Embed Size (px)
Citation preview

Long-Term Supportsin Massachusetts
Long-Term Care Financing Advisory Committee Meeting March 5, 2009

Long Term Supports (LTS) in Massachusetts
Massachusetts has a lengthy history of supporting the long-term care needs of elders and people with disabilities across the lifespan.
The Patrick Administration’s long-term care policy is community first, an approach that emphasizes maximizing independence in home and community settings while assuring access to needed institutional care.
2

Key Facts IllustrateWhy We Are Here

People who need LTS are represented among all age groups
Figure 1: People with Disabilities in Massachusetts, by Age Group
* “Any disability” refers to an individual self-reporting any of 6 types of disabilities, as defined by the ACS survey.
** “Self-care disability” refers to an individual reporting difficulty with dressing, bathing, or getting around because of a physical, mental, or emotional condition lasting 6 months or more.
Ages
Total Non-Institutional Population 5 Years and
OlderWith Any Disability*
With a Self-Care
Disability**
Self-Care as % of Any Disability
Any Disability as % of Total Population
5 - 20 1,349,334 97,561 13,360 13.7% 7.2%
21 - 44 2,120,128 162,042 21,983 13.6% 7.6%
45 - 64 1,708,314 275,909 50,187 18.2% 16.2%
65+ 812,382 294,374 72,544 24.6% 36.2%
All 5 and Older
5,990,158 829,886 158,074 19.0% 13.9%
4

The population with disabilities is projected to grow significantly in the next decade
Figure 2: Comparisons of the 2004 Actual and 2015 ProjectedNumber of Disabled 16-64 Year Old Persons in Massachusetts (in
1000s)
Projected Disabled in 2015
Number of Disabled in 2004
Number(thousands)
0
100
200
300
400
500
Total 16-6445-6425-4416-24
5342
123135
271
224
447
401
28% Change
-9% Change
21% Change
12% Change
5

The elder population is projected to grow significantly in the next decade
Figure 3: Comparisons of the 2005 Actual and 2020 ProjectedNumber of 65-85+ Year Old Persons in Massachusetts
2020 Projected % ofT Total Population
2005Actual % ofT Total Population
% Change inAge Group Population
% of totalpopulation
% changein agegrouppopulation
0%
2%
4%
6%
8%
10%
12%
14%
16%
18%
Total 65+85+75-8465-740%
10%
20%
30%
40%
50%
60%
70%
80%
Total 65+85+75-8465-74
9.6%
6.1%
4.8%5.0%
2.5%2.2%
16.9%
68%
3%
21%
36%
13.3%
6

LTS spending is projected to increase with the changes in the population
Figure 4: Projected National Spending on Long-Term Care Expenditures
for the Elderly, 2000, 2020, 2040 (in 2000 dollars)
2020
2000
2040
Payers of Long-Term Care Services
Total Spending$0 billion
$50 billion
$100 billion
$150 billion
$200 billion
$250 billion
$300 billion
$350 billion
Out of PocketPrivateLong-Term Care
Insurance
MedicaidMedicare
$50.6
$29.4
$75.4
$43.3 $36.2$5.0
$42.9$42.8
$207.3
$346.1
$123.1
Spending
Note: comparable figures on spending for non-elderly individuals with disabilities are not currently available.
7

The current LTS system is heavily dependent on institutional care…
Licensed Census MassHealth Empty Beds# of nursingfacility beds
0
10000
20000
30000
40000
50000
60000
20082006200420022001200019971995
Figure 5: Comparison of Massachusetts Licensed Nursing Facility Bedsto Census (All Payers), 1995-2008
8

…but community LTS spending is increasing
Figure 6: MassHealth Nursing Facility Spending as a Percent of Total MassHealth Long-Term Care Spending
9
Institutional Community
Spending
$0.0 billion
$0.5 billion
$1.0 billion
$1.5 billion
$2.0 billion
$2.5 billion
$3.0 billion
F Y 2008 F Y 2007 F Y 2006 F Y 2005 F Y 2004 F Y 2003
73% 68% 71% 72% 64% 60%

