Embed Size (px)
Citation preview
British Journal of Addiction (1991) 86, 1111-1117
RESEARCH REPORT
Locus of control of behaviour: is high externalityassociated with substance misuse?
PHILIP HAYNES & GLENDA AYLIFFE
Options Community Drug Team, Worthing, West Sussex, UK
AbstractPersonal control and responsibility are key themes in the therapeutic use of 'motivational interviewing'. Thispopular method of counselling has suggested that clients need to believe they have a significant degree of controlover their behaviour if they are to make progress. Using a well validated psychological test on locus of control ofbehaviour, our research sought to establish whether active misusers really believed thay had less personalcontrol than non-misusers. To establish this a sample of misusers was tested and compared with three diverse,comparable groups. Possible confounding factors such as age, sex and class were controlled for. T testsestablished a significant difference between the active misusers and the other sampled groups. Further, aregression analysis of variance, calculated to explain the differing external scores offered no reasonableexplanation as far as age, sex and class were concerned. Alternatively, self diagnosed substance misuseaccounted for 23% of the variation in scores. We concluded, therefore, that high externality scores are a goodindicator of active misusing behaviour and that beliefs about personal control are important to address, if one isto increase the chances of a positive client outcome.
IntroductionA broad psychological overview of substance misusehas become increasingly relevant in the last 20years. Many were disillusioned with the traditionaldisease model (Alcoholics Anonymous, 1952; Jelli-nek, 1960; LeBlanc, 1973) and an expanding level ofservices demanded new methods of pragmaticintervention. Society's wish to engage clients, at allstages of misuse—not just the ultimate recovery—dictated a need for a practice philosophy whichcould engage apparently unmotivated and ambiva-lent clients. There became a new desire to under-stand motivation, to seek to find the key factorsinvolved when a misuser makes a self-assessment of
Correspondence: Philip Haynes, Options, 29 Wordsworth Road,Worthing, West Sussex BNll 3NJ.
the advantages and disadvantages for makingchanges.
Today, there is arguably more emphasis on seeingeach misuser as an individual, each having their ownunique psychological needs. Despite the concept ofpersonalised treatment programmes and flexibletreatment, some psychological constructs have beenoffered as an explanation of the hypotheticalpersonality deficit which might preclude and fuelmisusing behaviour.
The therapeutic concept of motivational inter-viewing (Prochaska & Diclemente, 1984; Miller,1983) suggests that key personal constructs, internalattribution, self-efficacy and self esteem must beaddressed if substance misusing behaviour is to bechanged. Motivational interviewing is founded onthese psychological constructs and refiects a cogni-tive behavioural approach to assessment. Motiva-
1111

1112 Philip Haynes & Glenda Ayliffe
tion is defined as a changing state, rather than apersonality trait:
Surely motivation waxes and wanes over time, asis characteristic of background variables. Motiva-tion may also be subject to momentary fluctua-tions that precipitate acute relapse episodes.. . . Our failure to consider motivation as a staterather than a trait may have unduly narrowed ourunderstanding of its contribution to maintenance.(Gossop & Shiffman, 1989, p. 160)
Attribution is the psychological process by whichpersonal change is linked to certain causal factors: ifthe individual believes that they have caused thechange then this is usually referred to as internalattribution; if, however, an external factor is thoughtto have caused the change, such as a disease, or aprescribed drug, then this would be an example ofexternal attribution (Miller, W., 1983). Motiva-tional interviewing, as a therapy, cites that a misusermust be moved towards an internal attribution state,via reflective counselling, if misusing or otherdestructive behaviour is to be changed. Thus,ambivalent or contemplative patients, unsure as towhether they wish to modify or abstain fromsubstances, should not be criticised or directlyconfronted for their lack of apparent motivation,but rather encouraged to attend interviews wherethey can explore their own paradoxical feelings in arelaxed and unthreatening manner. Negative state-ments such as: "I'm still using heroin", may berestructured by the therapist and reflected in thelight of other more positive evidence, such as:"You're using less frequently than before": the aimbeing to restructure the client's own assessment ofthe possibilities for change, so that they think morepositively—and with an increased level of confi-dence that change is indeed possible. In addition,cognitive dissonance is highlighted and the patientencouraged to make priorities out of the conflictinginformation that they present. For example: wheretheir own liberty is threatened by imprisonment,despite their constant reports of the positive emo-tional feelings generated from taking drugs. Theclient is encouraged to make internal outcomeattributions.
