Embed Size (px)
Citation preview

LOGO
UPPER URINARYTRACT T.C.C.
Presented by:
Dr.HashimNaji
R3

CONTENT
DefinitionEpidemiologyRisk factors & associationsDiagnosisStagingTreatment

definition
any neoplastic growth that affects the lining of the urinary tract from the calyces to the distal
ureter.

Epidemiology
Renal pelvic Ca is 10% of renal tumor.5 % of urothelial tumor.Ureteric tumor is 1% of urothelial tumor.
( 73% :distal , 24% :mid , 3% : prox. )M : F is 2 : 1W : B is 2 : 1

Epidemiology
10/100000/year in white male .Peak age is 75—79 years .2 – 5% is bilateral.2-4 % incidence Of upper tract TCC in pts
with bladder TCC.20% risk of upper urinary tract TCC in
bladder CIS at 10 y.40-80% risk of bladder TCC in upper tract
T.C.C. pt.

Risk Factors
Balkan nephropathy:Degenerative interstitial nephropathy, in
rural areas of Balkan countries100-200 time incidence of upper tract T.C.C.
in these families.
Generally low grade, multiple & bilateral more than other T.C.C.
It is familial but not obviously inherited, suggesting an environmental etiology that has yet to be identified.
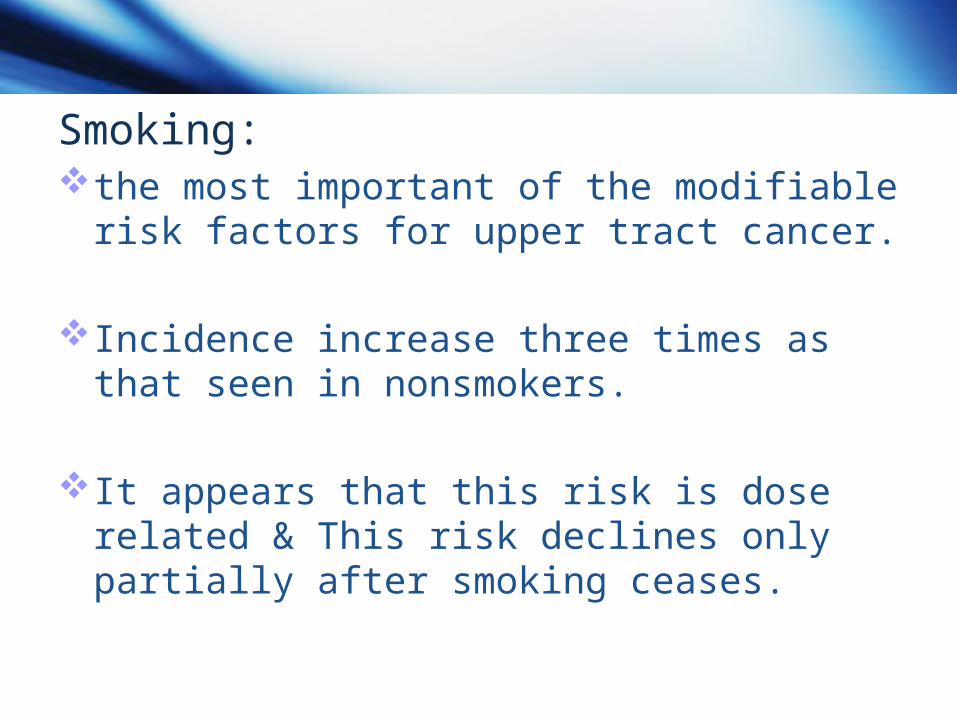
Smoking:the most important of the modifiable risk
factors for upper tract cancer.
Incidence increase three times as that seen in nonsmokers.
It appears that this risk is dose related & This risk declines only partially after smoking ceases.

Analgesics: phenacetin increase risk by 3.6 times,
become 20 if combined with papillary necrosis.
Histologic findings associated with analgesic abuse include thickening of the basement membrane (pathognomonic) and papillary scarring.
Thickening of the basement membrane has been demonstrated in 15% of patients with upper tract tumors

Risk FactorsCoffee: A relative risk of 1.8 times normal has been
described in individuals who consumed more than seven cups of coffee per day.
Ocupational factors: chemical,petrochem. Plastic industries ,coal ,coke
, asphalt, tar.
Hereditary: Lynch syndrom ll is a familial proximal colonic
nonpolypotic Ca with extracolonic Ca mostly endometreal, may have increase risk of upper T.C.C. pts tend to be younger with female predominance.

Symptoms and SignsThe most common presenting symptom of
upper tract urothelial tumors is hematuria, either gross or microscopic.
Dull flank pain in 30% secondary to gradual obstruction.
Acute renal colic if clots obstruct collecting system.
About 15% of patients are asymptomatic
symptoms of advanced disease, including flank or abdominal mass, weight loss, anorexia, and bone pain.

Radiologic evaluationIVP:Traditional means of diagnosis of TCC.
Radiolucent filling defects, obstruction or incomplete filling of a part of the upper tract, and nonvisualization of the collecting system are the typical findings suggestive of an upper tract tumor.
D/D..blood clot, stones, overlying bowel gas, external compression, sloughed papilla, and fungus ball.

