Embed Size (px)
Citation preview

Lp(a) hyperlipoproteinemia
Rossella Marcucci Malattie Aterotrombotiche
Università degli Studi di Firenze
18 dicembre 2015

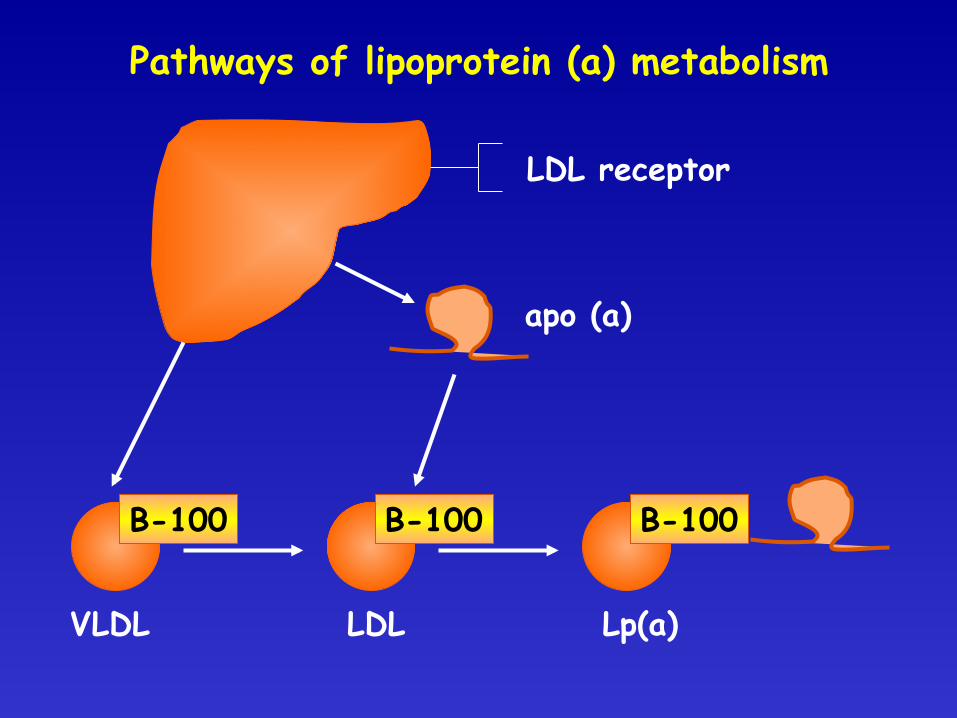
Pathways of lipoprotein (a) metabolism
LDL receptor
apo (a)
VLDL LDL Lp(a)
B-100 B-100 B-100

CATABOLISM OF LIPOPROTEIN (a)
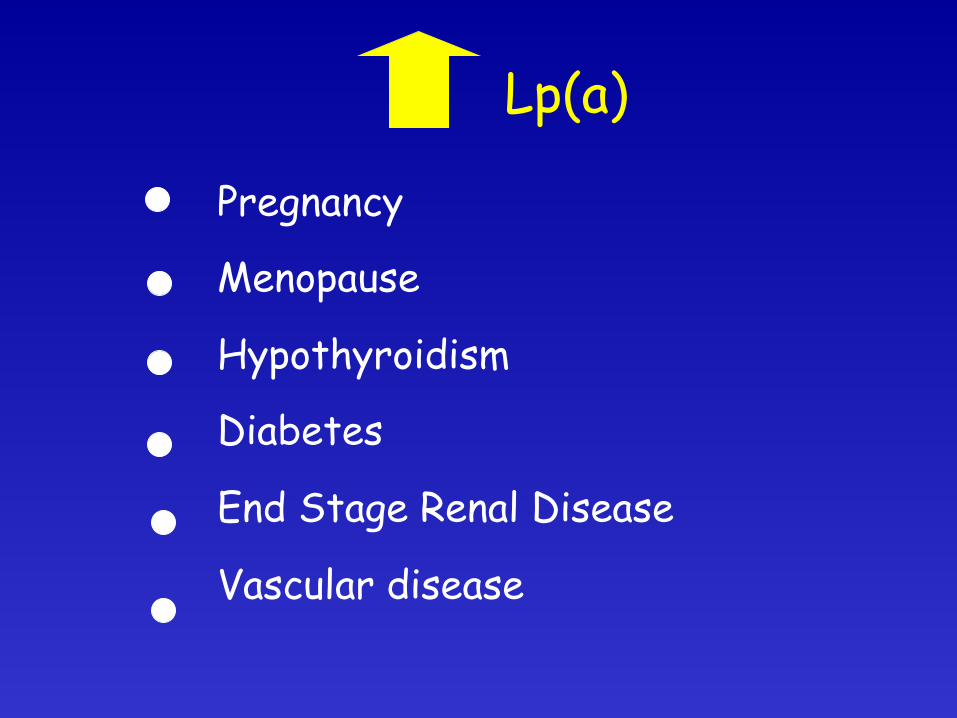
Lp(a)
Pregnancy Menopause Hypothyroidism Diabetes End Stage Renal Disease Vascular disease

Lp(a)
Hepatic Cirrhosis HRT Thyroid Hormones

Lp(a) in relation to age and sex Framingham Offspring Study
Men (n=1,284) Women (n=1,394) Age n Lp(a) (mg/dl) n Lp(a) (mg/dl) p* 20-29 34 11.3±12.4 23 10.6±11.7 NS
30-39 245 13.5±14.3 279 12.8±14.6 NS
40-49 432 14.4±17.2 475 15.1±16.0 NS
50-59 360 15.3±17.7 396 17.0±19.3 NS
60-69 189 13.2±17.1 191 16.2±18.6 NS
70+ 11 17.6±18.8 17 16.6±23.0 NS *=difference between men and women
Jenner et al, Circulation 1993
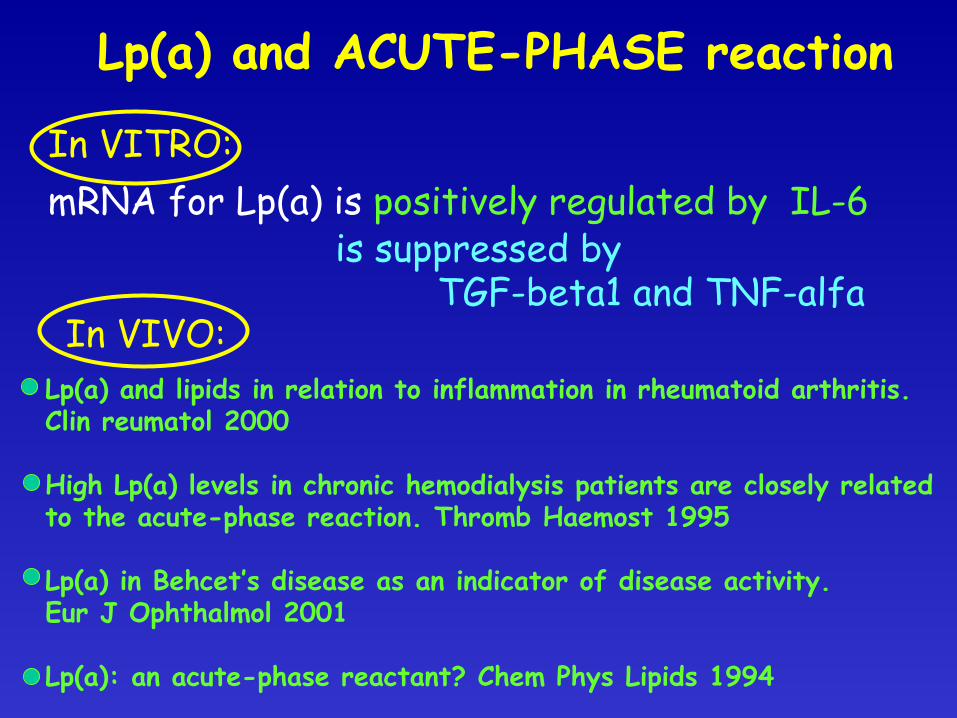
Lp(a) and ACUTE-PHASE reaction
In VITRO: mRNA for Lp(a) is positively regulated by IL-6
is suppressed by TGF-beta1 and TNF-alfa In VIVO:
Lp(a) and lipids in relation to inflammation in rheumatoid arthritis. Clin reumatol 2000 High Lp(a) levels in chronic hemodialysis patients are closely related to the acute-phase reaction. Thromb Haemost 1995 Lp(a) in Behcet’s disease as an indicator of disease activity. Eur J Ophthalmol 2001 Lp(a): an acute-phase reactant? Chem Phys Lipids 1994
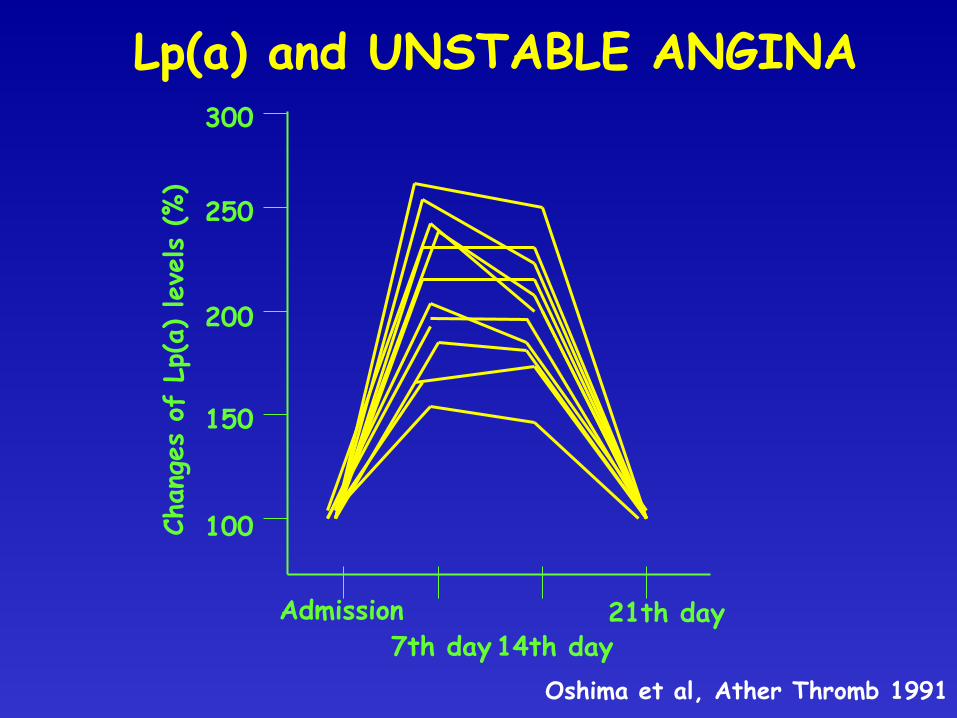
Lp(a) and UNSTABLE ANGINA
Admission 7th day 14th day
21th day
Chan
ges
of L
p(a)
lev
els
(%)
100
150
200
250
300
Oshima et al, Ather Thromb 1991

Lipoprotein (a)
ATHERO-THROMBOSIS
APO (a) APO B-100 Cholesterol

LIPOPROTEIN (a): PROATHEROGENIC PROPERTIES

Lipoprotein (a)
ATHERO-THROMBOSIS
APO (a) APO (b)

LIPOPROTEIN (a): PROTHROMBOTIC PROPERTIES
IV IV IV IV IV IV IV IV IV
V
IV IV IV IV IV V p
p IV III II I T S
S
5’
5’ 3’
3’
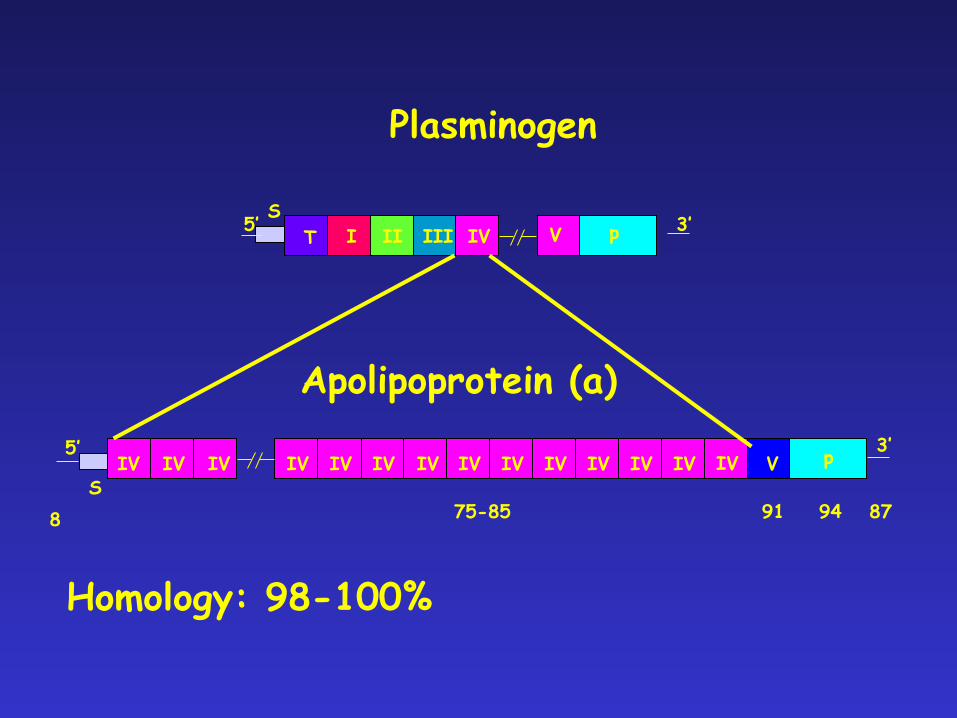
Plasminogen
Apolipoprotein (a)
8 75-85 91 94 87
IV
Homology: 98-100%

