Embed Size (px)
Citation preview

25
Chapter 2
Long-Term Care Policy: Past, Present, and Future
What You Will Learn
• Public policy can take many different forms and can come from dif-ferent governmental sources.
• There is no single process or model that can describe how policiesare made, except that legislative policymaking follows a well-defined process.
• Policies do not always achieve their intended objectives and sometimesproduce unintended side effects that can be positive or negative.
• In the United States, long-term care policy and general welfare havebeen closely intertwined. The Social Security Act of 1935 and thecreation of Medicare and Medicaid in 1965 were landmark policiesthat indirectly started the nursing home industry. Regulation of theindustry soon followed.
• Quality of care issues in nursing homes took center stage during the1980s. The Nursing Home Reform Act of 1987 provides currentnursing home regulations dealing with patient care, but the regula-tions also have some serious drawbacks.
• Most of the current activity in long-term care policy is at the statelevel. Community-based services and purchase of private insuranceare receiving various degrees of state-level attention.
• The complex interaction of financing, access, utilization, and ex-penditures is critical to current and future long-term care policy.
• Future policy initiatives are necessary in the areas of prevention, fi-nancing, workforce development, health information systems, men-tal health, and evidence-based practices.
74035_CH02_5368.qxd 8/4/09 9:43 AM Page 25
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION

Policy OverviewLong-term care (LTC) policy is specificallycrafted to address issues pertaining to access,financing, delivery, quality, and efficiencyof LTC services. Long-term care policy is asubset of broader health policies that fallwithin the domain of public policy.
Public policy refers to decisions madeand actions taken by the government that areintended to address current and potential is-sues that the government believes are in thebest interest of the public. As with other typesof decisions, policy is intended to accom-plish certain defined purposes. However, theintended objectives of public policy are notalways achieved. On the other hand, publicpolicy can produce some unintended conse-quences, even though such unintended re-sults are not always bad.
When the intended goals of public policypertain to health care, the government’s de-cisions and actions are referred to as healthpolicy. Health policies pertain to health carein all aspects, including production, delivery,and financing of health care services. Healthpolicies affect groups or classes of individu-als, such as physicians, the poor, the elderly,or children. They can also affect various typesof organizations, such as medical schools,managed care organizations, nursing homes,manufacturers of medical technology, oremployers in the American industry. Healthpolicy can have a major effect on access toservices, shifts in utilization, market compe-tition, availability of an adequate and quali-fied workforce, and development and use oftechnology.
Long-term care policies particularly af-fect the recipients of services such as the el-derly or disabled; provider organizations suchas nursing homes, home health agencies, and
senior centers; caregivers such as physiciansand certified nursing assistants; managerssuch as nursing home administrators; manu-facturers and purveyors of technology andmedical supplies; and, sometimes, potentialconsumers of long-term care. For example,favorable tax policies adopted by many statesare intended to provide financial incentives sothat more consumers can buy long-term careinsurance to enable them to cover high LTCexpenses later on. However, research showsthat tax incentives have not induced the pur-chase of LTC insurance any more than otherfactors such as income, health status, andfamily support (Nixon, 2007). This is one ex-ample in which public policy may not producethe intended effects.
The term policy is sometimes also usedin the context of private policy. More ap-propriately, however, private policies arestrategic decisions that various private or-ganizations make to better serve their mar-kets. In the health care sector, public policy isoften an important consideration when pri-vate organizations make strategic decisions.For example, a strategic decision by a skillednursing facility to convert some of its bedsto deliver subacute care may be driven by apublic policy to increase reimbursement forsubacute care. This would be an importantconsideration in addition to market demandfactors.
Forms and Sources of PolicyCommonly, policy takes the form of lawspassed by legislative bodies such as the U.S.Congress or state legislatures. Administra-tive bodies, such as the Centers for Medicareand Medicaid Services (CMS) or state healthboards, interpret the legislation and formu-late rules and regulations to implement thelaws. In the process of interpretation and im-
26 CHAPTER 2 • Long-Term Care Policy: Past, Present, and Future
74035_CH02_5368.qxd 8/4/09 9:43 AM Page 26
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION

plementation, the administrative bodies alsoend up creating public policy. The term poli-cymakers is generally applied to legislatorsand decision makers in regulatory agencieswho become actively involved in craftinglaws and regulations to address health careissues. The two sources of policymakingjust mentioned are the most common. Lessfrequently, certain decisions rendered by thecourts and executive orders issued by thePresident of the United States or state gover-nors also become public policy. The presidentoften plays an important role in policymakingby generating support of his agenda in Con-gress, by appealing to the American people asto why certain issues are important, and byproposing legislation. Hence, all three branch-es of government—legislative, judicial, andexecutive—can make policy. The executiveand legislative branches can establish healthpolicies; the judicial branch can uphold, strikedown, or modify existing laws affectinghealth and health care. Examples in all threeareas follow. (1) Legislation contained inthe Balanced Budget Act of 1997 requiredMedicare to develop a prospective paymentsystem (PPS) to reimburse skilled nursingfacilities. This legislative policy triggeredseveral rounds of policymaking. First, theHealth Care Financing Administration (nowcalled Centers for Medicare and MedicaidServices) developed and implemented a newpayment methodology in 1998. Subsequently,to address concerns from nursing home op-erators, Congress instituted a series of tem-porary payment increases through two piecesof legislation—the Balanced Budget Refine-ment Act of 1999 and the Medicare, Medic-aid, and SCHIP Benefits Improvement andProtection Act of 2000 (MedPAC, 2002). (2)A 1999 decision by the U.S. Supreme Courtin Olmstead v. L.C. directed states to providecommunity-based services for persons with
disabilities—including persons with devel-opmental disabilities, persons with physicaldisabilities, persons with mental illness, andthe elderly—when such services were deter-mined to be appropriate by professionals re-sponsible for rendering health care to thesepeople. (3) The 2004 Executive Order 13335provided incentives for the use of health in-formation technology (HIT) and establishedthe position of a National Health InformationTechnology Coordinator. One of the mainobjectives of this executive order was to de-velop a nationwide HIT infrastructure thatwould allow a patient’s electronic healthrecords to be portable and available to dif-ferent health care providers (i.e., make elec-tronic health records interoperable). The LTCprofession has been actively participating toensure that it is included in this national pol-icy. These examples also illustrate that pub-lic policy can take many different forms thatcan have far-reaching consequences. Whenpolicies require that certain individuals or or-ganizations perform or behave in a certainmanner, the policies carry the force of law.Violations can result in various kinds ofpenalties that can include monetary fines, ex-pulsion from participation in public programs,and prison terms for criminal offences.
Health policy may be made at the nation-al, state, or local level of government. For ex-ample, national building and fire safety codesgovern the construction, design, and safetyfeatures for LTC facilities. State policies gov-ern licensure of facilities and health care pro-fessionals. States also establish guidelines thatinsurance companies must follow in the de-sign and sale of LTC insurance. Local gov-ernments establish zoning laws specifyingwhere LTC facilities may be built. Local gov-ernments may also decide on the availabilityof certain community-based services on thebasis of budget constraints.
Policy Overview 27
74035_CH02_5368.qxd 8/4/09 9:43 AM Page 27
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION

PolicymakingThere is no single process or model that candescribe how policies are made because thereare different sources of policy. Hence, poli-cymaking is difficult to describe, and theprocess can be obscure (Cockrel, 1997). Onthe other hand, policymaking does not occurin a vacuum. In a representative democracy,the policymaking process must insure thatall relevant viewpoints are heard and that therights of individuals are protected. The largerand more diverse the constituency, the moredifficult policymaking becomes (MRSC,1999).
The formation and implementation oflegislative policy generally occurs in a policycycle that has six main stages: (1) issue rais-ing, (2) policy design, (3) building of publicsupport, (4) building of policy support, (5)legislative decision making, and (6) policyimplementation. The enactment of a new pol-icy is generally preceded by a variety of ac-tions that first create a widespread sense thata problem exists and that it must be addressed.The actions are intended to bring issues to theforefront with some degree of importance andurgency. At the second stage, specific poli-cy proposals are designed in the form of abill, which is simply a proposed piece oflegislation. If the bill is crafted at the federallevel, the proposal is reviewed by variouscommittees and subcommittees in Congress.Amendments may be added. At the thirdstage, to build public support, policy propos-als are sent to organizations and interestgroups that may be affected by them. In-terest groups are an organized sector ofsociety—such as a business association, cit-izen group, labor union, or professionalassociation—whose main purpose is to pro-tect its members’ interests through activeparticipation in the policymaking process.
Hearings are held and testimonies, both infavor of and in opposition to the proposedpolicy, are given by citizens, business repre-sentatives, labor groups, interest groups, pro-fessional associations, and experts in thefield. At the fourth stage, internal support ofthe policy becomes critical for it to pass. In-fluential members of Congress meet withmembers of their own party, influential lead-ers from the opposition, and with the presi-dent in an effort to gain support. At the fifthstage, the issues are debated on the congres-sional floor. In the end, a majority vote isneeded, and subsequently the bill becomeslaw if the president signs it. At the sixth stage,once legislation has been signed into law, it isforwarded to the appropriate administrativeagency, such as the CMS, for implementa-tion. The agency publishes proposed regula-tions in the Federal Register and holdshearings on how the law would be imple-mented.
Policymaking can be triggered by eventssuch as natural disasters, growing socialproblems such as crime, severe economicshocks such as the Great Depression (start-ed in 1929 and ended in the late 1930s), in-creasing burden on taxpayers such as therising cost of health care services, demandfrom consumers such as product safety, etc.For example, the Social Security Act of 1935was passed during the Great Depression.Widely reported events such as fires and cas-es of food poisoning in nursing homes dur-ing the early 1970s prompted developmentof nursing home regulations in 1974.
Policy and PoliticsPolicymaking and politics are often closelyintertwined because most policymakers arepoliticians. The danger is that policymakingoften becomes highly politicized and be-
28 CHAPTER 2 • Long-Term Care Policy: Past, Present, and Future
74035_CH02_5368.qxd 8/4/09 9:43 AM Page 28
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION

comes hostage to the ideologies of a politi-cal party. The primary concern of politiciansis to get elected or reelected. Hence, certainpublic policies are driven by the desire tokeep campaign promises or to please somepowerful constituent group. For example,politicians pay attention to powerful organi-zations, such as the AARP, that represent thegrowing population of the elderly. It was inthis political context that the Medicare Pre-scription Drug, Improvement, and Modern-ization Act of 2003 was passed. Going againstthe wishes of the elderly would have beenpolitical suicide for some.
The policy-for-politics approach gener-ally does not ask for or consider the cost ben-efit of a proposed policy. It is pushed throughmainly for ensuring votes. For example, noone cared to inquire what impact the newprescription drug program would have on re-ducing future disability among the elderly.
Long-Term Care Policy: HistoricalPerspectivesPolicy evolution in the United States did notprogress according to some planned design.This follows the general pattern of Ameri-can health policymaking. Health care poli-cymaking has followed an ad hoc approachto incrementally address issues as they havecropped up.
Welfare Policies and Long-Term CareThe history of LTC policy in the United Statesgoes back to the building of poorhouses (oralmshouses) in the late 17th century. A poor-house was a government-operated institutionduring colonial and post-colonial times wherethe destitute of society, including the elder-
ly, the homeless, the orphan, the ill, and thedisabled, were given food and shelter, andconditions were often squalid. The first poor-house in the United States is recorded to haveopened in 1660 in Boston (Wagner, 2005, p.10). The poorhouse program was adoptedfrom the Elizabethan system of public char-ity based on English Poor Laws. In the Unit-ed States, cities, counties, and states operatedthese facilities, which were often located onfarms and, hence, referred to as poor farms.The poorhouses were part of a very limitedpublic relief system that was financed main-ly by local governments. These facilities ad-mitted poor and needy persons of all kinds,including those released from prison, and theill who did not have family or relatives to takecare of them. In response to the growing con-cerns about abuse and squalid living condi-tions, some states created state-run Boardsof Charities in the mid-1800s to oversee andreport on the local poorhouse operations. TheBoards’ efforts led to some improvement inliving conditions and to separation of the in-sane from the sane and the dependent elder-ly from the able bodied (Stevenson, 2007).The tireless efforts of Dorothea Lynde Dix(1802–1887), a social reformer, were partic-ularly instrumental in convincing Massa-chusetts’ legislature to pass laws that wouldput the mentally ill in separate facilities.These reform efforts spread to other statesand even abroad to Canada and Europe.
Passage of the Social Security Act in1935 was a landmark piece of legislation. Theelderly were particularly hard hit during theGreat Depression as many of them saw theirlifetime savings disappear. Hence, the feder-al government specifically addressed theneeds of America’s elderly. Simultaneously,deplorable conditions in the poorhouses fu-eled a reform movement that favored com-munity-based care over institutionalization.
Long-Term Care Policy: Historical Perspectives 29
74035_CH02_5368.qxd 8/4/09 9:43 AM Page 29
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION

An Old Age Assistance (OAA) program wasincluded in the Social Security Act. Howev-er, instead of providing direct community-based services, the OAA program madefederal money available to the states to pro-vide financial assistance to needy elderlypersons. The Social Security program, eventhough it left out a relatively large numberof Americans (including many elderly anddisabled people) was instrumental in puttingan end to the poorhouse system (Wagner,2005, pp. 132–133). For the fiscal year thatended on June 30, 1936, Congress authorizedthe sum of $49,750,000 under Title I of theAct in the form of matching grants, mean-ing the states participating in the programwould share in the total cost of the program(Social Security Administration, undated).Prior to this, several states had their own oldage assistance programs. The new law pur-posely prohibited payments to anyone livingin a public institution (i.e., a poorhouse). Anunintended side effect of this policy was thatit started a private nursing home industry inthe United States because many elderly nowwere able to pay for services in homes for theaged and boarding homes (Eustis et al.,1984, p. 17).
The Hospital Survey and ConstructionAct of 1946, commonly known as the Hill-Burton Act, provided federal funds to statesfor the construction of new hospital beds. Anunplanned result of the Hill-Burton legisla-tion was that many of the old hospitals thatwere being replaced were converted to nurs-ing homes (Stevenson, 2007).
Policies during the 1950s provided fed-eral funds for the construction of nursinghomes while, at the same time, OAA pay-ments were increased, and a 1950 Social Se-curity Amendment required payments formedical care to be made directly to nursing
homes rather than to the recipients of care.Nursing homes could now contract directlywith the state governments and get reim-bursed for services delivered to the elderlypoor. Also, at this time, nursing homes wererequired to be licensed by the states. The leg-islation contained no specific standards forlicensure; hence, each state set its own stan-dards (Phillips, 1996).
Financing and Growth of Nursing HomesThe creation of Medicare and Medicaid in1965 as Title 18 and Title 19 amendments,respectively, to the Social Security Actbrought about the most transforming changeson the American health care landscape.Medicare and Medicaid are two major publicinsurance programs. Medicare covers healthcare services for the elderly, certain disabledpeople, and those who have end-stage renaldisease (kidney failure). Medicaid covershealth care services for the poor. These pro-grams are more fully discussed in Chapter 7.
With the creation of Medicare and Med-icaid, LTC became a part of the health caredelivery system in the United States. Also,the federal and state governments becamethe largest payers for LTC services, and thepolitics of long-term nursing home care tookroots. Medicare and Medicaid funding fornursing homes also attracted Wall Street in-vestors and real estate developers to a fast-growing nursing home industry dominatedby chains—that is, multifacility systems thatown and operate nursing homes in severalstates (Hawes et al., 2007). Medicare andMedicaid policies favored payments to nurs-ing homes that lawmakers could regulaterather than payments for community-basedservices that would be difficult to regulate.These policies led to the institutionalization
30 CHAPTER 2 • Long-Term Care Policy: Past, Present, and Future
74035_CH02_5368.qxd 8/4/09 9:43 AM Page 30
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION

of a large number of people, many of whomdid not belong in nursing homes.
Nursing home utilization and governmentexpenditures exploded shortly after Medicareand Medicaid went into effect. The massiveinfusion of dollars into the nursing home in-dustry, which had already acquired a tar-nished image, prompted regulations to holdindividual nursing homes accountable formeeting minimum standards of care. In 1968,Congress passed legislation, commonlyknown as the Moss Amendments (named af-ter Senator Frank Moss), that paved the wayfor comprehensive regulations to improvecare in the nation’s nursing homes. It was notuntil 1974, however, that final regulations forskilled nursing facilities were promulgated,and their enforcement began in earnest. Com-pliance with standards such as staffing levels,staff qualifications, fire safety, and deliveryof services now became a requirement forparticipation in the Medicare and Medicaidprograms. Later, these regulations were wide-ly criticized that they concentrated on a facil-ity’s capacity to give care, not on the qualityof services actually delivered (DHEW, 1975).
Interestingly, licensing of health careprofessionals and hospitals was initiated bythe professionals themselves and by the in-stitutional providers, respectively. In contrast,licensing of nursing homes and of nursinghome administrators (NHAs) came aboutthrough federal laws. As mentioned earlier,the 1950 amendments to the Social SecurityAct required that states license nursing homesin order to participate in the OAA program.Licensing of NHAs was a major exception tothe general trend of requests from profes-sionals that anyone practicing in their respec-tive professions be licensed. The demand forqualified persons to manage nursing homeswas not initiated by the industry, but came
about as a result of public outcry over fraudand abuse. As a result, the 1967 amendmentsto the Social Security Act included a provi-sion that, for states to participate in theMedicaid program, they had to pass laws togovern the licensing of NHAs. In contrast,hospital administrators were not required tobe licensed. One key characteristic of licen-sure is that it is a responsibility of each state,not the federal government. Licensure by thestate permits an institution to begin and con-tinue operations and health care profession-als to begin and continue to practice (Eustiset al., 1984, pp. 143–145).
Financing of Community-Based ServicesSocial Security amendments in 1974 autho-rized federal grants to states for various typesof social services. These programs includedprotective services, homemaker services,transportation services, adult day care, train-ing for employment, information and referral,nutrition assistance, and health support (Lee,2004). The Social Security Amendment of1975 created Title 20, which consolidated thefederal assistance to states for social servicesinto a single grant. Under Title 20, one of thegoals for the states was to prevent or reduce“inappropriate institutional care by providingfor community-based care, home-based care,or other forms of less intensive care.”1 In1981, Title 20 was amended to create SocialServices Block Grants. The single blockgrants actually reduced federal funding to thestates for social services. Also, Title 20 cov-ered services for all ages, not just the elderly.Consequently, block grants have provided rel-atively little money for LTC services.
Long-Term Care Policy: Historical Perspectives 31
1Title XX appears in the United States Code as §§1397-1397f, subchapter XX, chapter 7, Title 42.
74035_CH02_5368.qxd 8/4/09 9:43 AM Page 31
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION

Also in 1981, the Home and CommunityBased Services waiver program was enactedunder Section 1915(c) of the Social SecurityAct. The 1915(c) waivers, as they are com-monly referred to, allow states to offer LTCservices that are not otherwise availablethrough the Medicaid program, which hadauthorized payments for institutional careonly. The waivers have been particularly suc-cessful, and states have increasingly usedthem to expand community-based LTC ser-vices, thus saving money on institutionalcare. Today, all states provide waiver servicesto the elderly, working-age people with dis-abilities, and those with developmental dis-abilities. Some states also serve people withAIDS and those with serious mental healthproblems (Miller et al., 2006). Between 1987and 1997, spending on waiver programssoared from $451 million to $8.1 billion(Coleman, 1999), an increase of 1,696%. By2006, there were 329 waivers, and the ex-penditures amounted to $25.6 billion in stateand federal Medicaid dollars (Acosta & Hen-drickson, 2008).
Deregulation AvertedIn the early 1980s, nursing home regulationscame under the broader sweep to deregulateindustry and downsize the federal bureaucra-cy. Rumors leaked out that a task force onregulatory reform in the Reagan adminis-tration was planning to downgrade sanita-tion standards, eliminate staff developmentrequirements, reduce physician visits, deletemedical director requirements, reduce socialwork programs, and ignore certain staff qual-ifications (Trocchio, 1984). Various interestgroups such as consumer advocates and pro-fessional associations representing medicaldirectors, social workers, and activity per-sonnel lobbied Congress. In the end, interest
group politics and congressional oppositionderailed any attempts to deregulate the nurs-ing home industry.
Efforts to Address Quality IssuesThe nursing home industry remained fraughtwith scandals about severely substandardquality of care and an ineffective regulatorysystem to enforce compliance with standards.At the request of Congress, the Institute ofMedicine (IOM) conducted a comprehensivestudy that culminated in a scathing report onthe state of nursing homes in the UnitedStates. The study found that residents of nurs-ing homes were being abused, neglected, andgiven inadequate care. Sweeping reformswere proposed (IOM, 1986). The IOM’s pres-tige lent scientific credibility to its recom-mendations, and the report triggered the mostcomprehensive revision of the federal stan-dards, inspection process, and enforcementsystem for nursing homes since the creationof Medicare and Medicaid in 1965 (Hawes etal., 2007). National organizations represent-ing consumers, nursing homes, and healthcare professionals worked together to createconsensus positions on major nursing homeissues and supported them before Congress.Their consensus positions on most IOM rec-ommendations laid the foundation for a newfederal law (Turnham, 2001). Although theIOM report has been widely credited to bethe impetus for the Nursing Home ReformAct of 1987, it has also been observed that theEstate of Smith v. Heckler (1984) class-actionlawsuit in Colorado may have played a role.The suit was brought on behalf of all theMedicaid beneficiaries in the state’s nursinghomes. In essence, the suit charged that theconstitutional rights of the nursing home res-idents were violated because the federal andstate governments failed to enforce its laws
32 CHAPTER 2 • Long-Term Care Policy: Past, Present, and Future
74035_CH02_5368.qxd 8/4/09 9:43 AM Page 32
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION

and regulations. The district court judge,Richard T. Matsch, ruled against the plain-tiffs, but his decision was later overturnedon appeal. The appeals court ruled that theSecretary of the Department of Health andHuman Services (DHHS) did have a duty toestablish a system that could determinewhether a nursing facility was providing thehigh-quality care required by the Social Se-curity Act (Phillips, 1996, pp. 10–14).
In 1987, President Reagan signed intolaw the Omnibus Budget ReconciliationAct of 1987 (OBRA-87), which containedthe Nursing Home Reform Act. OBRA-87brought enormous changes to nursing homeoperations. The most important provisions ofthe law are summarized (Castle, 2001; Turn-ham, 2001) as follows:
• Emphasis on a resident’s quality of lifeas well as quality of care.
• New expectations that each resident’sability to walk, bathe, and perform oth-er activities of daily living will be main-tained or improved absent medicalreasons.
• A resident assessment process leading todevelopment of an individualized careplan.
• 75 hours of training and testing of para-professional staff, such as nursingassistants.
• Right to remain in the nursing home ab-sent nonpayment, dangerous resident be-haviors, or significant changes in aresident’s medical condition.
• New opportunities for services insideand outside a nursing home to addressthe needs of residents with mental retar-dation or mental illnesses.
• Right to safely maintain or bank person-al funds with the nursing home.
• Right to return to the nursing home af-ter a hospital stay or an overnight visitwith family and friends.
• Right to choose a personal physician andto access medical records.
• Right to organize and participate in aresident or family council.
• Access to an ombudsman to resolve dis-putes and grievances.
• Right to be free of unnecessary and in-appropriate physical and chemicalrestraints.
• New remedies to be applied to certifiednursing homes that fail to meet mini-mum federal standards.
OBRA-87 also changed the way state in-spectors approached nursing home inspec-tions. Inspectors were to no longer spendtheir time exclusively with staff or with fa-cility records, as was the case in the past.Conversations with residents and familiesand observation of dining and medication ad-ministration became critical steps in the in-spection process (Turnham, 2001).
Ironically, OBRA-87 reforms were near-ly repealed in 1995 as part of a larger attemptto reform Medicaid. This time, part of thenursing home industry supported repeal of theOBRA reforms, particularly the enforcementprovisions. But consumer advocates, aided byresearchers, were able to use empirical evi-dence about the positive effects of OBRA pro-visions to effectively oppose the dilution offederal regulations. Once consumer advocatesredefined the issue as one of quality of care,Congress opposed the repeal of the NursingHome Reform Act (Hawes et al., 2007).
OBRA-87 altered the regulatory land-scape in a significant way. Even though sub-stantial funds were allocated to carry outthe legislative mandate, it was a complex
Long-Term Care Policy: Historical Perspectives 33
74035_CH02_5368.qxd 8/4/09 9:43 AM Page 33
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION

piece of legislation, and numerous hurdleswere encountered in developing regulations.The final rules were published at the end of1994 to be effective in July 1995, more thaneight years after the law had been passed(Phillips, 1996, p. 35).
Oversight for Other ServicesIt is interesting to note that while the nursinghome industry has been under the spotlightfrom federal policymakers for more than halfa century now, the same policymakers haveshown little interest in the assisted living in-dustry. The latter has been one of the fastestgrowing areas of LTC delivery in recent years,and the aging-in-place philosophy has raisedthe level of clinical acuity of residents inthese facilities. The absence of direct feder-al reimbursement to assisted living facilitiesis perhaps the reason any federal regulatoryoversight is unlikely, unless at some pointcrises and failure of care similar to those en-countered during the long history of nursinghomes become apparent (Edelman, 2003).Most regulatory efforts for assisted living fa-cilities have occurred at the state level. Sim-ilar variations in state regulations exist foradult day care centers. Medicaid-funded adultday care services must meet applicable statelicensing and regulatory requirements suchas minimum staff-to-participant ratios. Themajority of states have instituted inspections(O’Keeffe & Siebenaler, 2006).
A 1988 court ruling on a class-actionlawsuit, Duggan v. Bowen, opened up broadaccess to Medicare-covered home health ser-vices, and for some time, home health had be-come the fastest growing health care servicein the United States. In August 1997, Con-gress enacted the Balanced Budget Act (BBA)of 1997, which mandated that Medicare’scost-based, retrospective reimbursement pol-
icy for home health agencies as well as skillednursing facilities be replaced by a prospectivepayment system (PPS). This policy was partof a broader financial reform to slow downthe growth of Medicare spending. A prospec-tive reimbursement method for skilled nurs-ing facilities was implemented in July 1998and a home health PPS reimbursement wasimplemented in October 2000.
Current State of Long-Term Care PolicyThe national stage for LTC policy has beenlargely silent as other pressing issues preoc-cupy politicians. Long-term care is not ex-pected to see any major changes in the nearfuture. States, on the other hand, continue toforge incremental policy initiatives to expandthe purchase of private LTC insurance andreduce the level of institutional care in favorof community-based services. Both initiativesare intended to curtail the states’ burden ofnursing home expenditures and to save mon-ey overall in the LTC delivery system. A thirdarea of state-level policymaking encompass-es ongoing efforts to license alternative hous-ing and care facilities. As pointed out inChapter 1, the institutional continuum of LTCincludes various types of living and carearrangements other than traditional nursinghomes.
Public policy in long-term care hasevolved in three main directions: financing,utilization, and quality. Almost all health carepolicy can be classified into these categories.
Financing, access, and utilization go handin hand. Utilization is the actual use of healthcare occurs when people needing serviceshave access to them. Access is the ability of aperson needing services to obtain those ser-vices. Two main factors drive access: financ-ing and availability of services. If financing
34 CHAPTER 2 • Long-Term Care Policy: Past, Present, and Future
74035_CH02_5368.qxd 8/4/09 9:43 AM Page 34
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION

(i.e., the ability to pay for services) is ade-quate but availability is limited, the servicesget rationed and access is restricted. On theother hand, if services are available but fi-nancing is not, access becomes restricted forthose who cannot afford the services. Also,increased utilization negatively affects fi-nancing. Increased utilization makes totalexpenditures rise, and financing becomesconstrained.
FinancingFinancing is the means by which patients payfor the services they receive. Financing variesby the type of service, and there can be dif-ferent sources of financing even for the sameservice. For example, care in a skilled nursingfacility can be financed through Medicaid,Medicare, private insurance, Veterans HealthAdministration, or one’s own personal funds.Hence, LTC financing is quite fragmentedbecause no single source can be tapped on topay for services. Consequently, access andutilization become uneven. People face fi-nancial obstacles in a system that is complexand nonintegrated. Complexities arise whenpeople have to move from one type of serviceto another, such as from nursing home to thecommunity or vice versa, or even when theyhave to stay within one LTC sector. For ex-ample, many who require nursing home carefor a long period of time can face a financingnightmare. Medicare pays only for post-acuteshort-term stays, and Medicaid requirespeople to exhaust their financial resourcesto become eligible. Many elders who do notqualify for either program have to pay on aprivate basis either through private LTC in-surance or out of personal savings. In 2005,44% of the financing for nursing home carewas derived from Medicaid, and only 16%came from Medicare. Private out-of-pocket
payments financed 26%, and 7% was paidthrough privately purchased LTC insurance.The remainder was paid through miscella-neous private and public sources (Kaiser,2007).
Expansion of Community-Based ServicesMedicaid remains the largest source offunding for LTC services. It finances 41%of the total spending for LTC services of alltypes. Spending on Medicaid home- andcommunity-based services (HCBS) has beengrowing, but states vary greatly in financingHCBS. In 2006, spending on HCBS account-ed for 41% ($44.9 billion) of total MedicaidLTC services spending, up from 13% in 1990(Kaiser, 2007). As mentioned earlier, law-suits such as Duggan v. Bowen and Olmsteadv. L.C. played an important role in shiftingutilization from institution-based care tocommunity-based services. More recently, theDeficit Reduction Act of 2005 provided fed-eral funding to states to expand community-based care. As part of this legislation,Congress granted $1.8 billion over five yearsfor states to provide 12 months of LTC ser-vices in a community setting to individualswho currently receive Medicaid services innursing homes (Kasper & O’Malley, 2006).This legislation may be a turning point innational LTC policy because it makes rebal-ancing between institutional and community-based services a national priority (Mor et al.,2007) under a federal–state joint initiative re-ferred to as Money Follows the Person. Underthis program, when a person transfers froma nursing home to the community, funds thathad previously paid for nursing home careare transferred to community-based servicesfor that person.
HCBC has been viewed as a potentiallymore cost-effective option than nursing home
Current State of Long-Term Care Policy 35
74035_CH02_5368.qxd 8/4/09 9:43 AM Page 35
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION

care, but research evidence remains incon-clusive that expanding community-based carelowers overall LTC spending (Grabowski,2006; Long et al., 2005). It reduces expen-ditures for nursing home services, but opensup access to HCBS for many who previouslydid not have access. On the other hand, stud-ies do show that community-based servicessignificantly improve the quality of life ofclients. People prefer less restrictive nonin-stitutional settings over services received inLTC facilities.
Reimbursement to ProvidersOther policy issues related to financingsurround the levels of reimbursement toproviders from Medicare and Medicaid. Nurs-ing home operators have long contended thatpayments from public payers have been in-adequate to support quality services. Inde-pendent experts have also voiced opinionsthat reimbursement levels should be raised.However, Medicaid and Medicare adminis-trators have been concerned about rising ex-penditures, while the public is not inclinedto pay more in taxes. The paradox is that, un-like many other industries, nursing home careis highly labor intensive because caregivershave to render services one on one. Hence,few options are available to increase produc-tivity or slash operating costs.
Incentives for Private InsuranceCoverage for nursing home care from privateLTC insurance has increased slightly in re-cent years, but fewer than 10% of people 50years of age and older have purchased privateinsurance for long-term care (Seff, 2003).The elderly population most likely to benefitfrom private LTC coverage also has a loweraverage income than the general population.
Hence, LTC insurance is difficult to marketbecause premiums must be high enough tocover costs but low enough to attract clients.Insurance is based on the principle of ade-quately spreading risk among a large segmentof the population. However, younger healthygroups have shown little interest in buyingLTC insurance because they see the need forLTC only as a remote possibility.
A few states offer tax deductions or cred-its for purchasing private insurance, but theincentives appear to be too small to inducemany people to purchase LTC plans (Wieneret al., 2000). Another state-based policy ini-tiative that is designed to increase the num-ber of middle-income people who buy privateinsurance is the Partnership for Long-TermCare program. The program was designed bythe Robert Wood Johnson Foundation, aprivate nonprofit organization, through ademonstration project in California, Con-necticut, Indiana, and New York. Currently,about half the states have implemented theprogram. The Partnership program encour-ages individuals to purchase insurance, and,if these individuals require LTC services, theycan apply for Medicaid after their insurancebenefits have been exhausted. To qualify forMedicaid, these individuals would be allowedto keep all or some of their financial assets.Otherwise, under Medicaid policy, peoplehave to first use up their income and assetsbefore they can qualify for benefits. Under thePartnership program, exceptions are made tothis rule. States have been permitted to dothis under the Deficit Reduction Act of 2005.Some experts believe that the Partnershipprogram has made progress toward meetingits goals. For example, the original four stateshave been modestly successful in promotingquality insurance products. As of mid-2006,about 240,000 Partnership insurance planshad been sold, and about 194,000 were being
36 CHAPTER 2 • Long-Term Care Policy: Past, Present, and Future
74035_CH02_5368.qxd 8/4/09 9:43 AM Page 36
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION

used to obtain services. There are critics, butthe program was not intended to be a com-prehensive solution to all LTC needs; it wasdesigned to fill a financial gap (Alliance forHealth Reform, 2007).
Another area in which progress has beenmade is information to consumers. Long-termcare, with its many service and financing op-tions, is confusing for most people. Peoplehave also assumed that the government willsomehow pay for their LTC needs. Govern-ment resources, however, have been shrink-ing and it is unlikely that public resources willbe enough to meet the needs of a burgeoningelderly population. The DHHS has created theNational Clearinghouse for Long-Term CareInformation (see For Further Learning). Thewebsite is designed to help people understandwhy planning for LTC is important and howthey can plan for it.
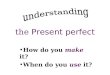
UtilizationTable 2–1 provides capacity and utilizationdata for nursing homes. During the 1990s,nursing home beds in the United States con-tinued to increase while their utilization con-
tinued to decrease. Between 2000 and 2006,both the number of nursing homes and bedsdecreased. As a result, there was some im-provement in capacity utilization as reflect-ed in the occupancy rates. On the other hand,the utilization of nursing homes by the pop-ulation, as reflected in the resident rates, hascontinued to decline at a rather dramatic rate.
During the 1980s, nursing homes enteredthe subacute and rehabilitation markets, main-ly as a result of the DRG-based (diagnosis-related group) prospective payment systemimplemented in hospitals, which created in-centives for early discharge of patients fromhospitals. The trend accelerated during the1990s because the proliferation of managedcare put further pressures on reducing thelength of stay in hospitals. While these trendsshould have increased nursing home utiliza-tion, other factors in play since the 1980s pro-moted the use of alternative settings such ashome health care, other community-basedLTC services, and assisted living facilities.
It is estimated that 5 to 12% of residentsin nursing homes require low levels of careaccording to their functional and clinical char-acteristics (Mor et al., 2007). Their needs
Current State of Long-Term Care Policy 37
Table 2–1 Nursing Home Utilization (Selected Years)
1992 1995 2000 2006
Number of nursing homes 15,846 16,389 16,886 15,899Number of beds 1,692,123 1,751,302 1,795,388 1,716,102Occupancy ratesa 86.0% 84.5% 82.4% 83.5%Resident ratesb 444.4 404.5 349.1 270.6
Sources: Data from Health, United States 1996–97, p. 248; Health, United States 2007, pp. 370–371.aPercent of beds occupied (number of residents per 100 available beds).bNumber of nursing home residents of all ages per 1,000 population 85 years of age and over.
74035_CH02_5368.qxd 8/4/09 9:43 AM Page 37
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION

could be met with appropriate community-based LTC services. However, HCBS pro-grams, being part of the state-administeredMedicaid programs, have not developed uni-formly across states. Also, states vary in theirenthusiasm for nursing home transition pro-grams. Some states, for example, have transi-tioned residents to assisted living facilitiesinstead of home- and community-basedservices. Motivation of individuals and theirfamilies and the availability of a communitysupport system to supplement formal servicesare viewed as key factors in determiningwho transitions back to the community fromnursing homes. Logistical barriers may alsohamper transitions. For example, hospital dis-charge planners find it easier to move patientsfrom the hospital to nursing homes. Arrang-ing for appropriate community-based servicesis generally time consuming and complex be-cause it requires coordination and determina-tion of how services will be financed. Otherobstacles include shortage of housing alter-natives (Mor et al., 2007) and waiting lists forcommunity-based care in some states (Kasper& O’Malley, 2006).
Some efforts are being made at the statelevel to carry out evaluations of HCBS to im-prove the programs. In the meantime, policy-makers are hesitant to broadly implementnew initiatives because they have not beenvalidated for quality and evaluated for howmuch they would end up costing (Acosta &Hendrickson, 2008).
Private paying patients have found theresidential and social lifestyles in assisted liv-ing facilities to be much more appealing thanthose in skilled nursing facilities. Many peo-ple have figured that they might as well spendtheir personal savings in an upscale assistedliving home and later apply for Medicaid ifthey need care in a skilled nursing facility.
QualityQuality has been a well-recognized issue inLTC for some time. Because Medicare andMedicaid finance more than half of the na-tion’s nursing home care, government regu-lations play a major role in establishingstandards to ensure at least the minimum lev-el of quality. Research has demonstrated thatthe overall effects of this regulation havebeen positive. On the other hand, little hasbeen done to ensure quality of care in assist-ed living facilities and for community-basedservices.
From the standpoint of quality of care de-livered to nursing home residents, OBRA-87was revolutionary. For example, the sharpdecline in the use of physical and chemicalrestraints has been attributed to the require-ments of OBRA-87. Other positive care prac-tices since the implementation of OBRA-87standards include improved staffing levels,more accurate medical records, comprehen-sive care planning, increased use of inconti-nence training programs and a decrease in theuse of urinary catheters, and increased partic-ipation of residents in activity programs(Hawes et al., 1997; Marek et al., 1996; Tenoet al., 1997; Zhang & Grabowski, 2004).OBRA-87 also mandated a comprehensivepatient assessment process, which led to thedevelopment of a standardized Resident As-sessment Instrument (RAI). The assessmentprotocols are designed to help nursing homesidentify and treat or manage chronic condi-tions, the onset of acute illnesses, adverseeffects of medications, or other factors thatcaused or contributed to a clinical problem(Hawes, 2003).
Although substantial progress has beenmade, OBRA-87 remains controversial forseveral reasons:
38 CHAPTER 2 • Long-Term Care Policy: Past, Present, and Future
74035_CH02_5368.qxd 8/4/09 9:43 AM Page 38
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION

• In 2006, nearly one-fifth of the facilitieswere cited for violations that causedharm or presented immediate jeopardyto residents. Improvements appear tohave reached a plateau (Wiener et al.,2007).
• Regulations continue to be inconsistent-ly applied both within and across regions(Miller & Mor, 2006). Over a decadeago, Phillips (1996) had pointed out thatthere were significant differences in howinspectors applied the regulations andgave citations for noncompliance withthe regulations. The oversight process isreliable only for assessing aggregate re-sults, but inspectors frequently disagreeon the scope and severity of problemsuncovered (Lee et al., 2006).
• Phillips (1996) concluded that only 16%of the OBRA-87 regulations actually fo-cused on clinical care and therefore didnot primarily focus on high-quality care.
• Enforcement of OBRA-87 regulationstakes on a punitive rather than a remedi-al tone. Nonflagrant violations can bebetter addressed with a focus on im-provement rather than punishment (Will-ging,2 2008).
• Staffing levels have been relatively sta-ble for many years, despite the increasedclinical acuity in the patient population(Wiener et al., 2007).
• There is practically no available quanti-tative data on quality of life, which is animportant component of LTC (Wiener etal., 2007).
Policy for the FutureThe future of LTC will be shaped by bothpolicy and innovation, but policy will con-tinue to play the dominant role. Long-termcare faces many serious challenges ahead.Much will depend on (1) the health status ofAmericans and the prevalence of disability inthe population; (2) birth and mortality rates;(3) quality of education for the younger gen-eration, innovations that generate nationalwealth, and quality of immigration that wouldbe necessary for a strong economy; and (4)availability of financial resources as well aspriorities for their use. These factors are crit-ical from a broad policy perspective. Thefuture need for LTC services is just one partof the equation; much will depend on the na-tion’s ability to actually finance and deliverthe needed services. For example, if the in-frastructure for delivery (such as a skilledworkforce) is inadequate, many people mayhave to do without the services they may oth-erwise need.
The complex interaction among financ-ing, access, and utilization for LTC serviceswould play out within a broader context ofhealth policy for two main reasons: (1) Theaging of the population will have far-reach-ing repercussions beyond LTC, withspillover effects for retirement, Social Secu-rity, primary health care, acute care in hos-pitals, and numerous other health careservices. With aging, the utilization for alltypes of health care services increases, notjust the need for LTC. (2) Financing for LTCservices is an integral part of the Medicareand Medicaid programs, which also covervarious types of other health care services.
Life expectancy for a newborn in theUnited States has risen from 68.2 years in
Policy for the Future 39
2Dr. Willging was president of the American Health Care As-sociation (AHCA) at the time OBRA-87 was passed. TheAHCA was heavily involved in representing the for-profitnursing home sector, which supported the legislation.
74035_CH02_5368.qxd 8/4/09 9:43 AM Page 39
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION

1950 to 78.1 years in 2006, the highest everrecorded (Heron et al., 2008). During thesame time period, birth rates3 dwindled from24.1 to 14.2 (Martin et al., 2009). More than75 million baby boomers are about to enterretirement age in 2011 and beyond. Between2005 and 2050, the nation’s elderly popula-tion is projected to more than double, whilethe number of working-age Americans andchildren will grow more slowly than the el-derly population (Passel & Cohn, 2008).
Future growth of one population groupat the expense of another group (in this case,growth of the elderly population while at thesame time a contraction of the working pop-ulation) is called the demographic impera-tive. It has potentially serious consequencesat two main fronts: (1) With fewer workingpeople and a burgeoning elderly population,the financial burden for LTC on future gen-erations is expected to be enormous. This isan impending dilemma that policymakershave been reluctant to bring up for public pol-icy debates. (2) A labor force crisis for LTCdelivery is already beginning to emerge be-cause a smaller proportion of people from ashrinking pool of new workers are choosingemployment in health care delivery settings(Stone & Wiener, 2001). Commissions havebeen organized at both federal and state lev-els to recommend solutions to address the is-sue of labor shortages (Friedland, 2004).
The future need for LTC will be closelyassociated with health and disability trends inan aging population. Actually, some researchhas shown that there are positive trends in thehealth of older Americans, thanks to advancesin medical treatments. The bad news, howev-er, is that obesity and diabetes have both in-creased among older people as it has in the
younger age groups, and hypertension hasincreased in older women (Kramarow et al.,2007). Nevertheless, at least according to onesource, the rise in the number of people withactivity limitations is expected to moderateover time. Acosta and Hendrickson (2008)projected the number of people with activitylimitations to rise 14% between 2010 and2020, but the rate of increase would moder-ate to 10.5, 7.9, and 5.8%, respectively, dur-ing the subsequent 10-year periods between2020 and 2050. Even according to this sce-nario, the aging demographic lends urgency tohow best to restructure federal and state bud-gets to pay for more than 12 million olderAmericans who will probably need LTC ser-vices starting in 2010 (Acosta & Hendrick-son, 2008). On the other hand, policymakerswill continue to explore new ways for pro-viding cost-effective LTC services withoutturning LTC into an expanded social programbecause both Medicare and Medicaid faceserious cost challenges in the future. As partof these efforts, funding for community al-ternatives will continue, but many recipientsof care in the home- and community-basedsettings will eventually need to be institu-tionalized. In addition to policies that pro-mote community-based care, other policiescan help strengthen the LTC system.
PreventionLTC policy issues tend to focus on receivingand delivering care, rather than on actions thatcan prevent or delay the need for care. En-hancing community environments that canpromote walking—such as repairing or build-ing sidewalks, ensuring safety from traffic,protecting older adults from crime, and pro-moting leisure activities—can improve phys-ical activity and promote better health. Other
40 CHAPTER 2 • Long-Term Care Policy: Past, Present, and Future
3Birth rate is number of live births per 1,000 population.
74035_CH02_5368.qxd 8/4/09 9:43 AM Page 40
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION

preventive measures include a balanced diet,obesity control, smoking cessation, and vac-cinations against influenza and pneumonia.Both community-based and institution-basedfall prevention programs are critical becausethey result in high medical costs, disability,functional limitations, and diminished qual-ity of life (CDC/Merck, 2007).
FinancingCurrently, most middle-class families are un-prepared to meet LTC expenses. Most peoplethink that Medicare would pay for their LTCneeds, but Medicare covers only short-termpost-acute care after discharge from a hospi-tal. Less than 10% of the elderly have privateLTC insurance (Burke et al., 2005). Withouta strong reliance on private LTC insurancecoverage, the public sector will see its expen-ditures grow rapidly. Purchasing LTC insur-ance is both expensive and confusing. Also,current tax policies provide greater incentivesto business owners and older adults than toyounger people when they purchase LTC in-surance. The Congressional Budget Office(CBO, 2004) recommended improving theway private markets for LTC insurance cur-rently function, but policy initiatives are need-ed to expand purchase of private insurance.
WorkforceIt is estimated that between 2000 and 2010alone, when the baby boomers are about toreach retirement age, an additional 1.9 mil-lion direct care workers would be needed inLTC settings (DHHS, 2003). Stone (2003) be-lieves that shortage of a stable and qualifiedworkforce may be the most important andmost neglected policy concern. The infra-structure can be severely restricted in its ca-
pacity to provide services without an adequatenumber of qualified workers. Experts in LTCrate workforce issues at par with the agingof the population itself (Miller et al., 2008).An inadequate supply of qualified workershinders recruitment efforts. Once recruited,retention becomes equally challenging. Somehealth care workers have low preferencesabout caring for elderly people who havephysical and mental incapacities. Hard workwithout adequate pay is another factor thatmakes people leave employment in the LTCsector (see Chapter 16 for details on effectiverecruitment and retention).
Another issue that must be addressed istraining deficits in geriatrics among physi-cians, nurses, therapists, social workers, andpharmacists. Ironically, all 125 U.S. medicalschools have a pediatrics department, butonly three have a geriatrics department. Ev-idence shows that care of older adults byhealth care professionals prepared in geri-atrics yields better physical and mental out-comes without increasing costs (Cohen et al.,2002). It is estimated that only about 9,000practicing physicians in the United States(2.5 geriatricians per 10,000 elderly) haveformal training in geriatrics. This number isexpected to drop down to 6,000 in the nearfuture. Among nurses, less than 0.05% haveadvanced certification in geriatrics (CDC/Merck, 2004).
There are also not enough well-trainedadministrators to provide leadership in theLTC field. Recruitment and retention ofNHAs is a growing problem nationwide(Maine Department of Professional and Fi-nancial Regulation, 2004). Lack of appro-priate educational standards as a requirementfor licensure of NHAs no doubt contributesto the problem. In turn, the shortage of NHAsprevents the raising of national educational
Policy for the Future 41
74035_CH02_5368.qxd 8/4/09 9:43 AM Page 41
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION

standards to a minimum of a bachelor’s de-gree in health care administration.
Health Information TechnologyLeaders in the LTC field tend to look to thegovernment for direction in health informa-tion technology (HIT) adoption (Hudak &Sharkey, 2007). Interoperable HIT can en-able providers to track patients’ care acrosshospitals, nursing homes, home health agen-cies, pharmacies, and physicians’offices. In-teroperability is essential for an integratedsystem of health care that interfaces with LTCservices. Long-term care needs to be fullyrepresented in all future interoperable elec-tronic health records. Such systems areparticularly critical because the elderly fre-quently make transitions between LTC andnon-LTC settings. Currently, such transitionsrarely occur smoothly because of high ratesof missing or inaccurate information (Miller& Mor, 2006). HIT can also help reduce iso-lation among seniors and caregivers throughelectronically enabled social networks andonline training for caregivers (Martin et al.,2007). HIT applications can also improvestaff efficiency, interface with quality mea-sures, reduce billing errors, improve clinicalaccuracy, and improve communication amongproviders.
Mental HealthThe quality of mental health services in LTCsettings remains a challenge. There are con-cerns that patients are not receiving themental health care they need or that they arereceiving inappropriate, and sometimes un-necessary, mental health services. Eventhough certain aspects of mental health andpsychiatric care are addressed in the OBRA-87 legislation, outcome evaluations have pre-sented challenges (Streim et al., 2002).
Evidence-Based PracticesAs pointed out earlier, quality improvementin LTC has come to a standstill. Also, there islittle evidence that merely increasing theamount of spending improves quality. To thecontrary, quality improvement often reducescosts. Evidence-based practices will drive thefuture of quality improvement in all types ofhealth care delivery settings. Best practices inthe form of clinical practice guidelines havebeen developed for long-term care. However,no policy initiatives have emerged to provideincentives for their use.
42 CHAPTER 2 • Long-Term Care Policy: Past, Present, and Future
For Further Thought1. Why is it important for administrators in the long-term care field to understand poli-
cy and policymaking?
2. What lessons in U.S. policymaking can be learned from the passage of the NursingHome Reform Act in 1987 and its near-repeal in 1995?
3. Do interest groups help or hinder the policymaking process?
4. Should policy be made only after due consideration of its cost-benefit?
74035_CH02_5368.qxd 8/4/09 9:43 AM Page 42
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION

For Further LearningClearinghouse for the Community Living Exchange Collaborative: A joint effort of the Institute forRehabilitation and Research and Rutgers Center for State Health Policy. The Exchange is a vital hubof information collection, sharing, and dissemination.
http://www.hcbs.org
National Clearinghouse for Long-Term Care Information. U.S. Department of Health and HumanServices
http://www.longtermcare.gov/LTC/Main_Site/index.aspx
Overview of the Nursing Home Reform Act
http://www.ltcombudsman.org/uploads/OBRA87summary.pdf
REFERENCES
Acosta, P., & Hendrickson, L. 2008. Discussion Brief: Advancing Medicaid HCBS Policy: FromCapped Consumer to Consumer-Directed. Rutgers Center for State Health Policy. RetrievedSeptember 2008 from http://www.hcbs.org/files/136/6774/ConsumerChoice.pdf.
Alliance for Health Reform. 2007. Long-Term Care Partnerships: An Update. Washington, DC:Alliance for Health Reform.
Burke, S.P., et al. 2005. Developing a Better Long-Term Care Policy: A Vision and Strategy forAmerica’s Future. Washington, DC: National Academy of Social Insurance.
Castle, N.G. 2001. Citations and compliance with the Nursing Home Reform Act of 1987. Journalof Health and Social Policy 13, no. 1: 73–95.
CBO. 2004. Financing Long Term Care for the Elderly. Washington, DC: Congressional BudgetOffice.
CDC/Merck. 2004. The State of Aging and Health in America, 2004. Centers for Disease Controland Prevention and Merck Company Foundation. Retrieved October 2008 fromhttp://www.cdc.gov/aging/pdf/State_of_Aging_and_Health_in_America_2004.pdf.
CDC/Merck. 2007. The State of Aging and Health in America. Centers for Disease Control and Pre-vention and Merck Company Foundation. Retrieved October 2008 from http://www.cdc.gov/aging/pdf/saha_2007.pdf.
Cockrel, J. 1997. Public Policymaking in America. Retrieved September 2008 fromhttp://www.ca.uky.edu/agc/pubs/ip/ip19/ip19.pdf.
Cohen, H.J., et al. 2002. A controlled trial of inpatient and outpatient geriatric evaluation and man-agement. New England Journal of Medicine 346, no. 12: 906–912.
Coleman, B. 1999. Trends in Medicaid Long-Term Care Spending. Research report, AARP PublicPolicy Institute. Retrieved September 2008 from http://www.aarp.org/research/assistance/medicaid/aresearch-import-646-DD38.html#community.
DHEW (Department of Health, Education, and Welfare). 1975. Long Term Care Facility ImprovementStudy: Introductory Report. Washington, DC: Department of Health, Education, and Welfare.
References 43
74035_CH02_5368.qxd 8/4/09 9:43 AM Page 43
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION

DHHS (Department of Health and Human Services). 2003. The Future Supply of Long-Term CareWorkers in Relation to the Aging Baby Boom Generation, Report to Congress. Washington, DC:Department of Health and Human Services.
Edelman, T.S. 2003. Enforcement in the assisted living industry: Dispelling the Industry’s Myths.NAELA Quarterly 3, no. 2: 9–12.
Eustis, N., et al. 1984. Long-Term Care for Older Persons: A Policy Perspective. Monterey, CA:Brooks/Cole Publishing.
Friedland, R.B. 2004. Caregivers and Long-Term Care Needs in the 21st Century: Will Public PolicyMeet the Challenge. Washington, DC: Health Policy Institute, Georgetown University.
Grabowski, D.C. 2006. The cost-effectiveness of noninstitutional long-term care services: Reviewand synthesis of the most recent evidence. Medical Care Research and Review 63, no. 1: 3–28.
Hawes, C. 2003. Ensuring quality in long-term care settings. In D. Blumenthal et al. (eds.). Long-term Care and Medicare Policy: Can We Improve the Continuity of Care? (pp. 131–143). Wash-ington, DC: National Academy of Social Insurance.
Hawes, C., et al. 1997. The impact of OBRA-87 and the RAI on indicators of process quality innursing homes. Journal of the American Geriatrics Society 45, no. 8: 977–985.
Hawes, C., et al. 2007. The RAI and the Politics of Long-Term Care: The Convergence of Scienceand Politics in U.S. Nursing Home Policy. Report published by the Milbank Memorial Fund.Retrieved September 2008 from http://www.milbank.org/reports/footnotes/US.html.
Heron, M.P., et al. 2008. Deaths: Preliminary data for 2006. National Vital Statistics Reports, Vol.56, no. 16. Hyattsville, MD: National Center for Health Statistics.
Hudak, S., & Sharkey, S. 2007. Health Information Technology: Are Long Term Care ProvidersReady? Oakland, CA: California HealthCare Foundation.
IOM. 1986. Improving the Quality of Care in Nursing Homes. Washington, DC: National AcademyPress, Institute of Medicine.
Kaiser (Kaiser Commission on Medicaid and the Uninsured). 2007. Medicaid Facts. The Henry J.Kaiser Family Foundation. Retrieved September 2008 from http://www.kff.org/medicaid/upload/2186_05.pdf.
Kasper, J., &. O’Malley, M. 2006. Nursing Home Transition Programs: Perspectives of State Medic-aid Officials. Kaiser Commission on Medicaid and the Uninsured. Retrieved September 2008from http://www.kff.org/medicaid/upload/7484.pdf.
Kramarow, E., et al. 2007. Trends in the health of older Americans, 1970–2005. Health Affairs 26,no. 5: 1417–1425.
Lee, J. 2004. Aging Policy and Policy in U.S. Center for Human Resource Research, Ohio State Uni-versity (PowerPoint slides, June 2004). Retrieved September 2008 from www.kspa.org/multy_board/bbs_files/20060406041206.ppt.
Lee, R.H., et al. 2006. Reliability of the nursing home survey process: A simultaneous survey ap-proach. The Gerontologist 46, no. 6: 772–780.
Long, S.K., et al. 2005. Getting by in the community: Lessons from frail elders. Journal of Agingand Social Policy 17, no. 1: 19–44.
Maine Department of Professional and Financial Regulation. 2004. Report of the Board of NursingHome Administrators. Retrieved February 2009 from http://www.maine.gov/pfr/legislative/documents/nursingh.pdf.
44 CHAPTER 2 • Long-Term Care Policy: Past, Present, and Future
74035_CH02_5368.qxd 8/4/09 9:43 AM Page 44
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION

Marek, K.D., et al. 1996. OBRA ‘87: Has it resulted in positive change in nursing homes? Journalof Gerontological Nursing 22, no. 12: 32–40.
Martin, J.A., et al. 2009. Births: Final data for 2006. National Vital Statistics Reports, Vol. 57, no. 7.Hyattsville, MD: National Center for Health Statistics.
Martin, R.D., et al. 2007. Essential but Not Sufficient: Information Technology in Long-Term Careas an Enabler of Consumer Independence and Quality Improvement. Report to the NationalCommission for Quality Long-Term Care. Mclean, VA: BearingPoint Management and Tech-nology Consultants.
MedPAC. 2002. Report to Congress: Medicare Payment Policy. Washington, DC: Medicare Pay-ment Advisory Commission.
Miller, E.A., & Mor, V. 2006. Out of the Shadows: Envisioning a Brighter Future for Long-TermCare in America. Providence, RI: Brown University.
Miller, E.A., et al. 2008. Assessing experts’ views of the future of long-term care. Research on Ag-ing 30, no. 4: 450–473.
Miller, N.A., et al. 2006. Strengthening home and community-based care through Medicaid waivers.Journal of Aging and Social Policy 18, no. 1: 1–16.
Mor, V., et al. 2007. Prospects of transferring nursing home residents to the community. Health Af-fairs 26, no. 6: 1762–1771.
MRSC. 1999. Local Government Policy-Making Process (Report No. 45). Seattle, WA: The Munici-pal Research Services Center of Washington.
Nixon, D.C. 2007. State Programs to Encourage Long Term Care Insurance: Worthwhile or Wast-ed? Paper presented at the annual meeting of the Midwest Political Science Association. PalmerHouse Hotel, Chicago, April 12, 2007. Retrieved September 2008 fromhttp://www.allacademic.com/meta/p198586_index.html.
O’Keeffe, J., & Siebenaler, K. 2006. Adult Day Services: A Key Community Service for OlderAdults. Washington, DC: U.S. Department of Health and Human Services.
Passel, J.S., & Cohn, D. 2008. U.S. Population Projections: 2005–2050. Washington, DC: Pew Re-search Center.
Phillips, R.E. 1996. Crises in the Regulation of Long-Term Care. Doctoral dissertation: WesternMichigan University, April 1996.
Seff, M.K. 2003. Clearing up health care myths. Golden Lifestyles (Jan. Feb. Mar.): 7.
Social Security Administration. Undated. Legislative history: Social Security Act of 1935. RetrievedSeptember 2008 from http://www.ssa.gov/history/35acti.html.
Stevenson, K. 2007. History of Long-Term Care. Retrieved September 2008 from http://www.elderweb.com/home/main.
Stone, R. 2003. Reality of caring for the long-term care population. In Long-term Care andMedicare Policy: Can We Improve the Continuity of Care?, D. Blumenthal et al. (eds.)(pp. 40–47). Washington, DC: National Academy of Social Insurance.
Stone, R., & Wiener, J. 2001. Who Will Care for Us? Addressing the Long-term Care Workforce Cri-sis. Washington, DC: Urban Institute and the American Association of Homes and Services forthe Aging.
Streim, J.E., et al. 2002. Regulatory oversight, payment policy, and quality improvement in mentalhealth care in nursing homes. Psychiatric Services 53, no. 11: 1414–1418.
References 45
74035_CH02_5368.qxd 8/4/09 9:43 AM Page 45
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION

Teno, J., et al. 1997. The early impact of the Patient Self-Determination Act in long-term care facili-ties: Results from a ten-state sample. Journal of the American Geriatrics Society 45, no. 8:939–944.
Trocchio, J. 1984. Nursing home deregulation: Regulatory reform efforts. Nursing Economics 2, no.3: 185–189.
Turnham, H. 2001. Federal Nursing Home Reform Act from the Omnibus Budget Reconciliation Actof 1987. National Long Term Care Ombudsman Resource Center. Retrieved September 2008from http://www.ltcombudsman.org/ombpublic/49_346_1023.cfm.
Wagner, D. 2005. The Poorhouse: America’s Forgotten Institution. Lanham, MD: Rowman & Little-field Publishers.
Wiener, J.M., et al. 2000. Federal and state initiatives to jump start the market for private long-termcare insurance. Elder Law Journal 8, no. 1: 57–102.
Wiener, J.M., et al. 2007. Nursing Home Care Quality: Twenty Years After the Omnibus Budget Rec-onciliation Act of 1987. Menlo Park, CA: The Henry J. Kaiser Family Foundation.
Willging, P. 2008. Personal electronic communication. September 23, 2008.
Zhang, X., & Grabowski, D.C. 2004. Nursing home staffing and quality under the Nursing HomeReform Act. The Gerontologist 44, no. 1: 13–23.
46 CHAPTER 2 • Long-Term Care Policy: Past, Present, and Future
74035_CH02_5368.qxd 8/4/09 9:43 AM Page 46
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION