglycemia, which contributes to micro- and macrovascular complica-tions [2,39,40]. The microvascular complications results in nephropathy, neuropathy, and retinopathy whereas macrovascular complications cause e.g. coronary arterial disease, peripheral arterial disease, and stroke. The severity of the complications correlates to how well plasma glucose levels can be normalized throughout the course of the disease [40].
The immune system and inflammation The immune system plays a profound role in both health and disease. It serves as a defense against pathogens, but can also become harmful for the host if unduly activated or if it leads to a chronic inflammation. The immune system contains of an innate and an adaptive branch. The former is rapidly initiated and the cellular components consist of phagocytic leukocytes, i.e. granulocytes and monocytes, which transmigrate from the blood to the in-fected area to kill and phagocyte pathogens. Granulocytic neutrophils consti-tute ~60% of all circulating leukocytes in human blood but only ~10% in mice [41]. Macrophages are the most efficient phagocytic cell of our im-mune system and differentiate in tissue from transmigrated monocytes. Be-sides the cellular components, the innate immune system includes several so-called Pattern Recognition Receptors such as Toll-like receptors and the complement system which play important roles, but will not be discussed further in this thesis.
The adaptive immune system consists mainly of T- and B-lymphocytes which adapt their responses towards specific antigens through interactions with antigen presenting cells, e.g. macrophages and dendritic cells. T-cells can further be functionally divided into helper (CD4+), killer (CD8+) and regulatory (CD4+CD25+Foxp3+) cells. The regulatory T-cells (Treg) consist of 5-20% of all CD4+ T-cells [42] and their main function is to suppress the immune system in order to maintain homeostasis in the tissue [43].
To initiate an acute inflammatory response, leukocytes migrate from the vessel lumen into the affected tissue. This occurs in series of events referred to as the leukocyte recruitment cascade (Figure 3.). In general, adhesion molecules such as E-selectin and P-selectin on endothelial cells in postcapil-lary venules are upregulated by chemokines, which are released from the site of inflammation. Circulating, marginated leukocytes begin to roll along the vessel wall through interactions i.e. between the L-selectin and P-selectin glycoprotein ligand 1 and their ligands on endothelial cells. Integrin activa-tion on leukocytes results in firm adhesion to immunoglobulins on the endo-

14
thelium, allowing the leukocytes to crawl along the vessel wall to optimal sites for transmigration and enter the tissue [44,45,46].
Phagocytes, such as macrophages and neutrophils, as well as T- and B-cells, express chemokine receptors on their surface. The binding of chemo-kines, which are chemotactic cytokines released from various cells, to these receptors induce cellular activation and locomotion of immune cells towards sites of inflammation.
Figure 3. Schematic illustration of the leukocyte recruitment cascade.
Inflammation in obesity and type 2 diabetes Obesity is associated with a low-grade, general inflammation in the body, especially manifest in WAT, which increases the risk for insulin resistance and type 2 diabetes [47]. Plasma concentrations of both pro-inflammatory cytokines and adipokines increase with obesity and are believed to contri-bute to the low-grade inflammation (Figure 1). However, the origin of this systemic inflammation was uncertain until the 1990s when it was discovered that adipocytes express the inflammatory cytokine tumor necrosis factor- (TNF- ) and that the expression is increased in obese animal models [5]. During this century, Crook et al and Pickup et al demonstrated that type 2 diabetes in humans could be an inflammatory condition as evidenced by increased inflammatory markers in plasma [48,49]. Since then, several stu-dies have confirmed these data in humans [39,47,50,51,52].
The present day view is that the inflammation in adipose tissue in obesity is due to a cross-talk between the innate and adaptive immune system. Adi-pocytes along with macrophages are the main cells releasing pro-

15
inflammatory mediators such as TNF- and interleukin-6 (IL-6) but T-cells also release pro-inflammatory cytokines. The number of Treg on the other hand declines with obesity, which may prevent suppression of the local in-flammation [42].
Besides the low-grade inflammation in adipose tissue, there is also an in-flammation process within the islets present in patients suffering from type 2 diabetes. The inflammation seems to contribute, together with glucotoxiticity and amyloid formation, to -cell death and defect insulin secretion in these patients [53]. Further, increased blood flow is one sign of inflammation and has been found in islets of animal models of diabetes [31], which suggest that islet inflammation is present.
Adipose tissue macrophage subtypes in obesity As mentioned above, macrophages infiltrating the adipose tissue during ob-esity are important for the local inflammation [54,55]. Macrophages can be divided into different functional subtypes based on surface markers and phe-notypic differences. In general, macrophages are either inflammatory ‘clas-sically activated’ (M1 phenotype) or ‘alternatively activated’ resident (M2 phenotype). Adipose tissue in lean animals or humans is enriched in resident macrophages to maintain normal tissue function by removing dead or dying cells and initiate angiogenesis, but also to attenuate inflammation and in-crease insulin sensitivity via local release of the insulin-sensitizing cytokine IL-10 [56]. Further, it has recently been shown that resident macrophages release catecholamines to stimulate thermogenic gene expression and lipoly-sis in BAT and WAT, respectively [57]. The ‘classically activated’ macro-phages produce high levels of pro-inflammatory cytokines and are mostly absent in adipose tissue in lean persons, but are increased via recruitment during obesity. They promote inflammation and insulin resistance via the release of e.g. TNF- and IL-1 [54,55]. The release of these cytokines acti-vates intracellular inflammatory regulators, which stimulate pro-inflammatory transcription factors, such as activator protein 1 (c-Jun/Fos) and NF- B. This results in a serine phosphorylation of the insulin receptor substrate, which impairs insulin actions [58].
The sympathetic nervous system The sympathetic nervous system represents part of the autonomic nervous system and regulates the fight-or-flight stress response together with the adrenal glands. During the stress response, catecholamine release increases heart rate and contractility, resulting in increased cardiac output. Norepi-nephrine is the major neurotransmitter of the sympathetic nervous system and binds to both - and -adrenoceptors. The sympathetic nervous system is

16
an important regulator of energy expenditure, where the -adrenoceptors stimulate lipolysis, whereas the -adrenoceptors act inhibitory in this respect [59,60,61] (Table 2). The sympathetic nervous system is usually overactive in disorders such as obesity and hypertension [62]. WAT and the islets of Lan-gerhans are richly innervated by sympathetic and parasympathetic nerves, as well as sensory nerves [63,64]. The high innervation of islets regulates hor-mone secretion from the various endocrine cells [63].
Both WAT and BAT in rats express primarily the 3-adrenoceptor sub-type [65], a G-protein-coupled receptor, which mediates effects on energy metabolism and lipolysis [59,61]. Under normal conditions this receptor has higher affinity to norepinephrine than epinephrine and might be important in the adipose tissue blood flow regulation. The receptor is also expressed in the islet of Langerhans, primarily on the -cells, but also on vascular cells [66,67].
The sympathetic nervous system has been long known to affect insulin secretion from the -cells, but also to modulate blood perfusion to islets [27,68,69]. Stimulation with the 3-adrenoceptor agonist CL-316243 in rats increased both islet blood flow and insulin secretion [70]. However, the ef-fects of inhibition of 3-adrenoceptors using a specific antagonist such as SR59230A, has never been investigated [71,72].
Table 2. Adrenergic receptor subtypes and their effects during stimulation in islets and white adipose tissue (WAT) Receptor subtype -cells Islet blood flow WAT
1 Insulin secretion [73] Lipolysis [74]
2 Insulin secretion [73] Islet blood flow [27] Lipolysis [60]
1 Lipolysis [60]
2 Insulin secretion [75] Islet blood flow [76] Lipolysis [60]
3 Insulin secretion [70] Islet blood flow [70] Lipolysis [59]
Gender aspects of type 2 diabetes The correlation between increased WAT and type 2 diabetes critically de-pends on the anatomic location of fat [77]. As mentioned above, WAT can be divided into visceral and subcutaneous adipose depots. Women usually accumulate subcutaneous adipose tissue in the gluteofemoral region, whe-reas men accumulate visceral adipose tissue in the abdominal/visceral region [78]. The latter is associated with hypertension, type 2 diabetes, insulin resis-tance and dyslipidemia [77]. The best way to reduce the risk to develop these conditions is by weight reduction. The prevalence of type 2 diabetes is in-creased in postmenopausal compared to premenopausal women [79] and this is probably associated with low estrogens levels. The estrogen receptor is

17
expressed both in WAT and within the islets and might stimulate insulin secretion through uncertain mechanisms [80,81]. Estrogen display anti-diabetic actions and estrogen replacement therapy seems to maintain -cell function intact and protect against visceral adipose tissue accumulation [81,82] although the mechanisms are not fully understood.

18
Aims
Type 2 diabetes is characterized by simultaneously occurring insulin resis-tance, often caused by a general, low-grade inflammation and an inherent -cell defect. The overall aim of the studies included in this thesis was to eva-luate the role of blood flow and inflammation in animal models of diabetes. More specifically, we aimed to examine pancreatic islet and adipose tissue blood perfusion after acute
and long-term inhibition of 3-adrenoceptors in control and type 2 di-abetic rats.
evaluate if hyperglycemia in alloxan- and high-fat diet-treated mice in-fluence leukocyte recruitment in models of acute inflammation.
investigate possible gender differences in mice on a high-fat diet with respect to obesity, hyperinsulinemia, systemic inflammation, and islet blood perfusion.

19
Methodology
Animals (study I-IV) All animals had free access to water and pelleted food (Type R36, Lantmännen, Kimstad, Sweden). All experiments were approved by the Swedish Laboratory Animal Ethical Committee in Uppsala, Sweden.
Rats (study I and II) Male Wistar-Furth (WF) and Goto-Kakizaki (GK) rats aged 3-4 months were used in study I and II. The GK rat is a nonobese substrain of Wistar rat origin with a concomitant insulin resistance and islet -cell defect, fulfilling both criteria of being a type 2 diabetes model [83,84]. The model was estab-lished via repeated inbreeding of Wistar rats with impaired glucose tolerance [85]. The WF rat was used as control. The animals were purchased from Taconic (Ry, Denmark) except some GK rats in study II which were pur-chased from Taconic (Germantown, NY, USA).
Mice (study III and IV) In study III and IV C57BL/6 mice weighing 25-30 g, purchased from Scan-bur B&K (Stockholm, Sweden) or Taconic (Ry, Denmark) were used.
Alloxan-induced diabetes (study III) To induce marked hyperglycemia (>28 mmol/l) and hypoinsulinemia, mice were injected intravenously with alloxan (75 mg/kg body weight, Sigma-aldrich, St. Louis, MO, USA) 3 days before the intravital microscopy expe-riments or inoculation of bacteria. A differential blood count was performed to exclude that alloxan affected leukocyte subtype populations.
High-fat diet (study III and IV) C57BL/6 mice were given high-fat diet (HFD; 60% kcal from fat, Research Diets, New Brunswick, USA) for 16 weeks (study III) or 14 weeks (study IV). Body weight and plasma glucose concentrations were registered week-ly.

