Embed Size (px)
Citation preview

ListServ Live Webinar SeriesHosted by the AAP Section on Hospital Medicine

Michelle Hofmann, MD, MPH, FAAP

Objectives
•Be Ready: Understand the role of medical technology and device complications as antecedents to potentially preventable hospitalizations
•Get Set: Examine a systematic approach to preparing technology‐dependent children for hospital discharge
•Go: Prepare to respond to emergencies related to device complications in technology‐dependent children

All U.S. Children
Children with Special Health Care Needs
13%
Children with Disability that Impairs Functional Daily Living
6.5%
Children Dependent on Technology
0.16%
Care of the Child Assisted by TechnologyLaurie J. Glader, Judith S. PalfreyPediatrics in Review Nov 2009, 30 (11) 439‐445

WebEx Multiple Choice Question
What proportion of your hospitalist practice includes caring for children assisted by technology?A. <1%B. 1‐5% C. 6‐25%D. 26‐50%E. >50%

https://www.abp.org/sites/abp/files/pdf/hospital_medicine_content_outline.pdf

Children with Medical Complexity (CMC)
A child with medical complexity…1. Has a diversity of conditions and
multisystem disease2. May be technology‐supported3. Has frequent inpatient admissions4. Requires multiple medications5. Requires multiple subspecialties6. Requires optimal care coordination
across inpatient & outpatient settings
Cohen et al. "Children with medical complexity: an emerging population for clinical and research initiatives.“
Pediatrics 127.3 (2011): 529‐538.

CMC: A High‐Need High‐Cost Population
Less than 1% of all children1
Equipment / suppliesTestingHome carePrimary careEmergency careMedicationsSpecialty careHospital care
30% of all pediatric healthcare costs2
1Kuo et al, Arch Ped Adol Med (2011)2Cohen et al, Pediatrics (2012)3Berry at al, JAMA Pediatrics (2013)4Bogetz et al, Pediatr Clinics North Amer (2014)5Berry at al, Health Affairs (2014)
$650 billion annually5
55% of all inpatient costs in children’s
hospitals3
85% of all 30‐day readmission costs in children’s hospitals4
85%

Longer LOS as Another Cost Driver
•Higher severity of acute illnesses•Prolonged recovery time in the hospital•Higher risk of adverse events in the hospital•Difficult to determine discharge readiness
•Many CMC do not return to a completely healthy baseline
Gold, J et al. (2016). Long length of hospital stay in children with medical complexity. Journal of Hospital Medicine, 11(11), 750‐756.

Gold, J et al. (2016). Long length of hospital stay in children with medical complexity. Journal of Hospital Medicine, 11(11), 750‐756.
Variations in Hospital Utilization Suggest LOS Reductions are Possible
22%
11%