Internal attribution is similar to another psycho-logical concept, internal locus of control. Rotter, forexample, made observations about the influence ofsubjects' beliefs on their behaviour, and he notedhow these beliefs influenced actual outcome (Rot-ter, 1966).
Of recent interest, however, is the idea that selfefficacy is more important to initiating behaviourchange than the outcome assessments a personmakes of the likely benefit they will experience ifthey change behaviour. Perhaps the most historicalsignificant contribution in this field is from Bandura(1977). He suggested a theoretical model of behav-iour change which hypothesized that expectations ofself-confidence, about whether or not change couldbe achieved, were essential to address, if behaviourwas to be stabilized or changed.
Subsequently, Bandura has continued his defini-tion of the construct (Flavell et al., 1981) andconcluded that self efficacy is concerned withjudgements about how well one can organise actionand execute change in specific situations. Saltzer(1982) clarifys various definitions of efficacy. Firstthere is a 'belief in efficacy': a subject believes thatthey are capable of performing a given behaviour.Secondly, 'behavioural efficacy', similar to outcomeexpectancy and locus of control, asks: how likely isit that performing the behaviour will lead to thedesired outcome. This theme has been continuedvery recently by Solomon & Annis (1990) whoundertook a field study of 100 male alcoholdependants from two treatment centres in Ontario.The study concluded that outcome expectancies(personal costs and benefits expected to result froma change in drinking) did not predict consumptionat post treatment follow-up. Alternatively, selfefficacy, or 'belief in efficacy', were strongly associ-ated with the level of consumption on drinkingoccasions, once that subjects had left residentialtreatment (n=90, Chi=72.7 at intake andChi=90.5 at follow-up; p<0.001). But Saltzer(1982, p. 215) states that outcome attributions andexpectancies appear to affect subsequent behaviour,by moderating the beliefs relating to personalefficacy (p. 217). In this sense self efficacy andlocus of control are related. Perhaps an increase ininternal outcome attribution contributes to a greaterself efficacy?
In Saltzer's view, locus of control is also closelyrelated to learned helplessness. This attributiontheory (Seligman, M. E. P., in Rehm L. R., et al.,1981) is more specific and is concerned as to whathappens to people when they realize that theycannot control outcomes, and as a result theirattributional style is affected. In Seligman's viewthis learning is dysfunctional and can be corrected intherapy by emphasising and amplifying internalprocesses. Thus, it is hypothesized that attributionalstyle has been erroneously learned.
Locus of control of behaviour 1113
Seligman has reported a relationship between selfreported external attribution style and depres-sion—regardless of intervening and traumatic lifeevents. Nevertheless, later writers (Rothwell &Williams, 1983), have developed this model, prefer-ing instead to link traumatic life events as a possiblecausal factor in the correlation of attributional styleand depression.
It is clear that locus of control has had sometheoretical and historical validity as an indicator ofpatients' outcome attributional states, but in recentyears the construct validity of Rotter's locus ofcontrol scale was questioned. These doubts took theform of questioning the measurement validity of thescales: that is, is the scale actually measuring otherconfounding factors? It was noted by P. T. P. Wongand C. F. Sproule (in Lefcourt et al., 1984) thatidealism and realism were such extraneous factors:for example some subjects, who were able to learnsuccessfully and make significant personal progress,scored externally, because they felt that the moresocial choices in the scale were 'realistically' out oftheir own control. Conversely, those who have veryhigh internal scores were oversold on their ability tocontrol the world around them and thus unrealistic.Therefore personal autonomy is always defined inthe context of some external constraints.
