Embed Size (px)
Citation preview
© 2013 Virginia Mason Medical Center
Locoregional Therapy for Hepatoma
Robert D. Crane, MDInterventional Radiology
Virginia Mason
© 2013 Virginia Mason Medical Center
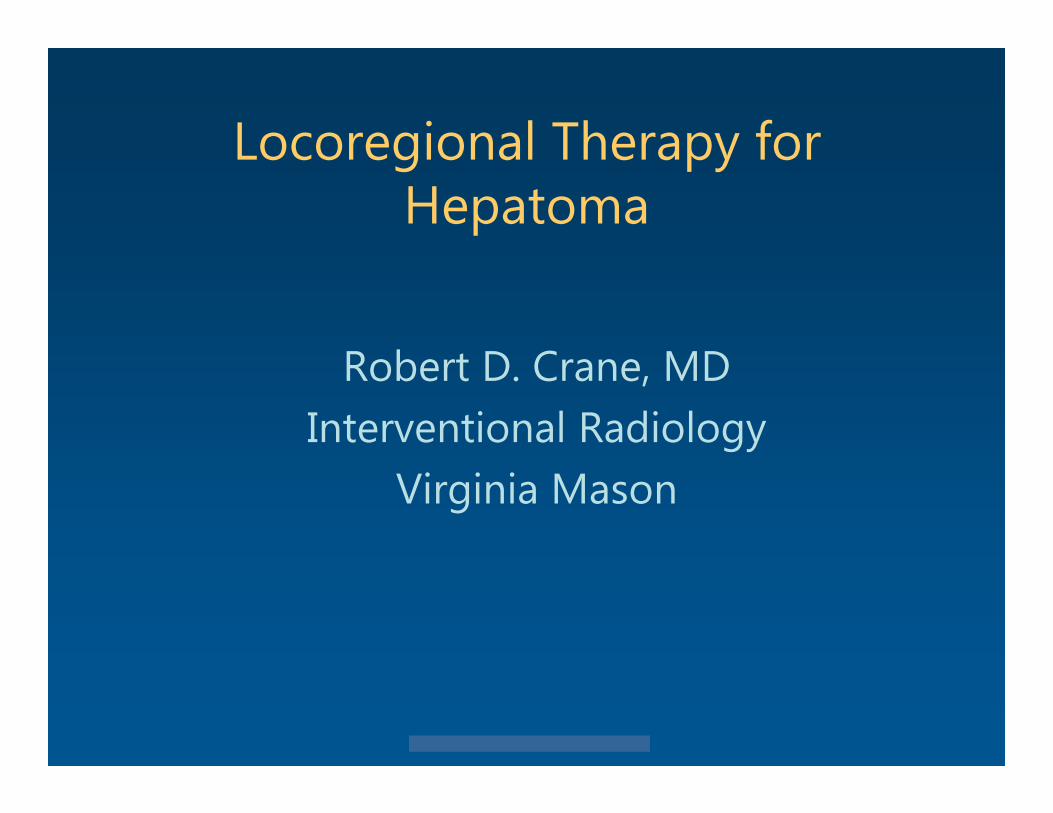
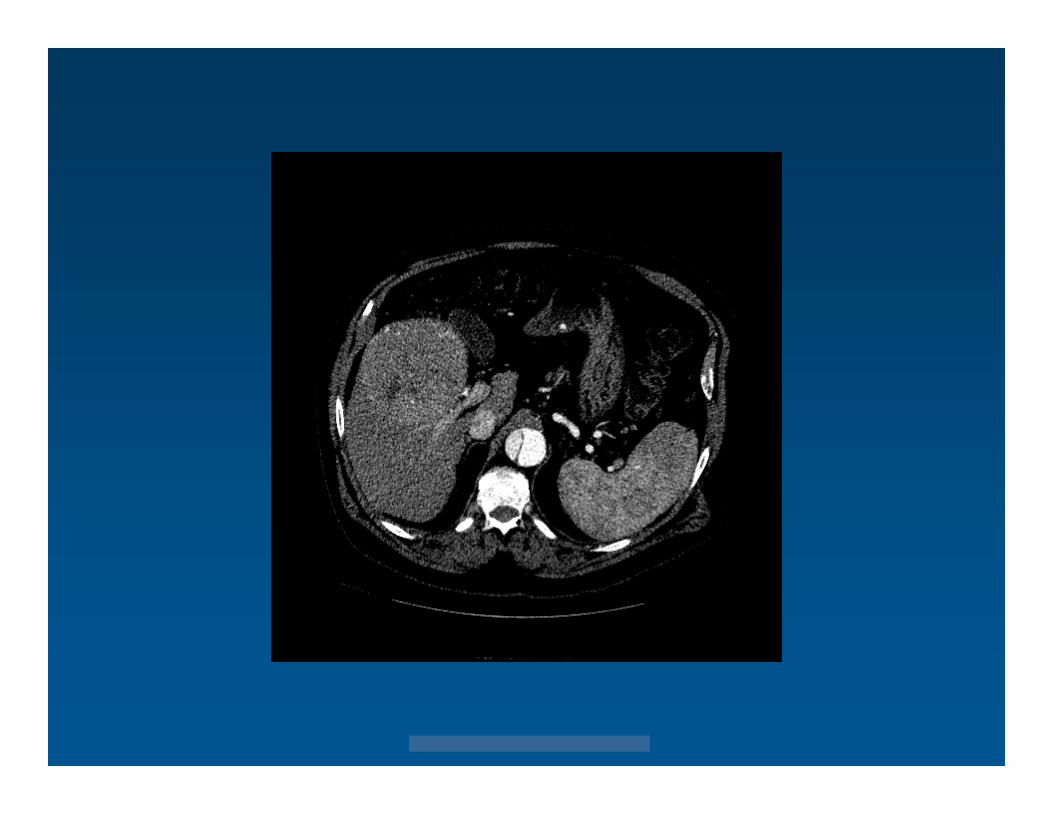
How do we know a liver mass is HCC ?
© 2013 Virginia Mason Medical Center
HCC : Bx
• Of pts getting liver transplantonly ~ 5% had Bx to establish Dx of HCC
• Risk of needle tract seeding from Bx estimated to be 2-3%
© 2013 Virginia Mason Medical Center
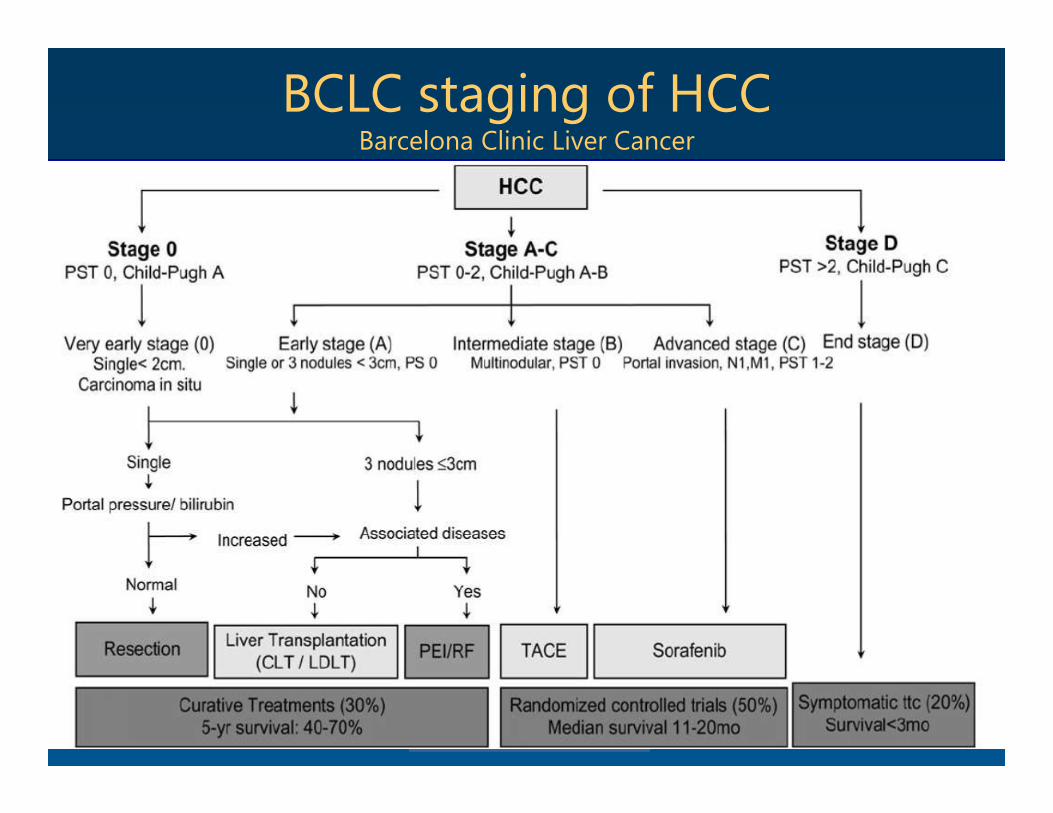
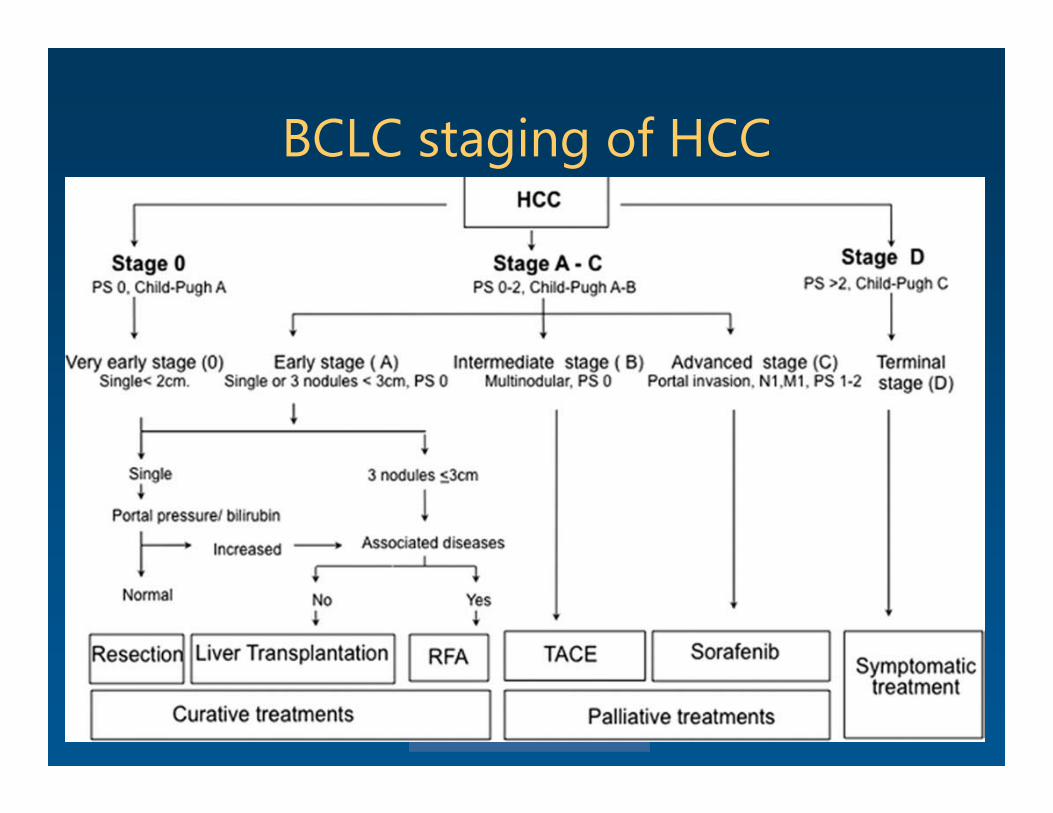
BCLC staging of HCCBarcelona Clinic Liver Cancer
© 2013 Virginia Mason Medical Center
HCC Tx : Locoregional methods• Percutaneous ethanol injection• Thermal ablation Radiofrequency Microwave
• Irreversible electroporation / IRE• Embolization Bland TACE/chemoembolization Drug eluting beads Y90 radioembolization
• External beam radiation
© 2013 Virginia Mason Medical Center
HCC Tx : Locoregional methods
• Tx Goal RFA/MWA potentially curative TACE/ Y90 palliative
• Downstaging Tx TACE , Y90, or ablation may allow pt to meet Milan
criteria for liver transplant• Bridging Tx Patients with HCC waiting for donor liver and who
have an estimated waiting time of at least 6 months.
© 2013 Virginia Mason Medical Center
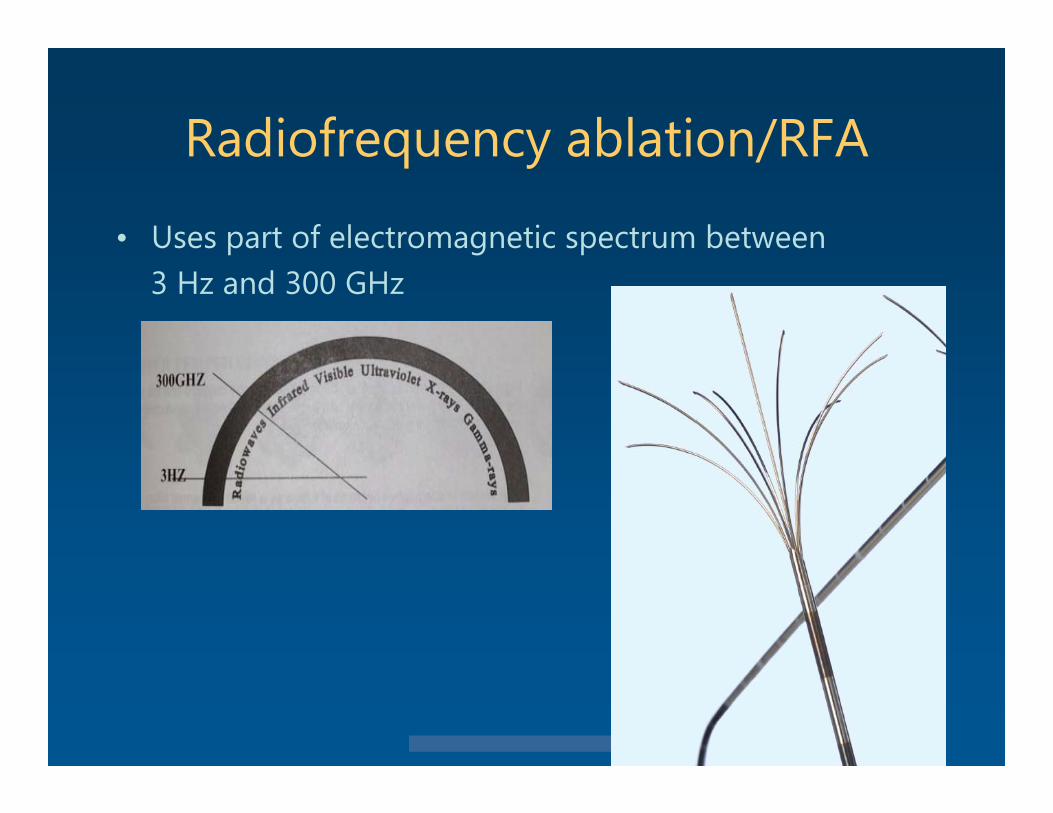
Radiofrequency ablation/RFA
