Embed Size (px)
Citation preview

Liver Tumors in Infancy and Childhood *
H. WILLIAM CLATWORTHY, JR., M.D., E. THOMAS BOLES, JR., M.D.,PETER K. KOTTMEIER, M.D.
From the Department of Surgery, Ohio State University College of Medicineand the Columbus Children's Hospital
THE MAJORITY of primary liver tumors ininfants and children are malignant, occurin the first two years of life, and until re-cently, have seldom been curable. Thereare, in addition, a significant number ofrelatively benign lesions which are amen-able to surgical treatment. The purpose ofthis paper is to review our experience with19 cases of primary liver tumors and topresent the results of a survey of the ex-perience of others with 75 collected casesof malignant tumors. Particular referenceis made to the surgical procedures thathave been employed to eradicate theselesions. The results that have been achievedby aggressive treatment will be empha-sized.Dargeon encountered only 13 cases of
cancer of the liver in a collected review of1,728 cases of malignant disease in theyounger age groups.4 By contrast, at theColumbus Children's Hospital primary tu-mors of the liver are the third most com-mon intra-abdominal neoplasm, exceededonly by neuroblastomas and Wilms tumors.It is obvious that clinicians dealing withchildren with abdominal masses should bealert to the possibility of primary livertumors, aware of the diagnostic criteria,and prepared to cope surgically with re-sectable lesions.
Classification and PathologyThere is a wide variety of gross and
microscopic characteristics in primary liver
* Presented before the American Surgical Asso-ciation, Boca Raton, Florida, March 21-23, 1961.
Supported by the Children's Hospital Investiga-tive Laboratory Division.
tumors, and only a relatively small numberof cases can be collected in any single in-stitution. The collected case review of Ed-mondson enabled him to adopt a patho-logic classification which may be used.5For the clinician such a classification ismore complex than is essential and doesnot take into account the clinical behaviorof individual lesions, which does not al-ways correlate closely with the microscopicappearance.For practical reasons, therefore, the liver
tumors that we have observed have beengrouped into four broad categories.
1. Tumors of Hepatic Cell Origin. Thisgroup includes all tumors derived fromentodermal cells such as hepatomas, chol-angiomas and cholangiohepatomas. In thisseries hepatoma was the most commontumor encountered, occurring in 13 of the19 cases. Six were in the right lobe, twoin the left and five were centrally located.These neoplasms may be either embryonalin type (hepatoblastoma) or of the adulttype.16 Twelve of the 13 were of theformer type, and in all 12 the initial clin-ical manifestations occurred within the firstthree years of life. The sole example of theadult type hepatoma occurred in a 14-year-old girl with post-necrotic cirrhosis, andshe is the only patient in the series withassociated cirrhosis. There were no ad-enomas in this group, and even the mature,relatively benign appearing hepatomas in-variably behaved as malignant lesions.There was one case of benign cholangio-hepatoma occurring in the right lobe of a10-weeks-old infant.
475

476 CLATWORTHY, BOLES AND KOTTMIEIER
TABLE 1. Collected Series * Hepatomas in Childhood
Total cases
Age:Under 2 years (66%/o)**
Sex:Female 33Male 42
Location of tumor:Right lobeL,eft lobeCentral or multicentric
Resections:Right lobectomy
Operative deaths-3Left lobectomy
Operative deaths-0Survivors:
6 months to 3 yearsOver 3 years
75
44
316
38
17
6
35
* Compiled from data received by request from 25pediatric surgical services, 1950-1960.
** 44 of 66 cases in which the age was recorded.
2. Tumors of Supporting Structures.Included in this group were those tumorsof mesodermal origin, including fibromas,hemangiomas, lymphangiomas, fibroangio-mas and mesenchymomas. Rhabdomyosar-comas and hemangio-endotheliomas havealso been described. Such neoplasms maybe diffuse or localized. There are fourexamples of this general group in thisseries. Two were giant lymphangiomas,both involving almost the entire right lobe.One fibroangioma occupied most of theleft lobe. Finally, there was one exampleof diffuse hemangiomatosis involving notonly the liver but pancreas and skin aswell.