Apo(a) isoforms and Lp(a) levels
IV IV IV IV IV IV IV IV IV
IV
IV IV IV IV IV V p
p IV III II I T S
S
5’
5’ 3’
3’
Plasminogen
Apolipoprotein (a)
IV
Kringle 4: classes 1-10 Each class is present as a single copy, except kringle 4 class 2 that is present in multiple copies (from 3 to 30)
many isoforms of apo(a) (from 300 to 800 KD)
LMW= Higher Lp(a) levels / HMW= Lower Lp(a) levels

J Intern Med 2013
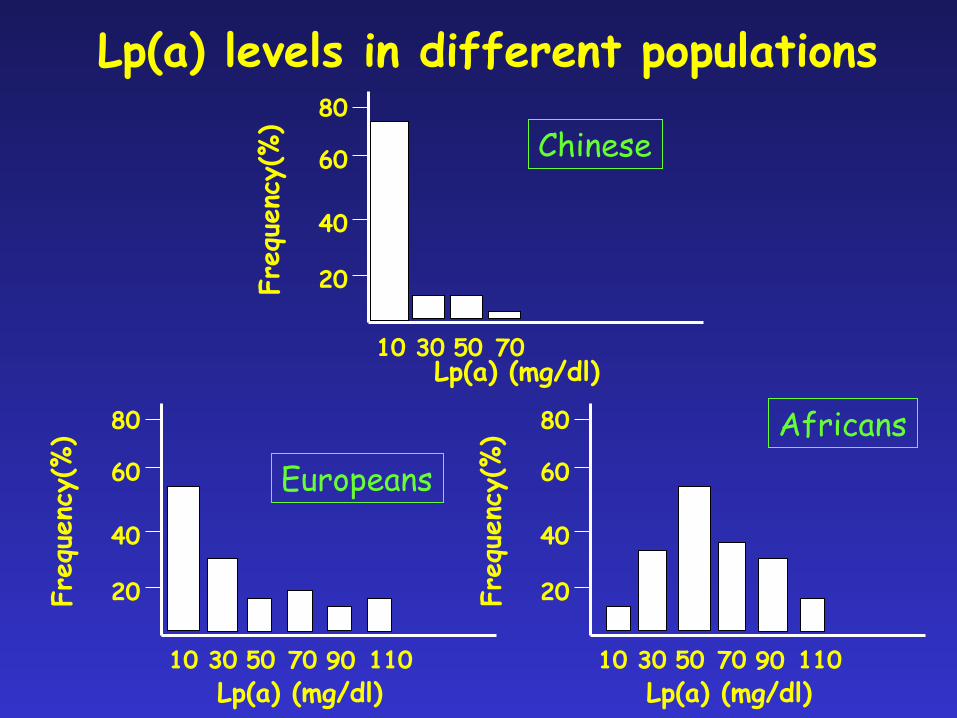
Lp(a) levels in different populations
10 30 50 70
Freq
uenc
y(%)
20
40
60
80 Chinese
10 30 50 70
Freq
uenc
y(%)
20
40
60
80
Europeans
Lp(a) (mg/dl)
90 110 Lp(a) (mg/dl)
10 30 50 70
Freq
uenc
y(%)
20
40
60
80 Africans
90 110 Lp(a) (mg/dl)

CLINICAL STUDIES
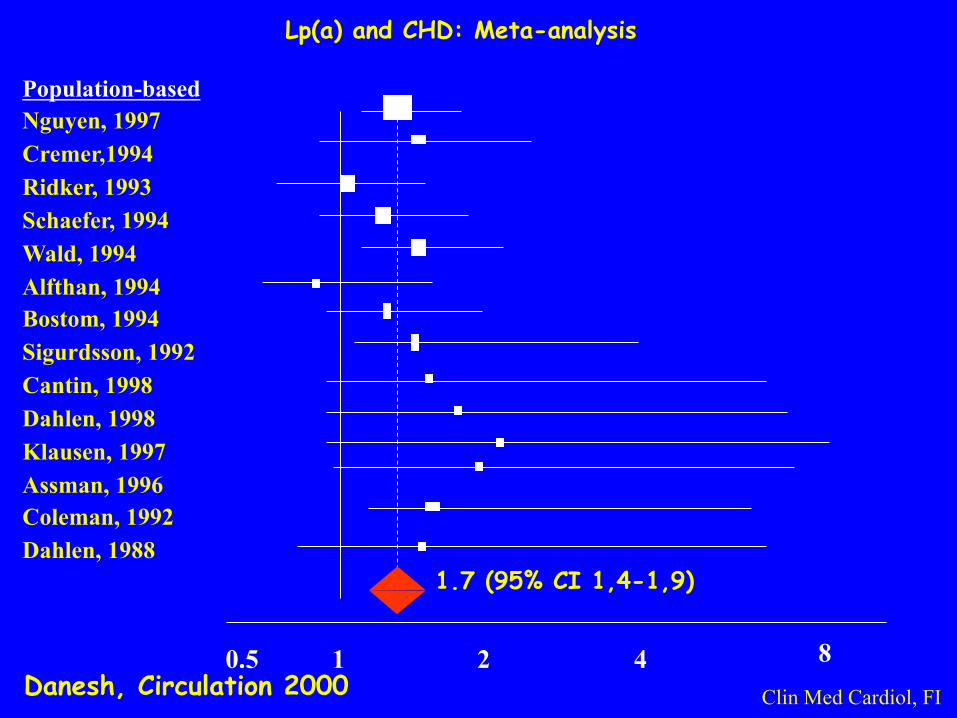
Lp(a) and CHD: Meta-analysis
Population-based Nguyen, 1997 Cremer,1994 Ridker, 1993 Schaefer, 1994 Wald, 1994 Alfthan, 1994 Bostom, 1994 Sigurdsson, 1992 Cantin, 1998 Dahlen, 1998 Klausen, 1997 Assman, 1996 Coleman, 1992 Dahlen, 1988
0.5 1 2 4 8 Danesh, Circulation 2000
1.7 (95% CI 1,4-1,9)
Clin Med Cardiol, FI
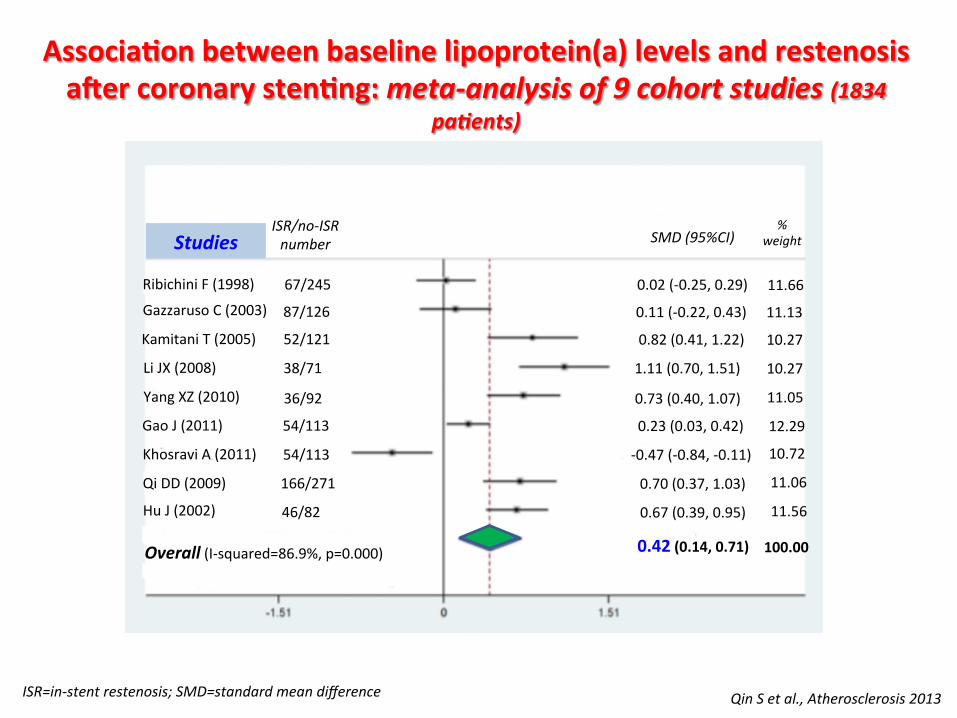
Associa'onbetweenbaselinelipoprotein(a)levelsandrestenosisa5ercoronarysten'ng:meta-analysisof9cohortstudies(1834
pa:ents)
QinSetal.,Atherosclerosis2013
RibichiniF(1998)
GazzarusoC(2003)
KamitaniT(2005)
LiJX(2008)
YangXZ(2010)
GaoJ(2011)
KhosraviA(2011)
QiDD(2009)
HuJ(2002)
Overall(I-squared=86.9%,p=0.000)
StudiesISR/no-ISRnumber
67/245
87/126
52/121
38/71
36/92
54/113
54/113
166/271
46/82
0.02(-0.25,0.29)
0.11(-0.22,0.43)
0.82(0.41,1.22)
1.11(0.70,1.51)
0.73(0.40,1.07)
0.23(0.03,0.42)
-0.47(-0.84,-0.11)
0.70(0.37,1.03)
0.67(0.39,0.95)
0.42(0.14,0.71)
SMD(95%CI)%
weight
11.66
11.13
10.27
10.27
11.05
12.29
10.72
11.06
11.56
100.00
ISR=in-stentrestenosis;SMD=standardmeandifference
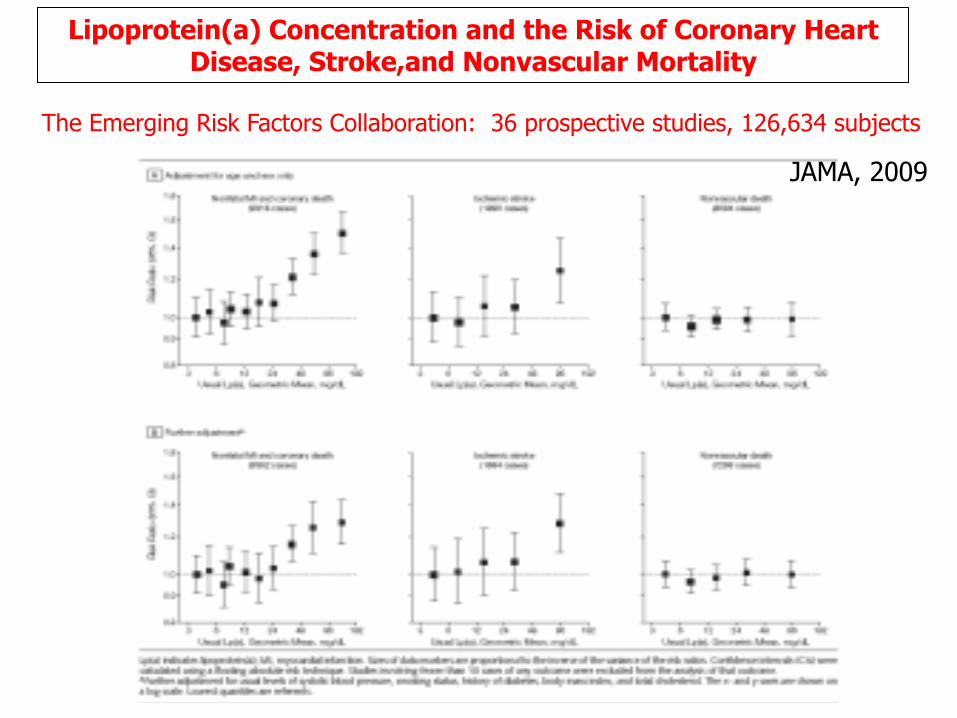
Lipoprotein(a) Concentration and the Risk of Coronary Heart Disease, Stroke,and Nonvascular Mortality
The Emerging Risk Factors Collaboration: 36 prospective studies, 126,634 subjects
JAMA, 2009
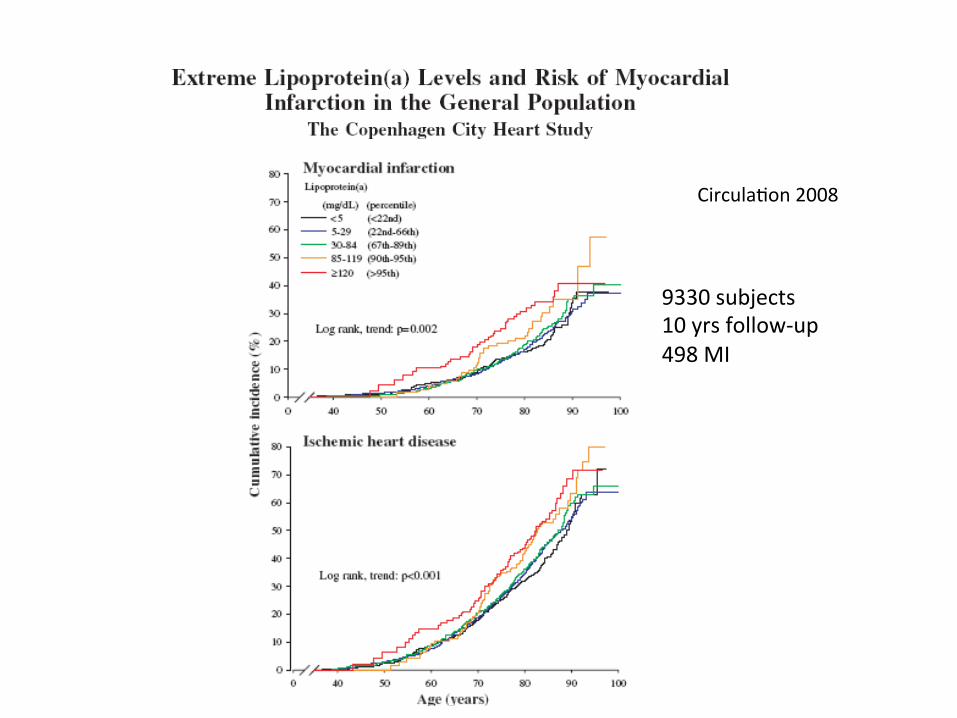
CirculaXon2008
9330subjects10yrsfollow-up498MI
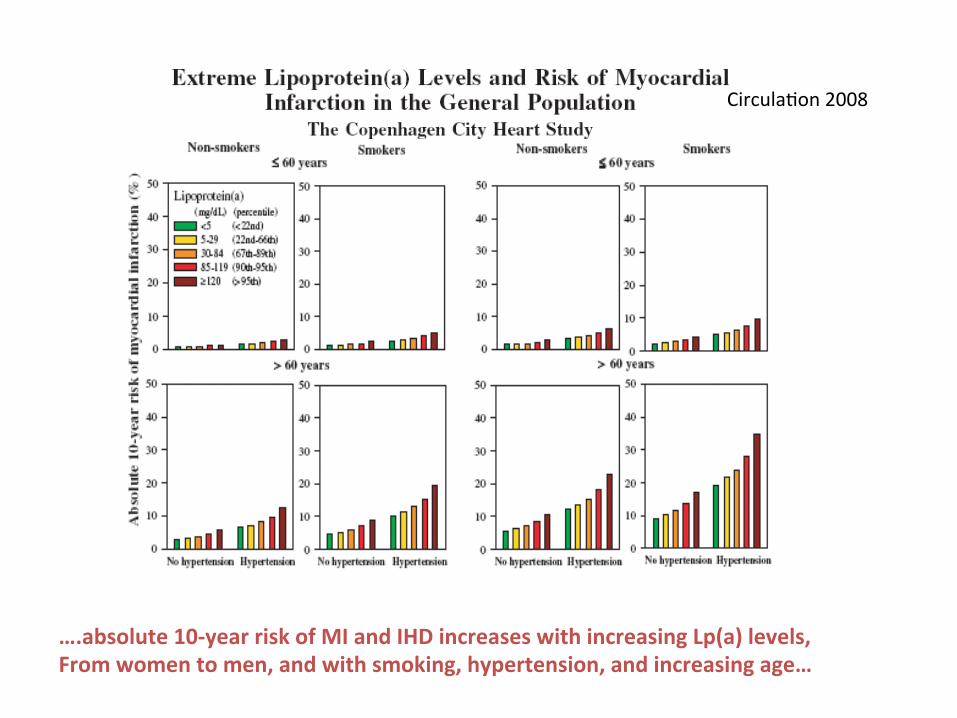
CirculaXon2008
….absolute10-yearriskofMIandIHDincreaseswithincreasingLp(a)levels,Fromwomentomen,andwithsmoking,hypertension,andincreasingage…
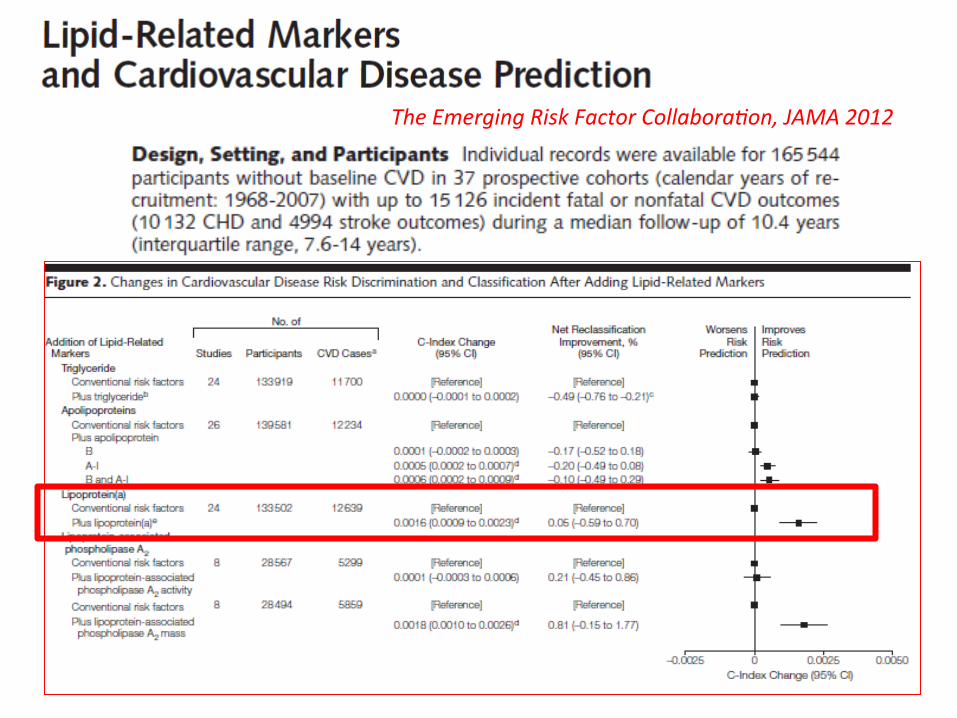
TheEmergingRiskFactorCollaboraOon,JAMA2012

