Embed Size (px)
Citation preview

Loh Tsee Foong Director Children ICU KKH
Dy/Director Education Office Paeds ACP A/Professor Duke NUS SoM
Lead, Child Protection Team Director PFCCS Singapore

Hypoxaemia
• ARDS, ALI, AHRF
• Oxygenation indices (P/F; OI)
• American European Consensus Conference
• Berlin definition update on ARDS
• PARDS PALICC group
Ventilator modes
• Basic P-CMV; P-AC; PRVC; VC-AC
• Non basic HFOV APRV BCV HFPV
• Adjuncts (iNO, PP, RM)
EmBase PubMed Medline
• Exclude case reports

Outcomes
• Mortality
• Oxygenation indices – OI P/F SaO2/FiO2
• Performance scores
• LOS length of stay
• VFD ventilator free days
• Side effects

Very often medical care for child is
based on what works for adults
• Selective adoption
Ventilator Induced Lung Injury VILI/ Open lung
Low Vt, higher PEEP, Limiting Ppk Pplat
Adjuncts (iNO, RM, PP, fluid management, steroids)
Permissive Hypercapnia and allowable saturations
VC-AC; PC-AC; PRVC
Mortality have improved
• What about lessons from neonatology?
Khemani R et al AJRCCM 182: 1465-74
Needham DM et al BMJ 344: e2124

PALIVE study “What the real world is”
• 59 PICU in North America and Europe
Variability in practise
Use of CMV 75% HFOV 16% NIV 8%
PC-CMV 44% with 8.3+/-3.3 ml/kg
No clear PEEP & FiO2 relationship
Adjunctive treatment not standardised
• Few explicit protocols in paediatric ventilation
• Use of ideal or actual body weight uncertain
Santschi M et al PCCM 11: 681-9

“What the ideal world is”
Given 3 hypothetical
cases to interact
• Mild, moderate, severe ALI
Discrepancy in
• Use of PEEP
Elevated PEEP to 12-
14cmH2O
50%kept PEEP <8cmH2O
• Vt used
None chose Vt>10ml/kg
20% used Vt>10ml/kg
• Adjuncts
iNO 12.7% PP 17.6%
90% use both
• HFOV use 8.5%
No uniformity in theory
Mismatch in
knowledge and
practise

Limited evidence to support PC or VC
• PC decelerating flow
• Pressure Regulated Volume Control
OI; PedsLIS; P/F; Cdyn relate to mortality • SCT n=398 AHRF PCV lung protective strategy
• Vt 610ml/kg
Trend for higher mortality with lower Vt & VFD
Worse lung had lower Vt
Higher Vt and better outcomes in less severe ALI

? Optimal Vt used under LPS
Use of permissive hypercapnia
PC CMV
• Generated Vt is function of severity of lung dis
• Do we need to standardised Vt?
Smaller diameter airways high resistance
Use of higher PEEP hyperinflation
Higher dead space in children hypo alveolar MV
Prella M et al Chest 122: 1382-8
Khemani G et al ICM 35: 1428-37

High Frequency Oscillation Ventilation
• Lung protective features
Use in 30-50% of paediatric ARDS/ALI
• Lack of universally accepted practice for
initiation or use
Evidence for variability
Practice has not changed over decades
Based on OI
>3d of MV before HFOV use
Mehta NM et al Curr Opin Crit Care 10: 7-12
Ben Jaballah N et al PCCM 7: 362-7
Arnold JH et al CCM 28: 3913-9
Erickson S et al PCCM 8: 317-23
Randolph AG et al JAMA 288: 2561-8

ARDS n=25
Failed CMV
Improved
oxygenation
• OI 38 17
• P/F 65152
• Unchanged
haemodynamics
Overall mortality
52%
AHRF n=17
Failed CMV
• PCO2 >85 PO2 <60
Improved
oxygenation
• 17% trachael bleeding
Overall mortality
47%
Pinzon AD et al Rev Assoc Med Bras 59: 368-74 Tassiou I et al ICM 36 (S2) S108