It is because of these paradoxical factorsthat some decided locus of control is too much aglobal concept. Key researchers in the field beganencouraging the proliferation of new scales tomeasure specific aspects of locus of control asrelevant to specific areas (Lefcourt, 1976). Leven-son, for example (Lefcourt et al., 1984), proposesan alternative three section scale, measuring: inter-nality, powerful others and chance. She commentsthat a small sample of men with alcohol problems(n=23) showed significant differences to controlgroups on the chance scale and scored higher,but this was not the case on the other twodimensions.
Certainly research, using Rotter's original scale,has identified different sub-scales within the mainindex which offer some insight into the differentcontrol concepts within the original construct.Mirels (1970) used factor analysis to isolate twodimensions: personal control and sociopolitical con-trol. Reid & Ware (1974) developed their own 40item scale and identified three sub scales within themain locus: these were; fatalism, social systemcontrol and self control. More recent research hasreplicated these three factors in a British neuroticsample (Fitch, 1984). It is the idea of a scale to
measure self control with which I am particularlyinterested, as those dependent upon substancesfrequently report that they are unable to controltheir own behaviour.
Craig, Franklin & Andrews (1984) developed oneof the most recent and, in my view, significant newscales. This measures locus of control of behaviour,rather than more general, social aspects. It wasdeveloped to predict likely relapse into previousunwanted behaviours. A 17 item Likert scale wassuccessfully developed and found to have internalreliability (Coefficient alpha=0.79; Test-Retestreliability over one week=0.90, over 6months=0.73). Other aspects of internal validitywere satisfied; confounding variables of age and sexwere adequately controlled for. Concurrent validitycould be shown by the close proximity of scores tothe personal control factor in Rotter's scale (Mirels,1970). This factor correlated at 0.70 males and 0.67females («=123). Predictive validity was satisfiedwith a population of stutterers.
The majority of locus of control studies usingsubstance misuse populations have used exclusivelyalcohol dependants. Many used small samples whichrelied on those who had entered residential orinpatient programmes; therefore there is often doubtabout whether the results are over generalized toassume all those with alcohol difficulties, rather thanthe specific sub populations measured. It might be alack of scrutiny of such detail in past research whichhas led some authors who examine psychologicalpredictors to conclude that locus of control isinconclusive (see Galizio & Maisto, 1985, also,Edwards et al., 1987). An alternative explanationwould be that the type of scale used needs to berefined, and that adequate sample types must belocated with which to test new and refined scales(see Hinrichsen, 1976 and Rohsenow & O'Leary,1987a).
Rohsenow & O'Leary (1987a,b) comment that inthe better designed studies, alcohol dependantsbecome internal over treatment (see Chess et al.,1971; Butts & Chotlos, 1973; O'Leary et al, 1975and Oblitz & Swanson, 1976).
Stafford (1980) surveyed three different treat-ment samples, an inpatient unit, a private hospitaland an outpatient psychological counselling pro-gramme (Total w = 96). He concluded that differentmean locus of control scores resulted from thedifferent therapies. Such research highlights thatcertain treatments actually teach external attribu-tion to patients as a method of recovery. Indeed,Marlatt comments:

1114 Philip Haynes &• Glenda Ayliffe
It is tempting to consider the possibility ofmatching a particular treatment approach withthe client's own expectancy system or locus ofcontrol orientation. (Marlatt & Gordon et al.,1986, p. 67)
MethodsThe aim was to measure locus of control ofbehaviour amongst a group of substance misusersand then compare this to several diverse groups of asimilar size. Within the control groups it was hopedto hold Mean age fairly constant, while selectingdifferent gender and class types (see Table 1). Thelocus of control of behaviour 17 item Likert scalewas used, with an additional questionnaire attachedso that a number of possible confounding indepen-dent variables, including age, sex and occupation,could be examined. Further, there was a questionasking if the respondents experienced any currentproblem with alcohol or drugs. This informationwas used to eliminate, from the misuser's group,misusers who felt that they had no current substancedifficulties and also, to ensure that, in the non-misusing control groups, self diagnosed misuserscould be extracted. It was stressed to subjects thatthe questionnaire would remain anonymous.