20
Blood measurements Plasma glucose measurements (study I-IV)
Plasma glucose levels were measured in blood from the tip of the tail with test reagent strips (detection range 1.1 – 27.8 mmol/l; Freestyle, Abbott, Stockholm, Sweden) during diet intake (III and IV), before injection of mi-crospheres (study I, II and IV), and before in vivo microscopy in the alloxan- and HFD-induced diabetes models (study III). Plasma glucose was also measured before and after anesthesia with isoflurane in the intravital micro-scopy experiments (study III).
Glucose tolerance test (study II, III and IV) To evaluate metabolic disturbances, glucose tolerance tests (GTT) were per-formed in rats before and after the 2-week treatment with SR59230A (study II) and in mice >14 weeks after commencing control diet or HFD (study III and IV). Animals were weighted and plasma glucose levels were measured in blood from the tip of the tail using test reagent strips before injection of 2 g/kg body weight D-glucose (300 mg/ml; Fresenius Kabi, Uppsala, Swe-den) intraperitoneally (II and IV) or intravenously (study III). Plasma glu-cose levels were then measured frequently after 10 (study III) or 15 (study II and IV), as well as 30, 60, and 120 min later.
Serum concentration measurements (study I-IV) Serum insulin concentrations were measured in rats (study I and II) or in mice after >14 weeks on control or HFD (study III and IV) with insulin ELISA (Mercodia Rat Insulin ELISA, Uppsala, Sweden) according to manu-facturer’s instructions. Serum concentrations of cholesterol and triglycerides (Architect c4000; Abbott Laboratories, Abbott Park, IL, USA), and inflam-matory markers (Mouse Pro-inflammatory 7-Plex Assay Ultra-Sensitive Kit; Mesoscale, Gaithersburg, MD, USA) were measured in male and female mice on control diet or HFD (study IV).
Blood flow measurements (study I, II and IV) Animals were anaesthetized by an intraperitonial injection of thiobutabarbit-al sodium (rats, 120 mg/kg body weight; Inactin; Sigma-Aldrich) or by aver-tin (mice, 2.5% [vol/vol] solution of 10 g 97% [vol/vol] 2,2,2-tribromoethanol [Sigma-Aldrich] in 10 ml 2-methyl-2-butanol [Kemila, Stockholm, Sweden]) and placed on a servo-controlled heated operating table to maintain body temperature at ~38°C. Animals were tracheostomized to facilitate respiration and polyethylene catheters were inserted into the

21
ascending aorta via the right carotid artery and into the left femoral artery. The carotid catheter was connected to a pressure transducer (PDCR 75/1; Druck, Groby, U.K). In study I, SR59230A was administered intravenously 10 min before blood flow measurements. To measure organ blood perfusion in the animals, a microsphere technique was used (Figure 4.). Briefly, ~1.5 x 105 black non-radioactive microspheres (EZ-Trac; Triton microspheres, San Diego, CA, USA) with a diameter of 10 µm (for studies of islet, pancreatic, intestinal, renal and adrenal blood flow) or 15 µm (for studies of adipose tissue blood flow) were injected through the catheter with its tip in ascending aorta for 5 seconds. Starting 5 seconds before the microsphere injection, and continuing for a total of 60 seconds, an arterial blood sample was collected by free flow from the catheter in the femoral artery (~ 0.5 ml/min). The exact withdrawal rate was confirmed in each experiment by weighing the sample. Animals were killed and adrenal glands were removed, blotted and weighed. Samples (~40-100 mg) from the colon, duodenum, pancreas, and kidney were also taken from the animals injected with 10-µm microspheres. To study adipose tissue blood flow, 15-µm microspheres were used. Note that this size of microspheres is used for blood flow measurements in these tis-sues, since smaller microspheres are shunted through adipose tissue micro-vessels. Samples from intra-abdominal WAT consisted of the retroperitoneal fat, pancreatic fat, perirenal fat, epididymal fat, and fat from the posterior surface of the xiphoid process (sternal fat), whereas subcutaneous WAT were taken from the inguinal part of the abdominal wall and interscapular region on the back. BAT was sampled from the interscapular region.
The number of microspheres in the samples above, including pancreatic islets, was visualized and counted by a freeze-thawing technique as pre-viously described [86]. Organ blood flow values were calculated according to the formula below.
Qorg is the organ blood flow (ml/min); Qref is the withdrawal rate of the refer-ence sample (ml/min); Norg is the total number of microspheres present with-in the organ, and Nref is the total number of microspheres present in the ref-erence sample.
The organ blood flow was expressed in ml/min x g tissue whereas the is-let perfusion was expressed as µl/min x g pancreas or as µl/ min x islet mass. Blood flow values based on the microsphere content of the adrenal glands were used to confirm that the microspheres were adequately mixed in the circulation. A difference less than 10% for both sizes of microspheres in the blood flow values between the two glands within each animal was taken to indicate sufficient mixing.

22
Figure 4. Schematic picture of blood flow measurements using the microsphere technique. Microspheres are injected into ascending aorta. Simultaneously, an arteri-al blood sample is collected from the femoral artery as a reference organ blood flow. Loss of fluid during the experimental period is supplemented with saline solution through the catheter in the femoral vein.
Leukocyte recruitment in vivo (study III) Intravital microscopy was used to study the leukocyte recruitment in venules of the cremaster muscle in normoglycemic as well as alloxan- and HFD-treated mice. The muscle was prepared as previously described [46,87] in mice anesthetized by spontaneous inhalation of isoflurane (Forene, Abbott) gas through a breathing mask. Briefly, the cremaster muscle was dissected free from other tissues, opened longitudinally with electric cautery and held flat on an objective glass by attaching five sutures in the corners of the tis-sue, whereafter it was constantly superfused (1 ml/min) with pre-warmed bicarbonate buffered saline (pH 7.4) throughout the experiment. After a rest-ing period of 30 min, a cremasteric venule with a diameter of ~25-35 µm was selected and a 5-minute period of blood flow was recorded through an intra vital microscope (Leica Microsystems DM5000B, Wetzlar, Germany) with a CCD camera (Hamamatsu Orca-R2, Hamamatsu City, Japan) con-nected to a computer with Volocity 5.0 Acquisition software. After the first recording period of basal recruitment after surgical stimulation, 0.5 nmol/l of the chemokine macrophage inflammatory protein-2 (MIP-2, CXCL2; R&D Systems, UK) was added to the superfusate throughout the remainder of the experiment. MIP-2 is an IL-8 murine homologue which binds the CXCR2 receptor and recruits mainly neutrophils [87]. Five-minute periods were rec-orded before and at 30, 60, and 90 min after MIP-2 addition. The number of rolling leukocytes was counted during the 5-minute period and the total number of rolling leukocytes per min was calculated. The cell velocity of the first ten rolling cells during each observation period was calculated. Also, the number of adherent leukocytes (stationary for >30 sec) in a 100 µm long venule, as well as the number of emigrated cells in the field of view (200 µm x 300 µm, 0.06 mm2) were analyzed.

23
Bacterial clearance and phagocytosis (study III) In order to study bacterial clearance in alloxan-treated (plasma glucose >28 mmol/l) and control mice, luminescent bacteria were inoculated subcu-taneously. Briefly, the fur on the back of the mice was removed using both shaver and application of depilator cream (Veet Reckitt Benckiser, Valora Trade Sweden) during spontaneous inhalation of isoflurane (Forene, Abbott) 24 hours before the bacteria inoculation. Bioluminescent Staphylococcus aureus strain Xen29 (Caliper life scienses, Alameda, USA) was cultured in LB-medium containing 200 µg/ml Kanamycin overnight. On the following day, a subculture was made and incubated ~1 hour until bacteria reached exponential growth level measured by spectrophotometry (OD600 = 0.5 ~1.4x108 CFU/ml). The bacteria were washed and diluted in PBS supple-mented with 10 mg/ml Cytodex Beads (Sigma Aldrich) used as a carrier. A total of 1 x106 bacteria in 100 µl PBS solution were inoculated subcutane-ously in anesthetized alloxan-treated or control mice. Bacterial clearance was monitored in isoflurane anesthetized mice using a Xenogen bioimaging device (IVIS Spectrum, Caliper Life Sciences, Hopkinton, USA) at 0, 2, 5, 12, and 24 hour and then every 24 hour for the next 14 days. Images were analysed and luminescence quantification was made using Living Image® 3.1 software (Caliper).
One part of the bacteria-infected mice was killed two days post-inocculation for myeloperoxidase (MPO) measurements using MPO ELISA (Hycult biotec, Uden, Netherlands). The remaining animals were stained for macrophages in the infected areas using Alexa Fluor555-conjugared F4/80 antibody.
Phagocytosis was analyzed using LPS-coated fluorescent beads (Polys-cience, Eppelheim, Germany) injected intraperitoneally in control or allox-an-treated mice followed by isolation of recruited leukocytes via peritoneal lavage three hours later. Leukocytes were isolated using percoll gradient isolation as previously described [88]. Total populations of phagocytic leu-kocytes as well as percentage of the population containing beads were de-termined using flow cytometry (FACScalibur, BD Biosciences).
Islet isolation and islet function (study I, II and IV) Islets were isolated by collagenase digestion as previous described [89]. Groups of 100-150 islets were cultured for two days (study II and IV) in 5 ml of RPMI 1640 culture medium (Sigma-Aldrich) supplemented with 11 mmol/l D-glucose, 2 mmol/l L-glutamine (Sigma-Aldrich), and 10% (vol/vol) fetal calf serum (Sigma-Aldrich) in 95% air/5% CO2 at 37 °C. Cul-ture medium was changed after 24h. In order to study islet function, tripli-cate groups of islets were incubated in 0.25 ml Krebs-Ringer bicarbonate

24
buffer supplemented with 2 mg/ml bovine serum albumin (fraction V; MP Biomedicals Inc., Aurora, OH, USA) and 1.7 or 16.7 mmol/l glucose [90].
Macrophage staining (study III-IV) Subsets of macrophages were stained in cryosections of gonadal adipose tissue (study IV) and in bacteria infected backs (study III). In adipose tissue, primary antibodies; rat anti-mouse F4/80 (1:200, eBioscience, San Diego, CA, USA) and Alexa Fluor488-conjugated rat anti-mouse MGL-1 (macro-phage galactose-type C-type lectin-1/CD301, 1:200, AbD Serotec, Düssel-dorf, Germany) were used, with NL577 goat anti-rat IgG (1:500, R&D Sys-tems, Minneapolis, MN, USA) as secondary antibody. In the bacteria-infected mice, an AlexaFlour555-conjugated F4/80 antibody was used. All slides were co-stained with Hoechst33342 (Invitrogen, Stockholm, Sweden). Images were captured using a Nikon confocal microscope (Nikon C-1 with Plan Apo VC 20x/0.75 objective) and analyzed using ImageJ.
Gene expression (study I and IV) In study I, the 3-adrenoceptor expression from isolated total RNA in islets of WF and GK rats was performed using the RNeasy Mini Kit (Qiagen, Hil-den, Germany). The RNA was converted to cDNA using a reverse-transcription system with oligo (dT)15 primers (Promega SDS Biosiences, Falkenberg, Sweden). The LightCycler System (Roche Diagnostics, Mann-heim, Germany) together with SYBR Green JumpStart Taq ReadyMix were used to amplify and analyze cDNA. The primer used and amplification pro-gram are listed in study I. Glucose 6-phosphate dehydrogenase was used as housekeeping gene. The results were evaluated as threshold cycle values (CT values) defined as the amplification cycle number when the fluorescence exceeds a specific threshold value. The CT-values were used to calculate the amount of PCR product in comparison to the housekeeping gene. Relative mRNA expression was calculated and expressed as 2- Ct.
In study IV, total RNA was extracted from frozen gonadal adipose tissue with Trizol (Invitrogen, Carlsbad, CA) and RNA concentrations were meas-ured on a Nanodrop™ 2000c spectrophotometer (Thermo-Scientific, Wil-mington, DE). cDNA was synthesized using 2 µg RNA from each sample using High Capacity cDNA kit (Applied Biosystems, Foster City, CA, USA). To measure Foxp3 and 18S mRNA, 2 µl of each cDNA sample were loaded in duplicate in TaqMan Gene Expression mastermix (Applied Biosys-tems) together with a MGB probe targeting Foxp3 (Mm00475162_m1) or 18S (hs99999901_s1; Applied Biosystems) on a MyIQ2 Real Time PCR System (Bio-Rad Laboratories, Sundbyberg, Sweden). According to the

25
comparative threshold method (Ct-method), Foxp3 mRNA levels were nor-malized to 18S mRNA levels ( Ct). The average Ct value from female mice on control diet was used as the 100 % reference ( Ct) for Foxp3 mRNA expression. The equation 2- Ct was applied to convert the logarith-mic Ct values to linear values.
Statistical analysis (study I-IV) All values are expressed as mean ± standard error of the mean (SEM). Stu-dent’s unpaired t-test was used for the statistical analysis and Mann Whitney was applied when the normality test failed in study I. In study II-IV, one way ANOVA with Fischer’s LSD post hoc test was used. In study III, one-way repeated measurements of ANOVA with Dunnett’s as post hoc test was also used when comparing the same animal at different time points. Statistical significance was set to P < 0.05. All statistical analyses were car-ried out using SigmaStat 3.5 (Systat Software, Richmond, VA, USA).

26
Study design
Study I WF and GK rats were treated with saline or the 3-adrenoceptor inhibitor SR59230A 10 minutes before blood flow measurements. Islets were also isolated from WF and GK rats for gene expression analysis of the
3-adrenoceptor within the islets.
Figure 5. The experimental outline of study 1.
Study II In study II, a glucose tolerance test (GTT) was performed before and after implantation of osmotic pumps in WF and GK rats. The pumps were filled with either saline or the 3-adrenoceptor inhibitor SR59230A. After two weeks, either blood flow or islet function (insulin release and insulin con-tent) were studied.
Figure 6. The experimental outline of study II.