CT urography:the sensitivity for detecting upper tract
malignant disease has been reported to approach 100%, with a specificity of 60% and a negative predictive value of 100% .
CT urography does, however, expose the patient to higher doses of radiation.
Transitional cell cancers have an average density of 46 Hounsfield units (HU) and a range of 10 to 70 HU. This is in contrast to an average of 100 HU seen in radiolucent uric acid stones (range, 80 to 250 HU).

MRI: no advantage over CT.
CT or MRI is most useful in determining the extent of invasion, an associated mass lesion outside the collecting system, and the presence of lymph node or distant metastases.
U/S : Little value in definitive Dx. And staging.



Diagnostic proceduresCystoscopy:mandatory in the evaluation to exclude
coexistent bladder lesions.
Retrograde pyelography:An incompletely filled or obstructed renal
infundibulum or calyx, occurring in 10% to 30% of cases, again typically requires retrograde urography with urine cytology

Ureteroscopy:should probably be reserved for situations
in which the diagnosis remains in question after conventional radiographic studies.
In addition to visualization of the tumor, ureteroscopy allows more accurate biopsy of suspected areas, with either biopsy forceps or brushing .

STAGING TNM Staging System
Ta : epithelial confined, usually papillary.
Tis : CIS . T1 : lamina propria . T2: muscularis propria . T3:
peripelvic/periureteric tissue or renal parenchyma .
T4 :contiguous organs .
N1 : L.N. <= 2 cm. N2 : L.N. >2 <=5cm or
multiple L.N. < 5 cm. N3 : L.N. > 5 cm.
………………………………………..
MO : no mets. M1 : distant mets.

Prognostic FactorsStage :the most important predictor of survival in
patients with upper tract urothelial tumors.
the most significant decrease in survival is observed in T3 tumors.
Grade:tumors of high grade are more likely to
invade into the underlying connective tissue, muscle, and surrounding tissues.

Location:renal pelvic tumors have a better prognosis
than ureteral cancers.
Associated Carcinoma In Situ: poor prognosis and a likelihood of future
development of invasive urothelial cancers.
P53 mutation: has important role in tumor development &
progression .

treatmentOptions:
1.Nephroureterectomy.2.Segmental Resection (Nephron-Sparing
Surgery) of Renal Pelvic Tumors.3.Segmental (Partial) Ureterectomy .4.Endoscopic Resection or Fulguration
(Retrograde and Antegrade).5.Use of Topical Immunotherapy and
Chemotherapy.

nephroureterectomy
Radical nephroureterectomy with resection of a bladder cuff remains the “gold standard”
1. large2. high grade 3. invasive 4. and for large, multifocal or rapidly recurring,
medium-grade, noninvasive tumors of the renal pelvis or proximal ureter.
can be done totally by open technique totally laparoscopically and by a combination of laparoscopic and
open techniques (usually laparoscopic nephrectomy and ureterectomy except for the distal or intramural portion, which is done by an open approach).

The entire ureter, including the intramural portion and ureteral orifice, should be removed.
The risk of tumor recurrence in a remaining ureteral stump is 33% to 75%.

Segmental Resection (Nephron-Sparing Surgery) of Renal Pelvic Tumors
indicated in the rare patient with a large, localized tumor in a solitary kidney and synchronous bilateral tumors.
after standard flank incision and dissection of the kidney and renal pelvis are accomplished, pyelotomy and resection of the tumor are undertaken, and its base (if it is abutting the renal parenchyma) is cauterized with electrocautery, laser, or argon bean coagulator.

In larger tumors that invade the renal parenchyma, standard partial nephrectomy may be used.
Risk of recurrence is 10% for grade 1 tumors to 30% for grade 2 and 60% for grade 3.
high-grade, muscleinvasive, organ-confined tumors may be best treated by nephroureterectomy even if this means that dialysis will be necessary.

Segmental (Partial) Ureterectomy
indicated for noninvasive, grade 1 or grade 2 tumors of the proximal or middle ureter that are too large for endoscopic management and for grade 3 or invasive tumors when nephron sparing must be done to preserve renal function.

Endoscopic Resection or Fulguration (Retrograde and Antegrade)
Endoscopic treatment of patients with upper tract transitional cell carcinoma is generally recommended in those patients with a solitary kidney, bilateral disease, renal dysfunction.
appropriate in selected patients with small, low-grade lesions in the presence of a normal contralateral kidney.
recurrence is likely even with frequent reinspection

retrograde approacheis less invasive but limited to some degree by the size of instrument that can be introduced through the ureter.

Use of Topical Immunotherapy and Chemotherapy
The agent most commonly employed for treatment or adjuvant therapy is BCG
Methods of delivary: PCN(best),retrograde , refluxing ureter .
Complications: scarring,sepsis,BCGosis (systemic absorption
greater than in bladder).
No statistical improvement in survival or recurrence rate .

Chemotherapy for Advanced Disease
Upper tract transitional cell cancers, like bladder cancers, are relatively chemosensitive.
Single agent chemotherapy with cisplatin, methotrexate, cyclophosphamide, or gemcitabine has yielded response rates only in the 25% to 35% range, so combination therapies have commonly employed.













![7 Catheter-associated Urinary Tract Infection (CAUTI) · UTI Urinary Tract Infection (Catheter-Associated Urinary Tract Infection [CAUTI] and Non-Catheter-Associated Urinary Tract](https://img.pdfslide.net/doc/110x75/5c40b88393f3c338af353b7f/7-catheter-associated-urinary-tract-infection-cauti-uti-urinary-tract-infection.jpg)