• Uses part of electromagnetic spectrum between 3 Hz and 300 GHz
© 2013 Virginia Mason Medical Center
RFA
• RFA probe acts as cathode, circuit is closed by dispersing pads on the patient’s thighs
• Water molecules forced to vibrate with alternating current frictional energy loss heat
• probe itself is not the source of heat• at 55 C, get tissue death in 2 sec• at 45 C, takes 15 minutes
© 2013 Virginia Mason Medical Center
Microwave ablation/MWA• Uses higher frequency part of radiofrequency spectrum• larger ablation zone, less dependent on tissue
thermal conductivity• grounding pads not needed
• Both RFA and MWA can be done percutaneously or with laparoscope
• very little information comparing the 2 modalities in clinical practice
© 2013 Virginia Mason Medical Center
RFA / MWA
• "heat sink effect“ can limit effectiveness of thermal ablation occurs when target tissue abuts or is near a blood
vessel flowing blood acts as radiator
• carries heat away and prevents creation of lethal temperatures
© 2013 Virginia Mason Medical Center
Liver lesion ablation
• Size lesions < 3 cm, ~95-100% complete ablation lesions > 5 cm, complete ablation unlikely
can combine ablation with TACE for lesions up to 7-8 cm
For lesions smaller than 3 cm, RFA has been shown to be equivalent to surgical resection with fewer complications
© 2013 Virginia Mason Medical Center
Liver lesion ablation