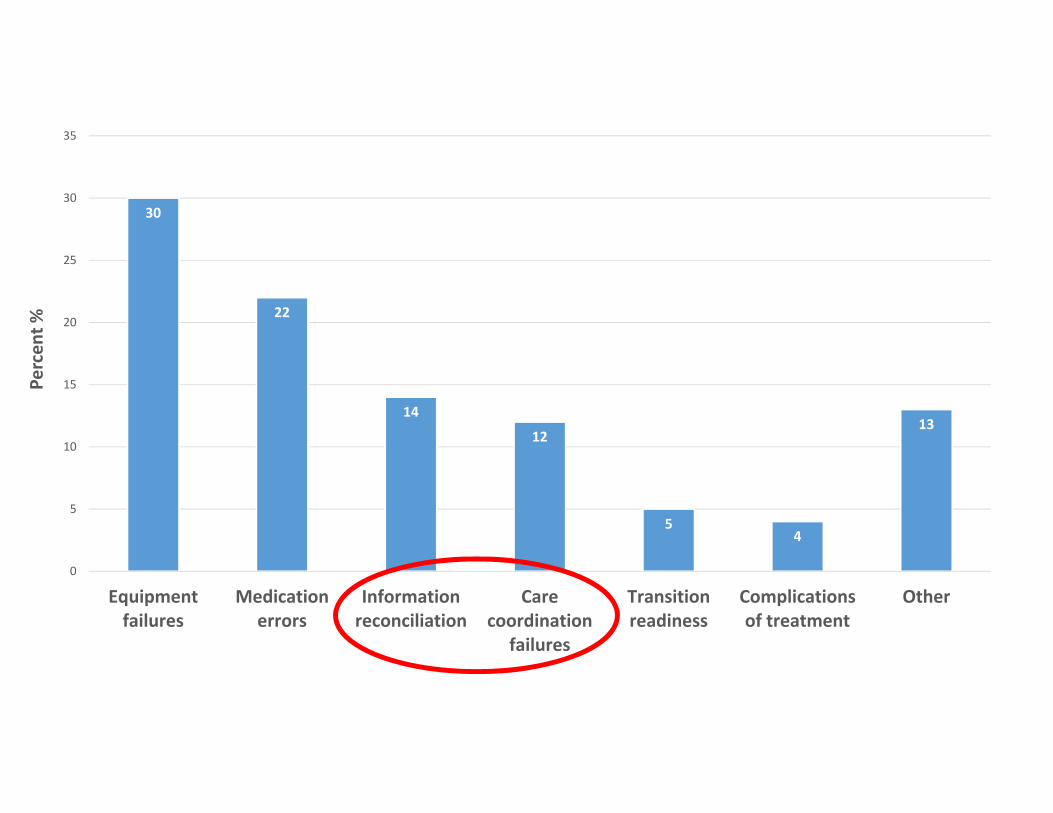
Technology Complications are Common and May be Preventable
• 53% with ≥4 rehospitalizations had technology assistance1• Device complications in 8‐9% of admissions1,2,3
• Tracheostomy complications in 12‐17% of readmissions in year following initiation of home mechanical ventilation4
• Among 248 unscheduled ICU admissions, 19% in technology assisted group labeled potentially preventable5
• 43% of 15‐day readmissions associated with central line infections or ventricular shunt malfunctions labeled potentially preventable6
1. Berry JG et al. JAMA. 2011;305(7):682–6902. Gay JC et al. Pediatrics. 2011;127 (6)3. Berry JG et al. J Pediatr. 2011;159(2):284–2904. Kun SS et al. Pediatr Pulmonol. 2012;47(4):409–4145. Dosa NP et al. Pediatrics. 2001;107(3):499–5046. Hain PD et al. Pediatrics. 2013;131(1)

30
22
14
12
54
13
0
5
10
15
20
25
30
35
Equipmentfailures
Medicationerrors
Informationreconciliation
Carecoordination
failures
Transitionreadiness
Complicationsof treatment
Other
Percen
t %

12 year old with tracheostomy dependency readmitted shortly after discharge following prolonged a hospitalization for pneumonia
• Ordinarily on room air, but discharged on 2 liters of trach mask oxygen• Mucus plugging event resulting in oxygen need exceeding what could be delivered at home so caregiver called 911
• Pneumonia was first hospitalization in many years• He is generally very healthy with minimal suction need when well• On readmission, caregiver reports not remembering emergency measures she had been taught so many years ago
“I just didn’t know what to do or who to call. It’s been so long since he has had any problems.”
4 year old with Down’s syndrome and gastrostomy dependency admitted every few months for recurrent episodes of vomiting
• On admission, caregiver is asked what has worked well during prior hospitalizations and the team implements her recommendations
• Patient generally tolerates enteral fluids without the need for an IV but consistently requires 3‐4 days to return to baseline feeds
• Caregiver hesitant to go home even when child is back to baseline
“We live 2 hours away in a small town. I don’t trust anyone. The last time I went to emergency, they poked her 5 times to get an IV. Now I drive straight here when she starts vomiting.”