The substance misuse group consisted of 25clients attending a community drug project inWorthing, West Sussex. Subjects were selected atrandom from a possible 103 attending the agencyduring February/March 1990; this was achieved bya visiting social work diploma student administeringthe questionnaire on different, consecutive week-days over a period of 6 weeks, the research databeing completed after any other therapeutic or crisiswork had been done. The total number of clientsavailable on these specific sampling days was 34. Ofsix non respondents, three refused to take part, tworeturned incomplete questionnaires and one com-pleted questionnaire was rejected because the sub-
ject declared himself problem free concerningsubstance misuse. A further three clients left theagency whilst other subjects were being interviewedand were not requested to wait and take part. Meanage for the respondent sample was 34.4. Unfortu-nately the student administering the research ques-tionnaire was only able to ascertain numbers of nonrespondents, and not their age, sex and social class.Nevertheless, yearly data records at the host agencygive some indications as to the nature of thepopulation sampled; in 1989/1990 the Options newreferrals contained the following primary problemgroups: Opiates 26.9%, Alcohol 35.3%, Benzodia-zepines (Minor Tranquillisers) 16.7% and others21.2%. Of this population (N=156) the Mean Agewas 31.73 and 33.3% were women and 66.6% men.In our responding sample Mean age was 34.4 andthere were 8 women and 17 men. Chaotic andproblematic patients were more likely to be repre-sented in our sample because such people attend theagency more regularly.
Group two, the first of the control groups,contained 25 postmen. The Mean age for this groupwas 38.9. Selection was on the basis of whichworkers were available for interview, on twoseparate visits to the sorting office. The size of thepossible population was 202 (Mean age 40), allemployed at one particular office in the South East.The aim was to use the group as an indicator oflikely test scores from a working class, malepopulation and for this reason the small number ofwomen employed at the office were not asked toparticipate. All the postmen were coded social classD. There were no refusals, but one completedquestionnaire was rejected because the subjectdeclared an alcohol problem.
The third group (second control group) con-tained 21 women, taken from a wider population of240 members of a branch of Working Association ofMothers in the South East. Mean age for theselected group was 34.1 (Mean age of total popula-
Table 1. Experimental and control groups: sample characteristics
Sample
Substance misusegroup
Postmen
Women'sgroup
Traineesocial workers
Mean Age
34.4
38.9
34.1
38.9
Gender
17m8w
25m
21w
9m16w
Social Class
MajorityC2, D
D
MajorityAB, Cl
MajorityCl
Locus of control of behaviour 1115
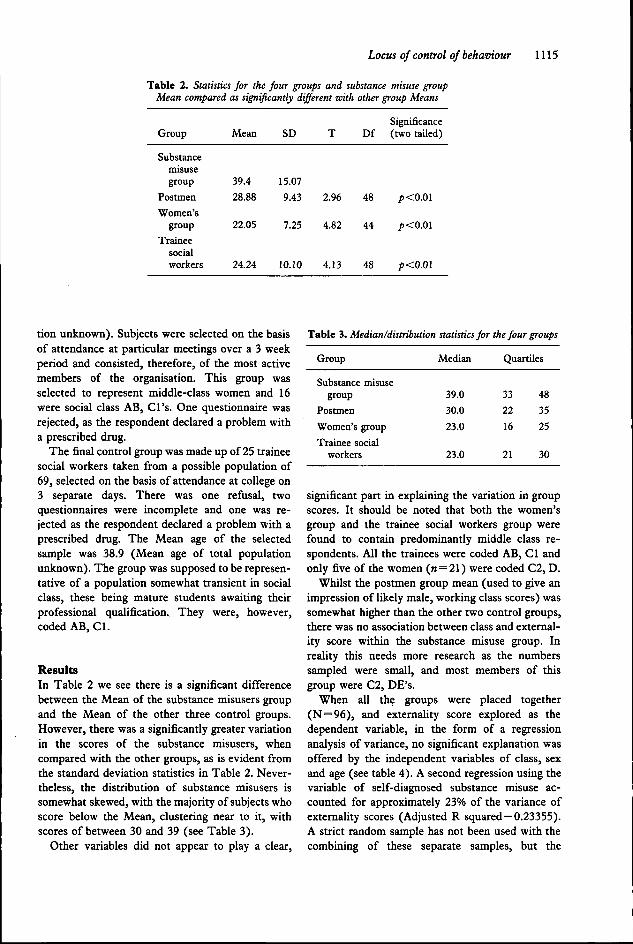
Table 2. Statistics for the four groups and substance misuse groupMean compared as significantly different with other group Means
Group
Substancemisusegroup
Postmen
Women'sgroup
Traineesocialworkers
Mean
39.4
28.88
22.05
24.24
SD
15.07
9.43
7.25
10.10
T
2.96
4.82
4.13
Df
48
44
48
Significance(two tailed)
p<O.Ol
p<O.Ol
p<0.0\
tion unknown). Subjects were selected on the basisof attendance at particular meetings over a 3 weekperiod and consisted, therefore, of the most activemembers of the organisation. This group wasselected to represent middle-class women and 16were social class AB, Cl's. One questionnaire wasrejected, as the respondent declared a problem witha prescribed drug.