• Location avoid central hilar lesions , risk of bile duct or vascular
injury want ablation margin of > 0.5 cm
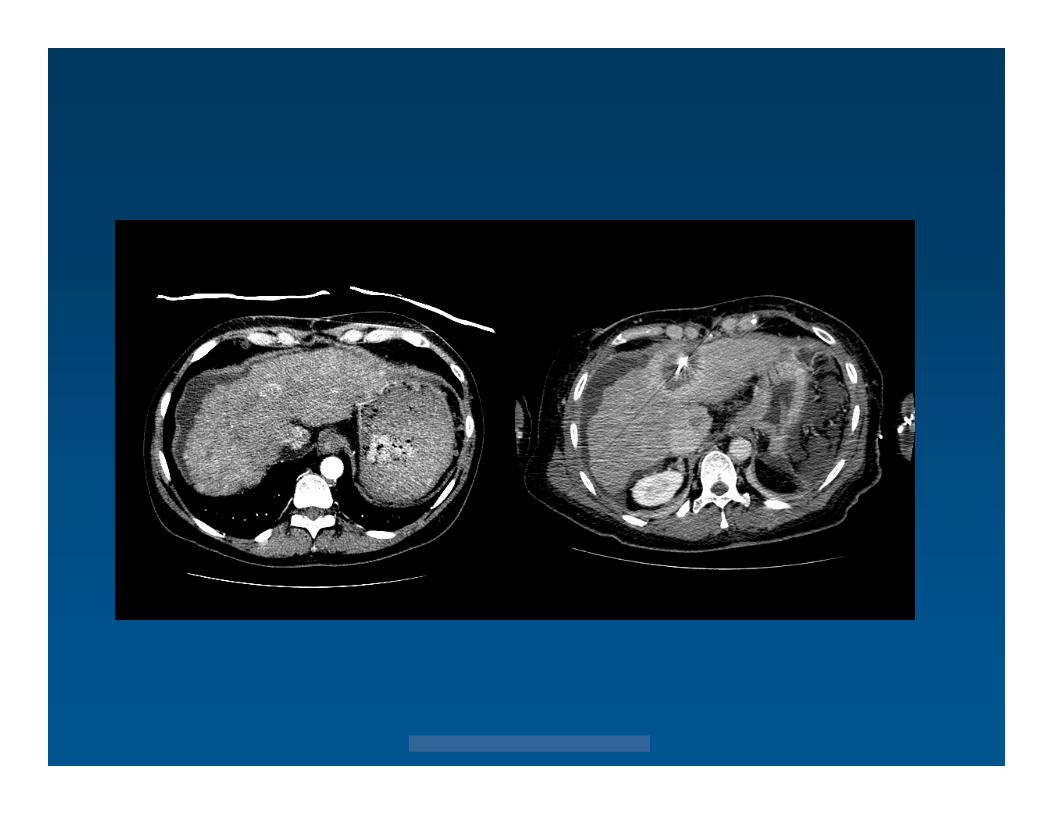
• diaphragm, heart/pericardium, gut, GB Hydrodissection
• introduction of artificial ascites
© 2013 Virginia Mason Medical Center
© 2013 Virginia Mason Medical Center
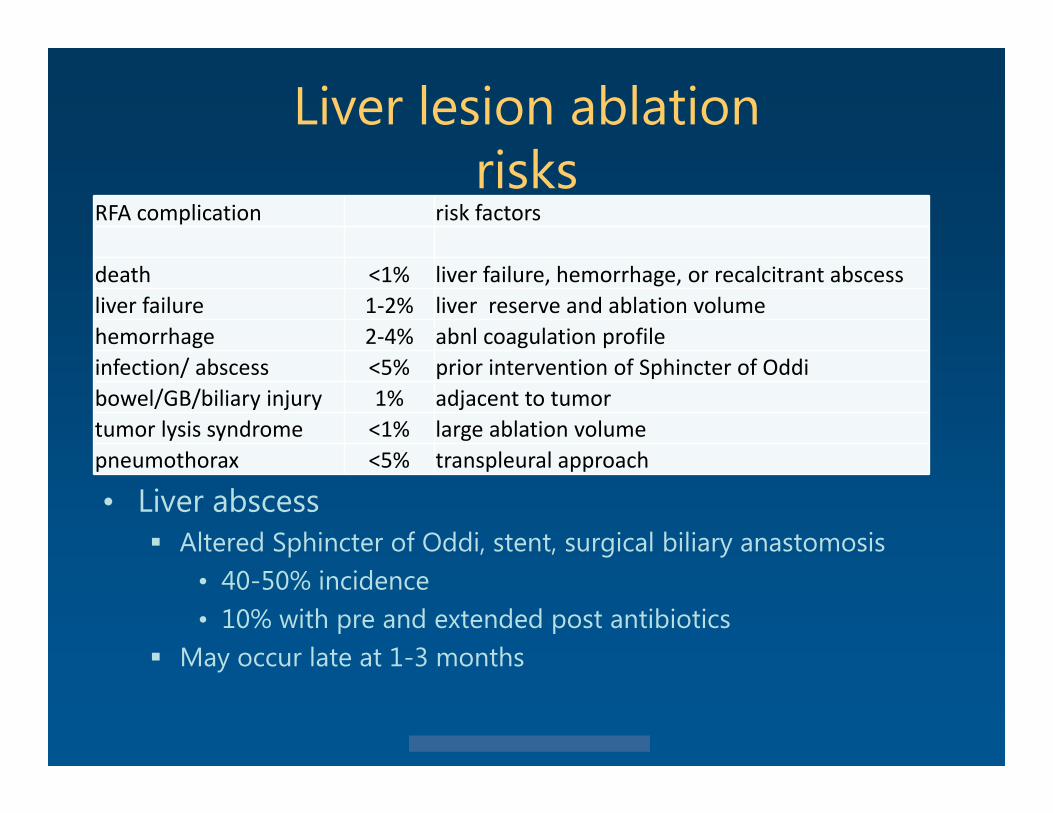
Liver lesion ablationrisks
• Liver abscess Altered Sphincter of Oddi, stent, surgical biliary anastomosis
• 40-50% incidence• 10% with pre and extended post antibiotics
May occur late at 1-3 months
RFA complication risk factors
death <1% liver failure, hemorrhage, or recalcitrant abscessliver failure 1‐2% liver reserve and ablation volumehemorrhage 2‐4% abnl coagulation profileinfection/ abscess <5% prior intervention of Sphincter of Oddibowel/GB/biliary injury 1% adjacent to tumortumor lysis syndrome <1% large ablation volumepneumothorax <5% transpleural approach
© 2013 Virginia Mason Medical Center
IRE Irreversible Electroporation
• Strong, short pulsed external electrical field is applied to tissue
• increased cell membrane permeability• cell death due to pores permanently opened• doesn't depend on temperature to kill tissue no heat sink effect
• spares connective tissues (vessels, duct ) Can Tx central lesions
• But, need 6 or more probes within 1-2 cm from each other to Tx a 4 x 4 cm lesion
• IRE not widely available