WebEx Multiple Choice Question
Reflecting on these cases, which represent potentially preventable hospitalizations?A. 12 year old with trach readmitted after hospital discharge with
increased oxygen needB. 4 year old with G‐tube feeds with recurrent admissions for vomiting C. Both of the aboveD. Neither of the above

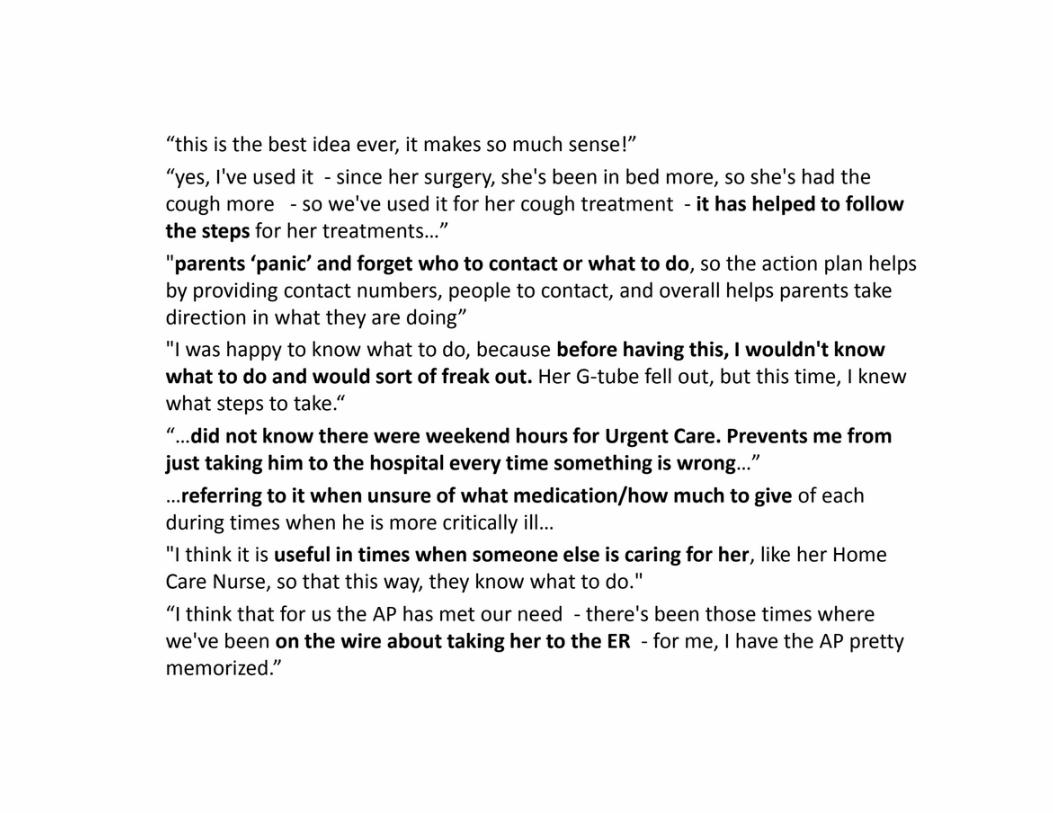
Plans for Action and Care Transitions (PACT) have 2 elements:(1) customized written plans to address triggers of hospital use (“action plans”) (2) structured care transition coaching around hospital discharge

Coller, Nelson, Klitzner, Saenz, Shekelle, Lerner, & Chung. (2017). Strategies to Reduce Hospitalizations of Children With Medical Complexity Through Complex Care: Expert Perspectives. Academic Pediatrics, 17(4), 381‐388.

