Embed Size (px)
Citation preview

Journal of PathologyJ Pathol 2003; 200: 640–646.Published online 31 March 2003 in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/path.1378
Original Paper
Loss of PDCD4 expression in human lung cancercorrelates with tumour progression and prognosis
Yuan Chen,1 Thomas Knosel,l Glen Kristiansen,1 Agnieszka Pietas,1 Mitchell E Garber,2 Sachiko Matsuhashi,3
Iwata Ozaki3 and Iver Petersen1*1 Institute of Pathology, University Hospital Charite, Schumannstrasse 20–21, D-10098 Berlin, Germany2Department of Genetics, Stanford University School of Medicine, Stanford, CA, USA3Department of Internal Medicine, Saga Medical School, Saga 849-8501, Japan
*Correspondence to:Dr Iver Petersen, MD, Institute ofPathology, Charite MedicalSchool, Humboldt-University,D-10098 Berlin, Germany.E-mail: [email protected]
Received: 1 October 2002Revised: 11 November 2002Accepted: 14 February 2003
AbstractThe programmed cell death 4 gene (PDCD4), a newly identified transformation suppressor,was analysed in lung tumour cell lines and primary lung carcinomas. Reduced PDCD4mRNA expression was observed in two immortalized lung cell lines and 18 cancer cell linesby northern blot analysis. In the survey of primary lung tumours, PDCD4 cDNA was poorlyrepresented in 47 lung tumours compared with normal lung tissue by cDNA microarrayanalysis and this poor representation was significantly associated with high-grade (G3)adenocarcinomas (p = 0.012). Immunohistochemical analysis of 124 primary carcinomascomprising all subtypes demonstrated that PDCD4 protein expression was widely lost intumour samples (83%) and was negatively related to poor prognosis (p = 0.013). The lossof PDCD4 expression correlated with higher grade and disease stage (p = 0.045 and 0.034,respectively), but not tumour size and nodal status. Similarly to the cDNA data, lack ofPDCD4 expression was significantly linked to tumour grade in adenocarcinoma (n = 59,p = 0.048), while in squamous cell carcinoma (n = 58), no relationship between PDCD4expression and clinicopathological parameters was established. These data suggest that theloss of PDCD4 expression is a prognostic factor in lung cancer and may correlate withtumour progression. Copyright 2003 John Wiley & Sons, Ltd.
Keywords: PDCD4; suppression subtractive hybridization (SSH); lung cancer; loss ofexpression and prognosis
Introduction
Lung cancer is the number one cause of cancerdeath in the United States [1]. In 1999 alone, therewere an estimated 171 600 new cases and 158 900deaths from this disease [2]. Unlike the other threemajor cancers, namely colorectal, breast, and prostatecancer, there has been little improvement in the 5-year survival for lung cancer patients over the pastthree decades [3]. Overall survival is less than 15%,despite advances in chemotherapy, radiation therapy,and surgery. Improving the survival of patients withthis disease requires a better understanding of tumourbiology, pathogenesis, and the ultimate developmentof novel therapeutic strategies.
Lung carcinogenesis, like the development of othercancers, is a multistage process involving alterationin multiple genes and diverse pathways [4]. A multi-tude of genetic aberrations have been detected at thechromosomal and molecular levels. In order to under-stand this genetic variability, we analysed the geneexpression profiles of lung cancer using a 24 000 ele-ment cDNA microarray [5]. In addition, we performedsuppression subtractive hybridization (SSH) to gen-erate libraries of differentially expressed genes when
comparing human bronchial epithelial cells (HBECs)with the lung carcinoma cell line H2170. Thereby, 869individual sequences were identified (Petersen et al,in press) [6]. The clone HBEC-254 with high similar-ity to the human PDCD4 (H731) gene [7] was foundin the library enriched for the genes that are down-regulated in tumour cell lines.