TheEmergingRiskFactorCollaboraOon,JAMA2012

Erqou, JACC 2010

Pa'ents Controls pvalue (n=520) (n=520)
Hcy(mmol/L) 12.7(3-95) 10(6-24) 0.001
PAI-1(IU/ml) 16(1-64) 8(4-38) 0.001
Lp(a)(mg/L) 170(1-2141) 135(7-1390)0.02
HeterozygosityforFactorVLeiden20(3.8%) 20(3.8%) ns
HeterozygosityforFactorIIG20210A 21(4.0%) 19(3.6%) ns
HomozygosityforPAI-14G/5G 166(31.9%) 156(30.0%) ns
ThrombophilicriskfactorsinCADpa'ents
Dataaremedianandrangeornumber(%).PAI-1=plasminogenacXvatorinhibitortype1.
Marcuccietal.,Heart2006
1 2 3 4 5 6 7 8 9 10
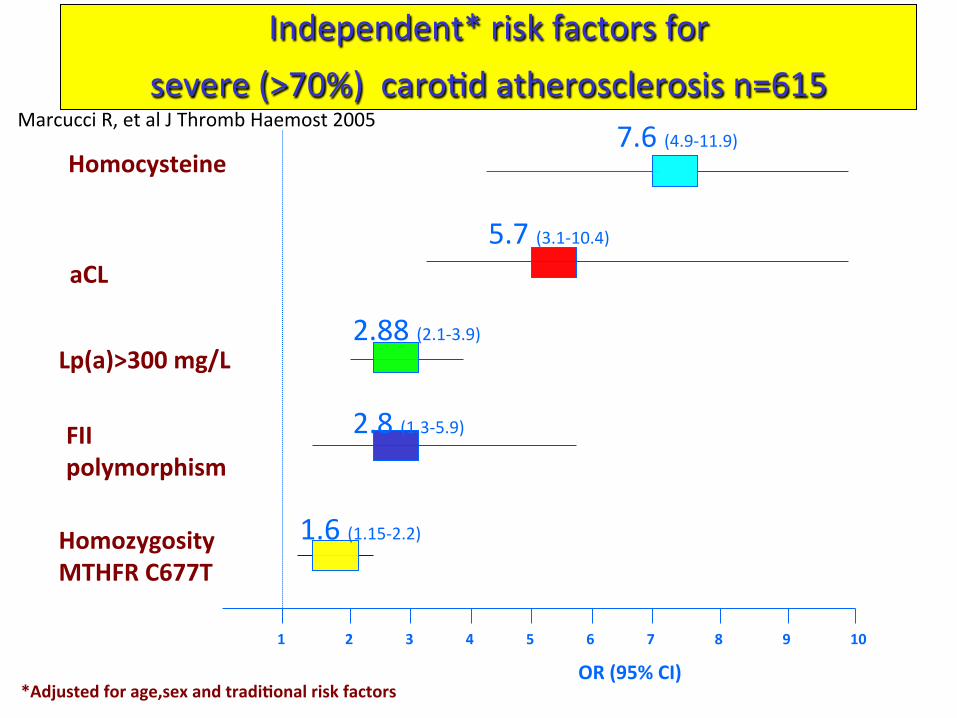
Independent*riskfactorsforsevere(>70%)caroXdatherosclerosisn=615
aCL
OR(95%CI)*Adjustedforage,sexandtradi'onalriskfactors
5.7(3.1-10.4)
2.88(2.1-3.9)
1.6(1.15-2.2)
7.6(4.9-11.9)
HomozygosityMTHFRC677T
Lp(a)>300mg/L
Homocysteine
FIIpolymorphism
2.8(1.3-5.9)
MarcucciR,etalJThrombHaemost2005

0
50
100
150
200
250
300
Patients (n=280) Controls (n=280)
Lp(a)(mg/L) Lp(a)>300mg/L
207
85
p<0.0001
Lipoprotein(a)andPAD
0%
10%
20%
30%
40%
50%
Patients (n=280) Controls (n=280)
14.3%
39.3%
p<0.0001
ClinMedCardFI
SofietalJVascSurg2005
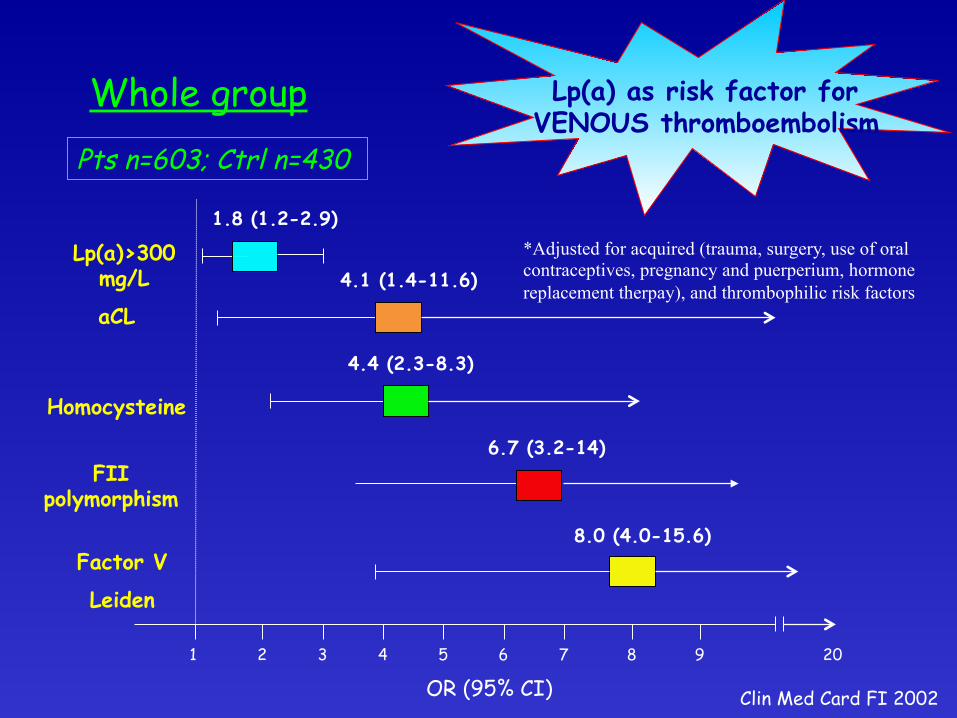
1 2 3 4 5 6 7 8 9 20
Whole group
aCL
Homocysteine
Factor V
Leiden
OR (95% CI)
*Adjusted for acquired (trauma, surgery, use of oral contraceptives, pregnancy and puerperium, hormone replacement therpay), and thrombophilic risk factors 4.1 (1.4-11.6)
4.4 (2.3-8.3)
8.0 (4.0-15.6)
Clin Med Card FI 2002
Lp(a)>300 mg/L
1.8 (1.2-2.9)
Lp(a) as risk factor for VENOUS thromboembolism
Pts n=603; Ctrl n=430
FII polymorphism
6.7 (3.2-14)

