Embed Size (px)
Citation preview
Invited Review
Magnetic Resonance and Computed TomographyImaging of Arrhythmogenic Right VentricularDysplasia
Harikrishna Tandri, MD,1 Chandra Bomma, MD,1 Hugh Calkins, MD,1 andDavid A. Bluemke, MD, PhD2*
Arrhythmogenic right ventricular dysplasia (ARVD) is afamilial cardiomyopathy that causes fibro-fatty replace-ment of the right ventricle (RV), leading to sudden deathdue to ventricular arrhythmias. The disease is an impor-tant cause of sudden death in individuals younger than35 years of age. Structural and functional abnormalitiesof the RV constitute an important diagnostic criterion forthe disease. Diagnosis of ARVD is often a challenge asconventional imaging modalities have significant limita-tions to visualize the RV. Recently, magnetic resonanceimaging (MRI) and computed tomographic (CT) imaginghave emerged as robust clinical tools for evaluation ofmyocardial pathology. In addition to providing morpho-logic and functional information, both imaging modali-ties have the ability to demonstrate intramyocardial fat,which is the pathological hallmark in ARVD. This articlediscusses the current status and role of MRI and CTimaging in the diagnosis of ARVD.
Key Words: MRI; CT; right ventricular dysplasia; cardio-myopathy; diagnosisJ. Magn. Reson. Imaging 2004;19:848–858.© 2004 Wiley-Liss, Inc.
ARRHYTHMOGENIC RIGHT VENTRICULAR dysplasia(ARVD) is a genetic cardiomyopathy characterized byfibro-fatty replacement of the right ventricular (RV)musculature, which leads to ventricular arrhythmiasand RV failure (1,2). This condition accounts for up to5% of sudden deaths in young individuals less than 35years of age in the United States, and 25% of exercise-related deaths in the Veneto region of Italy (3,4). The
exact prevalence of this condition is not known, but isestimated to be around 1 in 5000. The disease rarelymanifests before adolescence and usually presents inthe second or third decade of life (1). Affected individu-als are often men who have an athletic lifestyle. Pre-senting symptoms vary from asymptomatic individualswith occasional palpitations to syncope or even to sud-den death. The disease is inherited in an autosomaldominant fashion. A common clinical scenario is thedeath of a family member with autopsy showing ARVD,which prompts screening of the first-degree relatives.
Diagnosis of ARVD presents a challenge for the clini-cian, as the nature of RV involvement in early stages ofARVD is poorly understood. The diagnosis is based on aset of major and minor criteria proposed by the TaskForce of cardiomyopathies in 1994 (5). These criteriaencompass electrical, anatomic, and functional abnor-malities that are a consequence of progressive fibro-fatty infiltration, which results in loss of RV myocytes.Structurally, this manifests as regional reduction inwall thickness, wall hypertrophy, and focal bulging ofthe RV wall in diastole. Focal or global contraction ab-normalities, chamber enlargement, enlarged RV out-flow tract (RVOT), and RV aneurysms have been de-scribed. Accurate and detailed evaluation of the RVstructure and function is essential for the diagnosisand for screening of the first-degree relatives.
Noninvasive modalities commonly used to evaluatethe RV include two-dimensional echocardiography andradionuclide ventriculography. Both modalities havesignificant limitations in assessing the RV due to itscomplex geometry (6,7). Because RV involvement inARVD is nonuniform, complete and multiplanar as-sessment of the RV is desirable. Recently, magneticresonance imaging (MRI) and computed tomography(CT) have emerged as robust tools to evaluate cardiacstructure and function (8–11). Both techniques canprovide direct evidence of fatty infiltration and struc-tural alterations of the RV (12,13). The noninvasivenature of these investigations, multiplane capability,and unique ability to provide tissue characterizationare ideal for assessment of ARVD. The purpose of thecurrent review is to discuss the current status,
1Division of Cardiology, The Johns Hopkins University, Baltimore,Maryland.2Department of Radiology, The Johns Hopkins University, Baltimore,Maryland.Contract grant sponsor: National Institutes of Health; Contract grantnumber: Research Grant 1 UO1 HL65594-01A1; Contract grant spon-sor: Johns Hopkins ARVD center (funded by a private grant from theBogle Foundation).*Address reprint requests to: D.A.B., MRI, Room 143 (Nelson Base-ment), The Johns Hopkins Hospital, 600 N. Wolfe St., Baltimore MD21287. E-mail: [email protected]; ;www.arvd.comReceived July 14, 2003; Accepted March 4, 2004.DOI 10.1002/jmri.20078Published online in Wiley InterScience (www.interscience.wiley.com).
JOURNAL OF MAGNETIC RESONANCE IMAGING 19:848–858 (2004)
© 2004 Wiley-Liss, Inc. 848

strengths, and limitations of MRI and cardiac CT inevaluation of patients with suspected ARVD.
MRI OF ARVD
Among the current cardiac MR applications in cardio-myopathies, the greatest potential as well as biggestchallenges are in the diagnosis of ARVD. Compared toconventional imaging modalities, MR is uniquely suitedto evaluate ARVD. The three-dimensional depiction ofanatomy by MRI allows both qualitative and quantita-tive analysis of RV function (14). MR has the ability todemonstrate intramyocardial fat, which is the patho-logical hallmark of ARVD (12). The last 10 years haveseen significant improvements in MR hardware, withtremendous increases in acquisition speed and imagequality. The development of ECG gating and the use ofbreath-hold imaging have significantly reduced motionartifacts. Improved tissue contrast is currentlyachieved by the use of inversion recovery black-bloodimaging techniques for depiction of cardiac morphology(15). Improvements in cine imaging using ECG-gatedsteady-state free precession imaging (SSFP) pulse se-quence have resulted in better delineation of endocar-dial borders, enabling accurate and reproducible volu-metric measurements (14). For these reasons, MRI hasbeen increasingly used in evaluation of the RV and hasevolved as the noninvasive modality of choice in ARVD.
Casolo et al (12) were the first to describe the use ofMRI to assess ARVD in 1987. They demonstrated in-tramyocardial fat deposits in the RV on conventionalspin echo (SE) imaging in a patient with advancedARVD. Since that time, several authors, including ourgroup, have reported MR abnormalities in ARVD (16–25). Broadly, MRI abnormalities in ARVD can begrouped into two major categories: 1) morphologicalabnormalities and 2) functional abnormalities. Mor-phologic abnormalities include intramyocardial fat de-posits, focal wall thinning, wall hypertrophy, trabeculardisarray, and RVOT enlargement. Functional abnor-malities include regional contraction abnormalities, an-eurysms, RV global dilation/dysfunction, and RV dia-stolic dysfunction. The sites of involvement of theseabnormalities are observed in the “triangle of dyspla-sia,” which is constituted by the inferior subtricuspidarea, RV apex, and RV infundibulum (26) (Fig. 1). Thegoal of MRI in ARVD is to accurately assess the RV forthe presence or absence of these abnormalities, whichaids not only in the diagnosis but also in follow-up ofpatients.
MR Assessment of Cardiac Morphology in ARVD
Accurate depiction of morphology is very important inmost cardiac applications, and ARVD exemplifies thisstatement. Morphologic evaluation is generally per-formed by the use of black-blood techniques. Conven-tional SE pulse sequences were initially used to evalu-ate cardiac morphology, and the majority of studies inliterature have used SE imaging for ARVD. Black bloodin the cardiac chambers is obtained by the saturation ofinflowing blood signal both above and below the ac-quired volume. Disadvantages include long acquisition
times, precluding breath holding, and resulting motionartifacts, which degrades image quality. Blood suppres-sion is often poor in the long-axis planes and is ineffec-tive for slow flow in the atria and RV.
Currently, black-blood techniques using breath-holdimaging with double-inversion recovery fast SE (DIR-FSE) techniques are preferred to traditional SE imag-ing. Breathhold FSE sequences consistently provideend-diastolic images with minimal motion artifacts andimprove resolution of myocardial detail (27–29). Black-blood inversion-prepared half-Fourier single-shot turboSE (HASTE) imaging has not been systematically eval-uated, but is currently not recommended due to blur-ring of detail with this sequence. A dedicated cardiaccoil is recommended for best results, although we useonly the anterior coil elements to prevent wraparoundartifact when using a small field of view (FOV). An an-terior saturation band (Fig. 2) is placed over the anteriorsubcutaneous fat for further suppression of motion ar-tifacts.
