Embed Size (px)
Citation preview
Lower Extremity Contractures and Hip
Dysplasia in SMA
David A. Spiegel, M.D. Children’s Hospital of Philadelphia
Associate Professor of Orthopaedic Surgery University of Pennsylvania School of Medicine
Context
• Flaccid, progressive, proximal, LE • Phenotype varies • Promising strategies, alter the natural history – Gene therapy (AAV9) – SMN2 splicing modulation
• Challenging convention
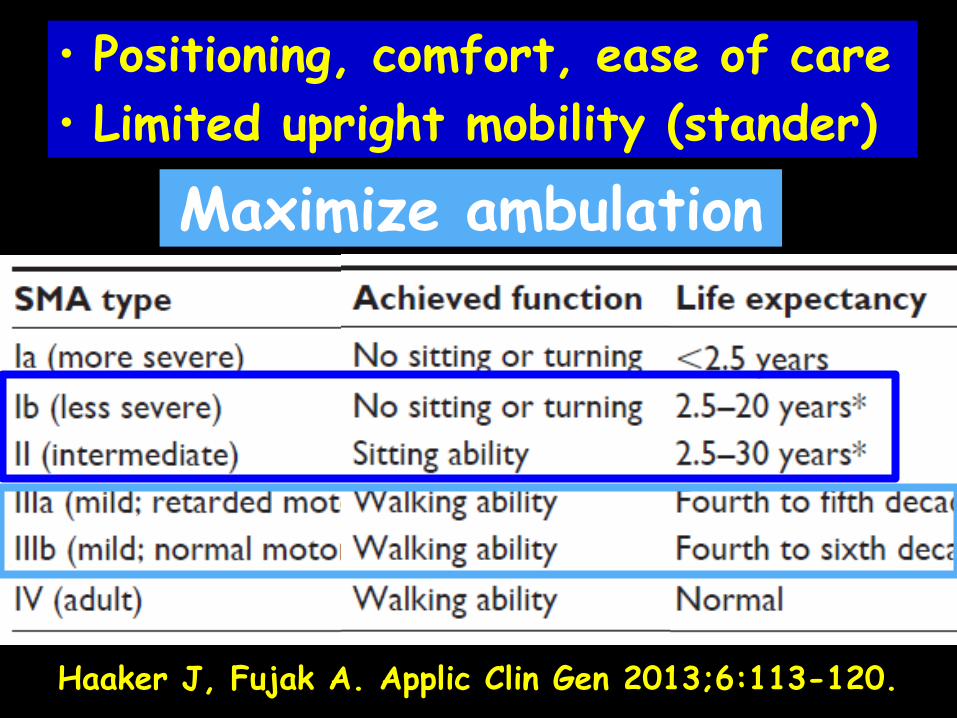
Haaker J, Fujak A. Applic Clin Gen 2013;6:113-120.
• Positioning, comfort, ease of care • Limited upright mobility (stander)
Maximize ambulation
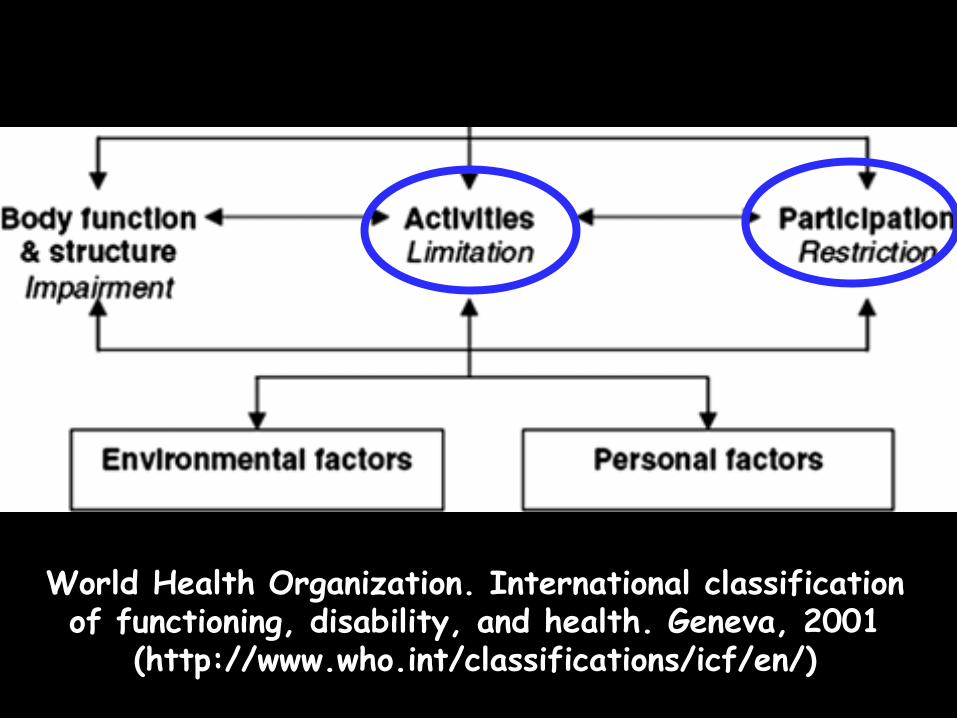
World Health Organization. International classification of functioning, disability, and health. Geneva, 2001
(http://www.who.int/classifications/icf/en/)

Decision Making
“The Boy with a Clubfoot”
Jusepe de Ribera (1642)
“The Clubfoot” Jusepe de Ribera (1623)
• What we see versus what pt/family sees
• Establish realistic, functional goals
• Proactive versus reactive
Contractures
• Why? Denervation/weakness, immobilization/positioning • What? Contractile Tissue ( connective tissue) Connective tissue (lose extensibility) Joint (fibrofatty connective tissue) Farmer SE, James M. Disability and Rehabilitation 2001;23:549.
