Embed Size (px)
Citation preview
My collaboratorsNeurology: DALE ROBERTS, JORGE OTERO-MILLAN, PREM JAREONSETTASIN
Otolaryngology: BRYAN WARD, JOHN CAREY, CHARLES DELLA SANTINA,
GRACE TAN, MICHAEL SCHUBERT
Magnetic Vestibular Stimulation (MVS): An Update
DalePremBryan
Grace
DSZ Jorge
DSZ
Michael
NO CONFLICTS OF INTEREST
Take home messages about MVS (magneto
vestibular stimulation)
– EVERYBODY (humans, mice, zebra fish) develops nystagmus (or postural
abnormalities) in an MRI machine from the magnetic field itself (no imaging
needed) due to static magneto-hydrodynamic (Lorentz) forces acting on the ion-
carrying endolymph within the inner ear semicircular canals.
– MVS is a simple, safe, comfortable tool to elicit a sustained vestibular imbalance
and study
• The functional anatomy of vestibular stimulation and visual-vestibular
interaction
• Mechanisms of vestibular adaptation as a model of motor learning (“set-
point” or “bias” adaptation)
• Mechanisms of vestibular perception
• Effects of drugs and other therapies, genetic manipulations, development,
etc., on vestibular function
• A potential rehabilitative technique, for balance as well as for higher level
cognitive disorders such as neglect
• BEWARE effects on functional MRI and resting state connectivity
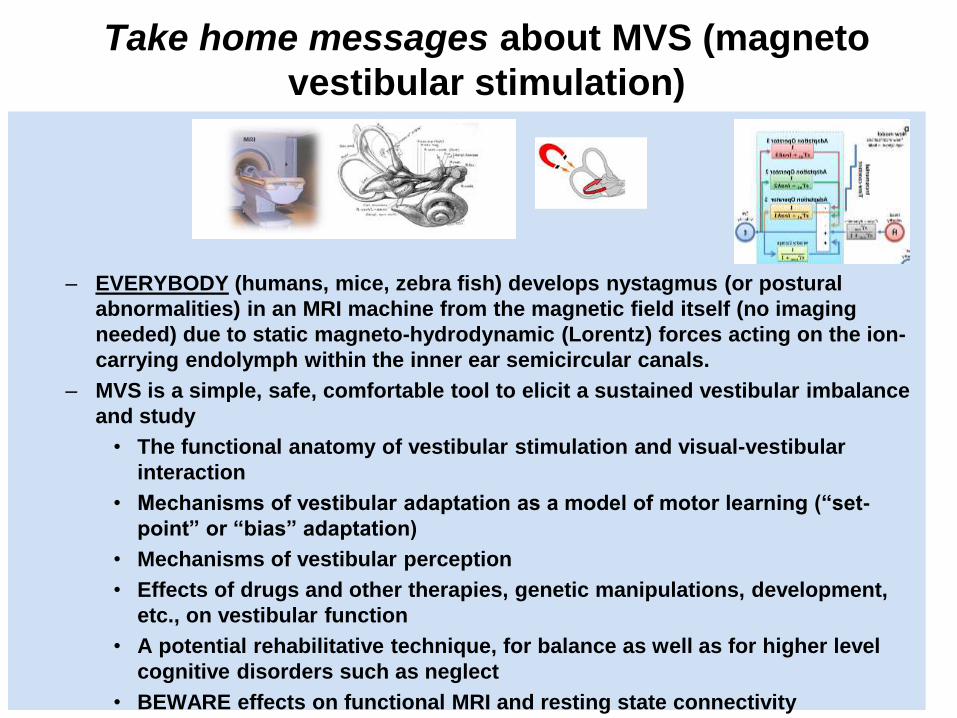
How do we normally sense head
rotation? Fluid flow, cupula
movement, hair cells bending,
neural discharge
1 Canals respond to head acceleration
2. Position of the cupula signals head velocity
3. Constant acceleration needed to keep cupula deviated and hence to produce a constant slow-phase velocity.
Carey, Della Santina

Marcelli, Vincenzo, otolaryngologist
Spatio-temporal pattern of vestibular information processing after
brief caloric stimulation. (1.5T magnet)
European Journal of Radiology 70 (2009) 312–316
“… spontaneous nystagmus (jerking of the eyes induced
by excitation of the labyrinth) preceding the injection (of
water) …
The beginning in 2010 with a
conversation in Siena, Italy
Marcelli speculated this was due to the magnetic field itself!
Il Campo Il Palio
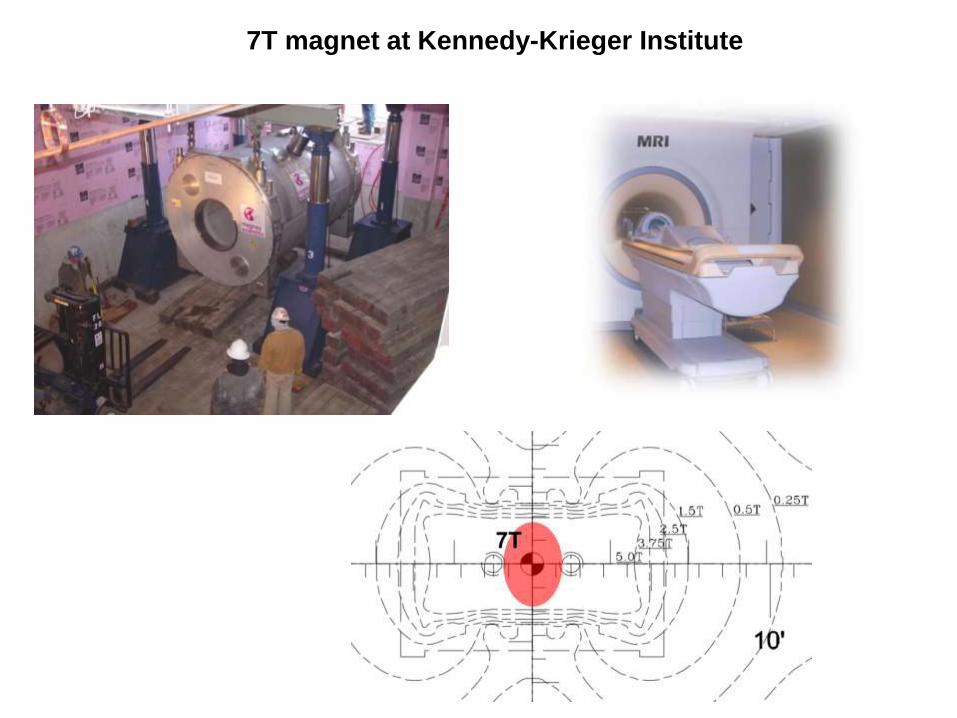
7T magnet at Kennedy-Krieger Institute
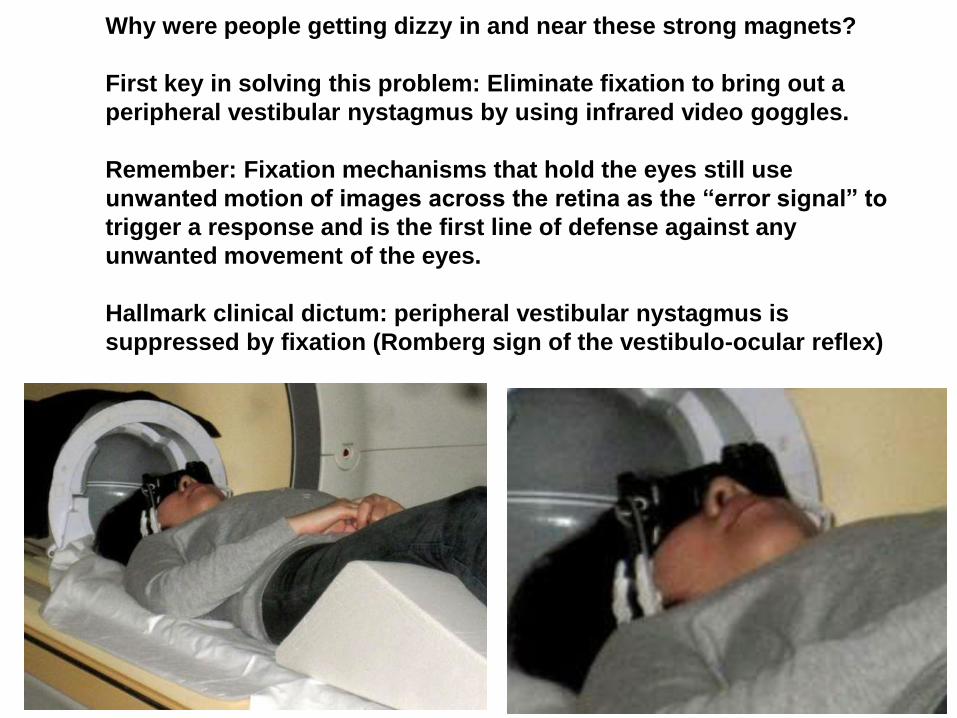
Why were people getting dizzy in and near these strong magnets?
First key in solving this problem: Eliminate fixation to bring out a
peripheral vestibular nystagmus by using infrared video goggles.
Remember: Fixation mechanisms that hold the eyes still use
unwanted motion of images across the retina as the “error signal” to
trigger a response and is the first line of defense against any
unwanted movement of the eyes.