3. Teratomas and Hamartomas havebeen discussed by others but were notencountered in this series.
4. Inflammatory. Although not neoplas-tic, a final case of inflammatory origin isincluded because its gross appearance was
remarkably similar to that of a hepatoma.This newborn infant had a tumor-like le-sion involving the entire left lobe whichproved on microscopic examination to be a
Annals of SurgerySeptember 1961
nodular type of cirrhosis, presumably theend result of intra-uterine hepatitis.The gross appearance of solid tumors in
the liver is so strikingly similar that dif-ferentiation at the operating table is indeedunreliable. Even microscopic differentia-tion between benign and malignant livercell tumors is occasionally virtually impos-sible. For example, one of the hepatomasin this series exhibited an architecture mostsuggestive of a benign adenomatous typeneoplasm. However, metastases were pres-ent and established the true malignant na-ture of this lesion.
DiagnosisThe majority of primary neoplasms of
the liver come to the attention of thephysician in the first two years of life. Onlythree of the 19 cases in this series had theonset of symptoms after two years of age,and in ten there was clinical evidence ofthe tumor in the first six months of lite. Asurvey by questionnaire of surgeons activein pediatric surgical practice has permittedus to collect certain data on 75 additionalcases of malignant tumors of the liver.' Inthis group 66 per cent were diagnosed inthe first two years of life, although scat-tered cases through the eighteenth yearwere reported * * (Table 1).
* The authors express their grateful apprecia-tion to the 25 surgeons in pediatric surgical centerswho cooperated in the compilation of this data.
* * 66 per cent represents 44 out of 66 cases inwhom the age of the patient was reported.
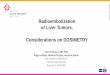
FIG. 1. Seven-month-old male infant with alarge visible mass in the epigastrium. At explora-tion an embryonal hepatoma of the left lobe withmetastases to the right lobe was found.
.... .... ala

LIVER TUM\IORS IN INFANCY ANI) CHILDHOOD
Tlhe dc-veloplment of ad(lolninal elaLlroe-men'lt andl( 1 plpall)tlle l]<ss lmvc Ow1(''}l(presenting complaints iln 11lost illstaneeis
(Fig. 1 ). The distrihiition in the liver ofthese 19 ttunors w-as as follows: ninie e-rein the right lohe, fouir in the left andi therema.liniig(r six centrally placed or dliffuise(Fig. _2). In imiost inistaciiecs, therefore, themass wN-ill l)e fotind( in the rig(rlt utpper
quadrant. Fixation is rare, and the ttuinmor,
therefore, m-oves xv-ith respiration. The
characteristics of the lesion 1by palpationvary considerablv, hut mnost are hard,
rouinded or contain larrge i7odtiles w-hiciare inseparahle froim the liver edge. Trains-illtminaitioni is at useful techliie in differ-entiatinfg solid froIml cystic lesions, an(d was
diacgnostic in hoth lvmphangiomas. Ani-
orexia, fever, and xweight loss have heen
observed, particularly in late cases, hutj.auindice is rare. Tlh latter sign xvas pres-ent in l)ut one instance, the 14-year oldgirl xv-ithi a hepatoma associated with post-niecrotic cirrhosis. Cyainiosis xvas noted in a
newbhorn infanit v-lho (lie(1 at eight xveeksof atge of heart failure. At autopsy thisinfaiit wvas fotiui(n to have at (lifftlse lhemiiani-griomatosis witli involvemncit of the liver,skin, anid pancreas, a syndrome previouslydescrihed 1v Winters, Iobminson tand Bates,in 1954, and Levick and Rliuie, in 195:3.. 17
