Embed Size (px)
Citation preview

Lymphoma Tumor Board09TH AUG 2018

CASE 1
KG• 43 Yo Male, African
• Truck Driver• Lives in Khiruhura~3hrs from Kampala
• H/o Regular Alcohol intake but quit 4/12 ago, No Tobacco or any other illicit substance abuse• Single father of 10 children from two relationships• HIV+ since 2011,
• on HAART since,(now on second line: 3TC/ABC/Atazanavir+Ritonavir). • Nadir CD4+: 012(3/0CT/2011)• Ois: PTB (X2)

09 July 2018
• Referral Diagnosis (Oral Surgery Dept)
DIFFUSE LARGE CELL LYMPHOMA (Plasmablastic Variant)
(Soft Tissue from right gum/maxilla Swelling)• Microscopyè Squamous mucosa with high grade lymphoma comprising of
large lymphoid cells some with plasmablastic features. There are rare tumor giant cells. There are prominent nucleoli and vesicular chromatin
Conc: Diffuse Large Cell Lymphoma (Plasmablastic variant)

Presenting History
March 2018 • 5/12 h/o• Right gum/jaw swelling • a/w:-
• Loosening of teeth• Halitosis• Occasional bleeding on brushing
• No B-Symptoms• Fevers, night sweats, weight loss
• No headache, seizures, focal weakness, vomiting• No swellings else where
H/O Glans penis swelling x 1 year a/w foul smell

Physical Exam
G/E• Young male, well nourished , and not in distress, ecog-o, no pallor, no
Lymphadenopathy, no KS lesions, no HZ scars.• Locally: right jaw (maxillary) tumor ~ 7x5 cm multi-nodulated with
distortion of tooth architecture and Halitosis.
• Not circumcised, Infected genital warts in the glans penis/corona area
Systemic exam• Unremarkable

WORK-UP EVA
• CBC: • HBsAg: • LFTs: • RFTs: • LDH: • ECG+ECHO:• CD4+/VL:• ABD US:• BMA/BX:• LP-CSF:

Differentials
• Plasmacytoma / Myeloma• Cutaneous Violaceous KS• Bacillary angiomatosis• High Grade Lymphoma-DLCL

Histology Review + IHC
H&E• Tissue composed of diffuse infiltrate of atypical hyperchromatic
lymphoid cells with open nuclear chromatin some with plasmablastic/ immunoblastic morphology
IHC• CD20 NEGATIVE• Ki-67 ~ 70%
• CONC: HIGH GRADE NHL (PLASMABLATIC)

Diagnosis
• 43 YO HIV+ on Second Line HAART / Bactrim since 2011 with PBL, Genital warts & history of MTB therapy in the Past

DISCUSSION
• ?PBL vs Plasmacytoma• What is the Diagnostic Test of Choice?• What is IHC pattern in PBL?• ? Need for CD38. CD138, CD79a, MUM1
• What is the BAT for PBL?• EPOCH• Hyper-CVAD• CODOX-M/IVAC• CHOP


CASE 2
KP• 21 YO, Male African• University student• Social alcohol intake• No illicit substance abuse
• HIV: NEGATIVE

29 June 2018• Referral Diagnosis
ACUTE LYMPHOBLASTIC LYMPHOMA(Mediastinal Mass Bx)
• H&Eè Tissue composed of a monomorphic infiltrate of medium sized
atypical lymphoid cells in a fibrous stroma
• IHCè CD45+, CD20+, TdT+, Ki-67 ~90%, CD3-ve
• Flow Cytometryè Acute LBL with CD45, bright CD20, CD22 and bright HLA-
DR
Conc: Acute B LBL

KP
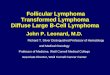
CD 45 Ki 67CD 20Tdt
H and E –monomorphic infiltrate of medium sized atypical lypnoid cells infiltrating stromaIHC- CD 45+,CD20+TDT+CD3-Ki67-(90%)Flow cytometry of the tissue-CD45 ,bright CD 20m,CD 22 and bright HLA –DRDiagnosis: B –LBLNo bone marrow involvement
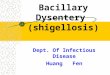
H and E

H and E- diffuse infiltrate of atypical hyperchromatic cells with open nuclear chromatin some with some plasmablastic /immunoblastic morphologyIHC- CD 20 -,Ki 67- 70%Dx: High grade NHL ?? Plasmblastic/immunoblasticNeed to do CD 138/38/56
H and E CD 20 Ki 67

Presenting History
February 2018 • 5/12 h/o• unwell• 4/52 worsening:-
• Dry cough• Retrosternal Chest Pain (on supination)
• + B-Symptoms• Fevers, night sweats, weight loss