It has been reported that the murine Pdcd4 geneis identical to murine MA-3, TIS, A7-1, and chickenPDCD4. Expression of the mouse MA-3 gene wasassociated with apoptosis in several systems [8]and the TIS gene was suppressed by topoisomeraseinhibitors in mouse lymphoma cells [9], while chickenPDCD4 was identified as the target gene of retroviraloncogene v-myb [10]. Most interestingly, A7-1 wasfound to be able to inhibit tumour promoter-inducedtransformation in the JB6 model system throughrepression of AP-1 activation in combination withslightly enhanced NF-κB activation [11,12]. However,the biological role that PDCD4 plays in human cancer,especially in lung cancer, is largely unclear.
In this study, we used several approaches, includingthe two molecular profiling techniques cDNA and tis-sue microarray analysis, to examine PDCD4 mRNAand protein expression in a set of patient samples.
Copyright 2003 John Wiley & Sons, Ltd.

PDCD4 expression in lung cancer 641
Materials and methods
Tumour samples
Tumour specimens used in this study were obtainedfrom 124 patients aged between 42 and 80 years(mean 61 years) who underwent surgical operation forlung cancer at the Department of Surgery, ChariteUniversity Hospital from 1995 to 2000. Local ethicalguidelines were followed for this study. No adjuvantradiotherapy or chemotherapy was administered beforesurgery. The pathological stage, grade, and nodalstatus were obtained from the primary pathologyreports. Table 1 summarizes the clinicopathologicalcharacteristics according to the TNM criteria of theUICC [13]. Survival data were present for 66 patients.The median follow-up period was 24 months (range2–66 months).
Tumour specimens used for cDNA microarray anal-ysis or RT-PCR were transferred to the Institute ofPathology within 1 h of surgical removal. They weresnap-frozen in liquid nitrogen and keep at −80 ◦C untilRNA isolation.
Cell lines and primary cell culture
Human lung carcinoma cell lines and immortalizedHBEC cell lines were purchased from the Ameri-can Type Culture Collection (ATCC, Rockville, MD,USA) and from the German Collection of Micro-organisms and Cell Culture (DSMZ, Braunschweig,Germany). Human lung carcinoma cell lines werederived from small cell lung carcinomas (SCLCs)(COLO668, COLO677, COLO699, N417, CPC-N,H526, DMS79, H82, SHP77) and non-SCLCs (A427,H2170, H2228, H23, H322, A549). ImmortalizedHBEC lines consisted of H2078 and H9442. HBECprimary cultures and human small airway epithelialcells (SAECs) were obtained from Clonetics (Bel-gium) and cultured in BEG media (Clonetics) to a
Table 1. Study cohort
PDCD4-negative
n (%)
PDCD4-positive
n (%)
Total No(n = 124) 103 (83%) 21 (17%)ADC 51 (41%) 8 (6%)SCC 46 (37%) 12 (10%)LCLC 4 (3%) 1 (1%)SCLC 2 (2%) 0 (0%)Grade 1–2 44 (35%) 14 (11%)Grade 3 59 (48%) 7 (6%)pT1 23 (19%) 8 (6%)pT2+ 80 (65%) 13 (10%)pN0 59 (48%) 10 (8%)pN1+ 44 (35%) 11 (9%)Stage I–II 38 (31%) 13 (10%)Stage III–IV 65 (53%) 8 (6%)
ADC = adenocarcinoma; SCC = squamous cell carcinoma; LCLC =large cell lung carcinoma; SCLC = small cell lung carcinoma; T =tumour; N = node.
maximum population doubling of 10. In addition, threeNSCLC cell lines were established in our laboratory,including D51, D97, and D117. They were derivedfrom primary tumours from patients who were oper-ated on at the Charite University Hospital. These cellswere grown in Leibovitz 15 media supplemented with10% FCS and 1% glutamine.
