Embed Size (px)
Citation preview

2061
Lymphatic Flow in Carcinoma of the Head of the Pancreas Masato Kayahara, M.D., Takukazu Nagakawa, M.D., Hironobu Kobayashi, M.D., Kazuhiro Mori, M.D., Tatsuo Nakano, M.D., Naotaka Kadoya, M.D., Tetsuo Ohta, M.D., Keiichi Ueno, M.D., and ltsuo Miyazaki, M.D.
The lymphatic pathway from the head of the pancreas to the para-aortic lymph nodes was examined on the basis of the frequency of lymph node involvements. Forty-four patients were examined. All patients had extended radi- cal operations. Thirty-one of 44 (70.5%) patients had lymph node involvement. The lymph nodes that had a high metastatic rate included the following: (1) lymph nodes around the common hepatic artery (number 8 lymph node); (2) lymph nodes of the hepatoduodenal liga- ment (number 12 lymph node); (3) the posterior pancrea- ticoduodenal lymph node (number 13 lymph node); (4) lymph nodes around the superior mesenteric artery (number 14 lymph node); (5) para-aortic lymph nodes (number 16 lymph node); and (6) the anterior pancreati- coduodenal lymph node (number 17 lymph node). Twenty-eight of these 31 patients had disease in the poste- rior pancreaticoduodenal lymph node. The patterns of lymph node involvement consisted of four combinations: number 13-number 17, number 13-number 14, number 14-number 16, and number 17-number a. All of the pa- tients with number 16 nodal involvement had number 14 lymph node metastasis. However, there was no relation- ship between tumor size and lymph node involvement.
Based on these results, the main lymphatic pathway from the head of the pancreas to the para-aortic lymph nodes was thought to be via the lymph nodes around the superior mesenteric artery, assuming that lymphatic flow is anterograde. In addition, this study demonstrates that it is necessary to perform an extensive lymph node dissection, including the para-aortic lymph node, even in patients with small tumors. Cancer 1992; 702061-2066.
Key words: pancreas cancer, lymphatic flow, para-aor- tic lymph node, extensive lymph node dissection.
From the Second Department of Surgery, School of Medicine, Kanazawa University, Kanazawa, Japan.
Address for reprints: Masato Kayahara, M.D., Second Depart- ment of Surgery, School of Medicine, Kanazawa University, 13-1 Takaramachi, Kanazawa 920, Japan.
Accepted for publication January 27, 1992.
The incidence of pancreatic cancer is increasing. The 5-year survival rate of patients with pancreatic cancer has remained unsatisfactorily poor. To improve the prognosis of pancreatic carcinoma, extended radical surgical procedure was advocated by Fortner in 1973.’ Lymph node dissection is one of the main components of radical surgical procedure. Our group demonstrated that retroperitoneal infiltration, including neural inva- sion, extends to the superior mesenteric artery, and we emphasized that a radical retroperitoneal dissection is necessary to cure the patients.’r3 It has been thought that the survival rate is increased if the regional lymph nodes and retroperitoneal tissue are excised. An appro- priate evaluation of extirpated lymph nodes is impor- tant at the time of the operation. Anatomic studies of the normal lymphatic pathway have been done by other investigator^,^,^ but a clinicopathologic study of lymph node involvement was deemed practical and useful for operative therapy. This study evaluates the lymphatic pathway from the pancreas to the para-aortic lymph nodes from the standpoint of the frequency of lymph node involvement.
Materials and Methods
Forty-four patients with ductal carcinoma of the head of the pancreas were examined histopathoIogicaIly. All operations were performed according to the surgical technique of the translateral retroperitoneal approach.’ Thirty-one patients were treated with pancreatoduo- denectomy and 13 with total pancreatectomy. Systemic lymph node dissection, including the regional and para-aortic lymph nodes, was performed in all patients.
