Embed Size (px)
Citation preview
Making it happen Improving quality to improve
productivity
The Great Ormond Street Hospital for Children Experience
Can it really be done?
© Great Ormond Street
Key note Lord Howe
Aim to achieve best outcomes but using less Pay freeze Innovation and creativity
Aim to combine work of on care with levels of equity, excellence in clinical outcomes, free from micro management from above from a whole top down system – a system that progress of what we can do
Way forward is to have ideas flowing from the bottom up form innovation and creativity
© Great Ormond Street
Some of the key changes
Structural change PCTs and replacement by GP consortia – align clinical decision making with funding
All foundation trusts and competition Open health market to any willing provider –
benefits of competition Devolve power to the front line Improve quality and release funds Improve quality –patient empowerment
clinical leadership and competition
© Great Ormond Street
Key question to be answered
Can we look at ways of delivering health care at lower cost and with increased productivity (or value) while we increase quality and safety? (4% per year)

Most health care today is sought, created, delivered and purchased at the level of the clinical micro-system. It is there that real gains in the quality, value, and safety of care can occur.
Integration of information Measurement of outcomes Interdependence of the care
teams Supportiveness of the larger
system Constancy of purpose Connection to the community
and client involvement Investment in improvement –
want to be better Alignment of role and training
with improvement methods
More on micro-systems
J J Mohr and P B Batalden: Improving safety on the front lines: the role of clinical micro-systems 2002;11;45-50 Qual. Saf. Health Care
© Great Ormond Street
Is there evidence?
“Does improving quality save money? Sometimes, but sometimes not, and mostly we do not know because the research is limited. There is a great potential for savings, but it depends what we mean by quality improvement, who makes the savings and when.”
© Great Ormond Street
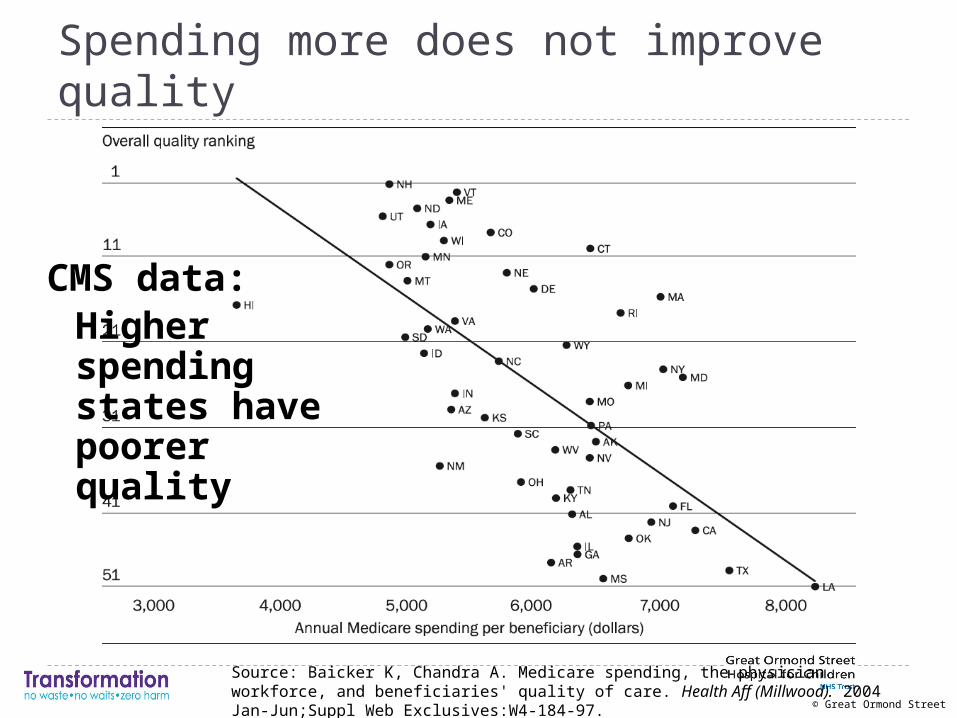
Spending more does not improve quality
CMS data: Higher spending states have poorer quality
Source: Baicker K, Chandra A. Medicare spending, the physician workforce, and beneficiaries' quality of care. Health Aff (Millwood). 2004 Jan-Jun;Suppl Web Exclusives:W4-184-97.