Northern blot analysis
Ten micrograms of total RNA extracted from HBECs,SAECs, and lung tumour cell lines together withimmortalized cell lines were separated in a 1.2%agarose/2.2 M formaldehyde gel and run for 4 hat 60 V, followed by capillary transfer onto nylonmembranes (Amersham, Braunschweig, Germany)overnight. The cDNA clone of HBEC-254 wasamplified by nested PCR as described previously [14]and used as a probe after labelling by random primingwith [32P]-dCTP (Megaprime labelling, Amersham).Following at least 30 min of pre-hybridization withExpresshyb solution (Clontech), the denatured probewas added and hybridization was carried out at 58 ◦Covernight. Blots were washed with 2 × SSC/0.1% SDSat room temperature and 0.1 × SSCP/0.1% SDS at60 ◦C and exposed to X-ray film at −80 ◦C.
cDNA microarray analysis
Poly A(+) RNA was isolated from frozen normallung tissue or primary lung tumour and examinedon 24 000-element cDNA microarrays. This workhas been described in detail previously [6] andthe raw data are readily available at http:/genome-www.stanford.edu/lung cancer/adeno/. PDCD4 wasone of the 24 000 cDNA clones on the spotted cDNAmicroarray. A total of 51 samples consisting of fournormal lung tissues and 47 primary tumours [28 ade-nocarcinomas (ADCs), 12 squamous cell carcinomas(SCCs), three large cell lung carcinomas (LCLCs), andfour small cell lung carcinomas (SCLCs)] were exam-ined for PDCD4 mRNA expression.
Tissue microarray construction
Tissue microarrays (TMAs) were constructed using amanual tissue arrayer purchased from Beecher Instru-ments (Woodland, USA). All sections were reviewedby two pathologists (T Knosel and YW Yu). Suit-able areas for tissue retrieval were marked on standardhaematoxylin and eosin (H&E) sections. Tissue cylin-ders with a diameter of 0.6 mm were punched outof the paraffin block and transferred into a recipientarray block. After construction, 4 µm sections contain-ing 248 tumours from 124 patients were cut from the‘donor’ blocks and transferred to glass slides withoutany sectioning aids such as adhesive tapes or addition-ally coated slides.
Copyright 2003 John Wiley & Sons, Ltd. J Pathol 2003; 200: 640–646.

642 Y Chen et al
Immunohistochemical analysis
Standard indirect biotin–avidin immunohistochemicalanalysis was used to evaluate PDCD4 protein expres-sion. Briefly, a section from the tissue array wasdewaxed with xylene and gradually hydrated. Anti-gen retrieval was performed by treatment in a pressurecooker for 6 min. The human H731 antibody, preparedas previously described [15], was incubated at roomtemperature for 1 h. Detection was carried out accord-ing to the manufacturer’s instructions (LSAAB-kit,DAKO). Additionally, 11 conventional large sectionswere used for immunostaining to compare the resultswith the TMA analysis. Three large sections fromnormal lung tissue were used as controls. All slideswere manually read by one pathologist (TK). Proteinexpression was scored as negative (score = 0), weak(1), moderate (2), or strong (3).
Semi-quantitative RT-PCR
Total RNA was prepared from 32 tissue speci-mens, human bronchial epithelial cells (HBECs), andlung carcinoma cell lines including COLO668, H82,H2228, COLO677, H2170, H23, CPC-N, H322, A427,SHP77, H23, N417, D97, and D51 by using Trizol(Life Technologies, Gaithersburg, MD) and treatedwith RQDNaseI (Promega, Madison, WI, USA) for40 min at 37 ◦C.