Hallmark clinical dictum: peripheral vestibular nystagmus is
suppressed by fixation (Romberg sign of the vestibulo-ocular reflex)
Nystagmus induced by exposure to a magnetic field
(magneto-vestibular stimulation (MVS))
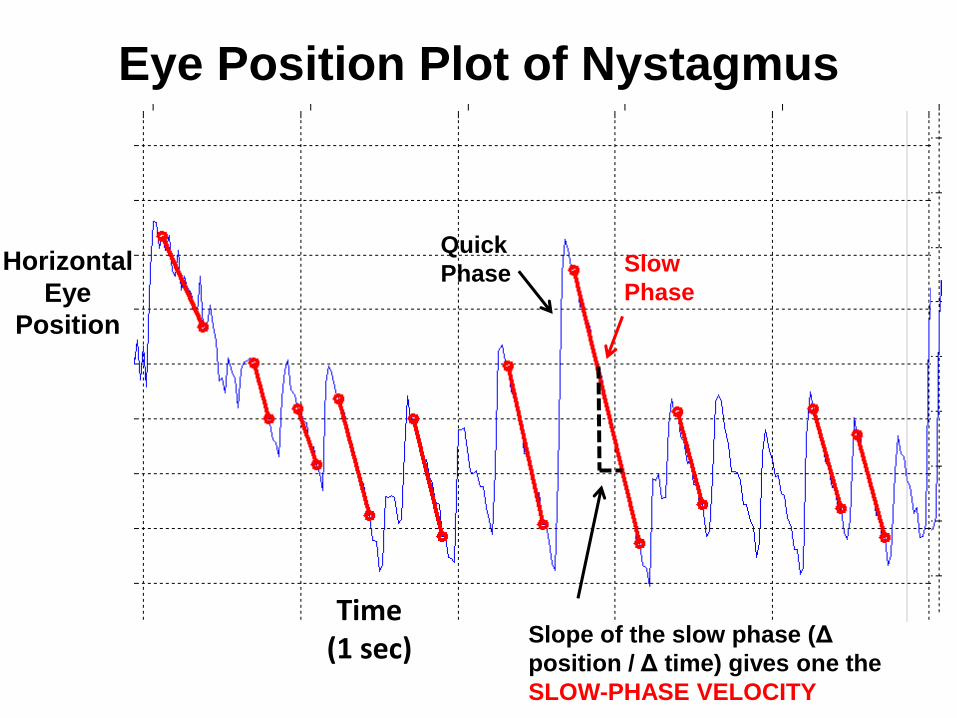
Eye Position Plot of Nystagmus
Horizontal
Eye
Position
Slow
Phase
Quick
Phase
Slope of the slow phase (Δ
position / Δ time) gives one the
SLOW-PHASE VELOCITY
Time(1 sec)
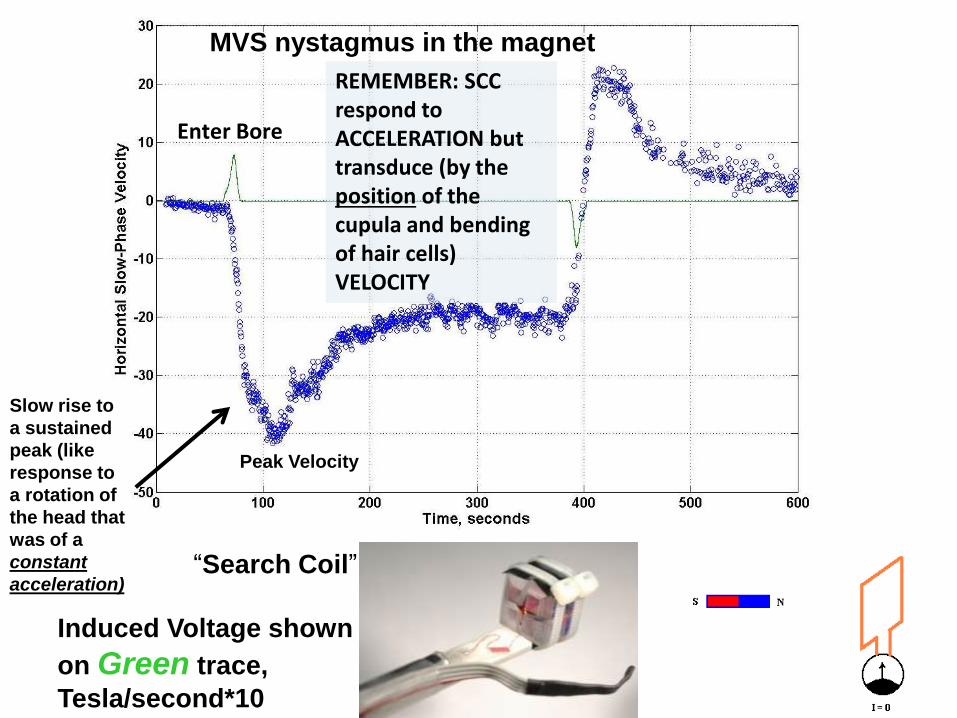
Enter Bore
MVS nystagmus in the magnet
“Search Coil”
Induced Voltage shown
on Green trace,
Tesla/second*10
Peak Velocity
Slow rise to
a sustained
peak (like
response to
a rotation of
the head that
was of a
constant
acceleration)
REMEMBER: SCC respond to ACCELERATION but transduce (by the position of the cupula and bending of hair cells) VELOCITY
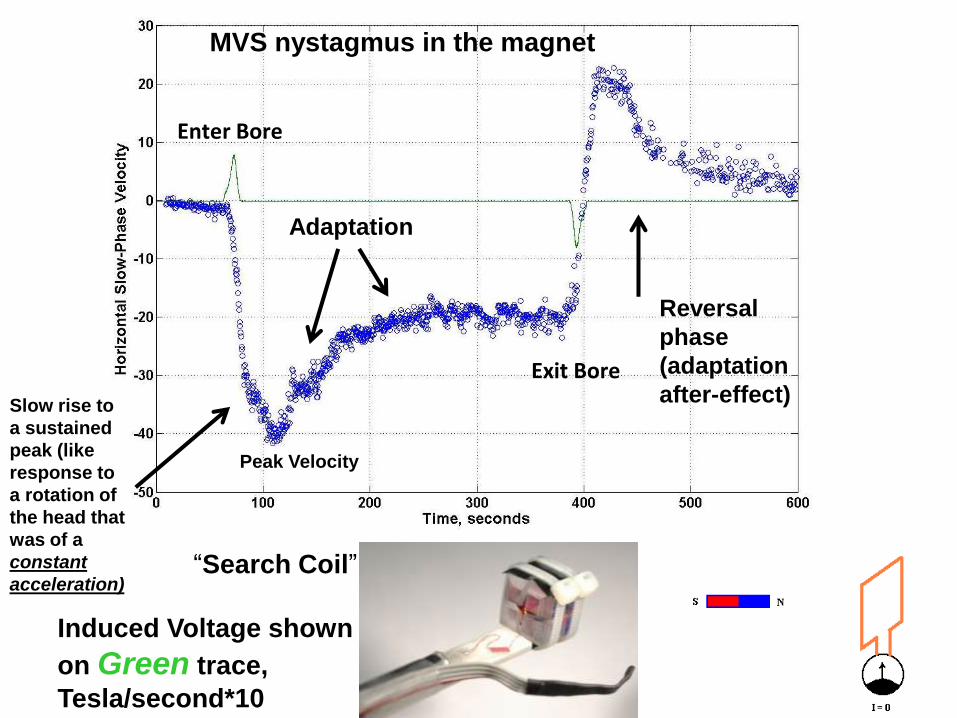
Enter Bore
Exit Bore
Reversal
phase
(adaptation
after-effect)
MVS nystagmus in the magnet
“Search Coil”
Induced Voltage shown
on Green trace,
Tesla/second*10
Peak Velocity
Adaptation
Slow rise to
a sustained
peak (like
response to
a rotation of
the head that
was of a
constant
acceleration)
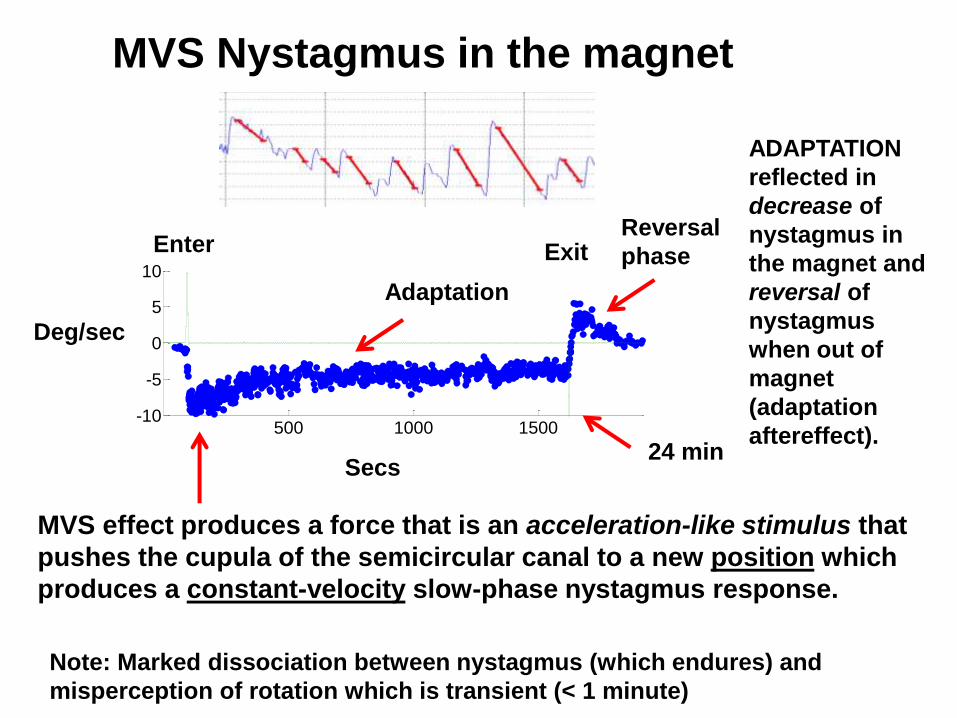
MVS Nystagmus in the magnet
500 1000 1500-10
-5
0
5
10
Slo
w P
hase E
ye V
elo
cit
y(d
eg
rees/s
eco
nd
)
Time (seconds)
Secs
Deg/sec
24 min
Reversal
phase
ADAPTATION
reflected in
decrease of
nystagmus in
the magnet and
reversal of
nystagmus
when out of
magnet
(adaptation
aftereffect).
Enter
Adaptation
Exit
MVS effect produces a force that is an acceleration-like stimulus that
pushes the cupula of the semicircular canal to a new position which
produces a constant-velocity slow-phase nystagmus response.
Note: Marked dissociation between nystagmus (which endures) and
misperception of rotation which is transient (< 1 minute)
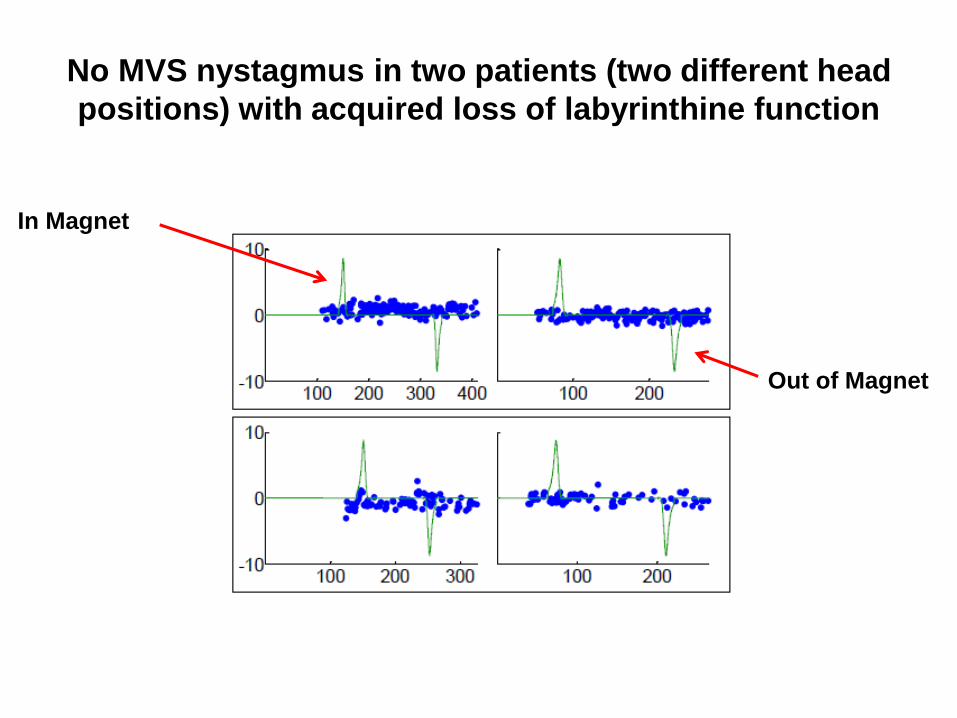
No MVS nystagmus in two patients (two different head
positions) with acquired loss of labyrinthine function
In Magnet
Out of Magnet
What is the mechanism of Magneto-Vestibular Stimulation (MVS)?
• (Dia-, Para-, Ferro-) Magnetic Susceptibility (MS)
• Electromagnetic Induction (dB/dt) (Faraday) – Dynamic
• MHD (Magneto-Hydrodynamics, interaction of ion currents
in fluids and magnetic fields)
– Dynamic
– Static (Lorentz forces)
How might magnetic fields affect biological tissues?
PHYSICS!
