Embed Size (px)
Citation preview

Magnetic Resonance Colonography IncludingDiffusion-Weighted Imaging in Children andAdolescents With Inflammatory Bowel Disease
Do We Really Need Intravenous Contrast?
Selma Sirin, MD,* Simone Kathemann, MD,Þ Bernd Schweiger, MD,* Maria L. Hahnemann, MD,*Michael Forsting, MD,* Thomas C. Lauenstein, MD,* and Sonja Kinner, MD*
Objectives: Magnetic resonance colonography (MRC) is a well-accepted,noninvasive imaging modality for the depiction of inflammatory bowel dis-ease. Diffusion-weighted imaging (DWI) is very helpful to display inflam-matory lesions. The aim of this retrospective study was to assess whetherintravenous contrast is needed to depict inflammatory lesions in bowel mag-netic resonance imaging if DWI is available.Materials and Methods: Thirty-seven patients (23 females, 14 males; meanage, 14.6 years) underwent MRC on a 1.5-T scanner (MAGNETOM Avanto;Siemens). Contrast-enhanced T1-weighted (ce-T1-w) sequences and DWIsequences in axial and coronal planes (b = 50, 500, 1000) were acquired. Tworeviewers evaluated (1) DWI, (2) ce-T1-w MRC, as well as (3) DWI andce-T1-w MRC concerning lesion conspicuity. The preferred b value wasassessed. Colonoscopy was performed within 1 week, including biopsiesserving as the reference standard. Sensitivities and specificities were calcu-lated, and interobserver variability was assessed.Results: Mean sensitivity and specificity of the 2 readers for the depiction ofinflammatory lesions were 78.4%/100% using ce-T1-w MRC, 95.2%/100%using DWI, and 93.5%/100% combining both imaging techniques comparedwith colonoscopy including results of the histopathological samples. In 6 pa-tients, inflammatory lesions were only detected by DWI; in another 6 patients,DWI detected additional lesions. The J values for the 2 readers were excellent(k = 0.92Y0.96). The preferred b value with the best detectability of the lesionwas b1000 in 28 of the 30 patients (93.3%) with restricted diffusion.Conclusions: Diffusion-weighted imaging of the bowel identified inflamma-tory lesions with high accuracy and revealed lesions that were not detectable withce-T1-w imaging alone. A b value of 1000 showed the best lesion detectability.
Key Words: diffusion-weighted imaging, inflammatory bowel disease, MRI,MR colonography, colonoscopy
(Invest Radiol 2015;50: 32Y39)
T he reliable detection of inflammatory lesions is the basis for anoptimal patient management in pediatric patients with inflam-
matory bowel disease (IBD). Cross-sectional imaging including com-puted tomography and magnetic resonance imaging (MRI) all playimportant roles in the detection of these lesions. However, severalreports advise against the routine use of computed tomographicenterography for the detection of inflammatory lesions because of the
risk for ionizing radiation.1,2 Therefore, MRI of the small and largebowel (magnetic resonance [MR] enterography and colonography)should be the first-line imaging techniques in the assessment of pa-tients with IBD because of the high diagnostic accuracy and the lackof ionizing radiation, which is especially desirable in pediatricpatients.3Y5 In addition, some studies have demonstrated that thetherapeutic strategy often changed because of the results of MRI inpatients with IBD.6,7 However, MRI of the bowel, by now, necessi-tates the administration of an intravenous contrast agent. Especiallysince the detection of nephrogenic systemic fibrosis, a rare but se-rious complication of gadolinium-based contrast agents, there is lesswillingness to use intravenous contrast agents in MRI,8 mainly inpatients with a high probability of renal insufficiency that occasion-ally occurs in patients with IBD.9
Diffusion-weighted imaging (DWI) is an emerging MR tech-nique that allows the visualization of thermally induced motion of watermolecules. Initially, it has been used in cerebral MRI,10,11 but in recentyears, DWI has also been applied to the whole body, including the ab-domen.12,13 Several studies show the potential of DWI for tumor de-tection and staging.14Y16 Furthermore, DWI has been proven useful forthe evaluation of inflammation and infections.17,18 Initial studies usingDWI in adult and pediatric patients with IBD such as Crohn’s disease andulcerative colitis revealed a high diagnostic accuracy regarding the de-tection of inflammatory lesions.17,19Y21 To our knowledge, only 2 veryrecent studies comparing the diagnostic accuracy of DWI and conven-tional bowel MRI using a gadolinium-based contrast agent exist.17,22
However, colonoscopy as the criterion standard for the detection ofinflammatory bowel lesions was only available in two thirds of the pa-tients in the first study and not included in the second study. In addition,these studies focus on the evaluation of patients with a confirmed di-agnosis of Crohn’s disease, whereas studies for patients with ulcerativecolitis and patients suspected as having IBD are missing.
The aims of this retrospective study were the following: (1) toassess the diagnostic accuracy of (a) DWI, (b) conventional MRcolonography using a gadolinium-based contrast agent, and (c) thecombined data set using colonoscopy as the reference standard and(2) to compare the results of the 3 MR data sets to assess whether acontrast agent is indeed essential for the reliable diagnosis of in-flammatory lesions in children and adolescents with IBD.
MATERIALS AND METHODS
PatientsThirty-seven consecutive patients (23 females, 14 males) with
a mean (SD) age of 14.6 (3.0) years (range, 7.2Y21.0 years) wereenrolled. All patients were referred from the pediatric gastroentero-logical outpatient clinic for an MRI of the bowel because ofsuspected (n = 21) or confirmed IBD (n = 16). Thirteen of the16 patients with known IBD had Crohn’s disease, and 3 patients hadproven ulcerative colitis.