Radiologic evaluation of all. ahdominalmiaulsses is mcanlatorv and is milost tisefuil in
distingcuishinlg hepatic ttiuimors froim emii-
brvomas of the kidncv and(I neurobl astomas.Tlhe plain filmil of the ahdomen and theintravenous pvelogramn are grenerally per-
formiied as emergrenev procedures in 'a Child
with a solid intra-ahdominal ttiuimor in otirinistittitioni. The intravenous pvclogram isparticularly elpfuil. In the presencee ofliver ttiuimors, the kidneys functioni normallyhilaterallv and are usually in niorm-lcal posi-tioll, althoutgl the pelvis and calvces may
he compresse(l. Distortioni of the initra-renal configuration. as ol)scrve(l in \V ilmnis
ttiuimor, or displacement. as seen in nciuro-
hlastoma, areutn1comI1111on1. Recently thec, con1-
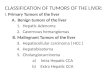
DISTRIBUTTION OF L/VER TUMORS/9 CASES
HEPATOMA (liver cell carcinoma)LYMPHANGIOMABENIGN CHOLANGIOHEPATOMAFIBROANGIOMAHEMANGIOMATOSISLOCALIZED NODULAR CIRRHOSIS
32
FIG. 2. Pathologic types of tilinioirs (en,ouIlterd and
thieir anatomic locattioni w-ithlini the liv-er.
trast material tused for intravcnous pvelor-raphv hias heens injected inito the greater
saphenous veinl to providle visualization of
the inlferior v-enail cavx a in abdominal ttuimlors.
Ohstruction of the iniferior v-enia cava, as
demiiionstraited this techlinic, haiis corre-
spondcled to involvemenit of the central por-
tion of the liver or invasion patst the milidlinlein those cases of lhepattoimias in xvhomi1 tIlisproceduresIi heen usedl. Barium stuidies
of the stro-initestinail trItact a,Ire rarel-needed sincee the air-soft tissui,e conitrastwill demiionstr cate downw-ard andinlmedial
displacemienlit of the intestinal viscera.Lahoratorv tests have heeni of little addi-
tionatl valtue in preoperative evaluation ofthese cases, a point also noted b1 others.
An1 elevated alkatline phosphatase has heen
noted occasionally, ancdl is elpftil if fotiundl.Alteration in the sertiuim electroph oretic patt-terin w-ithi elevation of the alpha-2 and(c heta(lobulins hIs recently heeni descrihed 1,
Otiaki, ct all." Liver function studies wN-erei
essenitially normli in this series except inthe chiild wN-ithl post-iiecrotic cirrlhosis and
a stiperimiipose(d nieopliasimi. Actually, ifmarkedly abnornmal liver ftiunction tests atre
ohserved, the diagnosis of primary ttiuimorof the liver is uilikely.
Rladiographic studies of the chest and
hones an(l honie marrow aspiration atre cs-
senitiail patrts of the evaluation of at chiildw-ithi a soli(d tuiimior of the abdomen. If these
V]lume 154Number 3 477

478 CLATWORTHY, BOI
do not disclose any evidence of distantmiietastases, early suirgical exploration is iii-dicated. If an isolated lesion is present andis surgically resectable, the histologic diag-nosis of a solid tumor of the abdomen isprobably best established by an excisionalbiopsy of the mass through adjacent nor-mal liver substance. Pre-excisional orneedle biopsy in the absence of distantmetastases and in the presence of an op-erable lesion is inadvisable, as viable tumorcells may be spread locally by such maneu-vers. If excision of the tumor cannot beaccomplished, a generous biopsy should beobtained.