27
Study III Mice were either given HFD for 16 weeks or treated with alloxan to induce hyperglycemia before leukocyte recruitment was studied. Separate alloxan-treated and control mice were used for bacterial clearance and phagocytosis analysis.
Figure 7. The experimental outline of study III.
Study IV C57Bl/6 mice were fed control or HFD for 14 weeks before allocated in two different sets of groups. Blood flow measurements and serum parameters were measured in one set of groups, whereas adipose tissue inflammation and islet function were investigated in the other set.
Figure 8. The experimental outline of study IV.

28
Results and Comments
Study I We investigated if the high islet and WAT blood perfusion previously seen in GK rats, a type 2 diabetes model [31], are regulated by signaling through the 3-adrenoceptor.
Mean body weight of the GK rats was significantly lower compared to age-matched control WF rats, whereas the retroperitoneal fat pad weight was higher, indicating an increased body fat content in these non-obese type 2 diabetic rats [91]. In the control WF rats, infusions of 3-adrenoceptor antagonist SR59230A affected neither subcutaneous nor intra-abdominal WAT blood flow suggesting that 3-adrenoceptors are not a main blood flow regulator under basal conditions. The augmented WAT blood flow observed in both depots in GK rats was reversed by the antagonist to levels similar to those seen in the WF rats (Figure 9.a-b).
Blood flow to interscapular BAT, where the adrenergic system affects both lipolysis and thermogenesis [14], was similar in GK rats when com-pared to that of WF rats under normal conditions. Surprisingly, there was a remarkable and more than nine-fold increase in blood flow after SR59230A administration in the GK rat. This is contradictory to previous findings where 3-adrenoceptor agonists were found to increase BAT blood flow [92]. The reasons for this discrepancy are unknown and further studies are required to resolve this matter.
Both whole pancreatic and islet blood flow were increased in the GK rat compared to control rats. After administration of SR59230A, islet blood perfusion decreased to the same level as that seen in WF rats, whereas the whole pancreatic blood flow was unaffected (Figure 9.c-d).
The serum insulin concentrations in SR59230A-treated GK rats were higher compared to control GK rats, indicating that the insulin release can be augmented already after an acute islet blood flow decrease or that the inhibi-tion affected the insulin secretion per se. To investigate if the described find-ings were caused by changes in receptor number, gene expression of the
3-adrenoceptors was analyzed. However, no significant difference in mRNA expression levels of 3-adrenoceptors was seen in the islets from GK and WF rats.
To conclude, our results indicate that 3-adrenoceptors participate in the specific regulation of WAT and islet blood flow in a type 2 diabetes model.

29
The significance of the 3-adrenoceptor-induced decrease in WAT blood flow seen in these experiments is, however, not fully understood. Neverthe-less, administration of a 3-adrenoceptor antagonist might be of interest for normalization of the increased islet blood flow, which in turn might improve the endocrine function of the islets.
Figure 9. Blood perfusion of subcutaneous WAT (a), intra-abdominal WAT (b), pancreas (c), and pancreatic islets (d) in control (white bars) or SR59230A-treated (black bars) WF and GK rats. Data are means ± SEM for 7-9 experiments in each group. *P < 0.05. Figure is based on results from study I.
Study II To further study the effect of 3-adrenoceptors on islet and WAT blood flow, we examined the effect of continuous 2-week administration of the antagon-ist SR59230A on blood perfusion. In this study, the type 2 diabetic GK rats showed increased mean body weight (~9%) and visceral retroperitoneal fat pad (~50%) as well as plasma glucose concentrations (~60%) compared to control WF rats.

30
The effect of 3-adrenoceptor inhibition on glucose tolerance in these an-imals was investigated. However, this was not improved after the 2-week treatment period. Neither could differences in serum insulin concentrations between saline- or SR59230A-treated WF or GK rats be detected.
The endocrine function of the islets from WF and GK rats was examined in vitro via glucose-stimulated insulin release after the 2-week in vivo treat-ment period. Both WF-treated groups responded to high-glucose stimulation, whereas this effect was absent in saline-treated GK-rats. Interestingly, the insulin secretion was improved in the GK-rat after SR59230A treatment, indicating an improved islet function. However, the glucose-stimulated re-sponse in isolated islets did not differ between rat strains or treatment groups.
Unlike the results seen after acute administration of the 3-adrenoceptor antagonist, long-term inhibition had no effect on either subcutaneous or in-tra-abdominal WAT. Also the pronounced increase in BAT blood flow seen after acute administration in study I was abolished after prolonged treatment.
No differences in whole pancreatic blood flow were seen irrespective of treatment of rat strains (Figure 10.a). Despite this, islet blood flow was in-creased in saline-treated GK rats compared to WF rats, but was revered with SR59230A-treatment during a 2-week period (Figure 10.b).
In conclusion, prolonged treatment with the 3-adrenoceptor antagonist SR59230A decreased the augmented islet blood flow in the type 2 diabetes model without affecting glucose tolerance per se.
Figure 10. Blood perfusion of pancreas (a) and pancreatic islets (b) in control (white bars) or SR59230A-treated (black bars) Wistar-Furth (WF) and Goto-Kakizaki (GK) rats after 2-week treatment. Data are means ± SEM for 7-10 experiments in each group. *P < 0.05 when compared to all other groups. Figure from study II.
Study III In this study, we were interested in how hyperglycemia affects leukocyte recruitment in response to inflammatory stimuli. High-fat-fed and alloxan-

31
treated mice were used as moderate and severe hyperglycemic models, re-spectively. The 16 weeks of HFD increased the body weight with approx-imately 30% compared to aged-matched control mice at the time for the leukocyte recruitment study. Further, the HFD impaired glucose tolerance and caused a moderate hyperglycemia (~11 mmol/l) and pronounced hyper-insulinemia with serum insulin concentrations increased >30-fold compared to mice on control diet.
Leukocyte recruitment under basal conditions in the cremaster muscle re-vealed increased numbers of both adherent and emigrated cells to a similar extent in all hyperglycemic mice. This observation might reflect hypergly-cemia-induced upregulation of adhesion molecules on endothelial cells and/or leukocytes. After administration of the inflammatory chemokine MIP-2, the numbers of adherent and emigrated leukocytes increased with time in all groups, but this was more pronounced in the alloxan-treated group (Figure 11.). Thus, in this group, an increased number of emigrated leuko-cytes was found at all time points after MIP-2 addition compared to control mice. A trend towards this, however not significant (P = 0.061), was seen in the HFD mice after 90 min of MIP-2 addition. These results suggest that leukocytes in the diabetes models are more prone to migrate out into tissues after stimulation with MIP-2, which may reflect a more activated innate im-mune system compared to that seen in normoglycemic mice.
Recurrent infections are often observed in patients suffering from diabetes and are probably caused by disease-related complications such as peripheral neuropathy, impaired peripheral blood perfusion, and probably also a defec-tive immune response [2,39,40,93,94]. We therefore wanted to investigate how our observations of an increased ability to recruit leukocytes during hyperglycemia would influence bacterial clearance of luminescent S. aureus inoculated subcutaneously. Despite the increased leukocyte recruitment seen in the cremaster model (Figure 11.), the alloxan-treated mice were unable to eliminate the bacterial infection to the same extent as the control mice (Figure 12.a-b). Interestingly, the alloxan-treated mice showed a more rapid and effective initial clearance during the first 7 days, but were unable to era-dicate the infection after 14 days (Figure 12.c). Staining of the bacteria-infected area confirmed the increased number of leukocytes seen in the re-cruitment studies, and the MPO-content in this area seemed to be increased, however not significantly (P = 0.063).
To investigate reasons for the defective bacterial clearance, the phagocyt-ic ability of leukocytes were investigated by injecting LPS-coated fluores-cent beads into the peritoneal cavity of mice. A 50% decrease of the number of phagocytizing cells was observed in the alloxan-treated mice compared to control mice.
In summary, hyperglycemia increases leukocyte-endothelial cell interac-tion and increases the number of emigrated cells in tissue. Despite this, the

32
leukocytes of hyperglycemic mice in this acute inflammatory model were less efficient in eradicating a bacterial infection due to impaired phagocytosis.
Figure 11. Number of adherent (a) and emigrated (b) leukocytes in recruitment studies in the cremaster muscle of control (white bars), alloxan-treated (dark grey bars), HFD-fed (light grey bars), and acute glucose-infused mice (black bars) before (time 0) or after MIP-2 addition to the superfusate. Data are means ± SEM. *P <0.05 compared to other groups at the same time point. †P<0.05 compared to time 0 with-in the group. Figure from study III.

33
Figure 12. Bacterial clearance in control and alloxan-treated mice. a, clearance rate of bioluminescent Staphylococcus aureus in control (black line) or alloxan-treated (grey line) mice until 50% of the control mice were free from bacteria (dashed line). b, representative images of bioluminescent S. aureus-infected areas in control (upper panel) and alloxan-treated (lower panel) mice at different time points post inoccula-tion. c, total bioluminescence in control (white boxes) and alloxan-treated (black boxes) mice over time. Dashed line represents average bioluminescent background. Figure from study III.

34
Study IV In this study, we investigated the outcome of HFD-treatment separately in male and female mice with respect to insulin levels, glucose tolerance, sys-temic inflammation, and islet blood perfusion. Mice gained weight to the same extent after 14 weeks of HFD, irrespective of gender. Intra-abdominal adipose tissue depots and serum concentrations of triglycerides and choles-terol were increased in both genders on HFD, indicating a diet-induced ef-fect on both adipose tissue and circulating lipids. Notably, high-fat-fed male mice exhibited increased serum cholesterol concentrations compared to fe-male mice on HFD. Furthermore, plasma glucose concentrations and serum insulin levels were augmented and glucose tolerance was impaired in male mice compared to female mice on HFD. Moreover, both islet fraction and mean islet diameter were increased in male mice on HFD compared to all other groups, indicating islet hypertrophy or hyperplasia.
Blood flow was studied in whole pancreas and in the pancreatic islets. Neither gender nor diet affected total pancreatic blood flow. Islet blood flow per pancreas weight was increased in the high-fat-fed male mice, but when expressed as islet blood flow per islet weight in order to compensate for the increased islet mass in the high-fat-fed male mice, no differences could be detected.
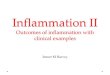
Besides increased insulin and circulating lipid concentrations, the in-flammatory cytokines IL-6 and mKC were also increased in serum of high-fat-fed male mice compared to all other groups (Figure 13.a-b). There was also a tendency towards decreased levels of the anti-inflammatory marker IL-10 in the high-fat-fed mice compared to control-fed animals.
To summarize, these results showed that contrary to what was observed for male mice, female mice on HFD did not develop hyperinsulinemia, glu-cose intolerance, and increased islet mass, despite similar weight gain.
To investigate if high-fat-fed male mice had developed a -cell defect, glucose-stimulated insulin release and insulin content were measured in vitro in isolated islets. Islets from the different groups did respond to glucose and no significant differences could be detected. These results imply that despite hyperinsulinemia, the islets in the high-fat-fed male mice maintain an ability to adequately respond to increased glucose concentrations.
The next step was to study the origin of the systemic inflammation. Therefore, gonadal WAT was analyzed for macrophage subtypes and anti-inflammatory Treg. No differences in the number of resident macrophages (F4/80+MGL-1+) between the groups were seen. However, male mice on HFD had an increased number of inflammatory macrophages (F4/80+MGL-1-) compared to all other groups indicating that the origin of the inflammation, at least in part, derives from WAT (Figure 13c). Further, the inflammatory macrophages were situated in crown-like structures sur-rounding adipocytes as previously found in obese adipose tissue [95]. Treg

35
function as anti-inflammatory regulators in adipose tissue of both mice and men and their number decreases with obesity [42,96]. To examine if gender affected the Treg population in mice on HFD, gene expression of Treg was measured. High-fat-fed female mice augmented the Treg expression 7-fold, whereas the expression in male mice on HFD remained unchanged (Figure 13.d).
In conclusion, female mice fed a HFD are protected against hyperinsuli-nemia and islet hypertrophy or hyperplasia, which might be explained by less intra-abdominal and systemic inflammation and the maintenance of a non-inflammatory milieu in intra-abdominal adipose depots.
Figure 13. Inflammatory markers in serum (a-b) after 14 weeks on control- or high-fat diet (HFD). c, number of inflammatory (F4/80+MGL-1-, white) and resident (F4/80+MGL-1+, grey) macrophages in adipose tissue in mice on control- or HFD for 14 weeks. d, gene expression of Foxp3 (regulatory T-cell marker) in adipose tissue in control- or high-fat-fed mice. Data are means ± SEM. P < 0.05 compared with control (*), compared with female control (†) and compared with female on HFD (‡). Figure is based on results from study IV.