ORIGINAL ARTICLE
32 www.investigativeradiology.com Investigative Radiology & Volume 50, Number 1, January 2015
Received for publication May 5, 2014; and accepted for publication, after revision,July 25, 2014.
From the *Department of Diagnostic and Interventional Radiology and Neurora-diology, and †Clinic for Pediatrics II, University Hospital Essen, University ofDuisburg-Essen, Essen, Germany.
Conflicts of interest and sources of funding: none declared.Reprints: Selma Sirin, MD, Department of Diagnostic and Interventional Radiology
and Neuroradiology, University Hospital Essen, University of Duisburg-Essen,Hufelandstrasse 55, 45147 Essen, Germany. E-mail: [email protected].
Copyright * 2014 by Lippincott Williams & WilkinsISSN: 0020-9996/15/5001Y0032
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

Patient Preparation and MRIMagnetic resonance imaging was performed on a 1.5-T MR
system (MAGNETOMAvanto; Siemens Healthcare Sector, Erlangen,Germany) with 2 torso phased-array surface coils for coverage of theentire abdomen for signal reception. The patients were placed in proneposition to reduce artifacts due to bowel or respiratory movement.23
Bowel cleansing was perfomed in all patients starting 1 day before theexamination (Golytely; Braintree Laboratories). On the day of theexamination, the patients started to drink a solution containing man-nitol and locust bean gum (the aim was 1500 mL, but according toability and disease severity) 45 minutes before the MR examination.24
A rectal enema was not performed, but the oral contrast agenthad already passed the small bowel, leading to sufficient distensionof the large bowel. All patients received scopolamine (Buscopan,Boehringer Ingelheim, Germany), adapted to body weight, to reducemotion artifacts and to increase bowel distention.25 No general anes-thesia or sedation was necessary for imaging.
A dose of 0.1-mmol/kg body weight gadobutrol (Gadovist;Bayer Health Care, Berlin, Germany) was injected intravenously.T1-weighted turbo spin echo sequences in axial and coronal planeswere performed in the equilibrium phase (starting 3 minutes aftercontrast administration; repetition time, 190 milliseconds; echo time,1.84 milliseconds; flip angle, 70 degrees; field of view, 400 mm; slicethickness, 5 mm; gap, 0.5 mm; matrix size, 230 � 256; time of acqui-sition, 16 seconds). Afterward, DWI sequences in the axial and coronalplanes were collected (b = 50, 500, 1000 s/mm2). The DWI sequencewas a 2-dimensional nonYbreath-hold sequence without navigator orgating (slice thickness, 7 mm; acquired slices [coronal/axial], 60/30;repetition time [coronal/axial], 5600/10100 milliseconds; echo time,76 milliseconds; bandwidth, 2004 Hz per pixel; time of acquisition[coronal/axial], 2 minutes 48 seconds/5 minutes 3 seconds; field of view,343 � 440 mm; voxel sizes, 2.3 � 2.3 � 7 mm3; echo planar imagingfactor, 150) and was acquired with a parallel imaging accelerator factorof 2 (syngo generalized autocalibrating partially parallel acquisition),and 3 averages were used for DWI. Corresponding apparent diffusioncoefficient (ADC) maps were calculated.
ColonoscopyAll patients underwent conventional colonoscopy within 1 week
after bowelMRI. All procedures were performed by or under supervisionof a pediatric gastroenterologist using standard equipment (CF-HQ190Lor CF-H180DI; Olympus Medical Systems, Tokyo, Japan).
Sedatives (2Y3 mg of midazolam hydrochloride, Dormicum;Roche, Germany) and analgesics (25Y50 mg of pethidin, Dolantin;Hoechst, Germany) as well as 40- to 280-mg propofol (Disoprovan;AstraZeneca, Wedel, Germany) were routinely administered. Targetedand step biopsies were performed, which were subsequently analyzedthrough histopathology.
Evaluation of histopathological samples was performed accordingto the recent guidelines of Crohn’s disease and ulcerative colitis.26,27
Data AnalysisTwo radiologists (9 and 4 years’ experience in abdominal im-
aging) analyzed the 3 data sets separately on a dedicated postprocessingworkstation (syngo; Siemens Healthcare, Erlangen, Germany). To re-duce any bias, the radiologists were blinded to clinical and laboratorydata of the patients and data sets were reviewed in random order with atime interval between 3 and 5 weeks between readout.
The 2 reviewers evaluated (1) DWI, (2) contrast-enhancedT1-weighted MRC (ce-T1-w MRC), as well as (3) a combined dataset including DWI and ce-T1-w MRC concerning determinable lesionsof the terminal ileum and colon (1, none; 2, 1/continuous lesion(s); 3,multiple, discontinuous lesions). Furthermore, bowel distension(1, good; 2, moderate; 3, poor distension), b values, in which the lesion(s)
is/are visible (1 = 50, 2 = 500, 3 = 1000, 4 = 50/500, 5 = 50/1000,6 = 500/1000, 7 = 50/500/1000), and the preferred b value (50, 500,1000) were assessed and correlated. For DWI, all b values and the ADCmaps were used: an increased signal in the DWI images, together with asignal loss in the ADC maps, was rated as positive for a lesion. Colo-noscopy and biopsy probes served as the reference standards.
Statistical calculations were performed using the StatisticalPackage for the Social Sciences Software Package (SPSS Statistics,version 19.0; SPSS Inc, Chicago, IL). Sensitivities, specificities, as wellas positive and negative predictive values (PPVs, NPVs) for the presenceof lesions were calculated for all 3 data sets and compared with colo-noscopy alone and with the combination of colonoscopy and the resultsof the biopsy probes. The assessment results of the DWI and ce-T1-wMRCdata sets were compared using the W2 test for each reader. In addition,sensitivity, specificity, and accuracy of the different data sets (referencestandard: the combination of colonoscopy and the results of the histo-pathological samples) were compared using the Fisher exact test.