Morphologic Features of ARVD
Intramyocardial Fat
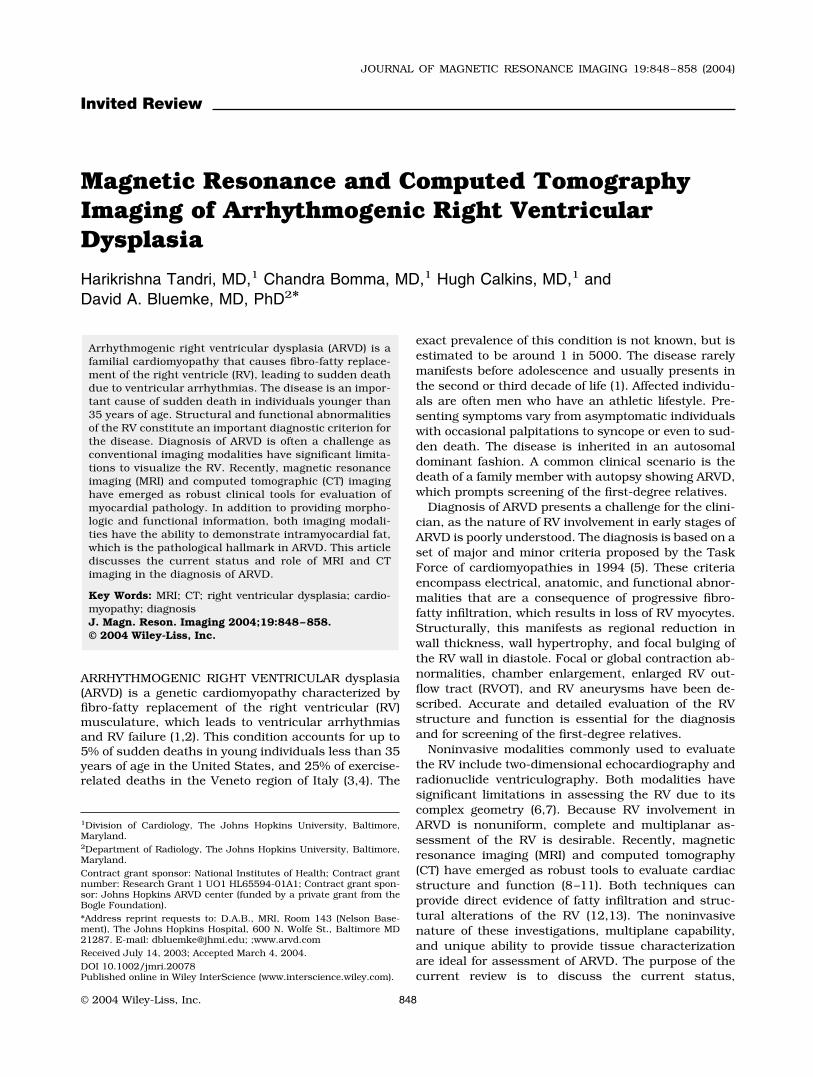
Normal myocardium shows an intermediate signal sim-ilar to that of skeletal muscle, and fat appears as ahyperintense signal (bright) on black-blood images. Fig-ure 3A shows a black-blood image from a normal vol-unteer. In normal individuals epicardial fat overlies theRV and is abundant toward the RV apex and in theatrioventricular groove. There is often a clear line ofdemarcation between the gray RV myocardium and theepicardial fat. Disruption of this line of demarcation(Fig. 3B) and extension of the hyperintense signals intothe RV myocardium are frequently noted in ARVD, in-dicating infiltration of epicardial fat into the RV wall.
Figure 1. GRE image in the oblique saggital plane showing thetriangle of dysplasia, which is constituted by the inferior sub-tricuspid area (thick white arrow), RV apex (black arrow), andRV infundibulum (thin white arrows). RA, right atrium; PA,pulmonary artery.
MR and CT Imaging of ARVD 849
The prevalence of intramyocardial hyperintense sig-nals in ARVD on T1-weighted SE imaging has rangedfrom 22% to 100% in different studies (16–25). Thelargest series is by Auffermann et al (20), who imaged36 biopsy-proven ARVD patients and found intramyo-cardial hyperintense signals in only 22% of patients.The patients in this study had different stages of ARVD,and a significant number had localized ARVD. An in-teresting finding of this study was that fat infiltration onMRI, not on biopsy, predicted inducibility of ventriculartachycardia at electrophysiologic testing. Wichter (21)added 16 additional patients to the series by Auffer-mann et al (52 total patients) and concluded that pa-tients with extensive ARVD had higher incidence offatty replacement of the RV, compared to localizedforms (96% vs. 58%). Menghetti et al (25) described SEMRI findings in 15 ARVD patients diagnosed using theTask Force criteria and reported intramyocardial hy-perintense signals in 62% of patients. The differences inincidence of fat signal in ARVD are largely based ondifferences in patient selection and the definition ofabnormal intramyocardial hyperintense signals.
We used the breath-hold DIR-FSE technique to eval-uate intramyocardial fat in ARVD and found a highintramyocardial T1 signal (fat) in 9 of 12 patients (75%)who were prospectively diagnosed using the currentTask Force criteria (16). The use of spectrally selectivefat suppression with the DIR-FSE sequence providedadditional evidence of fat infiltration due to high con-trast between epicardial fat and the RV myocardium. Afat-suppressed sequence may demonstrate a signalvoid within the myocardium, in a location where a highsignal was observed in the non-fat-suppressed image.This increases the confidence for the diagnosis of fatsignal, in particular in exams where the results of non-fat-suppressed images are inconclusive (Fig. 4A and B).Fatty infiltration was more commonly noted in thebasal regions (RV inflow and outflow) and less fre-quently at the RV apex (one of nine patients). Biopsywas abnormal in six of the nine patients and the rest
had normal biopsies. Biopsies, however, may be incon-clusive due to sampling error, since the biopsy site isoften the RV septum, which may not be involved in thedisease process. Biopsy of the thin anterior RV wallcarries a risk of perforation and hemopericardium.
Wall Thinning
RV wall thinning is defined focal abrupt reduction inwall thickness of �2 mm, surrounded by regions ofnormal wall thickness. The exact pathogenesis of wallthinning is not known, but it is thought to be due toapoptotic loss of RV myocytes. Progressive loss of epi-
Figure 2. Axial black-blood image showing the location ofanterior saturation band (arrow).
Figure 3. A: Axial black-blood image from a normal volunteershowing a clear line of demarcation between the epicardial fatand the underlying myocardium. Also note the abundance ofepicardial fat in the atrioventricular groove (arrowhead) and atthe apex (arrow). B: Axial black-blood image from a patientwith RV dysplasia showing lack of demarcation between epi-cardial fat and myocardium (arrows).
850 Tandri et al.
cardial and myocardial layers leaves behind a thin rimof endocardial cells, which are usually not involveduntil late in the disease process. This finding oftenobserved in pathologic specimens was not revealed invivo until the emergence of MRI. Compared to intramyo-cardial fat, fewer reports have addressed the issue ofwall thinning in ARVD. Typically the in-plane resolu-tion of DIR-FSE is approximately 1.5 mm. The resolu-tion is further reduced by motion artifacts. Auffermannet al (20) reported wall thinning in 67% of biopsy-proven ARVD patients on SE MRI. In our series we
found wall thinning in less than 25% of patients whomet the Task Force criteria (Fig. 5). Wall thickness isoften difficult to assess due to adjacent high epicardialfat signal and motion artifacts that are increased inpatients with arrhythmias. The use of chemical shift fatsuppression may reveal the true thickness of the RVwall, making its identification more reliable.
Wall Hypertrophy
Wall hypertrophy is defined as RV wall thickness of �8mm. This finding is seldom observed in pathologic spec-imens as the true RV myocardium is measured exclu-sive of the epicardial fat (30). In vivo this differentiationis sometimes not possible due to extensive fibro-fattyinfiltration with loss of distinction between epicardialfat and the true myocardium. In such cases the RV wallappears hypertrophied with MR images showing is-lands of gray muscle surrounded by bright signals com-patible with fat. This finding was observed in 5 of the 12patients (42%) in our series. Use of fat suppressionreveals multiple signal voids within the RV myocardiumin locations that showed hyperintense signals in thenon-fat-suppressed images (Fig. 6A and B).