36
Discussion
Animal models of type 2 diabetes are usually associated with -cell defects that are unmasked by a simultaneous peripheral insulin resistance. The de-veloped insulin resistance may result in augmented pancreatic islet blood flow in order to compensate for the increased demand of insulin. The studies included in this thesis demonstrates that the increased islet blood flow during type 2 diabetes is at least in part regulated by the adrenergic nervous system via 3-adrenoceptors, without affecting the insulin secretion. Further, di-abetes-induced hyperglycemia affects leukocytes in the circulation, and we found increased leukocyte recruitment during basal and inflammatory condi-tions in diabetic mice. Despite this effect, bacterial clearance was defect in these mice due to impaired phagocytosis. Type 2 diabetes is frequently pre-ceded by obesity and in the last paper included in this thesis, we aimed to investigate obesity-induced effects in male and female mice on HFD. We found a low-grade, systemic inflammation manifested in increased levels of circulation inflammatory agents in male but not in female mice. Obesity-triggered inflammation is present in different organs, in particular the adi-pose tissue, and the main mediator is pro-inflammatory macrophages, which increased manifold in numbers in the obese male mice. By contrast, and probably due to their ability to maintain their adipose tissue non-inflammatory by increasing the Treg population, female mice were resistant to onset of obesity-induced inflammation and concomitant metabolic adapta-tions compared to male mice.
Of mice and men The physiology of mice and rats differs from that of man in several aspects and results from animal models cannot always be directly translated and applied to humans. This has partly been shown with regard to islet physiolo-gy [97] and particularly fat cell biology [98]. However, mechanistic studies are difficult to perform on humans, whereby disease models in rodents pro-vide important information to fill knowledge gaps.
The GK rat used in study I and II is a well-known nonobese, animal mod-el of type 2 diabetes with defect -cell function [83] including oxidative stress formation in the -cells [99], as well as peripheral insulin resistance [84]. GK rats also show adipose tissue inflammation with increased circulat-

37
ing levels of TNF- and IL-6, and a redistribution of adipocyte size with a decreased number of large adipocytes [100].
In study III and IV, C57Bl/6 mice were used. This is a commonly used standard strain worldwide which increases their adipose tissue mass when fed a high calorie diet enriched in both carbohydrates and fat.
Islet blood flow in relation to endocrine function -cells in islets of Langerhans have a great capacity to compensate for in-
creased demands for hormone secretion, as seen during e.g. pregnancy and weight increase. In line with this, animals subjected to a partial pancreatect-omy (60%), with concomitant reduction of islet mass, are still able to main-tain an adequate insulin production [101,102]. However, if this compensa-tion fails, type 2 diabetes develops. Combined data from both human and animal studies suggest a sequence of processes consisting of four different stages of -cell failure [32]. Briefly, the first stage constitutes successful compensation to the increased demand, caused by e.g peripheral insulin re-sistance, by increases in -cell mass with a maintained functional glucose-stimulated insulin secretion. During the second stage, plasma glucose levels are increasing as a first sign of a -cell defect. Further, the glucose-stimulated insulin secretion becomes inadequate, but the response to other insulin secretagogues, e.g. arginine, is still present. In the third stage, -cell hypertrophy continues, and now also the other factors which stimulate insu-lin-release fail to increase insulin secretion. At the final stage, -cell mass decreases and lipid droplets, amyloid, and fibrosis form within the islet con-tributing to -cell apoptosis [103]. The high-fat-fed male mice in study IV demonstrated an increased islet mass, but the islets maintained an intact glu-cose-stimulated insulin release suggesting that the -cells are still functional and in the first stage of the -cell failure according to the scheme given above.
Pancreatic islets are among the most vascularized organs in the body. Their blood flow is regulated independently from that of the exocrine paren-chyma by several mechanisms, including locally produced endothelial me-diators and metabolic substances, as well as the autonomic nervous system. However, the ambient glucose concentration seems to be the most influential stimulus to balance islet blood perfusion to the metabolic needs of the islets [28,104].
We have previously shown that animal models of type 2 diabetes initially have an increased islet blood flow compared to controls [31,105]. This hyperperfusion increases the pressure within the islet capillaries, as observed in the GK rat, which might be harmful to the endothelial cells [106]. GK rats are also known to decrease both their vessel density and islet blood perfusion with increasing age [107]. One mechanism that could explain this scenario is

38
that the increased metabolic demands caused by insulin resistance, stimu-lates compensatory mechanisms in the pancreas, such as increased islet blood perfusion and increased -cell mass. This hyperperfusion accompanied by prolonged hyperglycemia and glucotoxiticity will with time damage en-dothelium and -cells resulting in decreased vessel density [107] and -cell death.
The microsphere technique used in this thesis is the only readily available method for measurements of total islet blood flow in native pancreas. The optimal size of the microspheres varies due to the capillary diameters in the organ of interest [68]. In order to adequately measure islet and WAT blood flow we had to use 10- and 15-µm microspheres, respectively, as discussed in detail previously [31]. Immediately after injection of the microspheres into the arterial blood stream, a blood sample is collected from the femoral artery, representing an artificial organ with known blood flow. By counting the microspheres in the organs, the blood flow can be calculated. The disad-vantages with this method are that it only measures the blood perfusion at one given time and that it is difficult to perform repeated injections in the same animal.
Autonomic innervation of islets and adipose tissue Innervation of both islets and adipose tissue is crucial for modulation of their function. The 3-adrenoceptor constitutes the cornerstone of the adrenergic nervous system in WAT and BAT, but is also a major player in the islets of Langerhans [65,66,67,108]. The receptor is situated on smooth muscle cells and -cells, and affects islet blood flow and insulin release [67,70,109,110]. The gene expression of the 3-adrenoceptors was similar in the islets of both WF and GK rats in study I, demonstrating that differences in the amount of receptors are unlikely to cause the decreased islet blood perfusion seen in the GK rat. Further, if the receptor affinity is changed during diabetes is not known, but the antagonist was given in a high concentration and therefore probably able to inhibit all receptors. However, the different blood flow res-ponses seen after 3-adrenoceptor inhibition in the two strains, both in study I and II, can be explained by the location of the adrenoceptors. The islet blood flow is mainly regulated through the afferent arterioles, usually 1-3 in number, which enter the islet [111]. The distal portion of the arterioles pene-trates into the islet core, and will therefore be included in islet isolations. These cells, i.e. smooth muscle and endothelial cells, can contribute to the measured gene expression in study I. The exact anatomical location of the expressed adrenoceptors cannot be deduced from these experiments. It should be noted that we in yet unpublished experiments have found reactivi-ty to 3-adrenoceptor stimulation in isolated islet arterioles from WF rats suggesting their existence in these vessels.

39
Neither acute reduction (study I) of islet blood flow nor reduced blood flow levels for 2 weeks (study II) affected insulin secretion. Thus, possible effects on insulin secretion by blood flow reduction probably require pro-longed times of 3-adrenoceptor inhibition. A very important finding in the present studies was that 3-adrenoceptor inhibition did not by itself interact and blunt insulin secretion, which is crucial for eventual therapeutic applica-tions.
WAT nerves help to control adipocyte function, and this regulation is more developed in visceral, intra-abdominal compared to subcutaneous adi-pose tissue [108]. The 3-adrenoceptors are also important blood flow regu-lators in adipose tissue in which differences in receptor distribution and sub-types have been demonstrated [108,112,113]. 3-adrenoceptors also affect metabolism through stimulation of lipolysis, which improves insulin resis-tance and decreases fat mass, which make them a target for anti-diabetic drugs [110,114]. Indeed, anti-diabetic effects have been seen in rats and mice [115]. However, increased lipolysis increases free fatty acid concentra-tions in the circulation, which contributes to harmful triglyceride accumula-tions in other organs [116]. Further, people suffering from obesity usually develop catecholamine resistance in their WAT with blunted lipolysis as a consequence [117,118,119,120,121], which contributes to adipose tissue storage. Together, these findings strongly limit the therapeutic anti-diabetic effects by 3-adrenoceptor agonists.
Leukocytes and hyperglycemia Leukocytes play an important role in the defense against microorganisms and other foreign substances and the fact that patients suffering from di-abetes have impaired resistance against infections is well-established [122]. Although the effects of hyperglycemia on leukocytes have been frequently studied, the mechanisms behind the observed impaired function are still not fully understood.
We studied leukocyte-endothelial interactions in two hyperglycemic models, the alloxan-treated mice and the high-fat-fed mice. These models of diabetes differ both in the degree and duration of hyperglycemia, since the HFD creates moderately increased plasma glucose levels for a longer time period, then seen after alloxan, where the hyperglycemia is acute and more severe. Furthermore, the mice on HFD are hyperinsulinemic probably due to a concomitant insulin resistance, whereas the alloxan-treated animals are hypoinsulinemic.
In these sets of experiments, it is important not to manipulate the numbers of circulating leukocytes with the alloxan-treatment and the differential count showed no differences in leukocytes between alloxan-treated or con-trol mice blood.

40
Previous studies have shown conflicting results with regard to how hyperglycemia affects leukocyte recruitment. Both decreased [123] and in-creased [124] number of leukocyte-endothelial cell interactions have been reported as well as increased levels of adhesion molecules on leukocytes [125]. One possible explanation for the variations in study outcome might be the magnitude as well as the length of hyperglycemia which might affect leukocytes function differently. Our findings are in line with those seen in a previous study in which the leukocyte-endothelial interactions were investi-gated in the mesentery during ischemia-reperfusion injury in streptozotocin-treated rats [124]. Ischemia-reperfusion increased both adhesion and emigra-tion of leukocytes in the mesentery of streptozotocin-treated rats compared to control animals. However, another study demonstrated decreased leuko-cyte-endothelial interactions in the internal spermatic fascia in alloxan-treated rats [123]. An obvious discrepancy between the latter study and our findings is the time period of severe hyperglycemia. Our mice were alloxan-treated 3-8 days prior experiment, whereas the alloxan-treated rats were hyperglycemic during 33 days, with an associated higher degree of protein glycosylation and metabolic changes. Therefore, it may be that the hypergly-cemia increases the leukocyte-endothelial interaction initially, but with time the interactions may be blunted. The cremaster muscle is a well-established tissue for leukocyte recruitment studies, since it is a thin, transparent muscle. Leukocyte recruitment to adipose tissue would of course be interesting to study but the properties of adipose tissue per se make it difficult to visualize intravascular leukocytes.
Even though leukocytes of alloxan-treated mice were present at the in-flammatory site in our study, they were unable to eradicate a subcutaneous S. aureus infection. These data are in line with clinical findings, which show that patients suffering from diabetes show increased susceptibility to bacteri-al infections [93,94,122]. An experimental study where S. aureus was in-jected in the hindpaw of the non-obese diabetic (NOD) mouse of an au-toimmune model of type 1 diabetes reported exacerbated bacterial clearance in the diabetic mice [126]. In contrast to our results, these authors found that the tissue inflammation was reduced with lower concentrations of chemo-kines. The correlation of these results with our own is difficult to evaluate since NOD mice exhibits more profound immune defects.
An interesting finding in our study was that the amount of luminescent bacteria initially decreased at a faster rate, but could not be totally eliminated with time in the alloxan-treated mice compared to controls. This might re-flect the initial increase in emigrated leukocytes at the infection site observed in the leukocyte recruitment experiments. The disability to clear the infection by leukocytes from alloxan-treated mice was demonstrated to be due to de-fect phagocytosis.