Interrater variability was evaluated using the J coefficient. AJ values less than 0.2 indicated poor agreement; 0.21 to 0.4, fairagreement; and 0.41 to 0.6, moderate agreement. The J values of0.61 to 0.8 showed good agreement and values from 0.81 to 1 indi-cated an excellent interobserver agreement.
Ethical ConsiderationsThis retrospective study was performed in accordance with the
regulations of the local ethics committee. Informed written consentwas obtained from all patients before the examination.
RESULTSMagnetic resonance images and colonoscopies of the 37 pa-
tients were performed without any adverse effects, technical failure,or withdrawal. No data set had to be excluded because of artifacts orother reasons. Oral contrast was well tolerated by the patients, and theaverage intake was approximately 1000 mL because of the patients’limited ability caused by illness and incompliance to drink 1500 mL.Bowel distension was rated ‘‘good’’ in 11 (29.7%), ‘‘moderate’’ in 17(45.9%), and ‘‘poor’’ in 9 (24.3%) patients.
ColonoscopyInflammatory lesions were detected in 29 of the 37 patients
using colonoscopy. One/continuous lesion(s) were detected in 17 ofthese 29 patients; multiple discontinuous lesions, in the remaining12 patients. All these lesions were confirmed through histopathology.
In 8 of the 37 patients, colonoscopy did not detect pathologicalfindings. However, in 2 of these 8 patients, inflammation was detectedin the histopathological samples taken during the colonoscopy.
Detection of Inflammatory Lesions Usingce-T1-w MRC
In the ce-T1-w MRC data set, both readers agreed in theassessment of 35 of the 37 patients regarding inflammatory lesions(J = 0.92): they identified no lesions in 13, 1/continuous lesion(s) in 15(Fig. 1), and multiple discontinuous lesions in 7 patients. Mean sensi-tivity was 77.6% (reader 1, 75.9%; reader 2, 79.3%) for the detection oflesions in the ce-T1-w MRC data set compared with colonoscopy, witha specificity of 87.5% for each reader. Including the results of the his-topathological probes taken during the colonoscopy, sensitivity andspecificity increased for both readers (mean sensitivity, 78.4% [reader1, 76.7%; reader 2, 80.0%]; specificity, 100% for both readers; Table 1).The readers disagreed in 2 patients. In 1 of these 2 patients, the firstreader rated for multiple, discontinuous lesions, whereas the secondreader identified only 1 lesion. Diffusion-weighted imaging and colo-noscopy revealed multiple lesions in this patient. In the second patient,the first reader rated for no lesion, whereas, in the other reader, DWIand colonoscopy identified 1 lesion.
Investigative Radiology & Volume 50, Number 1, January 2015 DWI in Children With IBD
* 2014 Lippincott Williams & Wilkins www.investigativeradiology.com 33
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

Detection of Inflammatory Lesions Using DWIIn the DWI data set, both readers agreed in the assessment
of 35 of the 37 patients regarding inflammatory lesions (J = 0.92):they identified no lesions in 7, 1/continuous lesion(s) in 16 (Fig. 1),and multiple, discontinuous lesions in 12 patients. The meansensitivity for the detection of pathological lesions using the DWIdata set was 94.9% (reader 1, 93.1%; reader 2, 96.6%); specificitywas 75.0% for each reader. Including the results of the histopatho-logical samples during the colonoscopy, sensitivity and specificityalso increased for both readers (mean sensitivity, 95.2% [reader 1,93.5%; reader 2, 96.8%]; specificity was 100% for both readers;Table 1). In 1 of the 2 patients with discordant assessment, reader 2suspected additional lesion(s) in 1 patient (discontinuous lesions in-stead of 1/continuous lesion(s)), which was affirmed neither byreader 1 nor by colonoscopy. In the second patient, reader 2suspected 1/continuous lesion(s), which was confirmed by colonos-copy (ce-T1-w MRC: both readers, ‘‘no lesions’’; DWI: first reader,‘‘no lesion’’; second reader, ‘‘1/continuous lesion(s)’’; combinedDWI and ce-T1-w MRC: both readers, ‘‘no lesions’’; colonoscopy:pancolitis; Fig. 2).