© 2013 Virginia Mason Medical Center
Embolization methods
• Bland / TAE Particles only, no chemo drug
• Chemoembolization / TACE / cTACE Drugs mixed with particles or Ethiodol
• Drug eluting beads / DEBs / DEBDOX / DEBTACE Beads with chemo, doxorubicin
• Radioembolization / TARE Y90 beads
© 2013 Virginia Mason Medical Center
Embolization
• Liver has 2 blood supplies Normal liver
• Portal vein 90 %• Hepatic artery 10 %
HCC• 90-100 % blood from hepatic artery
• Can cause selective ischemia of HCC• Can preferentially deliver higher concentration of
embolic agent to tumor, relative to adjacent liver
© 2013 Virginia Mason Medical Center
TACE / cTACE
• Multiple different methods of performing TACE• Embolic agent Particles
• 100-500 microns Gelfoam Ethiodol
• Oily contrast agent• ChemoTx drugs Single- doxorubicin, cis platinum Multiple- doxorubicin, cis platinum, mitomycin C
© 2013 Virginia Mason Medical Center
TACE / cTACEresults
• cTACE better than best supportive care• cTACE not better than bland embolization / TAE• No clear consensus on methods or procedural
techniques
© 2013 Virginia Mason Medical Center
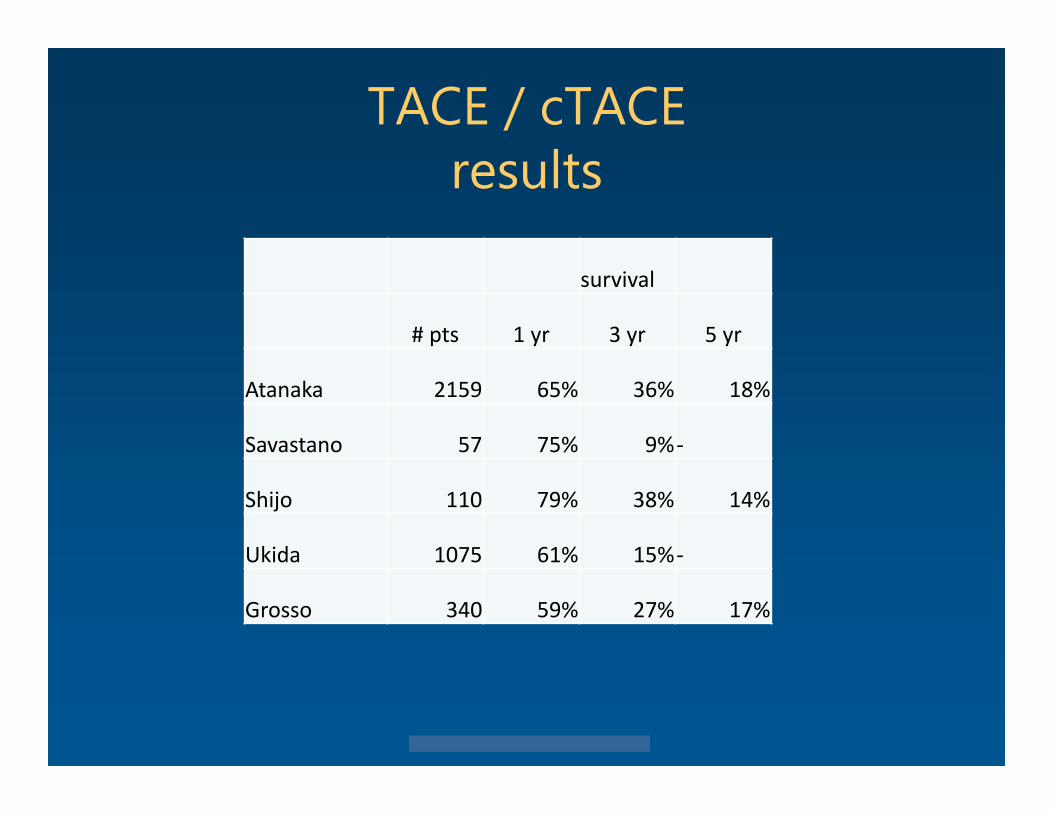
TACE / cTACEresults
survival
# pts 1 yr 3 yr 5 yr
Atanaka 2159 65% 36% 18%
Savastano 57 75% 9%‐
Shijo 110 79% 38% 14%
Ukida 1075 61% 15%‐
Grosso 340 59% 27% 17%
© 2013 Virginia Mason Medical Center
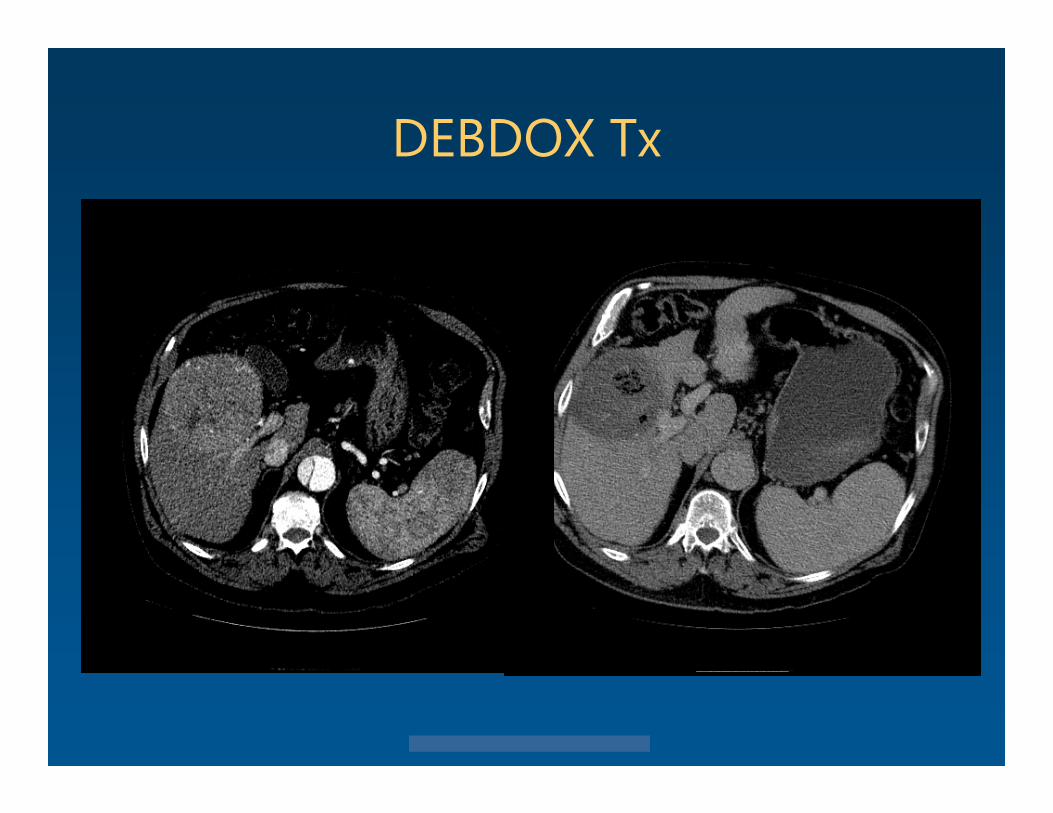