Resected specimens with attached peripancreatic lymph nodes were immediately fixed in 10% buffered formaldehyde solution after careful gross descriptions of the primary tumors. The separation of the peripan- creatic lymph nodes was not performed because (1) peripancreatic, in particular, pancreaticoduodenal
2062 CANCER October 25,1992, Volume 70, No. 8
lymph nodes often were within the substance of the pancreas, and (2) lymph nodes around the superior mes- enteric artery are intermingled with the nerve plexus, and it is important to evaluate nerve invasion and lymph node involvement at the same time. Para-aortic lymph nodes were mapped in accordance with intraop- erative marking. After serial 5-mm sections were made, tissues were embedded in paraffin and stained with he- matoxylin and eosin, and elastica van Gieson staining was used for some of them. The site of tumor origin usually was determined at the time of gross and histo- pathologic examinations. Tumor size was measured in diameter histologically in one of the serial sections con- taining the largest portion of the tumor. The tumors were classified into five groups: TI , tumors smaller than 2 cm; T2a, tumors 2.1-3 cm; T2b, tumors 3.1-4 cm; T3, tumors 4.1-6 cm; and T4, tumors larger than 6 cm.
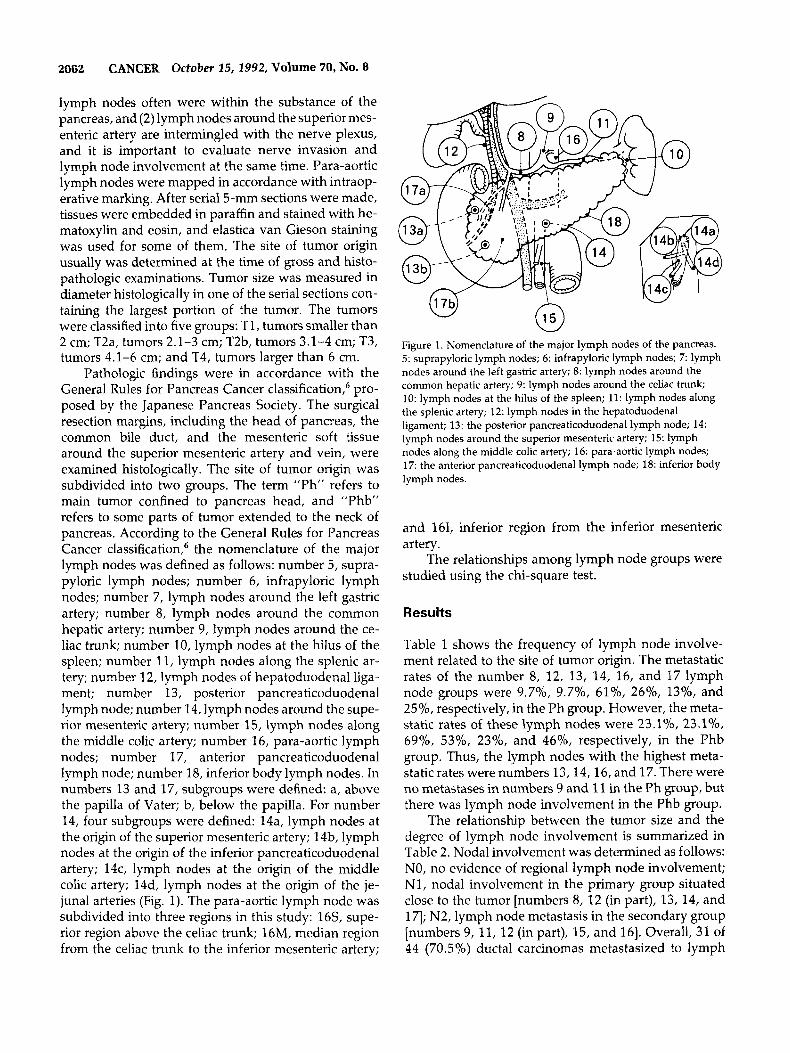
Pathologic findings were in accordance with the General Rules for Pancreas Cancer classification,6 pro- posed by the Japanese Pancreas Society. The surgical resection margins, including the head of pancreas, the common bile duct, and the mesenteric soft tissue around the superior mesenteric artery and vein, were examined histologically. The site of tumor origin was subdivided into two groups. The term "Ph" refers to main tumor confined to pancreas head, and "Phb" refers to some parts of tumor extended to the neck of pancreas. According to the General Rules for Pancreas Cancer classification,6 the nomenclature of the major lymph nodes was defined as follows: number 5, supra- pyloric lymph nodes; number 6, infrapyloric lymph nodes; number 7, lymph nodes around the left gastric artery; number 8, lymph nodes around the common hepatic artery; number 9, lymph nodes around the ce- liac trunk; number 10, lymph nodes at the hilus of the spleen; number 11, lymph nodes along the splenic ar- tery; number 12, lymph nodes of hepatoduodenal liga- ment; number 13, posterior pancreaticoduodenal lymph node; number 14, lymph nodes around the supe- rior mesenteric artery; number 15, lymph nodes along the middle colic artery; number 16, para-aortic lymph nodes; number 17, anterior pancreaticoduodenal lymph node; number 18, inferior body lymph nodes. In numbers 13 and 17, subgroups were defined: a, above the papilla of Vater; b, below the papilla. For number 14, four subgroups were defined: 14a, lymph nodes at the origin of the superior mesenteric artery; 14b, lymph nodes at the origin of the inferior pancreaticoduodenal artery; 14c, lymph nodes at the origin of the middle colic artery; 14d, lymph nodes at the origin of the je- junal arteries (Fig. 1). The para-aortic lymph node was subdivided into three regions in this study: 16S, supe- rior region above the celiac trunk; 16M, median region from the celiac trunk to the inferior mesenteric artery;