100 200
-10
0
10
20
100 200 100 200
100 200-20
-10
0
10
100 200 300
50 100 150 200-10
-5
0
5
10
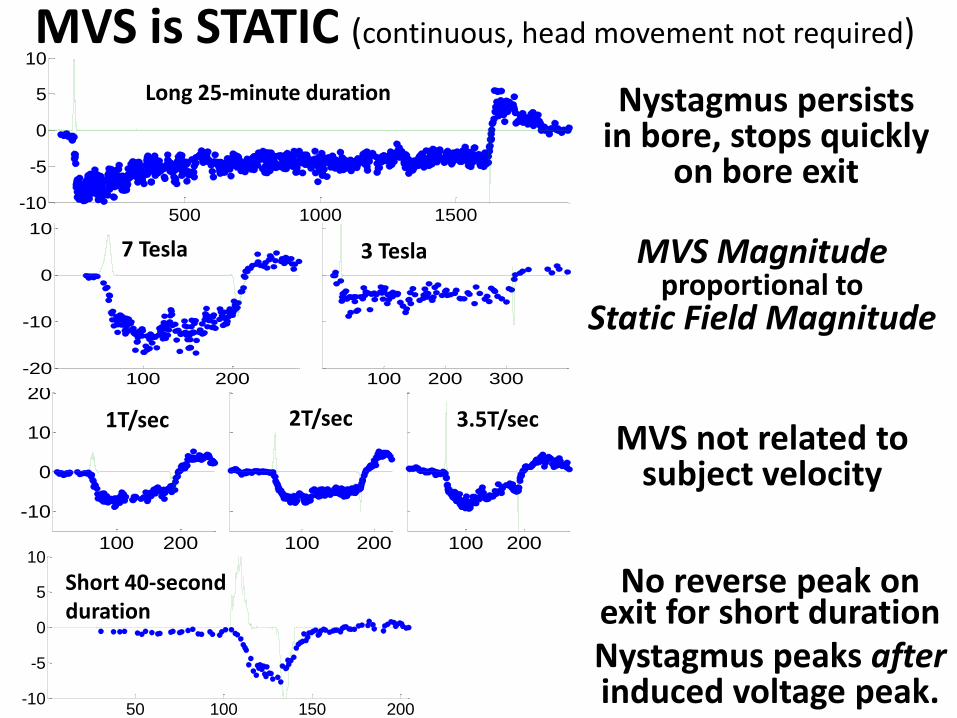
MVS is STATIC (continuous, head movement not required)
MVS not related to subject velocity
MVS Magnitudeproportional to
Static Field Magnitude
7 Tesla 3 Tesla
500 1000 1500-10
-5
0
5
10
Slo
w P
hase E
ye V
elo
cit
y(d
eg
rees/s
eco
nd
)
Time (seconds)
Nystagmus persists in bore, stops quickly
on bore exit
No reverse peak on exit for short durationNystagmus peaks afterinduced voltage peak.
Long 25-minute duration
Short 40-second duration
1T/sec 2T/sec 3.5T/sec

100 200 300 400-10
0
10
50 100 150
MVS is Sensitive to Polarity
Front of magnet Back of magnet
This rules out Magnetic Susceptibility, which is not polarity sensitive.
Magnetic Vestibular Stimulation is:
• Static - continuous, not related to transiently induced voltages (e.g., electromagnetic induction, Faraday forces)
• Polarity Sensitive – Reversing the magnetic field vector reverses the nystagmus direction, therefore not do to magnetic susceptibility properties of tissues.
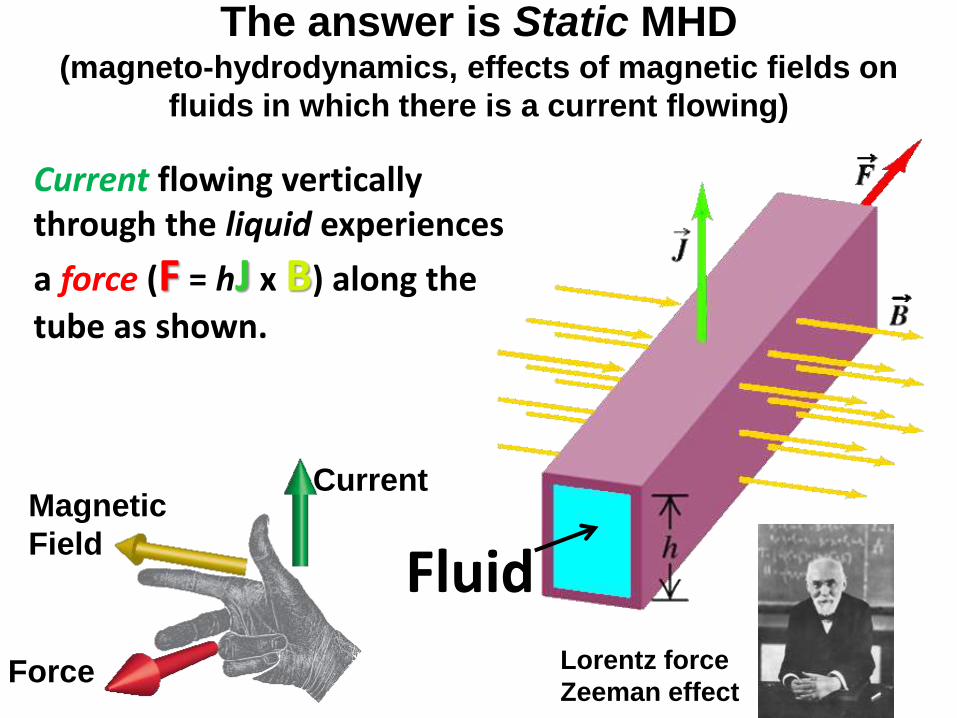
Current flowing vertically through the liquid experiences
a force (F = hJ x B) along the
tube as shown.
The answer is Static MHD(magneto-hydrodynamics, effects of magnetic fields on
fluids in which there is a current flowing)
Fluid
CurrentMagnetic
Field
Force Lorentz force
Zeeman effect
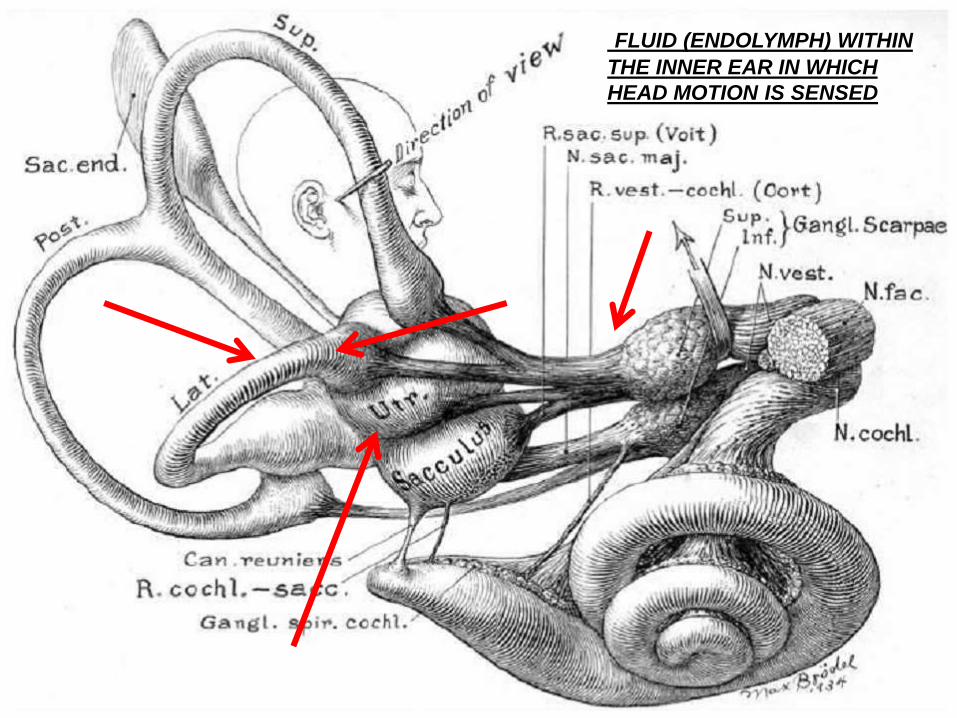
FLUID (ENDOLYMPH) WITHIN
THE INNER EAR IN WHICH
HEAD MOTION IS SENSED
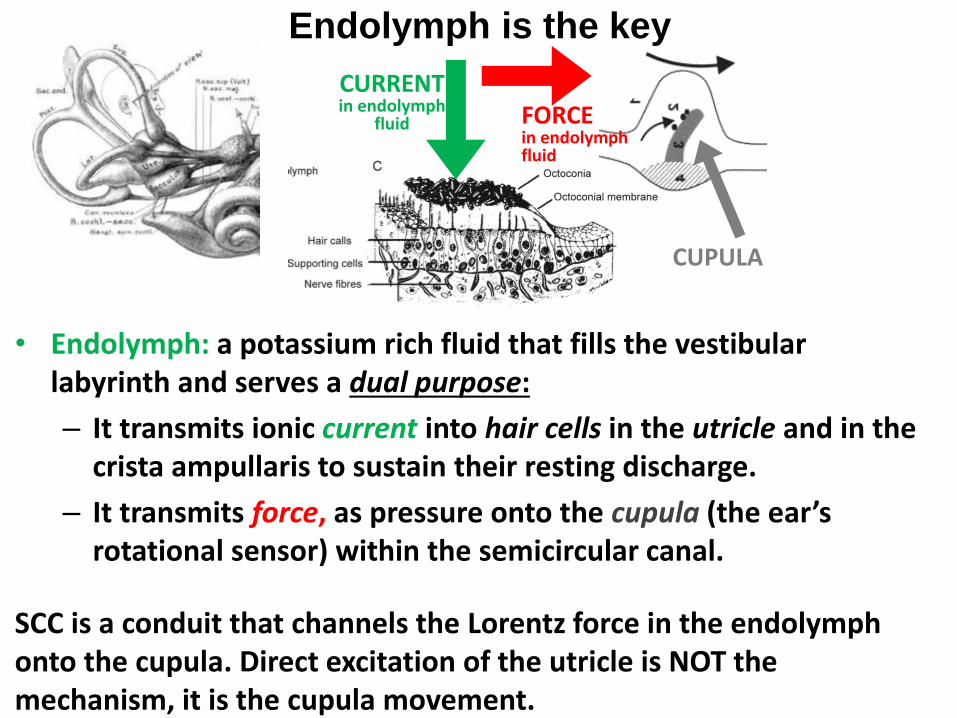
Endolymph is the key
• Endolymph: a potassium rich fluid that fills the vestibular labyrinth and serves a dual purpose:
– It transmits ionic current into hair cells in the utricle and in the crista ampullaris to sustain their resting discharge.
– It transmits force, as pressure onto the cupula (the ear’s rotational sensor) within the semicircular canal.
SCC is a conduit that channels the Lorentz force in the endolymph onto the cupula. Direct excitation of the utricle is NOT the mechanism, it is the cupula movement.
CURRENTin endolymph
fluid FORCEin endolymph fluid
CUPULA

•What is the source and path by which a horizontal nystagmus could be produced?
•Are MHD forces sufficient to cause
nystagmus?
Two Key Questions

SOURCE AND PATH
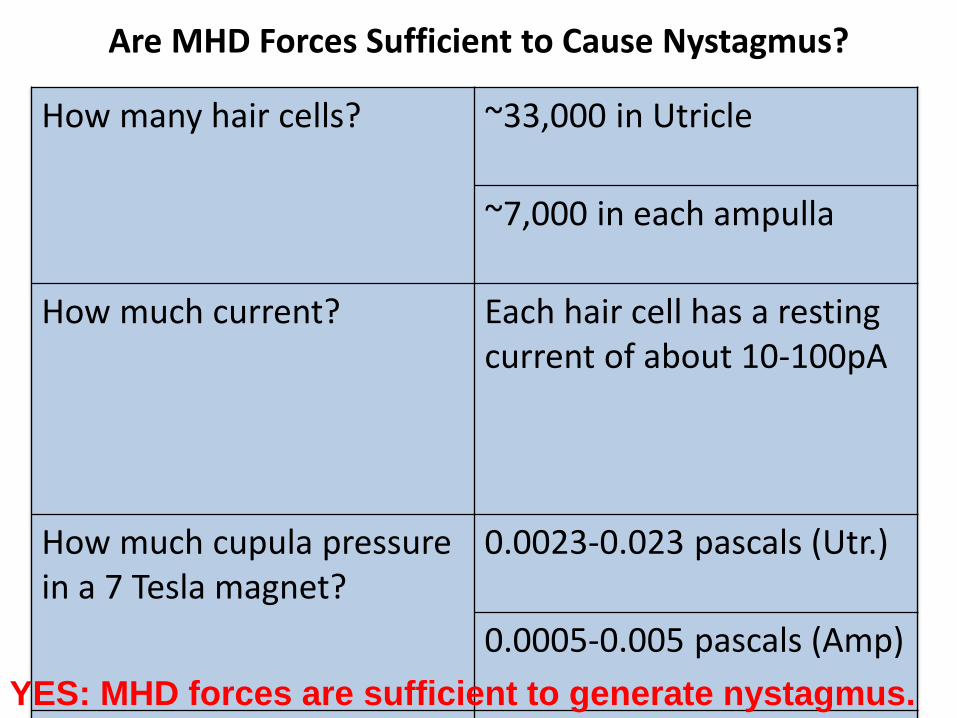
Are MHD Forces Sufficient to Cause Nystagmus?
How many hair cells? ~33,000 in Utricle
~7,000 in each ampulla
How much current? Each hair cell has a resting current of about 10-100pA
How much cupula pressure in a 7 Tesla magnet?
0.0023-0.023 pascals (Utr.)
0.0005-0.005 pascals (Amp)
How much cupula pressure 0.0001 pascalsYES: MHD forces are sufficient to generate nystagmus.
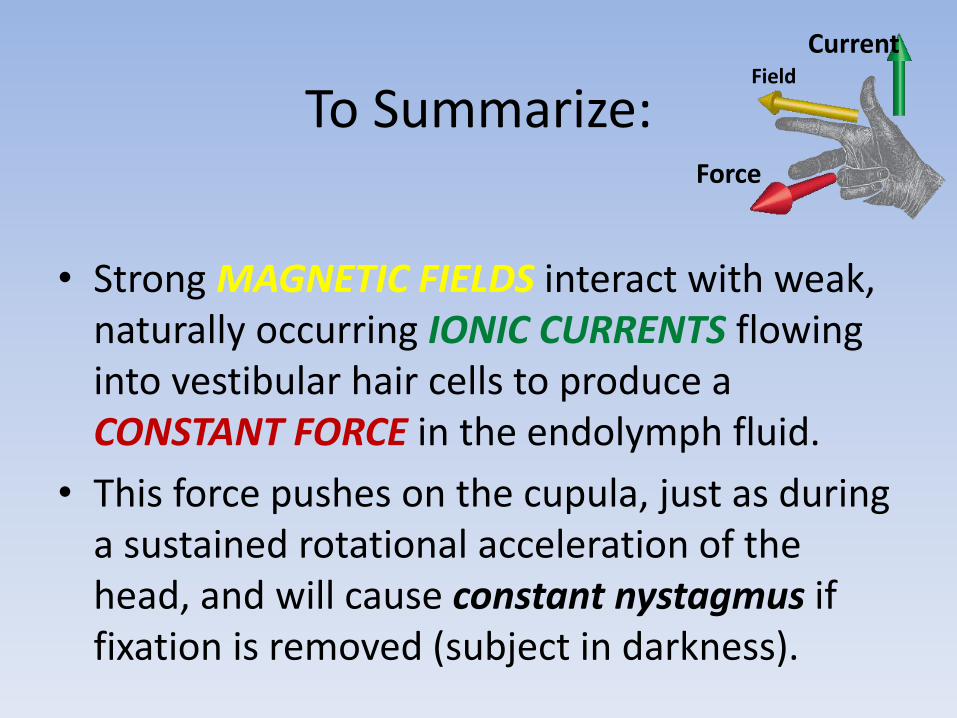
To Summarize:
• Strong MAGNETIC FIELDS interact with weak, naturally occurring IONIC CURRENTS flowing into vestibular hair cells to produce a CONSTANT FORCE in the endolymph fluid.
• This force pushes on the cupula, just as during a sustained rotational acceleration of the head, and will cause constant nystagmus if fixation is removed (subject in darkness).
CurrentField
Force
The Lorenz forces are sufficient,
but are the directions correct?
Must explore the geometrical relationships between the
orientation of the semicircular canals and the utricle in
the head and the position of the head relative to the
direction of the magnetic field in the bore.
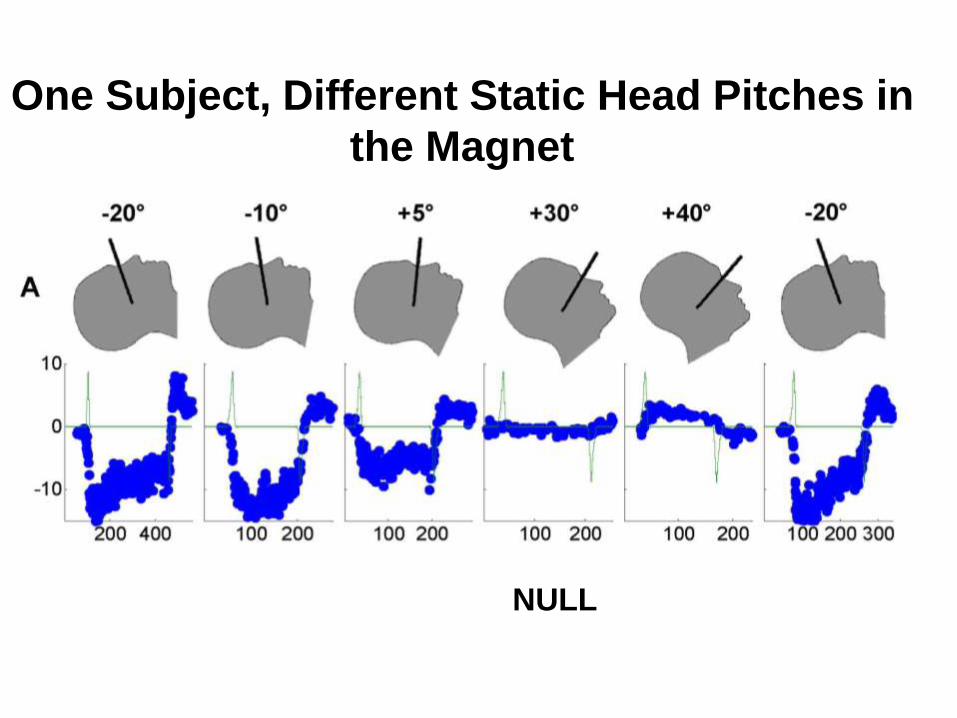
One Subject, Different Static Head Pitches in
the Magnet
NULL
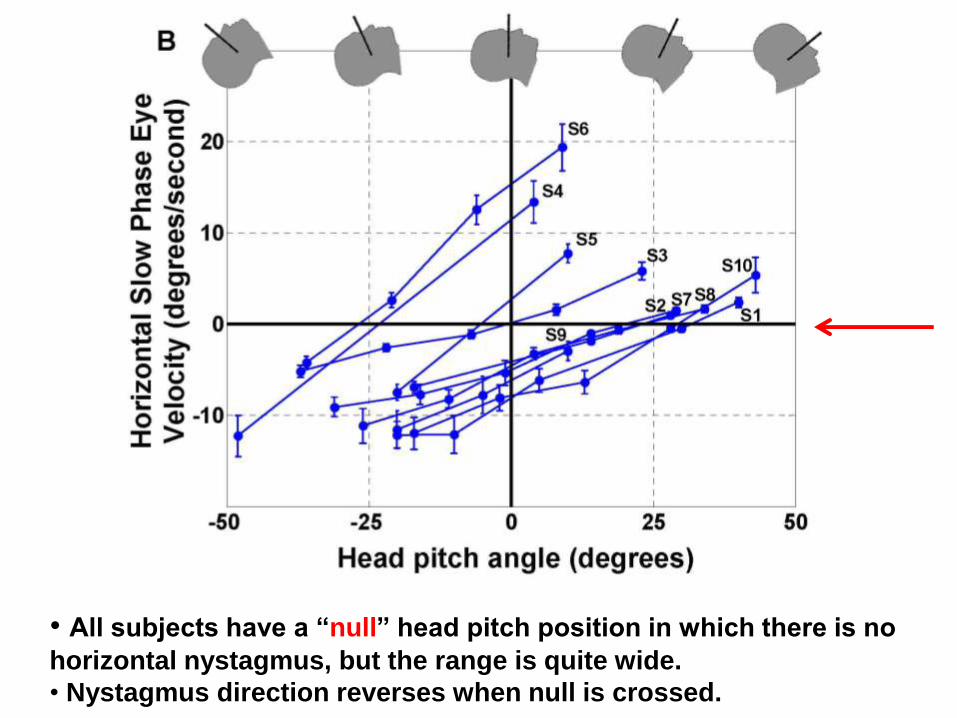
• All subjects have a “null” head pitch position in which there is no
horizontal nystagmus, but the range is quite wide.
• Nystagmus direction reverses when null is crossed.
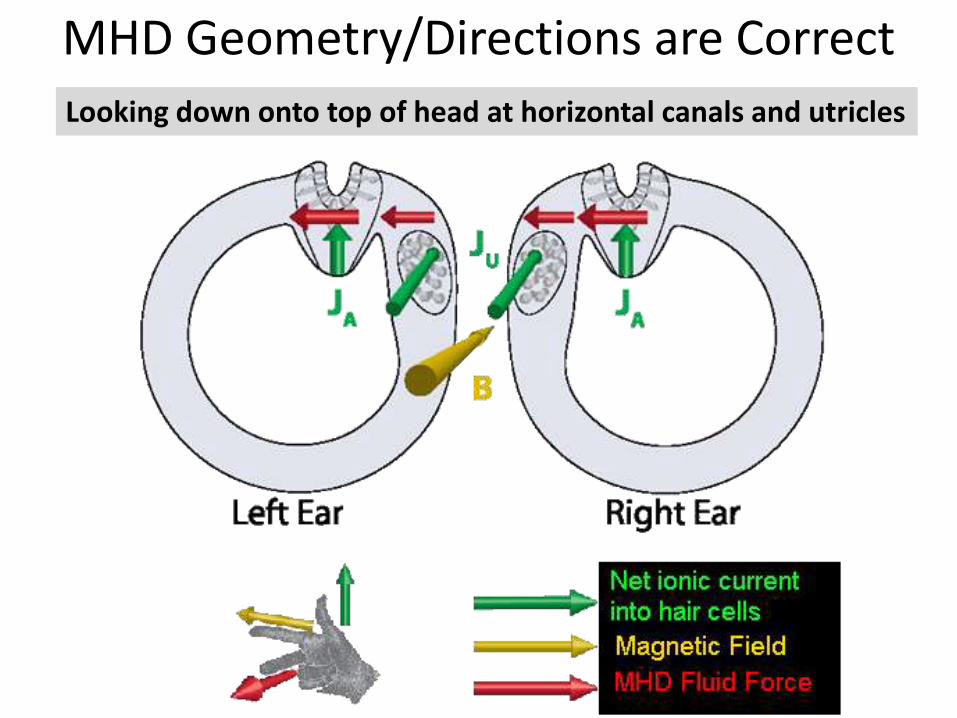
MHD Geometry/Directions are Correct
Looking down onto top of head at horizontal canals and utricles
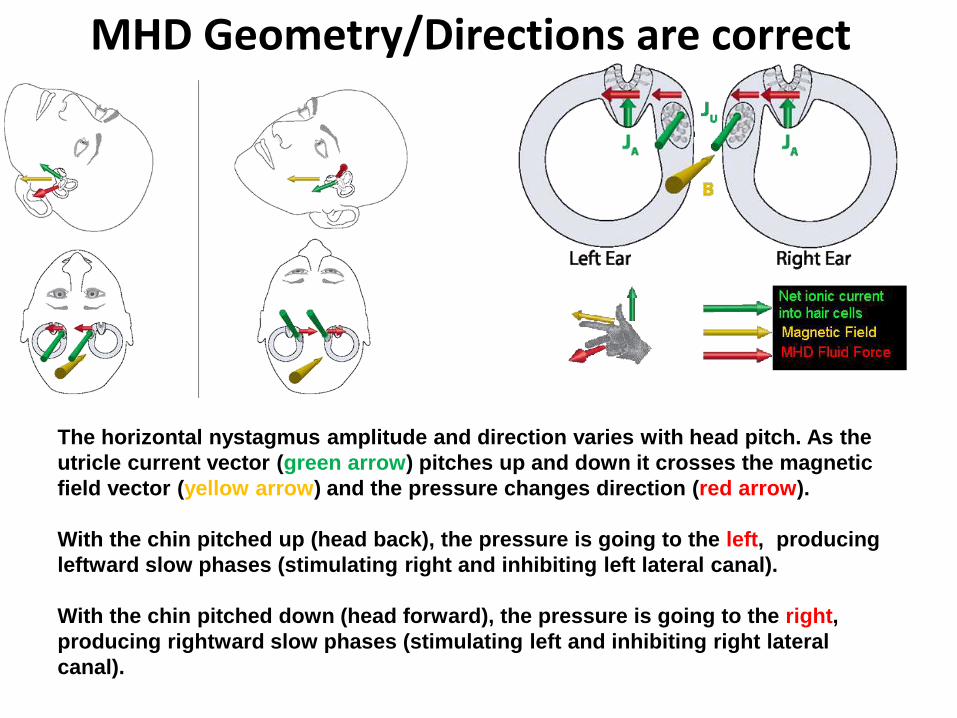
MHD Geometry/Directions are correct
The horizontal nystagmus amplitude and direction varies with head pitch. As the
utricle current vector (green arrow) pitches up and down it crosses the magnetic
field vector (yellow arrow) and the pressure changes direction (red arrow).
With the chin pitched up (head back), the pressure is going to the left, producing
leftward slow phases (stimulating right and inhibiting left lateral canal).
With the chin pitched down (head forward), the pressure is going to the right,
producing rightward slow phases (stimulating left and inhibiting right lateral
canal).
Conclusion: Nystagmus in the MRI bore is
explained by the effects of magnetic fields on
the labyrinth, specifically Lorenz forces
Roberts, DC, Marcelli, V, Gillen, JS, Carey, JP, Della Santina, CC, Zee,
DS, MRI magnetic field stimulates rotational sensors of the brain,
Current Biology, 2011

BPPV (benign paroxysmal
positional vertigo)
Ward et al. (2015)
CSF leak (after
endonasal surgery
for a pituitary
adenoma) opened
by vomiting induced
in MRI magnetic
field
A few clinical implications
– Unilateral loss vestibular patients (UVL)
• Parsing out which parts of the labyrinth are
affected based on the pattern of MVS
– AS PREDICTED: UVL patients show a vertical slow-
phase component and the direction depends on
which labyrinth is affected
– This is due to the proximity of the opening of the
superior (anterior) canal as well as the lateral canal
to the utricle
FURTHER SUPPORT FOR MVS
MECHANISM
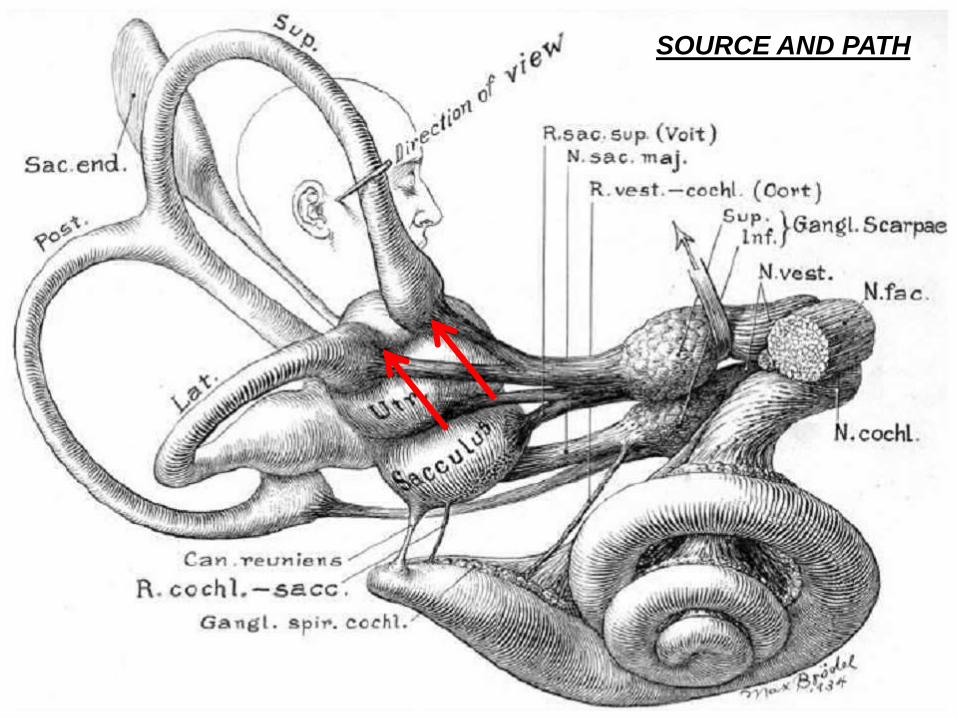
SOURCE AND PATH
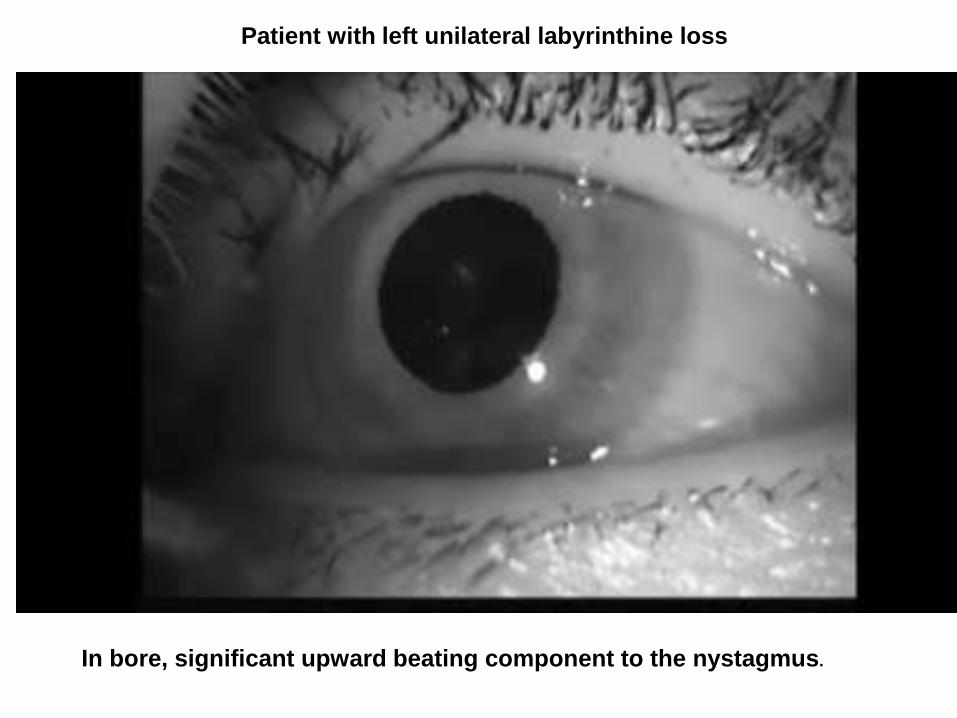
In bore, significant upward beating component to the nystagmus.
Patient with left unilateral labyrinthine loss
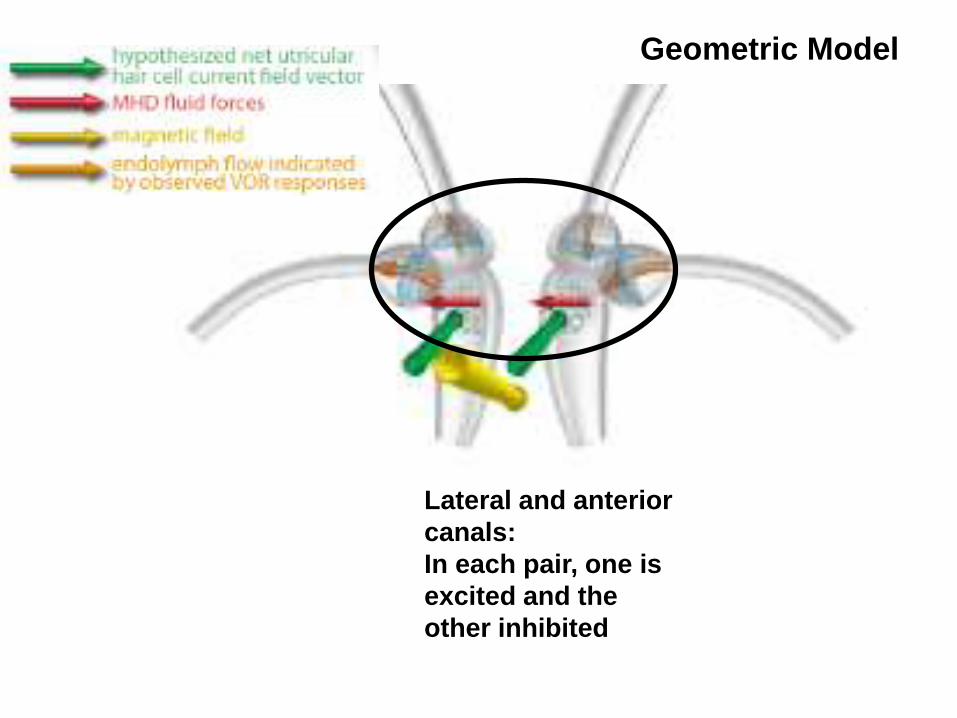
Lateral and anterior
canals:
In each pair, one is
excited and the
other inhibited
Geometric Model
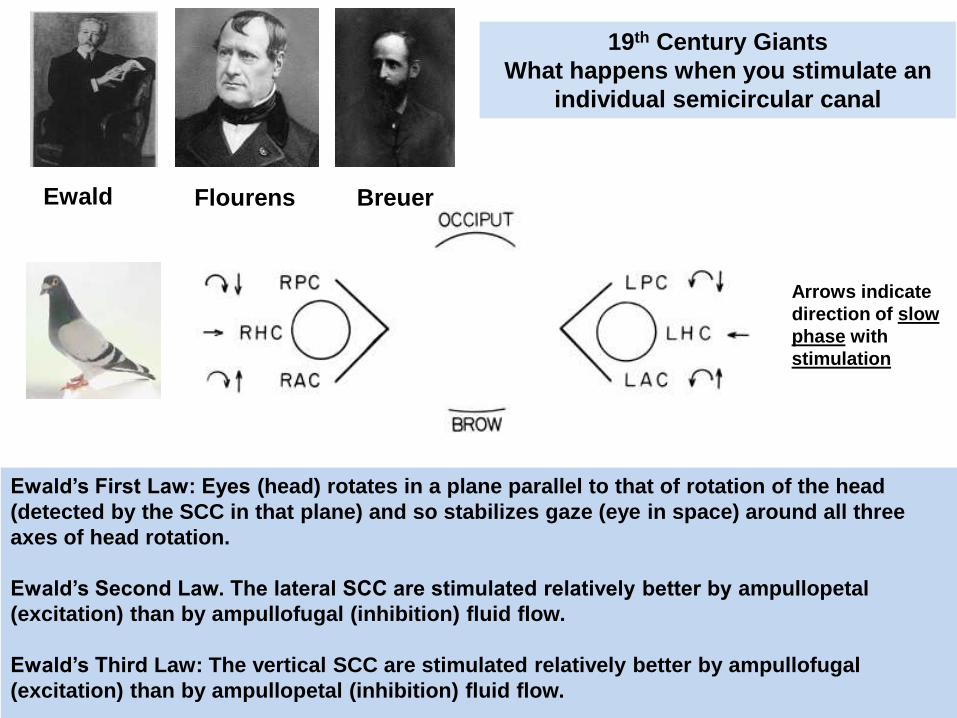
Ewald’s First Law: Eyes (head) rotates in a plane parallel to that of rotation of the head
(detected by the SCC in that plane) and so stabilizes gaze (eye in space) around all three
axes of head rotation.
Ewald’s Second Law. The lateral SCC are stimulated relatively better by ampullopetal
(excitation) than by ampullofugal (inhibition) fluid flow.
Ewald’s Third Law: The vertical SCC are stimulated relatively better by ampullofugal
(excitation) than by ampullopetal (inhibition) fluid flow.
19th Century Giants
What happens when you stimulate an
individual semicircular canal
Arrows indicate
direction of slow
phase with
stimulation
Ewald Flourens Breuer
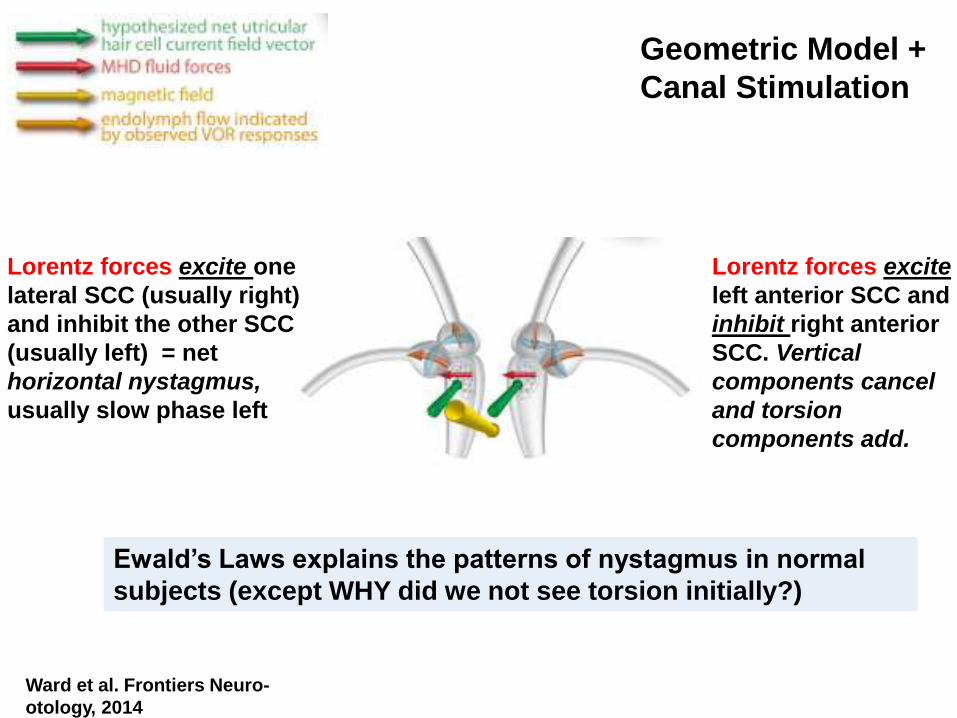
Lorentz forces excite one
lateral SCC (usually right)
and inhibit the other SCC
(usually left) = net
horizontal nystagmus,
usually slow phase left
Lorentz forces excite
left anterior SCC and
inhibit right anterior
SCC. Vertical
components cancel
and torsion
components add.
Ward et al. Frontiers Neuro-
otology, 2014
Ewald’s Laws explains the patterns of nystagmus in normal
subjects (except WHY did we not see torsion initially?)
Geometric Model +
Canal Stimulation
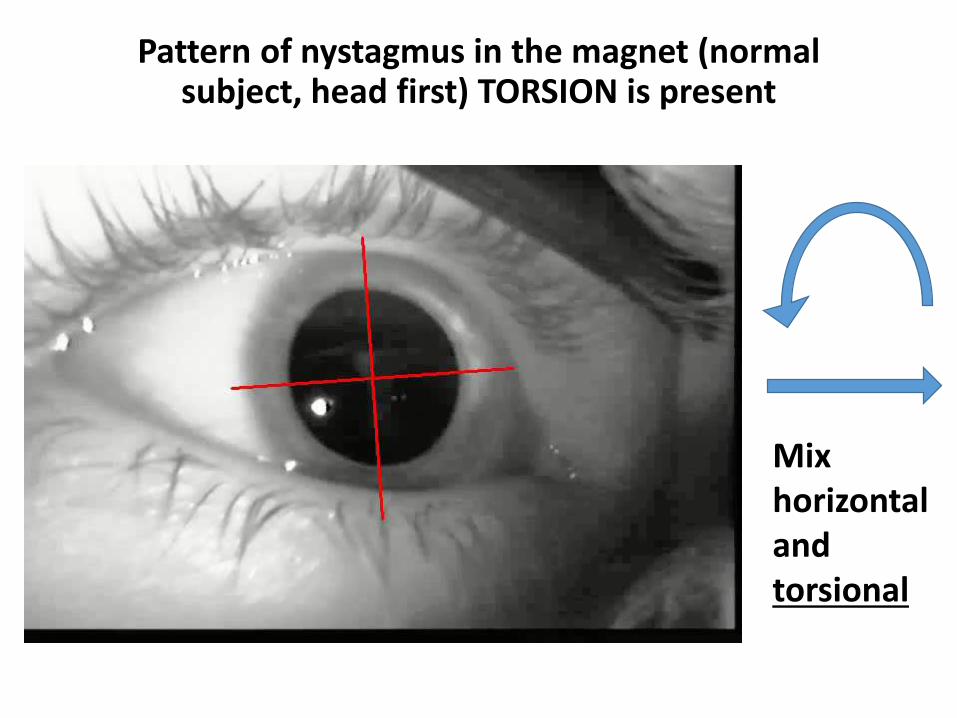
Pattern of nystagmus in the magnet (normal subject, head first) TORSION is present
Mix horizontal and torsional

LEFT-SIDED
LOSS, inhibition
of remaining
right anterior
SCC = upbeat
nystagmus
RIGHT-SIDED
LOSS, excitation
of remaining left
anterior SCC =
downbeat
nystagmus
Ewald’s Laws explain the patterns of
nystagmus in unilateral loss patients
Animal models
Mice (genetic mutants) and Zebra fish (ototoxicity)
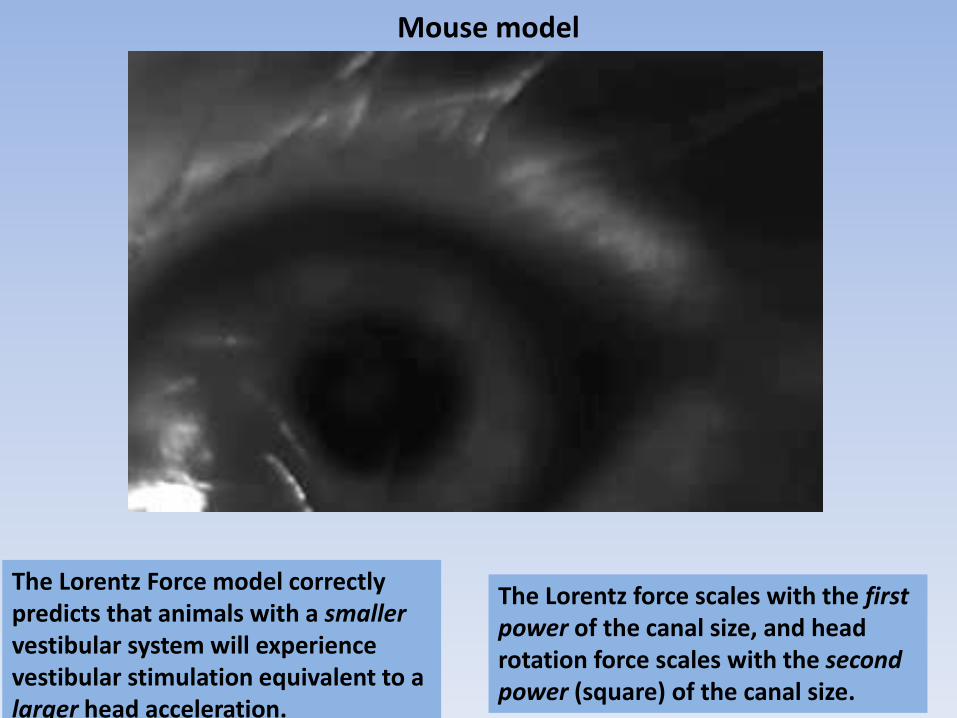
Mouse model
The Lorentz Force model correctly predicts that animals with a smallervestibular system will experience vestibular stimulation equivalent to a larger head acceleration.
The Lorentz force scales with the first power of the canal size, and head rotation force scales with the second power (square) of the canal size.
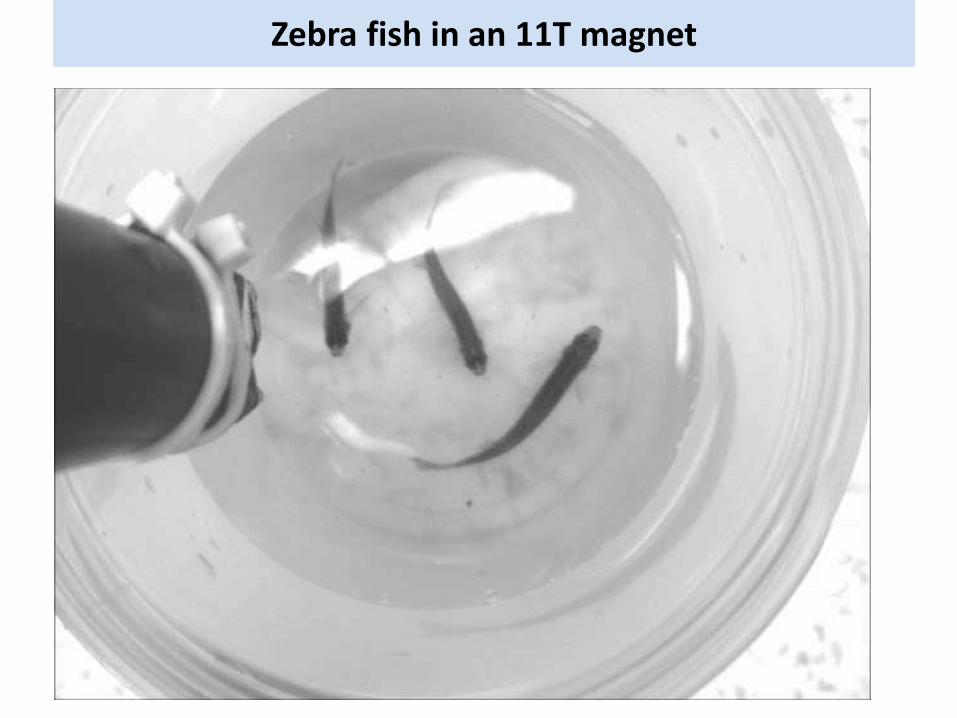
Zebra fish in an 11T magnet
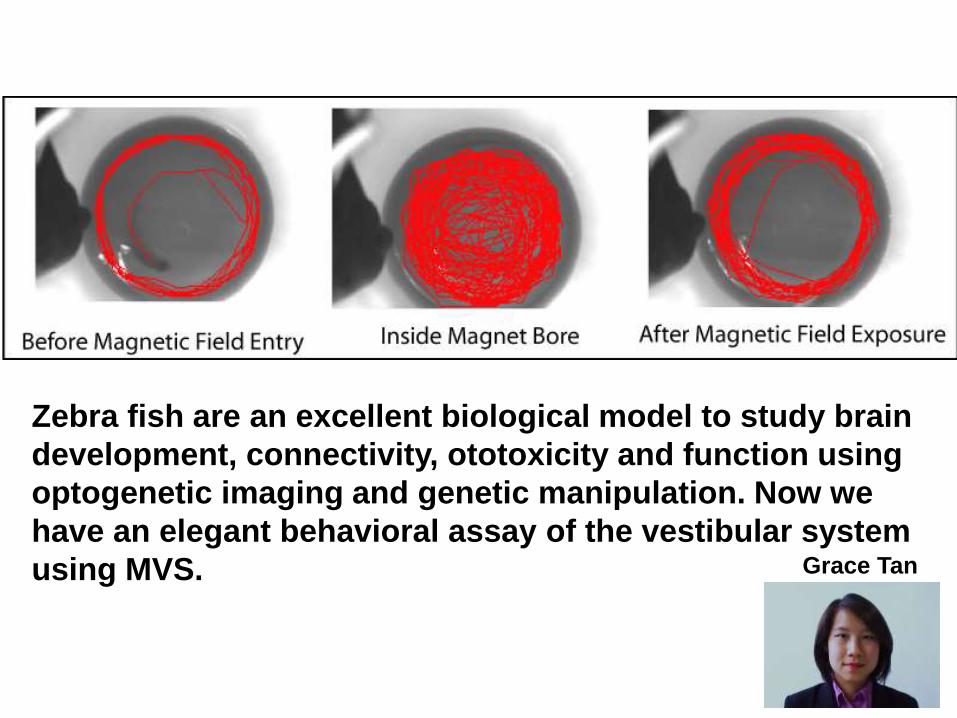
Zebra fish are an excellent biological model to study brain
development, connectivity, ototoxicity and function using
optogenetic imaging and genetic manipulation. Now we
have an elegant behavioral assay of the vestibular system
using MVS. Grace Tan
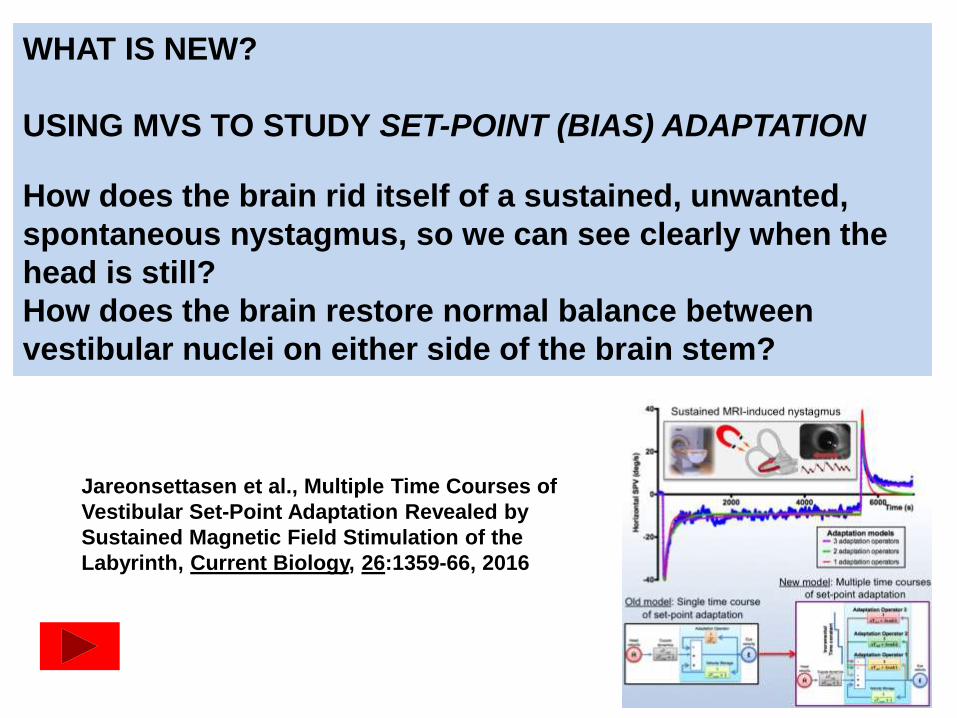
Jareonsettasen et al., Multiple Time Courses of
Vestibular Set-Point Adaptation Revealed by
Sustained Magnetic Field Stimulation of the
Labyrinth, Current Biology, 26:1359-66, 2016
WHAT IS NEW?
USING MVS TO STUDY SET-POINT (BIAS) ADAPTATION
How does the brain rid itself of a sustained, unwanted,
spontaneous nystagmus, so we can see clearly when the
head is still?
How does the brain restore normal balance between
vestibular nuclei on either side of the brain stem?
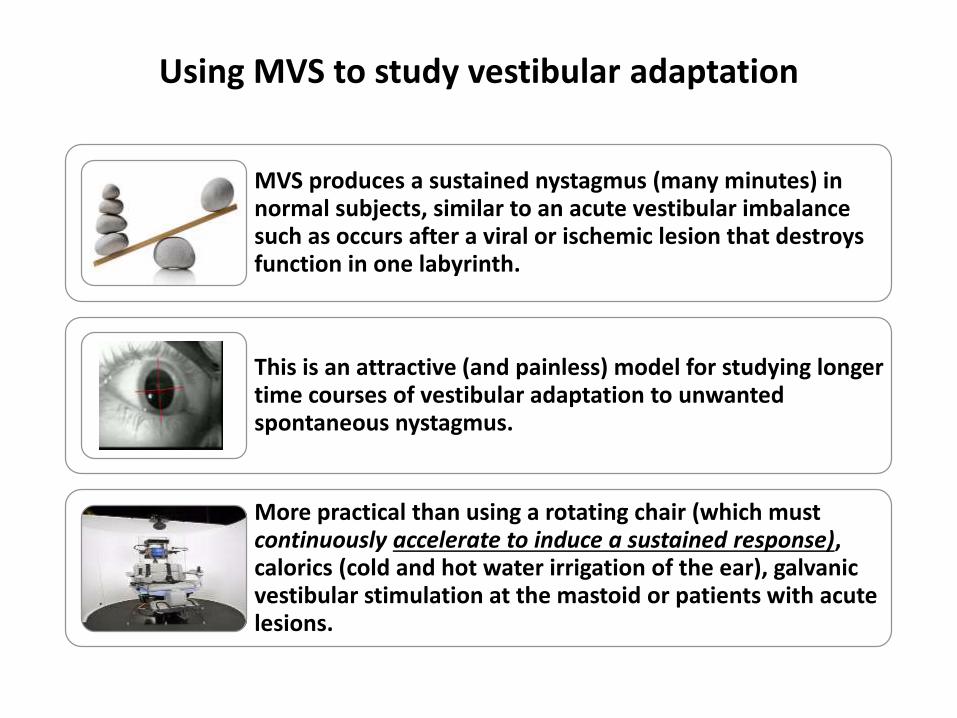
Using MVS to study vestibular adaptation
MVS produces a sustained nystagmus (many minutes) in normal subjects, similar to an acute vestibular imbalance such as occurs after a viral or ischemic lesion that destroys function in one labyrinth.
This is an attractive (and painless) model for studying longer time courses of vestibular adaptation to unwanted spontaneous nystagmus.
More practical than using a rotating chair (which must continuously accelerate to induce a sustained response), calorics (cold and hot water irrigation of the ear), galvanic vestibular stimulation at the mastoid or patients with acute lesions.
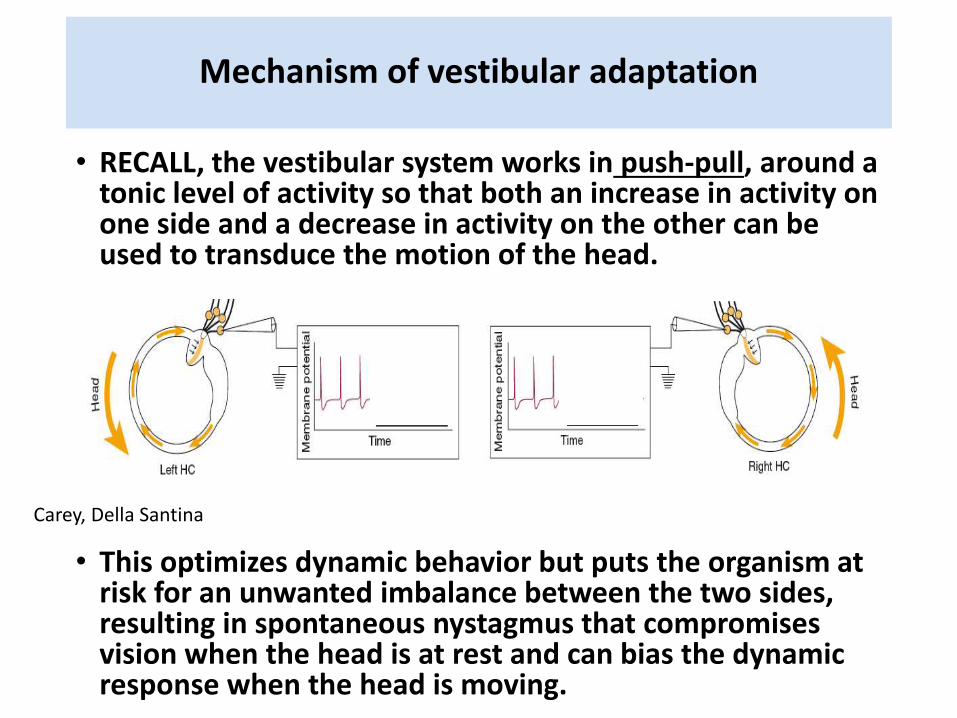
Mechanism of vestibular adaptation
• RECALL, the vestibular system works in push-pull, around a tonic level of activity so that both an increase in activity on one side and a decrease in activity on the other can be used to transduce the motion of the head.
• This optimizes dynamic behavior but puts the organism at risk for an unwanted imbalance between the two sides, resulting in spontaneous nystagmus that compromises vision when the head is at rest and can bias the dynamic response when the head is moving.
Carey, Della Santina

The early lines of defense against a spontaneous nystagmus
• VISUAL fixation mechanisms to suppress a spontaneous nystagmus• Limited velocity range so does not do well for high
velocities of spontaneous nystagmus
• Not as effective for suppression of torsional or vertical nystagmus
• Short-term vestibular adaptation• Reversal phases of rotational, caloric, post head
shaking nystagmus and includes pathological periodic alternating nystagmus (PAN)
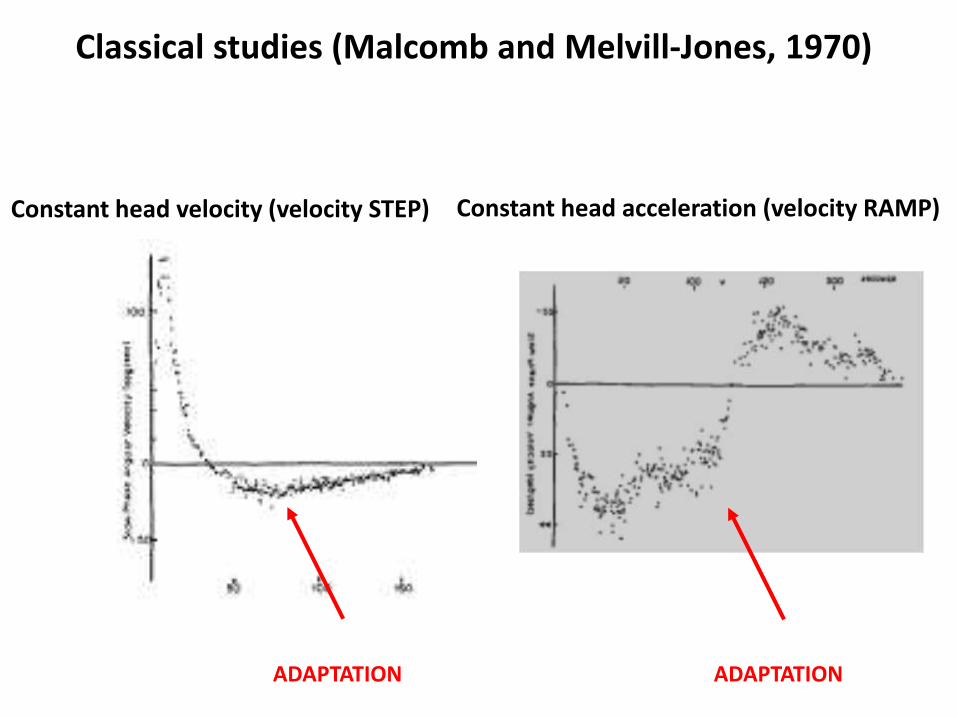
Classical studies (Malcomb and Melvill-Jones, 1970)
Constant head velocity (velocity STEP) Constant head acceleration (velocity RAMP)
ADAPTATION ADAPTATION
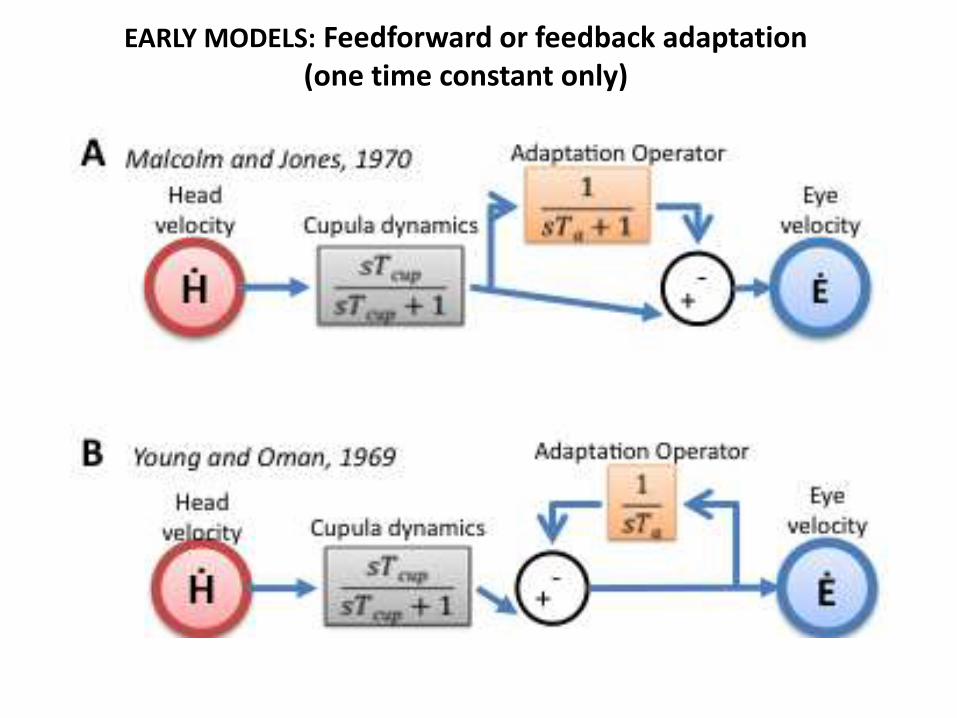
EARLY MODELS: Feedforward or feedback adaptation (one time constant only)
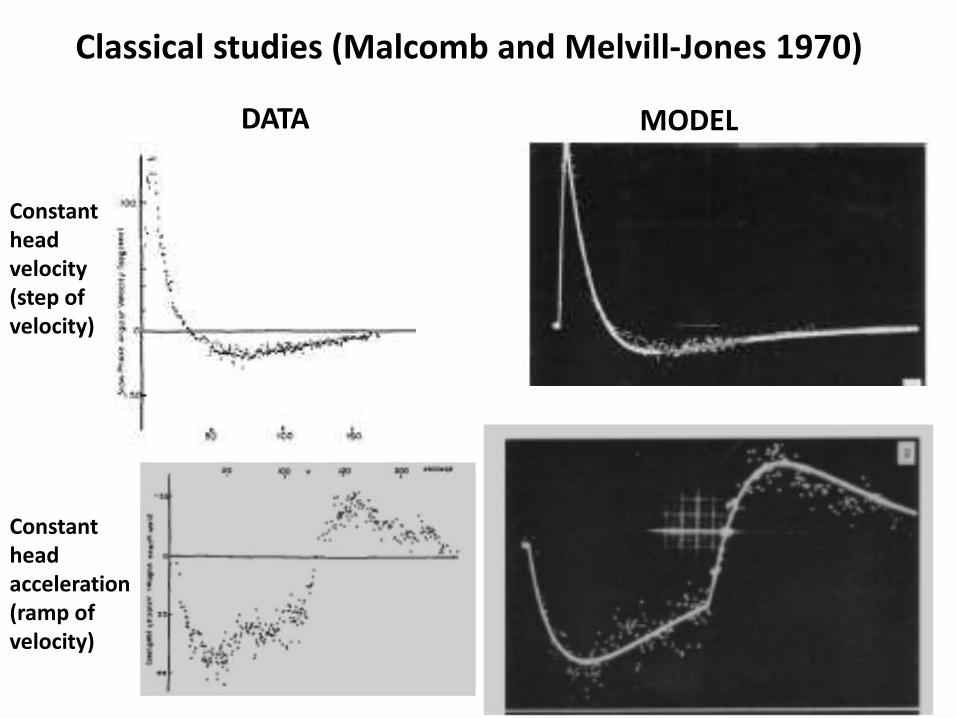
Classical studies (Malcomb and Melvill-Jones 1970)
DATA MODEL
Constant head velocity (step of velocity)
Constant head acceleration (ramp of velocity)
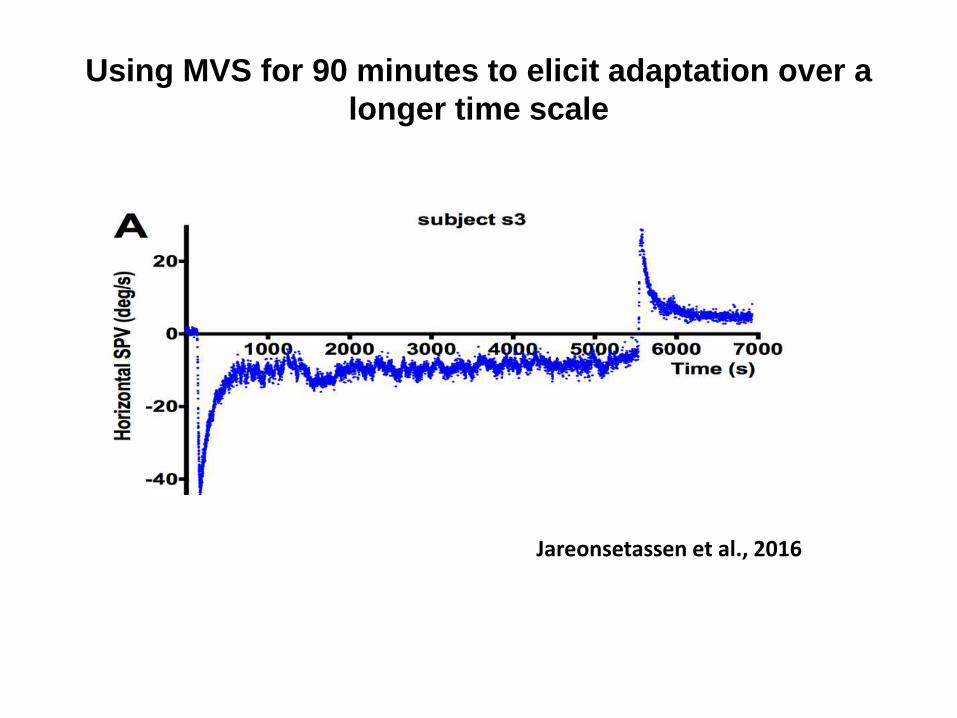
Using MVS for 90 minutes to elicit adaptation over a
longer time scale
Jareonsetassen et al., 2016

Constant acceleration responses: MVS and chair rotations elicit similar adaptation responses
Malcomb, Melvill-Jones, 1970 Jareonsetassen et al., 2016

TWO NEW IDEAS• Adaptation operators are variably leaky integrators (modifiable leak and tc
parameters)• Multiple adaptation operators with progressively different dynamics (Ta3 >
Ta2 > Ta1)
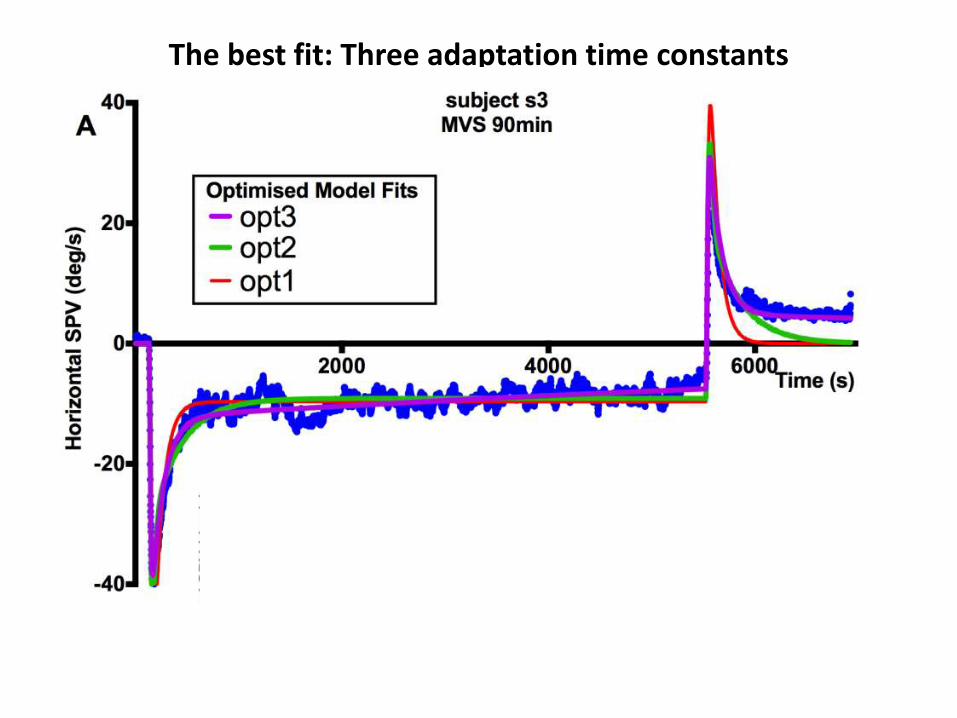
The best fit: Three adaptation time constants

Take home messages about MVS (magneto
vestibular stimulation)
– EVERYBODY (humans, mice, zebra fish) develops nystagmus (or postural
abnormalities) in an MRI machine from the magnetic field itself (no imaging
needed) due to static magneto-hydrodynamic (Lorentz) forces acting on the ion -
carrying endolymph of the inner ear semicircular canals.
– MVS is a simple, safe, comfortable tool to elicit a sustained vestibular imbalance
and study
• The functional anatomy of vestibular stimulation and visual-vestibular
interaction
• Mechanisms of vestibular adaptation as a model of motor learning (“set-
point” or “bias” adaptation)
• Mechanisms of vestibular perception
• Effects of drugs and other therapies, genetic manipulations, development,
etc., on vestibular function
• A potential rehabilitative technique, for balance as well as for higher level
cognitive disorders such as neglect
• BEWARE effects on functional MRI and resting state connectivity

![Electrical Vestibular Stimulation after Vestibular ......electrical stimulation of the vestibular system to one ear [4,5,9]. However studies have also reported vestibular responses](https://img.pdfslide.net/doc/110x75/60f6b0762ca1b41e91018b73/electrical-vestibular-stimulation-after-vestibular-electrical-stimulation.jpg)