Retrospective study n=69 SCT Argentina
• ARDS failed CMV 8h no ECMO use
• 80% LRTI or sepsis
• 60% co-morbidities
• 93% refractory hypoxia
• 33.4% survival
• Non survivors
Higher acuity scores MOF
Worse LIS & oxygenation indices
Taffarel P et al Arch Argent Pediatr 110: 214-20

N=80 ARDS 40%
• SCT Portugal
• 85% prior CMV 12h
• 70% refractory
hypoxia <90%
• Sat/FiO2 improve 24h
• Reduction in FiO2
• Reduction PCO2
• 84% survivors
• Death
MOF, HLHS, shock & resp
failure
Time on CMV
• 8.8h (survivor) vs 133h
(non survivor)
• 30h (survivor) vs 63h
(non survivor)
• Mortality 40-50%
Fort et al 5.1d
Mehta et al 5.6d
Moniz M et al J Pediatr 89: 48-55
Fedora M et al Scr Med 74: 233-44
Slee-Wijffels FY et al Crit Care 9: R274-9
Fort P et al CCM 149: 818-24
Mehta S et al CCM 29: 1360-9

Rescue or preemptive use?
Cochrane review 2011 update

AHRF n=28
Lung protective
strategy
Improved
oxygenation indices
• P/F 30-40%
• reduction in FiO2
• HFOV better at T8hr
• Similar after 24hrs
Fioretto JR et al Pediatr Pulmonary 46: 809-16

Theoretical advantage
• Constant distending pressure
Higher MAP lower Ppeak
• Spontaneous breathing
• Concern over release phase
Not new!
Limited RCT in adult
None in paediatrics
Varpula T et al Acta Anaesth Scand 48: 722-31
Siau C et al CCM 37: 2448-54
Randolph AG et al CCM 37: 2448-54

Very short release time TL – I:E reverse “CPAP with release” or “BiPAP IRV”
• Recruitment effect
No feedback loop, PS and all SB at TH
Synchronized Transition
Spontaneous Breath
P PEEPH
PEEPL

• Release ventilation during
APRV assoc with decreasing
Paw and lung distension
• Tidal ventilation during
CMV assoc with increasing
Paw and lung distension
Habashi NM et al CCM 33(3)supp: 228-240

• SB in APRV
improve lung
aeration in OA ALI
– N=24 pigs OAALI
assign to APRV+/-
SB
– PaO2 better in SB gp
– Higher EELV on CT
Wriggle et al Anesthesiology 99: 376-84
APRV - SB
APRV + SB

Effectiveness of spontaneous respiration
• Improved pulmonary perfusion
Prospective crossover cohort study APRV vs PC-SIMV
N=20 post-tetralogy, BCPC or Fontan repair
Demonstrated improved pulmonary blood flow and
oxygen delivery in patients post tetralogy rand BCPC
repair
• Better cardiopulmonary interactions
Walsh et al CCM 39(12): 2599

Assess effectiveness of APRV in children
• PRCT crossover MV<7d APRV vs VCV-SIMV
• n=15 mild-mod lung disease (postop,
pneumonia)
Excludes obstructive airway disease, CHD
SIMV and APRV crossover
Inspiratory Paw lower with APRV
Comparable oxygenation and ventilation
Schultz TR et al PCCM 2: 243-46

Retrospective review Single center PICU n=13
• Assess efficacy and effectiveness
• American -European Consensus ARDS criteria
• OI > 10 or clinical decision by physicians
No deterioration in haemodynamics & respiratory by APRV
pO2/FiO2 no change in 1 and 12 hr post-APRV, improved
thereafter
OI increased at 1 and 12 hr post APRV, none thereafter
N=5 died (38%)
4/5 were immunocompromised with HFOV introduced
Kawaguchi A. et al CCM 37(12S): A465

