Embed Size (px)
Citation preview

Ludwig TraubeThe Man and His Space
The detection of dullness to percus-sion in the left hemithorax raises thepossibility of pleural effusion, consol-idation, or atelectasis. Percussion ofTraube's space, a semilunar tympa-nitic area overlying the gas bubble inthe stomach, is a valuable maneuver inthis regard: obliteration of Traube'sspace favors a pleural effusion. Knowl-edge of the remarkable life of Traube,and the ability to demonstrate theutility of his sign on rounds, providesan opportunity in a technologic age toremind the medical student of the ro-mance of bedside medicine.(Arch Intern Med. 1992;152:701-
703)To carefully observe the phenomena of life in
all its phases, normal and perverted, to makeperfect the most difficult of all arts, the art ofobservation, to call to aid the science of exper¬imentation, to cultivate the reasoning facultyso as to be able to know the true from thefalse—these are our methods.
William Osler
Contemporary medicine has abasis in the experimental and
imaginative methods of scientists ofthe past. By the unique medium ofthemedical eponym, some names areinvoked daily at the patient's bed¬side1; those whose names were neverso associated may vanish into obscu¬rity. A third and perhaps worse fateis to have generated a medical ep¬onym only to have the eponymbe un¬
taught, or poorly understood evenwhen it is taught.2 If the physical signdescribed by Ludwig Traube (Fig 1)did not remain useful at the bedside,there would be little cause for lament.We contend that an understandingand demonstration of Traube's spaceis a practical and handy clinical skill.Additionally, a knowledge of the re¬markable Ufe of Ludwig Traubemight perhaps be inspirational to stu¬dent and specialist alike.
THE MAN
Ludwig Traube was born in 1818 inSilesia. During his medical studies inGermany at the University of Breslauand later at the University of Berlin,he was influenced by JohannesMüller (1805-1858), François Ma-gendie (1783-1855), René Laënnec(1781-1826), and Johann Schönlein(1793-1864). The work of Laënnec onauscultation and percussion was tohave deep influences on his think¬ing.3In 1840, he received his medical
degree from the University of Berlinand moved to Vienna, Austria,where he spent a year of stimulatingworkwith JosefSkoda (1805-1881) (of"skodaic resonance" fame) in clinicalmedicine and with Carl Rokitansky(1804-1874) in pathologic anatomy.He returned permanently to Berlin in1843, equipped to begin a career inexperimental and clinical medicine.3During the early 19th century,
Germany was in the throes of polit¬ical and economic upheaval. The pre¬vailing system of investigation at thattime was one of Naturphilosophie, a
speculative and mystical approach tomedical practice and scientific under¬standing, largely influenced by thephilosophers Friedrich von Schellingand Hegel. In the early 1820s, disil¬lusioned by the "armchair theoriz¬ing" of their contemporaries and in¬fluenced by the French schools ofMagendie and Claude Bernard (1813-1878), German physicians in themold of Wilhelm von Humboldt(1767-1835) began to use scientificreasoning and controlled experimen¬tation. It was at this critical transitionthat Ludwig Traube made his entryinto the world of experimental med¬icine.4In 1847 Traube secured a position
as Privatdocent at the Charité Hospi¬tal under Schönlein. This acceptance
Fig 1.-Ludwig Traube (1818-1876).
at Charité was later recorded byTraube as the happiest day of his life.Traube immersed himself in experi¬mental medicine. One of his first pa¬pers, on pneumonia resulting fromthe cutting of the vagus nerves, ap¬peared alongwith the experiments ofRudolf Virchow (1821-1902) onthrombosis and embolism in theearly editions of a journal thatTraubecofounded with Virchow. Traube'swork on suffocation was done in1847, and he introduced the ther¬mometer in his clinic in 1850. In 1853,he was made an assistant professorat Charité, and by this time he wasmarried to Cora Markwald.5
Between 1862 and 1867, Traubewent through turbulent times, suf¬fering from angina pectoris and los¬ing a son to diphtheria. However,the same period saw him describethe Traube-Herring waves. Traubehad a particular interest in correlat¬ing clinical pulmonary disease withthe underlying abnormality: he de¬scribed the characteristic sputum oflung abscess and gangrene, he de¬scribed putrid bronchitis, and, in thecourse of his study of "ileotyphus"(presumably typhoid fever), he de-

scribed the respiratory aspects of thedisease, including the laryngitis andbronchitis. He demonstrated bron¬chial breathing in alveolar con¬solidation, coined the term metallic-sounding wheeze in asthma, and wasable to describe accurately the clinicalpicture of pleurisy and croup.6 In1872, he was nominated professor,and by that time had published twovolumes of his work on physiologyand clinical medicine. In 1872 he wasnominated as an honorarymemberofthe society of German doctors inParis, and in the same year the fa¬mous William Osier visited the labo¬ratories of Traube, Virchow, and Fre-richs. Osier was so impressed that heis said to have stated his ambitionwas"to build a great clinic on Teutonic
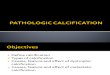
Fig 2.—Surface anatomy of Traube's space.
lines here in America . . . lines whichhave placed the scientific medicine ofGermany in the forefront of theworld."4 After the celebration ofTraube's 25th anniversary at the Uni¬versity of Berlin, he received manyhonors and continued his academictenure until his death due to anginaand heart failure in 1876, only2monthsafter his wife's death due to cancer.