Trabecular Disarray
Molinari et al (24) were the first to describe giant Y-shaped trabeculae and hypertrophy of the moderatorband in patients with ARVD. This finding has beenequated to the angiographic finding of deep fissureswith a “pile d’assiettes” (stack of plates) appearance. Wefound a prevalence (40%) of trabecular hypertrophyand disarray similar to that of the above study in ARVDpatients (Fig. 7). This finding is not specific for ARVD
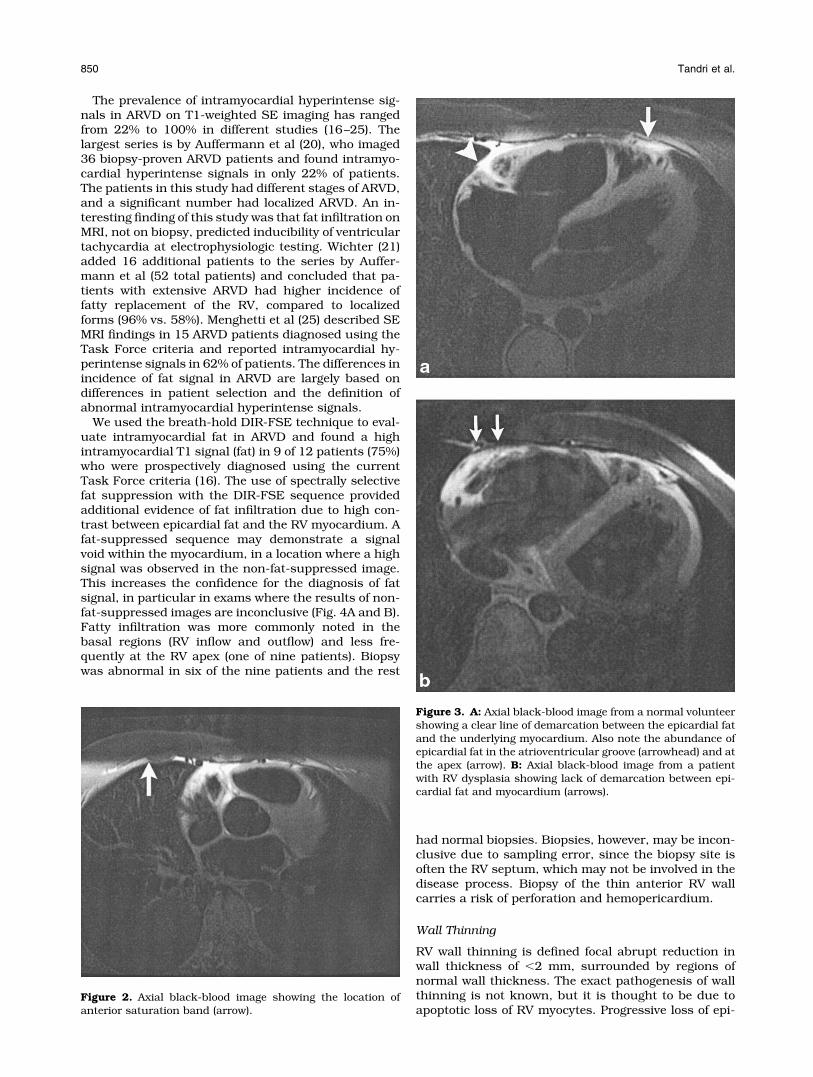
Figure 4. A: Axial black-blood image from a control subjectshowing heterogeneously increased T1 signal (arrow) towardthe RV inflow region. B: Fat-suppressed version at the samelevel reveals normal RV wall without any abnormality (arrow).
Figure 5. Fat-suppressed axial black-blood image from a pa-tient with RV dysplasia showing focal abrupt thinning (arrow-heads) of the anterior wall of the RV.
MR and CT Imaging of ARVD 851
and may be present in any condition that results in RVhypertrophy or enlargement.
RVOT Enlargement
The RVOT is a common location for localized ARVD. TheRV outflow is usually equal to or marginally smallerthan the aortic outflow tract at the level of the aorticvalve. An exception to this rule is pediatric patients inwhom the RVOT may be larger than the left ventricularoutflow. Presence of an enlarged RVOT beyond adoles-cence is uncommon. Ricci et al (22) reported enlarged
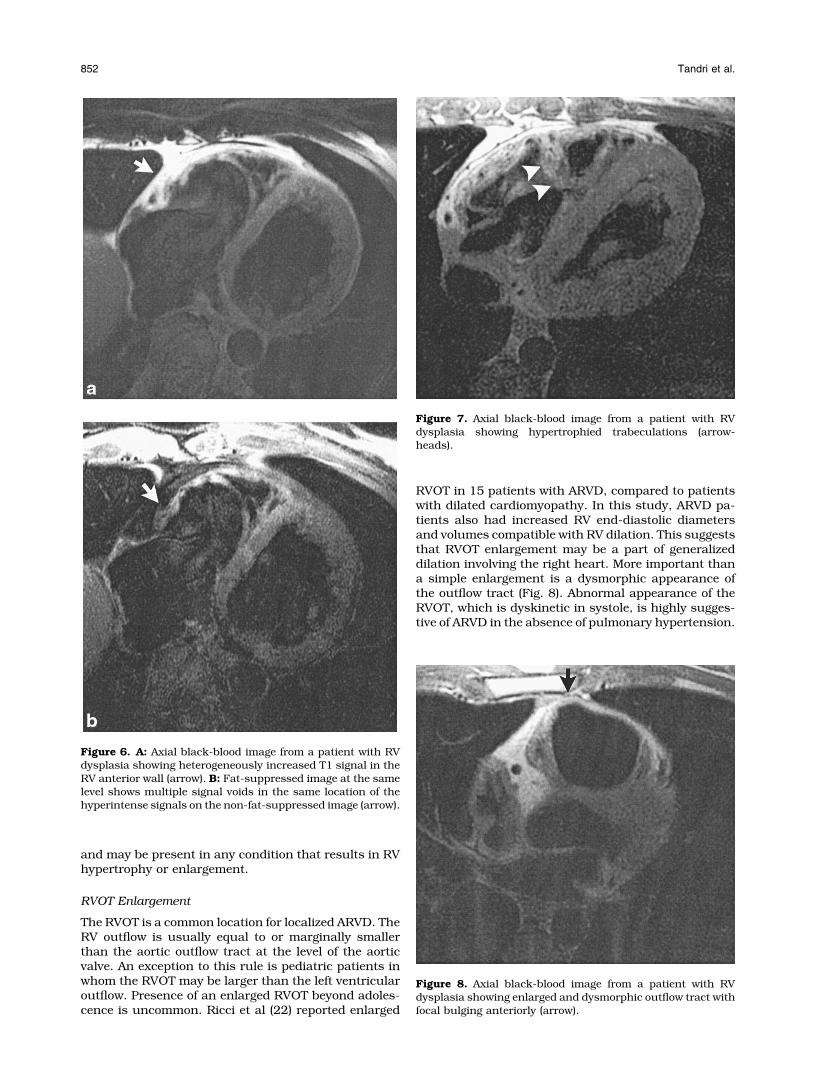
RVOT in 15 patients with ARVD, compared to patientswith dilated cardiomyopathy. In this study, ARVD pa-tients also had increased RV end-diastolic diametersand volumes compatible with RV dilation. This suggeststhat RVOT enlargement may be a part of generalizeddilation involving the right heart. More important thana simple enlargement is a dysmorphic appearance ofthe outflow tract (Fig. 8). Abnormal appearance of theRVOT, which is dyskinetic in systole, is highly sugges-tive of ARVD in the absence of pulmonary hypertension.