ManagementThree modes of therapy have been uti-
lized in the management of these cases, buteffective treatment of primary hepatic neo-plasms is at present limited almost entirelyto adequate surgical resection. Such hasbeen attempted and completed in all of ourlong-term survivors. Radiotherapy may beof value in hemangiomas and has beenundertaken in three cases of inoperablehepatic cell malignancies.t Radiotherapy,has appeared to result in dramatic shrink-age of the tumor when used in high dos-ages, usually totaling 6,000 to 6,500 pertumor given as rapidly as can be toleratedby the patient. No hepatic cell tumors orpulmonary metastases have been eradicatedby irradiation, although some palliation hasbeen obtained. In two instances secondlook surgical procedures have been at-tempted following irradiation. In neitherinstance were the previously nonresectabletumors made resectable by this adjunctivetherapy. Phillips and Murikami recentlyhave reported beneficial but no curativeeffects with radiation in the treatment ofprimary liver neoplasms.12
After Curreri, et al., reported some suc-
AND KOTTMEIER Annals of SurgerySeptember 1961
cess with hepatomas in adults using 5-Hii irotracil, a single five-rnontlh-old infantNvith an inoperable, radiation-resistant he-patoblastoma was treated with two couirsesof this drug (15 mg./kg. intravenously perday for 10 days per course. Total dose,1,300 mg.) * withouit any definite shrinkageof the abdominal mass, although calcifica-tion did appear within it.3 In three addi-tional cases, actinomycin D in therapeuticdoses has been used in conjunction withradiotherapy without avail. Liver perfusionhas not been used in our treatment pro-gram. At the present time we are unawareof anv chemotherapeutic agents whichhave been shown to definitely affect he-patomas in childhood.
Technic of Surgical ExtirpationThe major obstacles to the successful re-
section of liver tumor remain essentiallythose outlined by Wangensteen, in 1951:excessive blood loss; air embolism, and bileperitonitis.15 Liver insufficiency has notpresented a serious problem in reportedcases or in our experience. Three typesof surgical procedures are currently em-ployed.
1. Wedge Resection. The wedge resec-tion of small or pedunculated lesions hasbeen successfully accomplished by utiliz-ing through and through sutures. Whensnugly tied these control leakage of bloodand bile and permit relatively easy closureand reperitonealization. None of the tumorsin the patients reviewed here were of atype to permit the use of this technic.
2. Left Lobectomy. Left lobectomy ofthe liver has been successfully accom-plished in a fashion similar to that de-scribed for wedge resection and withoutdissection of the hilar structures (Fig. 3).The left lobe is first mobilized by dividingthe left triangular ligament, and overlap-
* Under the direction of Dr. Stella Kontras,Assistant Professor of Pediatrics, Ohio State Uni-versity College of 'Medicine and the ColumbusChildren's Hospital.
f Under the direction of Dr. Thomas C. Pom-eroy, Chief of the Therapeutic and RadiologicDivision of the Department of Radiology, OhioState University.
LES

Volume 154 LIVER TUMORS IN INFANCY AND CHILDHOODNumber 3
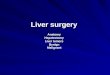
FIG.3.Resectionof~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~.....
left lobe of liver. Over-lapping mattress sutures_- ^placed after mobilization::
P~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~ ...!.} :.:
.. .. .. ..:
of lobDe. A. Hemotasis : : ::controlled after lobectomy .:by mattress sutures. B. =-
sponge used to cover the :, : ;"X ::iarea of excision. :a2
ping mattress sutures are then placed alongthe junction of the right and left lobes. Thistechnic has been used in three instanceswithout troublesome operative problems.Both this procedure and wedge resectionare relatively simple to perform, and whenthe line of excision is carried through nor-
mal liver substance, effectively rid the pa-
tient of a primary lesion. However, theresults following such procedures withhepatic cell malignancies have not beenencouraging because of the early develop-ment of contralateral or pulmonary metas-tases.
3. Right Lobectomy. Surgical extirpa-tion of the entire right lobe of the liver hasbeen successfully accomplished for bothbenign and malignant tumor masses bymany surgeons since the original report byWangensteen, in 1951.15 Such procedures,when performed for primary disease in theright lobe, offer the best opportunity forlong-term survival and should be part ofthe armamentarium of all surgeons whoundertake the care of these patients today.