Drug eluting beads DEBs / DEBDOX
• Negatively charged polymer• Interacts with positively charged drugs such as
doxorubicin • ChemoTx released over days
T1/2 = 6 days
• Minimal systemic chemo levels
© 2013 Virginia Mason Medical Center
Drug eluting beads / DEBs
• Hydrated size 100-300 micron 300-500 micron Newly released 75-150 micron
• Superior results with 100-300 vs 300-500• Dose of doxorubicin 50-75mg / vial
© 2013 Virginia Mason Medical Center
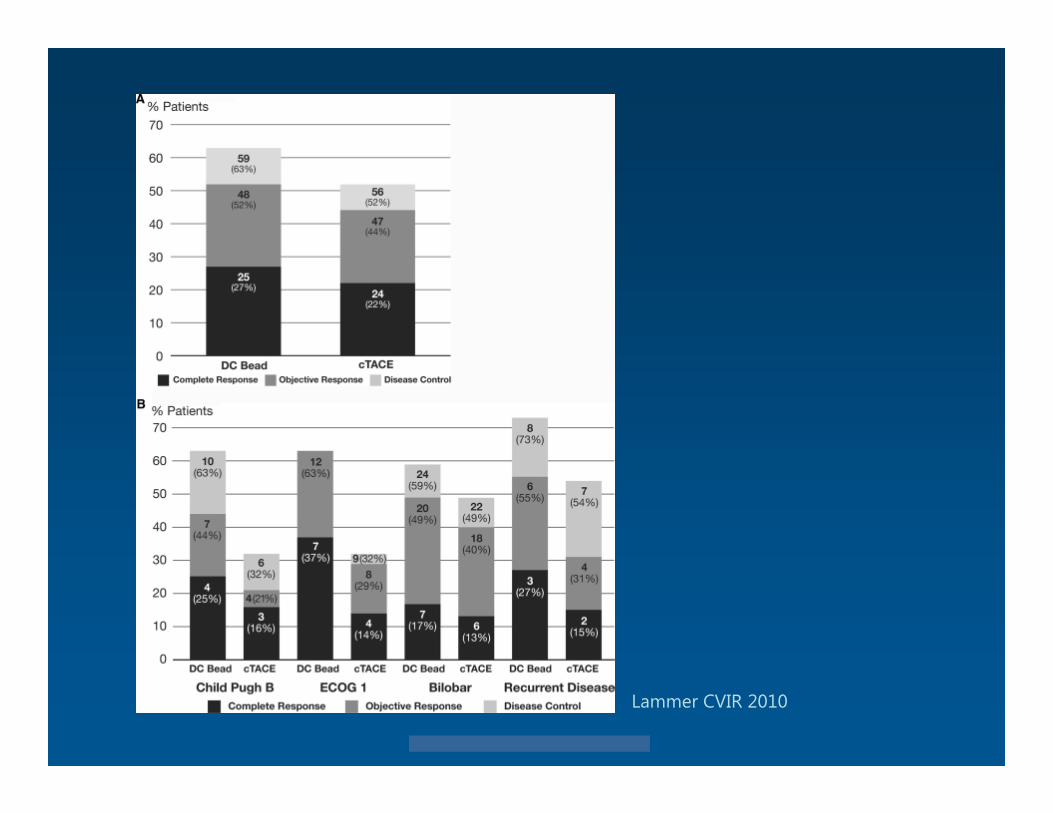
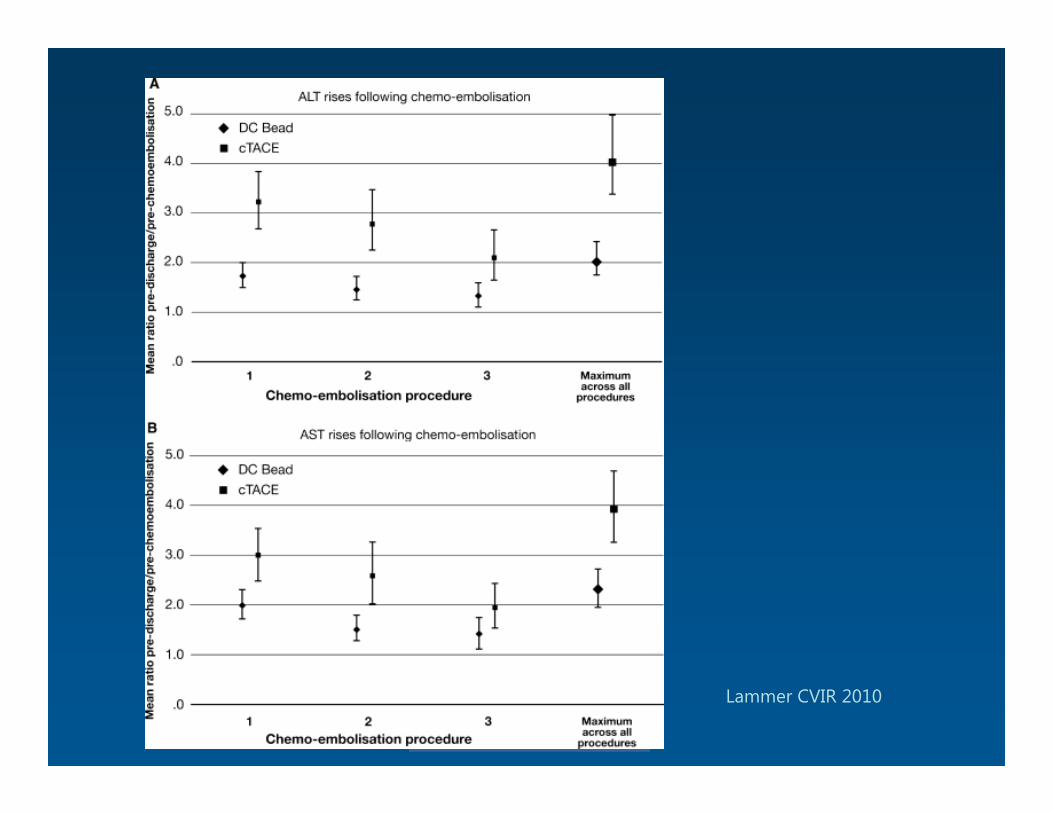
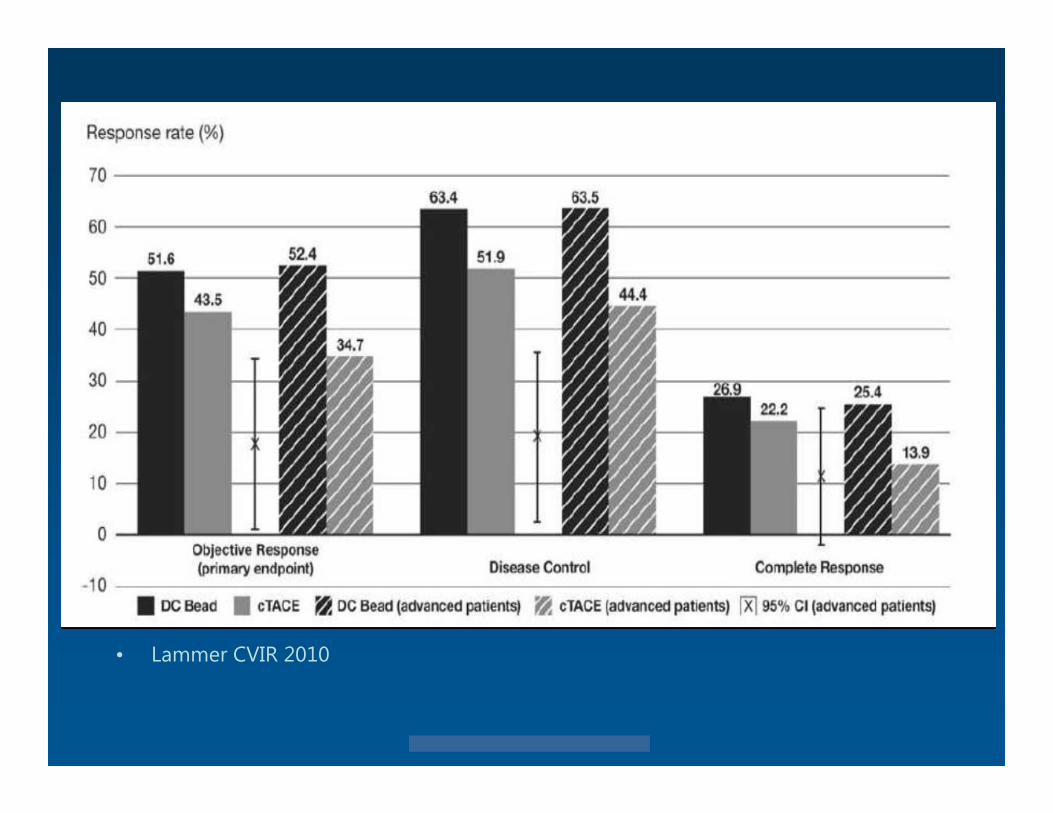
DEBDOX vs. cTACEPrecision V study
• Lammer et al CVIR 2010 • Multicenter , randomized, DEBDOX vs cTACE• 212 pts w Child-Pugh A/B cirrhosis, and large and/or
multinodular, unresectable HCC• tumor response at 6 months following blinded review of
MRI studies
79% DEBDOX vs 66% cTACE
© 2013 Virginia Mason Medical Center
© 2013 Virginia Mason Medical Center
© 2013 Virginia Mason Medical Center
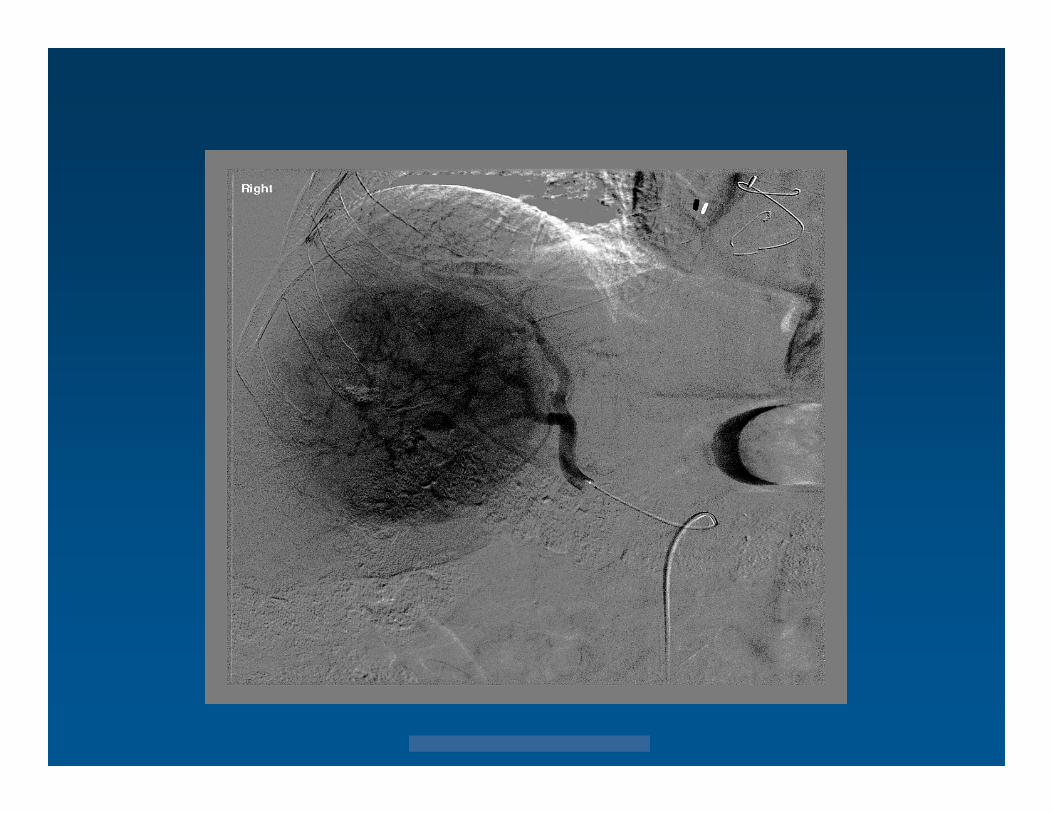
DEBDOX Tx
© 2013 Virginia Mason Medical Center
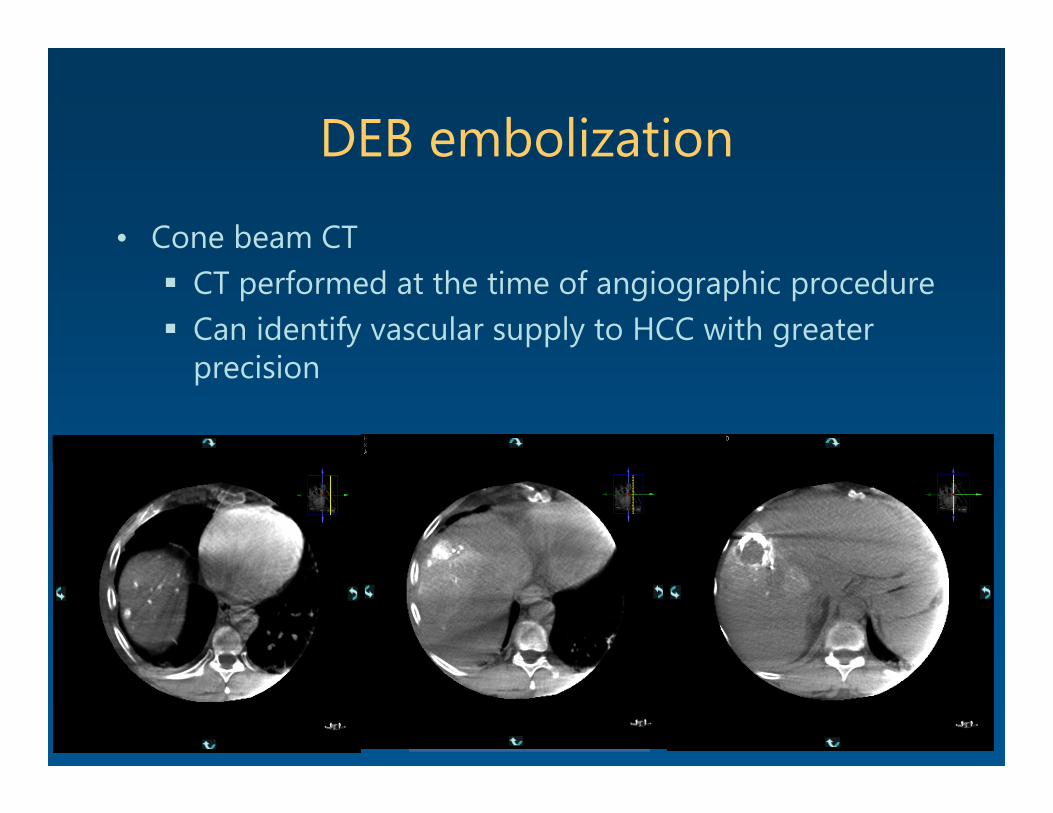
DEB embolization
• Cone beam CT CT performed at the time of angiographic procedure Can identify vascular supply to HCC with greater
precision
© 2013 Virginia Mason Medical Center
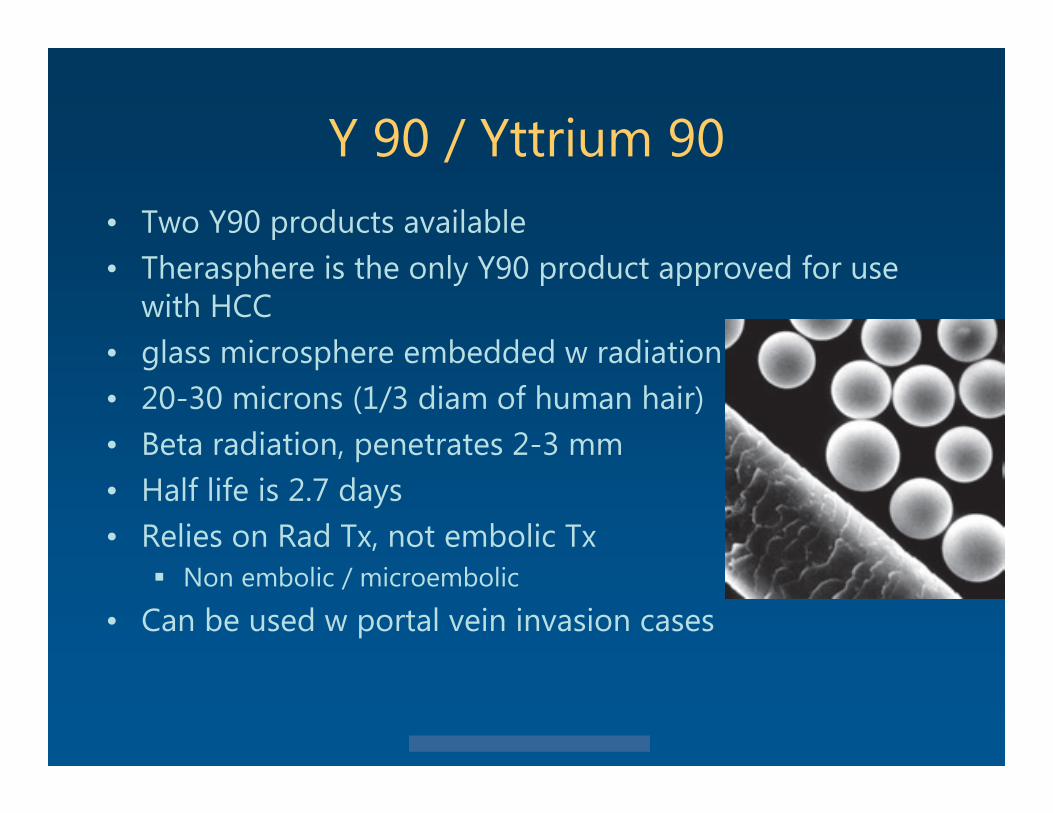
Y 90 / Yttrium 90• Two Y90 products available• Therasphere is the only Y90 product approved for use