Figure 1. Nomenclature of the major lymph nodes of the pancreas. 5: suprapyloric lymph nodes; 6: infrapyloric lymph nodes; 7: lymph nodes around the left gastric artery; 8: lymph nodes around the common hepatic artery; 9: lymph nodes around the celiac trunk; 10: lymph nodes at the hilus of the spleen; 11: lymph nodes along the splenic artery; 12: lymph nodes in the hepatoduodenal ligament; 13: the posterior pancreaticoduodenal lymph node; 14: lymph nodes around the superior mesenteric artery; 15: lymph nodes along the middle colic artery; 16: para-aortic lymph nodes; 17: the anterior pancreaticoduodenal lymph node; 18: inferior body lymph nodes.
and 161, inferior region from the inferior mesenteric artery.
The relationships among lymph node groups were studied using the chi-square test.
Results
Table 1 shows the frequency of lymph node involve- ment related to the site of tumor origin. The metastatic rates of the number 8, 12, 13, 14, 16, and 17 lymph node groups were 9.7%, 9.7%, 6l%, 26%, 13%, and 25%, respectively, in the Ph group. However, the meta- static rates of these lymph nodes were 23.1%, 23.1°/o, 69%, 53%, 23%' and 4670, respectively, in the Phb group. Thus, the lymph nodes with the highest meta- static rates were numbers 13,14,16, and 17. There were no metastases in numbers 9 and 11 in the Ph group, but there was lymph node involvement in the Phb group.
The relationship between the tumor size and the degree of lymph node involvement is summarized in Table 2. Nodal involvement was determined as follows: NO, no evidence of regional lymph node involvement; Nl, nodal involvement in the primary group situated close to the tumor [numbers 8, 12 (in part), 13, 14, and 171; N2, lymph node metastasis in the secondary group [numbers 9, 11, 12 (in part), 15, and 161. Overall, 31 of 44 (70.5%) ductal carcinomas metastasized to lymph
Lymphatic Flow of Pancreatic Carcinoma/Kayahara et al. 2063
Table 1. Lymph Node Involvement in 44 Patients With Ductal Carcinoma in the Head of the Pancreas
Ph (n = 31) (%) No. Phb (n = 13) (%)
5 0 0 6 l (3 .3) 0 7 0 0 8 3 (9.7) 3 (23) 9 0 2 (15)
11 0 2 (15) 12 3 (9.7) 3 (23) 13 19 (61) 9 (69)
10 0 0
a 15 7 b 13 5
a 4 4 b 4 5 C 2 1 d 4 2
15 0 0
14 8 (26) 7 (53)
16 4 (13) 3 (23) 17 8 (25) 6 (46)
a 6 5 b 5 2
18 0 4 (31) No: nomenclature of lymph nodes; Ph: main tumor confined to pancreas head; Phb: some parts of tumor extended to the neck of pancreas.
nodes. There is a relationship between lymph node me- tastasis and tumor size for the smallest tumors, for which there are no metastases. For the larger sizes, there is no correlation. For example, 2 of 12 patients with T2a disease and 3 of 15 patients with t2b disease had tumor metastasize to para-aortic lymph nodes.