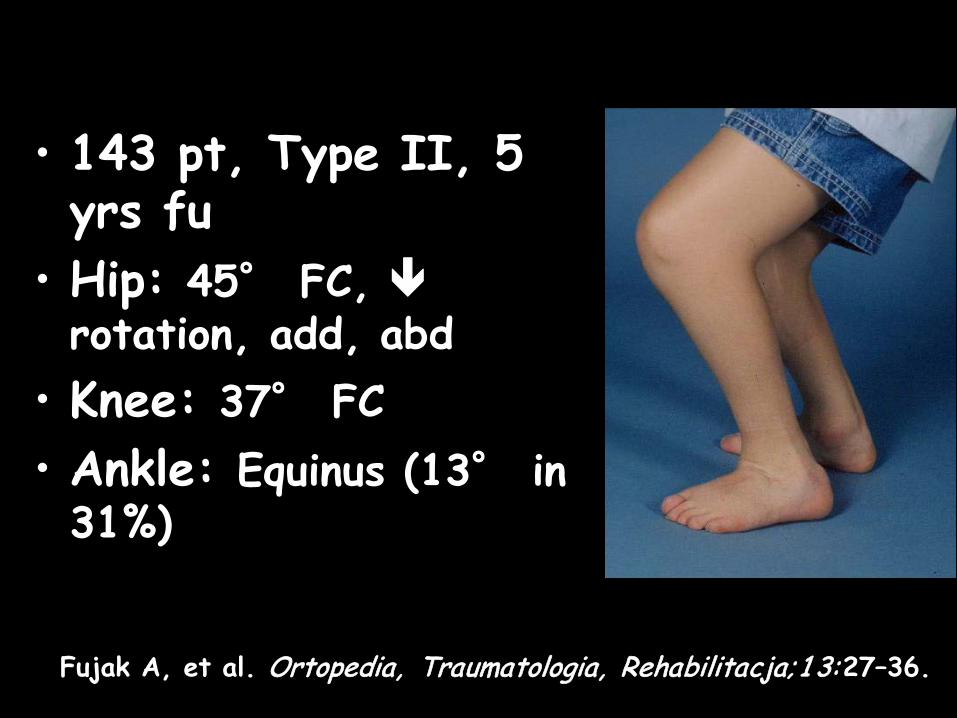
• 143 pt, Type II, 5 yrs fu
• Hip: 45° FC, rotation, add, abd
• Knee: 37° FC • Ankle: Equinus (13° in 31%)
Fujak A, et al. Ortopedia, Traumatologia, Rehabilitacja; 1 3:27–36.
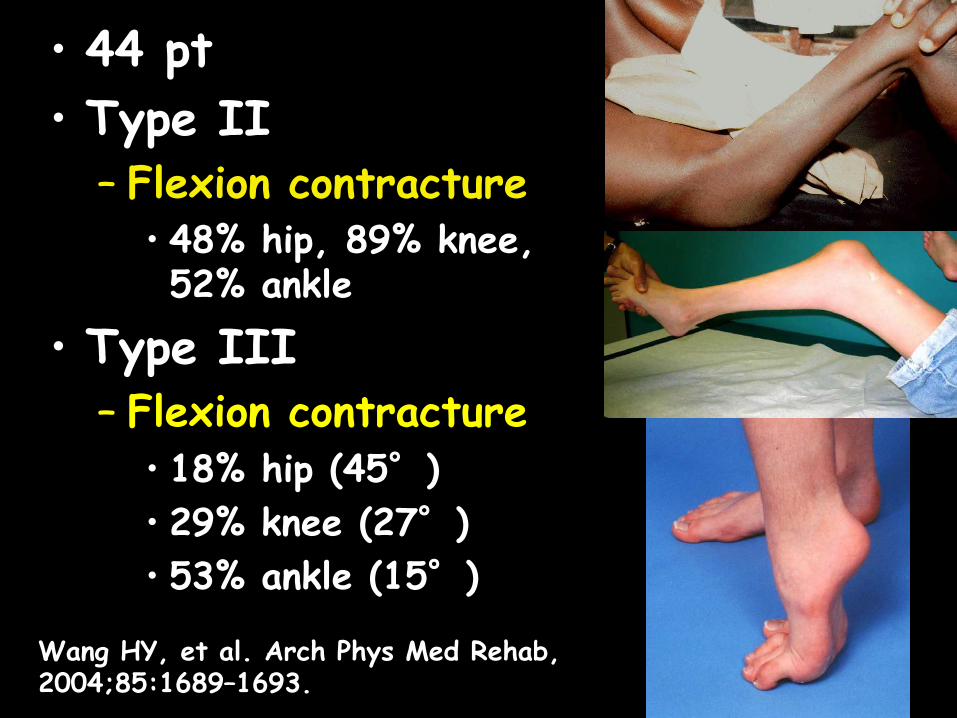
• 44 pt • Type II
– Flexion contracture • 48% hip, 89% knee, 52% ankle
• Type III – Flexion contracture
• 18% hip (45°) • 29% knee (27°) • 53% ankle (15°) Wang HY, et al. Arch Phys Med Rehab,
2004;85:1689–1693.
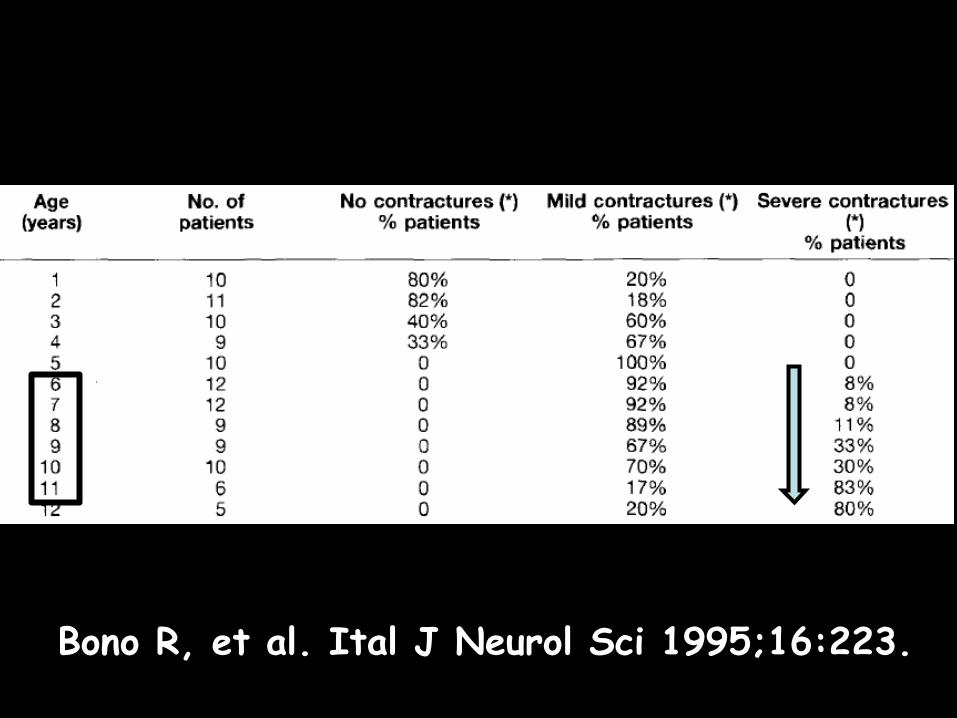
Bono R, et al. Ital J Neurol Sci 1995;16:223.