The final control group was made up of 25 traineesocial workers taken from a possible population of69, selected on the basis of attendance at college on3 separate days. There was one refusal, twoquestionnaires were incomplete and one was re-jected as the respondent declared a problem with aprescribed drug. The Mean age of the selectedsample was 38.9 (Mean age of total populationunknown). The group was supposed to be represen-tative of a population somewhat transient in socialclass, these being mature students awaiting theirprofessional qualification.. They were, however,coded AB, Cl.
ResultsIn Table 2 we see there is a significant differencebetween the Mean of the substance misusers groupand the Mean of the other three control groups.However, there was a significantly greater variationin the scores of the substance misusers, whencompared with the other groups, as is evident fromthe standard deviation statistics in Table 2. Never-theless, the distribution of substance misusers issomewhat skewed, with the majority of subjects whoscore below the Mean, clustering near to it, withscores of between 30 and 39 (see Table 3).
Other variables did not appear to play a clear.
Table 3. Median/distribution statistics for the four groups
Group
Substance misusegroup
Postmen
Women's group
Trainee socialworkers
Median
39.0
30.0
23.0
23.0
Quartiles
33
22
16
21
48
35
25
30
significant part in explaining the variation in groupscores. It should be noted that both the women'sgroup and the trainee social workers group werefound to contain predominantly middle class re-spondents. All the trainees were coded AB, Cl andonly five of the women (n=21) were coded C2, D.
Whilst the postmen group mean (used to give animpression of likely male, working class scores) wassomewhat higher than the other two control groups,there was no association between class and external-ity score within the substance misuse group. Inreality this needs more research as the numberssampled were small, and most members of thisgroup were C2, DE's.
When all the groups were placed together(N=96) , and externality score explored as thedependent variable, in the form of a regressionanalysis of variance, no significant explanation wasoffered by the independent variables of class, sexand age (see table 4). A second regression using thevariable of self-diagnosed substance misuse ac-counted for approximately 23% of the variance ofexternality scores (Adjusted R squared=0.23355).A strict random sample has not been used with thecombining of these separate samples, but the

1116 Philip Haynes & Glenda Ayliffe
Table 4. All group samples combined. Multiple regression analysis of variance
Dependent variable = external locus of behaviour scores.
First regression. IV=Age, Sex, Class. All entered.
Multiple R 0.24937Adjusted R squared
F =
VariableClassAgeSex(Constant)
0.03160
2.03345
Beta-0.3127-0.16782-0.19195
(3,92)
Multiple
T-0.249-1.659-1.524
4.577
Significance (p<0.001)Not significant
regression
SigT(/i<0.001)Not significantNot significantNot significant
Second regression. IV=Self diagnosed substance misuse.