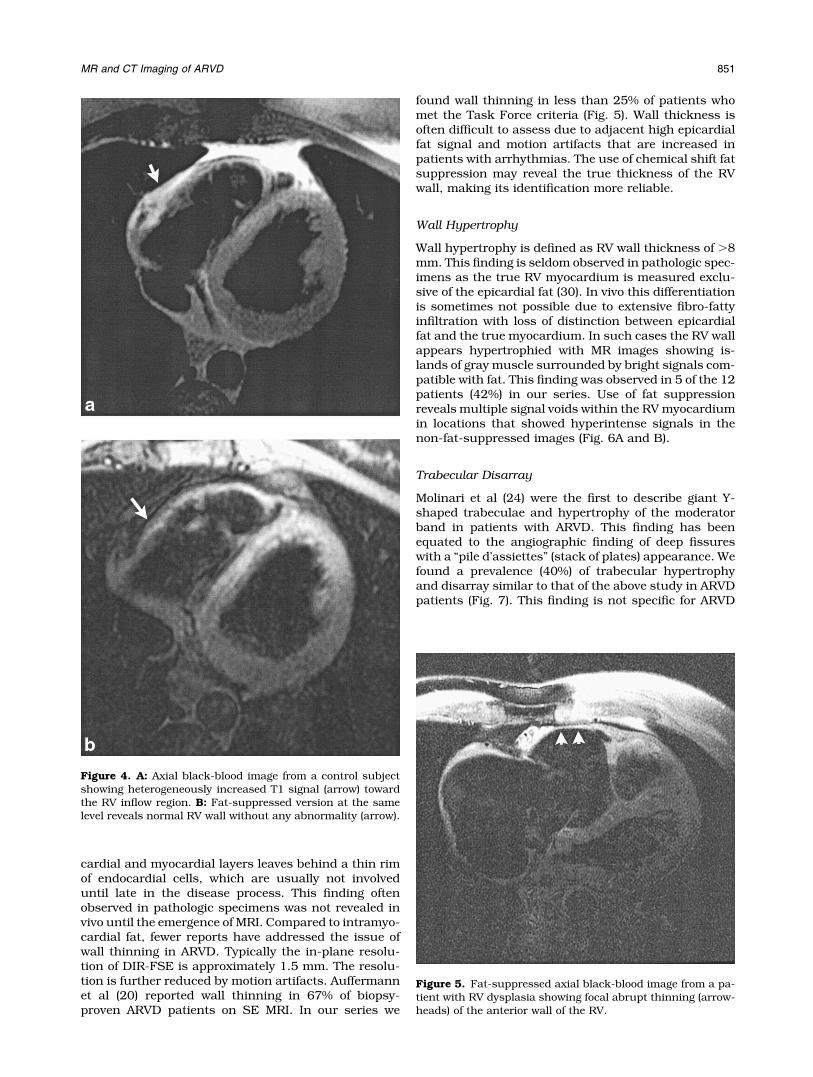
Figure 6. A: Axial black-blood image from a patient with RVdysplasia showing heterogeneously increased T1 signal in theRV anterior wall (arrow). B: Fat-suppressed image at the samelevel shows multiple signal voids in the same location of thehyperintense signals on the non-fat-suppressed image (arrow).
Figure 7. Axial black-blood image from a patient with RVdysplasia showing hypertrophied trabeculations (arrow-heads).
Figure 8. Axial black-blood image from a patient with RVdysplasia showing enlarged and dysmorphic outflow tract withfocal bulging anteriorly (arrow).
852 Tandri et al.

MR Assessment of Cardiac Function in ARVD
One of the major advances in MR cardiac imaging hasbeen the ability to accurately assess global and regionalventricular function without using geometric assump-tions. Until the availability of cine MRI, the complexgeometry of the RV made quantification by conven-tional two-dimensional techniques impossible. Thetechniques to image cardiac function are called bright-blood techniques, derived from the appearance of int-racavitary blood. These techniques yield both morpho-logic and functional data. Multiple consecutive imagesthat are acquired with a high temporal resolution canbe viewed dynamically to generate functional informa-tion. Ventricular volumes and masses using bright-blood imaging have been shown to be accurate andreproducible, and MRI is considered the standard ofreference (31,32). Although a number of sequences ex-ist for bright-blood imaging, SSFP imaging is the mostpreferred technique (FIESTA, true FISP, Balanced FastField Echo). SSFP sequences result in improved con-trast between the blood pool and the myocardium withbetter delineation of papillary muscles and trabecula-tion compared to segmented k-space cine gradient echo(GRE) images (33). Blood signal is hyperintense onSSFP images, and this is especially important in imag-ing the RV. If SSFP is not available, segmented k-spacecine gradient echo images (e.g., fast low-angle shot(FLASH), fast cardiac-gated gradient echo (FASTCARD))can be used. Conventional cine k-space GRE imagesrely on flowing blood to generate bright blood. In thedysfunctional RV, blood velocities are reduced and sig-nal intensity decreases with conventional GRE imaging.With SSFP, the signal intensity remains high since thesignal intensity is proportional to T2 time.
Global functional assessment is useful and can beaccurately performed using cine imaging. But it is wellknown that ejection fraction reduction and ventriculardilation may not be sensitive indicators of myocardialpathology. This is especially true of ARVD where re-gional functional abnormalities often precede changesin global function. The multiplane nature of MRI, thehigh contrast between the blood pool and myocardium,and the high spatial resolution have made it possible tovisually assess regional RV dysfunction, which hasbeen the focus of several authors in ARVD assessment.There exists an excellent correlation between MRI andRV angiography (17), the later being the traditional goldstandard for RV function. For the above reasons, MRI isa noninvasive alternative for RV functional assessmentin screening of first-degree relatives for ARVD and alsofor follow-up.
Functional Abnormalities in ARVD
Global RV Dilation/Dysfunction
Fibro-fatty replacement of the RV in ARVD eventuallyleads to RV dilation and dysfunction. RV dysfunction isoften asymptomatic (34), but is preceded by symptomsrelated to an associated arrhythmia. MRI does not offerany advantage in patients who have severe reduction inRV function (ejection fraction � 35%), as this can bedetected even on echocardiography. The advantage of
MRI is to be able to detect minor changes in ventricularvolumes over time, which provides insight into an evolv-ing disease process. MR has the capability to accuratelyand quantitatively measure ventricular volumes, andminor increases in RV end-diastolic volumes may be asubtle and early sign of ARVD. Auffermann et al (20)reported an increased RV end-diastolic volume index in10 patients with ARVD who were inducible on electro-physiologic studies, compared to control subjects. TheRV volume indices and the global function of ARVDpatients, who were noninducible, did not differ fromthose of the control subjects, suggesting that the pa-tients in this group had localized ARVD. Several otherauthors have reported RV enlargement and dysfunctionusing a variety of patient selection criteria. In our reportwe found that a majority of patients (75%) who meet theTask Force criteria have some degree of RV enlargementand dysfunction at presentation. Also, there was a lin-ear correlation between the RV end-diastolic volumesand the duration of symptoms, suggesting the progres-sive nature of the disease (16). Serial quantitative volu-metric assessment of RV may play an important role inassessing disease progression and may have an impor-tant role in evaluation of first-degree relatives.
Regional Dysfunction
Much remains to be understood about the pathophys-iology of regional dysfunction in ARVD, but regionaldysfunction is generally thought to be due to focal fibro-fatty infiltration. Areas of fibrosis result in wall thinningwith focally reduced contraction and aneurysm forma-tion. These are thought to precede changes in globalventricular function, and accurate identification mayimprove the sensitivity of diagnosis. RV angiographywas traditionally used to evaluate this, but currentlyMRI has replaced RV angiography due to its noninva-sive nature.
