Embed Size (px)
Citation preview

References
1. Scottish Government (2013), Scotland's National Dementia Strategy 2013-2016. Edinburgh, Scottish Government.
2. Alzheimer Scotland (2017). Connecting People Connecting Support. Available from: http://www.alzscot.org/ahp
3. McGrath, M. and Passmore, P. (2009) Home-based memory rehabilitation programme for persons with mild dementia. Irish Journal of medical Science. 178 (Suppl 8), S330
4. Duncan, E.A.S. & Murray, J.(2012) The barriers and facilitators to routine outcome measurement by allied health professionals in practice: a systematic review. BMC Health Services Research201212:96 DOI: 10.1186/1472-6963-12-96
5. Chambers, W. and Groat, A. (2015) Home Based memory rehabilitation programme: an OT early intervention for dementia. British Journal of Occupational Therapy, 78(8 suppl), 20-21
Living well with dementia: connecting people to occupational therapy and Home Based Memory Rehabilitation
Wendy Chambers (NHS Dumfries and Galloway); Alison McKean (Alzheimer Scotland); Lynda Forrest (NHS Dumfries and Galloway); Elaine Hunter (Alzheimer Scotland);Duncan Pentland (Queen Margaret University Edinburgh)
Results
Improving access
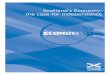
Since 2015 when NHS D&G was the only provider, occupational therapy services from another 11 areas have begun offering HBMR (Fig 1). The current test cycle aims to deliver HBMR to 72 people living with dementia (6
from each board area) before review in summer 2017.
Successfully adoption in these areas will mean HBMR is available in the regional boards responsible for providing services to approximately 94% of people who could benefit (Fig 2).
Aims and objectives Improve access across Scotland to an evidence based, occupational therapy led, post diagnostic intervention in dementia .
Aligned with the National Dementia Strategy 2013-161 and the ambitions in “Connecting People, Connecting Support” 20172, this project aims to build capacity within AHP services, ensuring timely access to therapy after diagnosis by:
Increasing partnership working, collaboration and communication Developing clear implementation pathways for Home Based Memory Rehab (HBMR) Improving the ability to evaluate and measure impact Expanding the AHP evidence base Developing an improvement model to support future expansion within AHP services
Methods Partnership working
A strategic partnership was formed between lead clinical staff in NHS Dumfries and
Galloway (NHS D&G), Alzheimer Scotland’s AHP consultant and Queen Margaret
University to underpin the project.
Occupational therapy teams from across Scotland were invited to participate and
supported to develop their own project charters, based on a National Charter template,
setting out their commitment to the partnership.
These have facilitated a planned process of testing new ways of working in these services
and have improved communication between national and local stakeholders.
Developing an implementation pathway for HBMR
HBMR is an evidenced based, early intervention in dementia. Developed by a specialist occupational therapist3, it is a 6-session programme based on principles of cognitive rehabilitation.
The team in NHS D&G developed a set of resources which structure the intervention and supports fidelity of provision. These have been provided for no-cost to participating teams, enabling an initial test cycle at each site including implementation, data collection and a review of process.
Collaboration and communication
In addition to ensuring access to the HBMR resources, active engagement by each of the
clinical teams within participating areas was recognised as fundamental to successful
adoption and implementation of the intervention. A range of spaces have been created
to develop, maintain and facilitate engagement.
Building capacity to evaluate outcomes
Effectively evaluating the impact of interventions is central to quality assurance and
future planning but can be difficult to achieve in practice4. To build capacity for
evaluation we:
Identified core outcomes and reviewed available measurement tools
Collaboratively agreed a basic uniform data set measuring; function/occupation (Lawton-Brody ADL scales), cognition (MoCA), self-reported memory problems, and quality of life (AQOL-8D), as well as key process indicators.
Developed paper-based and electronic spaces for teams to record data, with outcomes analyses and case management calculations embedded within these
Maintained an evaluation thread on the list serve for quick responses to issues encountered in daily practice
Initial progress resulting from the partnership is promising
There has been a positive response and commitment from occupational therapy services across Scotland with twelve areas involved in the national pilot of HBMR
Pilot testing indicates positive clinical and quality of life outcomes
Effective collaboration across both organisational levels and geography has been established and is supporting an increased rate of change in practice
Knowledge is being developed about how to support the fidelity and quality of HMBR as it is implemented in local areas
The testing of a planned evaluation methodology is progressing well
Ave
rage
num
ber
repo
rted
Pre-therapy 1 year post-therapy
3 months post-therapy
End of therapy
Reported memory problems
Reported use of HBMR strategies
all these things...the routines...have helped me tremendously and given me the
confidence to cope
Clinical outcomes
Initial evaluation in NHS D&G focussed on measuring the number of strategies learned and retained by HBMR recipients and the number of everyday problems they encountered because of memory difficulties5.
Review of measures over a year indicated that people were able to adopt and partially maintain the use of compensatory strategies over time (Fig 3).
Qualitative outcomes
A range of qualitative feedback methods are used when reviewing the HBMR process with people.
Data collected so far indicates that strategies and tools adopted during HBMR support people to maintain and re-engage with activities which they find important and meaningful.
I used to go out shopping and realise I didn’t have any money. Now when I go I
look at my list on the cupboard that reminds me what I need to take...my
stick...my money...my keys...my handbag
Partnership, collaboration and communication
The range of communication structures used have helped ensure all participating services can contribute to shared decisions and collaborative problem solving. To date we have held: 2 national workshops 1 webex 9 teleconferences Membership of the listserve and posts about HBMR have steadily increased (Fig 5).
Total number of group members Total number posts
Figure 5: HBMR Listserve subscription and post activity by month
Figure 1: NHS Boards
Currently piloting HBMR
Figure 2: Coverage of national >30
population in participating boards
Realising I have the skills... I can
still be responsible for myself…
makes me happy
Conclusions Next Steps
1. Review of current collaborative test cycle in summer 2017
2. Establish if positive clinical and qualitative outcomes are replicated across Scotland
3. Review and update HBMR resources including branding for NHS Scotland use
4. Progress from the current test cycle into future research work to consolidate the
evidence base and explore improvement options
5. Develop an initial model for successful sharing and implementation of other AHP
interventions for post diagnostic support in dementia
6. Consider expanding the reach of occupational therapy led HBMR across integrated and
social care providers
Figure 3: HBMR strategy use and memory problems
Not offering HBMR but discussing
inclusion in pilot phase 2