The GOSH strategy- aiming for high reliability and
zero harm
High reliability means the patient gets exactly the treatment needed when it is needed and how it is wanted …..every time
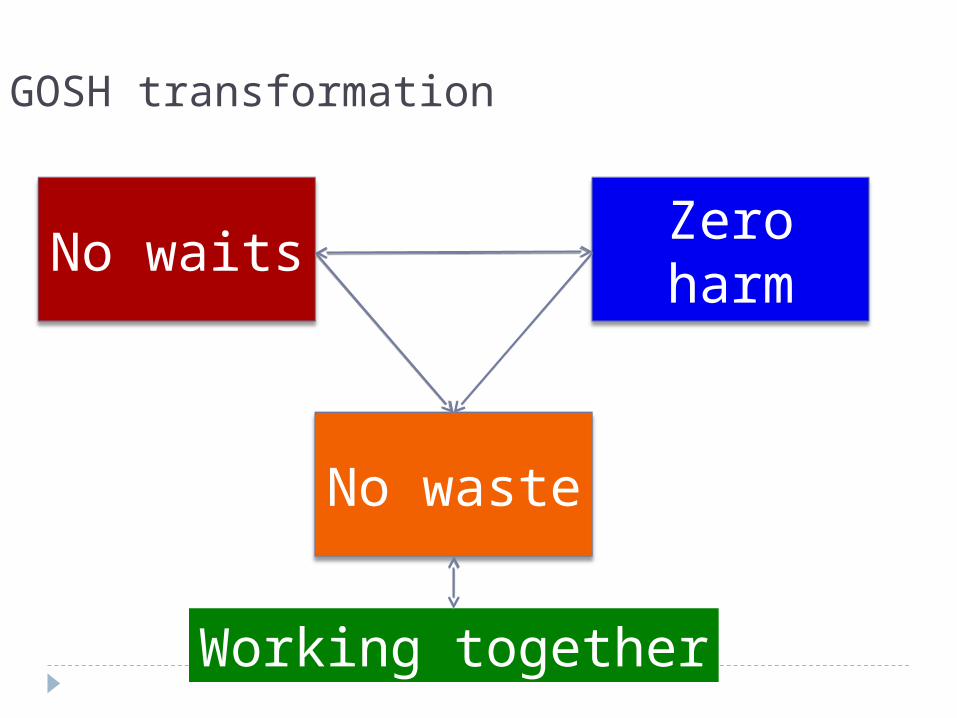
No waits
No waste
Zero harm
Working together
GOSH transformation
© Great Ormond Street
Increasing productivity needs a platform
Leadership Knowledge - improvement
methodology and skills Information Data Understanding the problem Resource to implement change Redesign of services
© Great Ormond Street
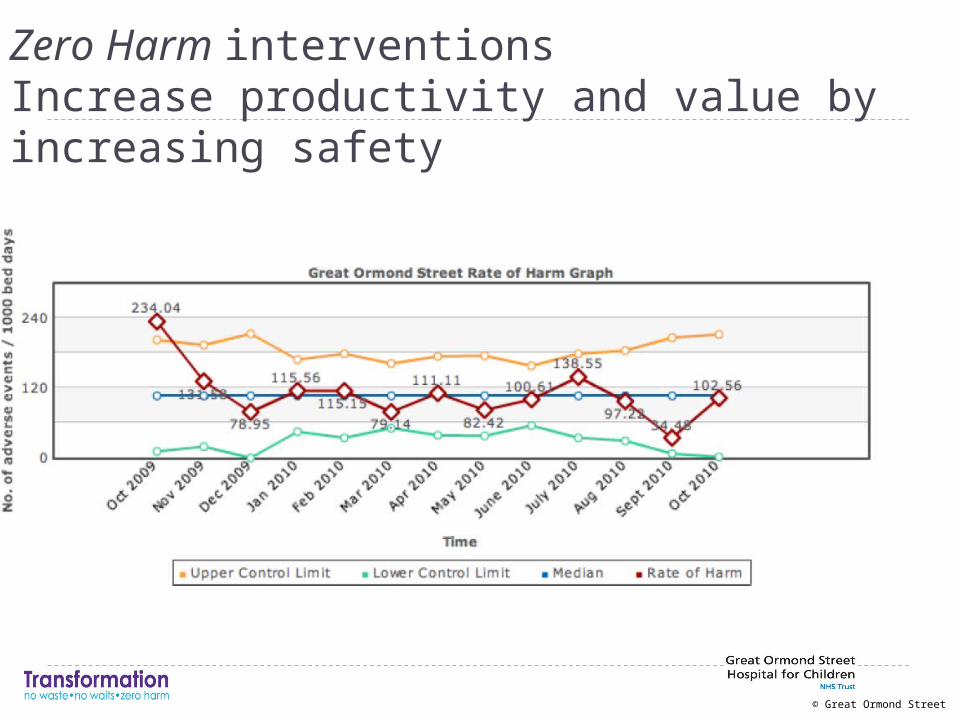
Zero Harm interventionsIncrease productivity and value by increasing safety
© Great Ormond Street
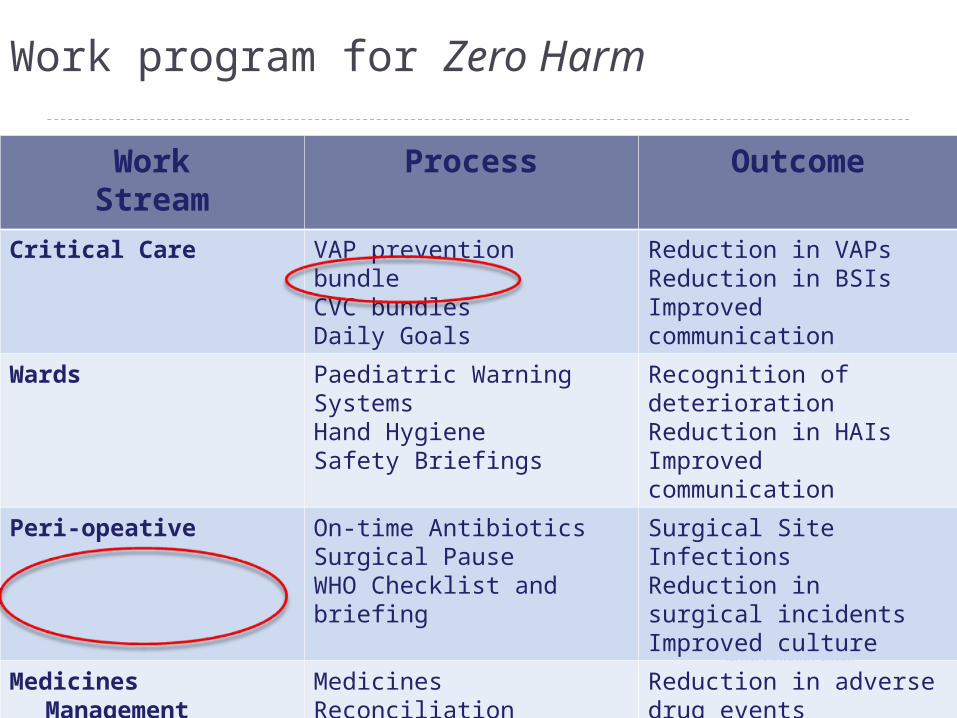
Work program for Zero Harm
WorkStream
Process Outcome
Critical Care VAP prevention bundleCVC bundlesDaily Goals
Reduction in VAPsReduction in BSIsImproved communication