41
Adipose tissue inflammation Adipose tissue constitutes both a source of inflammatory mediators, in terms of cytokine and adipokine production, as well as a site of inflammation with increased macrophage recruitment [54,55]. The connection between obesity, inflammation and insulin resistance was discovered ~20 years ago [5,7]. This changed the view of adipose tissue from being an energy reservoir only to also constituting the largest endocrine organ in the body with an important function as a metabolic sensor. Lately, major focus of research has been on the accumu-lation of macrophages in adipose tissue, which seems to constitute one link to local inflammation and the development of insulin resistance [54,55]. Normal-ly, adipose tissue macrophages (ATMs) control several processes in the adi-pose tissue including angiogenesis, removal of dead adipocytes, responses to hypoxia, as well as adipogenesis in lean and obese states [95,127].
ATMs exhibit diverse phenotypic heterogeneity depending on their cur-rent immune function, and they can be divided into M1/M2 phenotypes. Obesity causes a phenotype switch in the subsets of ATMs from the resident M2 to the inflammatory M1 macrophage, which causes an adipose tissue inflammation [128]. However, this classification of ATMs as M1 and M2 is a matter of controversy, since these subsets show considerable heterogeneity. It has recently been shown that ATMs have different activation states and phenotypes not consistent with this classification [129]. With this in mind, we chose to differentiate the macrophages in study IV according to their surface markers, and not after their M1/M2 phenotype. Thus, we used F4/80 which is a marker expressed on all macrophages and MGL-1, which is ex-pressed only on resident macrophages [130].
Adipose tissue in obesity not only changes their subsets of ATMs from the resident into a predominance of the inflammatory macrophage subtype via increased recruitment. The recruited inflammatory ATMs also cluster around dead adipocytes and form ‘crown-like’ structures [95]. These results are in line with our findings in high-fat-fed male mice were we observed increased number of F4/80+MGL1- macrophages in crown-like structures. The origin of the latter structures has been claimed to be due to the high turnover and remodeling of adipose tissue in obesity. This increases the number of dead adipocytes that per se recruits the inflammatory ATMs, in a similar way as neutrophils are recruited towards necrotic tissue [131]. How-ever, despite similar weight gain, this phenomenon was absent in the high-fat-fed female mice.
Macrophage recruitment is both regulated and increased by lipolysis, which can be enhanced further by addition of 3-adrenoceptor agonists [57,132]. During lipolysis, recruited ATMs increase their lipid uptake [132]. It should be noted that GK rats express increased inflammatory markers in adipose tissue [100]. One can hypothesize that increased WAT blood flow seen in the GK rat may correlate to increased lipolysis and increased macro-

42
phage recruitment. Macrophage content has been investigated in adipose tissue of GK rats and found to be normal [31], but specific subtypes of ma-crophages have not been analyzed. A blunted lipolysis, induced by the 3-adrenoceptor inhibitor SR59230A, might therefore decrease the macrophage recruitment to adipose tissue and prevent or modulate the inflammation.
Macrophages are not the only immune cell present in adipose tissue and interplay between pro- and anti-inflammatory innate and adaptive immune cells is likely to regulate the local micro-environment. Lately, there has been a growing interest in Treg populations, since these cells have inflammation suppressing actions [43]. Treg are enriched in lean adipose tissue of both mice and men but decrease in number with obesity [42,96]. This could not be observed in the high-fat-fed male mice with systemic inflammation and hyperinsulinemia (study IV), probably due to the short time on HFD. Surpri-singly, we found that the fraction of Treg was upregulated in female mice on HFD compared to lean female mice, which indicates an increased demand of anti-inflammatory mediators to counterbalance the pro-inflammatory actions of increased adipocytes. Since female mice on HFD did not increase the inflammatory macrophage population in WAT, developed systemic inflam-mation or hyperinsulinemia despite similar weight gain, the maintenance of the non-inflammatory adipose tissue seems to be successful.
Another intriguing finding was that the population of Treg was much lower in lean female mice compared to lean non-inflammatory male mice. Consi-dering the increased IL-6 concentrations in serum of lean male mice com-pared the lean female mice, we hypothesize that the enhanced inflammation in the former group is compensated for by the increased Treg in WAT. How-ever, we found no differences in other serum cytokine concentrations and more data is required to understand the mechanisms.
Worthy of note and important to keep in mind is that not all people suffer-ing from obesity develop type 2 diabetes. In addition to obesity, there are other factors which make the disease manifest, such as heredity, ethnicity and environment [133]. Further, if the adipose tissue is situated in visceral or in subcutaneous, gluteofemoral regions is also important, since the former is more associated with hyperinsulinemia and insulin resistance [77,134]. The visceral and gluteofemoral subcutaneous adipocytes are phenotypically dif-ferent and the latter have in several studies shown to be protective against cardiovascular and metabolic diseases. Further, this adipose tissue is asso-ciated with beneficial adipokines but not pro-inflammatory cytokines [134].
Anti-inflammatory therapies such as anti-TNF- are used to treat many inflammatory diseases. There have been several attempts to use such anti-inflammatory agents to alleviate adipose tissue inflammation. The results were impressive in obese rodent models of type 2 diabetes in which neutrali-zation of TNF- improved peripheral insulin-stimulated glucose uptake [5]. On the other hand, effects in human studies were lacking [135,136]. A re-cently published paper investigated the prolonged effect of a TNF- compet-

43
itor in patients suffering from obesity and found improved plasma glucose concentrations and increased levels of the anti-inflammatory adipokine adi-ponectin, whereas no effects on fasting insulin and insulin resistance could be detected [137]. Different study designs might explain these outcomes. In the first set of studies, the TNF- inhibitor was given intravenously as a sin-gle dose, and repeated administration might be necessary in order to obtain an effect. Moreover, there are also several other pro-inflammatory agents apart from TNF- present in adipose tissue during obesity, which contribute to insulin resistance.
Does gender matter? Human adipose tissue distribution differs between genders. Generally, wom-en exhibit enriched subcutaneous adipose tissue, e.g. within the gluteofe-moral region whereas the predominantly male visceral enrichment is asso-ciated with increased risk of several diseases [134]. Another and potentially related observed gender difference in humans is the levels of circulating inflammatory markers, even though contradictory data exist [138,139,140].
One possible explanation for these gender differences might be anti-inflammatory effects of estrogen. Estrogen induces multiple effects on meta-bolism in both humans and rodents and regulates body fat distribution, as well as promotes accumulation of subcutaneous adipose tissue [78]. In line with this, the prevalence of type 2 diabetes is increased in postmenopausal women with decreased estrogen levels compared to fertile women. In addition, viscer-al adipose tissue accumulates in women during postmenopause when the le-vels of estrogens are low [141,142], which might be caused by altered expres-sion of sex hormone receptors within adipose tissue [143]. In humans as well as in animal models, females are protected against FFA-induced insulin resis-tance [144,145]. Further, women who suffer from polycystic ovary syndrome with hyperandrogenaemia develop visceral accumulation of adipose tissue and insulin resistance which indicate a protective role of estrogen [82].
Interestingly, the estrogen receptor is also present in the islets of Langer-hans [146] and isolated islets from ovariectomized rats had impaired insulin release compared to control animals [147]. Further, stimulation of the estro-gen receptor within the -cells in rodent models of type 2 diabetes reduced lipid synthesis and protected the -cells from failure [148], but the mechan-isms are not fully understood.
Taken together, these different studies demonstrate that estrogen has po-tential anti-diabetic effects in both adipose tissue and pancreatic islets. The exact mechanisms behind these observations are still not fully understood. In agreement with this, our data (study IV) clearly demonstrated a reduced in-flammatory response to obesity in female compared to male mice, which might be due to non-inflammatory actions of estrogen.

44
Conclusions
This thesis concludes that:
Augmented blood flow in both pancreatic islets and white adipose tissue in the GK rat can be reduced to similar levels as in control rats by inhibition of
3-adrenoceptors. Serum insulin concentrations were not affected, demon-strating intact -cell function even after reduced islet blood flow.
Leukocyte recruitment is more effective in both alloxan- and diet-induced diabetic mice compared to control animals during basal conditions and after acute inflammation. Despite this effect, bacterial clearance is impaired in diabetes due to defect leukocyte phagocytosis.
High-fat diet induces low-grade inflammation only in male mice, since fe-male mice were resistant to recruitment of inflammatory macrophages into adipose tissue, to increased levels of circulating inflammatory chemokines, to hyperinsulinemia, and to islet hypertrophy. Instead, female mice increased the Treg population of WAT to preserve a non-inflammatory status.

45
Future perspectives
We will further investigate the mechanisms of how the leukocytes from hyperglycemic mice kill bacteria. In particular, we would like to investigate formation of neutrophil extracellular traps (NETs), in response to S. aureus. Moreover, the production of reactive oxygen species, ROS, from these leu-kocytes will be investigated.
Since recently published data show that catecholamines are important in recruitment of macrophages to both brown and white adipose tissue, it would be interesting to investigate the subsets of macrophages in adipose tissue of the GK rat, before and after treatment with the 3-adrenoceptor antagonist. Also, the effects, both on islet blood flow and islet insulin secretion, of a chronic treatment with the 3-adrenoceptor antagonist would be interesting to examine.

46
Populärvetenskaplig sammanfattning
Bakgrund Fetma ökar globalt i alla åldersgrupper på grund av livsstilsförändringar såsom ökat matintag och en mer stillasittande vardag. Vid fetma uppstår en låggradig inflammation i fettvävnaden som ökar risken för insulinresistens, dvs kroppens oförmåga att ta upp glukos i cellerna, och därmed risken för diabetes typ 2.
Insulin är ett hormon som produceras av beta-cellerna belägna i de Lang-erhanska öarna i bukspottkörteln. Dess främsta funktion är att stimulera glu-kosupptag från blodet till kroppens celler. Diabetes typ 2, eller ”vuxendiabe-tes”, karaktäriseras förutom av insulinresistens även av en beta-cellsdefekt. Insulinresistensen tvingar beta-cellerna att öka sin insulinproduktion, en situation som tillslut blir ohållbar, vilket leder till att blodsockernivåerna ökar i cirkulationen, så kallad hyperglykemi. Det sistnämnda påverkar i sin tur makro- och mikrocirkulationen i kroppen och ökar, via ej helt klarlagda mekanismer, risken för diabetesrelaterade komplikationer. Fetma, tillsam-mans med insulinresistens, högt blodtryck, och diabetes typ 2 är alla tillstånd som ökar risken för förtidig död.
Delarbete I och II Ett återkommande fynd inom forskningen är att tillstånd med ökade krav på insulinfrisättning, t ex insulinresistens och manifesterad diabetes typ 2, är associerade med en blodflödesökning i de Langerhanska öarna. Denna blod-flödesökning samt efterföljande blodtrycksökning i ö-kapillärerna stressar cellerna som bekläder kärlen i öarna, endotelcellerna, vilket i sin tur kan leda till försämrad beta-cellsfunktion.
Syftet med de två första studierna var att undersöka det adrenerga nervsy-stemets roll, vilket reglerar psykisk och fysisk stress i kroppen, vid blodflö-desreglering i normala (Wistar F) och diabetiska (GK) råttor. GK-råttan är en normalviktig modell för diabetes typ 2 med en ökad ö-genomblödning. För att undersöka det adrenerga nervsystemets effekt på ö-blodflödet admi-nistrerades en beta3-receptorantagonist (SR59230A) akut eller konstant un-der två veckor innan blodflödet mättes med mikrosfärteknik. Resultaten vi-sade att denna antagonist minskade GK-råttornas ökade blodflöde i de Lang-