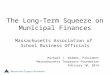
Unlike “acute” care, there is little employer/commercial insurance participation in financing LTS
Figure 7: Estimated Percentage of Share of Spending forLong-Term Care for the Elderly
* Values are calculated on the basis of how much such care would cost if it were provided through formal means. Estimates are from Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation, Administration on Aging, Informal Caregiving: Compassion in Action (June 1998), inflated to 2004 dollars.Note: comparable figures on spending for non-elderly individuals with disabilities are not currently available.
W ithout Informal Care W ith Informal Care*
Other3%
Private Insurance4%
Medicaid35%
Medicare25%
Out-of-Pocket
33%
Other 2%
Private Insurance 3%
Medicaid22%
Medicare16%
Out-of-Pocket
21%
InformalCare36%
10

Medicaid is the primary payer of LTS nationally and in Massachusetts
Figure 8: National Spending for Long-Term Care, by Payer (2005)
2.6%
2.7%
7.2%
18.1%
20.4%
48.9%
Other Public
Other Private
Private Health <C Insurance
Out-of-Pocket
Medicare
Medicaid
11

Community First Olmstead Plan

The MA Community First Olmstead Plan
Olmstead v. L.C decision (U.S. Supreme Court, 1999)
Americans with Disabilities Act (ADA) requires states to provide services in the most integrated settings appropriate to the needs of individuals with disabilities
The development of the Plan:
An Olmstead Planning Committee was convened in late Fall 2007
Olmstead Plan was approved by the Governor in Fall 2008
13

CF Olmstead Plan principles1. People with disabilities and elders should have access to
community living opportunities and supports.
2. The principle of “community first” should shape policy development and funding decisions.
3. A full range of long-term supports, including HCBS, housing, employment opportunities and nursing facility services, are needed.
4. Choice, accessibility, quality, and person-centered planning should be the goals in developing LTS.
5. Systems of community-based care and support must be strengthened, expanded and integrated to ensure access/efficiency.
6. Public and private mechanisms of financing LTS must be expanded.
7. LTS must address the diversity of individuals with disabilities and elders in terms of race, ethnicity, language, ability to communicate, sexual orientation, and geography.
14

CF Olmstead Plan goals1. Help individuals transition from institutional care.
2. Expand access to community-based long-term supports.
3. Improve the capacity and quality of community-based long-term supports.
4. Expand access to affordable and accessible housing with supports.
5. Promote employment of people with disabilities and elders.
6. Promote awareness of long-term supports.
15

Select Related Community First Activities
Systems Transformation Grant State Profile Tool Grant Long Term Care Options Counseling Massachusetts Aging and Disability Information Locator Aging and Disability Resource Center Expansion Grant CF 1115 Waiver Real Choice Pilot Person Centered Planning Grant Medicaid Infrastructure and Comprehensive Employment
Opportunities Grant (MI-CEO) EOHHS Agency Internal Housing Working Group EOHHS Agency Internal Quality Working Group Personal Care Attendant Improvement Workgroup Personal Care Attendant Quality Workforce Council
16

The Advisory Committee’s Rolein the Olmstead Plan

Advisory Committee role
Reform of the LTS system is “contingent upon the availability of re-aligned as well as new public and private long-term support funding.”
Community First Olmstead Plan, p. 3
"A Long-Term Care Financing Advisory Group will be established to determine a roadmap for public and private financing development.”Community First Olmstead Plan, p. 10
18

Advisory Committee problem statementThe financing system for long-term care supports (LTS) in Massachusetts is:
1) fragmented among various public and private payers and unpaid informal caregiver supports;
2) centered on insurance-based programs that primarily cover services that are medically necessary, when most individuals’ LTS needs and preferences are for community-based social supports;
3) insufficient to support current and projected needs; and
4) heavily dependent on state public assistance programs that have limited resources and base access to LTS on an individual’s income, age, type of disability, etc.
Projected increases in the population of elders and individuals with disabilities who will need LTS, a projected decline in the availability of informal supports for LTS, and continued insufficient workforce capacity to provide LTS will exacerbate these problems.
19