Independent Risk Factors for Idiopathic Venous Thromboembolism
(n=341)
Marcucci et al, AM J Med 2003
* multivariate analysis adjusted for acquired (trauma, surgery, use of oral contraceptives, pregnancy and puerperium, hormone replacement therapy), and thrombophilic risk factors
30% (n=101) pts had no thrombophilic factor Among them 35 (35%) had elevated Lp(a) levels In pts with secondary VTE OR for high Lp(a)
was 1.4 (0.7-1.8) ns

IndependentRiskFactorsforRecurrentVenousThromboembolism
(n=136-23%ofthetotalsample)
Marcucci et al, AM J Med 2003
*Adjusted for acquired (trauma, surgery, use of oral contraceptives, pregnancy and puerperium, hormone replacement therapy), and thrombophilic risk factors
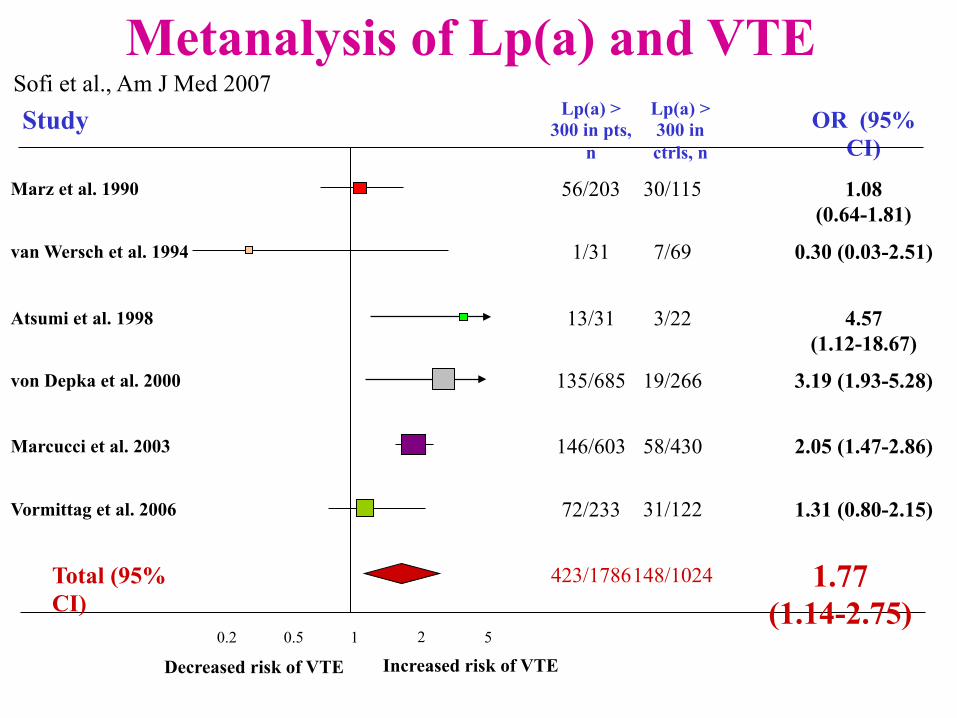
Study OR (95% CI)
Marz et al. 1990
van Wersch et al. 1994
Atsumi et al. 1998
von Depka et al. 2000
Marcucci et al. 2003
0.2 0.5 1 2 5
1.08 (0.64-1.81)
0.30 (0.03-2.51)
4.57 (1.12-18.67)
3.19 (1.93-5.28)
2.05 (1.47-2.86)
1.31 (0.80-2.15)
Total (95% CI)
1.77 (1.14-2.75)
Decreased risk of VTE
Metanalysis of Lp(a) and VTE
Vormittag et al. 2006
Lp(a) > 300 in pts,
n
Lp(a) > 300 in ctrls, n
56/203 30/115
1/31 7/69
13/31 3/22
135/685 19/266
146/603 58/430
72/233 31/122
423/1786 148/1024
Increased risk of VTE
Sofi et al., Am J Med 2007

PHENOTYPE or GENOTYPE?

GENETICEPIDEMIOLOGICSTUDIESANDCAUSALITYLp(a)levelsarepredominantlygene'callydeterminedandnotgreatlyinfluencedbylifestylefactorsandmayvaryupto1000–foldbetweenindividuals.TheLPAgeneonchromosome6codesfortheapo(a)moietyoflipoprotein(a)
PLG (6q26)
LPA (6q26-q27)

GENOME-WIDEHAPLOTYPEASSOCIATIONSTUDYIDENTIFIESTHESLC22A3-LPAL2-LPAGENECLUSTERASARISKLOCUSFORCAD
HaplotypicORforCADassociatedwithCCTCandCTTGhaplotypesderived
fromrs2048327,rs3127599andrs10755578onchromosome6q26-q27
Tregouet et al., Nature Genetics 2009
Clarkeetal.,NEJM2009
48,742 single-nucleoXde polymorphisms (SNPs) in 2,100candidategenes
• 3,145caseswithcoronarydisease• 3,352controls
ReplicaXonwastested in3 independentpopulaXons involving4,486addiXonalcasesand4,594controls
Threechromosomalregion(6–9-1)werestronglyassociatedwiththeriskofcoronarydisease.TheLPAlocuson6q26-27hadthestrongestassociaXon

Clarkeetal.,NEJM2009
Gene'cvariantsassociatedwithLp(a),lipoproteinlevelandcoronarydisease

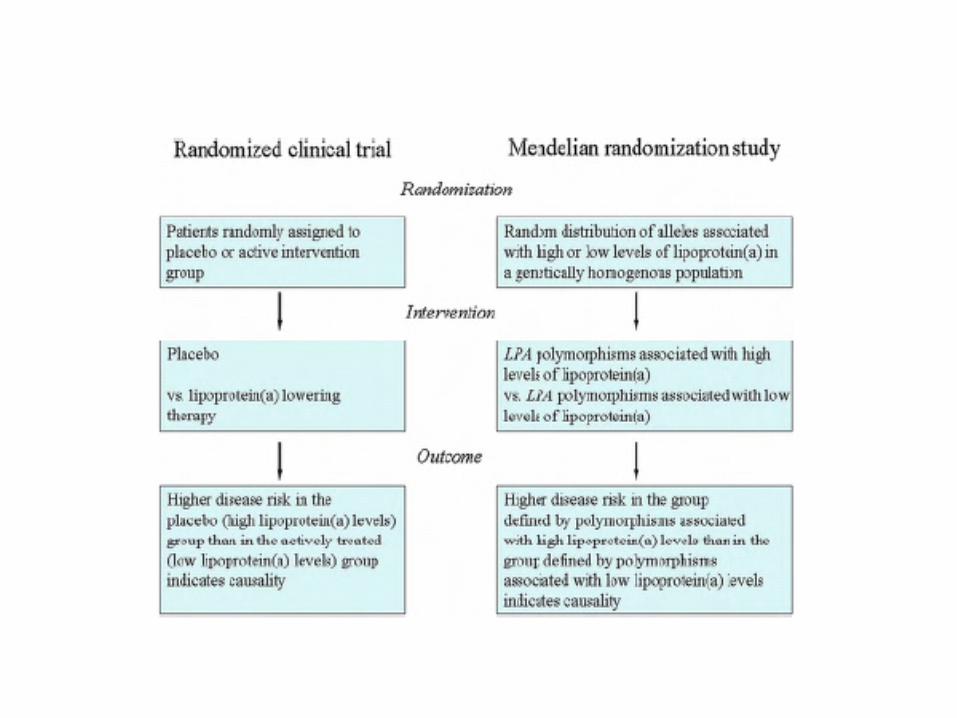
GENETICEPIDEMIOLOGICSTUDIESANDCAUSALITYLp(a)levelsarepredominantlygene'callydeterminedandnotgreatlyinfluencedbylifestylefactorsandmayvaryupto1000–foldbetweenindividuals.TheLPAgeneonchromosome6codesfortheapo(a)moietyoflipoprotein(a).Varia'oninthisgenehasaprofoundeffectonplasmalevelsofLp(a).Ofpar'cularimportanceistheso-calledKIVtype2sizepolymporphismdefinedbyasequencethatmayoccurbetweentwoandmorethan40-'mesperalleledependentonthespecificgenotype.Thispolymorphismdeterminesthesizeoftheexpressedapo(a)THISMAKESLP(a)ANATTRACTIVETARGETFORAMENDELIANRANDOMIZATIONSTUDY

JInternMed2013

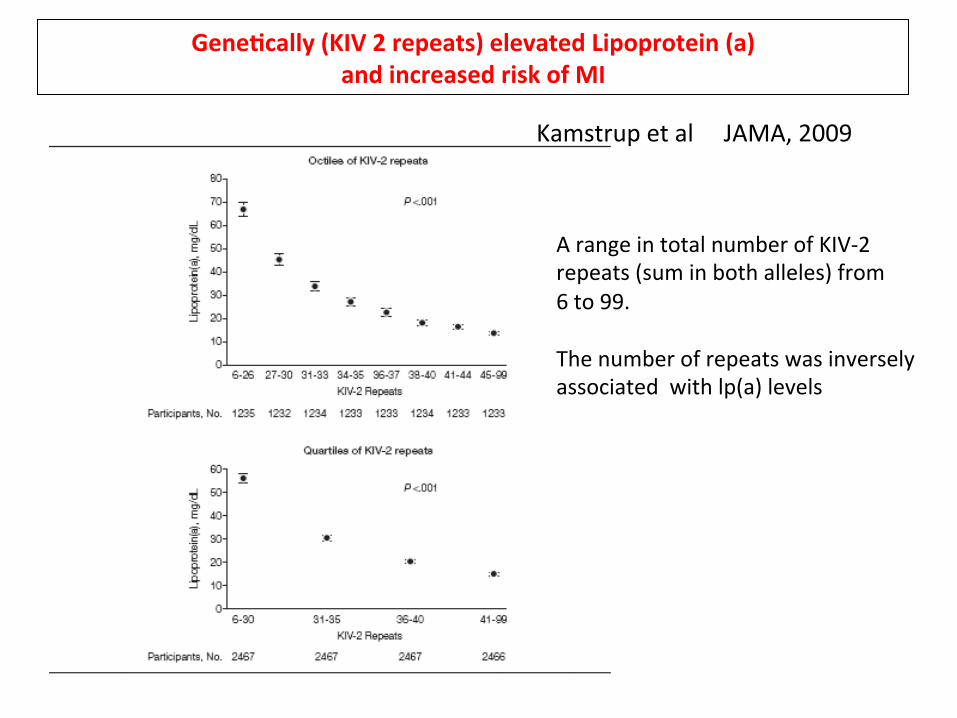
Genetically (KIV 2 repeats) elevated Lipoprotein (a) and increased risk of MI
Kamstrup et al JAMA, 2009
Gene'cally(KIV2repeats)elevatedLipoprotein(a)andincreasedriskofMI
KamstrupetalJAMA,2009
ArangeintotalnumberofKIV-2repeats(suminbothalleles)from6to99.Thenumberofrepeatswasinverselyassociatedwithlp(a)levels

Gene'cally(KIV2repeats)elevatedLipoprotein(a)andincreasedriskofMI
KamstrupetalJAMA,2009
AlownumberofKIV-2repeatswasassociatedwithincreasedriskofMI
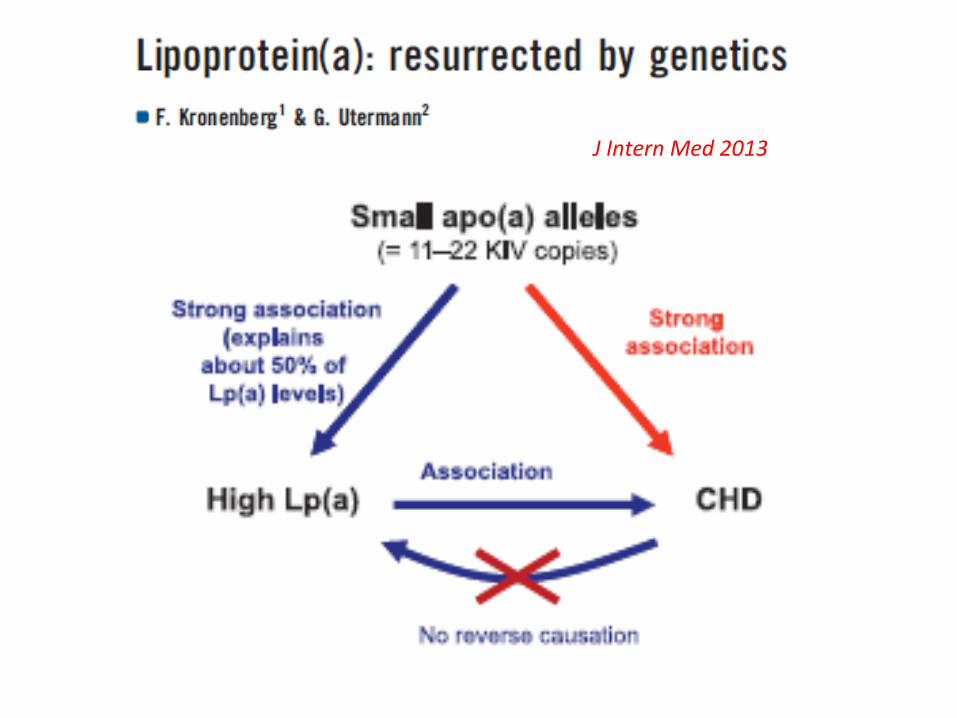
JInternMed2013