H1N1 pneumonia
Infants with ARDS
H1N1 on PCR with <7d N=5 diagnosed with ALI (a/A < 0.2), PEEP >=7
cmH2O,
Open Lung ventilation with protective lung strategy
If OI >0.1 or FiO2 >0.8 converted to APRV
Better oxygenation and ventilation indices over 24hr
Decrease FiO2 and MAP over 24hr
N=4 survive N=1 death (on HFOV & iNO)
Reduced sedation needs after APRV in all patients
Hisashi et al Ind J Paed 78: 348-350
Demet D et al Ind J Paed77(11) 1322
Loh TF et al CCM 37(12S) 395

0
10
20
30
40
50
60
70
80
90
100
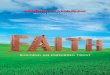
2006 2008 2010 2012
Use of HFOV 2006-2012
Admissions
tens/yrPercent MV %
APRV introduced

Pre-emptive application of APRV in rat
model of trauma/ haemorrhagic shock
with ARDS n=10 VC-SIMV Tv 10ml/kg PEEP 0.5cmH2O
APRV Ph 15-20 Pl 0 cmH20 Th 1.3-1.5s Tl 0.11-0.14s
Prevented ALI measured on P/F ratio
Correlated with histopathology between 2 groups
BAL dcr bronchial protein, incr Prot B and epithelial
cadherin
• APRV attenuates clinical and
histological lung injury in
trauma/ haemorrhagic shock
Roy SK et al Shock 40(3): 210-216

Retrospective n=60 failed CMV SCT
• Immunocompromised ARDS
• Either HFOV (n=31) or APRV(n=29) no crossover
Left to physician discretion
• CMV 1d
• Improvement in P/F OI PCO2 with lower MAP
• Mortality APRV 62% HFOV 65%
Stem Cell Transplant worse outcome
• N=6 started on ECMO (only 1 survivor)
• P/F 24h predicted survivors
• Other cutoffs for APRV & HFOV for survivors Yehya N et al PCCM 15: e147-56

Yes
• Even as rescue when CMV fails
• HFOV use early
• APRV use possibly preemptively

PARDS diverse etiologies
myraid of inter-related pathophysiological events
patient comorbidities and concurrent treatments
differing responses and rehabilitative potential
No particular ideal ventilatory mode
What is lung protective strategy in paed?
Need to translate theory into practice
Preemptive therapy or early rescue
Role of adjuncts

• Spontaneous breaths at 2 pressure levels
• PH transition to PL during expiratory
phase
Synchronized Transitions
Spontaneous Breaths
P Pressure Support PL
PH

Pressure support of SB at PH & PL TH : TL 1:2-3 ratio
PEEPHigh Pressure Support
P
PEEPL
PEEP
H
Pressure Support

Preservation of respiratory muscle
Better patient-ventilator synchrony
• Less sedation, blockage, ?ventilator days
Encourages diaphragmatic contractions
• Allow gas to enter dependent (ventilation) portion of lung
Recruit dependent units without Paw increases
V/Q matching
Improve OI with less Paw
SB at TH allows for further recruitment
• Unlike mechanical breaths preference for non-dep part
lungs
Froese A et al Anesthesiology 41: 242-55
Rehder K et al J Appl Physio 42: 391-402

Haemodynamic effects • Reductions in pleural pressures Improve venous return, renal/splanchnic flow by lowers
RAP
• Increasing abdominal pressure encourages venous return

Pressure High (PH) • Higher of 2 Baseline airway pressure • Oxygenation goal
Time High (TH) • Length for which PH is kept
Pressure Low (PL) • Set to deliver release volume • CO2 clearance
Time Low (TL) • Length for which PL is kept

Not new! 1987
Time triggered pressure limited time
cycled mode
Allow spontaneous during breathing
cycle
Breathing at 2 levels CPAP - BiPAP
Benefits of CPAP in ALI
• Improved PV and less WOB
Downs JB et al CCM 15: 459-61
Stock CM et al CCM 15: 462-66