Detection of Inflammatory Lesions Using DWICompared With ce-T1-w MRC
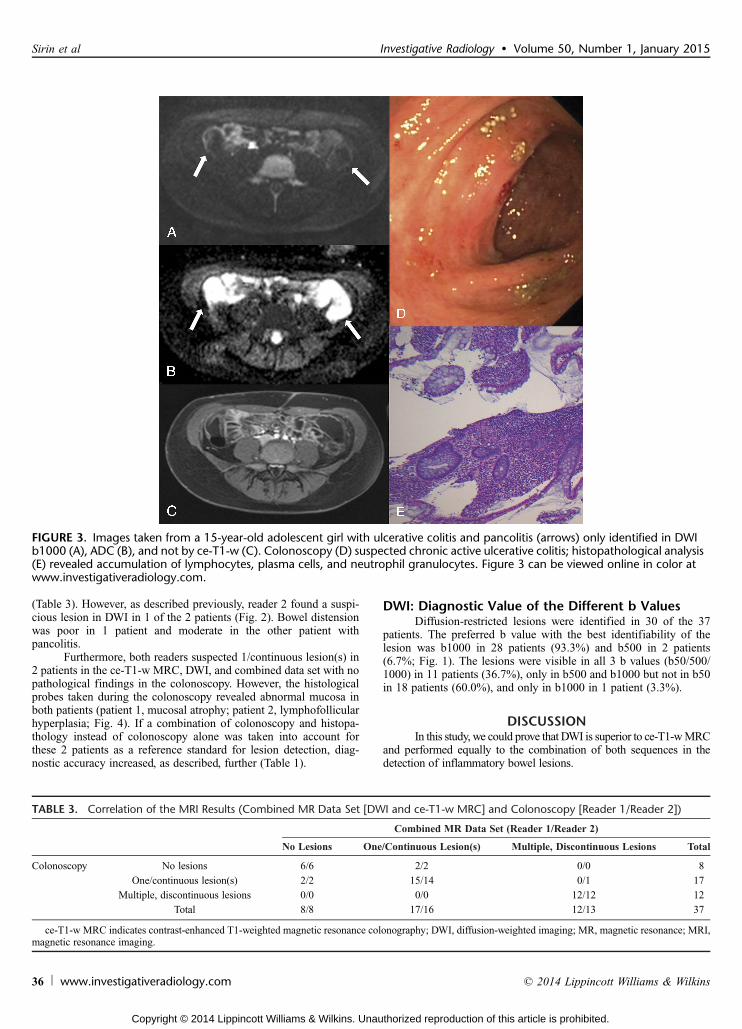
In 6 of the patients (2 patients with suspected IBD, 2 patientswith Crohn’s disease, and 2 patients with ulcerative colitis) withnonambiguous lesions identified in DWI, no inflammatory lesionwas suspected in ce-T1-w MRC (Table 2). Colonoscopy confirmedthe suspected inflammatory lesions in 5 of the 6 patients (Fig. 3). Inthe remaining patient, colonoscopy was unspecific. However, thehistological samples collected during the colonoscopy revealed amucosal atrophy in the suspected area in DWI. Furthermore, additionallesions were identified in DWI in 6 other patients (DWI: multiple, dis-continuous lesions; ce-T1-w MRC, 1/continuous lesion(s)). All theseadditional lesions were confirmed through colonoscopy. The differentresults of the DWI data set and ce-T1-w MRC were statistically signif-icant for each reader using the W2 test (P G 0.001). No statistically sig-nificant differences were detected for sensitivity (P = 0.05 for reader 2,P = 0.08 for reader 1), accuracy (P = 0.06 for reader 2, P = 0.08 forreader 1), and specificity (P 9 0.99 for both readers) using the combi-nation of colonoscopy and the results of the histopathological samples asa reference standard (the Fisher exact test; Table 1).
FIGURE 1. Images taken from a 15-year-old adolescent girl with known Crohn’s disease showing inflammatory changes at theterminal ileum (arrows). Both the readers correctly identified the lesion in b500 (B) and b1000 (C); corresponding ADC is shown inD, in ce-T1-w (E), and in the combined data set. The inflammatory changes were not identified in b50 (A).
TABLE 1. Mean Accuracy, Sensitivity, Specificity, PPV, and NPV for the Presence of Lesions in the 3 MR Data Sets Compared WithColonoscopy Alone and the Combination of Colonoscopy and Histopathological Results
Reference Standard Accuracy Sensitivity Specificity PPV NPV
ce-T1-w MRC Colonoscopy 79.8 77.6 87.5 95.8 51.9
Colonoscopy + histology 82.5 78.4 100 100 51.9
DWI Colonoscopy 90.6 94.9 75.0 93.2 80.4
Colonoscopy + histology 96.0 95.2 100 100 80.4
Combined data set Colonoscopy 89.2 93.1 75.0 93.1 75.0
Colonoscopy + histology 94.6 93.5 100 100 75.0
ce-T1-w MRC indicates contrast-enhanced T1-weighted magnetic resonance colonography; DWI, diffusion-weighted imaging; MR, magnetic resonance; NPV,negative predictive value; PPV, positive predictive value.
Sirin et al Investigative Radiology & Volume 50, Number 1, January 2015
34 www.investigativeradiology.com * 2014 Lippincott Williams & Wilkins
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

In the ce-T1-w MRC data set, 72.3% (for reader 1) and 81.8%(for reader 2) of the sets with good bowel distension were ratedcorrectly, 94.1% (both reader) in the children with moderate boweldistension and only 55.6% (both readers) in children with poor dis-tension. In the DWI data set, 100% of the children with good boweldistension were rated correctly (both readers), 94.1% (reader 1) /100% (reader 2) in the children with moderate bowel distension and88.9% (both readers) in children with poor bowel distension.
Detection of Inflammatory Lesions Using theCombined Data Set
In the combined data set (DWI and ce-T1-w MRC), the readersagreed in the assessment of 36 of the 37 patients with regard to in-flammatory lesions (J = 0.96). Except for 1 patient (the second patient
with nonconcordant assessment described in the DWI data set), allevaluations were exactly similar to the ones for the DWI data set.Comparedwith colonoscopy as the criterion standard, reader 1 correctlyidentified 33 and reader 2 correctly identified 32 of the 37 patients inthe combined MR data set (Table 3). This results in a sensitivity of93.1% and a specificity of 75.0% for each reader. Including the resultsof the histopathological probes during the colonoscopy, sensitivity andspecificity also increased for both readers (sensitivity/ specificity forboth readers, 93.5%/100%; Table 1). No statistically different resultswere detected between DWI, ce-T1w MRI, and the combination of the2 in terms of sensitivity, specificity, and accuracy.