Physical Exam
• GE• Unremarkable
• SYSTEMIC • Unremarkable

WORK-UP EVA
CXRè (14/06/2018)• Widening of the superior Mediastinum, cardiac shadow enlargement with
CTR of 9/19• Hilar shadows are dense and nodular• The lung fields show increased bronchovascular markings• Both costophrenic angles and hemi diaphragmatic contours appear normal.
The rib cage is normal.Conc: widened mediastinum, pneumonitis, cardiomegaly + ? Hilar adenopathy

CT-Scan- CHEST (20/06/2018)
• Large soft tissue attenuating mass occupying the anterior mediastinum, displaying homogenous attenuation with low desnityareas of cystIc changes (27HU) inside. It extends to the middle mediastinum to occupy the pretracheal space and involve the right hilum. Inferiorly it is inseparable from the anterior pericardium and the mediastinal pleura laterally. Compression & encasement of the SVC, left innominate vein, encasement of aorta an dpulmonary trunk is noted. The mass extends from the thoracic inlet, anteriorly bound by the sternum, posteriorly bound by the trachea and inferiorly bound by the pericardium with loss of fat planes between them.

• It shows heterogenous enhancement 27-33 HU pre contrast to 38-72 HU post contrast, no clacifications seen within the mass.• The mass measures 12.3x7.8x13.0 cm (LXWXH)• There is no bronchial obstruction. There are no lung nodules or areas
of consolidation seen bilaterally, no pleural or pericardial effusion.• No neck masses seen. No significant axillary adenopathy.• No suscipcious bone lesions seen. No abnormalities in the
demonstrated part of the abdomen.Conc: Features are of a huge soft tissue attenuating anterior
mediastinal mass with vascular encasement; this is likely Lymphoma.DDx: Thymoma, Teratoma

• ECGè Sinus Tachycardia• ECHOè Large Mediastinal Mass compressing the RV and anterior
outlet parts of the RV outflow with no Hemodynamic compromiseEF à 52.1%
• CBC: WCC 14.11, ANC 11.27 HB 13.7 PLT 646• HBsAg: Negative, HCV Negative• BMA/Bx: Negative for Lymphoma• LP-CSF: NEGATIVE

• LDH: 435.4• LFTS-Normal• RFTS-Normal

DIAGNOSIS
• KP, 21 YO Male HIV / Hepatitis Negative with Acute B LBL

TREATMENT-OPD
• ALL-INDUCTION REMISSION with LINKER’S REGIMEN• Daunorubicin 75mg D1-D3• Vincristine 2mg D1 D8 D15 & D22• Prednisolone 100mg D1-D28• L-Asparaginase 9,000 IU D17-D28

OUTCOME POST INDUCTION REMISSION
• Tolerated Treatment well
WCC ANC HB PLT26/6/18 14.11 11.27 13.7 64605/7/18 13.37 11.95 13.8 57109/7/18 8.26 7.52 14.4 46516/7/18 1.51 0.72 13.8 28619/7/18 1.49 0.68 14.5 27223/7/18 5.73 4.27 13.8 36230/7/18 7.18 5.98 15.8 395

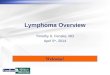
Post-Induction Remission CT-Scan CHEST(3/AUG/2018)• è Anterior mediastinal mass in the region of the thymic gland; it measures
106x82x75mm and traverses T2-T6; there is no abnormal enhancement. There are no solid mediastinal masses seen.• The lung parenchyma is normal; no focal lesions are seen.• There is no interlobular septal thickening.• There are no enlarged mediastinal /hilar/axillary lymphnodes seen.• Normal thoracic aorta and pulmonary arteries.• The pleura and pericardial spaces are normal, no fluid accumulation is
seen.• The demonstrable bones show no suspicious lesions.• The demonstratble liver, spleen, gallbladder and both kidneys are normal.
(Initial: 123x130x78)

Conc: • Anterior Mediastinal mass in keeping with diffuse homogenous
enlargement of the thymic gland; Thymic hyperplasia is a differential.• Mass is reduced in size compared to previous.

DISCUSSION
KP, 21 YO with Acute B LBL PR/SD Status Post INDUCTION REMISSION
• If True Acute B LBL----What is BAT?
• WHAT IS WAY-FORWARD• MANTLE RADIATION• CONSOLIDATION• SALVAGE INDUCTION
• IS DIAGNOSIS RIGHT?• THYMOMA• TERATOMA• T-CELL LBL