47
erhanska öarna till samma nivå som i kontrolldjur både vid akut administre-ring och efter en två-veckorsbehandling. Samma effekt syntes även i bukfett och subkutan fettvävnad vid akut tillförsel, medan denna effekt uteblev i de långtidsbehandlade djuren. Dessa resultat visar att det adrenerga nervsyste-met har en betydande roll i blodflödesreglering i både Langerhanska öar och fettvävnad.
Delarbete III
I det tredje arbetet ville vi i två olika inflammationsmodeller undersöka hur måttligt förhöjda eller höga blodsockernivåer påverkar rekrytering av vita blodkroppar (leukocyter) från blod till vävnad samt deras funktion. För att studera detta behandlades möss med ett beta-cellsgift (alloxan) som dödar de insulinproducerande cellerna vilket ger en kraftig hyperglykemi. För att stu-dera måttligt förhöjda blodglukosnivåer vilket motsvarar en diabetes typ 2-modell, sattes möss på högfettsdiet under >14 veckor. Leukocytrekyteringen studerades i venolerna i en tunn muskel, först under basala förhållanden och sedan efter tillsats av inflammationsstimuli, en kemokin som attraherar leu-kocyter (MIP-2, macrophage inflammatory protein-2).
Samtidigt som det uppstår en låggradig inflammation i kroppen vid diabe-tes typ 2 har dessa patienter ofta svårt att bekämpa bakterieinfektioner. För att studera förmågan att bekämpa en bakterieinfektion, injicerades lumine-scerande Stafylococcus aureus-bakterier i kontroll- och alloxan-behandlade möss, för att sedan följa infektionen under 14 dagar.
Våra resultat visade att andelen rekryterade leukocyter var förhöjda i båda våra hyperglykemiska modeller både basalt, samt efter tillsats av inflamma-tionsstimuli (MIP-2) jämfört med i kontrollmöss. Trots att fler leukocyter därmed tog sig från blodet till inflammerad vävnad vid hyperglykemi, visade våra diabetiska möss en försämrad förmåga att bekämpa bakterieinfektionen. Detta orsakades av att leukocyterna i de hyperglykemiska mössen uppvisade en defekt förmåga att äta upp bakterierna (fagocytering). Slutsatsen från dessa försök var att både måttlig samt kraftig hyperglykemi ökar antalet rekryterade leukocyter till ett inflammationsområde, men att dessa leukocy-ter har en defekt förmåga att bekämpa bakterieinfektioner via försämrad fagocytos.
Delarbete IV
Syftet med det sista arbetet var att undersöka effekten av kontroll- och hög-fettsdiet mellan hon- och hanmöss med avseende på utvecklandet av fetma,

48
metabolt syndrom och diabetes typ 2. Efter 14 veckor på högfettsdiet utveck-lade både hon- och hanmössen fetma i likartad utsträckning. Trots liknande viktuppgång hos båda könen utvecklade feta hanmöss högre blodsockernivå-er, insulinnivåer och kolesterolkoncentrationer jämfört med de feta honmös-sen. Dessutom hade de en sämre glukostolerans samt en ökning av en del inflammationsmarkörer jämfört med de feta honmössen, vilka inte visade några tecken på en ökad inflammation. De feta hanmössen påvisade även förstorade Langerhanska öar och ett ökat ö-blodflöde, vilket kan förklaras av en ökad metabol belastning i de insulinproducerande öarna. Trots detta fun-gerade öarna normalt när insulininnehåll och insulinfrisättning undersöktes.
För att hitta orsaken till varför honmössen var skyddade mot utvecklandet av inflammation och glukosintolerans i denna modell, undersöktes fettväv-naden i både han- och honmöss med avseende på makrofager (en vit blod-kropp med stor fagocyterande förmåga) och regulatoriska T-lymfocyter, en cell vars främsta funktion är att hämma inflammationssvaret i kroppen. Re-sultaten visade att honmössen ökade populationen regulatoriska T-lymfocyter i sin fettvävnad som svar på ökad kroppsvikt vid högfettsdiet, medan andelen inflammatoriska makrofager markant ökade i fettet hos de feta hanmössen.

49
Acknowledgements
This work was carried out at the department of Medical Cell Biology, Upp-sala University. This work was not a one-woman job and had never been accomplished without all the people at the department who have contributed in different ways. In particular, I would like to express my sincere gratitude to:
Mia Phillipson, my supervisor, for your never-ending enthusiasm, inspira-tion, and support and for always having patience with me. You are a true mentor and a great researcher. Thank you again for sharing your entertaining drawings and mixtapes, I appreciate it!
Leif Jansson, my co-supervisor, for being the “walking Google”, for always having time or taking your time for discussions about research and teaching. No one knows so much about pancreas in the three-toed sloth and other mammals as you.
Johanna Henriksnäs, my co-supervisor, for introducing me to scientific re-search, excellent guidance in the lab, being a “doer”, and for always being so enthusiastic about our research.
All co-writers who contributed to the studies.
Technical assistance from Birgitta Bodin, the guru of microspheres, Astrid Nordin, Ing-Britt Hallgren, Anders Ahlander, and Lisbeth Sagulin for all help over the years, you are the best!
The Phillipson/Holm group for creating a great atmosphere in the lab. Lena, for great discussions about obesity, adipose tissue, and mesoscale. Gustaf for being the “klippa” in the lab, for great travel company, and for NOT laugh-ing when I fall skiing. Sara, for the help with S. aureus analysis, and for bringing a little bit of the south European mentality into the lab. Cilla, you are such a great source of energy. Evelina, for your passion for research and your unlimited ideas. Tomas, for sharing my enthusiasm about fat. David, for never-ending discussions about MPO and mesoscale, and Annika for hands-on help in the lab.

50
The former and present members of the Jansson/Carlsson group: P-O for introducing me to scientific research and for teaching me to be a tactical player and what questions you should not ask. Monica, Rickard, Johan, Joey, Daniel, Sara, and Åsa for great help in the lab.
Professors and senior scientists at the department; Andreea, Arne, Stellan, Nisse, Micke, Peter, Anders, Erik, Fredrik, Peter, Erik, Gunilla, Ulf, and Parri for collaborations and significant questions and discussions at Brain Pubs.
Marianne, Agneta, Shumin, Camilla, Gunno, GöS, Lina, and Björn for the assistance with administration, technical issues, and teaching.
My Roomies throughout the years; Sara B, Joey, Nina, Sara M, Jenny, Jo-han, and Liza for laughs, important and sometimes not so important discus-sions and for creating a great atmosphere. Åsa for being the best band leader and Liselotte, for being as enthusiastic as me during our weekly routine, the intro quiz, and both of you for your sarcasm and great sense of humor.
All former and present PhD-students for lunches, coffee breaks, and for making the department a pleasant place to work at.
Johan Hübinette for the beautiful original picture of adipose tissue. I owe you a delicious potato-twister!
Mina gamla kursare för sushiluncher, fredagsöl och för er förståelse vid forskningsmotgångar (även om de varit otroligt få, ja, knappt existerande). Speciellt tack till Helena och Helén som guidat mig genom blankettdjungeln och avhandlingsmallskaos inför disputationen samt till Oskar för att du alltid är så lugn när jag ringer panikartat och för du knappt ens motvilligt läste min kappa, trots att du inte behövde.
Mina vänner utanför forskarvärlden för att ni vet så lite om forskning och så mycket om andra livserfarenheter såsom surf, beachvolley, mat, musik och andra livsförnödenheter, en utsökt kombination. Ni är fantastiska!
Mamma och pappa för att ni tror på mig, ständigt ställer upp, supportar och uppmuntrar mig samt för ert genuina intresse för min forskning, även om ”det låter svårt”. Min bror Fredrik och Gina som alltid får mig på bra humör och för oräkneliga diskussioner om hur man egentligen uppnår ett perfekt HbA1c, samt min gudson Milton, världens bästa charmör!
Rasmus, hur många läsk är jag skyldig?

51
Financial support for these studies was provided by: the Swedish Medical Research Council (57X-20675, 72x-109, 55x-15043), the Royal Swedish Academy of Sciences, the Novo Nordisk Foundation, the Swedish Diabetes Association, the Juvenile Diabetes Research Foundation, the EFSD/MSD European Studies on Beta Cell Function and Survival, the Juvenile Diabetes Research Foundation, Magnus Bergvalls Foundation, the Swedish Society for Medical Research, Lars Hiertas Foundation, Harald and Greta Jeanssons Foundation and the Family Ernfors Fund.
Travel grants from Anna-Maria Lundins foundation, Upsala läkareförening, and Swedish Society for Medical Research are also gratefully acknowl-edged.
Uppsala, January 2012

52
References
1. http://www.who.int/mediacentre/factsheets/fs311/en/index.html (2011) Obesity and overweight.
2. Zimmet P, Alberti KG, Shaw J (2001) Global and societal implications of the diabetes epidemic. Nature 414: 782-787.
3. Chan JM, Rimm EB, Colditz GA, Stampfer MJ, Willett WC (1994) Obesity, fat distribution, and weight gain as risk factors for clinical diabetes in men. Diabetes Care 17: 961-969.
4. Colditz GA, Willett WC, Rotnitzky A, Manson JE (1995) Weight gain as a risk factor for clinical diabetes mellitus in women. Ann Intern Med 122: 481-486.
5. Hotamisligil GS, Shargill NS, Spiegelman BM (1993) Adipose expression of tumor necrosis factor-alpha: direct role in obesity-linked insulin resistance. Science 259: 87-91.
6. Zhang Y, Proenca R, Maffei M, Barone M, Leopold L, et al. (1994) Positional cloning of the mouse obese gene and its human homologue. Nature 372: 425-432.
7. Scherer PE, Williams S, Fogliano M, Baldini G, Lodish HF (1995) A novel serum protein similar to C1q, produced exclusively in adipocytes. J Biol Chem 270: 26746-26749.
8. Cinti S (2011) Between brown and white: novel aspects of adipocyte differentiation. Ann Med 43: 104-115.
9. Jensen MD (2008) Role of body fat distribution and the metabolic complications of obesity. J Clin Endocrinol Metab 93: S57-63.
10. Tilg H, Moschen AR (2006) Adipocytokines: mediators linking adipose tissue, inflammation and immunity. Nat Rev Immunol 6: 772-783.
11. Cypess AM, Lehman S, Williams G, Tal I, Rodman D, et al. (2009) Identification and importance of brown adipose tissue in adult humans. N Engl J Med 360: 1509-1517.
12. Virtanen KA, Lidell ME, Orava J, Heglind M, Westergren R, et al. (2009) Functional brown adipose tissue in healthy adults. N Engl J Med 360: 1518-1525.
13. van Marken Lichtenbelt WD, Vanhommerig JW, Smulders NM, Drossaerts JM, Kemerink GJ, et al. (2009) Cold-activated brown adipose tissue in healthy men. N Engl J Med 360: 1500-1508.
14. Cannon B, Nedergaard J (2004) Brown adipose tissue: function and physiological significance. Physiol Rev 84: 277-359.
15. Ricquier D (1989) Molecular biology of brown adipose tissue. Proc Nutr Soc 48: 183-187.
16. Trayhurn P, Wood IS (2004) Adipokines: inflammation and the pleiotropic role of white adipose tissue. Br J Nutr 92: 347-355.
17. Andersson CX, Gustafson B, Hammarstedt A, Hedjazifar S, Smith U (2008) Inflamed adipose tissue, insulin resistance and vascular injury. Diabetes Metab Res Rev 24: 595-603.

53
18. Trayhurn P (2005) Endocrine and signalling role of adipose tissue: new perspectives on fat. Acta Physiol Scand 184: 285-293.
19. Lau DC, Dhillon B, Yan H, Szmitko PE, Verma S (2005) Adipokines: molecular links between obesity and atheroslcerosis. Am J Physiol Heart Circ Physiol 288: H2031-2041.
20. Arner P (2005) Insulin resistance in type 2 diabetes -- role of the adipokines. Curr Mol Med 5: 333-339.
21. Spalding KL, Arner E, Westermark PO, Bernard S, Buchholz BA, et al. (2008) Dynamics of fat cell turnover in humans. Nature 453: 783-787.
22. Rutkowski JM, Davis KE, Scherer PE (2009) Mechanisms of obesity and related pathologies: the macro- and microcirculation of adipose tissue. Febs J 276: 5738-5746.
23. Steppan CM, Bailey ST, Bhat S, Brown EJ, Banerjee RR, et al. (2001) The hormone resistin links obesity to diabetes. Nature 409: 307-312.
24. Van Snick J (1990) Interleukin-6: an overview. Annu Rev Immunol 8: 253-278.
25. Sartipy P, Loskutoff DJ (2003) Monocyte chemoattractant protein 1 in obesity and insulin resistance. Proc Natl Acad Sci U S A 100: 7265-7270.
26. Weir GC, Bonner-Weir S (1990) Islets of Langerhans: the puzzle of intraislet interactions and their relevance to diabetes. J Clin Invest 85: 983-987.
27. Atef N, Ktorza A, Picon L, Penicaud L (1992) Increased islet blood flow in obese rats: role of the autonomic nervous system. Am J Physiol 262: E736-740.
28. Jansson L, Hellerstrom C (1983) Stimulation by glucose of the blood flow to the pancreatic islets of the rat. Diabetologia 25: 45-50.
29. Jansson L (1994) The regulation of pancreatic islet blood flow. Diabetes Metab Rev 10: 407-416.
30. Brunicardi FC, Stagner J, Bonner-Weir S, Wayland H, Kleinman R, et al. (1996) Microcirculation of the islets of Langerhans. Long Beach Veterans Administration Regional Medical Education Center Symposium. Diabetes 45: 385-392.
31. Kampf C, Bodin B, Kallskog O, Carlsson C, Jansson L (2005) Marked increase in white adipose tissue blood perfusion in the type 2 diabetic GK rat. Diabetes 54: 2620-2627.
32. Weir GC, Laybutt DR, Kaneto H, Bonner-Weir S, Sharma A (2001) Beta-cell adaptation and decompensation during the progression of diabetes. Diabetes 50 Suppl 1: S154-159.
33. Rothman DL, Shulman RG, Shulman GI (1992) 31P nuclear magnetic resonance measurements of muscle glucose-6-phosphate. Evidence for reduced insulin-dependent muscle glucose transport or phosphorylation activity in non-insulin-dependent diabetes mellitus. J Clin Invest 89: 1069-1075.
34. Dinneen S, Gerich J, Rizza R (1992) Carbohydrate metabolism in non-insulin-dependent diabetes mellitus. N Engl J Med 327: 707-713.
35. Sladek R, Rocheleau G, Rung J, Dina C, Shen L, et al. (2007) A genome-wide association study identifies novel risk loci for type 2 diabetes. Nature 445: 881-885.
36. Pierce M, Keen H, Bradley C (1995) Risk of diabetes in offspring of parents with non-insulin-dependent diabetes. Diabet Med 12: 6-13.
37. Reaven G (2002) Metabolic syndrome: pathophysiology and implications for management of cardiovascular disease. Circulation 106: 286-288.
38. Gale EA (2005) The myth of the metabolic syndrome. Diabetologia 48: 1679-1683.