Patients with ALI or low compliance
• Goal to recruit with PH and avoid de-recruitment
during releases PL
Airway disease
• High peak expiratory flows during release phase
Little or no PEEP to resist expiratory flow
• Expiration can occur throughout cycle
Habashi NM et al CCM 33(3)supp: 228-240

Animals • Lamb in OA ALI
Retrospective reviews
Case reports • Cardiac surgery
• Preterm infant with BPD
• APRV vs SIMV
Martin LD et al Crit Care Med. 1990;18:231
Hales R et al Respir Care 49: 1441
Foland JA et al Respir Care 46: 1019-23
Jone R et al Respir Care 49: 1414
De Carvalho WB et al Rev Assoc Med Bras 46: 166-73
Hutchison AA et al Abstract 10th
REaSoN meeting Warwick 2004
Crooke C et al Respir Care 49: 1376

N=24 adult severe ARDS APRV+/-SB vs PSV with equal MV and Paw
• Effect seen in APRV/SB
• Reduce intrapulmonary shunt, Vd
• Increase in RVeDV, SV, CI, mixed venous and DO2
• Decrease in PVR, oxygen extraction
Putensen C et al AJRCCM 159: 1241-8
Putensen C et al Anesth Int Care 33: 218-22

N=30 ARDS trauma APRV/SB vs PCV(+NMB) weaned with
APRV APRV/SB assoc
Better compliance, CI, PaO2, DO2
Reduced shunt, O2 extraction
• Lower ventilator, intubation and LOS
Concerns PCV group 3d treatment with NMB
PaO2/FiO2 much lower from baseline
Putensen C et al AJRCCM 164(1): 43-9

PRCT n=58 ARDS APRV vs SIMV/PS • Better inspiratory Paw in APRV
• PEEP, gas exchange and haemodynamic indices, LOS, mortality similar
PRCT PP in SIMV PCV/PS vs APRV n=45 • PP for 6hr at 6hr and 24hr admission according P/F
• Pre prone APRV better oxygenation
• 1st prone same improvement in P/F
• 2nd prone better P/F on APRV
• >24hrs to max benefits? Varpula T et al Acta Anesth Scand 47(5): 516-24
Varpula T et al Acta Anesth Scand 47(5): 516-24

APRV vs CMV in ARDS trauma n=30 PRCT • Better gas exchange and haemodynamics
• Less sedation
• Less ventilator and ICU days
APRV vs PCV-IRV ARDS • Similar oxygenation and ventilation
• Better haemodynamic CI, DO2, SV
• Less sedation needs
Varpula T et al Acta Anesth Scand 2003
Kaplan LJ, et al. Crit Care 2001; 5(4):221-6

PRCT uneven randomisation APRV vs CMV vs SIMV post cardiac op
n=596 • Intubation time 10hr vs 15hr vs 13hr
• Less sedation and anaglesia
Rathgeber J et al Eur J Anaesth 14: 576-82

Open lung strategy • Recruitment ripple effect of stablising alveoli
• Promote airway opening
• Continuous recruitment manoeuvre with SB
• Target settings most vent cycle PV relationship above LIP
Release tidal breath to clear CO2 without need for positive pressure tidal ventilation
Spontaneous breathes Ventilation release phase at expiratory limb PV loop
• Open lung TL too short for de-recruitment
• Maintain autoPEEP in PL
Rimensberger P et al CCM 27: 1946-52

Lower Pk
Less WOB, sedation needs
Improve oxygenation and able to
ventilate
Better haemodynamics
Limited outcome studies
? Reduce need in HFOV

High PH levels with low pleural pressures
• High transpulmonary pressures and volutrauma
PL at 0 cmH2O may result in large release
volume
? Cyclical release and opening of alveoli
Titrate TL to autoPEEP need constant adjustment
autoPEEP not heterogeneous amongst disease
lung
Obstructive airway disease