First-strand cDNA was reverse-transcribed using200 U of superscript II transcriptase (Gibco, Eggen-stein, Germany) from 3 µg of total RNA, in the pres-ence of 1 × RT buffer, 100 mM DTT, 20 U of RNaseinhibitor and 5 mM dNTPs, using the random hexamerprimers supplied in the kit. The reaction took place at42 ◦C for 1 h, followed by 15 min at 70 ◦C. Reac-tions lacking RT were used to verify the absence ofamplification from genomic DNA contamination (datanot shown). PCR was performed in a 50 µl volume(10 ng of template DNA, 2.0 mM dNTPs, and 10 pmolof the gene-specific primers designed from the 3′untranslated region of the PDCD4 gene, ie forwardprimer 5′-CCA, AAG, AAA, GGT, GGT, GCA-3′,and reverse primer 5′-TGA, GGT, ACT, TCC, AGT,TCC-3′). Amplification resulted in a DNA product of736-bp length. PCR conditions were 95 ◦C for 1 min,53 ◦C for 30 s, and 72 ◦C for 30 s. Controls were per-formed with commercially available glyceraldehyde-3-phosphate dehydrogenase (GAPDH ) primers (Clon-tech). All PCR products were subjected to elec-trophoresis on a 1.5% agarose gel and visualized bystaining with ethidium bromide.
Statistical analysis
RNA expression values within lung tissue for thegene encoding PDCD4 were obtained from cDNAmicroarray analysis. Specifically, we used the fol-lowing data which can be found at http:/genome-www.stanford.edu/lung cancer/adeno/: [log (base2) of
Red/Green normalized Ratio (Mean)]. Student’s t-test was carried out to evaluate the ratio value forthe PDCD4 gene. To compare the protein expressionof PDCD4 with clinicopathological parameters, 2 × 2contingency tables (eg PDCD4-negative and PDCD4-positive and G1 and G2 versus G3) were set up andthe χ2 test was applied. Survival curves were plot-ted according to Kaplan–Meier. A log-rank test wasapplied to examine the relationship between PDCD4-positive (or negative) and tumour-specific survival. Allp values were calculated two-sided. p values less than0.05 were considered statistically significant. All cal-culations were performed on a PC using the statisticalsoftware package SPSS.
Results
PDCD4 mRNA expression analysis in cultured lungcell lines
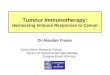
Northern blot analysis of cultured lung cell linesshowed that PDCD4 mRNA expression was notablyreduced in tumour cell lines compared with normalhuman bronchial epithelial cells (HBECs) and smallairway epithelial cells (SAECs) (Figure 1a). Espe-cially in the lung immortalized cell line, H9442, andin eight lung tumour cell lines including COLO-668,H2228, COLO-677, H526, A427, A549, SHP77, andCOLO-699, there was no clear signal detectable. Thisresult was also confirmed by RT-PCR (Figure 1b).
PDCD4 mRNA expression in primary lung tumour
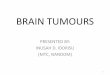
PDCD4 mRNA expression was examined in 51lung samples including four normal samples and 47tumours by cDNA microarrays. The mRNA expressionlevel was evaluated from the logarithmic ratio valueof PDCD4 (Figure 2a). The transcript level in pri-mary lung carcinoma was reduced compared with thatin normal lung tissue, which otherwise reaches one-sided significance in the t-test. In 28 adenocarcino-mas, PDCD4 mRNA expression was decreased. Thiswas most apparent in high-grade tumours (G3), whichshowed very significantly decreased PDCD4 expres-sion compared with low-grade tumours (p = 0.012).Reduced PDCD4 expression was also observed insquamous cell carcinoma but this did not achieve sta-tistical significance.
To evaluate PDCD4 mRNA expression further, RT-PCR was performed in 14 primary adenocarcinomasand 12 squamous cell carcinomas (Figure 2b). Com-pared with six normal controls, mRNA expression wasmarkedly reduced in adenocarcinoma, especially thoseof higher grade (G3), but not in squamous cell carci-noma.
PDCD4 protein expression in primary lungtumours
A tissue microarray was constructed to explorePDCD4 protein expression by immunohistochemistry
Copyright 2003 John Wiley & Sons, Ltd. J Pathol 2003; 200: 640–646.