54
39. Sjöholm A, Nyström T (2006) Inflammation and the etiology of type 2 diabetes. Diabetes Metab Res Rev 22: 4-10.
40. (1993) The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. The Diabetes Control and Complications Trial Research Group. N Engl J Med 329: 977-986.
41. Wilkinson K, Fikes J, Wojcik S (2001) Improved mouse blood smears using the DiffSpin slide spinner. Vet Clin Pathol 30: 197-200.
42. Feuerer M, Herrero L, Cipolletta D, Naaz A, Wong J, et al. (2009) Lean, but not obese, fat is enriched for a unique population of regulatory T cells that affect metabolic parameters. Nat Med 15: 930-939.
43. Maloy KJ, Powrie F (2001) Regulatory T cells in the control of immune pathology. Nat Immunol 2: 816-822.
44. Springer TA (1994) Traffic signals for lymphocyte recirculation and leukocyte emigration: the multistep paradigm. Cell 76: 301-314.
45. Ley K, Laudanna C, Cybulsky MI, Nourshargh S (2007) Getting to the site of inflammation: the leukocyte adhesion cascade updated. Nat Rev Immunol 7: 678-689.
46. Phillipson M, Heit B, Colarusso P, Liu L, Ballantyne CM, et al. (2006) Intraluminal crawling of neutrophils to emigration sites: a molecularly distinct process from adhesion in the recruitment cascade. J Exp Med 203: 2569-2575.
47. Dandona P, Aljada A, Bandyopadhyay A (2004) Inflammation: the link between insulin resistance, obesity and diabetes. Trends Immunol 25: 4-7.
48. Crook MA, Tutt P, Pickup JC (1993) Elevated serum sialic acid concentration in NIDDM and its relationship to blood pressure and retinopathy. Diabetes Care 16: 57-60.
49. Pickup JC, Mattock MB, Chusney GD, Burt D (1997) NIDDM as a disease of the innate immune system: association of acute-phase reactants and interleukin-6 with metabolic syndrome X. Diabetologia 40: 1286-1292.
50. Freeman DJ, Norrie J, Caslake MJ, Gaw A, Ford I, et al. (2002) C-reactive protein is an independent predictor of risk for the development of diabetes in the West of Scotland Coronary Prevention Study. Diabetes 51: 1596-1600.
51. Wellen KE, Hotamisligil GS (2005) Inflammation, stress, and diabetes. J Clin Invest 115: 1111-1119.
52. Schmidt MI, Duncan BB, Sharrett AR, Lindberg G, Savage PJ, et al. (1999) Markers of inflammation and prediction of diabetes mellitus in adults (Atherosclerosis Risk in Communities study): a cohort study. Lancet 353: 1649-1652.
53. Donath MY, Boni-Schnetzler M, Ellingsgaard H, Ehses JA (2009) Islet inflammation impairs the pancreatic beta-cell in type 2 diabetes. Physiology (Bethesda) 24: 325-331.
54. Weisberg SP, McCann D, Desai M, Rosenbaum M, Leibel RL, et al. (2003) Obesity is associated with macrophage accumulation in adipose tissue. J Clin Invest 112: 1796-1808.
55. Xu H, Barnes GT, Yang Q, Tan G, Yang D, et al. (2003) Chronic inflammation in fat plays a crucial role in the development of obesity-related insulin resistance. J Clin Invest 112: 1821-1830.
56. Chawla A, Nguyen KD, Goh YP (2011) Macrophage-mediated inflammation in metabolic disease. Nat Rev Immunol.
57. Nguyen KD, Qiu Y, Cui X, Goh YP, Mwangi J, et al. (2011) Alternatively activated macrophages produce catecholamines to sustain adaptive thermogenesis. Nature 480: 104-108.

55
58. Kanety H, Feinstein R, Papa MZ, Hemi R, Karasik A (1995) Tumor necrosis factor alpha-induced phosphorylation of insulin receptor substrate-1 (IRS-1). Possible mechanism for suppression of insulin-stimulated tyrosine phosphorylation of IRS-1. J Biol Chem 270: 23780-23784.
59. Strosberg AD, Pietri-Rouxel F (1996) Function and regulation of the beta 3-adrenoceptor. Trends Pharmacol Sci 17: 373-381.
60. Fain JN, Garcija-Sainz JA (1983) Adrenergic regulation of adipocyte metabolism. J Lipid Res 24: 945-966.
61. Nonogaki K (2000) New insights into sympathetic regulation of glucose and fat metabolism. Diabetologia 43: 533-549.
62. Tentolouris N, Argyrakopoulou G, Katsilambros N (2008) Perturbed Autonomic Nervous System Function in Metabolic Syndrome. Neuromolecular Med.
63. Ahren B (2000) Autonomic regulation of islet hormone secretion--implications for health and disease. Diabetologia 43: 393-410.
64. Bartness TJ, Bamshad M (1998) Innervation of mammalian white adipose tissue: implications for the regulation of total body fat. Am J Physiol 275: R1399-1411.
65. Granneman JG, Lahners KN, Chaudhry A (1991) Molecular cloning and expression of the rat beta 3-adrenergic receptor. Mol Pharmacol 40: 895-899.
66. Alemzadeh R, Tushaus KM (2004) Modulation of adipoinsular axis in prediabetic zucker diabetic fatty rats by diazoxide. Endocrinology 145: 5476-5484.
67. Perfetti R, Hui H, Chamie K, Binder S, Seibert M, et al. (2001) Pancreatic beta-cells expressing the Arg64 variant of the beta(3)-adrenergic receptor exhibit abnormal insulin secretory activity. J Mol Endocrinol 27: 133-144.
68. Jansson L (1984) The blood flow to the pancreas and the islets of Langerhans during an intraperitoneal glucose load in the rat. Diabetes Res 1: 111-114.
69. Jansson L, Hellerstrom C (1986) Glucose-induced changes in pancreatic islet blood flow mediated by central nervous system. Am J Physiol 251: E644-647.
70. Atef N, Lafontan M, Double A, Helary C, Ktorza A, et al. (1996) A specific beta 3-adrenoceptor agonist induces increased pancreatic islet blood flow and insulin secretion in rats. Eur J Pharmacol 298: 287-292.
71. Skeberdis VA (2004) Structure and function of beta3-adrenergic receptors. Medicina (Kaunas) 40: 407-413.
72. Manara L, Badone D, Baroni M, Boccardi G, Cecchi R, et al. (1996) Functional identification of rat atypical beta-adrenoceptors by the first beta 3-selective antagonists, aryloxypropanolaminotetralins. Br J Pharmacol 117: 435-442.
73. Skoglund G, Lundquist I, Ahren B (1986) Effects of alpha 1- and alpha 2-adrenoceptor stimulation and blockade on plasma insulin levels in the mouse. Pancreas 1: 415-420.
74. Flechtner-Mors M, Jenkinson CP, Alt A, Adler G, Ditschuneit HH (2002) In vivo alpha(1)-adrenergic lipolytic activity in subcutaneous adipose tissue of obese subjects. J Pharmacol Exp Ther 301: 229-233.
75. Ahren B, Schersten B (1986) Beta 2-adrenoceptor induced increase of plasma insulin levels in man: evidence of direct and indirect B-cell stimulation and liver effects. Diabetes Res 3: 443-445.
76. Jansson L, Eizirik DL, Sandler S (1989) Terbutaline decreases the blood flow of the pancreatic islets but does not reduce the diabetogenic action of streptozotocin in the rat. Eur J Pharmacol 161: 79-83.

56
77. Wajchenberg BL (2000) Subcutaneous and visceral adipose tissue: their relation to the metabolic syndrome. Endocr Rev 21: 697-738.
78. Krotkiewski M, Bjorntorp P, Sjostrom L, Smith U (1983) Impact of obesity on metabolism in men and women. Importance of regional adipose tissue distribution. J Clin Invest 72: 1150-1162.
79. Wild S, Roglic G, Green A, Sicree R, King H (2004) Global prevalence of diabetes: estimates for the year 2000 and projections for 2030. Diabetes Care 27: 1047-1053.
80. Mizutani T, Nishikawa Y, Adachi H, Enomoto T, Ikegami H, et al. (1994) Identification of estrogen receptor in human adipose tissue and adipocytes. J Clin Endocrinol Metab 78: 950-954.
81. Godsland IF (2005) Oestrogens and insulin secretion. Diabetologia 48: 2213-2220.
82. Sathyapalan T, Atkin SL (2010) Mediators of inflammation in polycystic ovary syndrome in relation to adiposity. Mediators Inflamm 2010: 758656.
83. Portha B, Serradas P, Bailbe D, Suzuki K, Goto Y, et al. (1991) Beta-cell insensitivity to glucose in the GK rat, a spontaneous nonobese model for type II diabetes. Diabetes 40: 486-491.
84. Bisbis S, Bailbe D, Tormo MA, Picarel-Blanchot F, Derouet M, et al. (1993) Insulin resistance in the GK rat: decreased receptor number but normal kinase activity in liver. Am J Physiol 265: E807-813.
85. Goto Y, Kakizaki M, Masaki N (1975) Spontaneous diabetes produced by selective breeding of normal Wistar rats. . Jpn Acad 51: 80-85.
86. Jansson L, Hellerstrom C (1981) A rapid method of visualizing the pancreatic islets for studies of islet capillary blood flow using non-radioactive microspheres. Acta Physiol Scand 113: 371-374.
87. Cara DC, Kaur J, Forster M, McCafferty DM, Kubes P (2001) Role of p38 mitogen-activated protein kinase in chemokine-induced emigration and chemotaxis in vivo. J Immunol 167: 6552-6558.
88. Heit B, Robbins SM, Downey CM, Guan Z, Colarusso P, et al. (2008) PTEN functions to 'prioritize' chemotactic cues and prevent 'distraction' in migrating neutrophils. Nat Immunol 9: 743-752.
89. Andersson A (1978) Isolated mouse pancreatic islets in culture: effects of serum and different culture media on the insulin production of the islets. Diabetologia 14: 397-404.
90. Holstad M, Jansson L, Sandler S (1996) Effects of aminoguanidine on rat pancreatic islets in culture and on the pancreatic islet blood flow of anaesthetized rats. Biochem Pharmacol 51: 1711-1717.
91. Eizirik DL, Migliorini RH (1984) Reduced diabetogenic effect of streptozotocin in rats previously adapted to a high-protein, carbohydrate-free diet. Diabetes 33: 383-388.
92. Takahashi H, Yoshida T, Nishimura M, Nakanishi T, Kondo M, et al. (1992) Beta-3 adrenergic agonist, BRL-26830A, and alpha/beta blocker, arotinolol, markedly increase regional blood flow in the brown adipose tissue in anesthetized rats. Jpn Circ J 56: 936-942.
93. Rayfield EJ, Ault MJ, Keusch GT, Brothers MJ, Nechemias C, et al. (1982) Infection and diabetes: the case for glucose control. Am J Med 72: 439-450.
94. Wheat LJ (1980) Infection and diabetes mellitus. Diabetes Care 3: 187-197. 95. Cinti S, Mitchell G, Barbatelli G, Murano I, Ceresi E, et al. (2005) Adipocyte
death defines macrophage localization and function in adipose tissue of obese mice and humans. J Lipid Res 46: 2347-2355.