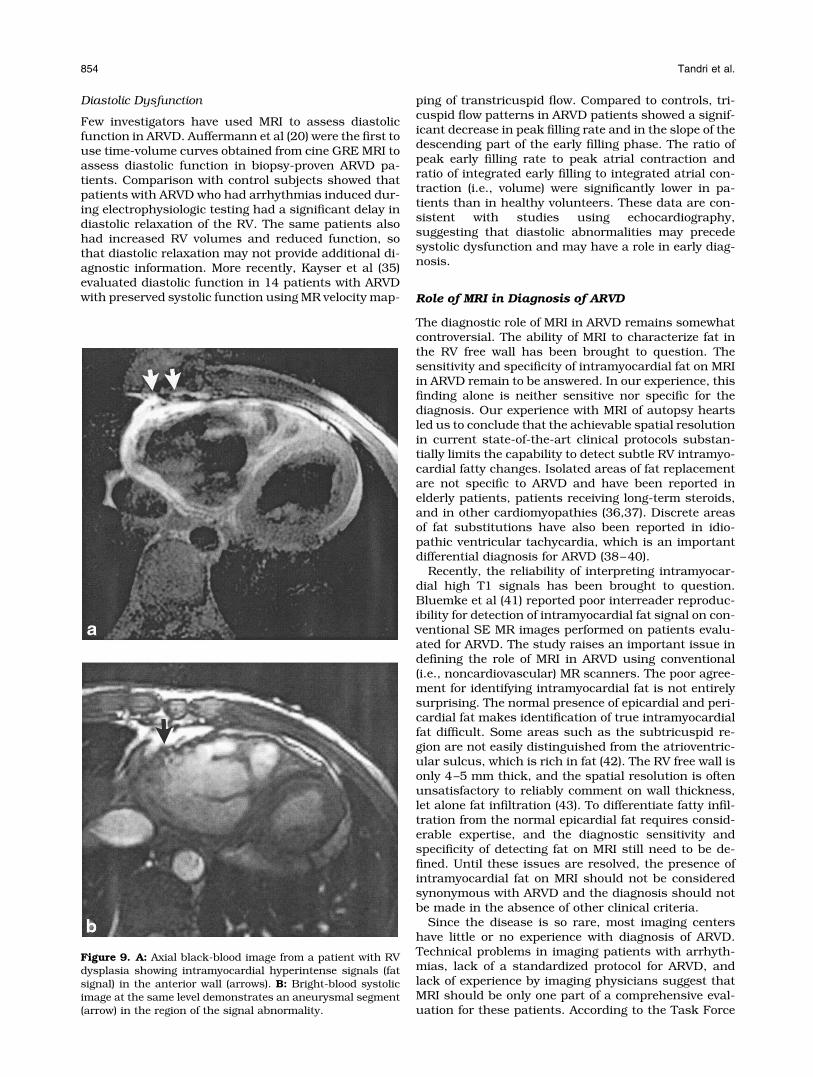
Regional functional abnormalities of the RV de-scribed in ARVD include focal hypokinesis (wall thick-ening of �40%), akinesis (systolic wall thickening of�10%), dyskinesis (myocardial segment, which movesoutward in systole), and aneurysms (segments withpersistent bulging in diastole and dyskinetic in systole).Studies have consistently reported high incidence ofregional dysfunction in ARVD (16–25). One study,which compared MRI to angiography, showed 86% cor-relation between the two modalities (17). The areas ofdysfunction corresponded to the areas of signal abnor-mality observed on black-blood MRI. In patients pre-senting with arrhythmias of RV origin, the finding ofisolated regional functional abnormalities limited to theRV may not be specific for the diagnosis of ARVD. Butthe presence of signal abnormality associated with ab-normal wall motion is more suggestive of ARVD thaneither of them alone. In our series, 67% of the patientshad regional contraction abnormalities, which corre-lated to the area of adipose replacement on MRI (Fig. 9Aand 9B). Of these patients, 50% had aneurysms local-ized to the region of adipose replacement. But overall,aneurysm formation was only observed in 25% of thepatients with a final diagnosis of ARVD.
MR and CT Imaging of ARVD 853
Diastolic Dysfunction
Few investigators have used MRI to assess diastolicfunction in ARVD. Auffermann et al (20) were the first touse time-volume curves obtained from cine GRE MRI toassess diastolic function in biopsy-proven ARVD pa-tients. Comparison with control subjects showed thatpatients with ARVD who had arrhythmias induced dur-ing electrophysiologic testing had a significant delay indiastolic relaxation of the RV. The same patients alsohad increased RV volumes and reduced function, sothat diastolic relaxation may not provide additional di-agnostic information. More recently, Kayser et al (35)evaluated diastolic function in 14 patients with ARVDwith preserved systolic function using MR velocity map-
ping of transtricuspid flow. Compared to controls, tri-cuspid flow patterns in ARVD patients showed a signif-icant decrease in peak filling rate and in the slope of thedescending part of the early filling phase. The ratio ofpeak early filling rate to peak atrial contraction andratio of integrated early filling to integrated atrial con-traction (i.e., volume) were significantly lower in pa-tients than in healthy volunteers. These data are con-sistent with studies using echocardiography,suggesting that diastolic abnormalities may precedesystolic dysfunction and may have a role in early diag-nosis.
Role of MRI in Diagnosis of ARVD
The diagnostic role of MRI in ARVD remains somewhatcontroversial. The ability of MRI to characterize fat inthe RV free wall has been brought to question. Thesensitivity and specificity of intramyocardial fat on MRIin ARVD remain to be answered. In our experience, thisfinding alone is neither sensitive nor specific for thediagnosis. Our experience with MRI of autopsy heartsled us to conclude that the achievable spatial resolutionin current state-of-the-art clinical protocols substan-tially limits the capability to detect subtle RV intramyo-cardial fatty changes. Isolated areas of fat replacementare not specific to ARVD and have been reported inelderly patients, patients receiving long-term steroids,and in other cardiomyopathies (36,37). Discrete areasof fat substitutions have also been reported in idio-pathic ventricular tachycardia, which is an importantdifferential diagnosis for ARVD (38–40).
Recently, the reliability of interpreting intramyocar-dial high T1 signals has been brought to question.Bluemke et al (41) reported poor interreader reproduc-ibility for detection of intramyocardial fat signal on con-ventional SE MR images performed on patients evalu-ated for ARVD. The study raises an important issue indefining the role of MRI in ARVD using conventional(i.e., noncardiovascular) MR scanners. The poor agree-ment for identifying intramyocardial fat is not entirelysurprising. The normal presence of epicardial and peri-cardial fat makes identification of true intramyocardialfat difficult. Some areas such as the subtricuspid re-gion are not easily distinguished from the atrioventric-ular sulcus, which is rich in fat (42). The RV free wall isonly 4–5 mm thick, and the spatial resolution is oftenunsatisfactory to reliably comment on wall thickness,let alone fat infiltration (43). To differentiate fatty infil-tration from the normal epicardial fat requires consid-erable expertise, and the diagnostic sensitivity andspecificity of detecting fat on MRI still need to be de-fined. Until these issues are resolved, the presence ofintramyocardial fat on MRI should not be consideredsynonymous with ARVD and the diagnosis should notbe made in the absence of other clinical criteria.
Since the disease is so rare, most imaging centershave little or no experience with diagnosis of ARVD.Technical problems in imaging patients with arrhyth-mias, lack of a standardized protocol for ARVD, andlack of experience by imaging physicians suggest thatMRI should be only one part of a comprehensive eval-uation for these patients. According to the Task Force
Figure 9. A: Axial black-blood image from a patient with RVdysplasia showing intramyocardial hyperintense signals (fatsignal) in the anterior wall (arrows). B: Bright-blood systolicimage at the same level demonstrates an aneurysmal segment(arrow) in the region of the signal abnormality.
854 Tandri et al.

criteria (5), MRI provides information related to RV size,global and regional function, and aneurysm formation.Even using conventional SE imaging, the morphologicfeatures appear to distinguish ARVD patients from nor-mal individuals (41).
MRI, on the other hand, can identify patients requir-ing invasive testing. A completely normal MR study in apatient with no abnormalities on electrocardiography orechocardiography is reassuring, and such patients maynot need invasive testing (angiography/biopsy) in theabsence of other clinical criteria. If signal abnormalitiesand wall motion abnormalities coexist, invasive testingshould be undertaken to confirm the findings. Minorstructural abnormalities, i.e., signal abnormalities inthe absence of wall motion changes, present a challengeas further evaluation of such patients is unclear. Ad-herence to Task Force criteria is recommended, andthese minor criteria may not necessitate invasive test-ing. Further, it must be recognized that ARVD TaskForce criteria do not currently recognize fat signal onMR (or CT) as a diagnostic criterion for the disease.
Future Directions
In spite of the current problems faced by MRI, it isundeniable that MR certainly has enormous potentialin ARVD. If the significant strides that have been madein MR technology over the last 10 years continue, eachof the above-mentioned problems will be systematicallyaddressed and solutions will hopefully emerge.
A current limitation for black-blood imaging as men-tioned above is poor spatial resolution. Increases inspatial resolution results in longer and prohibitivebreath-hold duration, which is often counterproduc-tive. One approach would be the use of navigator echo-gated techniques, which allow free breathing. Thistechnique was initially described by Ehman and Felm-lee (44) in 1989 and is currently used in coronary im-aging. Navigator echoes are positioned over the rightdiaphragm and imaging is triggered for a 4- to 5-mmwindow. In conjunction with three-dimensional black-blood techniques, this approach could improve spatialresolution for detection of intramyocardial fat. Limita-tions to this technique include increased scanningtimes (by a factor of two), increased edge blurring, andsusceptibility to motion artifact due to arrhythmias andin patients with irregular breathing patterns.