Lesser procedures, such as enucleation or
local excision, not only are less desirablefrom the standpoint of adequate cancer
surgery but are also particularly hazardousin that the control of blood loss may beexceedingly difficult.Our present technic for total right he-
patectomy, evolved over a period of nineyears since our first successful case is as
follows: Hypothermia (32.2°-33.3° C.) isinstituted after the induction of generalanesthesia. A cut-down intravenous can-
nula is placed in an antecubital vein. Ex-posure is best obtained by an initial long,right rectus-retracting incision to determineoperability (Fig. 4). Extension of this in-cision into the seventh or eighth interspaceand through the diaphragm to the inferiorvena cava provides excellent exposure ifresection is feasible. Tapes are placedaround the inferior vena cava below theright atrium and above the renal veins tocontrol the venous drainage (Fig. 5).
Air embolization (a fatal complicationin one instance) has not occurred when
479* . g .: -j - .................. _ | M-wei ............ : .: ::: :: ............ St* :::.: .j Z .:: _ S.i "2 i : j : .: : ). .: .. : . .. ': .............. :: :: . ^S;d'::m}: ...... : :. '.: : ::: :: : : : |. : ::. :::: ::: .:: ....... :.: :::': ........... aXy.§ ... ^r : . :.: .. A ........... :g.:. :: :_ ... :: : :R_ ........... -; i'.'2!M : . :.:>io _W. L*.:: :o::: : ...... ::: : ::._ ... r: ::S.: ':} . ..... : : . . ........ X*: .. z . : w s [". .: ................... \ .^:: :. :: :: ^ ::; . .............................................
.. r :. i__ ....* _ . .. .. _ .... . - . i:Q
X X_1>:! :: :. 3* $:: . :. .. i _:' ...... : .: : .{ q J}s \ tE : X . L.. .. \ : .. j: _ : \_ ............ s s . . . 9 Z* :: .:. \ ... : : .i. (: a . :. w.... . . ne : r v . : . . v.. : .: YK . :.i _::: J ................................. .. S* E i, _B_ .................. 1 . .. .. .. . ............. ...... .a. .... a_ .......... ] . ..... . . ... ::"b:: :." We X .sr* ...... .. .. . . w . i _ .............. e _E^. Z . no.. . . .. .. .. w; s _ ..... z v w!0 gy . i...... : : :.: . :: .. . .. :: . s .-f: 9:9 7* ... ...... .. :. .. Mb.,;,. w ... o+f* : ,. ^::' .. : S ........ : lob _:.
.. ....

480 CLATWORTHY, BOLES AND KOTTMIEIER
!1
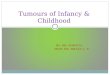
FIG. 4. Exploration of tumors of the right lobethrough a laparotomy incision. If resection pos-sible, further exposure is obtained by extension ofthe incision into the right side of the thorax.
the chest has been opened prior to thedissection of the hepatic veins. After di-vision of the right triangular ligament andmobilization of the right lobe of the liver,the hepatic artery, portal vein, and bileducts are dissected and identified. Ligationand division of the branches of these struc-tures entering the right lobe are then ac-
complished. Temporary occlusion beforedivision of the right hepatic artery andright portal vein will clearly indicate bydemarcation that the blood supply to theleft lobe remains intact. If the gallbladderis not involved in the tumor, it is removedfrom its bed and temporarily retained. Thesix to ten short and sometimes extremely,fragile right hepatic veins can then be ap-
proached directly inferiorly and laterally.Dealing with the highest hepatic vein has
Annals of SurgerySeptember 1961
been the most difficult step in this proce-dure particularly in the presence of a largetense tumor. A vena caval tear with result-ing air embolism or hemorrhage led to twosurgical fatalities early in this series. How-ever, this complication can be avoided bytightening the previously placed inferiorvena caval tapes and, if the veins are tooshort to ligate, transecting them at thecaval level and oversewing the orificesrapidly with a whip-stitch of 5-0 arterialsilk.