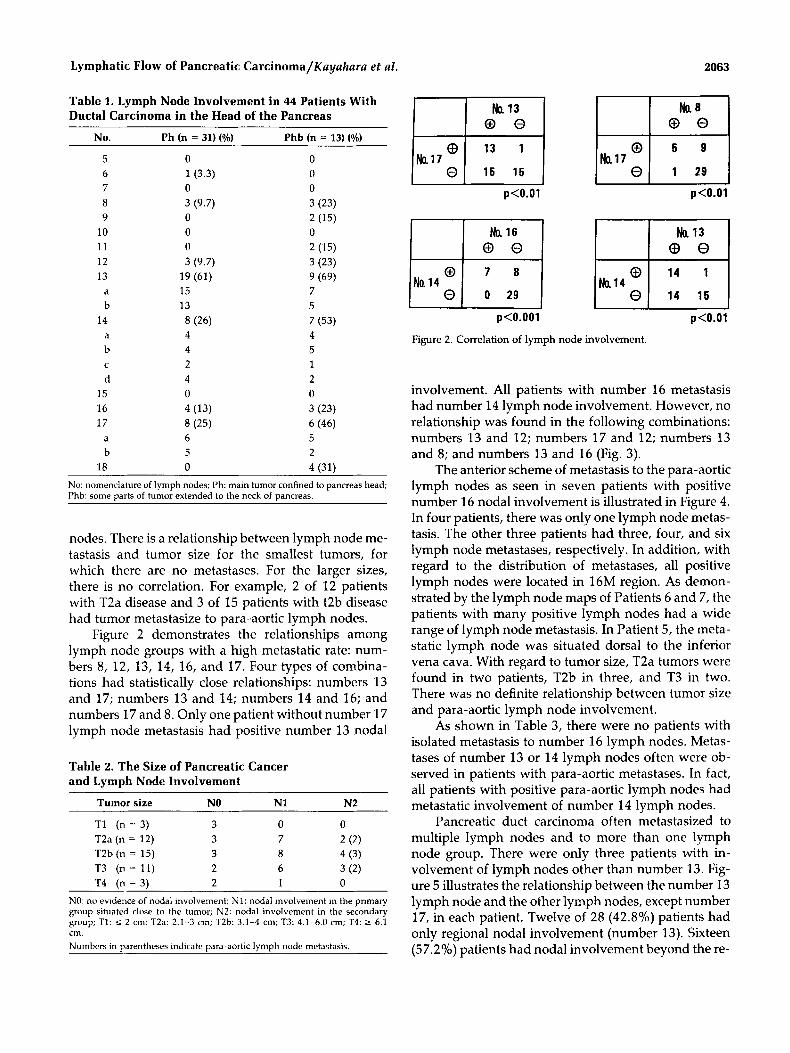
Figure 2 demonstrates the relationships among lymph node groups with a high metastatic rate: num- bers 8, 12, 13, 14, 16, and 17. Four types of combina- tions had statistically close relationships: numbers 13 and 17; numbers 13 and 14; numbers 14 and 16; and numbers 17 and 8. Only one patient without number 17 lymph node metastasis had positive number 13 nodal
Table 2. The Size of Pancreatic Cancer and Lymph Node Involvement
Tumor size NO N1 N2
T1 (n = 3) 3 0 0 T2a (n = 12) 3 7 2 (2) T2b (n = 15) 3 8 4 (3) T3 (n = 11) 2 6 3 (2) T4 (n = 3) 2 1 0
NO: no evidence of nodal involvement; N1: nodal involvement in the primary group situated close to the tumor; N2: nodal involvement in the secondary group; TI: 5 2 cm; T2a: 2.1-3 cm; T2b: 3.1-4 cm; T3: 4.1-6.0 cm; T4: 2 6.1 cm . Numbers in narentheses indicate oara-aortic lvmoh node metastasis
Na17 Nal7 0 1 29
p<O.Ol p<O.Ol
Nal4
p<O.OOl
Figure 2. Correlation of lymph node involvement.
p<O.Ol
involvement. All patients with number 16 metastasis had number 14 lymph node involvement. However, no relationship was found in the following combinations: numbers 13 and 12; numbers 17 and 12; numbers 13 and 8; and numbers 13 and 16 (Fig. 3).