Strategy
• Multidisciplinary • Multimodality • Relentless/sustainable
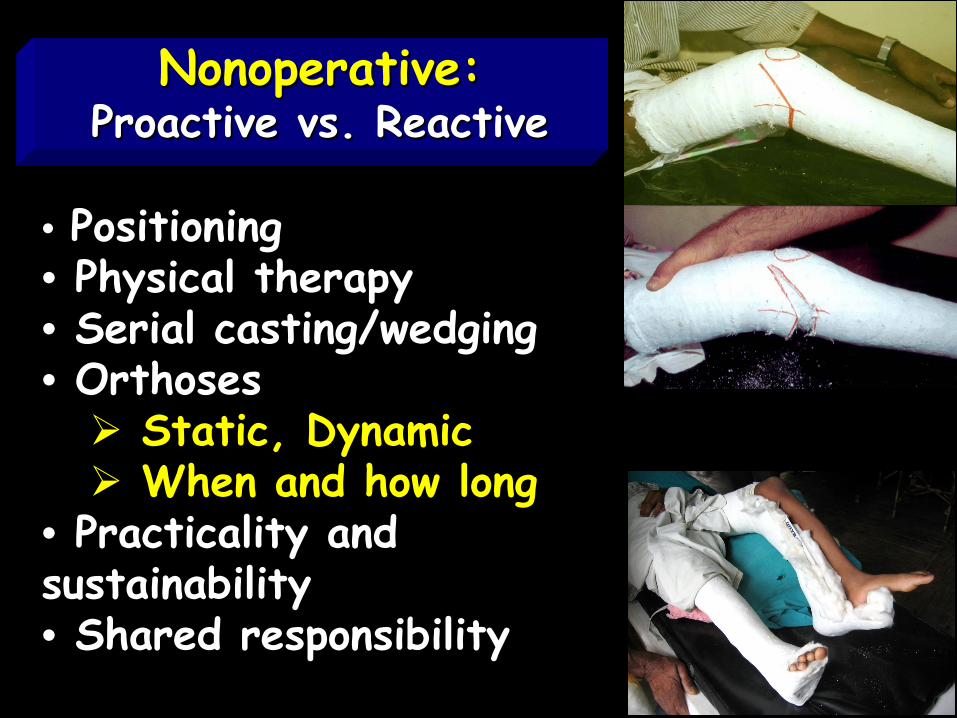
• Positioning • Physical therapy • Serial casting/wedging • Orthoses Static, Dynamic When and how long
• Practicality and sustainability • Shared responsibility
Nonoperative: Proactive vs. Reactive
Reactive:
• Operative – Soft tissue
• Muscle lengthening or release – Osteotomy
• Early mobilization • Risk of losing function • Deterioration/recurrence over time