Another aspect of ARVD evaluation that needs im-provement is regional function assessment. Visualanalysis is often inadequate due to the complex con-traction pattern of the RV. Myocardial tissue taggingprovides accurate and quantitative data regarding re-gional function and may potentially improve the sensi-tivity of MRI to detect regional dysfunction in ARVD.Fayad et al (45) have previously described this ap-proach in the RV. However, tissue tagging is not easilyapplied due to the very thin RV free wall and resultantpoor signal to noise ratio.
Currently, two large clinical trials in ARVD patientsare under way. The European ARVD registry (46) at-tempts to prospectively validate criteria for clinical di-agnosis of ARVD/cardiomyopathy (ARVD/C), evaluatethe accuracy of clinical diagnosis, and assess the nat-
ural course of the disease. The Multidisciplinary Studyof Right Ventricular Dysplasia (U.S. ARVD study) (47),which aims to prospectively enroll 100 patients withARVD and 500 first-degree relatives, attempts to de-velop quantitative methods to assess RV function toenhance the specificity and sensitivity of the diagnosisof ARVD/C. These studies may define the diagnosticrole of MRI in ARVD as well as in family members.
CT OF ARVD
CT imaging utilizing x-ray technology was developed inthe early 1970s, and ever since has been used exten-sively for its ability to provide cross-sectional images ofthe body (48). There has been a continuous and accel-erated development of CT technology, particularly inthe last 10 years, focused toward cardiac imaging. Thelatest-generation CT scanners, namely, electron beamCT (EBCT) and multidetector CT (MDCT), provide excel-lent spatial resolution and allow accurate high-resolu-tion assessment of morphological detail of both cardiacchambers (49–51). The use of a nonionic contrast agentprovides excellent contrast resolution with clear delin-eation of the ventricular endocardium. Multiple cardiacphases can be extracted, with animated movies of thebeating heart made available for visual assessment ofglobal and regional function (49). Quantitative determi-nations of ventricular mass, right and left ventricularvolumes, and global ventricular function can be per-formed in a variety of cardiac pathologic states (50). Thewidespread availability of MDCT scanners and less de-pendence on technical factors have made CT imagingpopular compared to MRI in cardiovascular evaluation.In addition, CT is fast, easy to perform, and has morereliable image quality. Although images are acquiredonly in the axial plane, the acquisition of a three-dimen-sional data set allows reformatting in any desirableplane. For the above reasons, CT is a clinically valuable,noninvasive tool for assessment of myocardial pathol-ogy.
Similar to MRI, CT imaging also has the capability toprovide tissue characterization of the myocardium. Theability to depict fatty tissue along with cardiac morphol-ogy makes CT imaging an option for evaluation ofARVD. Dery et al (52) were the first to demonstrate adilated hypokinetic RV with a markedly thin anteriorwall and normal left-sided chambers using CT in anelderly patient with ARVD who presented with RV fail-ure. However, the ability of conventional CT to detectintramyocardial fat in ARVD was first reported by Villaet al (53) in a series of seven patients with ARVD, andsubsequently Sotozono et al (54) provided biopsy con-firmation of CT findings. They also demonstrated theability of CT imaging to provide excellent anatomic de-tails of the RV and left ventricle in a patient with ad-vanced ARVD. Since that time, there have been only afew investigators who have used CT to image ARVD,utilizing EBCT and MDCT.
CT Imaging Findings in ARVD
There has been some speculation that CT might besuperior to MRI in ARVD due to factors inherent to the
MR and CT Imaging of ARVD 855
disease process. The arrhythmic nature of the diseaseoften leads to image degradation on MR images, andARVD patients receive defibrillator hardware, whichpresently precludes MRI. Hamada et al (55) imaged fourARVD patients with RV arrhythmias who had abnor-malities on electrocardiography and angiography usingEBCT. With contrast-enhanced volume mode scanning,they were able to demonstrate morphologic abnormal-ities in ARVD: 1) abundant epicardial fat, 2) low atten-uation trabeculations, 3) scalloping of RV free wall, and4) intramyocardial fat deposits. Quantification of ven-tricular volumes was performed on cine mode scan-ning, which showed regional dysfunction and de-pressed global RV function, respectively. Tada et al (56)added 10 more ARVD patients to the above series andcompared EBCT findings to 16 age-matched non-ARVDpatients with RV dilation/dysfunction and 13 controlsubjects. Intramyocardial fat was defined based on tis-sue attenuation values. The attenuation value for epi-cardial adipose tissue is around –65 � 10 Hounsfieldunits (HU), and 5 to –17 HU for intramyocardial fat,which is far less than that of myocardium. Using theabove values, none of the control subjects and no pa-tient without ARVD showed any evidence of intramyo-cardial fat or any other qualitative features of ARVD, asdescribed by Tada et al (56). The frequencies of abun-dant epicardial fat, low-attenuation trabeculae, scal-loping, and intramyocardial fat in this study were 86%,71%, 79%, and 50%, respectively. An important findingof this study was that the abnormal area on EBCTcorresponded to the areas of abnormality on electro-anatomic mapping and was frequently larger than theelectroanatomic maps.
Kimura et al (57) studied 32 ARVD patients usingcontrast-enhanced, nongated, single-row detector heli-cal CT. Similar to the findings of EBCT, they found
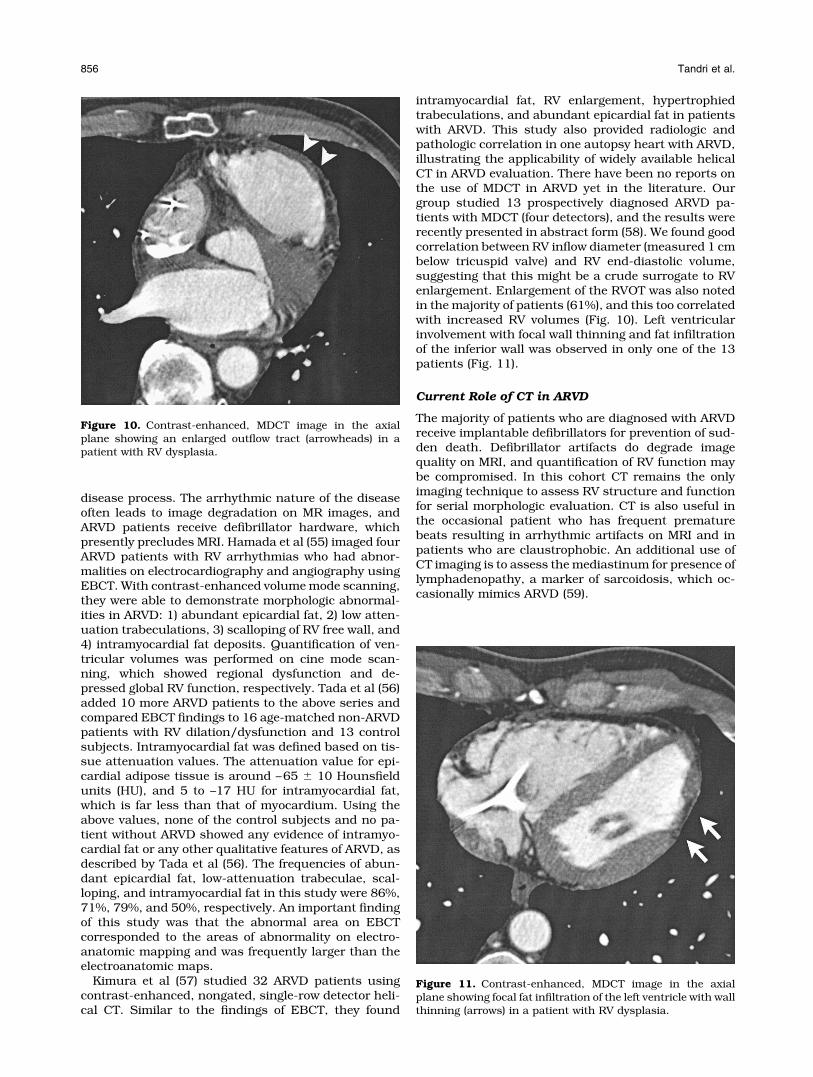
intramyocardial fat, RV enlargement, hypertrophiedtrabeculations, and abundant epicardial fat in patientswith ARVD. This study also provided radiologic andpathologic correlation in one autopsy heart with ARVD,illustrating the applicability of widely available helicalCT in ARVD evaluation. There have been no reports onthe use of MDCT in ARVD yet in the literature. Ourgroup studied 13 prospectively diagnosed ARVD pa-tients with MDCT (four detectors), and the results wererecently presented in abstract form (58). We found goodcorrelation between RV inflow diameter (measured 1 cmbelow tricuspid valve) and RV end-diastolic volume,suggesting that this might be a crude surrogate to RVenlargement. Enlargement of the RVOT was also notedin the majority of patients (61%), and this too correlatedwith increased RV volumes (Fig. 10). Left ventricularinvolvement with focal wall thinning and fat infiltrationof the inferior wall was observed in only one of the 13patients (Fig. 11).