Understand the unique features and
benefits of „new‟ modes of ventilation in
relation to patient lung disease and
targets
No „Ideal‟ mode of ventilation
Combination of modes use
Outcome studies ?realistic

Retrospective AHRF
P/F increased by
mean 28.5
OI not changed
Case reports
Kambhampati S et al CCM 40: 12(S)1015
Krishnan J et al Pediatr Pulmonol 42: 83-8
Schultz TR et al PCCM 2: 243-6
Demirkol D et al Ind J Pediatr 77: 1322-5

Based on ARDSnet
low Vt strategy Using SMA clamping and
release
Induced peritoneal
sepsis
Ventilated 1hr 10ml/kg
Low Vt 6ml/kg PEEP/FiO2
and Pplat <30
APRV
Antibiotics given
Sacrificed after 48h
Histology, BAL, IL-6
APRV group preserved P/F
Better lung compliance
Surfactant abundance
Less pulmonary edema
Reduced IL6
Fairly normal lung
histology
SIRS induced ARDS
can be altered with
preemptive APRV use

Outcome studies vs lung protective ventilation
Role in relation to HFOV


Sustained mean alv volume allows for gas diffusion and combined with cardiac output enable constant gas diffusion between blood and alveolar compartments
Habashi NM et al CCM 33(3)supp: 228-240
● Release ventilation cycle oxygen rich
gas with CO2 rich gas to re-establish
diffusive gradients

• EELV determined by PL and TL
– Artificial airway imposes resistance
– Non linear flow dependent resistive load from high lung volume
– Resistive pattern is highest at initial phase of TL
– Terminate before expiratory load is discharged to keep residual pressure and lung volume
– PL recommended b to be 0cmH2O
Habashi NM et al CCM 33(3)supp: 228-240

• EELV determined by PL and TL
– Artificial airway imposes resistance
– Non linear flow dependent resistive load from high lung volume
– Resistive pattern is highest at initial phase of TL
– Terminate before expiratory load is discharged to keep residual pressure and lung volume
– PL recommended b to be 0cmH2O
Habashi NM et al CCM 33(3)supp: 228-240

TH >> TL • TH 4-8s TL 0.2-0.8s
• 10-20 release breaths per minute
PH • match Pplat on CMV or >30cmH2O
PL allow release to clear CO2 but prevent de-recruitment by keeping end expiratory volume • 0cmH2O or match expiratory flow terminal 25% autoPEEP
• May add PL
• 6-8 (11-12) ml/kg IBW

Effect 6hours Allow SB with appropriate sedation High PH open lung units at critical opening
pressure High TH recruits lung units with long time
constants • Decrease in FiO2
• Increase release volume

Re-set CO2 goals Avoid over sedation Increase TL Increase PH or decrease TH

Reduce PH and PL keeping release volume 6-8ml/kg • Decrements of 2-3 cmH2O
Increase TH to allow more SB • Increments 0.5 to 12-15
Transition to PSV or CPAP/ATC when PH
10-15 cmH2O and PL 5 cmH2O • Concern of PS causing lung over-distension, high
transpulmonary pressure, uncoupling of SB
Habashi NM et al CCM 33(3)supp: 228-240

TH kept as much of the time as possible for continuous recruitment effect
Release tidal breath to clear CO2 without need for positive pressure tidal ventilation
Allowance of SB at all cycles Prevent de-recruitment by manipulating TL
and PL to maintain EELV

n=18 APRV vs VCIRV Better gas exchange and CP mechanics
n=50 APRV vs CMV Better oxygenation
Lang n=18 APRV vs CV Dart et al n=60 trauma ALI retrospective APRV vs PCV-
SIMV • Lower Paw and better P/F
1991 APRV vs CPAP vs CMV in OA ALI sheep model 1993 n=15 APRV vs SIMV ALI postop
• similar
Sydow et al AJRCCM 149: 1550-6
Rasanen et al AJRCCM 1991: 1234-41
Dart BWt et al J Trauma 59: 71-6
Martin LD et al CCM 19: 373-8
Davis K et al Arch Surg 128: 1348-52