Action Plans for CMC• Provide families with confidence / direction to manage crises in most appropriate setting
• Developed / refined by medical home with caregiver input 1. Identify focus areas based on history and caregiver opinion about what is most
likely to lead to future hospitalization 2. Define objective and subjective signs of baseline (green), worsening (yellow),
and severe (red) statuses3. Delineate specific actions caregivers can take to prevent / manage each status
• Uses caregivers’ preferred language / teach‐back to assess understanding• Gives direction on who and when to call (e.g., PCP, specialist, go to ED)


23%
15%
13%10%
9%
9%
9%
4%4%
4%Respiratory distressFeverTube feedsGeneral access issuesAbdominal painSeizuresAsthmaUrinary tract infectionTracheitisVomiting

PACT Usual Care
Adjusted Incidence Rate Ratio (IRR)
N 77 70
Hospitalization rates / 100 child years
81 101 0.61; 95% CI 0.38‐0.97
All‐cause 30‐day readmission rates / 100 child years
17 23 0.37; 95% CI 0.14‐0.98
Aggregate charges during study were $944,759 lower for the 77 PACT participants

Can I Play a Role in Escalation Planning?
• Time and a “captive” audience• Explicit knowledge
• What does “sick” look like• What works and doesn’t work• Caregiver comfort and capabilities
• Necessary skills• Additional resources

Does Your Patient Have a Medical Home?
Care coordinator employed by single primary care practice
Hospital‐ or specialty‐based complex care
programs
“Enhanced” pediatric health homes with
primary care and sub‐specialty co‐management

Who is the patient and family’s partner?

Super Parents Project, December 2016, Lucile Packard Foundation for Children’s Health
“To deliver on its promise, the medical home needs a hospitable and high‐performing medical neighborhood.”
Elliott Fisher, NEJM, 2008

What Do You Know about Local Access?
43% of pediatricians prefer a subspecialty medical home for CMC1
Nationally, 40% of CMC do not have an annual primary care visit2
1600 PCPs in Utah refer their patients to Primary Children’s Hospital and its affiliated clinics…only 12% are recognized as patient‐centered medical homes
1Van Cleave et al, Academic Pediatrics (2016)2Berry at al, Health Affairs (2014)

What Do You Know About Local Access?• Discharge delay (DD) in 68.5% of new home health patients and 9.2% of existing patients
• Average LOS increase of 53.9 days (range: 4–204) and 35.7 days (3–63) for new and existing patients, respectively
• Of 1582 DDs, 92% directly attributed to lack of home care nursing (HCN) availability
• DDs associated with estimated $170,954 per patient
1Hefner et al. Ventilator‐Dependent Children and the Health Services System: Unmet Needs and Coordination of Care. Ann Am Thorac Soc 2013; 10(5):482‐489.
2Home Health Care Availability and Discharge Delays in Children With Medical ComplexityMaynard et al. Pediatrics Jan 2019, 143(1).

“Hospital At Home”...at the Family’s Expense• 1.5 billion hours of skilled health care (distinct from care coordination) services provided by families in their homes annually
• Equivalent, in some aspects, to hospital level of care• Recently hospitalized CMC may need weeks or months of sustained, intense, daily caregiving to recover from illness
• Families’ efforts, out‐of‐pocket expenses, and missed days of work providing extensive home care are a financial and emotional burden
• 60% of families of CMC report having to stop work for pay• 57% report having financial problems
• Annual replacement cost of unpaid skilled labor provided by families at home estimated at $35.7 billion
Romley JA et al. Family‐Provided Health Care for Children With Special Health Care Needs. Pediatrics 2017; 139(1):e20161287.

Objectives
Be Ready: Understand the role of medical technology and device complications as antecedents to potentially preventable hospitalizations
•Get Set: Examine a systematic approach to preparing technology‐dependent children for hospital discharge
•Go: Prepare to respond to emergencies related to device complications in technology‐dependent children

2 year old with spinal muscular atrophy and nocturnal BiPAPdependency transferred to floor on Sunday night after 10 days in the PICU for pneumonia
• You begin attending on a new clinical service week on Monday• Before rounds you run the patient list with the senior resident, who says the patient has completed antibiotics, on his baseline oxygen, and ready for discharge
• You ask about his current airway clearance regimen and she tells you he is receiving albuterol, vest physiotherapy, and cough assist every 4 hours
• You ask about his baseline airway clearance regimen at home and who helps to provide this care
“I’m not sure.”