Noncorresponding Findings of MRI and ColonoscopyBoth readers independently did not suspect pathological le-
sions in 2 patients with pancolitis confirmed through colonoscopy
TABLE 2. Correlation of Contrast-Enhanced T1-Weighted MR Colonography and DWI Results (Reader 1/Reader 2)
Contrast-Enhanced T1-Weighted MR Colonography
No Lesions One/Continuous Lesion(s) Multiple, Discontinuous Lesions Total
DWI No lesions 8/7 0/0 0/0 8/7
One/continuous lesion(s) 6/6 11/11 0/0 17/17
Multiple, discontinuous lesions 0/0 4/6 8/7 12/13
Total 14/13 15/17 8/7 37
DWI indicates diffusion-weighted imaging; MR, magnetic resonance.
FIGURE 2. Images taken froma 17-year-old adolescent girl with knownulcerative colitis and inflammatory changes in thewhole colon(arrows) only detected inDWI b1000 (A) andADC (B) by1 reader,whereas the other reader inDWI andboth readers in ce-T1-w (C) andthe combineddata set did not suspect inflammatory changes. Colonoscopy (D) confirmed ulcerative pancolitis, andhistopathology (E)revealed a diffuse increase in lymphocytes, plasma cells, and neutrophil granulocytes. Figure 2 can be viewed online in color atwww.investigativeradiology.com.
Investigative Radiology & Volume 50, Number 1, January 2015 DWI in Children With IBD
* 2014 Lippincott Williams & Wilkins www.investigativeradiology.com 35
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
(Table 3). However, as described previously, reader 2 found a suspi-cious lesion in DWI in 1 of the 2 patients (Fig. 2). Bowel distensionwas poor in 1 patient and moderate in the other patient withpancolitis.
Furthermore, both readers suspected 1/continuous lesion(s) in2 patients in the ce-T1-w MRC, DWI, and combined data set with nopathological findings in the colonoscopy. However, the histologicalprobes taken during the colonoscopy revealed abnormal mucosa inboth patients (patient 1, mucosal atrophy; patient 2, lymphofollicularhyperplasia; Fig. 4). If a combination of colonoscopy and histopa-thology instead of colonoscopy alone was taken into account forthese 2 patients as a reference standard for lesion detection, diag-nostic accuracy increased, as described, further (Table 1).
DWI: Diagnostic Value of the Different b ValuesDiffusion-restricted lesions were identified in 30 of the 37
patients. The preferred b value with the best identifiability of thelesion was b1000 in 28 patients (93.3%) and b500 in 2 patients(6.7%; Fig. 1). The lesions were visible in all 3 b values (b50/500/1000) in 11 patients (36.7%), only in b500 and b1000 but not in b50in 18 patients (60.0%), and only in b1000 in 1 patient (3.3%).
DISCUSSIONIn this study, we could prove that DWI is superior to ce-T1-wMRC
and performed equally to the combination of both sequences in thedetection of inflammatory bowel lesions.
FIGURE 3. Images taken from a 15-year-old adolescent girl with ulcerative colitis and pancolitis (arrows) only identified in DWIb1000 (A), ADC (B), and not by ce-T1-w (C). Colonoscopy (D) suspected chronic active ulcerative colitis; histopathological analysis(E) revealed accumulation of lymphocytes, plasma cells, and neutrophil granulocytes. Figure 3 can be viewed online in color atwww.investigativeradiology.com.
TABLE 3. Correlation of the MRI Results (Combined MR Data Set [DWI and ce-T1-w MRC] and Colonoscopy [Reader 1/Reader 2])
Combined MR Data Set (Reader 1/Reader 2)
No Lesions One/Continuous Lesion(s) Multiple, Discontinuous Lesions Total
Colonoscopy No lesions 6/6 2/2 0/0 8
One/continuous lesion(s) 2/2 15/14 0/1 17
Multiple, discontinuous lesions 0/0 0/0 12/12 12
Total 8/8 17/16 12/13 37
ce-T1-w MRC indicates contrast-enhanced T1-weighted magnetic resonance colonography; DWI, diffusion-weighted imaging; MR, magnetic resonance; MRI,magnetic resonance imaging.
Sirin et al Investigative Radiology & Volume 50, Number 1, January 2015
36 www.investigativeradiology.com * 2014 Lippincott Williams & Wilkins
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

Prior studies assessing the detection of inflammatory lesionsin adult and pediatric patients with IBD using ce-T1-w MRC yieldedmoderate to good results.3,28Y30 Gee et al3 achieved a sensitivity of90% and a specificity of 82.6%, whereas Dillmann et al28 describedonly a sensitivity of 66% and a specificity of 90% for the detection ofactive inflammation in pediatric patients with Crohn’s disease. Theseresults are comparable with our findings using ce-T1-w MRC alone(mean sensitivity/specificity of 77.6%/87.5% compared with colo-noscopy and 78.4%/100% compared with colonoscopy including theresults of histopathological samples taken during the colonoscopy).
However, in recent years, DWI has been increasingly used forthe detection of inflammatory lesions in adults and children withIBD.17,19Y21,31,32 In our study, sensitivity and specificity were excel-lent for the detection of inflammatory lesions using DWI (meansensitivity/specificity of 94.9%/75.0% compared with colonoscopyand 95.2%/100% compared with colonoscopy including the results ofhistopathological samples taken during the colonoscopy). Our resultsof DWI were statistically significantly better than those of ce-T1-wMRC for both readers comparing the assessment results of DWIdata set and ce-T1-w MRC for each reader (P G 0.001). Unfortunately,the patient number seems too small to show statistically significantdifferences between the results of DWI and ce-T1-w MRC comparedwith the combination of colonoscopy and the results of the histo-pathological samples as the reference standard regarding sensitivity(P = 0.05 for reader 2, P = 0.08 for reader 1) and accuracy (P = 0.06for reader 2, P = 0.08 for reader 1) with a high tendency toward DWI.Therefore, future studies with higher patient numbers are necessary toconfirm our findings.