We invesOgated the KIV-2 repeat and SNPs
(rs1853021, rs1800769, rs3798220, rs10455872)
previouslyassociatedwithLp(a) levels inpaOents
withvenousthrombosis
SOcchietal,manuscriptinpreparaOon
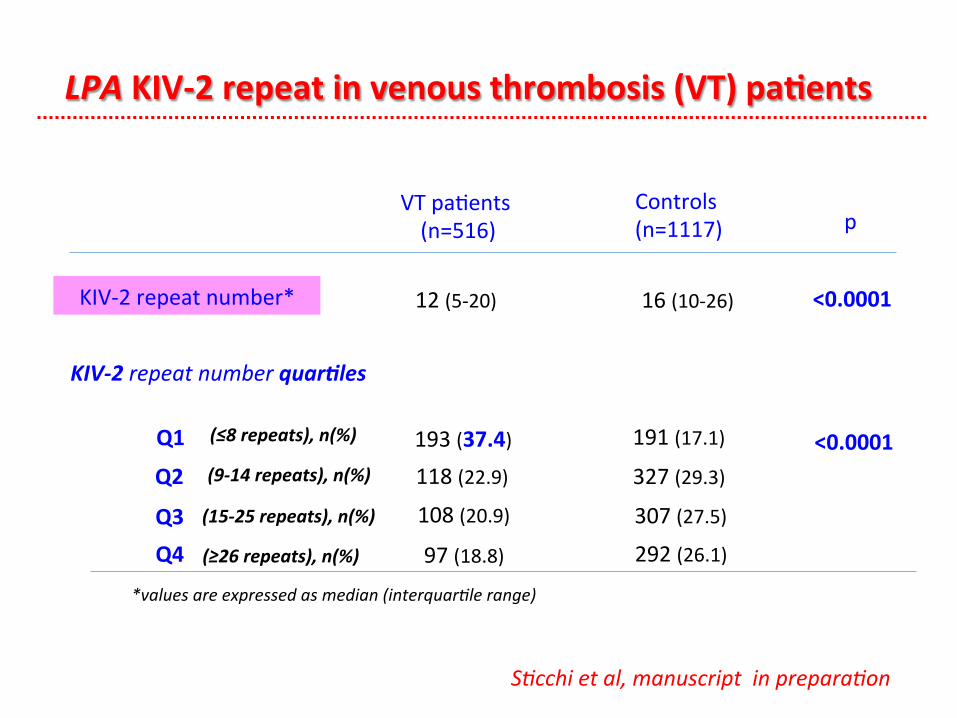
LPAKIV-2repeatinvenousthrombosis(VT)pa'ents
VTpaXents(n=516)
Controls(n=1117) p
KIV-2repeatnumber* 12(5-20) 16(10-26) <0.0001
KIV-2repeatnumberquar:les
Q1
Q2
Q3Q4
191(17.1)193(37.4) <0.0001
*valuesareexpressedasmedian(interquarOlerange)
(≤8repeats),n(%)
(9-14repeats),n(%)
(15-25repeats),n(%)
(≥26repeats),n(%)
327(29.3)118(22.9)
307(27.5)108(20.9)
292(26.1)97(18.8)
SOcchietal,manuscriptinpreparaOon

1 2 3 4 50
OR(95%CI)
KIV-2repeatquar'les
VTpa'ents,N=516
Controls,N=1117
Q4,n(%)
Q3,n(%)
Q2,n(%)
Q1,n(%) 193(37.4) 191(17.1)
118(22.9) 327(29.3)
108(20.9) 307(27.5)
97(18.8) 292(26.1)
2.99(2.16-4.14)p<0.0001
1.11(0.80-1.55)p=0.526
1.09(0.78-1.54)p=0.606
Associa'onofLPAKIV-2repeatquar'leswithvenousthrombosis(VT)MulOvariatelogisOcregressionanalysis*
*adjustedforage,gender,hypertension,diabetesmellitus,dyslipidemia,smokinghabit,BMI,hyperhomocysteinemia,andhormonaltherapy
Q1:≤8repeats;Q2:9-14repeats;Q3:15-25repeats;Q4:≥26repeats(referencegroup)
SOcchietal,manuscriptinpreparaOon

1-specificity
sensiXvity
Receiver operating characteristic curve for association with venous thromboembolism
Clinical model is based on nongenetic factors (age, gender, hypertension, diabetes, dyslipidemia, smoking habit, BMI, hyperhomocysteinemia, and hormonal therapy): area under the curve, 0.63 (95% CI, 0.60-0.66).
Genetic model contains LPA KIV-2 repeat number: area under the curve, 0.63 (95% CI, 0.60-0.66).
Combined (genetic + clinical) model contains all clinical and genetic predictors: area under the curve, 0.68 (95% CI, 0.65-0.70).
p=0.980
p=0.0038
p=7.98x10-6
SOcchietal,manuscriptinpreparaOon

THERAPY

JAMA 1995
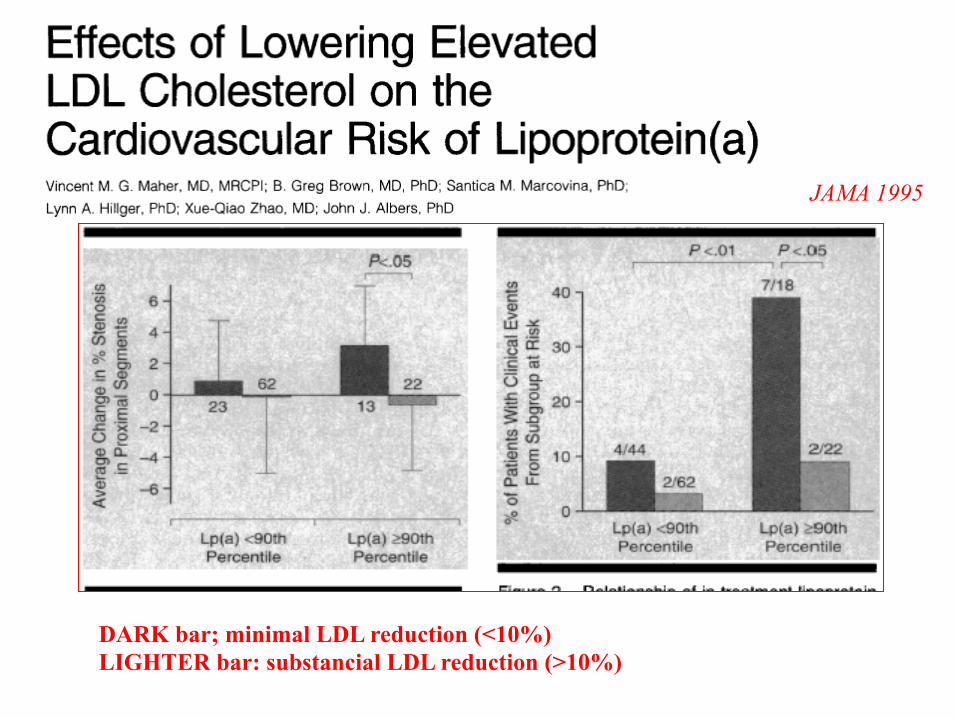
DARK bar; minimal LDL reduction (<10%) LIGHTER bar: substancial LDL reduction (>10%)
JAMA 1995
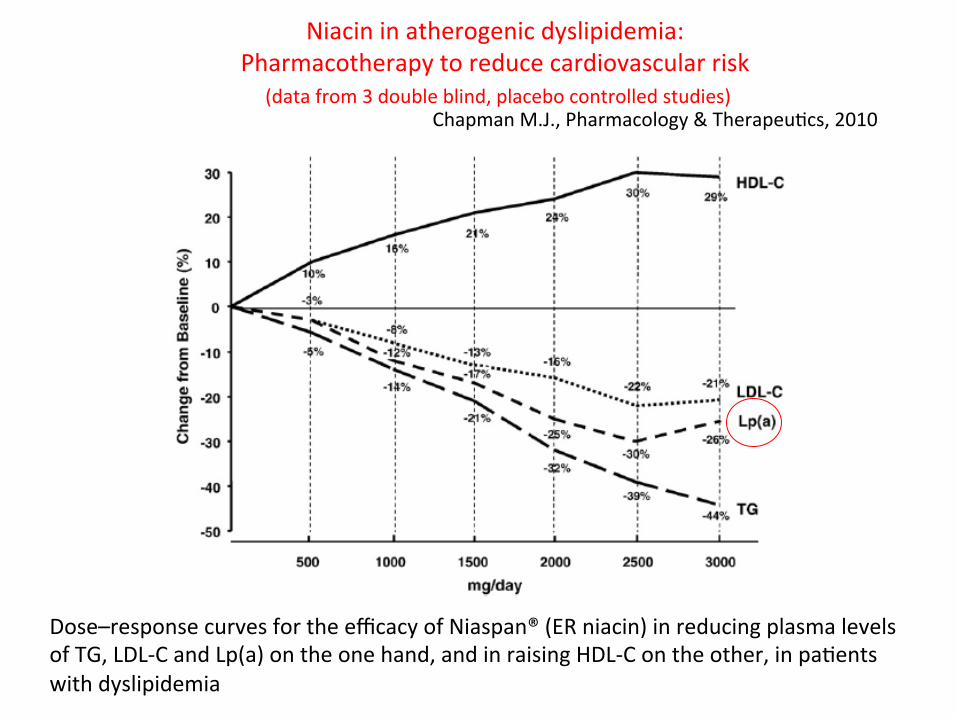
Niacininatherogenicdyslipidemia:Pharmacotherapytoreducecardiovascularrisk(datafrom3doubleblind,placebocontrolledstudies)
ChapmanM.J.,Pharmacology&TherapeuXcs,2010
Dose–responsecurvesfortheefficacyofNiaspan®(ERniacin)inreducingplasmalevelsofTG,LDL-CandLp(a)ontheonehand,andinraisingHDL-Contheother,inpaXentswithdyslipidemia

Extended-ReleaseNiacin(NicoXnicAcid)/Laropiprant
PerryC.M.,Drugs,2009.Efficacyofextended-release(ER)niacin/laropiprantinadultswithprimaryhypercholesterolaemiaor
mixedhyperlipidaemia.
Randomized,double-blind,placebo(PL)-controlled,mulXcentre,24-weektrial.
ERniacin/laropiprant1000mg/20mg(n=800)
*p<0.05,**p<0.001vsPL.

Mipomersen(ISIS301012),asecond-generaXonanXsensetherapytargeXngapolipoproteinB-100.
NatureReviewsDrugDiscovery:7,110-111(February2008)).

Mipomersen,anapolipoproteinBsynthesisinhibitor,forloweringofLDLcholesterolconcentraXonsinpaXentswithhomozygous
familialhypercholesterolaemia:arandomised,double-blind,placebo-controlledtrial
F.J.Raal,etal.Lancet,2010

Mipomersen,anapolipoproteinBsynthesisinhibitor,forloweringofLDLcholesterolconcentraXonsinpaXentswithhomozygous
familialhypercholesterolaemia:arandomised,double-blind,placebo-controlledtrial
F.J.Raal,etal.Lancet,2010