WebEx Multiple Choice Question
When caring for children assisted by technology at my hospital, it is easy to determine what treatments, equipment, nursing care and other services are in place at home. A. Strongly agreeB. AgreeC. NeutralD. DisagreeE. Strongly disagree

Clinical Information Reconciliation
At its most basic level, this entails comparing and reconciling simple lists of clinical information.
At a more sophisticated level, it assures that comparable data from multiple sources is consistent and accurate, or that inconsistencies are accounted for.
Healthcare Information and Management Systems Society
30
22
14
12
54
13
0
5
10
15
20
25
30
35
Equipmentfailures
Medicationerrors
Informationreconciliation
Carecoordination
failures
Transitionreadiness
Complicationsof treatment
Other
Percen
t %

A dvance directives, allergies, active problems F ollow‐up appointments, financial supportO rders for DME, home care, testsC are coordination, care team providersU rgent care / escalation plans S ocial / emotional supportE thnic / cultural / language supportD ietM edications, medical homeE quipmentN ursing care at home or in a rehabilitation facilityD evelopmental / educational services Mnemonic courtesy of Jay Berry,
Boston Children’s Hospital





30
22
14
12
54
13
0
5
10
15
20
25
30
35
Equipmentfailures
Medicationerrors
Informationreconciliation
Carecoordination
failures
Transitionreadiness
Complicationsof treatment
Other
Percen
t %

Conceptual framework illustrating 7 domains regarding parents’ priorities and goals for their hospital-to-home transition.
JoAnna K. Leyenaar et al. Pediatrics 2017;139:e20161581
©2017 by American Academy of Pediatrics

Objectives
Be Ready: Understand the role of medical technology and device complications as antecedents to potentially preventable hospitalizations
Get Set: Examine a systematic approach to preparing technology‐dependent children for hospital discharge
•Go: Prepare to respond to emergencies related to device complications in technology‐dependent children

2 month old term male with Pierre Robin S/P tracheostomy shortly after birth admitted for poor feeding and weight loss
• Progressive feeding difficulty, NG placed for hydration / nutrition with plan for lactation and speech therapy evaluations in the morning
• Overnight develops fever to 38.1, HR 150, BP 90/60, RR 58, SaO2 92% on room air
• Tired, less active, substernal retractions, tracheostomy site non‐erythematous with increased thick white secretions
• Initiate trach collar oxygen, suction with small amounts of saline• He abruptly desaturates and his HR drops to 70, not getting much with additional suctioning
WebEx Multiple Choice Question
You suspect the tube is occluded and needs to be changed. What should you do?A. Flush trach with saline and suction againB. Call ENTC. Change trach using spare in “go bag”D. Remove trach and insert age‐appropriate endotracheal tube
through stomaE. Call a code blue

Tracheostomy Emergency Pearls
• Stoma matures in one month – you can change it out after that
• Suction, suction, suction• Don’t forget the go bag• You can always place an ETT if the patient is critical

Ligoski Dal’Astra et al, Tracheostomy in childhood: review of the literature on complications and mortality over the last three decades, Braz J of Oto, 2017, 83(2):207‐214

Partially or Totally Occluded TracheostomySigns/Symptoms:• Absent air entry or chest rise• Increased inhalation/exhalation time
• Increased accessory muscle use • Hypoxemia• Inability or difficulty passing suction catheter
• High pressure alarm on ventilator
Response:• Place on high‐flow O2• Suction tracheostomy tube with normal saline
• If unable to clear secretions or plug by suctioning, change tracheostomy tube
Prevention:• Adequate humidification keeps tracheostomy secretions thin / helps prevent plugs