PDCD4 expression in lung cancer 643
CO
LO66
8
CO
LO67
7
HB
EC
H20
78
H94
42
N41
7
H22
28
H82
DM
S79
SH
P77
H52
6
PDCD4
GAPDH
SA
EC
CP
C-N
H32
2
A42
7
A54
9
H21
70
H23
D11
7
D97
D51
CO
LO69
9
Mar
ker
HBECCO
LO66
8H82 H22
28CO
LO67
7H21
70H23 CPC-N
A427
H526
SHP77N41
7D97 D51H32
2
b
a
PDCD4
GAPDH
PDCD4
GAPDH
Figure 1. (a) Northern blot analysis of mRNA from cultured human bronchial epithelial cells (HBEC), human small airwayepithelial cells (SAEC), immortalized cell lines, and lung cancer cell lines. The PDCD4 clone HBEC-254 was radiolabelled andhybridized against mRNA isolated from cultured cells. Upper panel: PDCD4 mRNA was underexpressed in immortalized cell linesand lung cancer cell lines, in contrast to HBEC and SAEC. Lower panel: control hybridization with β-actin. (b) RT-PCR showingdown-regulation of PDCD4 mRNA in lung tumour cell lines
in 248 primary lung cancer samples from 124 patients.Figure 3a shows a section from the TMA. In thetumour samples, 103 cases (83%) exhibited no rele-vant PDCD4 staining (Figure 3b), while in the other21 cases (17%), there was PDCD4 staining withthe signals localizing in both nuclei and cytoplasm(Figures 3c–3e). As a normal control, HBECs showedvery strong PDCD4 expression (Figure 3f). An asso-ciation was observed between PDCD4 protein under-expression and higher stage and grade tumours (p =
0.034, 0.045, respectively, Table 2). No significantcorrelations could be demonstrated with sex, age,tumour size, and node status.
Stratifying the data, we divided the primary tumoursinto different groups and analysed the data for ade-nocarcinomas and squamous cell carcinomas sepa-rately (Table 2). The sample sizes of small cell andlarge cell lung carcinomas were too small to beevaluated further. In adenocarcinoma, PDCD4 proteinunderexpression was linked to higher grade, with G3
Copyright 2003 John Wiley & Sons, Ltd. J Pathol 2003; 200: 640–646.

644 Y Chen et al
PDCD4
GAPDH
N Adeno G3 N Adeno G2 SCC
-1.2
-1
-0.8
-0.6
-0.4
-0.2
0a
b
N T ADC SCC
Figure 2. PDCD4 transcripts as determined by cDNA microarray analysis and by RT-PCR. (a) Diagram of PDCD4 mRNAexpression in four normal tissues, 28 adenocarcinomas, and 12 squamous cell carcinomas determined by cDNA microarrayanalysis. (b) PDCD4 and GAPDH expression detected by RT-PCR
Table 2. Correlation between PDCD4 underexpression andclinicopathological data (p values∗)
Stage (UICC) Grade pN+ pT
ADC 0.082 0.048 1.000 0.152SCC 0.291 0.864 0.279 0.648All tumours 0.034 0.045 0.417 0.128
∗ χ2 test.ADC = adenocarcinoma; SCC = squamous cell carcinoma.
tumours showing less PDCD4 protein staining (p =0.048), while no association was found with tumourstage, size, and nodal status. Unlike adenocarcinoma,PDCD4 expression in squamous cell carcinoma wasnot significantly related to any of the clinicopatholog-ical parameters that we investigated.
The absence of PDCD4 protein expression wasstrongly linked to adverse prognosis, revealed byKaplan–Meier statistical analysis (n = 66, p = 0.013,Figure 4), with the mean survival time for patientswith PDCD4-positive tumours reaching 47 monthscompared with 22 months in patients with PDCD4-negative tumours.
To confirm the utility of the tissue microarrayapproach for the analysis of PDCD4 protein expres-sion, we randomly selected 11 cases to compareimmunohistochemical evaluation of standard and tis-sue array slides. Three cases with positive staining forPDCD4 on the tissue microarray were also positive onthe large sections. The other eight cases were negativeon the tissue microarray: only one was positive on thelarge section.