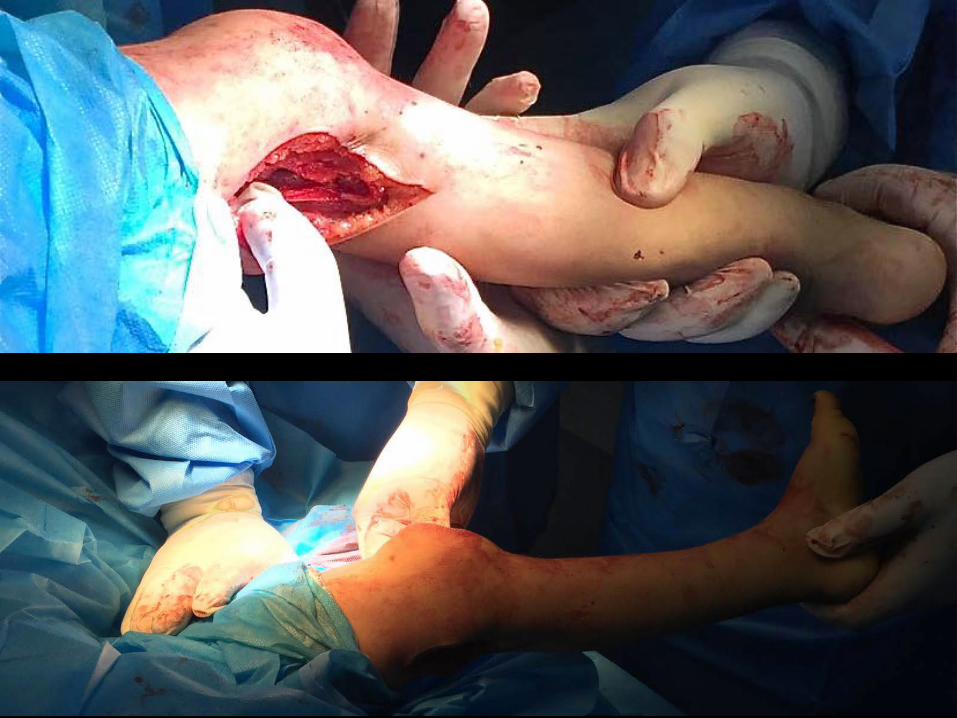
Hip Flexion Contracture
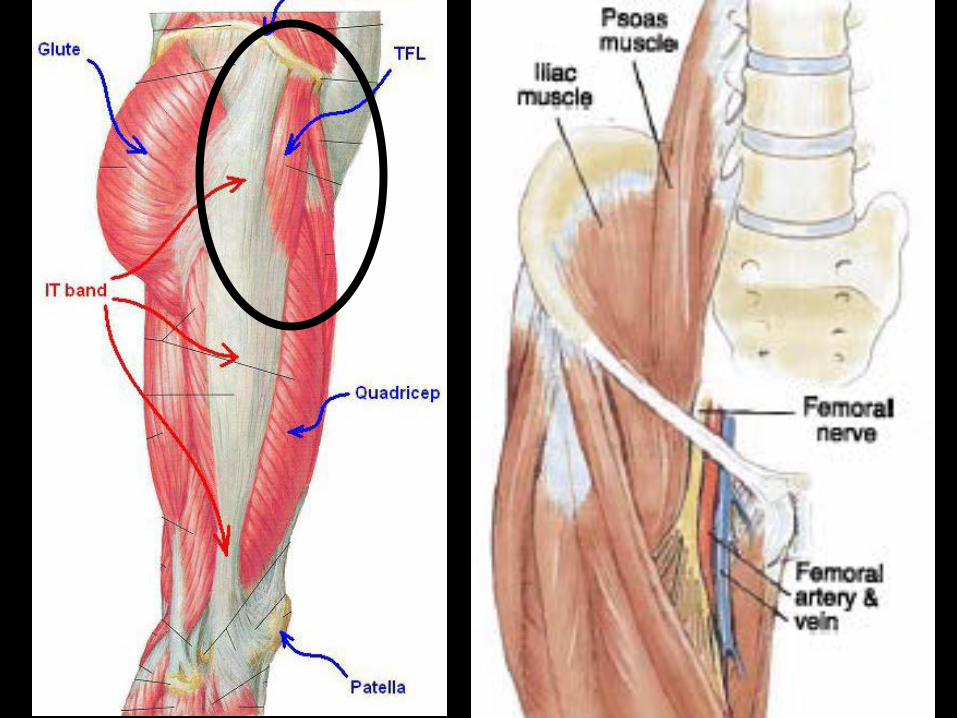
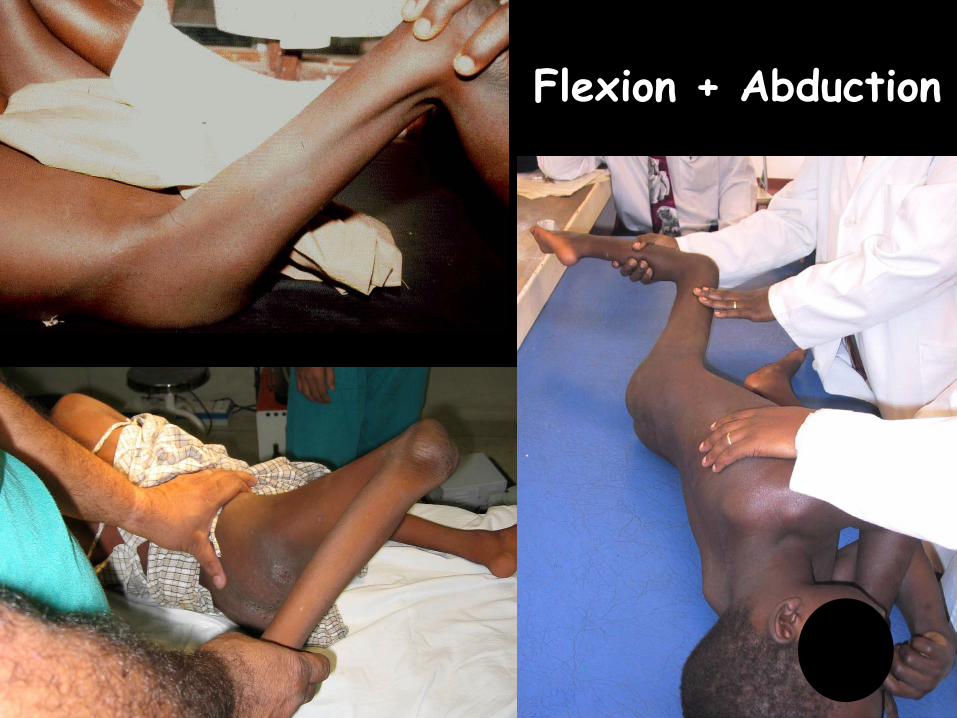
Flexion + Abduction
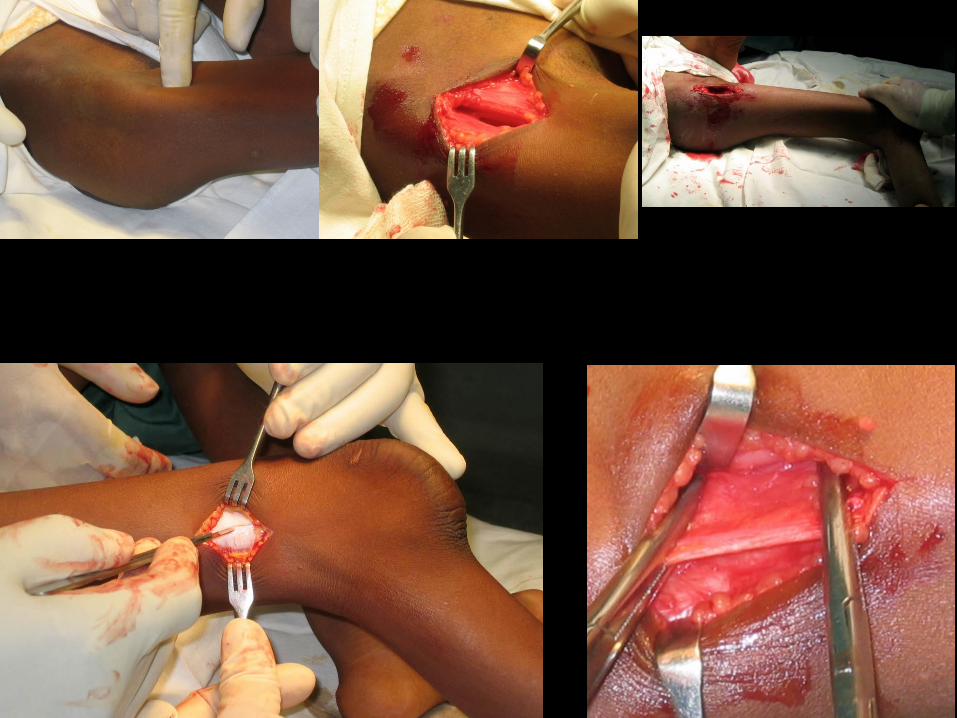


• Stretch casting • Soft tissue lemgthening/release – Hamstrings – Posterior capsule
• “Guided growth” • Extension osteotomy
Knee Flexion Contracture

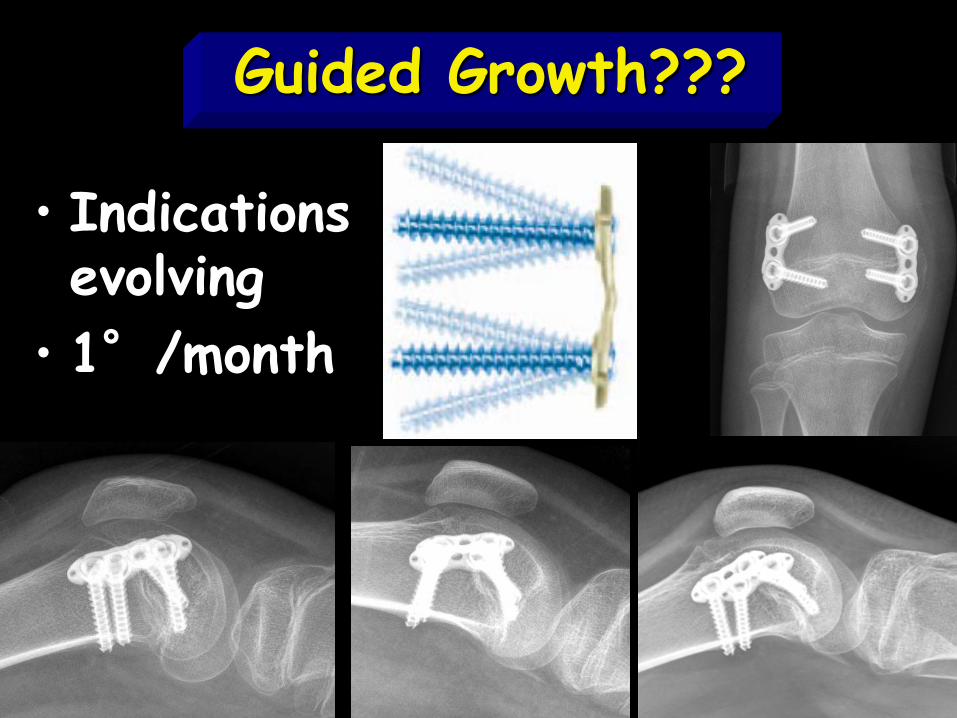
Guided Growth???