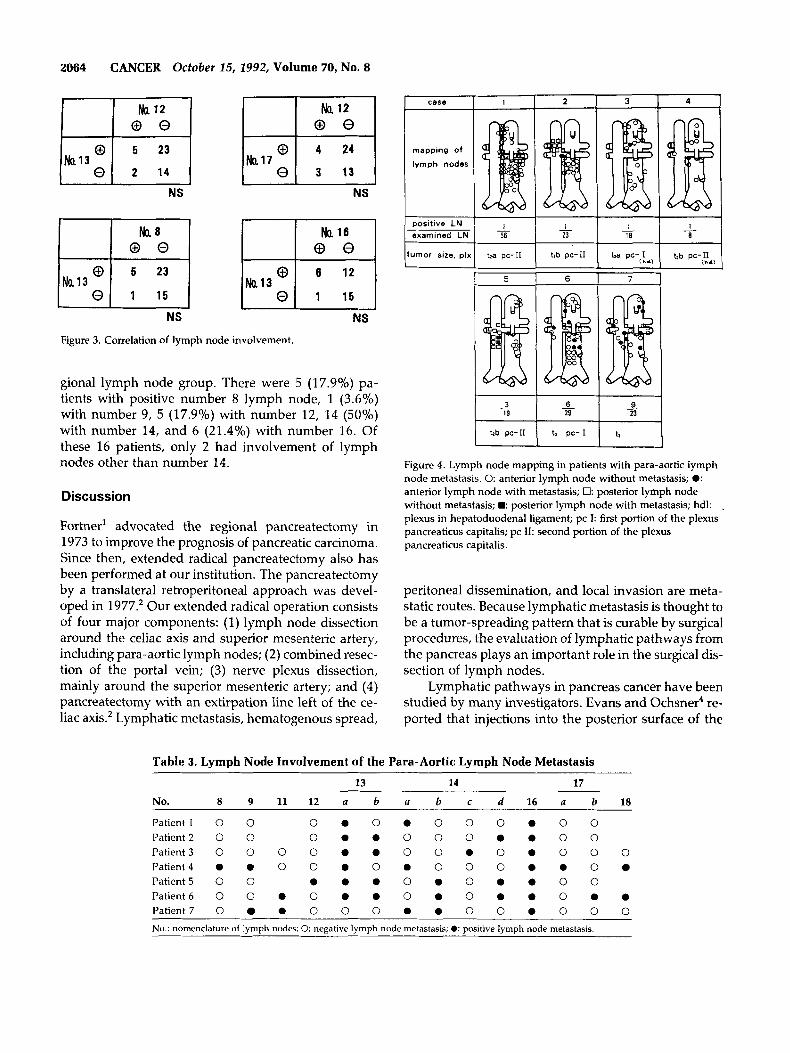
The anterior scheme of metastasis to the para-aortic lymph nodes as seen in seven patients with positive number 16 nodal involvement is illustrated in Figure 4. In four patients, there was only one lymph node metas- tasis. The other three patients had three, four, and six lymph node metastases, respectively. In addition, with regard to the distribution of metastases, all positive lymph nodes were located in 16M region. As demon- strated by the lymph node maps of Patients 6 and 7, the patients with many positive lymph nodes had a wide range of lymph node metastasis. In Patient 5, the meta- static lymph node was situated dorsal to the inferior vena cava. With regard to tumor size, T2a tumors were found in two patients, T2b in three, and T3 in two. There was no definite relationship between tumor size and para-aortic lymph node involvement.
As shown in Table 3, there were no patients with isolated metastasis to number 16 lymph nodes. Metas- tases of number 13 or 14 lymph nodes often were ob- served in patients with para-aortic metastases. In fact, all patients with positive para-aortic lymph nodes had metastatic involvement of number 14 lymph nodes.