However, 6 patients with inflammatory lesions confirmedthrough colonoscopy or histopathology were detected only by DWI andnot by ce-T1-w MRC. Without the performance of colonoscopy, theinflammatory lesions in these children would not have been detectedand therapy would have been either delayed or not performed at all. Inanother 6 patients, additional lesion(s) were detected by DWI only. Ourresults are superior to those of Kiryu et al,19 who achieved a sensitivityof 85.7% and a specificity of 75.7% in the detection of inflammatorylesions in patients with Crohn’s disease using free-breathing DWI.However, in this study, histopathological results after the surgery wereonly available in 14 patients, whereas conventional barium study servedas the criterion standard in the other 17 patients.
To our knowledge, only 2 other studies comparing the resultsof DWI and conventional bowel MR in patients with Crohn’s diseaseexist.17,22 Neubauer et al17 showed that DWI was superior to contrast-enhanced MRI in 27% of the assessed bowel segments in 33 childrenand young adults with Crohn’s disease compared with conventionalimaging. In the second study, Buisson et al22 postulated a comparablediagnostic accuracy for DWI and conventional MRI. However, incontrast to our study, in the first work, colonoscopy was only availablein two thirds of the patients and, in the second study, no colonoscopicresults were included as the reference standard. In addition, bothstudies used only 2 different b values (0 and 800 s/mm2), whereas weused 3 different b values (50, 500, 1000 s/mm2) and evaluated theusefulness of those. The influence of number and parameters of bvalues will be discussed later.
Similar to the patient group of Neubauer et al,17 the false-positive rate of DWI was very low in our study. The less experienced
FIGURE 4. Images taken from an 8-year-old girl with suspected Crohn’s disease and inflammatory changes at the terminal ileum(arrows) with locoregional lymph nodes (arrow heads) identified in DWI b1000 (A), ADC (B), ce-T1-w (C), and the combined dataset, but not colonoscopy (D). The histopathological samples taken during colonoscopy in the terminal ileum revealedlymphofollicular hyperplasia (E). Figure 4 can be viewed online in color at www.investigativeradiology.com.
Investigative Radiology & Volume 50, Number 1, January 2015 DWI in Children With IBD
* 2014 Lippincott Williams & Wilkins www.investigativeradiology.com 37
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

reader suspected an additional lesion in 1 patient (discontinuous lesionsinstead of 1/continuous lesion(s)). However, the more experiencedreader correctly quoted ‘‘1/continuous lesion(s)’’ in this patient. Thisfalse-positive finding might be caused by the lack of experience in theassessment of DWI.
It has been shown that inclusion of DWI in the bowel MRIprotocol improves diagnostic confidence.33 To our knowledge, this isthe first study showing that results of DWI alone are equally good asthose of the combination of DWI and ce-T1-w MRC in patients withIBD. In 1 patient, DWI alone was even superior to the combined dataset. Because of these results, we suggest that the use of contrast isnot essential for the detection of inflammatory lesions in patientswith suspected or confirmed IBD. Using DWI instead of ce-T1-wMRCor the combined data set would decrease acquisition time and theneed for an intravenous access, which is especially desirable inchildren. Especially in children with impaired renal function, MRIshould be performed without contrast because of the increased riskfor nephrogenic systemic fibrosis.8
Despite the excellent agreement between the results of DWI/the combined data set and colonoscopy, we had 4 patients withnonconcordant results. Two patients with pancolitis were missed bythe combined data set by both readers. This may be caused by theuniform presentation of the whole colon, which was mistaken as in-conspicuous or artificial. However, 1 reader noticed a suspiciousfinding in DWI in 1 of these 2 patients. In 2 other patients withsuspected lesions in DWI by both readers and unsuspicious colo-noscopy, the histopathological samples taken during the colonoscopyrevealed abnormal mucosa in the suspected areas. Because of theseresults, we chose to estimate sensitivity and specificity not only forcolonoscopy but also for the results of the combination of colonos-copy and histopathological samples taken during the colonoscopy. Inaddition, we suggest that the results of the histopathological samplesof suspected areas taken during the colonoscopy should always beincluded in future studies comparing DWI and colonoscopy to ex-clude confounding results. We might even be able to tell the clini-cians where to take the biopsy in patients with unsuspiciouscolonoscopy to maintain the diagnosis if MRI is performed beforecolonoscopy, but this possibility has to be assessed in future studies.
Another topic still under discussion is the question of howbowel distension influences overall diagnostic accuracy in ce-T1-w MRCand DWI. In our study group, there were a lot of incorrect results in thechildren with poor bowel distension (55.6% correct results) comparedwith those with moderate (94.1%) and good bowel distension (72.3%[for reader 1]/81.8% [for reader 2]) using ce-T1-w MRC. Therefore,good bowel distension seems to be very important in detectinginflammatory lesions reliably in ce-T1-w MRC. However, most ofthe children were not able to drink 1500 mL of the oral contrast,the average intake instead being approximately1000 mL. Using DWI,the degree of bowel distension had less impact on detection ofinflammatory lesions in our study group. Some investigators postu-lated that DWI even without bowel preparation is a reliable tool todetect inflammatory lesions.19,21 This is an interesting aspect, espe-cially for children, because bowel preparation is a time-consumingprocedure and some patients, especially young children, do not toler-ate it. This would be a further advantage using DWI in childrenwith IBD.