Discussion
Subtractive suppression hybridization (SSH) is a PCR-based subtraction method that selectively amplifiestarget cDNA fragments and simultaneously suppressesamplification of non-target cDNAs. Cloning by SSHhas identified a number of genes potentially involvedin cancer and other disease processes [16,17]. Usingthis approach, the clone HBEC-254 was initially foundin a library representing preferentially down-regulatedgenes when we compared HBECs and the lung cancercell line H2170. In good agreement with the genera-tion of the SSH library, DNA clone HBEC-254 wasexpressed at a much lower level in tumour cell lineH2170 by northern blot analysis. Moreover, dimin-ished or absent expression of this gene was alsoobserved in other lung tumour cell lines not usedfor library construction. Sequencing HBEC-254 andsearching the database in NCBI revealed that this clonehas high similarity with MA-3 (mouse Pdcd4 ) andH731 (human PDCD4 ) genes. The potential impor-tance of the PDCD4 gene was enhanced by the reportfrom Cmarik et al [11] that Pdcd4 is highly expressedin a tumour promoter-resistant clone of the mouseepidermal cell line JB6, but not in a tumour promoter-sensitive sub-clone of the same cell line, and theantisense-transfected cells were reverted to their ini-tial promotion-resistant phenotype by overexpressionof a Pdcd4 sense fragment. This observation indicatesthat Pdcd4 protein inhibits neoplastic transformation inthe JB6 murine epidermal model and raises the pos-sibility that Pdcd4 is a novel tumour suppressor [11].We therefore turned our attention to the investigationof the potential role of PDCD4 in human lung cancer.
Copyright 2003 John Wiley & Sons, Ltd. J Pathol 2003; 200: 640–646.

PDCD4 expression in lung cancer 645
f
d e
a b c
Figure 3. Examples of PDCD4 protein expression in TMA and in large sections. (a) A section from TMA (2.5× magnification);(b) PDCD4 negative (25× magnification); (c) PDCD4 weakly positive (25× magnification); (d) PDCD4 moderately positive (25×magnification); (e) PDCD4 strongly positive (25× magnification); (f) normal control of HBECs (25× magnification)
survival time (months)
706050403020100
Cum
ulat
ive
surv
ival
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.0
PDCD4 pos (n = 18)
PDCD4 neg (n = 47)
P = 0.013
Figure 4. Prognostic relevance of PDCD4 alteration. The lossof PDCD4 expression is linked to short patient survival
Our data show that PDCD4 mRNA expression isclearly reduced in lung cancer compared with normalcontrols in both cultured cells and primary tumoursamples. In the cell line model, two immortalizedHBEC cell lines, H2078 and H9442, displayed dimin-ished expression, suggesting that the loss of PDCD4might already play a role in early-stage lung car-cinogenesis. Consistently, primary lung carcinomasshowed significantly reduced PDCD4 mRNA levelsrevealed by cDNA microarray and RT-PCR analysisand no protein expression by immunohistochemistry in
the majority of samples. In addition, our data revealedsignificant associations with parameters related totumour progression, ie higher tumour grade and stageas well as reduced patient survival.
To our knowledge, this is the first study to linkdiminished PDCD4 expression to lung carcinogenesis.In contrast to the reduced PDCD4 expression observedin the lung, PDCD4 protein has been reported tobe highly expressed in bladder carcinoma and breastcarcinoma compared with the corresponding normaltissues [15]. The molecular basis for this expressionpattern is not yet clear. However, it may indicate dif-ferent and potentially tissue-specific roles for the gene.
PDCD4 overexpression was identified in cellsundergoing apoptosis [8]. Genes involved in apoptosishave been reported to be associated with patient sur-vival in lung cancer. Previously, Volm and Koomagifound that lack of expression of pro-apoptosis factors,such as Fas, Fas ligand, and caspase 3, was linkedto poor survival in patients with NSCLC [18]. Sasakiet al observed that patients with high-level expressionof the novel sensitive-to-apoptosis gene (SAG) had asignificantly poorer survival than those with low SAGexpression [19]. The regulation of PCDC4 expressionand its association with apoptosis, however, are stillunclear [10,12]. Very recently, the first evidence for thetransformation suppressor PDCD4 as a negative regu-lator of the urokinase receptor (u-PAR) was presented[20]. The expression of the gene u-PAR was found tobe associated with poor survival in lung cancer [21].