Multiple R 0.49155Adjused R squared 0.23355F = 29.94789 (1,94) Significance =/>(<0.001)
Variablemisuse(constant)
Beta0.49155
Multiple
T5.472
19.084
regression
SigT(/XO.OOl)(p<0.001)
regression analysis still has some value in exploringthe limited impact of class, sex and age onexternality. The result is that it would appear thesevariables are not related to score.
Conclusions and discussionThere is a clear suggestion from this research thatactive substance misusers are likely to have compar-ably higher external locus of control of behaviourscores than non-misusers. The variables of age, sexand class seem to add very little to our understand-ing of why certain people score higher than others.Previous research, using similar social psychologicalconstructs, has also found these demographic vari-ables unable to explain variance (see Wilkins, 1975;Strickland & Hayley, 1980; Greene, 1981).
Further research is needed to examine whethersubstance misusers who do well in community basedtreatment also achieve significantly lower externalscores over time. It might be that the type oftherapeutic model used is a confounding factor (seeBrickman et al., 1982) and that disease modelsdictate a degree of externality as necessary forabstinence, even if this has negative consequencesfor relapse management (see Marlatt & Gordon,1986). Where cognitive behavioural therapy is usedwe would expect increased internality to predict
behaviour change maintenance. The question israised as to whether the positive role of externalityin disease model therapies is in fact a model of'shifting dependence', where the difficulties ofefficacy and outcome expectancy are temporarilydisplaced and held in limbo, via the belief that: 'I amill and must depend on this explanation to survive'.This is not necessarily a criticism of the diseasemodel in practice, albeit a fundamental theoreticalindictment. It might well be that its success is due tothe cognitive shift which is achieved when subjects'passive, dependent condition is accepted.
AcknowledgementsWe wish to thank all the Options staff for their co-operation and assistance with this research andindeed all the clients who agreed to take part. Forreasons of confidentiality we do not want to identifythe specific source of the other groups, but SallyJenkins, Senior Clerical Officer at Options, wasparticularly instrumental in liaising with one ofthese sources. Our thanks also to Worthing DistrictPsychology Department and Mike George, TopGrade Psychologist, Options, for advising on the useof a suitable psychological test. West Sussex Proba-tion Service have provided important financial helpby seconding officers to substance misuse work and

Locus of control of behaviour 1117
funding Phil Haynes' MSc research studies. DrRoger Sapsford has encouraged much of this workand provided important consultation.
ReferencesALCOHOLICS ANONYMOUS (1952) Twelve Steps and
Twelve Traditions (New York, A.A. World ServicesIncorporated).
BANDURA, A. (1977) Self-efficacy: toward a unifyingtheory of behavioural change. Psychological Review, 84,pp. 191-215.
BwcKMAN, p., RABINOWITZ, V. C , KARUZA, J., COATES,D., COHN, E. & KiDDER, L. (1982) Models of helpingand coping, American Psychologist, 37, pp. 368-384.
BiTTTS, S. V. & CHOTLOS, J. (1973) A comparison ofalcoholics and non alcoholics on perceived locus ofcontrol. Quarterly Journal of Studies on Alcohol, 34, pp.1327-1332.
CHESS, S. B., NEURINGER, C. & GOLDSTEIN, G . (1973)Arousal and field dependency in alcoholics. Journal ofGeneral Psychology, 85, pp. 93-102.
CRAIG, A. R., FRANKLIN, J. A. & ANDREWS, G . (1984) Ascale to measure locus of control of behaviour, BritishJournal of Medical Psychology, 57, pp. 173-180.
EDWARDS, G. , BROWN, D. , DUCKITT, A., OPPENHEIMER,E., SHEEHAN, M . & TAYLOR, C . (1987) Outcome ofalcoholism: the structure of patient attributions as towhat causes change, British Journal of Addiction, 82, pp.533-545.
FLAVELL, J. , ROSS, L . & BANDURA, A. (1981) Cognitive
Social Development (New York, Guilford).FITCH, M . D . (1984) Locus of control factor structure in a
British neurotic sample, British Journal of ClinicalPsychology, 23, pp. 145-146.
GALIZIO, M & MAISTO, S. (1985) Determinants ofSubstance Abuse: biological, psychological and environ-mental factors (New York, Plenum Press).