• Indications evolving
• 1°/month
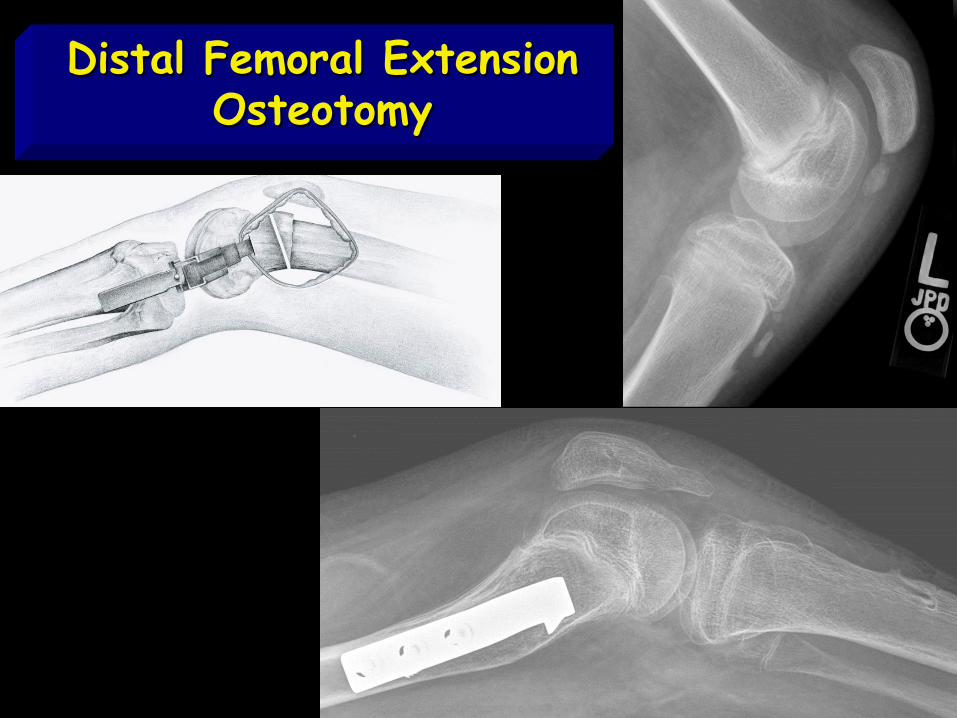
Distal Femoral Extension Osteotomy


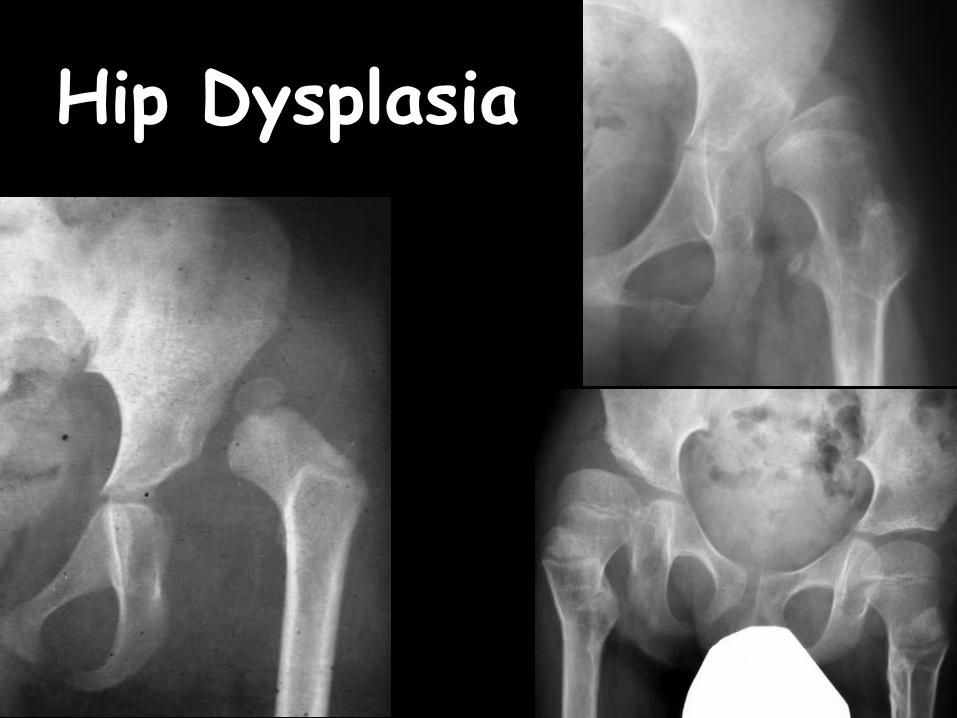
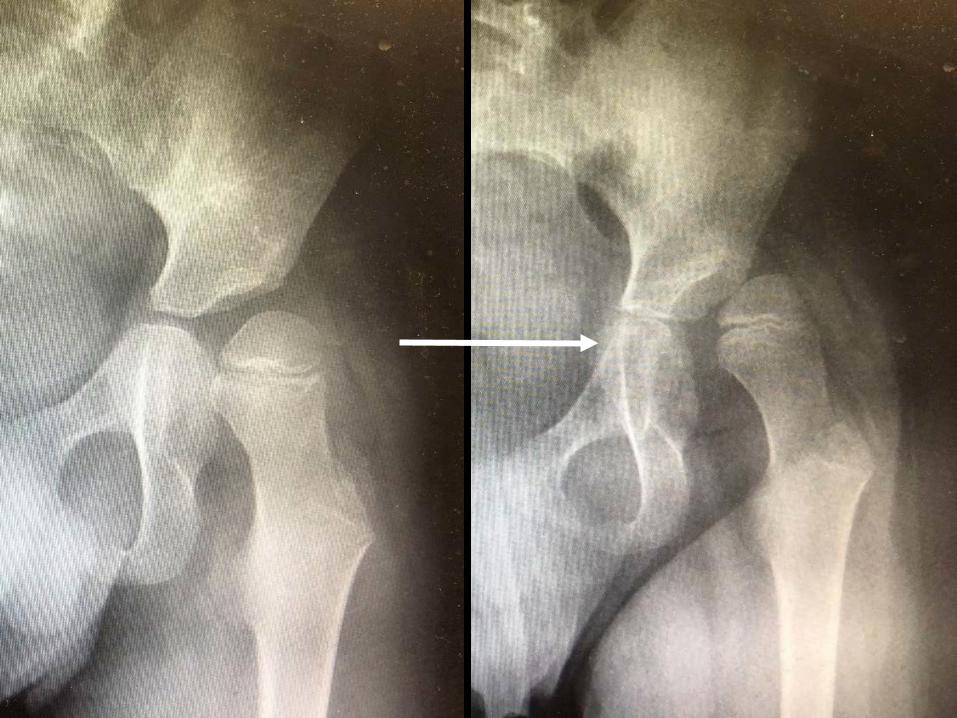
Hip Dysplasia
• Subluxation and dislocation very common, II > III
• Pain/functional consequences rare • Pathologic anatomy? • Reactive rather than proactive