Copyright 2003 John Wiley & Sons, Ltd. J Pathol 2003; 200: 640–646.

646 Y Chen et al
It is tempting to speculate that this is one mechanismfor the association of reduced PDCD4 expression andtumour progression.
Many studies have demonstrated that array-basedtissue analysis is a rapid, cost-effective, and tissue-saving method for high-throughput clinicopathologicalstudy [22,23]. However, concerns have been raisedthat this technology has obvious limitations; for exam-ple, the sampling of large potentially heterogeneoustumours, and insufficient tissues due to improperpunch, which inevitably leads to false-negative stain-ing [22]. In our study, tumour tissues from two dif-ferent regions of a paraffin block from one patientwere punched into the TMA block to overcome thisproblem. Additionally, immunostaining for PDCD4was performed in conventional large sections to com-pare with the TMA. This demonstrated that the dataobtained using TMA correlated well with those usingconventional sections. Indeed, this technology hasbeen successfully used to identify not only the genesthat are overexpressed, but also those that are under-expressed in tumours [24,25].
Overall, we have identified PDCD4 as a new lungcancer-associated gene based on its expression incultured cells and in primary tumours. Although thelack of expression suggests a suppressor function,positive evidence for tumour suppression may requirePDCD4 transfection into lung tumour cell lines and asensitive assay for the suppression of cells or tumourgrowth. If the only apparent action of PDCD4 is asa lung-tumour suppressor, this gene may constitute auseful molecular target for lung cancer prevention ormay lead to improved therapeutic modalities for thiscommon disease. The mechanism(s) of modulation ofPDCD4 expression in human lung cancer remains tobe investigated. Nonetheless, the result of our studysuggests that loss or reduction of PDCD4 is a commonmolecular abnormality in lung cancer and is associatedwith tumour progression. Additionally, PDCD4 maybe a useful prognostic factor for the prediction ofdisease outcome for patients with lung cancer.
Acknowledgements
We are particularly grateful to Dr YW Yu for constructing thetissue microarrays. We thank Dr K Schluns for ideas and helpin the statistical analysis. The excellent technical assistanceof Manuela Pacyna-Gengelbach and Nicole Deutschmann isgratefully acknowledged. This study was supported by theGerman Cancer Society (Deutsche Krebshilfe) and the GermanResearch Foundation (DFG).
References
1. Jemal A, Thomas A, Murray T, Thun M. Cancer statistics. 2002.CA Cancer J Clin 2002; 52: 23–47.
2. Landis SH, Murray T, Bolden S, Wingo PA. Cancer statistics1999. CA Cancer J Clin 1999; 49: 8–31.
3. Strauss GM. The Mayo lung cohort: a regression analysis focusingon lung cancer incidence and mortality. J Clin Oncol 2002; 20:1973–1983.
4. Schrump DS, Nguyen DM. Targets for molecular interventionin multistep pulmonary carcinogenesis. World J Surg 2001; 25:174–183.
5. Garber ME, Troyanskaya OG, Schluens K, et al. Diversity of geneexpression in adenocarcinoma of the lung. Proc Natl Acad Sci US A 2001; 98: 13784–13789.
6. Difilippantonio S, Chen Y, Pietas A, et al. Gene expressionprofiles in human non-small and small cell lung cancer. EuropeanJournal of Cancer (in press).
7. Matsuhashi S, Yoshinaga H, Yatsuki H, Tsugita A, Hori K.Isolation of a novel gene from a human cell line with Pr-28 MAbwhich recognizes a nuclear antigen involved in the cell cycle. ResCommun Biochem Cell Mol Biol 1997; 1: 109–120.