The aim of our study was a qualitative analysis focusing on thedetection, not on the differentiation, of lesions. Therefore, we did notperform ADC value measurements because the intention of this studywas not to assess diffusion restriction as in the previous studiesperformed in IBD to quantify disease activity20 or stage disease se-verity.34 In addition, we chose to assess interrater variability betweenan experienced and a less experienced radiologist to assess whetheror not the level of experience has an influence on lesion detection inDWI. Interrater variability was excellent for ce-T1-w MRC, DWI,
and the combined data set, showing that even less experiencedreaders are able to detect inflammatory lesions with these sequences.
Another important controversial issue in the literature relates tothe number and parameters of the b values in DWI. Although only 2b values (including a low b value, eg, of 0 or 50 s/mm2 and a higherb value of 500Y1000 s/mm2) are necessary, a greater number of b valueswill improve the accuracy of the calculated ADC.35 However, moreb values will result in longer scan times. Prior studies applyingDWI in the gut mostly used 2 b values (0/600 s/mm2 or 0/1000s/mm2),17,20Y22,34,36,37 whereas only a few studies used 3 (0/50/800s/mm2 or 0/500/1000 s/mm2).19,31,32 We used 3 b values to improve theaccuracy of the calculated ADC values and to compare the results of thedifferent b values. In our study, all inflammatory lesions were seen inb1000 and all but 1 in b500. In addition, b1000 was the preferred b valuein most of the patients. Diffusion-weighted imaging using high b valueshas been shown to provide strong background suppression and wastherefore used inmany studies for the detection of lesions throughout thebody.14,38 Nasu et al39 also observed that the occurrence of false-positiveresults decreases with the use of b1000. During our investigation, wenoticed that b1000 provides better suppression of bowel content com-pared with b50 and b500. In b50, it was often proven impossible todifferentiate between diffusion restriction and bowel content. Neverthe-less, b500was preferred in 2 patients; therefore, wewill go on to performDWI with 3 b values.
The limitations of our work should be acknowledged. Majorlimitations arise from the retrospective design of our study, and fur-thermore, we were only able to include 37 patients. However, despitethe small number of patients and the retrospective design, we believethat our findings are of high value as a preliminary study. Further,prospective studies are therefore needed to confirm our results.
In conclusion, DWI of the bowel shows inflammatory lesionswith high accuracy and identified lesions that were not detected withce-T1-w imaging. Therefore, DWI might to be able to replace or,certainly, to complement ce-T1-w MRC. This technique could beused for short examinations during therapy response assessments andshould be evaluated in future trials.
REFERENCES1. Swanson G, Behara R, Braun R, et al. Diagnostic medical radiation in in-
flammatory bowel disease: how to limit risk and maximize benefit. InflammBowel Dis. 2013;37:1686Y1693.
2. Sauer CG, Kugathasan S, Martin DR, et al. Medical radiation exposure inchildren with inflammatory bowel disease estimates high cumulative doses.Inflamm Bowel Dis. 2011;17:2326Y2332.
3. Gee MS, Nimkin K, Hsu M, et al. Prospective evaluation of MR enterographyas the primary imaging modality for pediatric Crohn disease assessment. AJRAm J Roentgenol. 2011;197:224Y231.
4. Litz C, Danielson PD, Wilsey M, et al. Impact of magnetic resonance imagingin management of pediatric Crohn’s disease. Am Surg. 2013;79:672Y675.
5. Friedrich C, Fajfar A, Pawlik M, et al. Magnetic resonance enterography withand without biphasic contrast agent enema compared to conventionalileocolonoscopy in patients with Crohn’s disease. Inflamm Bowel Dis.2012;18:1842Y1848.
6. Hafeez R, Punwani S, Boulos P, et al. Diagnostic and therapeutic impact of MRenterography in Crohn’s disease. Clin Radiol. 2011;66:1148Y1158.
7. Cheriyan DG, Slattery E, McDermott S, et al. Impact of magnetic resonanceenterography in the management of small bowel Crohn’s disease. Eur JGastroenterol Hepatol. 2013;25:550Y555.
8. Zou Z, Zhang HL, Roditi GH, et al. Nephrogenic systemic fibrosis: review of370 biopsy-confirmed cases. JACC Cardiovasc Imaging. 2011;4:1206Y1216.
9. Oikonomou K, Kapsoritakis A, Eleftheriadis T, et al. Renal manifestationsand complications of inflammatory bowel disease. Inflamm Bowel Dis.2011;17:1034Y1045.
10. Kluytmans M, van Everdingen KJ, Kappelle LJ, et al. Prognostic value ofperfusion- and diffusion-weighted MR imaging in first 3 days of stroke.Eur Radiol. 2000;10:1434Y1441.
11. van Everdingen KJ, van der Grond J, Kappelle LJ, et al. Diffusion-weightedmagnetic resonance imaging in acute stroke. Stroke. 1998;29:1783Y1790.
Sirin et al Investigative Radiology & Volume 50, Number 1, January 2015
38 www.investigativeradiology.com * 2014 Lippincott Williams & Wilkins
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

12. Schmid-Tannwald C, Oto A, Reiser MF, et al. Diffusion-weighted MRI of theabdomen: current value in clinical routine. J Magn Reson Imaging. 2013;37:35Y47.
13. Takahara T, Kwee TC, Van Leeuwen MS, et al. Diffusion-weighted magneticresonance imaging of the liver using tracking only navigator echo: feasibilitystudy. Invest Radiol. 2010;45:57Y63.
14. Hosonuma T, Tozaki M, Ichiba N, et al. Clinical usefulness of diffusion-weighted imaging using low and high b-values to detect rectal cancer. MagnReson Med Sci. 2006;5:173Y177.