Haaker J, Fujak A. Applic Clin Gen 2013;6:113-120. Sporer SM, Smith BG. J Pediatr Ortho 23:10-14. Thompson CE, Larsen LJ. J Pediatr Ortho 1990;10:638-641. Evans Zenios M, et al. JBJS [Br] 2005;87:1541-1544
Hip: What we think we know
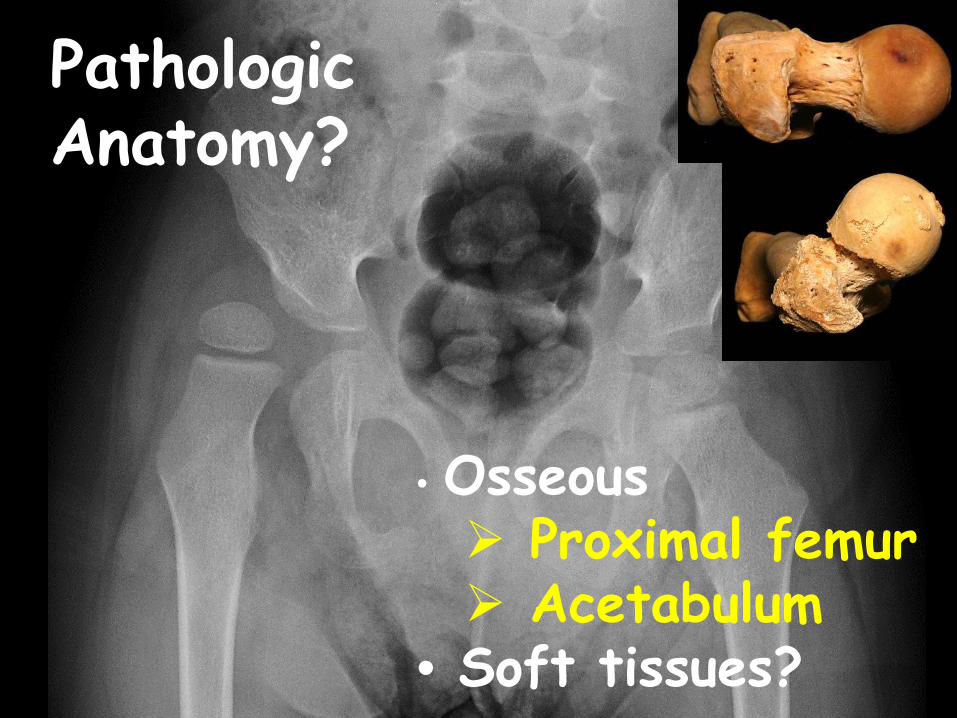
Pathologic Anatomy?
• Osseous Proximal femur Acetabulum
• Soft tissues?