After this mobilization and dissectionhas been accomplished, the right lobe isready for removal. The remaining hepato-denal ligament is cross-clamped for 12 to20 minutes with a Potts-Smith-Riker coarc-tation or ductus clamp and the lobe andtumor is cut away by a combination ofblunt and sharp dissection. Major vesselsand biliary radicles are grasped with hemo-stats as they are encountered and individ-ually ligated with 5-0 black silk until theface of the remaining left lobe is bloodless.Biliary stasis may be achieved by the retro-grade injection (via the remaining stump ofgallbladder) with methylene blue stainedsaline solution. Each patent duct is thusclearly demonstrated, clamped and ligated.
Resurfacing of the denuded left lobe hasbeen variously accomplished in the past,but at present we prefer to use compressedIvalon, cut to fit, and sutured in place witha running 4-0 chromic catgut suture to theliver capsule, as recommended by experi-mental work of Jones, et al. The lobe isthen covered partially with the falciformligament, perirenal fascia, and omentum orembedded with additional sutures againstthe right diaphragm. No serious biliaryleaks have occurred using this technic. Adrain is led into the right subdiaphragmaticspace and an appropriate chest tube isplaced.
Results
All of the long-term survivors in thisseries of 19 patients had an adequate sur-

V'olunme 154Number 3
LIVER TUMORS IN INFANCY AND CHILDHOOD
FIG. 5. Right lobec-tomy. A. Control of bloodsupply by tapes aroundthe inferior vena cavaabove and below theliver and by temporarycross clamping the hepa-toduodenal structures.Retrograde injection ofthe gallbladder disclosesopen bile ducts on rawliver face. B. Resurfacingof liver face by Ivalonsponge reinforced withfalciform ligament andperirenal fascia (above)or with diaphragm (be-low).
AI
gical excision of the tumor, either by rightor left lobectomy. Right lobectomy was
performed in seven patients, and three are
living and well two and one-half, three andeight years postoperatively. Of the threecases in whom left lobectomy was per-
formed, two are living with no evidence ofrecurrent tumor two and one-half and threeyears following operation. All five of thesurvivors had benign lesions and are pre-
sumably cured. Of the three with tumorsin the right lobe, one was a benign chol-angiohepatoma and two were giant lymph-angiomas. The lesions of the left lobe inthe remaining two survivors were a fibro-angioma and a localized nodular cirrhosis,respectively. None of these long-term sur-
vivors after resection of either the right or
left lobe show any evidence of liver im-pairment. A plateau in growth was ob-served for a few weeks after operation inthese children, but subsequent growth anddevelopment in all have been entirelynormal.Among the 14 patienits who htave Inot
survived, two had biopsies only performeedand both died within three months. In boththe diagnosis was an embryonal type of
hepatoma. Both were inoperable, one beingcentrally located and the other located inthe left lobe but with metastases to theright lobe. In five additional cases of he-
patoblastoma biopsy was performed in in-operable situations (three in the centralzone of the liver and two in the right lobewith direct extension past the midline).Radiation therapy alone was given to twoof these, and chemotherapy plus radiationin three. Although the tumor shrank in sizein three instances, none of these patientslived over nine months following comple-tion of treatment. Chemotherapy-eitherwith 5-flurouracil or actinomycin D-ap-peared to be of little benefit. In two addi-tional patients no treatment was given andthe diagnosis was established at postmor-tem examination. One of these had a cen-
trally placed hepatoma of the adult typesuperimposed on post-necrotic cirrhosis.The other was an infant with diffuse hem-angiomas of the liver, pancreas, and skinwho died at eight weeks of age with heartfailure and eyatnosis. The latter patient istlhe only instaniee of death due to a beinignprocess.