Gossop, M. & SHIFFMAN, S. (1989) Relapse and AddictiveBehaviour (London, Tavistock/Routledge).
GREENE, S. M . (1981) Levels of measured hopelessness inthe general population. The British Journal of ClinicalPsychology, 20, pp. 11-14.
HiNRlCHSEN, J. J. (1976) Locus of control among alcohol-ics: some empirical and conceptual issues. Journal ofStudies on Alcohol, 37, pp. 908-916.
JELLINEK, E. M. (1960) The disease concept of Alcoholism(New Brunswick, Hill House).
LEFCOURT, H. M. (1976) Locus of Control: current trendsin theory and research (New York, Wiley).
LEFCOURT, H . M . , WONG, P. T. P. & SPROULE, C . F .(1984) Research with the locus of control construct.Volume 3: Extensions and Limitations (Orlando, Acade-mic Press).
LEBLANC, A. H. (1973) The disease concept of alcoholism.The Journal, Toronto I (No. 12), p. 4.
MARLATT, G . A. & GORDON, J. R. et al. (1986) RelapsePrevention (New York, Guilford).
MILLER, W . (1983) Motivational interviewing with prob-lem drinkers. Behavioural Psychotherapy, 11, pp.147-172.
MiRELS, H. L. (1970) Dimensions of internal versusexternal control. Journal of Consulting and ClinicalPsychology, 34, pp. 226-228.
OBITZ, F . W . & SwANSON, M. K. (1976) Controlorientation in women alcoholics. Journal of Studies onAlcohol, 37, pp. 694-697.
O'LEARY, M . R. , DONOVAN, D . M . , HAGUE, W . H . & SHEA,R. A. (1975) Shifts in component factors of locus ofcontrol as a function of treatment in male alcoholics.Journal of Clinical Psychology, 31, pp. 359-361.
PROCHASKA, J. O . & DiCLBMENTE, C. (1984) The transthe-oretical approach: crossing traditional boundaries oftherapies (Homewood, Illinois, Dow Jones/Irwin).
REHM, L. R. et al. (1981) Behaviour Therapy andDepression (New York, Academic Press).
REID, D . W . & WARE, E . E. (1974) Multidimensionality ofinternal versus external control: addition of a thirddimension and non distinction of self versus others,Canadian Journal of Behavioural Science, 6, pp.131-142.
ROHSENOW, D. J. & O'LEARY, M . R. (1978a) Locus ofcontrol research on alcoholic patients: a review. I.Development, scales and treatment. International Jour-nal of the Addictions, 13, pp. 55-78.
RoHSENOW, D. J. & O'LEARY, M . R. (1978b) Locus ofcontrol research on alcoholic populations. II. Relation-ships to other measures. International Journal of theAddictions, I, pp. 213-226.
ROTHWELL, N. & WILLIAMS, J. M. G. (1983) Attributionalstyle and life-events, British Journal of Clinical Psycho-logy, 22, pp. 139-140.
ROTTER, J. B. (1966) Generalised expectancies for internalversus external control of reinforcement. PsychologicalMonographs, 80, p. 609.
SALTZER, E. B. (1982) The relationship of personalefficacy beliefs to behaviour, British Journal of SocialPsychology, 21, pp. 213-221.
SOLOMON, K. E. & ANNIS, H . M . (1990) Outcome andefficacy expectancy in the prediction of post-treatmentdrinking behaviour, British Journal of Addiction, 85, pp.659-665.
STAFFORD, R. A. (1980) Alcoholics' perceptions of inter-nal-external locus of their drinking. Journal of studieson Alcohol, 41, pp. 300-309.
STRICKLAND, B. R. & HALEY, W . E . (1980) Sex differenceson the Rotter I-E Scale, Journal of Personality andSocial Psychology, 39, pp. 930-939.
WiLKiNS, W. E. (1975) Trends in Powerlessness: a tenyear follow-up, J'oMnia/ of Psychology, 91, pp. 15-18.






