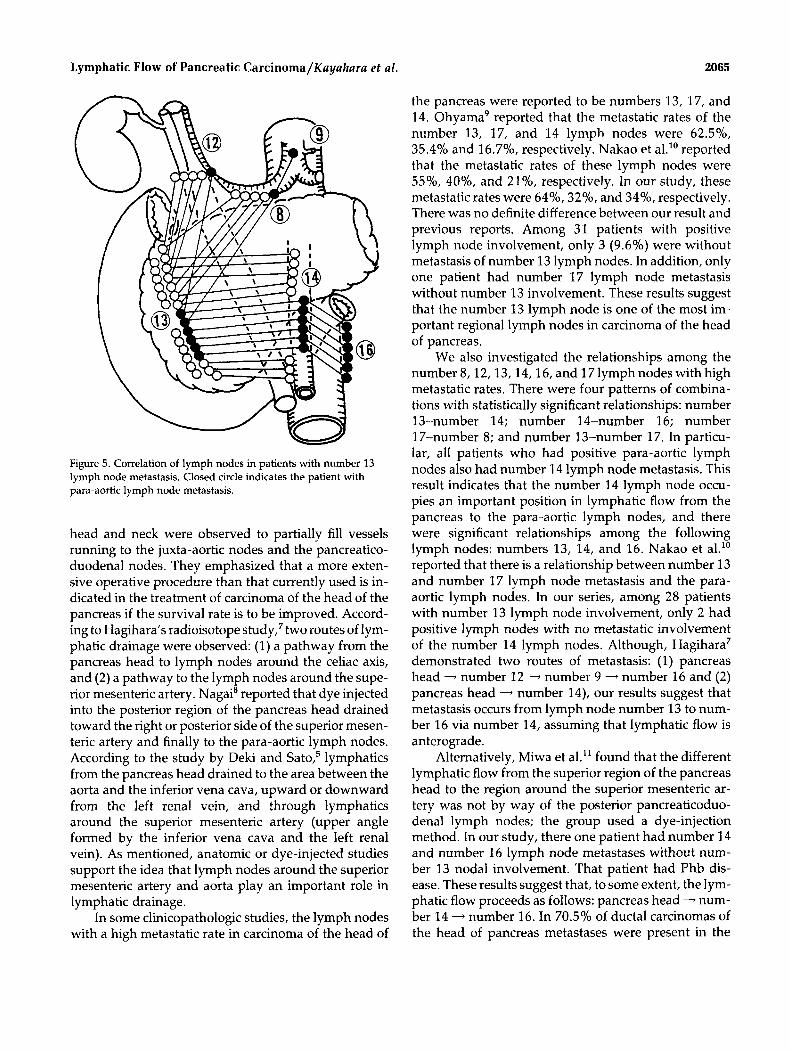
Pancreatic duct carcinoma often metastasized to multiple lymph nodes and to more than one lymph node group. There were only three patients with in- volvement of lymph nodes other than number 13. Fig- ure 5 illustrates the relationship between the number 13 lymph node and the other lymph nodes, except number 17, in each patient. Twelve of 28 (42.8%) patients had only regional nodal involvement (number 13). Sixteen (57.2%) patients had nodal involvement beyond the re-
2064 CANCER October 25, 2992, Volume 70, No. 8
NS
NS
El NS
Figure 3. Correlation of lymph node involvement.
gional lymph node group. There were 5 (17.9%) pa- tients with positive number 8 lymph node, l (3.6%) with number 9, 5 (17.9%) with number 12, 14 (50%) with number 14, and 6 (21.4%) with number 16. Of these 16 patients, only 2 had involvement of lymph nodes other than number 14.