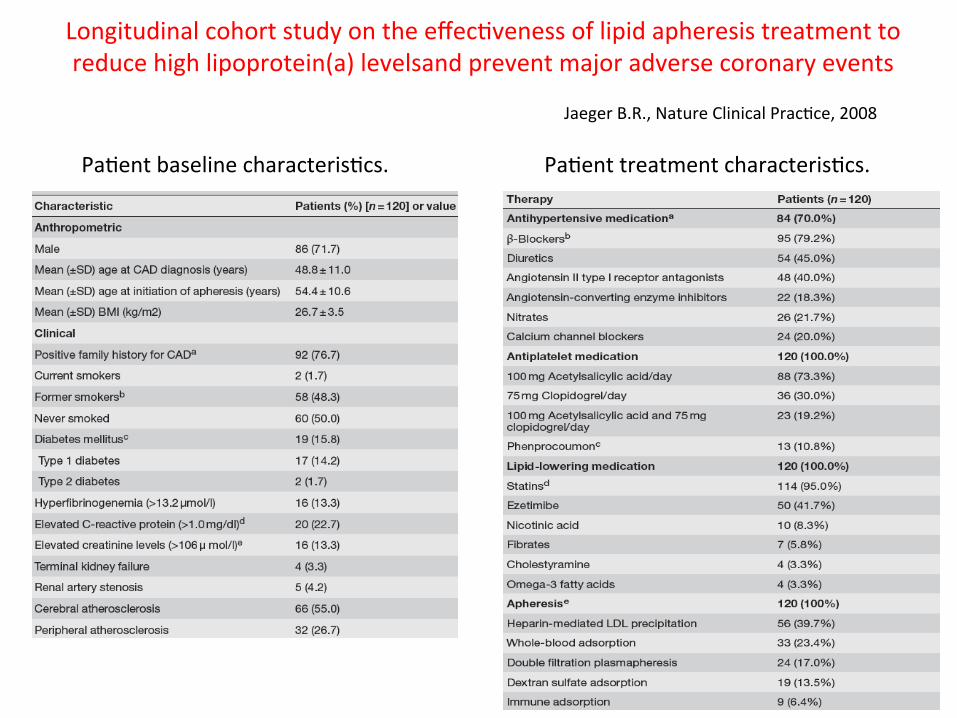
LongitudinalcohortstudyontheeffecXvenessoflipidapheresistreatmenttoreducehighlipoprotein(a)levelsandpreventmajoradversecoronaryevents
JaegerB.R.,NatureClinicalPracXce,2008
PaXenttreatmentcharacterisXcs.PaXentbaselinecharacterisXcs.
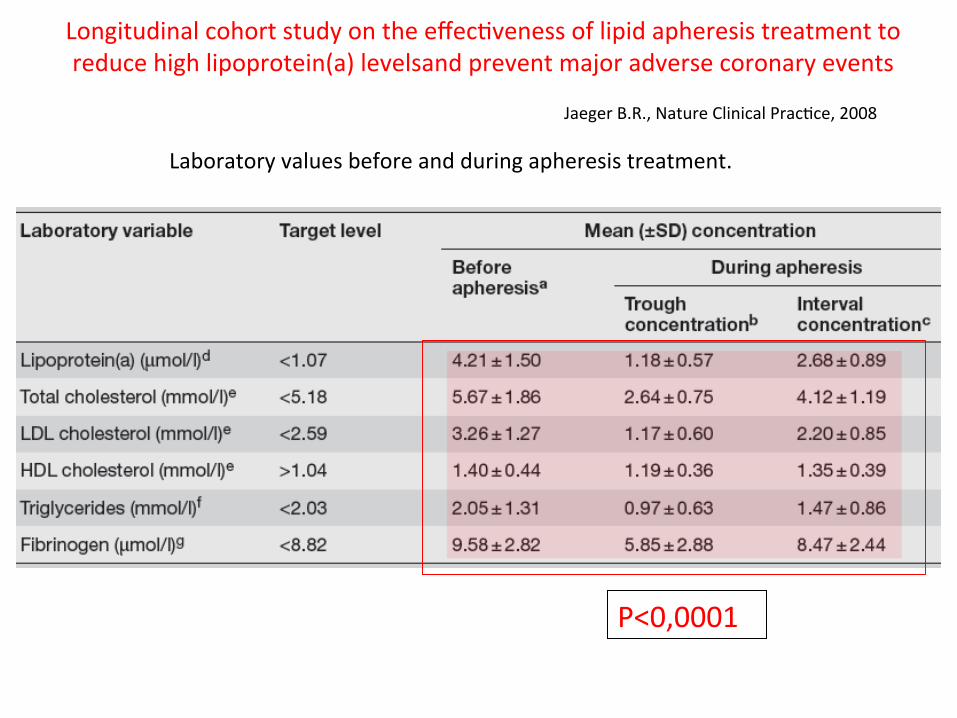
LongitudinalcohortstudyontheeffecXvenessoflipidapheresistreatmenttoreducehighlipoprotein(a)levelsandpreventmajoradversecoronaryevents
JaegerB.R.,NatureClinicalPracXce,2008
P<0,0001
Laboratoryvaluesbeforeandduringapheresistreatment.

LongitudinalcohortstudyontheeffecXvenessoflipidapheresistreatmenttoreducehighlipoprotein(a)levelsandpreventmajoradversecoronaryevents
Absolutenumbersofmajoradversecoronaryeventsduringlipid-loweringmedicaXonaloneandduringcombinedlipid-loweringmedicaXonandlipidapheresis.
JaegerB.R.,NatureClinicalPracXce,2008
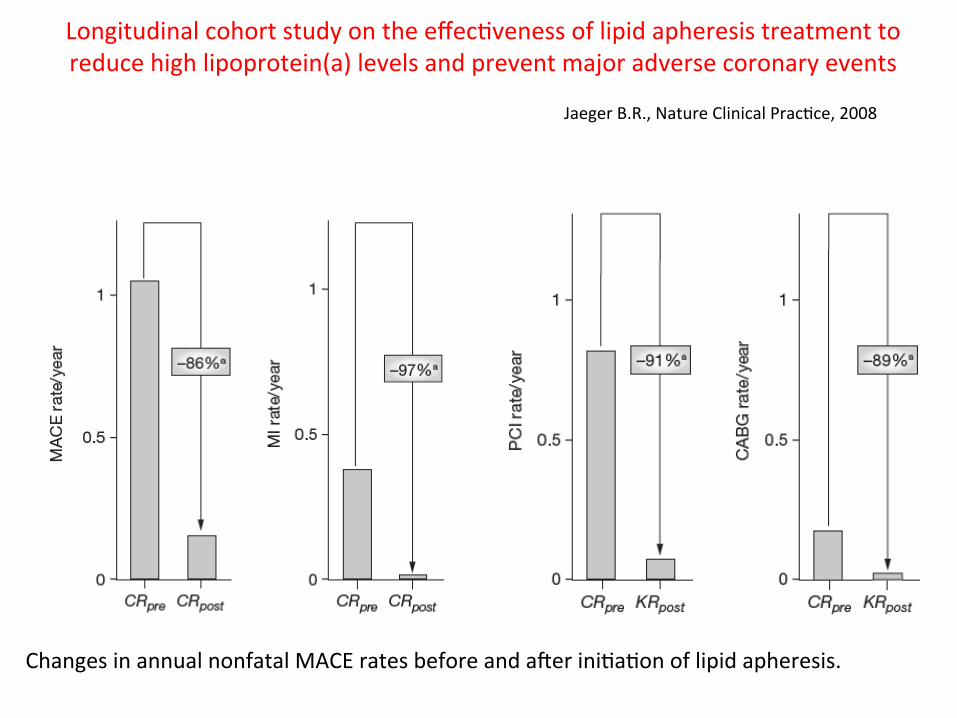
LongitudinalcohortstudyontheeffecXvenessoflipidapheresistreatmenttoreducehighlipoprotein(a)levelsandpreventmajoradversecoronaryevents
JaegerB.R.,NatureClinicalPracXce,2008
ChangesinannualnonfatalMACEratesbeforeandareriniXaXonoflipidapheresis.

JACC 2011

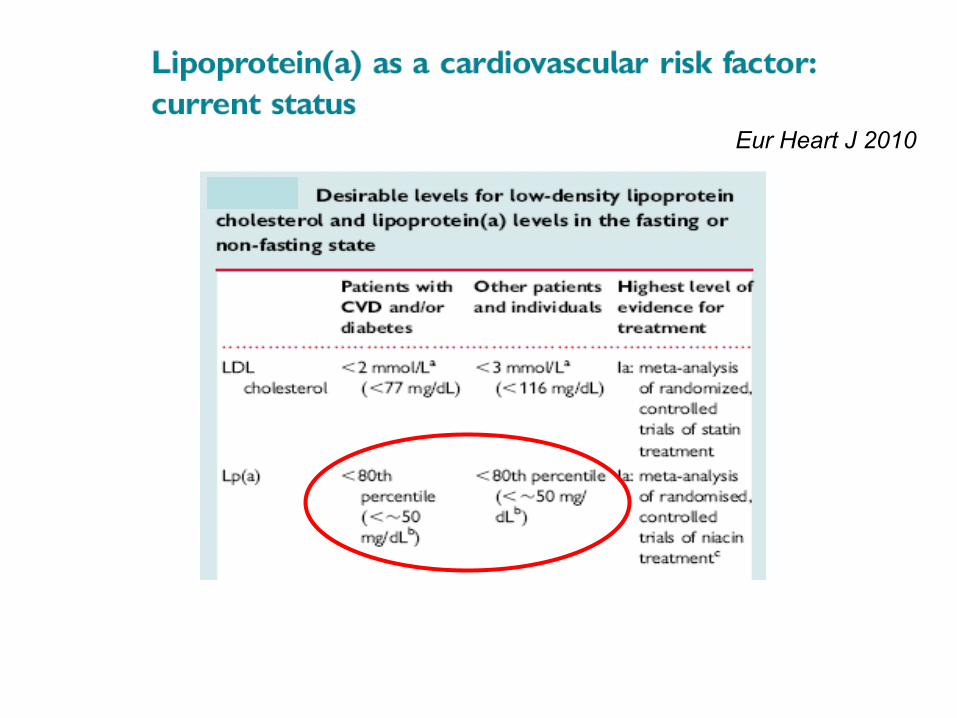
Eur Heart J 2010
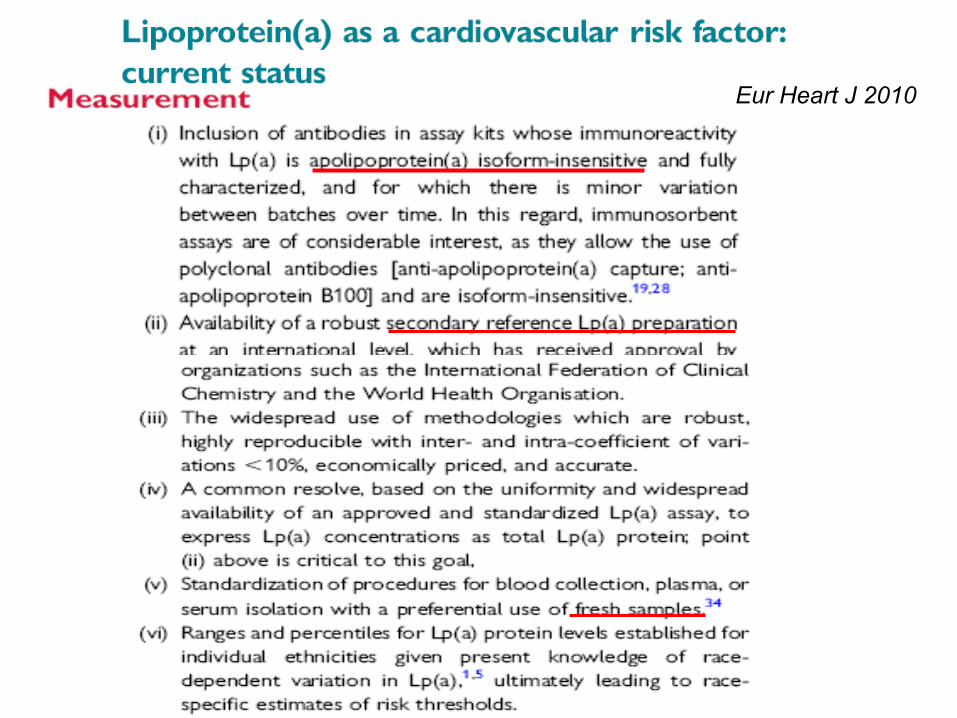
Eur Heart J 2010
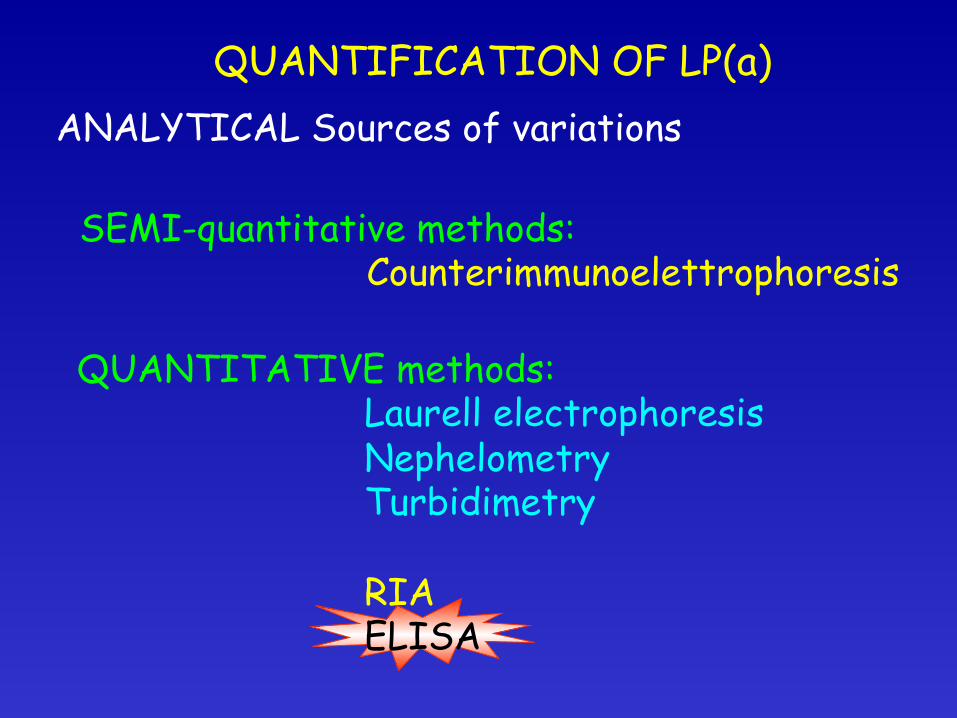
ANALYTICAL Sources of variations QUANTIFICATION OF LP(a)
SEMI-quantitative methods: Counterimmunoelettrophoresis
QUANTITATIVE methods: Laurell electrophoresis Nephelometry Turbidimetry RIA ELISA