Current Role of CT in ARVD
The majority of patients who are diagnosed with ARVDreceive implantable defibrillators for prevention of sud-den death. Defibrillator artifacts do degrade imagequality on MRI, and quantification of RV function maybe compromised. In this cohort CT remains the onlyimaging technique to assess RV structure and functionfor serial morphologic evaluation. CT is also useful inthe occasional patient who has frequent prematurebeats resulting in arrhythmic artifacts on MRI and inpatients who are claustrophobic. An additional use ofCT imaging is to assess the mediastinum for presence oflymphadenopathy, a marker of sarcoidosis, which oc-casionally mimics ARVD (59).
Figure 10. Contrast-enhanced, MDCT image in the axialplane showing an enlarged outflow tract (arrowheads) in apatient with RV dysplasia.
Figure 11. Contrast-enhanced, MDCT image in the axialplane showing focal fat infiltration of the left ventricle with wallthinning (arrows) in a patient with RV dysplasia.
856 Tandri et al.

Most centers currently rely on MRI instead of CTimaging for evaluating patients with suspected ARVD,mainly because the former is devoid of radiation. MDCTradiation can be quite high, exceeding conventional an-giography by a factor of two when performing retrospec-tive gating (60). Thus, MDCT may not be optional forscreening of ARVD in first-degree relatives. This wouldbe of particular importance especially in young femalesin whom breast radiation should be considered. Cur-rent temporal resolution of CT is of the order of 105msec (at a heart rate of 81 beats/minute), but is stillsuboptimal compared to MRI (61). Despite the abovelimitations, CT does provide certain advantages overMRI in terms of consistency in image quality, scan time,operator dependency, etc. With increase in familiarityof radiologists with the use of helical CT for ARVD andwith the advances in both the temporal and spatialresolution, CT imaging may play an important role bothin the diagnosis and in the follow-up of patients withARVD.
Future Directions
Current multiple-row detector scanners can scan 40-cm-volume lengths in less than 30 seconds with sub-millimeter near-isotropic resolution and excellent im-age quality. Higher spatial resolution may allowaccurate and reproducible evaluation of intramyocar-dial fat and RV wall thickness, thereby increasing thesensitivity in ARVD diagnosis. Increasing gantry speedswill improve temporal resolution approaching that ofMRI. Accurate calculation of radiation dose with cus-tomized adjustment individualized to a patient’s bodyhabitus may increase the utilization of CT in ARVD.Studies comparing MRI and MDCT in ARVD would fur-ther our knowledge of the relative utility of each of thesetechnologies in evaluation of ARVD.
ACKNOWLEDGMENTS
This work was supported in part by National Institutesof Health Research Grant 1 UO1 HL65594-01A1 (to D.Bluemke, PI, MRI ARVD reading center).
REFERENCES
1. Marcus FI, Fontaine GH, Guiraudon G, et al. Right ventriculardysplasia: a report of 24 adult cases. Circulation 1982;65:384–398.
2. Laurent M, Descaves C, Biron Y, et al. Familial form of arrhythmo-genic right ventricular dysplasia. Am Heart J 1987;113:827–829.
3. Corrado D, Thiene G, Nava A, Rossi L, Pennelli N. Sudden death inyoung competitive athletes: clinicopathologic correlations in 22cases. Am J Med 1990;89:588–596.
4. Thiene G, Nava A, Corrado D, Rossi L, Penelli N. Right ventricularcardiomyopathy and sudden death in young people. N Engl J Med1988;318:129–133.
5. McKenna WJ, Thiene G, Nava A, et al. Diagnosis of arrhythmogenicright ventricular dysplasia/cardiomyopathy. Task Force of theWorking Group Myocardial and Pericardial Disease of the Euro-pean Society of Cardiology and of the Scientific Council on Cardio-myopathies of the International Society and Federation of Cardiol-ogy. Br Heart J 1994;71:215–218.
6. Boxt LM. Radiology of the right ventricle. Radiol Clin North Am1999;37:379–400.
7. Foale R, Nihoyannopoulos P, McKenna W, et al. Echocardiographicmeasurement of the normal adult right ventricle. Br Heart J 1986;56:33–44.
8. Pettigrew RI, Oshinski JN, Chatzimavroudis G, Dixon WT. MRItechniques for cardiovascular imaging. J Magn Reson Imaging1999;10:590–601.
9. Higgins CB, editor. Special issue: cardiovascular MRI. J Magn Re-son Imaging 1999;10:589–899.
10. Araoz PA, Mulvagh SL, Tazelaar HD, Julsrud PR, Breen JF. CT andMR imaging of benign primary cardiac neoplasms with echocardio-graphic correlation. Radiographics 2000;20:1303–1319.
11. Becker CR, Ohnesorge BM, Schoepf UJ, Reiser MF. Current devel-opment of cardiac imaging with multidetector-row CT. Eur J Radiol2000;36:97–103.
12. Casolo GC, Poggesi L, Boddi M, Fazi A, Bartolozzi C, Lizzadro G,Dabizzi RP. ECG-gated magnetic resonance imaging in right ven-tricular dysplasia. Am Heart J 1987;113:1245–1248.
13. Klersy C, Raisaro A, Salerno JA, Montemartini C, Campani R.Arrhythmogenic right and left ventricular disease: evaluation bycomputed tomography and nuclear magnetic resonance imaging.Eur Heart J 1989;10(Suppl D):33–36.
14. Bloomer TN, Plein S, Radjenovic A, et al. Cine MRI using steadystate free precession in the radial long axis orientation is a fastaccurate method for obtaining volumetric data of the left ventricle.J Magn Reson Imaging 2001;14:685–692.
15. Simonetti OP, Finn JP, White RD, Laub G, Henry DA. “Black blood”T2-weighted inversion-recovery MR imaging of the heart. Radiology1996;199:49–57.
16. Tandri H, Calkins H, Nasir K, et al. MR imaging findings in patientsmeeting task force criteria for arrhythmogenic right ventriculardysplasia. J Cardiovasc Electrophysiol 2003;14:476–483.
17. Midiri M, Finazzo M, Brancato M, Hoffmann E, Indovina G, MariaMD, Lagalla R. Arrhythmogenic right ventricular dysplasia: MRfeatures. Eur Radiol 1997;7:307–312.
18. Pennell D, Casolo G. Right ventricular arrhythmia: emergence ofmagnetic resonance imaging as an investigative tool. Eur Heart J1997;18:1843–1845.
19. van der Wall EE, Kayser HW, Bootsma MM, de Roos A, Schalij MJ.Arrhythmogenic right ventricular dysplasia: MR imaging findings.Herz 2000;4:356–364.
20. Auffermann W, Wichter T, Breithardt G, Joachimsen K, Peters PE.Arrhythmogenic right ventricular disease: MR imaging vs. angiog-raphy. AJR Am J Roentgenol 1993;161:549–555.
21. Wichter T. Magnetic resonance imaging and 123I-MIBG scintigra-phy in arrhythmogenic right ventricular cardiomyopathy/dyspla-sia. In: First International Symposium on Arrhythmogenic RightVentricular Cardiomyopathy/Dysplasia, Paris, June 16–18, 1996.
22. Ricci C, Longo R, Pagnan L, et al. Magnetic resonance imaging inright ventricular dysplasia. Am J Cardiol 1992;70:1589–1595.