with HCC• glass microsphere embedded w radiation• 20-30 microns (1/3 diam of human hair)• Beta radiation, penetrates 2-3 mm• Half life is 2.7 days• Relies on Rad Tx, not embolic Tx
Non embolic / microembolic
• Can be used w portal vein invasion cases
© 2013 Virginia Mason Medical Center
Y 90
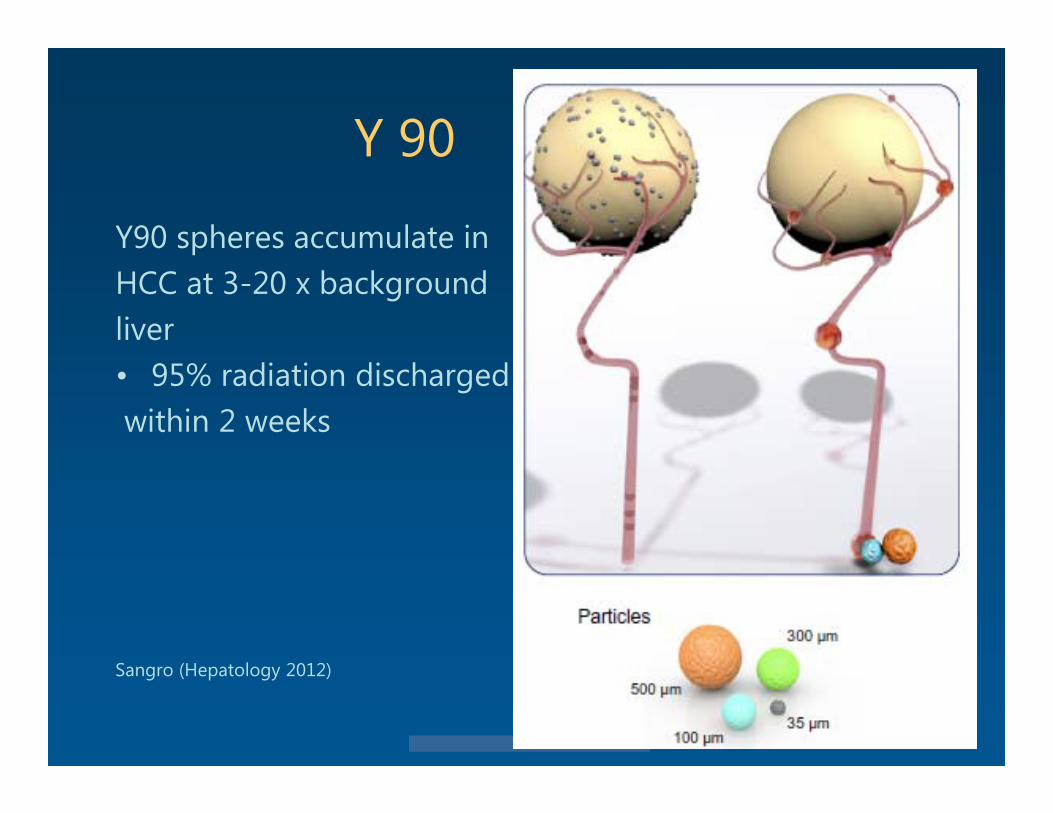
Y90 spheres accumulate inHCC at 3-20 x background liver• 95% radiation dischargedwithin 2 weeks
Sangro (Hepatology 2012)
© 2013 Virginia Mason Medical Center
Y 90 : planning & embo
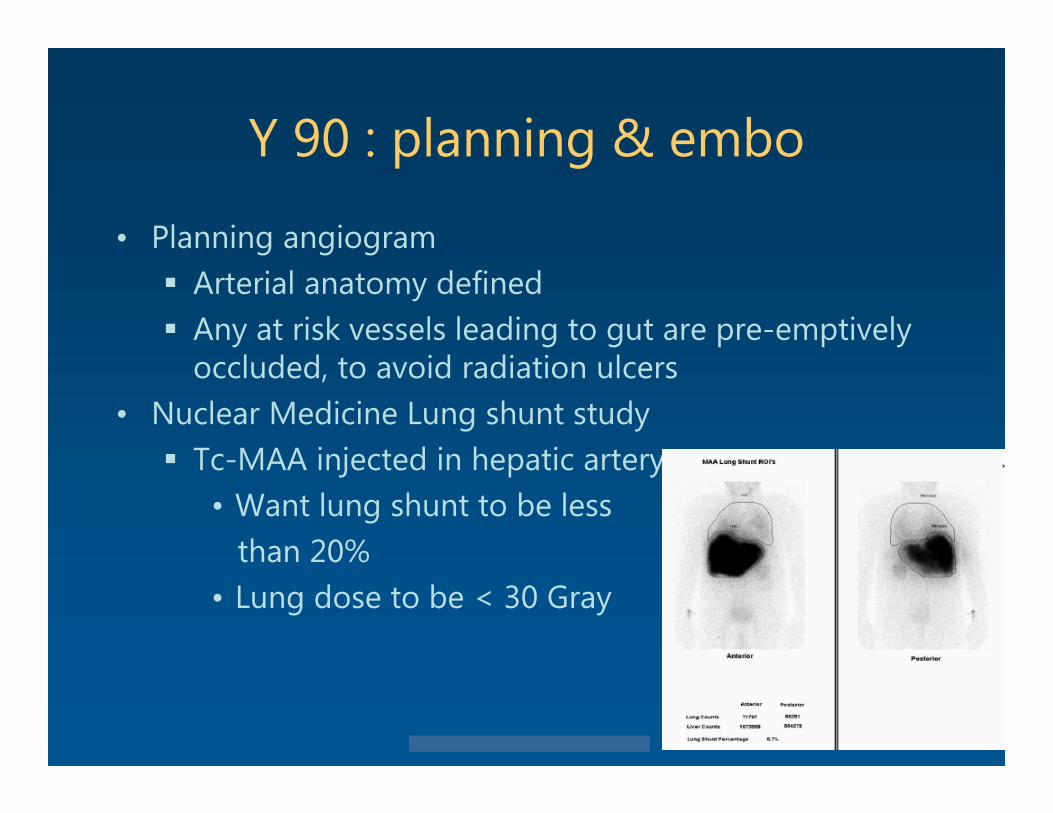
• Planning angiogram Arterial anatomy defined Any at risk vessels leading to gut are pre-emptively
occluded, to avoid radiation ulcers• Nuclear Medicine Lung shunt study Tc-MAA injected in hepatic artery
• Want lung shunt to be less than 20%
• Lung dose to be < 30 Gray
© 2013 Virginia Mason Medical Center
Y 90 : Tx
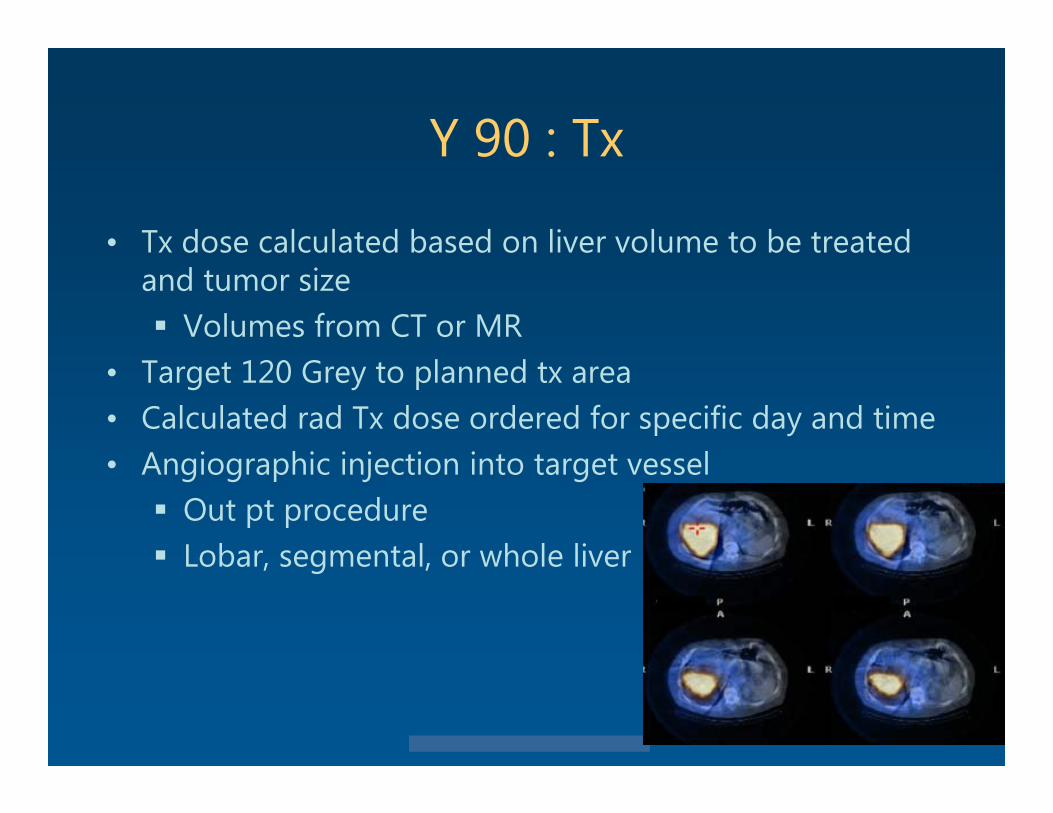
• Tx dose calculated based on liver volume to be treated and tumor size Volumes from CT or MR
• Target 120 Grey to planned tx area• Calculated rad Tx dose ordered for specific day and time• Angiographic injection into target vessel Out pt procedure Lobar, segmental, or whole liver
© 2013 Virginia Mason Medical Center
Y 90 : results
• No randomized studies with direct comparison of Y90 to cTACE or DEBs
• Retrospective single institution analysis showed similar results comparing Y 90 to cTACE