ANALYTICAL Sources of variations
QUANTIFICATION OF LP(a)
the choice of apo(a) size in the assay calibrator is ARBITRARY and would NOT be representative of all apo(a) sizes in plasma samples the reactivity of the antibodies directed to the repeated antigenic sites of apo(a) K4 type 2 will vary depending on the size of apo(a).
The size variations of apo(a) constitutes a serious challenge for the immunochemical
measurement of Lp(a) in plasma

Eur Heart J 2010

Eur Heart J 2010
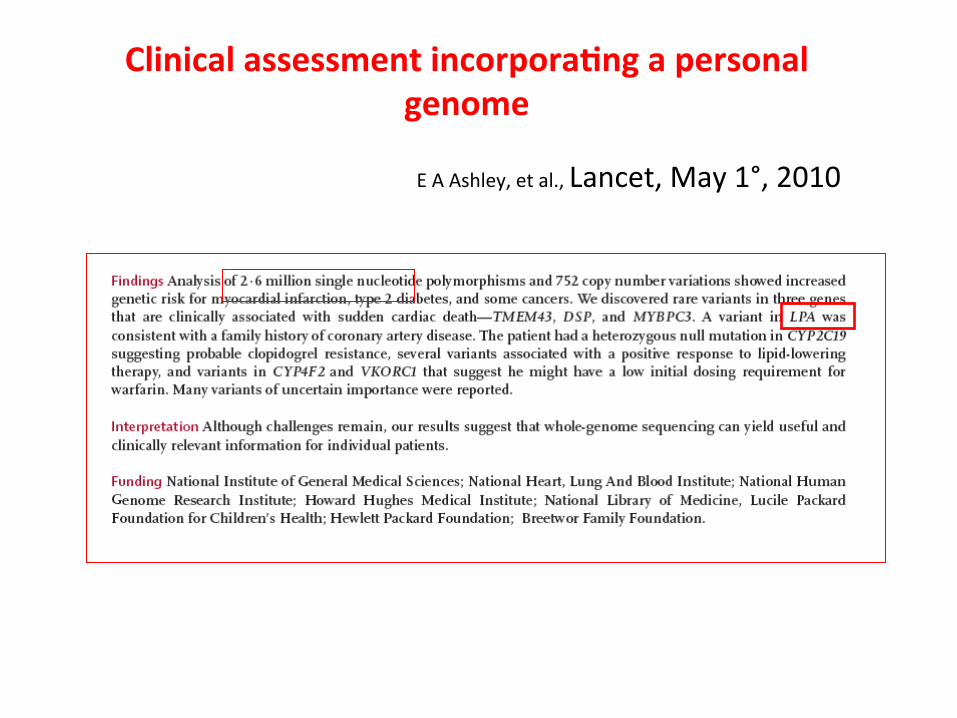
Clinicalassessmentincorpora'ngapersonalgenome
EAAshley,etal.,Lancet,May1°,2010

CioniG.1,MarcucciR.1,FaXniC.1,SXcchiE.1,FediS.1,CasolaG.1,TognacciniA.2,AbbateR.1,D'AlessandriG.2
1DiparOmentoAreaCriOcaMedico-Chirurgica,UniversitàdegliStudidiFirenze,Firenze.2SIMT,AziendaOspedalieraUSL3,Pistoia
ACIDONICOTINICO,COLESTEROLOHDLELIPOPROTEINA(a)INUNAPOPOLAZIONEDI
PAZIENTIADALTORISCHIOCARDIOVASCOLARESOTTOPOSTIADAFERESITERAPEUTICA
Valutazionedell'effevodell'acidonicoXnicosulprofilolipidico,inparXcolaresuilivellidicolesteroloHDLedilipoproteina(a),inpazienXsovoposXadaferesi.
Scopodellostudio
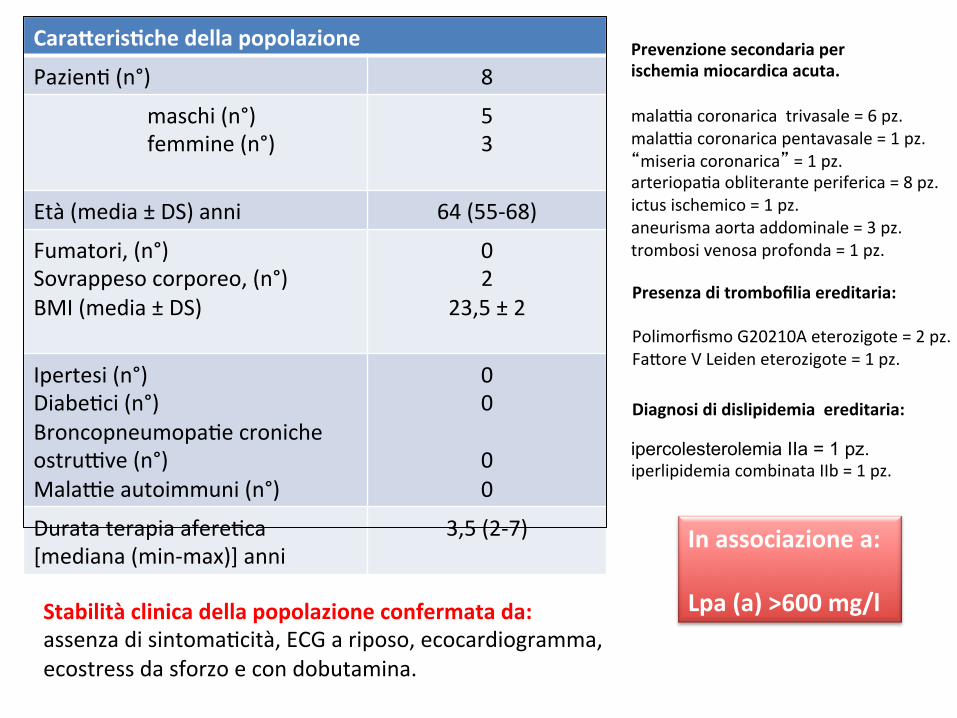
Caraperis'chedellapopolazione
PazienX(n°) 8
maschi(n°)femmine(n°)
53
Età(media±DS)anni 64(55-68)
Fumatori,(n°)Sovrappesocorporeo,(n°)BMI(media±DS)
02
23,5±2
Ipertesi(n°)DiabeXci(n°)BroncopneumopaXecronicheostruyve(n°)Malayeautoimmuni(n°)
0000
DurataterapiaafereXca[mediana(min-max)]anni
3,5(2-7)
ipercolesterolemia IIa = 1 pz. iperlipidemiacombinataIIb=1pz.
Diagnosididislipidemiaereditaria:
Prevenzionesecondariaperischemiamiocardicaacuta.malayacoronaricatrivasale=6pz.malayacoronaricapentavasale=1pz.“miseriacoronarica”=1pz.arteriopaXaobliteranteperiferica=8pz.ictusischemico=1pz.aneurismaaortaaddominale=3pz.trombosivenosaprofonda=1pz.
Inassociazionea:Lpa(a)>600mg/lStabilitàclinicadellapopolazioneconfermatada:
assenzadisintomaXcità,ECGariposo,ecocardiogramma,ecostressdasforzoecondobutamina.
Presenzaditrombofiliaereditaria:PolimorfismoG20210Aeterozigote=2pz.FavoreVLeideneterozigote=1pz.

Timing 7-10 giorni
Procedureafere'che
HELP:HEPARININDUCEDLIPOPROTEINPRECIPITATION
DESTRANOSOLFATO
IpazienXsonostaXsovoposXaproceduraafereXcaogni7-10giorni(lineeguidaASFA2010).1,5volumidiplasmatravaXadogniprocedura
TIMING
Sistemi disponibili nella nostra struttura, approvati da FDA (linee guida ASFA 2010)
Nessuneventoavversoregistratonelperiododitrapamento
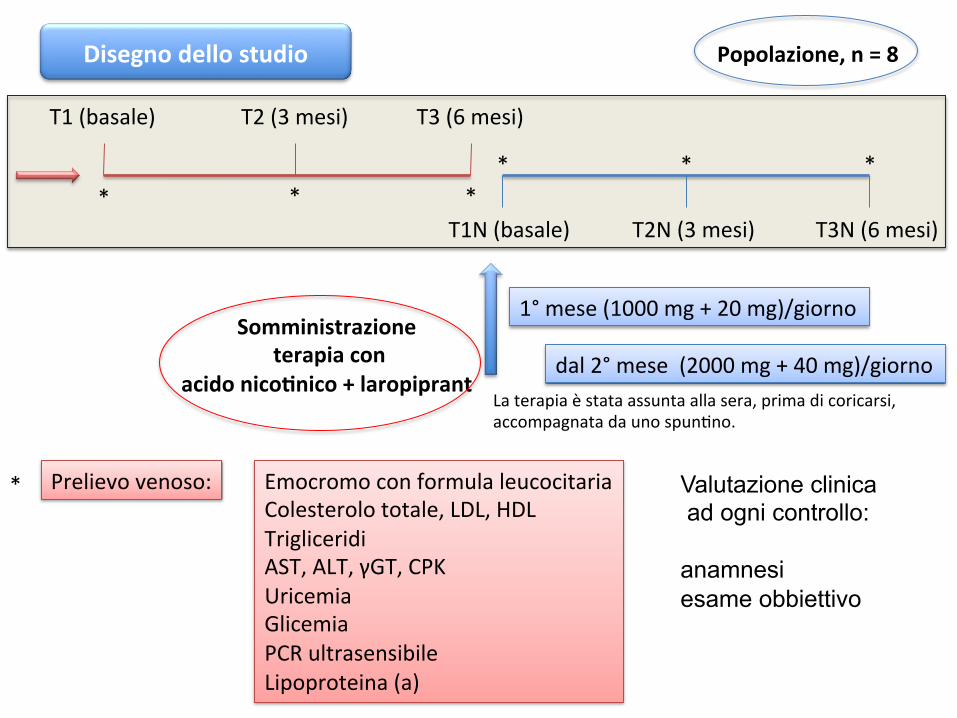
Disegnodellostudio
Somministrazioneterapiacon
acidonico'nico+laropiprant
T1(basale) T2(3mesi) T3(6mesi)
T1N(basale) T2N(3mesi) T3N(6mesi)* * *
* * *
1°mese(1000mg+20mg)/giorno
dal2°mese(2000mg+40mg)/giorno
Prelievovenoso: EmocromoconformulaleucocitariaColesterolototale,LDL,HDLTrigliceridiAST,ALT,γGT,CPKUricemiaGlicemiaPCRultrasensibileLipoproteina(a)
* Valutazione clinica ad ogni controllo: anamnesi esame obbiettivo
Popolazione,n=8
Laterapiaèstataassuntaallasera,primadicoricarsi,accompagnatadaunospunXno.