15. Ohno Y, Koyama H, Onishi Y, et al. Non-small cell lung cancer: whole-bodyMR examination for M-stage assessmentVutility for whole-body diffusion-weighted imaging compared with integrated FDG PET/CT. Radiology.2008;248:643Y654.
16. Kwee TC, van Ufford HM, Beek FJ, et al. Whole-body MRI, includingdiffusion-weighted imaging, for the initial staging of malignant lymphoma:comparison to computed tomography. Invest Radiol. 2009;44:683Y690.
17. Neubauer H, Pabst T, Dick A, et al. Small-bowel MRI in children and youngadults with Crohn disease: retrospective head-to-head comparison of contrast-enhanced and diffusion-weighted MRI. Pediatr Radiol. 2013;43:103Y114.
18. Goyal A, Sharma R, Bhalla AS, et al. Diffusion-weighted MRI in inflammatoryrenal lesions: all that glitters is not RCC! Eur Radiol. 2013;23:272Y279.
19. Kiryu S, Dodanuki K, Takao H, et al. Free-breathing diffusion-weighted im-aging for the assessment of inflammatory activity in Crohn’s disease. J MagnReson Imaging. 2009;29:880Y886.
20. Oto A, Zhu F, Kulkarni K, et al. Evaluation of diffusion-weighted MR imagingfor detection of bowel inflammation in patients with Crohn’s disease. AcadRadiol. 2009;16:597Y603.
21. Oussalah A, Laurent V, Bruot O, et al. Diffusion-weighted magnetic resonancewithout bowel preparation for detecting colonic inflammation in inflammatorybowel disease. Gut. 2010;59:1056Y1065.
22. Buisson A, Joubert A, Montoriol PF, et al. Diffusion-weighted magnetic res-onance imaging for detecting and assessing ileal inflammation in Crohn’sdisease. Aliment Pharmacol Ther. 2013;37:537Y545.
23. Gourtsoyiannis NC, Grammatikakis J, Papamastorakis G, et al. Imaging ofsmall intestinal Crohn’s disease: comparison between MR enteroclysis andconventional enteroclysis. Eur Radiol. 2006;16:1915Y1925.
24. Lauenstein TC, Schneemann H, Vogt FM, et al. Optimization of oral contrastagents for MR imaging of the small bowel. Radiology. 2003;228:279Y283.
25. Patak MA, Froehlich JM, von Weymarn C, et al. Non-invasive distension of thesmall bowel for magnetic-resonance imaging. Lancet. 2001;358:987Y988.
26. Dignass A, Eliakim R, Magro F, et al. Second European evidence-based con-sensus on the diagnosis and management of ulcerative colitis part 1: definitionsand diagnosis. J Crohns Colitis. 2012;6:965Y990.
27. Van Assche G, Dignass A, Panes J, et al. The second European evidence-basedconsensus on the diagnosis and management of Crohn’s disease: definitionsand diagnosis. J Crohns Colitis. 2010;4:7Y27.
28. Dillman JR, Ladino-Torres MF, Adler J, et al. Comparison of MR enterographyand histopathology in the evaluation of pediatric Crohn disease. PediatrRadiol. 2011;41:1552Y1558.
29. Grand DJ, Kampalath V, Harris A, et al. MR enterography correlates highlywith colonoscopy and histology for both distal ileal and colonic Crohn’s dis-ease in 310 patients. Eur J Radiol. 2012;81:e763Ye769.
30. Savoye-Collet C, Roset JB, Koning E, et al. Magnetic resonance colonographyin severe attacks of ulcerative colitis. Eur Radiol. 2012;22:1963Y1971.
31. Kilickesmez O, Atilla S, Soylu A, et al. Diffusion-weighted imaging of therectosigmoid colon: preliminary findings. J Comput Assist Tomogr. 2009;33:863Y866.
32. Kilickesmez O, Soylu A, Yasar N, et al. Is quantitative diffusion-weighted MRIa reliable method in the assessment of the inflammatory activity in ulcerativecolitis? Diagn Interv Radiol. 2010;16:293Y298.
33. Kinner S, Blex S, Maderwald S, et al. Addition of diffusion-weighted imagingcan improve diagnostic confidence in bowel MRI. Clin Radiol. 2013;69:372Y377.
34. Aoyagi T, Shuto K, Okazumi S, et al. Evaluation of ulcerative colitis usingdiffusion-weighted imaging. Hepatogastroenterology. 2010;57:468Y471.
35. Qayyum A. Diffusion-weighted imaging in the abdomen and pelvis: conceptsand applications. Radiographics. 2009;29:1797Y1810.
36. Ichikawa T, Erturk SM, Motosugi U, et al. High-B-value diffusion-weightedMRI in colorectal cancer. AJR Am J Roentgenol. 2006;187:181Y184.
37. Oto A, Kayhan A, Williams JT, et al. Active Crohn’s disease in the small bowel:evaluation by diffusion weighted imaging and quantitative dynamic contrastenhanced MR imaging. J Magn Reson Imaging. 2011;33:615Y624.
38. Takahara T, Imai Y, Yamashita T, et al. Diffusion weighted whole body imagingwith background body signal suppression (DWIBS): technical improvementusing free breathing, STIR and high resolution 3D display. Radiat Med.2004;22:275Y282.
39. Nasu K, Kuroki Y, Kuroki S, et al. Diffusion-weighted single shot echo planarimaging of colorectal cancer using a sensitivity-encoding technique. Jpn J ClinOncol. 2004;34:620Y626.
Investigative Radiology & Volume 50, Number 1, January 2015 DWI in Children With IBD
* 2014 Lippincott Williams & Wilkins www.investigativeradiology.com 39
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.





