Accidental Decannulation
Scenarios:• Child moves during tie change• Tracheostomy tube length to short
• Tracheostomy tube ties too loose
• Pull on tracheostomy from ventilator or other tubing
Response:• Change the tracheostomy tube
D islodged, displaced, damaged
O bstructed
P neumothorax, pulmonary problem
E quipment failure

Inability to Replace Tracheostomy• Oxygen over stoma, BMV through mouth
• Suction catheter in stoma TKO• ETT through stoma
• Same or smaller diameter• Measure against tracheostomy tube and don’t advance beyond carina
• Confirm with chest x‐ray• Orally intubate
• Depends on upper airway anatomy / reason for tracheostomy

5 year old female with craniopharyngioma S/P resection with prolonged hospitalization for panhypopituitarism and refractory diabetes insipidus• PEG placed 1 month ago for supplemental feeds and fluid management
• Progressive obesity with rapid weight gain despite calorie restriction• Intermittent complaints of pain around PEG site but abdominal exam and feeding tolerance always reassuring
• Today, bedside nurse reports feeds more difficult to infuse• Flushed tube with warm water, which leaked around tube and resulted in sharp, instantaneous pain
• On exam, she has normal vital signs and the PEG site mildly tender with minimal erythema and no induration or drainage
• You note the external bolster of PEG protruding more from skin surface and tube is not mobile

WebEx Multiple Choice Question
What is your diagnosis?A. Dislodged tubeB. Buried bumper syndromeC. Localized wound infectionD. Uncomplicated PEG tube leakageE. Clogged tube

Buried Bumper Syndrome (BBS)• Rare complication of PEG placement• Days to years post‐PEG• Life‐threatening—stomach perforation, peritonitis, death
• Risk factors—obesity, rapid weight gain, frequent / inadvertent tube traction, gauze placed beneath external bumper instead of over it, chronic cough
• Signs and symptoms—immobile tube, abdominal pain, difficulty infusing feeds, leakage, internal button palpable
• Diagnosis—Clinical, CT, endoscopically• Requires removal of PEG even if aymptomatic

Dislodged Gastrostomy TubeHistory• GJ tube—IR or surgery to replace
• Determine if mature or immature tract
• Generally matures in 4‐6 weeks
• Less than 3 moths, consider contacting service who placed it
• If out, how long? Stoma will close in 1‐3 hours
Stoma immature:• Place foley in stoma immediately, do not inflate balloon
• Do not force, avoid pushing stomach away from anterior abdominal wall
• Call GI or surgery for definitive care• Dye study to confirm replacementStoma mature:• Replace with same size of tube immediately• Unable to place same size, then place smaller tube

Objectives
Be Ready: Understand the role of medical technology and device complications as antecedents to potentially preventable hospitalizations
Get Set: Examine a systematic approach to preparing technology‐dependent children for hospital discharge
Go: Prepare to respond to emergencies related to device complications in technology‐dependent children

Resources• Complex Care Special Interest Group
https://sites.google.com/site/complexcarehome/home• Lucile Packard Foundation
http://www.lpfch.org/cshcn/advocacy/join‐advocacy‐network• Children’s Hospital Association
https://www.childrenshospitals.org/Issues‐and‐Advocacy/Children‐With‐Medical‐Complexity
• Med Ed Portal Simulation Series: Emergencies in Technology‐Dependent Children by Neha Shah, MD et alhttps://www.mededportal.org/publication/9310/
• Pediatric Emergency Playbook: The Technologically Dependent Child in the ED by Tim Horeczko, MDhttps://pemplaybook.org/podcast/234/
• Caring for Children Who Have Severe Neurological Impairment: A Life with Grace by Julie M. Hauer, MD
Thank You
All webinars are available at:
http://www.sohmlibrary.org/webinars.html