Wards Paediatric Warning SystemsHand HygieneSafety Briefings
Recognition of deteriorationReduction in HAIsImproved communication
Peri-opeative On-time AntibioticsSurgical PauseWHO Checklist and briefing
Surgical Site InfectionsReduction in surgical incidentsImproved culture
Medicines Management Medicines ReconciliationDosage calculations
Reduction in adverse drug events
Leadership WalkRoundsSafety strategic priority
Culture of Safety
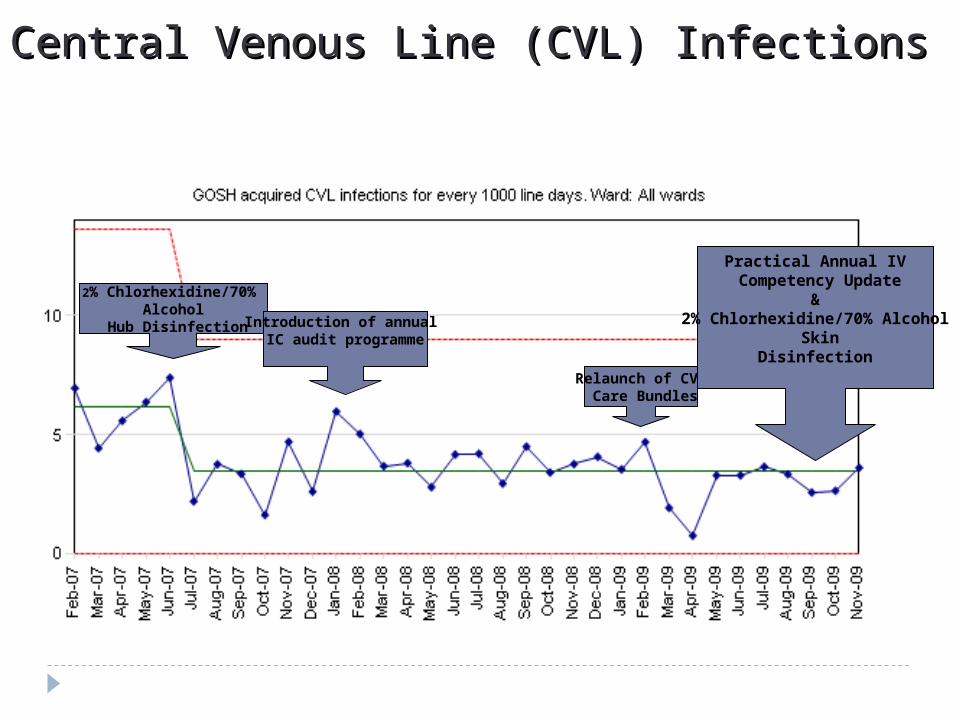
Central Venous Line (CVL) InfectionsCentral Venous Line (CVL) Infections
Relaunch of CVL Care Bundles
Practical Annual IV Competency Update
&2% Chlorhexidine/70% Alcohol
SkinDisinfection
2% Chlorhexidine/70% Alcohol
Hub Disinfection Introduction of annual IC audit programme
© Great Ormond Street
Impact of decreasing infections
Each infection costs from £5000 - £10000 Decrease in line infections from 30 per month