Artificial
Spontaneous
Oxygenation Level
CMV (IPPV) CMV (CPPV)
IMV, PSV, BIPAP
T Piece SBT CPAP
APRV
HFOV
IPPV: Intermittent positive pressure ventilation PSV: Pressure support ventilation
CPPV: Continuous positive pressure ventilation
IMV: Intermittent mandatory ventilation BIPAP: Biphasic positive airway pressure
APRV: Airway pressure release ventilation CPAP: Continuous positive airway pressure

Group of techniques using RR>>>CMV
• HFPPV 60-120bpm
• HFJV 400bpm
• HFOV 1000-2000bpm
Less Vt
Sub Vd
Slutsky AS et al Am Rev Resp Dis 138: 1175-183

Volume
Pressure
Zone of Overdistention
Barotrauma Alveolar stretch
Safe
window
Zone of
Derecruitment and
atelectasis
HFOV
CMV
To target “injury
free” zone
Epithelial injury
Pulmonary edema
Biotrauma

Slutsky & Drazen NEJM 347: 630-1
Pillow JJ et al CCM 33(Supp): S135-141

Premature <30wks RDS HFOV vs PSV/VG
• PRCT n=25
• Pre surfactant, 6-18hrs, 1-2d, pre-extubation
bronchial measurements of IL-1β, IL-8, IL-10
• Lower levels in HFOV group
HFOV associated reduction in lung
inflammation in preterms RDS vs PSV/VG
Dani C et al Paed Pulmono 41(3) 242-49

HFOV as rescue therapy Recruitment before HFOV
Improve oxygen indices
HFOV vs CMV with crossover to HFOV PRCT N=70 DAD
Open lung concept
Less O2 supp at 30d in HFOV group
Survival poorer in crossover to HFOV group
Arnold JH et al CCM 22: 1530-9
Arnold JH et al CCM 21: 272-8
Rosenberg RB et al Chest 104: 1216-21

Retrospective ARDS post CS
• Exclude uncorrected shunt
• Failed CMV
• N=84 ARDS N=64 HFOV
• OI <13 Pplat >28 pH <7.2 CMV 11d
• OI improved
More in survivors
• 40% mortality
MOF
Respiratory failure
Shengli L et al Pediatr Cardio 34: 1382-8

Retrospective n=23 Age 10yr+/-10yrs
• Mean OI 36 P/F 109
• Started 4.7d postburn CMV
• Improve oxygenation
OI & P/F may take up to 24h
Inhalational injury poor response
Responders n=16 non responders n=5
P/F 207 vs 78 (responder improve by D3)
TBSA 68 vs 42%
Mortality 29% (responder 60% non responder 20%)
Greathouse ST et al J Burns Care Res 33:425-35

AHRF
HFOV;CMV;+iNO
P/F in HFOV+iNO
better at T4 T8hrs
24hr HFOV gp better
oxygenation cf CMV
PPHN n=205
Failed CMV+iNO &
HFOV
• Started on HFOV+iNO
Kinsella JP et al J Pediatr 131: 55-62 Dobyns EL et al CCM 30: 2425

Retrospective observational study n=53
single center
• DAD, SAD
Rescue therapy HFOV • Noted higher OI in DAD >35
Survival 56% DAD 88% SAD Overall 64%
Slee-Wijffels FY et al Crit Care 9(3): R274-9

• N= 23 adult ARDS
(pneumonia, burn, BMT)
• Apache 21=/- 7 LIS 3.4+/-0.6
• Rescue HFOV failing CMV
• PIP (cmH2O) 37 + 4
• Paw 24 + 3
• PEEP 13.8 + 2.4
• PaO2/FiO2 (mm Hg) 100 + 41
• OI 33 + 20
• Outcomes
• ICU Survival 7/23 (30%)
• Burns 0/5
• 11 withdraw, 2 technicla
problems
• Nonburn patients 7/17 (41%)
• Prior Vent Days 6.1 + 5.6
days
– Non Survivors 7.8 + 5.8 days
– Survivors 1.6 + 1.2 days
Mehta et al. CCM 2001;1360-1369