© 2013 Virginia Mason Medical Center
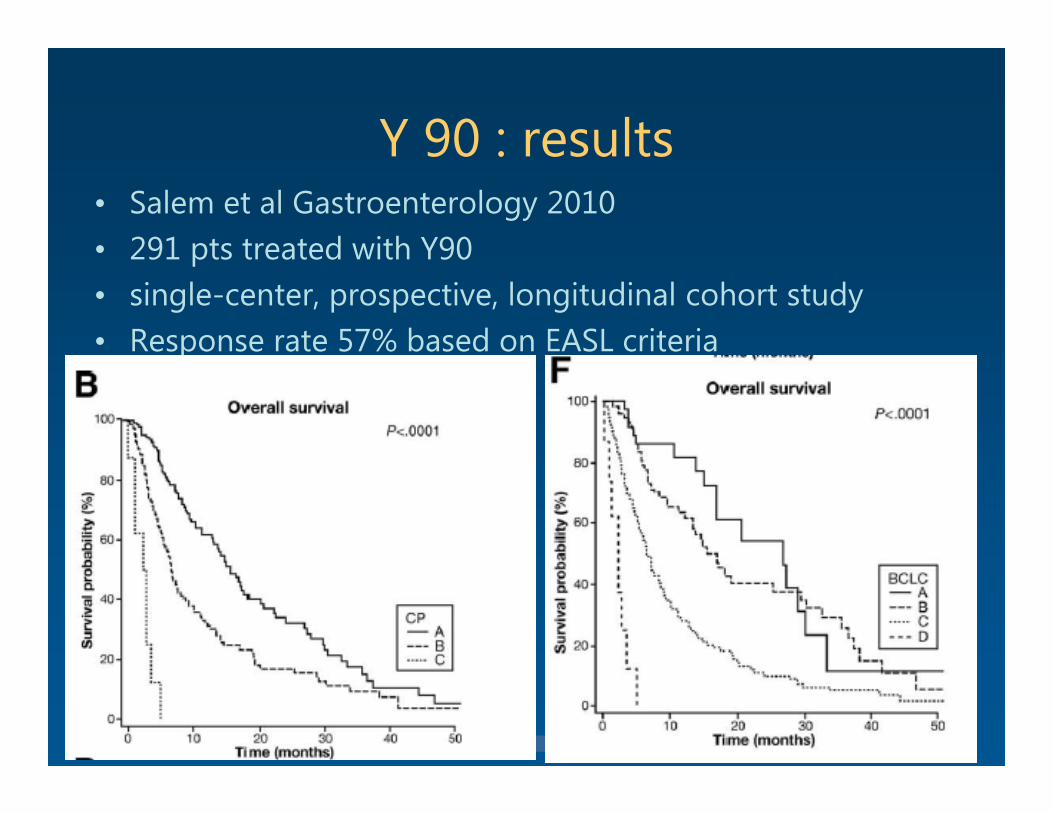
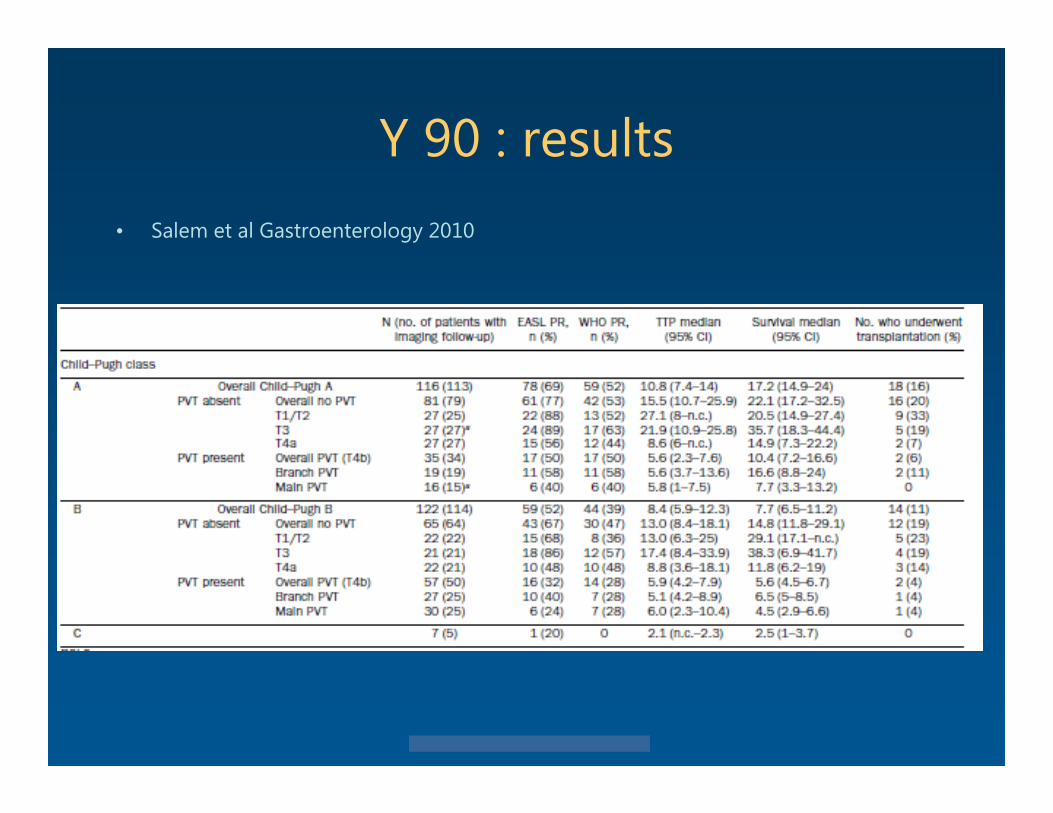
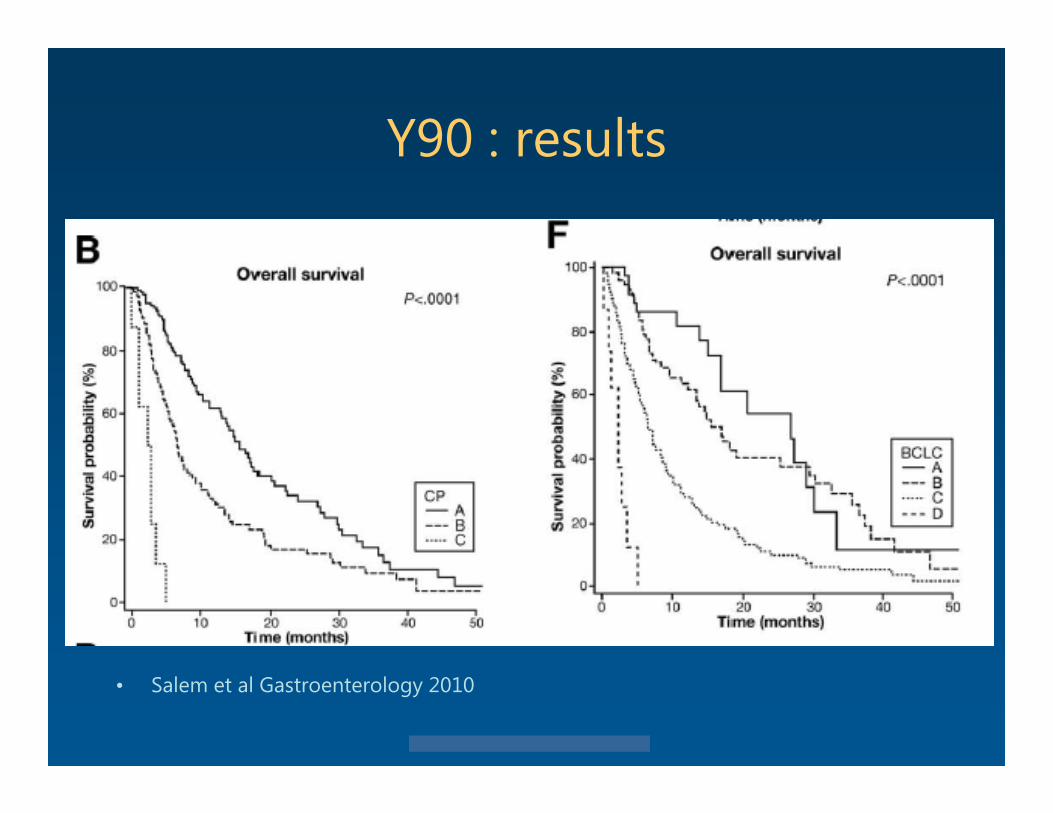
Y 90 : results• Salem et al Gastroenterology 2010• 291 pts treated with Y90 • single-center, prospective, longitudinal cohort study• Response rate 57% based on EASL criteria
© 2013 Virginia Mason Medical Center
Y 90 : results
• Sangro et al (Hepatology 2011)• Multicenter European study, RCT• 325 pts• overall survival was 12.8 mo
varied significantly by disease stage• BCLC A, 24.4 months • BCLC B, 16.9 months • BCLC C, 10.0 months
© 2013 Virginia Mason Medical Center
Y 90 : results
• Y90 Tx well tolerated by pts Outpt procedure with minimal side effects Mild fatigue for 1 week
• Improvement of HCC by CT or MR tends to be more gradual than DEB or TACE Tumor shrinkage seen after 3-6 months May have confusing appearance on imaging
prior to 3 months
© 2013 Virginia Mason Medical Center
Locoregional HCC Txsummary
• Don’t bx mass suspected to be HCC unless needed after evaluation by multidisciplinary liver tumor
board
• RFA/MWA preferred when feasible• IRE promising, but has limited role now• DEBDOX superior to cTACE and bland embolization• Y90 and DEBDOX Best embolization methods available now No direct RCT comparison studies

© 2013 Virginia Mason Medical Center
© 2013 Virginia Mason Medical Center
Y 90