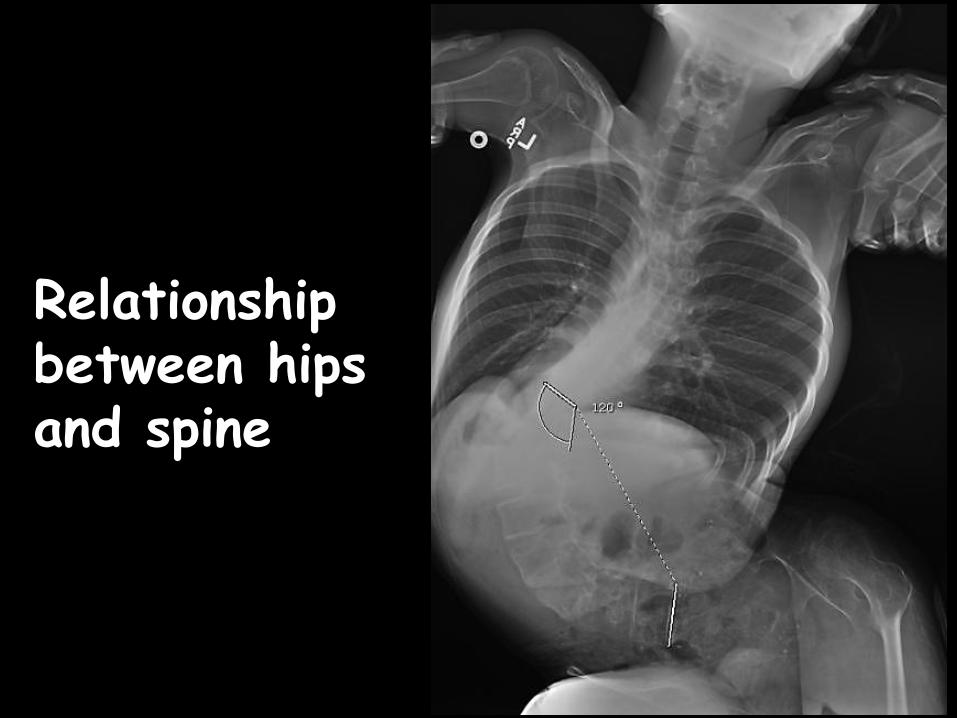
Relationship between hips and spine
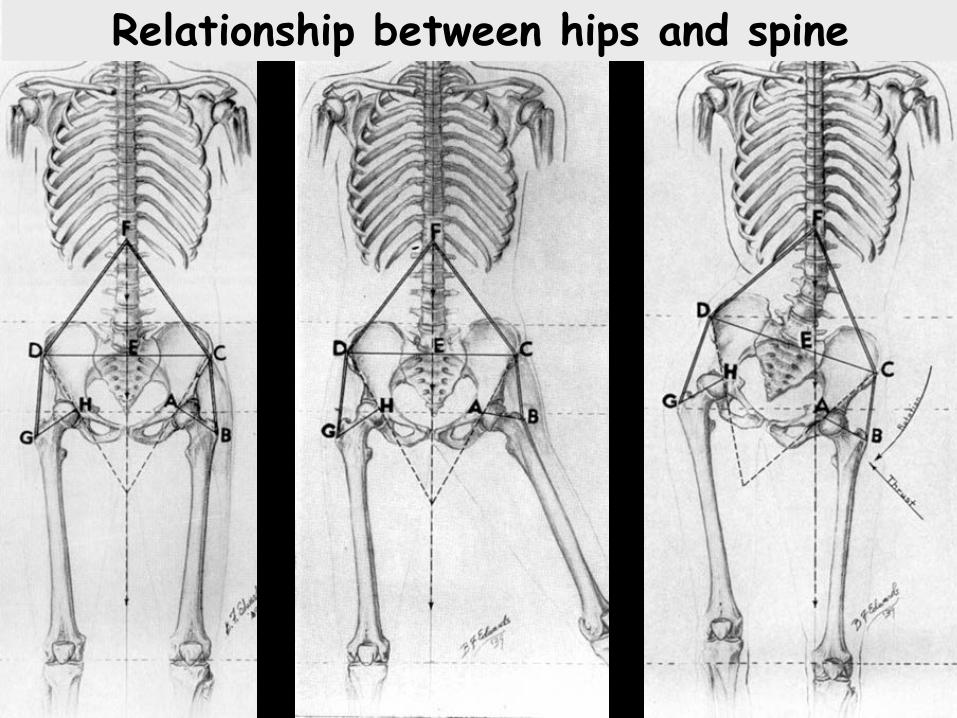
Relationship between hips and spine
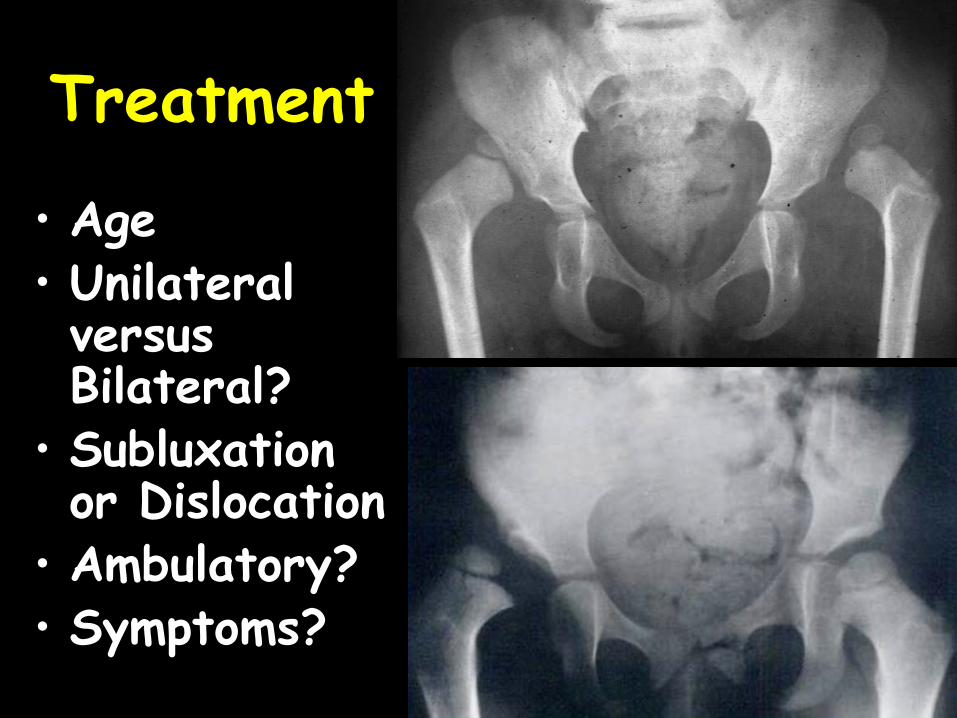
• Age • Unilateral versus Bilateral?
• Subluxation or Dislocation
• Ambulatory? • Symptoms?
Treatment
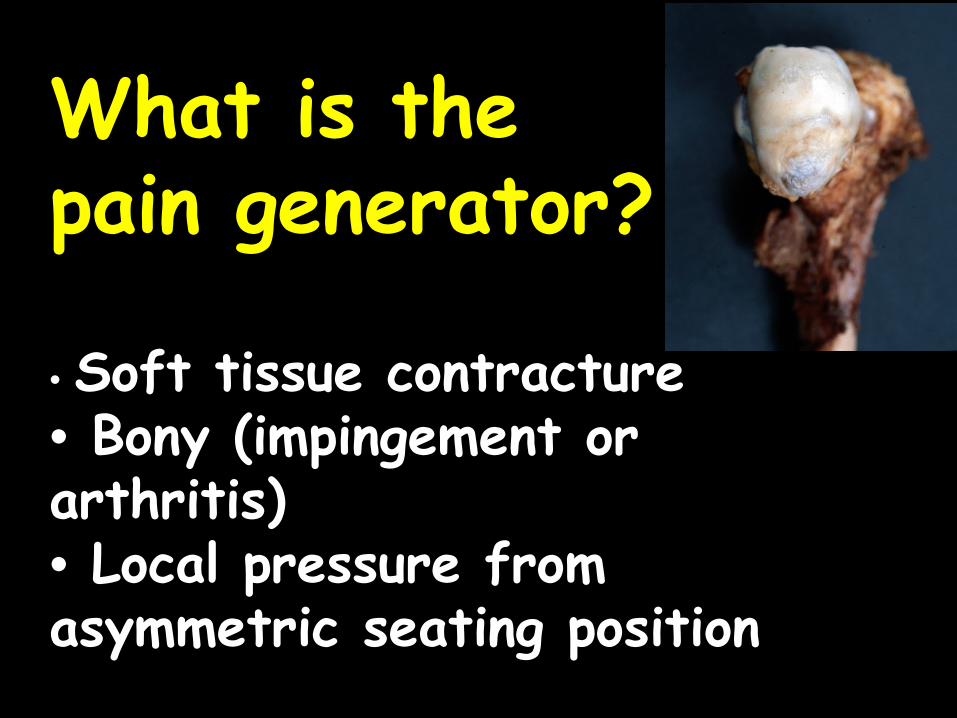
What is the pain generator?