57
96. Eller K, Kirsch A, Wolf AM, Sopper S, Tagwerker A, et al. (2011) Potential role of regulatory T cells in reversing obesity-linked insulin resistance and diabetic nephropathy. Diabetes 60: 2954-2962.
97. Kim A, Miller K, Jo J, Kilimnik G, Wojcik P, et al. (2009) Islet architecture: A comparative study. Islets 1: 129-136.
98. Arner P (2005) Resistin: yet another adipokine tells us that men are not mice. Diabetologia 48: 2203-2205.
99. Ihara Y, Toyokuni S, Uchida K, Odaka H, Tanaka T, et al. (1999) Hyperglycemia causes oxidative stress in pancreatic beta-cells of GK rats, a model of type 2 diabetes. Diabetes 48: 927-932.
100. Barbu A, Hedlund GP, Lind J, Carlsson C (2009) Pref-1 and adipokine expression in adipose tissues of GK and Zucker rats. Mol Cell Endocrinol 299: 163-171.
101. Leahy JL, Bonner-Weir S, Weir GC (1988) Minimal chronic hyperglycemia is a critical determinant of impaired insulin secretion after an incomplete pancreatectomy. J Clin Invest 81: 1407-1414.
102. Jansson L, Sandler S (1989) Pancreatic and islet blood flow in the regenerating pancreas after a partial pancreatectomy in adult rats. Surgery 106: 861-866.
103. Butler AE, Janson J, Soeller WC, Butler PC (2003) Increased beta-cell apoptosis prevents adaptive increase in beta-cell mass in mouse model of type 2 diabetes: evidence for role of islet amyloid formation rather than direct action of amyloid. Diabetes 52: 2304-2314.
104. Moldovan S, Livingston E, Zhang RS, Kleinman R, Guth P, et al. (1996) Glucose-induced islet hyperemia is mediated by nitric oxide. Am J Surg 171: 16-20.
105. Carlsson PO, Andersson A, Jansson L (1998) Influence of age, hyperglycemia, leptin, and NPY on islet blood flow in obese-hyperglycemic mice. Am J Physiol 275: E594-601.
106. Carlsson PO, Jansson L, Ostenson CG, Kallskog O (1997) Islet capillary blood pressure increase mediated by hyperglycemia in NIDDM GK rats. Diabetes 46: 947-952.
107. Svensson AM, Ostenson CG, Jansson L (2000) Age-induced changes in pancreatic islet blood flow: evidence for an impaired regulation in diabetic GK rats. Am J Physiol Endocrinol Metab 279: E1139-1144.
108. Arner P, Hellstrom L, Wahrenberg H, Bronnegard M (1990) Beta-adrenoceptor expression in human fat cells from different regions. J Clin Invest 86: 1595-1600.
109. Anthony A, Sim R, Guillaume JL, Strosberg AD, Dhillon AP, et al. (2000) Beta(beta)3-adrenergic receptors in human pancreatic islet and duodenal somatostatin neuroendocrine cells. Aliment Pharmacol Ther 14: 579-585.
110. Grujic D, Susulic VS, Harper ME, Himms-Hagen J, Cunningham BA, et al. (1997) Beta3-adrenergic receptors on white and brown adipocytes mediate beta3-selective agonist-induced effects on energy expenditure, insulin secretion, and food intake. A study using transgenic and gene knockout mice. J Biol Chem 272: 17686-17693.
111. Bonner-Weir S, Orci L (1982) New perspectives on the microvasculature of the islets of Langerhans in the rat. Diabetes 31: 883-889.
112. Barbe P, Millet L, Galitzky J, Lafontan M, Berlan M (1996) In situ assessment of the role of the beta 1-, beta 2- and beta 3-adrenoceptors in the control of lipolysis and nutritive blood flow in human subcutaneous adipose tissue. Br J Pharmacol 117: 907-913.

58
113. Lafontan M, Bousquet-Melou A, Galitzky J, Barbe P, Carpene C, et al. (1995) Adrenergic receptors and fat cells: differential recruitment by physiological amines and homologous regulation. Obes Res 3 Suppl 4: 507S-514S.
114. Bloom JD, Dutia MD, Johnson BD, Wissner A, Burns MG, et al. (1992) Disodium (R,R)-5-[2-[[2-(3-chlorophenyl)-2-hydroxyethyl]-amino] propyl]-1,3-benzodioxole-2,2-dicarboxylate (CL 316,243). A potent beta-adrenergic agonist virtually specific for beta 3 receptors. A promising antidiabetic and antiobesity agent. J Med Chem 35: 3081-3084.
115. Cawthorne MA, Carroll MJ, Levy AL, Lister CA, Sennitt MV, et al. (1984) Effects of novel beta-adrenoceptor agonists on carbohydrate metabolism: relevance for the treatment of non-insulin-dependent diabetes. Int J Obes 8 Suppl 1: 93-102.
116. Jocken JW, Blaak EE (2008) Catecholamine-induced lipolysis in adipose tissue and skeletal muscle in obesity. Physiol Behav.
117. Blaak EE, Van Baak MA, Kemerink GJ, Pakbiers MT, Heidendal GA, et al. (1994) beta-Adrenergic stimulation of skeletal muscle metabolism in relation to weight reduction in obese men. Am J Physiol 267: E316-322.
118. Blaak EE, Van Baak MA, Kemerink GJ, Pakbiers MT, Heidendal GA, et al. (1994) Beta-adrenergic stimulation of energy expenditure and forearm skeletal muscle metabolism in lean and obese men. Am J Physiol 267: E306-315.
119. Connacher AA, Bennet WM, Jung RT, Bier DM, Smith CC, et al. (1991) Effect of adrenaline infusion on fatty acid and glucose turnover in lean and obese human subjects in the post-absorptive and fed states. Clin Sci (Lond) 81: 635-644.
120. Arner P (1999) Catecholamine-induced lipolysis in obesity. Int J Obes Relat Metab Disord 23 Suppl 1: 10-13.
121. Reynisdottir S, Ellerfeldt K, Wahrenberg H, Lithell H, Arner P (1994) Multiple lipolysis defects in the insulin resistance (metabolic) syndrome. J Clin Invest 93: 2590-2599.
122. Marble A, White HJ, Fernald AT (1938) The Nature of the Lowered Resistance to Infection in Diabetes Mellitus. J Clin Invest 17: 423-430.
123. Cruz JW, Oliveira MA, Hohman TC, Fortes ZB (2000) Influence of tolrestat on the defective leukocyte-endothelial interaction in experimental diabetes. Eur J Pharmacol 391: 163-174.
124. Panes J, Kurose I, Rodriguez-Vaca D, Anderson DC, Miyasaka M, et al. (1996) Diabetes exacerbates inflammatory responses to ischemia-reperfusion. Circulation 93: 161-167.
125. Sampson MJ, Davies IR, Brown JC, Ivory K, Hughes DA (2002) Monocyte and neutrophil adhesion molecule expression during acute hyperglycemia and after antioxidant treatment in type 2 diabetes and control patients. Arterioscler Thromb Vasc Biol 22: 1187-1193.
126. Rich J, Lee JC (2005) The pathogenesis of Staphylococcus aureus infection in the diabetic NOD mouse. Diabetes 54: 2904-2910.
127. Cho CH, Koh YJ, Han J, Sung HK, Jong Lee H, et al. (2007) Angiogenic role of LYVE-1-positive macrophages in adipose tissue. Circ Res 100: e47-57.
128. Lumeng CN, Bodzin JL, Saltiel AR (2007) Obesity induces a phenotypic switch in adipose tissue macrophage polarization. J Clin Invest 117: 175-184.
129. Morris DL, Singer K, Lumeng CN (2011) Adipose tissue macrophages: phenotypic plasticity and diversity in lean and obese states. Curr Opin Clin Nutr Metab Care 14: 341-346.

59
130. Lumeng CN, Delproposto JB, Westcott DJ, Saltiel AR (2008) Phenotypic switching of adipose tissue macrophages with obesity is generated by spatiotemporal differences in macrophage subtypes. Diabetes.
131. McDonald B, Pittman K, Menezes GB, Hirota SA, Slaba I, et al. (2011) Intravascular danger signals guide neutrophils to sites of sterile inflammation. Science 330: 362-366.
132. Kosteli A, Sugaru E, Haemmerle G, Martin JF, Lei J, et al. (2010) Weight loss and lipolysis promote a dynamic immune response in murine adipose tissue. J Clin Invest 120: 3466-3479.
133. Goran MI, Ball GD, Cruz ML (2003) Obesity and risk of type 2 diabetes and cardiovascular disease in children and adolescents. J Clin Endocrinol Metab 88: 1417-1427.
134. Manolopoulos KN, Karpe F, Frayn KN (2010) Gluteofemoral body fat as a determinant of metabolic health. Int J Obes (Lond) 34: 949-959.
135. Ofei F, Hurel S, Newkirk J, Sopwith M, Taylor R (1996) Effects of an engineered human anti-TNF-alpha antibody (CDP571) on insulin sensitivity and glycemic control in patients with NIDDM. Diabetes 45: 881-885.
136. Di Rocco P, Manco M, Rosa G, Greco AV, Mingrone G (2004) Lowered tumor necrosis factor receptors, but not increased insulin sensitivity, with infliximab. Obes Res 12: 734-739.
137. Stanley TL, Zanni MV, Johnsen S, Rasheed S, Makimura H, et al. (2011) TNF-alpha antagonism with etanercept decreases glucose and increases the proportion of high molecular weight adiponectin in obese subjects with features of the metabolic syndrome. J Clin Endocrinol Metab 96: E146-150.
138. Chan JC, Cheung JC, Stehouwer CD, Emeis JJ, Tong PC, et al. (2002) The central roles of obesity-associated dyslipidaemia, endothelial activation and cytokines in the Metabolic Syndrome--an analysis by structural equation modelling. Int J Obes Relat Metab Disord 26: 994-1008.
139. Payette C, Blackburn P, Lamarche B, Tremblay A, Bergeron J, et al. (2009) Sex differences in postprandial plasma tumor necrosis factor-alpha, interleukin-6, and C-reactive protein concentrations. Metabolism 58: 1593-1601.
140. Giraldo E, Hinchado MD, Garcia JJ, Ortega E (2008) Influence of gender and oral contraceptives intake on innate and inflammatory response. Role of neuroendocrine factors. Mol Cell Biochem 313: 147-153.
141. Lee CG, Carr MC, Murdoch SJ, Mitchell E, Woods NF, et al. (2009) Adipokines, inflammation, and visceral adiposity across the menopausal transition: a prospective study. J Clin Endocrinol Metab 94: 1104-1110.
142. Poehlman ET, Toth MJ, Gardner AW (1995) Changes in energy balance and body composition at menopause: a controlled longitudinal study. Ann Intern Med 123: 673-675.
143. Crandall DL, Busler DE, Novak TJ, Weber RV, Kral JG (1998) Identification of estrogen receptor beta RNA in human breast and abdominal subcutaneous adipose tissue. Biochem Biophys Res Commun 248: 523-526.
144. Soeters MR, Sauerwein HP, Groener JE, Aerts JM, Ackermans MT, et al. (2007) Gender-related differences in the metabolic response to fasting. J Clin Endocrinol Metab 92: 3646-3652.
145. Hevener A, Reichart D, Janez A, Olefsky J (2002) Female rats do not exhibit free fatty acid-induced insulin resistance. Diabetes 51: 1907-1912.
146. Liu S, Mauvais-Jarvis F (2009) Minireview: Estrogenic protection of beta-cell failure in metabolic diseases. Endocrinology 151: 859-864.

60
147. El Seifi S, Green IC, Perrin D (1981) Insulin release and steroid-hormone binding in isolated islets of langerhans in the rat: effects of ovariectomy. J Endocrinol 90: 59-67.
148. Tiano JP, Delghingaro-Augusto V, Le May C, Liu S, Kaw MK, et al. (2011) Estrogen receptor activation reduces lipid synthesis in pancreatic islets and prevents beta cell failure in rodent models of type 2 diabetes. J Clin Invest 121: 3331-3342.