0
10
20
30
40
50
60
70
80
basale 3mesi 6mesi
Risulta'HDL
ValoridiHDLvalutaXinassenzaditerapiaconacidonicoXnico
ValoridiHDLvalutaXinterapiaconacidonicoXnico
T1 T2T3
T2NT3N
T1N
HDL[mg/dl]
p
T1N(basale) 46,5(26-67)
T2N 57,5(41-87) 0,195*
T3N 69,5(48-91) 0,013*
HDL[mg/dl] p
T1(basale) 52(33-71)
T2 43(29-57) 0,195*
T3 51,5(26-62) 0,878*
Popolazione,n=8
p for trend=0,041
52,8% T1N T3N
*pversobasale *pversobasale
mg/dl
0
20
40
60
80
100
120
basale 3mesi 6mesi
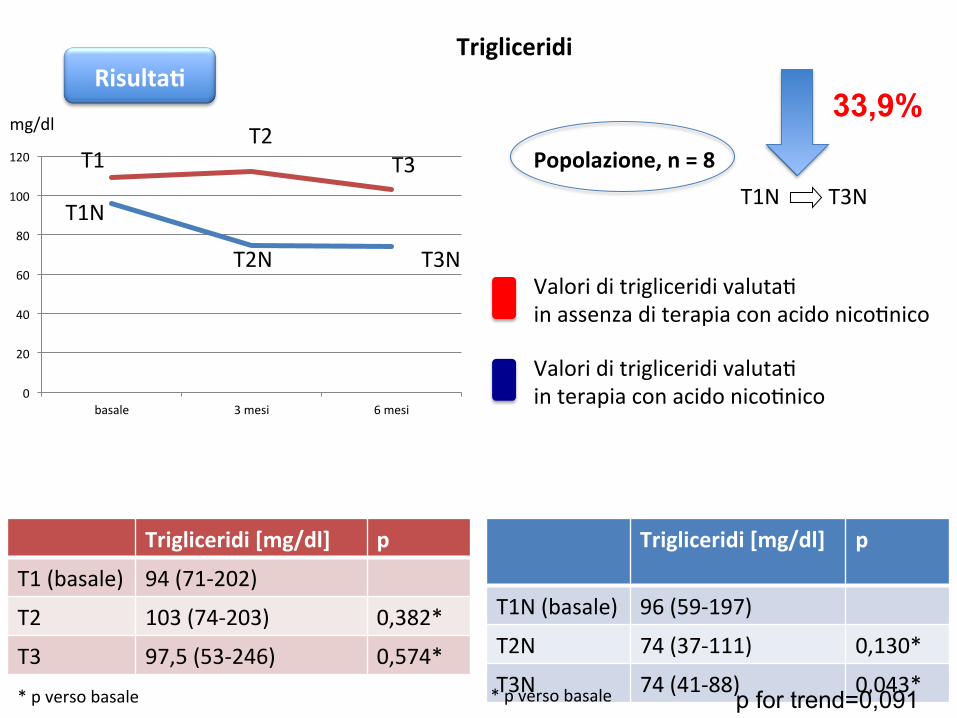
Risulta'Trigliceridi
ValoriditrigliceridivalutaXinassenzaditerapiaconacidonicoXnico
ValoriditrigliceridivalutaXinterapiaconacidonicoXnico
T1T2
T3
T2N T3N
T1N
Trigliceridi[mg/dl]
p
T1N(basale) 96(59-197)
T2N 74(37-111) 0,130*
T3N 74(41-88) 0,043*
Trigliceridi[mg/dl] p
T1(basale) 94(71-202)
T2 103(74-203) 0,382*
T3 97,5(53-246) 0,574*
Popolazione,n=8
p for trend=0,091
33,9%
T1N T3N
*pversobasale *pversobasale
mg/dl
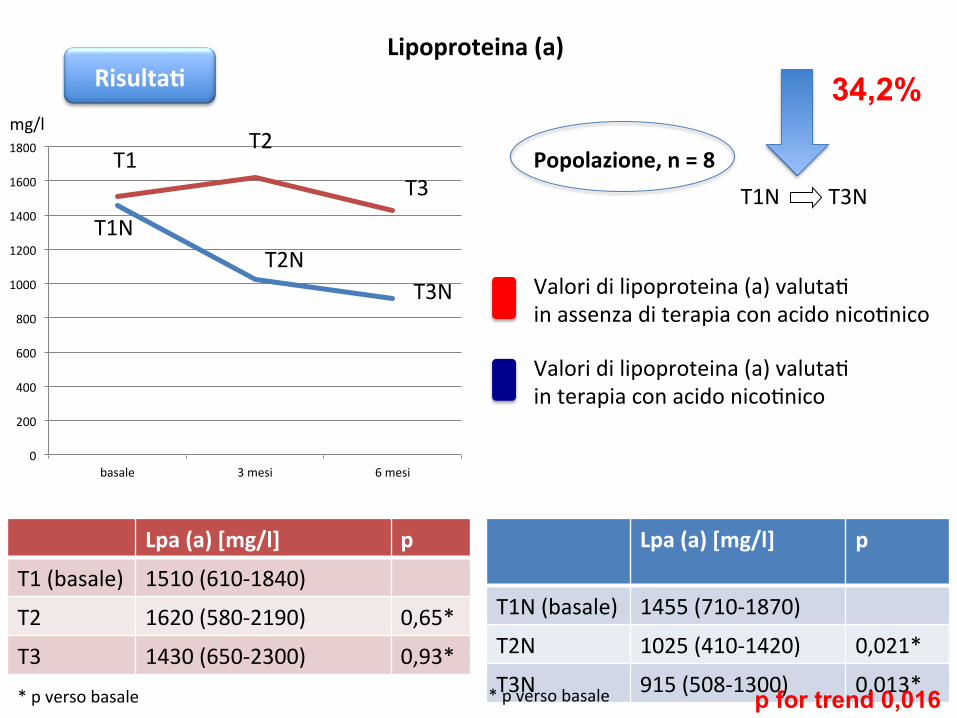
Risulta'Lipoproteina(a)
Valoridilipoproteina(a)valutaXinassenzaditerapiaconacidonicoXnico
Valoridilipoproteina(a)valutaXinterapiaconacidonicoXnico
0
200
400
600
800
1000
1200
1400
1600
1800
basale 3mesi 6mesi
T1T2
T3
T2NT3N
T1N
Lpa(a)[mg/l]
p
T1N(basale) 1455(710-1870)
T2N 1025(410-1420) 0,021*
T3N 915(508-1300) 0,013*
Lpa(a)[mg/l] p
T1(basale) 1510(610-1840)
T2 1620(580-2190) 0,65*
T3 1430(650-2300) 0,93*
Popolazione,n=8
p for trend 0,016
34,2%
T1N T3N
*pversobasale *pversobasale
mg/l

0
20
40
60
80
100
120
basale 3mesi 6mesi
LDL
125
130
135
140
145
150
155
160
165
170
basale 3mesi 6mesi
Colesterolo totale
ValorivalutaXinassenzaditerapiaconacidonicoXnicoValorivalutaXinterapiaconacidonicoXnico
LDL[mg/dl]
p
T1N(basale) 84(74-167)
T2N 66(43-149) 0,054*
T3N 90(57-118) 0,432*
LDL[mg/dl] p
T1(basale) 92,5(69-161)
T2 93(66-181) 0,65*
T3 79,5(53-180) 0,93*
Colesterolototale[mg/dl]
p*
T1N(basale) 158(116-294)
T2N 141(108-328) 0,2*
T3N 163(113-314) 0,9*
Colesterolototale[mg/dl] p*
T1(basale) 164(134-307)
T2 165(147-282) 0,9*
T3 166(116-342) 0,8*
*pversobasale
*pversobasale
pfortrend=0,180
mg/dl
mg/dl
pfortrend=0,180
0
0,2
0,4
0,6
0,8
1
1,2
basale 3mesi 6mesi
Crea'nina
270280290300310320330340
basale 3mesi 6mesi
Fibrinogeno
85
90
95
100
105
basale 3mesi 6mesi
Glicemia
010203040
basale 3mesi 6mesi
ALT
0
10
20
30
40
basale 3mesi 6mesi
AST
0
10
20
30
basale 3mesi 6mesi
γGT
0
0,01
0,02
0,03
basale 3mesi 6mesi
PCRultrasensibile
4
4,5
5
5,5
basale 3mesi 6mesi
Uricemia
0
50
100
150
200
basale 3mesi 6mesi
CPK
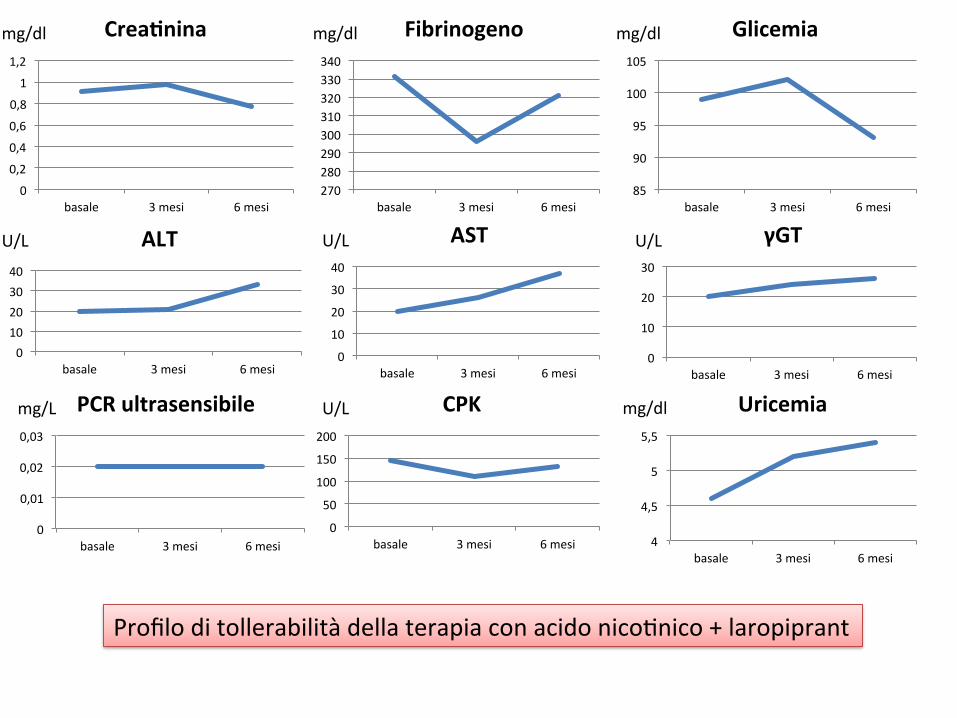
ProfiloditollerabilitàdellaterapiaconacidonicoXnico+laropiprant
mg/dlmg/dl mg/dl
U/L U/LU/L
U/L mg/dlmg/L
T1N(basale) T2N(3mesi) T3N(6mesi)
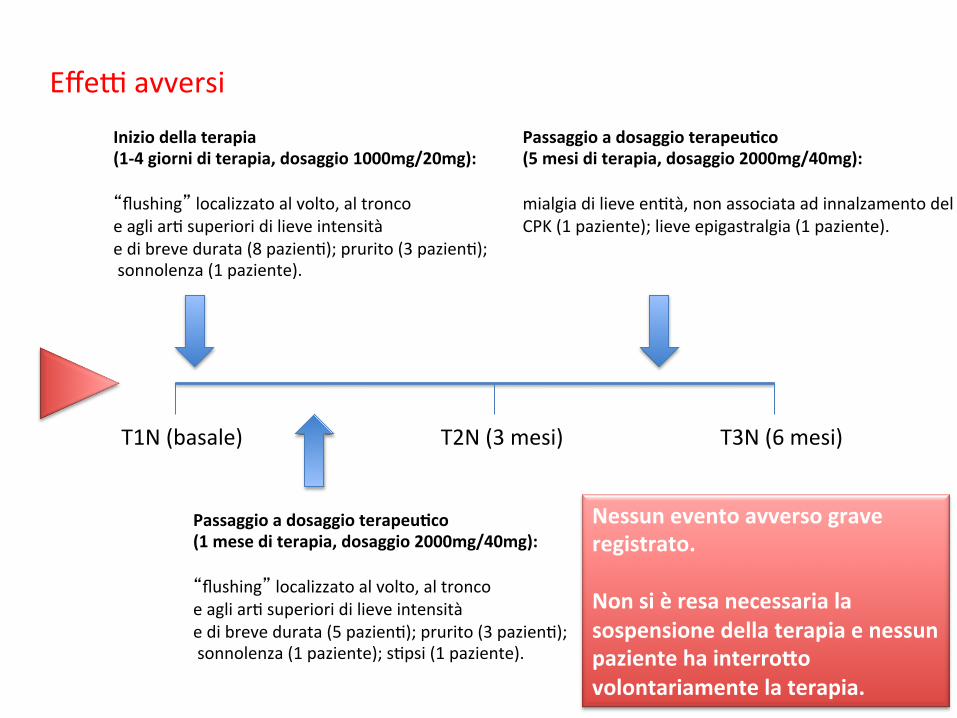
Effeyavversi
Iniziodellaterapia(1-4giorniditerapia,dosaggio1000mg/20mg):“flushing”localizzatoalvolto,altroncoeagliarXsuperioridilieveintensitàedibrevedurata(8pazienX);prurito(3pazienX);sonnolenza(1paziente).
Passaggioadosaggioterapeu'co(1mesediterapia,dosaggio2000mg/40mg):“flushing”localizzatoalvolto,altroncoeagliarXsuperioridilieveintensitàedibrevedurata(5pazienX);prurito(3pazienX);sonnolenza(1paziente);sXpsi(1paziente).
Passaggioadosaggioterapeu'co(5mesiditerapia,dosaggio2000mg/40mg):mialgiadilieveenXtà,nonassociataadinnalzamentodelCPK(1paziente);lieveepigastralgia(1paziente).
Nessuneventoavversograveregistrato.Nonsièresanecessarialasospensionedellaterapiaenessunpazientehainterropovolontariamentelaterapia.

Followup12 mesi
020406080100120140160180
Basale TN1 TN2 TN3 TN4
colesterolototale
0
10
20
30
40
50
60
70
80
Basale TN1 TN2 TN3 TN4
HDL
0102030405060708090
Basale TN1 TN2 TN3 TN4
LDL
0
20
40
60
80
100
120
Basale TN1 TN2 TN3 TN4
trigliceridi
mg/dl mg/dl
mg/dlmg/dlP=0,040
P=0,054
P=0,038

0
200
400
600
800
1000
1200
1400
1600
Basale TN1 TN2 TN3 TN4
lipoproteina(a)
Followup12 mesi
mg/dl
5/8pazienXhannoraggiuntolivellidiLp(a)<600mg/dldopo1annoditerapia
P=0,006
P=0,001
Conclusioni
In una popolazione ad alto rischio cardiovascolare,sovopostaaproceduraafereXca, lasomministrazionedi acido nicoXnico/laropiprant è in grado diowmizzare l'assepo lipidico con il significa'voaumentodei livelli di colesteroloHDL e la riduzionedeilivellidiLp(a).
Lostudio,tuvoraincorso,ciconsenXràdivalutaresela somministrazione di acido nicoXnico oltre allaterapia standard possa consenXre di allungare il'ming fra le procedure afere'che in pazien'seleziona'.


Mattiuzzi C, J Thromb Thrombol 2014

J Intern Med 2013





