• Radiation segmentectomy Subselective injection of Y 90 with intent to ablate
entire segment of liver including the target HCC
© 2013 Virginia Mason Medical Center
• Lammer CVIR 2010
© 2013 Virginia Mason Medical Center
Y 90 : results• Salem et al Gastroenterology 2010
© 2013 Virginia Mason Medical Center
-
»
» Lammer CVIR 2010
© 2013 Virginia Mason Medical Center
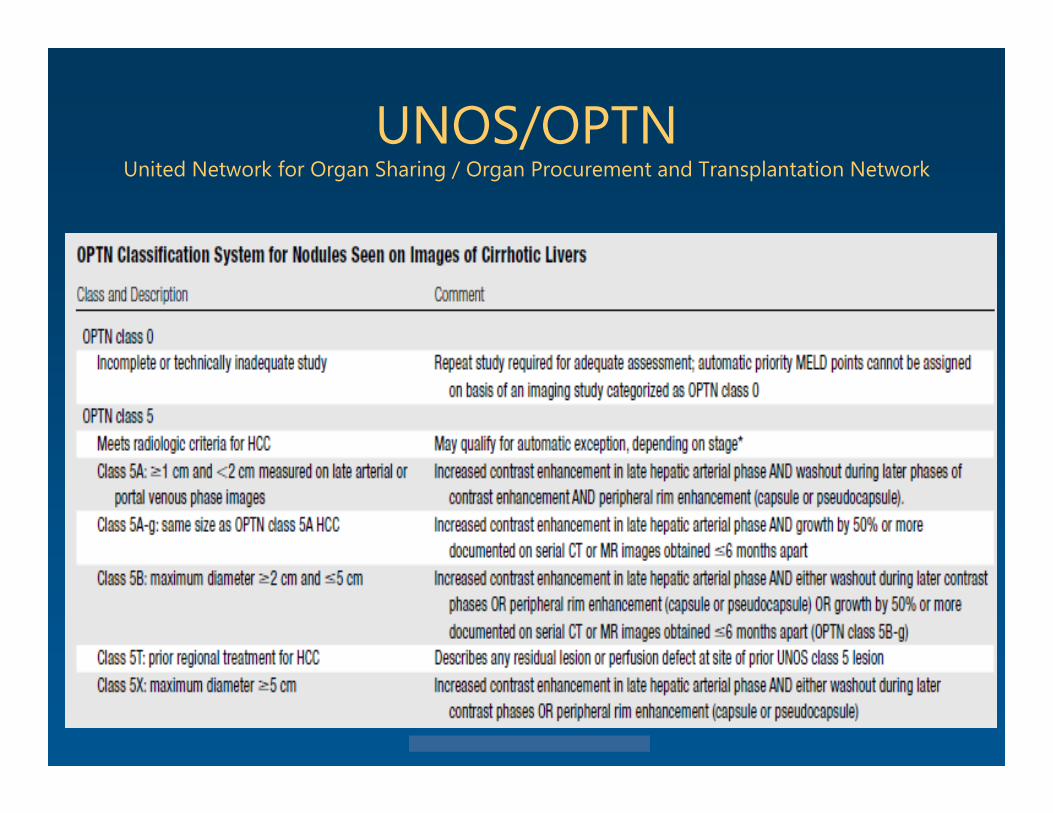
UNOS/OPTNUnited Network for Organ Sharing / Organ Procurement and Transplantation Network
© 2013 Virginia Mason Medical Center
BCLC staging of HCC
© 2013 Virginia Mason Medical Center
HCC Tx
• Surgical resection• Transplantation• Locoregional Tx• Chemotherapy• Best supportive care
© 2013 Virginia Mason Medical Center
HCC : Transplant candidateHCC size matters
• Milan criteria basis for selecting patients with cirrhosis and
hepatocellular carcinoma for liver transplantation. one lesion smaller than 5 cm up to 3 lesions smaller than 3 cm no extrahepatic manifestations no vascular invasion
• MELD score pts w HCC within Tx criteria get 22 MELD points ,
increasing q 3 months lesion needs to be 2 cm or greater to qualify
© 2013 Virginia Mason Medical Center
Y90 : results
• Salem et al Gastroenterology 2010
© 2013 Virginia Mason Medical Center
HCC
• VMMC Liver tumor boardHepatologyHPB surgeryInterventional radiologyOncologyRadiation oncology
© 2013 Virginia Mason Medical Center
• Lammer CVIR 2010