23. Blake LM, Scheinman MM, Higgins CB. MR features of arrhythmo-genic right ventricular dysplasia. AJR Am J Roentgenol 1994;162:809–812.
24. Molinari G, Sardanelli F, Gaita F, et al. Right ventricular dysplasiaas a generalized cardiomyopathy? Findings on magnetic resonanceimaging. Eur Heart J 1995;16:1619–1624.
25. Menghetti L, Basso C, Nava A, Angelini A, Thiene G. Spin-echo nu-clear magnetic resonance for tissue characterisation in arrhythmo-genic right ventricular cardiomyopathy. Heart 1996;76:467–470.
26. van der Wall EE, Kayser HW, Bootsma MM, de Roos A, Schalij MJ.Arrhythmogenic right ventricular dysplasia: MRI findings. Herz2000;25:356–364.
27. Arai AE, Epstein FH, Bove KE, Wolff SD. Visualization of aorticvalve leaflets using black blood MRI. J Magn Reson Imaging 1999;10:771–777.
28. Fayad ZA, Fuster V, Fallon JT, et al. Noninvasive in vivo humancoronary artery lumen and wall imaging using black-blood mag-netic resonance imaging. Circulation 2000;102:506–510.
29. Stuber M, Botnar RM, Kissinger KV, Manning WJ. Free-breathingblack-blood coronary MR angiography: initial results. Radiology2001;219:278–283.
30. Burke AP, Farb A, Tashko G, Virmani R. Arrhythmogenic rightventricular cardiomyopathy and fatty replacement of the right ven-tricular myocardium: are they different diseases? Circulation1998;97:1571–1580.
31. Sakuma H, Fujita N, Foo TK, et al. Evaluation of left ventricularvolume and mass with breath-hold cine MR imaging. Radiology1993;188:377–380.
32. Bloomgarden DC, Fayad ZA, Ferrari VA, et al. Global cardiac func-tion using fast breath-hold MRI: validation of new acquisition andanalysis techniques. Magn Reson Med 1997;37:683–692.
MR and CT Imaging of ARVD 857

33. Pereles FS, Kapoor V, Carr JC, et al. Usefulness of segmentedtrueFISP cardiac pulse sequence in evaluation of congenital andacquired adult cardiac abnormalities. AJR Am J Roentgenol 2001;177:1155–1160.
34. Candinas R, Duru F. Unusual clinical presentation of a patientwith an extreme form of right ventricular dysplasia. Circulation2001;104:848–849.
35. Kayser HW, de Roos A, Schalij MJ, Bootsma M, Wellens HJ, Vander Wall EE. Usefulness of magnetic resonance imaging in diagno-sis of arrhythmogenic right ventricular dysplasia and agreementwith electrocardiographic criteria. Am J Cardiol 2003;91:365–367.
36. Vikhert AM, Tsiplenkova VG, Cherpachenko NM. Alcoholic cardio-myopathy and sudden cardiac death. J Am Coll Cardiol 1986;8(Suppl A):3A–11A.
37. Hasumi M, Sekiguchi M, Hiroe M, Kasanuki H, Hirosawa K. Endo-myocardial biopsy approach to patients with ventricular tachycar-dia with special reference to arrhythmogenic right ventricular dys-plasia. Jpn Circ J 1987;51:242–249.
38. White RD, Trohman RG, Flamm SD, et al. Right ventricular ar-rhythmia in the absence of arrhythmogenic dysplasia: MR imagingof myocardial abnormalities. Radiology 1998;207:743–751.
39. Proclemer A, Basadonna PT, Slavich GA, Miani D, Fresco C, FiorettiPM. Cardiac magnetic resonance imaging findings in patients withright ventricular outflow tract premature contractions. Eur Heart J1997;18:2002–2010.
40. Globits S, Kreiner G, Frank H, Heinz G, Klaar U, Frey B, GossingerH. Significance of morphological abnormalities detected by MRI inpatients undergoing successful ablation of right ventricular outflowtract tachycardia. Circulation 1997;96:2633–2640.
41. Bluemke D, Krupinski EA, Ovitt T, et al. MR imaging in arrhyth-mogenic right ventricular cardiomyopathy: morphologic findingsand interobserver reliability. Cardiology 2003;99:153–162.
42. Pennell D. Cardiovascular magnetic resonance. Heart 2001;85:581–589.
43. Corrado D, Basso C, Thiene G. Arrhythmogenic right ventricularcardiomyopathy: diagnosis, prognosis, and treatment. Heart 2000;83:588–595.
44. Ehman RL, Felmlee JP. Adaptive technique for high-definition MRimaging of moving structures. Radiology 1989;173:255–263.
45. Fayad ZA, Ferrari VA, Kraitchman DL, et al. Right ventricularregional function using MR tagging: normal versus chronic pulmo-nary hypertension. Magn Reson Med 1996;35:771–780.
46. Corrado C, Fontaine G, Marcus FI, et al., for the Study Group onArrhythmogenic Right Ventricular Dysplasia/Cardiomyopathy. Ar-rhythmogenic right ventricular dysplasia/cardiomyopathy need foran international registry. Circulation 2000;101:E101–E106.
47. Marcus FI, Towbin JA, Zareba W, et al., for the ARVD/C Investiga-tors. Arrhythmogenic right ventricular dysplasia/cardiomyopathy(ARVD/C). A multidisciplinary study: design and protocol. Circu-lation 2003;107:2975–2978.
48. Hounsfield GN. Computerized transverse axial scanning (tomogra-phy). 1. Description of system. Br J Radiol 1973;46:1016–1022.
49. Berry E, Kelly S, Hutton J, Harris KM, et al. A systematic literaturereview of spiral and electron beam tomography: with particularreference to clinical application in hepatic lesions, pulmonary em-bolus and coronary artery disease. Health Technol Assess 1999;3:1–118.
50. Stanford W, Galvin JR, Weiss RM, et al. Ultrafast computed tomog-raphy in cardiac imaging: a review. In: Seminars in Ultrasound, CTand MR, 1991. p 45–60.
51. Becker CR, Ohnesorge BM, Schoepf UJ, Reiser MF. Current devel-opment of cardiac imaging with multidetector-row CT. Eur J Radiol2000;36:97–103.
52. Dery R, Lipton MJ, Garrett JS, Abbott J, Higgins CB, SchienmanMM. Cine-computed tomography of arrhythmogenic right ventric-ular dysplasia. J Comput Assist Tomogr 1986;10:120–123.
53. Villa A, Di Guglielmo L, Salerno J, Klercy C, Kluzer A, Codega S.Arrhythmogenic dysplasia of the right ventricle. Evaluation of 7cases using computerized tomography. Radiol Med (Torino) 1988;75:28–35.
54. Sotozono K, Imahara S, Masuda H, et al. Detection of fatty tissue inthe myocardium by using computerized tomography in a patientwith arrhythmogenic right ventricular dysplasia. Heart VesselsSuppl 1990;5:59–61.
55. Hamada S, Takamiya M, Ohe T, Ueda H. Arrhythmogenic rightventricular dysplasia: evaluation with electron-beam CT. Radiology1993;187:723–727.
56. Tada H, Shimizu W, Ohe T, et al. Usefulness of electron-beamcomputed tomography in arrhythmogenic right ventricular dyspla-sia. Circulation 1996;94:437–444.
57. Kimura F, Sakai F, Sakomura Y, et al. Helical CT features of ar-rhythmogenic right ventricular cardiomyopathy. Radiographics2002;22:1111–1124.
58. Bomma C, Tandri H, Nasir K, et al. Role of helical CT in qualitativeand quantitative evaluation of arrhythmogenic right ventriculardysplasia. Pacing Clin Electrophysiol 2003;26(Suppl 1):965.
59. Shiraishi J, Tatsumi T, Shimoo K, et al. Cardiac sarcoidosis mim-icking right ventricular dysplasia. Circ J 2003;67:169–171.
60. Hunold P, Vogt FM, Schmermund A, et al. Radiation exposureduring cardiac CT: effective doses at multi-detector row CT andelectron-beam CT. Radiology 2003;226:145–152.
61. Flohr TG, Schoepf UJ, Kuettner A, et al. Advances in cardiac im-aging with 16-section CT systems. Acad Radiol 2003;10:386–401.
858 Tandri et al.




