Discussion
Fortner' advocated the regional pancreatectomy in 1973 to improve the prognosis of pancreatic carcinoma. Since then, extended radical pancreatectomy also has been performed at our institution. The pancreatectomy by a translateral retroperitoneal approach was devel- oped in 1977.' Our extended radical operation consists of four major components: (1) lymph node dissection around the celiac axis and superior mesenteric artery, including para-aortic lymph nodes; (2) combined resec- tion of the portal vein; (3) nerve plexus dissection, mainly around the superior mesenteric artery; and (4) pancreatectomy with an extirpation line left of the ce- liac axis.' Lymphatic metastasis, hematogenous spread,
case I I
mapping of
lymph nodes
examined LN
umor I size. plx tla pc-I1
2 3 I
--t- tzb pc-U t,a pc- I
1 5 6 7 I I
Figure 4. Lymph node mapping in patients with para-aortic lymph node metastasis. 0: anterior lymph node without metastasis; 0: anterior lymph node with metastasis; 0: posterior lymph node without metastasis; .: posterior lymph node with metastasis; hdl: plexus in hepatoduodenal ligament; pc I: first portion of the plexus pancreaticus capitalis; pc 11: second portion of the plexus pancreaticus capitalis.
.
peritoneal dissemination, and local invasion are meta- static routes. Because lymphatic metastasis is thought to be a tumor-spreading pattern that is curable by surgical procedures, the evaluation of lymphatic pathways from the pancreas plays an important role in the surgical dis- section of lymph nodes.
Lymphatic pathways in pancreas cancer have been studied by many investigators. Evans and Ochsner4 re- ported that injections into the posterior surface of the
Table 3. Lymph Node Involvement of the Para-Aortic Lymph Node Metastasis 13 14 17
No. 8 9 11 12 a b R b c d 16 a b 18
Patient I 0 0 0 0 0 . 0 0 0 0 0 0 Patient 2 0 0 0 0 . 0 0 0 0 0 0 0 Patient3 0 0 0 0 0 0 0 0 0 0 0 0 0 0 Patient4 0 0 0 0 0 0 0 0 0 0 0 0 0 Patient 5 0 0 0 . 0 0 0 0 . 0 0 0 Patient6 0 0 0 0 0 0 0 0 0 0 0 0 0 0 Patient7 0 0 0 0 0 0 0 0 0 0 0 0 0 0
No.: nomenclature of lymph nodes; 0: negative lymph node metastasis; 0: positive lymph node metastasis.
Lymphatic Flow of Pancreatic Carcinoma/Kayahara et al . 2065
W Figure 5. Correlation of lymph nodes in patients with number 13 lymph node metastasis. Closed circle indicates the patient with para-aortic lymph node metastasis.
head and neck were observed to partially fill vessels running to the juxta-aortic nodes and the pancreatico- duodenal nodes. They emphasized that a more exten- sive operative procedure than that currently used is in- dicated in the treatment of carcinoma of the head of the pancreas if the survival rate is to be improved. Accord- ing to Hagihara's radioisotope study,7 two routes of lym- phatic drainage were observed: (1) a pathway from the pancreas head to lymph nodes around the celiac axis, and (2) a pathway to the lymph nodes around the supe- rior mesenteric artery. Nagai' reported that dye injected into the posterior region of the pancreas head drained toward the right or posterior side of the superior mesen- teric artery and finally to the para-aortic lymph nodes. According to the study by Deki and sat^,^ lymphatics from the pancreas head drained to the area between the aorta and the inferior vena cava, upward or downward from the left renal vein, and through lymphatics around the superior mesenteric artery (upper angle formed by the inferior vena cava and the left renal vein). As mentioned, anatomic or dye-injected studies support the idea that lymph nodes around the superior mesenteric artery and aorta play an important role in lymphatic drainage.
In some clinicopathologic studies, the lymph nodes with a high metastatic rate in carcinoma of the head of
the pancreas were reported to be numbers 13, 17, and 14. Ohyama' reported that the metastatic rates of the number 13, 17, and 14 lymph nodes were 62.5%, 35.4% and 16.7%, respectively. Nakao et al." reported that the metastatic rates of these lymph nodes were 5.570, 40%, and 21%, respectively. In our study, these metastatic rates were 64%, 32%, and 34%, respectively. There was no definite difference between our result and previous reports. Among 31 patients with positive lymph node involvement, only 3 (9.6%) were without metastasis of number 13 lymph nodes. In addition, only one patient had number 17 lymph node metastasis without number 13 involvement. These results suggest that the number 13 lymph node is one of the most im- portant regional lymph nodes in carcinoma of the head of pancreas.