THE SPACEIt is for his description of a semilu¬
nar space on chest percussion thatTraube will be remembered. Ana¬tomically the space is bounded me¬
dially by the left edge of the liver,laterally by the medial edge of thespleen, and superiorly by the lowerborder of the heart.7 The space can bemapped by dropping perpendicularlines down from the sixth rib at thecostochondral junction and the ninthrib at the anterior axillary line to thecostal margin. An irregularly quadri¬lateral space is thus defined (Fig 2).In the words of Professor Jacoud, "Inthe state of the vacuous stomach,and all the organs in the region beinghealthy, one can ascertain in thesemi-lunar space a sharp tympanismwith percussion, the absence of vocalvibrations by palpation and the ab¬sence of respiratory noise with aus¬cultation."8In the winter of 1868, Traube was
asked to see a young man admittedwith fever, chills, headache, and a"stitch-like" pain in the left side of
the chest. Traube noted the patient tobe dyspneic and coughing up rust-colored sputum. Examination of thepatient revealed a reduction in thehalf-moon space on percussion anddecreased pectoral fremitus on theleft. Moreover, the patient had loudbronchial breath sounds below theleft scapula and a systolic rub overthe sternum. The patient died 2 dayslater. On the basis of his clinicalfindings, Traube surmised the fol¬lowing: (1) The rusty sputum indi¬cated an inflammation of the lungparenchyma, ie, pneumonia. (2) Thediminution in the space associatedwith the stabbing left-sided chestpains indicated pleural exúdate, ie,empyema. (3) The systolic rub overthe sternum indicated an exúdatearound the heart. All of these find¬ings were confirmed at autopsy.9 Inanother patient with an accumula¬tion of pleural fluid due to trauma,Traube noted that résorption of thepleural fluid was heralded by an in¬crease (a return to normal) in the sizeof the semilunar space, long beforethe dull percussion note over the af¬fected lung resolved.10 Ironically,Traube did not write much moreabout this semilunar space, and itwas left to his student Fraentzel911 topopularize this space:The fact that in the lowest part of the leftthorax there is a tympanitic percussionnote has been known for a long time. In¬vestigation of this subject was under¬taken recently by professor Traube. The
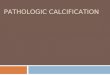
Fig 3.—Schematic drawing of percussion findings in the left lower hemithorax in a normal lung (left), consolidation (center), and pleuraleffusion (right).

results of this investigation may be sum¬marized as follows: a) The above men¬tioned area of tympany is shaped like a
half moon; below its border is the rim ofthe rib cage, above it is limited by a bow¬like line with its concavity pointed down¬wards, b) The half moon shape beginsanteriorly below the fifth or sixth rib andextends along the edge of the thorax, andposteriorly to the anterior end of theninth or tenth rib. c) Its greatest widthapproaches three to three and a halfinches, d) Percussion in this area differsnot only in its tympanitic note but also byits loudness in comparison with the restof the lung, e) When the lung expandsduring inspiration, the half moon spacebecomes smaller and thus shows that thelung is capable of expanding, f) A con¬siderable increase in the semilunar spaceis usually a sign of immobility of thelower edge of the lung and thus serves asan indicator of scarring, g) In the pres¬ence of pleural effusion, the half moon
space may disappear and its reappear¬ance heralds the beginning of reabsorp¬tion. The progress of recovery will be bestdetermined by the increase of the halfmoon space, h) During pneumonic infil¬tration of the entire lung, the half moon
space remains either intact or is onlyslightly narrowed.
Professor Jacoud, who undertookan intense evaluation of Traube'sspace, emphasized two caveats re¬
garding this sign. First, a reductionin the space may be the only sign ofa subpulmonic pleural effusion. Sec¬ond, and more important, a reduc¬tion in the tympanism over the spacecould arise with pleural adhesions("phrenocostal symphysis") and notsolely from pleural effusion.8 Given a
patient with reduction in the semilu¬nar space, differentiation betweenpleural fluid and adhesions would bepossible by observing respiratorymovements; in the latter, one wouldsee a classic retraction of the lowerintercostal spaces with each inspira¬tion, a finding not observed in effu¬sions.8 In the words of ProfessorNeumann, however, dullness over
Traube's space was highly sensitivefor effusions: "this can reveal thepresence of pleural effusions in theleft pleura that sometimes can bemissed by expert radiologists andthis has been confirmed on multipleoccasions by thoracentesis."12Traube never associated dullness
in this space with splenic enlarge¬ment, a common misconception thatpersists today. A recent report sug-
gested that percussion of Traube'sspace compares favorably with othercommonly used clinical maneuvers(none of which are sensitive) and isbetter than chance alone in determin¬ing the presence of an enlargedspleen.13We find demonstrating Traube's
space of the greatest utility (even inthis era of portable chest roentgen-ography and ultrasound) as a spe¬cialized maneuver when dealingwith a patient with dullness in theleft hemithorax (Fig 3). The maneu¬ver can be performed with the pa¬tient supine or sitting. Preservationof Traube's space suggests that thedullness is from consolidation or at-electasis; if Traube's space is obliter¬ated, a pleural effusion is suspected.An exceptionmay be the patientwithconsolidation of the left anteriorbasal segment and contiguous lin-gula, where the resonance ofTraube's space may be impaired (K.V. Thiruvengadam, MD, writtencommunication, April 22, 1991). Al¬though each of these conditions willhave their unique signs (bronchialbreathing in consolidation, stonydullness and mediastinal shift inpleural effusion), we believe that ac¬curate bedside diagnosis rests on theavailability of more than one physicalsign to buttress a diagnosis.