• Soft tissue contracture • Bony (impingement or arthritis) • Local pressure from asymmetric seating position
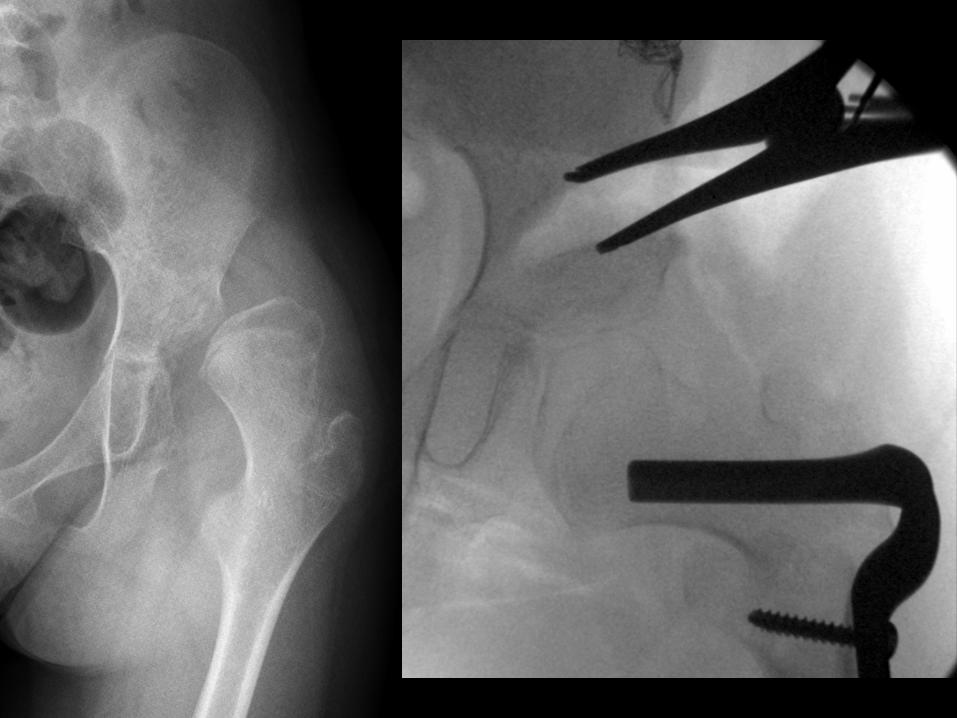
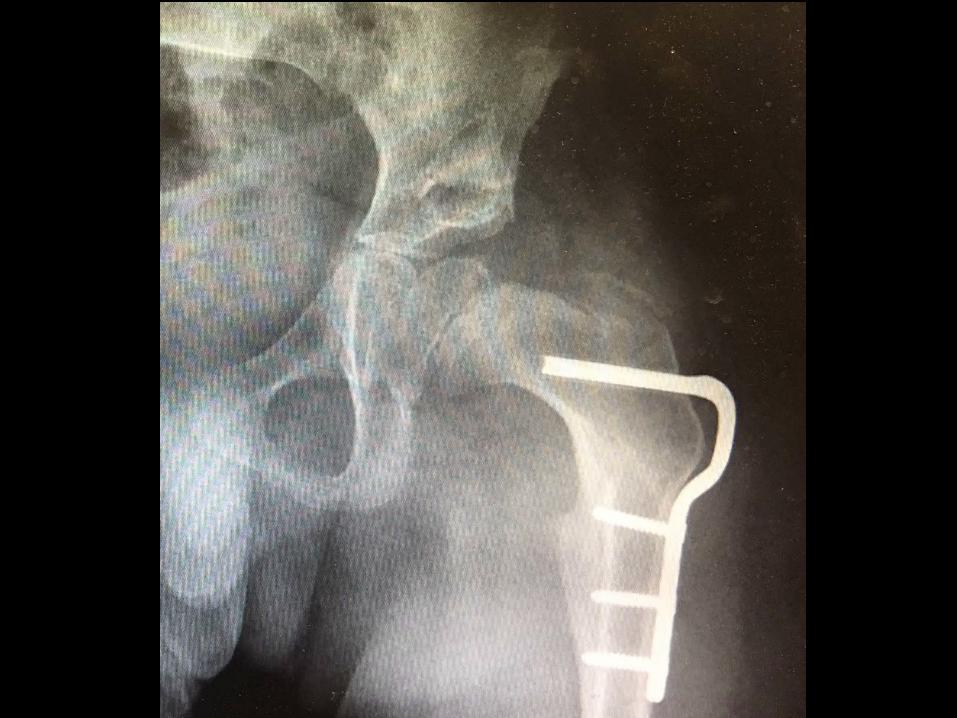
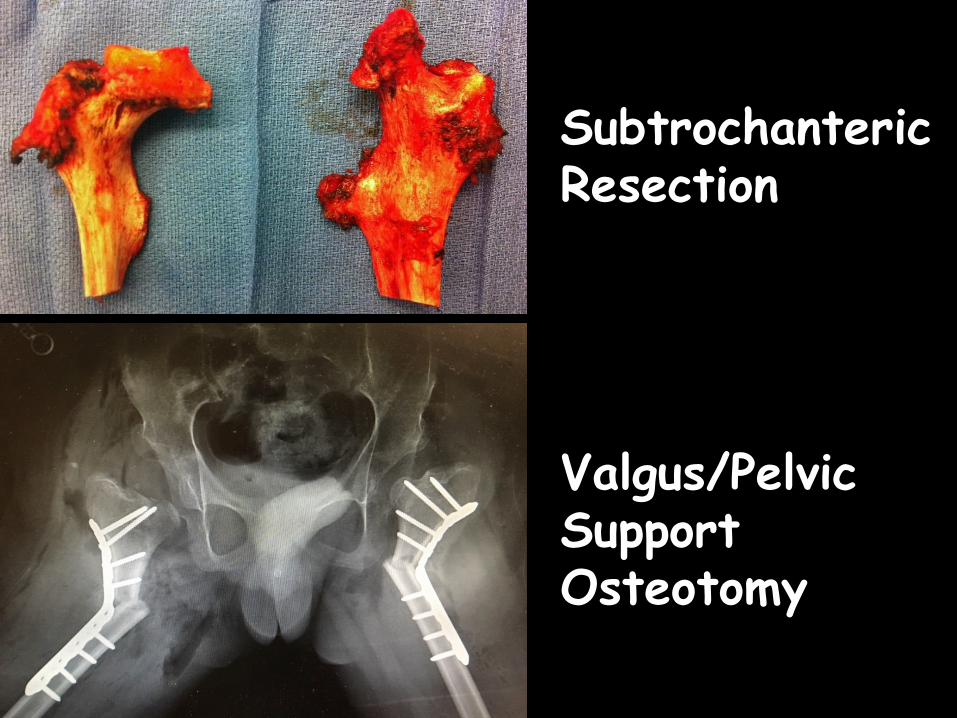
Subtrochanteric Resection
Valgus/Pelvic Support Osteotomy












![Functional Reconstruction of Post-Burn Hand Contractures · 39% of burn injuries involve the upper extremity, three while in severe burn cases, 80% of cases result in hand contracture.[4]](https://img.pdfslide.net/doc/110x75/5f0df88e7e708231d43cfbc4/functional-reconstruction-of-post-burn-hand-39-of-burn-injuries-involve-the-upper.jpg)