to less than 10 per month saves up to £200000 per month Decreased length of stay Decreased use of time Improved patient experience Ability to reinvest in other activities
© Great Ormond Street
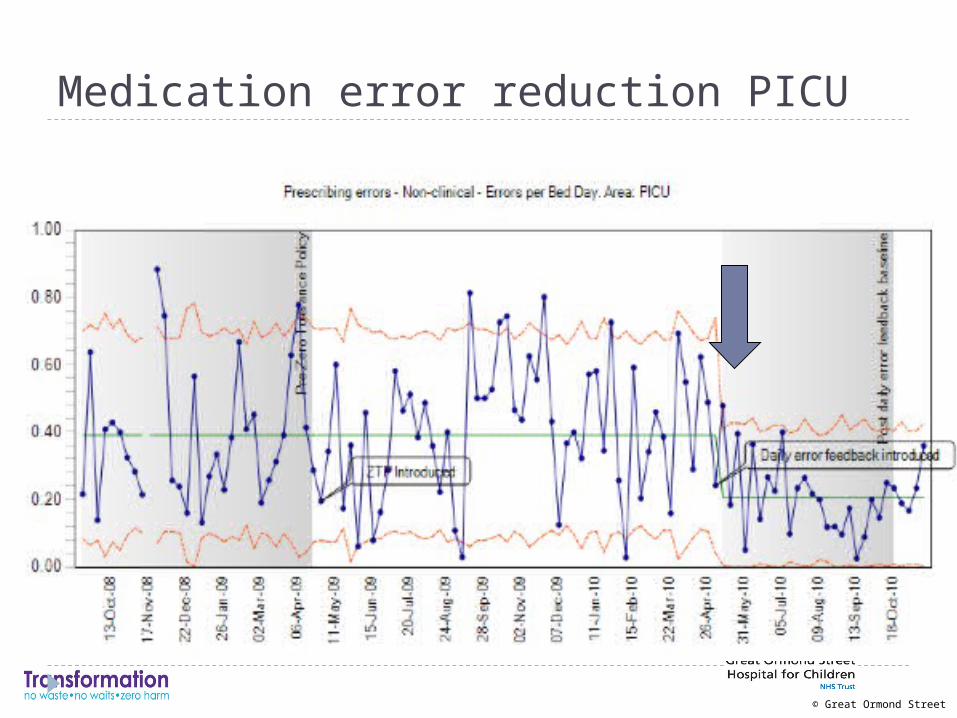
Cost of medication errors
The direct cost of medication errors in NHS hospitals may be £200 - 400 million per year. The potential savings from reducing serious medication errors are therefore substantial. Improving medication Safety DoH 2004
Researchers conducting an AHRQ-funded study at Brigham and Women's Hospital and Massachusetts General Hospital found that, on average, ADEs increased the length of stay by as much as 4.6 days and increased costs up to $4,685Bates DW, Spell N, Cullen DJ, et al. The costs of adverse drug events in hospitalized patients. JAMA 1997;277(4):307-11
.