8. Shibahara K, Asano M, Ishida Y, Aoki T, Koike T, Honjo T.Isolation of a novel mouse gene MA-3 that is induced uponprogrammed cell death. Gene 1995; 166: 297–301.
9. Onishi Y, Hashimoto S, Kizaki H. Cloning of the TIS genesuppressed by topoisomerase inhibitors. Gene 1998; 215:453–459.
10. Schlichter U, Burk O, Worpenberg S, Klempnauer KH. Thechicken Pdcd4 is regulated by v-Myb. Oncogene 2001; 20:231–239.
11. Cmarik JL, Min H, Hegamyer G, et al. Differentially expressedprotein PDCD4 inhibits tumor promoter-induced neoplastictransformation. Proc Natl Acad Sci U S A 1999; 96: 14037–14042.
12. Yang HS, Jansen AP, Nair R, et al. A novel transformationsuppressor, PDCD4, inhibits AP-1 transaction but not NF-κB orODC transactivation. Oncogene 2001; 20: 669–676.
13. Sobin LH, Wittekind Ch (eds). TNM Classification of MalignantTumors (5th edn). Wiley-Liss: New York, 1997.
14. Petersen S, Heckert C, Rudolf J, et al. Gene expression profilingof advanced lung cancer. Int J Cancer 2000; 86: 512–517.
15. Yoshinaga H, Matsuhashi S, Fujiyama C, Masaki Z. Novel humanPDCD4 (H731) gene expression in proliferative cells is expressedin the small duct epithelial cells of the breast as revealed by ananti-H731 antibody. Int Pathol 1997; 49: 1067–1077.
16. Diatchenko L, Lau YF, Campbell AP, et al. Suppression subtrac-tive hybridization: a method for generating differentially regulatedor tissue-specific cDNA probes and libraries. Proc Natl Acad SciU S A 1996; 93: 6025–6030.
17. Zhang L, Zhou W, Velculescu VE, et al. Gene-expression profilesin normal and cancer cells. Science 1997; 276: 1268–1272.
18. Volm M, Koomagi R. Relevance of proliferative and pro-apoptoticfactors in non-small-cell lung cancer for patient survival. Br JCancer 2000; 82: 1747–1754.
19. Sasaki H, Yukiue H, Kobayashi Y, et al. Expression of thesensitive to apoptosis gene, SAG, as a prognostic marker innonsmall cell lung cancer. Int J Cancer 2001; 95: 375–377.
20. Leupold JH, Colburn NH, Yang HS, et al. First evidence for thenew tumor suppressor PDCD4 as a regulator of u-APR, aninvasion-related gene. American Association for Cancer Research93rd Annual Meeting 2002, #3083.
21. Pedersen H, Brunner N, Francis D, et al. Prognostic impact ofurokinase, urokinase receptor, and type 1 plasminogen activatorinhibitor in squamous and large cell lung cancer tissue. CancerRes 1994; 54: 4671–4675.
22. Torhorst J, Bucher C, Kononen J, et al. Tissue microarrays forrapid linking of molecular changes to clinical endpoints. Am JPathol 2001; 159: 2249–2256.
23. Simon R, Struckmann K, Schraml P, et al. Amplification patternof 12q13–q15 genes (MDM2, CDK4, GLI) in urinary bladdercancer. Oncogene 2002; 21: 2476–2483.
24. Bowen C, Bubendorf L, Voeller HJ, et al. Loss of NKX3.1expression in human prostate cancers correlates with tumorprogression. Cancer Res 2000; 60: 6111–6115.
25. Mousses S, Bubendorf L, Wagner U, et al. Clinical validation ofcandidate genes associated with prostate cancer progression in theCWR22 model system using tissue microarrays. Cancer Res 2002;62: 1256–1260.
Copyright 2003 John Wiley & Sons, Ltd. J Pathol 2003; 200: 640–646.