The remaining five patients who expired
481

482 CLATWORTHY, BO]
all had surgical excision performed forhepatoblastomas. Of the four with rightlobectomy, one expired of operative hem-orrhage and another of hemorrhage andair embolism. A third and most unfortunateinfant expired of staphylococcal septicemiatwo weeks postoperatively, and no evidenceof residual tumor was found at autopsy.The fourth died at home two and one-halfmonths following a right lobectomy withsymptoms suggestive of recurrent tumor,but no autopsy was performed. In the fifthpatient a left lobectomy was followed bydeath seven months later from massive re-current tumor in the right lobe. This latterpatient was 18 months of age at the timeof the resection and had been known tohave an abdominal mass since the age ofthree months.
DiscussionPrimary tumors of the liver are of suffi-
cient frequency to merit consideration inthe diagnosis of abdominal masses in in-fants and young children. Prompt diagnosisand aggressive surgical treatment are es-sential in the management of these pa-tients, since the prognosis without treat-ment in the malignant and benign tumorsas well is extremely poor. Our experienceand that reported by Andersen, Gross, Leeand Newstedt, and Shorter, et al., attest tothe dismal fate of patients in whom eitherno treatment is given or nonsurgical meth-ods are used." 2, 6, 8, 13Adequate technics are available for re-
section of either the right or left lobes.These technics are based on anatomicprinciples and permit lobectomies withoutundue hazard from blood loss, air em-bolism or bile peritonitis. Remaining livertissue is entirely adequate in either casefor normal liver function. Determination ofresectability is determined by laparotomy.All tumors confined to one lobe and with-out evidence of distant metastases shouldbe considered operable. Resection of tu-mors in the left lobe by left lobectomy is
LES, AND KOTTMEIER Annals of SurgerySeptember 1961
a well standardized procedure. With le-sions of the right lobe, adequate exposureis obtained by extending the incision intothe right chest. Control of the inferior venacava above and below the liver, and liga-tion of the vessels and ducts to the rightlobe in the porta hepatis are importantsteps in assuring adequate hemostasis.Temporary occlusion of the structures inthe hepatoduodenal ligament during divi-sion of the liver adds security to the con-trol of blood loss. Hypothermia during theprocedure has been an additional helpfuladjunct in recent cases. Following resectionand meticulous hemostasis, resurfacing ofthe liver face and adequate drainage areessential details to prevent collections ofbile.With the use of such resections the
prognosis of benign tumors, even of mas-sive size, is uniformly excellent. The out-look for the young patients with hepatomais still not good, but an increasing numberof successes are being reported."'14 Thecollected experience of surgeons interestedin this problem further justify this opti-mism. Among 20 patients with malignanttumors in whom an adequate surgical re-moval was successfully accomplished, fiveare living without evidence of recurrencethree or more years following resection, andan additional three are similarly well forless than a three year follow up (Table 1).The results are sufficiently encouraging towarrant vigorous application of the pres-ently available surgical technics to suchpatients.
SummaryPrimary tumors of infants and children
are most common in the first two years oflife. Most are malignant parenchymal neo-plasms of embryonal derivation, but benigntumors divided from the supporting cellsare also encountered and may be massive.Teratomas and tumor-like masses of inflam-matory origin are rare.Adequate resection of these lesions by

Volume 154 LIVER TUMORS IN INFANCY AND CHILDHOOD 483Number 3
either right or left lobectomy may be ac-complished with reasonable safety aInIdIwithout serious hemorrhage, air embolism,bile peritonitis, or liver failure.
Results with 19 cases in ouir experienceand 75 collected from other centers indicatethat the prognosis with benign lesions man-aged by such resections is excellent. Inaddition the outlook for the malignant tu-mors so treated is sufficiently good to indi-cate that an aggressive surgical approachis the best hope of cure in these patients.
AcknowledgmentThe authors gratefully acknowledge the inval-
uable assistance of Mrs. Brenda Sutherland, MissDolores Britt, and the Department of Photography,Ohio State University, in the preparation of thismanuscript.