© Great Ormond Street
Medication error reduction PICU
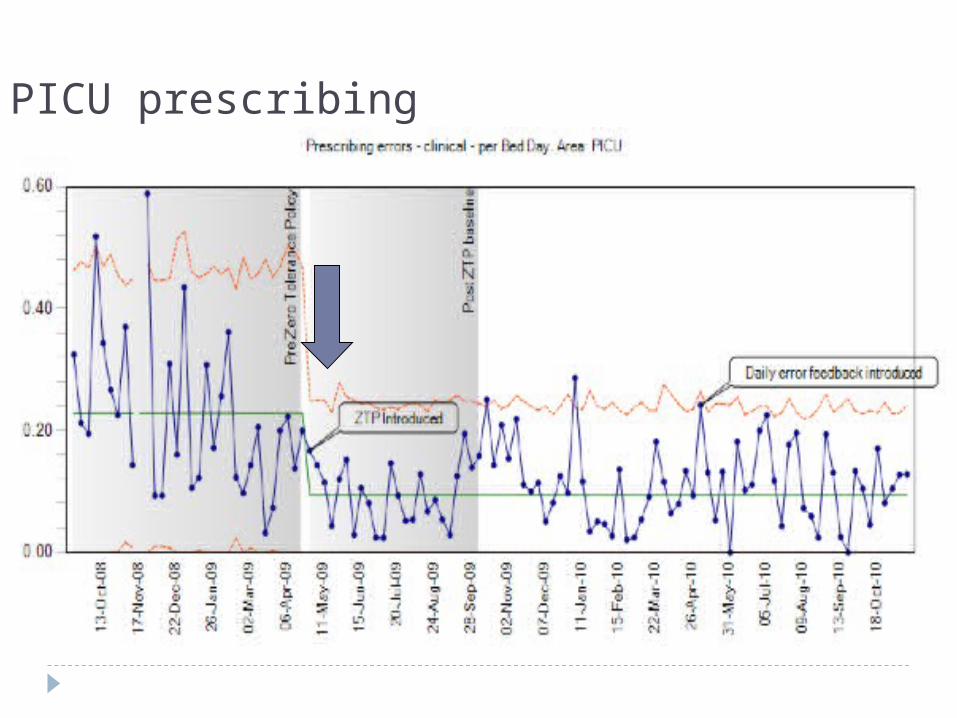
PICU prescribing
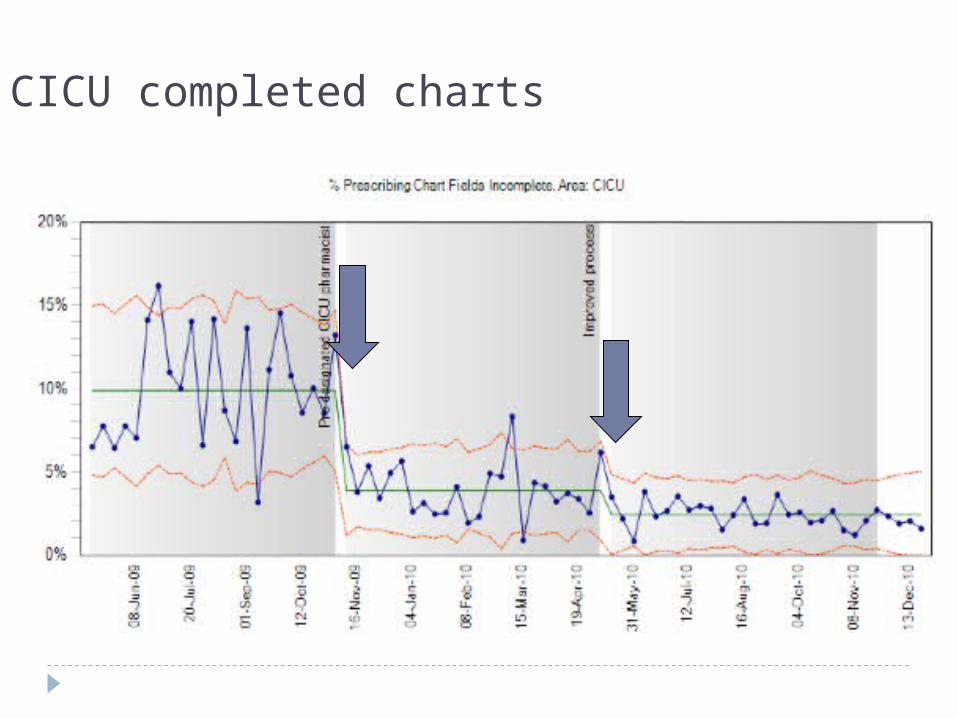
CICU completed charts
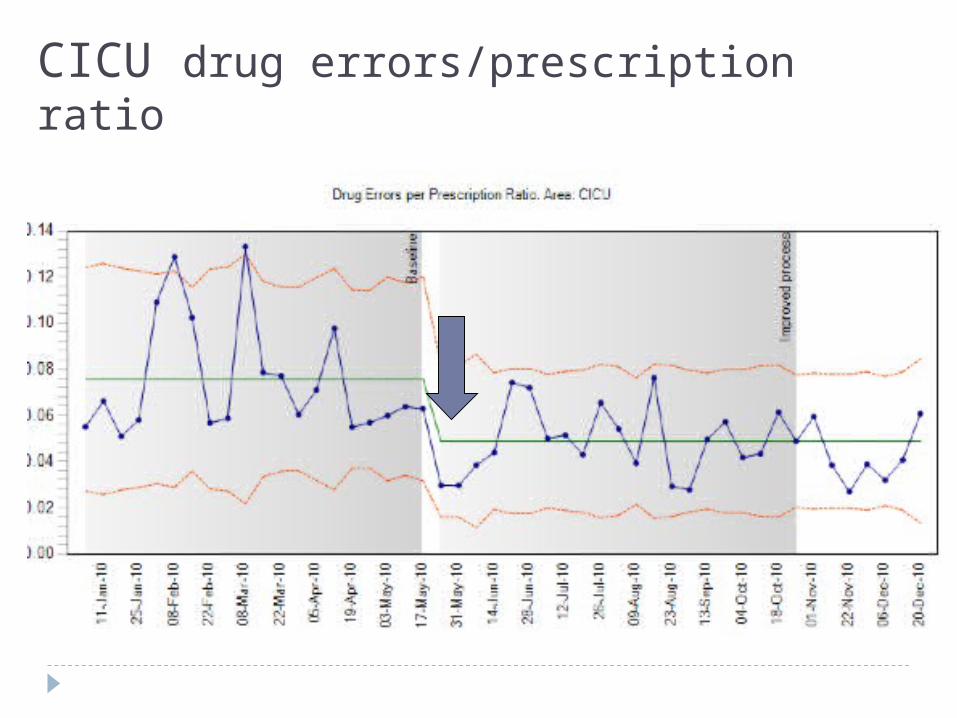
CICU drug errors/prescription ratio
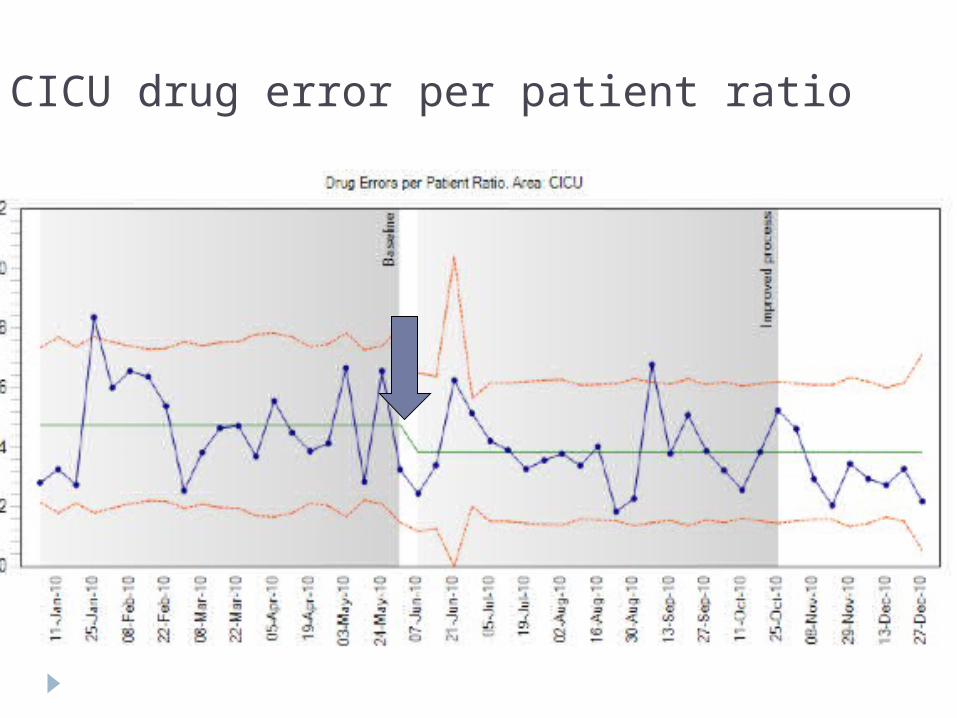
CICU drug error per patient ratio
© Great Ormond Street
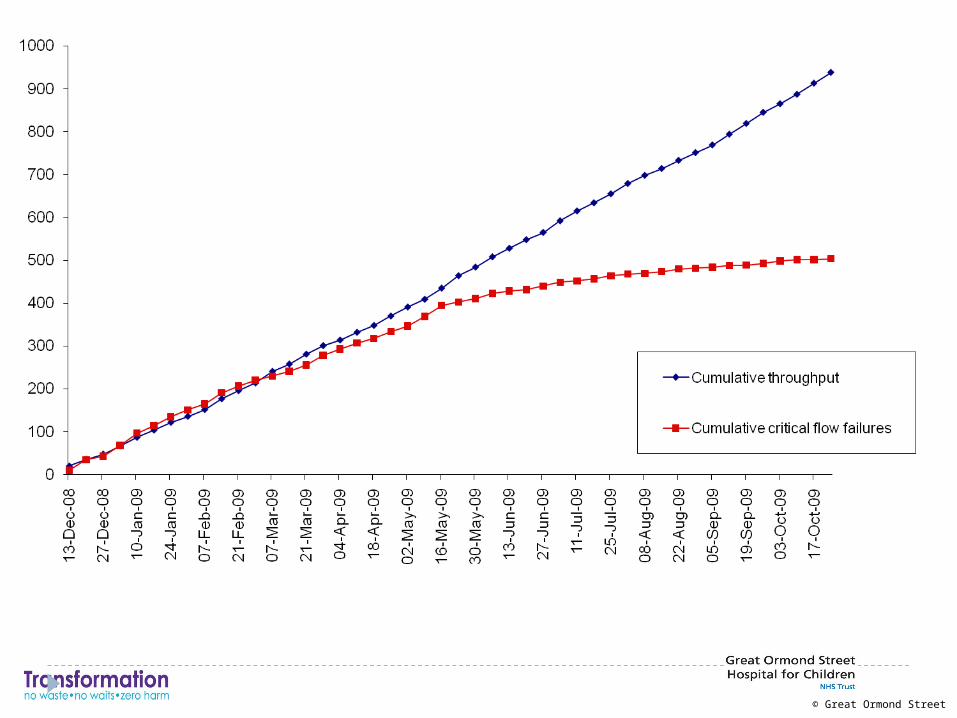
No waits and waste by eliminating variation
Improving productivity by decreasing flow failure Decrease waiting in outpatients
Advance Access Programme Decrease waits for procedures
MRI, interventional radiology etc Decrease waste from variation
© Great Ormond Street
Ways to improve productivity
Reduce length of stay Expand capacity Expand staff Increase bed capacity
and utilisationOr Increase flow by elimination
of variation
© Great Ormond Street
Can we understand variation?
Natural variation – must be actively managed Clinical stress affecting patient safety Stress by variation in professional abilities or teaching
responsibilities affecting both safety and efficiency
Artificial variation – must be eliminated Flow stress affecting efficiency
© Great Ormond Street
Can our health care delivery system become a Toyota product line?
What about Lean on its own?
NoPatients do not arrive at the same rate with the same acuity and providers are of unequal ability.