Overarching critical questions1. What is an appropriate mix of public and private financing
mechanisms for the whole system of LTS, given the current and projected needs and preferences of the populations to be served?
2. Assuming that some form of public-private partnership will remain as the predominant model for financing LTS, what is the role of a public safety net system that provides a minimum set of LTS for all who demonstrate need?
3. Within these parameters, what innovative formal or informal financing models exist or can be developed that will ensure that these LTS needs are met?
4. What investments or system reforms are necessary (and under what timeframes) to implement these financing models?
20

Advisory Committee goal
To identify and prioritize short-term and long-term strategic options for reforming the financing system for LTS for elders and individuals with disabilities in Massachusetts to support a range of LTS and a sustainable mix of personal and familial responsibility, private financing mechanisms and public assistance in a manner that:
maximizes independence; and assures access to the necessary continuum of
LTS.
21

Framework for Reform Discussion

Merlis: Reforming LTS financing involves a series of decisions about…
1. Sources of funding
2. Mix of funding
3. Eligibility for benefits
4. Nature/extent of covered services
23

These LTS financing reform decisions relatively value… Shared responsibility
Pool/spread risk through public or private insurance
Strong safety net for the poor
Focus on consumer needs and preferences
Popular support
Flexibility
Support for family caregivers
Integration of medical and social services
Quality
Access
Efficiency
24

Possible high-level strategies for designing an alternative system
Private at its core:
1. Improve and promote private long-term care insurance for the “middle” income
2. Establish public catastrophic long-term care insurance and improve/promote private long-term care insurance to “fill the gap”
Public at its core:
1. Improve and expand the public safety net for people with low-to-modest income
2. Establish universal public long-term care insurance
25

Things to Consider
These approaches are not mutually exclusive!
In deciding direction, we need to ask:
Who is most likely to benefit?
Who will be “left out”?
How broad is the risk spread?
How will costs be distributed?
26

Committee Business

Public communications
Committee communications
Future meetings Time change: all subsequent meetings will be from
9:00AM – 11:30AM
Location: most meetings will be on the 21st floor of One Ashburton Place. The April 17th meeting will be in the Ashburton Café on the basement floor of One Ashburton Place.
28
Business items

Addendum 1Feedback from the Advisory Committee
Content:
Additional perspective (either on Committee or at specific session) is needed: Federal, other States, health economist, international
Existing government/agency structure and data systems may not be optimal
All financing options should be on the table, including private strategies beyond LTC insurance and reverse mortgages
Process:
Additional educational opportunities are needed between meetings
We should not answer policy questions (e.g., need for rebalancing) that already have been answered
Deliverable should have concrete, tangible options for the State
29

Addendum 2Sources for Slides 23-26
Allen, K. “Long-Term Care Financing, Growing Demand and Cost of Services are Straining Federal and State Budgets,” U.S. Government Accountability Office (April 27, 2005).
Feder, J., H. Komisar, and R. Friedland. “Long-Term Care Financing: Policy Options for the Future.” Georgetown University Long-Term Care Financing Project (June 2007).
Gleckman, H. “How Can We Improve Long-Term Care Financing,” Center for Retirement Research at Boston College (June 2008, Number 8-8).
Merlis, M. “Long-Term Care Financing: Models and Issues.” Prepared for the National Academy of Social Insurance Study Panel on Long-Term Care (April 30, 2004).
National Commission for Quality Long-Term Care. “From Isolation to Integration. Recommendations to Improve Quality in Long-Term Care” (December 3, 2007).
Washington State Task Force on Long-Term Care Financing & Chronic Care Management, Final Report (January 2008).
30