• Prospective observational N=156
• Severe ARDS (P/F 91 +/- 48) Mean OI 31)
• Improvement in oxygen indices
• Almost quarter HFOV discontinued
• 22% pneumothroax
• 62% mortality
• Predictors Age, APACHE
pH at initiation
Duration of CMV
Mehta S et al Chest 126: 518-27

Use of HFOV paeds AHRF rescue failed
CMV
• PCT n=20 (pneumonia, sepsis, poisoning, pul
edema)
• Alv-artO2 578torr OI 26
• CMV 15.5hr (3.3=/-43hr)
• Improved FiO2 and PCO2 1hr to 24 hr
• Alv-artO2 and OI improve 1,4,12 hr
• 75% survival
Jaballah NB et al PCCM 7(4):362-367

• N=10 severe paeds ARDS (P/F 200) DAD with
sepsis
• CMV 7ml/kg Pplat < 30cmH2O
• Permissive Hypercapnia
• OI 13-35 (median 15)
• Duration of CMV 3-48hrs (median 4 hrs)
• Open lung concept with recruitment
• 80% survival
Jaballah NB et al Eur J Paed 164: 17-21

HFOV (recruitment) vs PCV (6-10ml/kg) MOAT PRCT MCT early ARDS (P/F = 200 PEEP 10)
HFOV Paw 45 cmH2O Dp 90 Hz 3-5
Use open lung strategies and permissive hypercapnia
Convert to CMV Paw 24cmH2O FiO2 0.5 SaO2 88%
Improve oxygen indices on HFOV
Survivors predicted by improving OI over 72hrs
30d mortality 52% (CMV) vs 37% (HFOV)
Concerns Safety study and not powered for difference
Days on CV pre HFO (2.7+/-2.7) vs PCV (4.4d+/-7.8)
Vt PCV 10.2ml/kg IBW and Pplat 38+/-8 cmH2O
Derak S et al AJRCCM 166: 801-8

PRCT crossover HFOV vs CV Vt 8-9ml/kg
N=61 adult ARDS (stop 3yrs)
No difference in mortality and morbidity
• Post hoc benefit sicker patients (higher OI) on
HFOV
Bollen CW et al Crit Care 9: R430-39

Prone positioning
• N=43 adult ARDS Prospective Comparative
Lung protective CMV 12hrs prone, then 12hr supine
Lung protective CMV 12hrs supine, then HFOV supine
12hr
Lung protective CMV 12hrs prone, then HFOV supine
12hr
• P/F and intrapulmonary shunt better in last gp
• HFOV maintained benefits of PP when patient
supine
Demory Didier et al CCM 35(1): 106-11

Tracheal gas insufflations improve
alveolar ventilation in HFOV
• PR crossover trial n=14 ARDS <3d OI 23
• HFOV with TGI (6l/min 1hr) and without 1hr for
1d
Session revered for 1d and 4 RM
CMV ARDSNet before and after HFOV sessions
• HFO-TGI better P/F , OI, intrapulmonary shunt
and mixed venous
• Haemodynamics, respiratory mechanics
unchanged Mentzelopoulos S et al CCM 35(6): 1500-8

RCT HFOV, CMV with iNO
n=108 pediatric AHRF HFOV plus iNO (n=14) HFOV alone (n=12)
CMV plus iNO (n=35) CMV alone (n=38)
Posthoc P/F ratio greatest in the HFOV plus iNO at 4
and 12 hrs
• HFOV plus iNO and HFOV gp greater P/F ratio
improvement at 24hrs
• Lung recruitment by HFOV enhances
iNO effects
Dobyns et al CCM 2002;30(11):2425

Type Piston Diaphragm – Magnet-
Coil Spinning Jet
Ventilator New Calliopeα VIASYS / Drager/
Sensor Medics SLE
Features
Oscillation created by a piston from the expiratory side.
Easy HFO settings. All parameters are independent.
Amplitude can be finely set by changing stroke volume in increments as small as 0.2ml.
PCV and PSV available.
Easy sterilization by detaching piston unit.
● Oscillation source is a speaker system.
● Weaker power.
● Oscillation wave becomes mixed with noise, unstable.
● Parameters cannot be set independently.
● Oscillation source from a jet flow with a spinning valve at the expiratory port.
● Weaker power.
● Settings cannot be set independently.
● It is likely to be affected by the compliance of the breathing circuit.

HFO Setting
Ventilator Calliopeα Babylog Stephanie SM3100A SLE5000 SLE2000HFO
Ventilation Mode
HFO, IMV, CPAP
CPAP+HFO, IMV+HFO
CPAP+HFO, IMV+HFO HFO
CPAP+HFO, IMV+HFO,
HFO
CPAP+HFO, IMV+HFO
MAP 3~40 cm
H2O 5~25cmH2O 0~35mbar
3 ~ 45 cm H2O 0~35cmH2O 0~40cmH2O
Frequency 5~17Hz 5~20Hz 5~15Hz 3 ~ 15Hz 3~20Hz 3~20Hz
Stroke volume 0~80 ml x x % x x
SI Manual ○ ○ x x x


VILI is major concern in ARDS/ALI
• HFOV would be ideal
Studies suggesting benefit esp early use
Outcome studies disappointing
Adjunct uses

To adjust HFOV, which machines to use
How to apply early – Who are responders?
Lung protective strategy in HFOV
• Recruitment
What is best surrogate marker
• OI, P/F? Role of adjuncts therapies
• Aerosols, iNO
Time for new ventilator?
OSCILLATE – Canadian Critical Care Trials Group

Understand the unique features and
benefits of „new‟ modes of ventilation in
relation to patient lung disease and
targets
No „Ideal‟ mode of ventilation
Combination of modes use
Outcome studies ?realistic


Compare weaning of infant recovering
from ARDS treated with HFOV
• N=10 NAVA & n=20 PSV historical control
• NAVA
Lower HR & MAP ? Comfortable
P/F decreased less
Lower PCO2 Ppeak Higher MV
COMFORT score better
Piastra M et al PCCM 15(4S) no 47

Retrospective ARHC SCT n=31 burns
• Failed CMV (HFOV 3; PC-CMV 15; PRVC 16)
1d OI 18.7 P/F 131.5
• Lower Ppk similar MAP post HFPV for 48h
OI 18.7 11/7 12h
PCO2 8455 6h
MAP 3830
• Airleak Haemodynamic Vasopressor unchanged
• Ventilated mean 4d
• Mortality 16.1%
• N=3 failed HFPV for P-V dyssynchrony
HFOV 1 ECMO 2 Rizkalla NA et al J Crit Care 314: e1-7

N=64 paediatric burn SCT
• CMV or HFPV
• Improved oxygenation at lower Ppk
• Mortality ARDS evolution sepsis not different
Used in adult and children smoke
inhalational and polytrauma
Carman B et al J Burn Care Rehabil 23: 444-8
Salim A et al CCM 33(3S): S241-5
Cioff Jr WG et al Ann Surg 213: 575-80
Cortiella J et al J Burn Care Rehabil 20: 232-5
Rue III RW et al Ann Surg 128: 772-8
Reper P et al Burns 28: 503-8

Retropsective n=60 early ARF SCT
• CMV; NIPPV; BCV
• Oxygenation, Ventilation & vital signs improve in
all 3 groups
• Duration CMV 182.3h; NIPPV 80.hd; BCV 64.2h
• LOS 17.7d CMV; 19d NIPPV; 10d BCV