We also investigated the relationships among the number 8,12,13,14,16, and 17lymph nodes with high metastatic rates. There were four patterns of combina- tions with statistically significant relationships: number 13-number 14; number 14-number 16; number 17-number 8; and number 13-number 17. In particu- lar, all patients who had positive para-aortic lymph nodes also had number 14 lymph node metastasis. This result indicates that the number 14 lymph node occu- pies an important position in lymphatic flow from the pancreas to the para-aortic lymph nodes, and there were significant relationships among the following lymph nodes: numbers 13, 14, and 16. Nakao et al." reported that there is a relationship between number 13 and number 17 lymph node metastasis and the para- aortic lymph nodes. In our series, among 28 patients with number 13 lymph node involvement, only 2 had positive lymph nodes with no metastatic involvement of the number 14 lymph nodes. Although, Hagihara' demonstrated two routes of metastasis: (1) pancreas head - number 12 - number 9 - number 16 and ( 2 ) pancreas head - number 14), our results suggest that metastasis occurs from lymph node number 13 to num- ber 16 via number 14, assuming that lymphatic flow is anterograde.
Alternatively, Miwa et al." found that the different lymphatic flow from the superior region of the pancreas head to the region around the superior mesenteric ar- tery was not by way of the posterior pancreaticoduo- denal lymph nodes; the group used a dye-injection method. In our study, there one patient had number 14 and number 16 lymph node metastases without num- ber 13 nodal involvement. That patient had Phb dis- ease. These results suggest that, to some extent, the lym- phatic flow proceeds as follows: pancreas head - num- ber 14 - number 16. In 70.5% of ductal carcinomas of the head of pancreas metastases were present in the

2066 CANCER October 15,1992, Volume 70, No. 8
lymph nodes, so it appears that pancreatoduodenec- tomy in which the lymph nodes are not removed is not an adequate operation for carcinoma of the head of the pancreas.
In conclusion, a detailed study of nodal involve- ment in carcinoma of the head of the pancreas indicated that it is necessary to perform an extensive lymph node dissection, including dissection of the para-aortic lymph nodes.
References
1. Fortner JG. Regional resection of cancer of the pancreas: a new surgical approach. Surgery 1973; 73:303-20.
2. Nagakawa T, Kurachi M, Konishi K, Miyazaki I. Translateral retroperitoneal approach in radical surgery for pancreatic carci- noma. ]pn J Surg 1982; 12:229-33.
3. Nagakawa T, Konishi I, Higashino Y, Ueno K, Ohta T, Kayahara M, et al. The spread and prognosis of carcinoma in the region of the pancreas head. ] p n ] Surg 1989; 5:510-8.
4. Evans BP, Ochsner A. The gross anatomy of the lymphatics of the human pancreas. Surgery 1954; 36:177-91.
5. Deki H, Sat0 T. An anatomical study of the peripancreatic lym- phatics. Surg Radiol Anat 1988; 10:121-35.
6. Japanese Pancreatic Society. General rules for surgery and pathological studies on cancer of the pancreas. 3rd ed. Tokyo: Kanehara, 1986.
7. Hagihara K. Experimental and clinicopathological studies on lymphatic flows of pancreas [in Japanese]. Zgaku Kenkyu 1982;
8. Nagai H. An anatomical and pathological study of autopsy mate- rial on metastasis of pancreatic cancer to para-aortic lymph nodes [abstract in English]. Jpn ] Surg 1987; 88:308-17.
9. Ohyama R. Clinicopathological studies on carcinoma of the pan- creas with special reference to pathological factors affecting the prognosis and lymph node involvement [abstract in English]. ]pn ] Surg 1984; 852320-34.
10. Nakao A, Takeda N, Kasuga T, Nora T, Harada A, Takagi H. The significance of para-aortic lymph node dissection on pancre- atic cancer [in Japanese]. Nichi Gekakei Renkaishi 1990; 21:23- 26.
11. Miwa K, Yonemura Y, Yamaguchi M, Takashima S , Miyazaki I. Lymph node metastasis in carcinoma of the head of pancreas [in Japanese]. Gun No Rinsho 1979; 25:21-5.
52161-85.