As the ward team troops en masseto Radiology at the end of wardrounds, we, as long-time clinicalteachers, continue to be amazed atthe slack-jawed expressions of won¬der on the faces of students andhouse staff when bedside diagnosiscorrelates with roentgenologicdiagnosis—as if an insidious anddeeply rooted distrust of thehands-on examination is beingshaken. It is ironic that the readyavailability of diagnostic technologyhas not, it seems, enhanced bedsideskills but instead has encouragedtheir atrophy.1415 The teaching ofTraube's space is a reminder of theremarkable bedside skills of yearsgone by; in addition, by invoking thismedical eponym, the memory of a
remarkable man lives on.ABRAHAM VERGHESE, MDDepartment of InternalMedicine
Texas Tech University4800 Alberta AveEl Paso, TX 79905-1298
GUHA KRISH, MDANAND KARNAD, MDDepartment of InternalMedicine
East Tennessee StateUniversity
Johnson City, TN 37614This article is dedicated to K. V. Thiru-
vengadam, MD, bedside clinician extraor¬dinaire.We gratefully acknowledge the assistance
of Christa Dison in translating the Germanreferences, the expert secretarial assistanceof Joyce Larimer, Kim Morris for assistancewith the figures, and staff at the Rare Bookssection of the Countway Library of Medi¬cine, Boston, Mass, for their help in locatingcrucial references.
References1. Verghese A, Dison C, Berk SL. Courvois-
ier's law: an eponym in evolution. Am J Gas-troenterol. 1987;85:248-250.
2. Verghese A, Gallemore G. Kernig andBrudzinski's signs revisited. Rev Infect Dis.1987;9:1187.
3. Lista GA. Ludwig Traube y el centenariodel espacio semilunar (1868-1968). Pren MedArgent. 1968;55:1839.
4. Harvey AM. Science at the Bedside: Clin-ical Research in American Medicine. Balti-more, Md: Johns Hopkins; 1981:13-24.
5. Garrison FH. An Introduction to the His-toryofMedicine. 4th ed. Philadelphia, Pa: WBSaunders Co; 1929:758.
6. Berndt H. Geschichte der medizin: Lud-wig Traubes Beitrag zur pulmonologie. Z ArztlFortbild. 1986;80:641-643.
7. Bailey H. Demonstration of PhysicalSigns in Clinical Surgery. 13th ed. Baltimore,Md: Williams & Wilkins; 1960:556.
8. Jacoud S. Treizieme lecon Semeiologiede l'espace semilunaire. In: Delahaye A, Le-crosnier E, eds. Lecons de clinique medicalefaites a I'hopital de la Pitie (1883-1884). Paris,France: Delahaye et Lecrosnier; 1885:238-255.
9. Fraentzel K. Linke lunge in ihrer ganzenausdehnung grau hepatisiert: fibrino-seroeses exudat im pericardium: bemerkun-gen uber den halbmondfoermigen raum undueber den vocalfremitus. Berl Klin Wochen-schr. 1868;50:854-859.
10. Traube L. Zur lehre von der resorptionpleuritischer exsudate mit bemerkungen ue-ber die ursachen des Tiefstandes des Zwerch-felles auf der gesunden seite in faellen von
umfaenglichen pleuraexudaten. Klin Unter-suchungen. 1871;1:326-328.
11. Talbott JH. A Biographical History ofMedicine: Excerpts and Essays on Men andTheir Work. New York, NY: Grune & StrattonInc; 1970:592-595.
12. Neumann W. Clinica de la Tuberculo-sis, Pulmonar en el Adulto. Buenos Aires, Ar-gentina: Editorial Labor; 1934.
13. Barkun A, Camus M, Meagher T, et al.Splenic enlargement and Traube's space: howuseful is percussion? Am J Med. 1989;87:562-566.
14. Verghese A. Malachi awaits. MD Maga-zine. September 1990;34:109-115.
15. Greganti MA. Where are the clinical rolemodels? Arch Intern Med. 1990;150:259-261.