References1. Andersen, D. H.: Tumors of Infancy and
Childhood. Cancer, 4:890, 1951.2. Clatworthy, H. W., Jr., E. T. Boles, Jr. and
W. A. Newton: Primary Tumors of the Liverin Infants and Children. Arch. Dis. of Child.,35:22, 1960.
3. Curreri, A. R., F. J. Ansfield, F. A. McIver,H. A. Waisman and C. Heidelberger: Clin-ical Studies with 5-Flurouracil. Cancer Res.,18:478, 1958.
4. Dargeon, H. W. (Chairman), P. A. Steiner,R. E. Herendeen, P. C. Bucy, J. H. Dale,Jr., H. L. Temple and S. N. Rowe: RoundTable Discussion on Tumors, Benign andMalignant. American Academy of Pediatrics.Published in J. of Pediat., 30:716, 1947.
5. Edmondson, H. A.: Differential Diagnosis ofTumors and Tumor-Like Lesions of Liver inInfancy and Childhood. A. 'M. A. J. Dis.of Child., 91:168, 1956.
6. Gross, R. E.: The Surgery of Infancy andClildhiood. Pliladelphia, W. B. SauindersCo., p. 532, 1953.
7. Jones, T. W., L. M. Nyhus and H. N. Harkins:Formalinized Polyvinyl Alcohol (Ivalon)Sponge in Repair of Liver Wouinds. A. M. A.Arch. of Surg., 76:583, 1958.
8. Lee, C. M., Jr., J. R. Newstedt and H. S.Siddall: Large Abdominal Tumors of Child-hood (Other than Wilms Tumors or Neuro-blastoma). Ann. Surg., 143:803, 1956.
9. Levick, C. B. and J. Rubie: Haemangioendo-thelioma of the Liver Simulating CongenitalHeart Disease in an Infant. Arch. Dis. ofChild., 28:49, 1953.
10. Otaki, A., A. E. Read, J. Stubbs and H. Schul-thorpe: Right Hemihepatectomy for PrimaryHepatoma. The British Med. J., p. 256, July23, 1960.
11. Peterson, R. D. A., R. L. Varco and R. A.Good: A 5-Year Survival of an Infant AfterSurgical Excision of an Embryonal He-patoma. Pediat., 27:474, 1961.
12. Phillips, R. and Koichi Murikami: PrimaryNeoplasms of the Liver. Cancer, 13:714,1960.
13. Shorter, R. G., A. H. Baggenstoss, G. B. Loganand G. A. Hallenbeck: Primary Carcinomaof the Liver in Infancy and Childhood (Re-port of 11 Cases and Review of the Litera-ture). Pediat., 25:191, 1960.
14. Tien-Yu Lin, Kai-Mo Chen, and Tang KueKiu: Total Right Hepatic Lobectomy forPrimary Hepatoma. Surgery, 48:1048, 1960.
15. Wangensteen, 0. H.: Cancer of the Esophagusand the Stomach. Am. Cancer Soc., Inc.,p. 92, 1951.
16. Willis, R. A.: The Borderland of Embryologyand Pathology. London, Butterworth andCompany, Ltd. 1958. Chapter II: EmbryonicTumors and Teratomas, p. 410.
17. Winters, R. W., S. J. Robinson and G. Bates:Hemangioma of the Liver with Heart Fail-ure: A Case Report. Pediat., 14:117, 1954.
DISCUSSION
DR. THOMAS C. MOORE: We have seen sixprimary tumors of the liver in infants and childrenat the Indiana University Medical Center duringthe past six years. Five of these tumors were ofthe hepatic cell carcinoma type. None of thesechildren survived.
One tumor was a huge benign cavernoushemangioma and was present at birth. The infantwas admitted to the hospital at 19 hours of age
because of progressive increase in the size of themass in the early hours after birth. At operation,a massive cavernous hemangioma of the liverwas found. It had almost completely replaced theleft lobe of the liver. A near total resection of theleft lobe of the liver was carried out. The infantrecovered and is living and doing well two andone half years after operation.
The hemangioma measured 11 X 9 X 5 cm.and weighed 278 Gm. On microscopic examina-