© Great Ormond Street
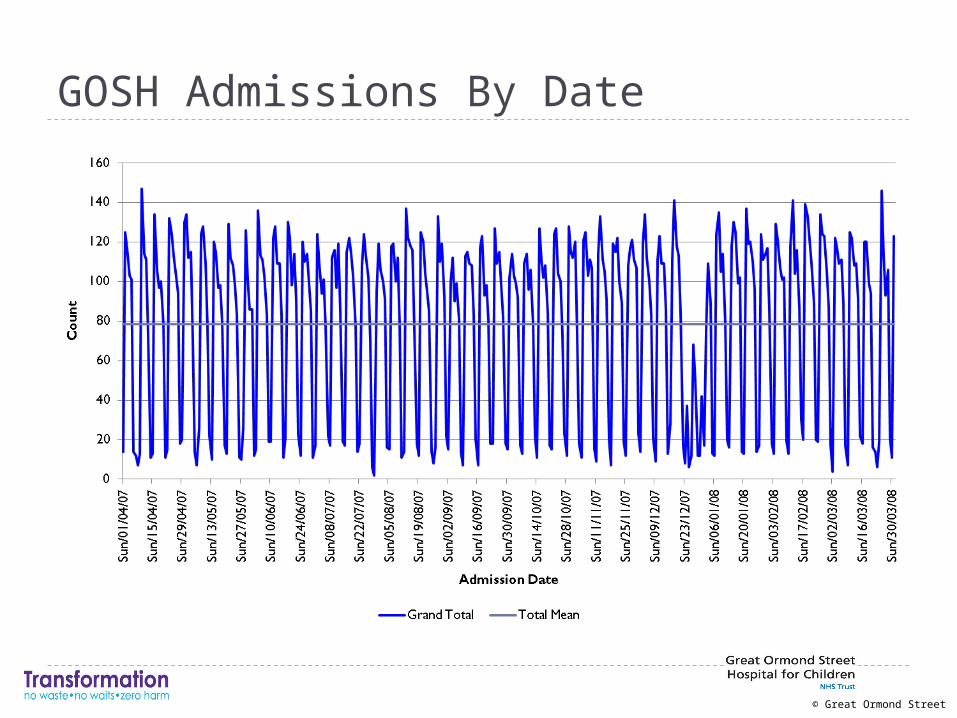
GOSH Admissions By DateProgram for Management of Variability in Health Care Delivery Boston University Health Policy Institute
© Great Ormond Street
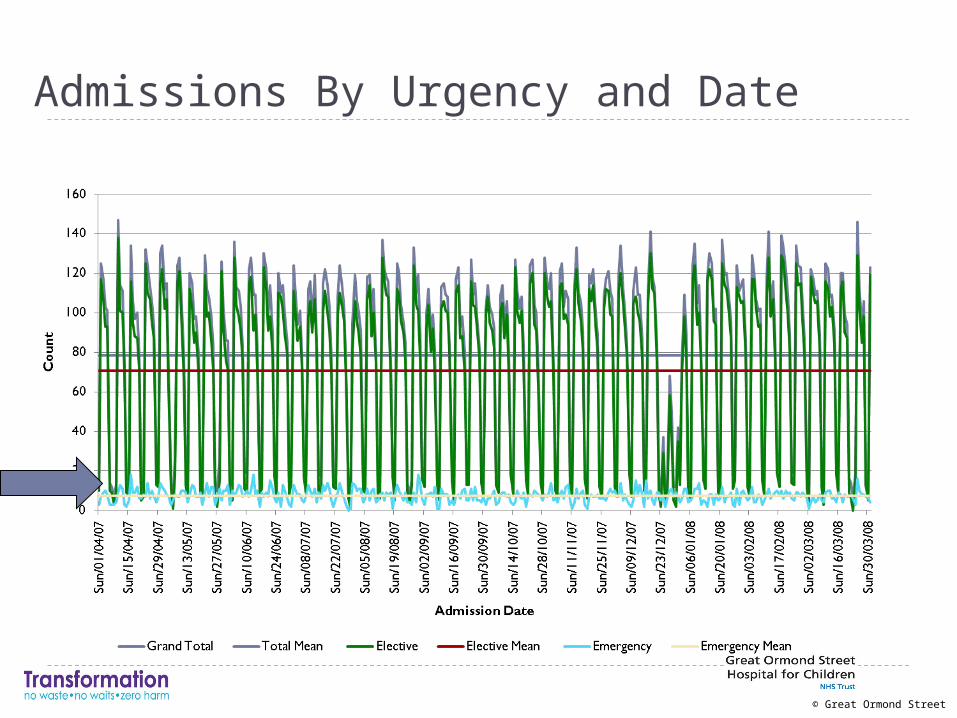
Admissions By Urgency and DateProgram for Management of Variability in Health Care Delivery Boston University
Health Policy Institute
© Great Ormond Street
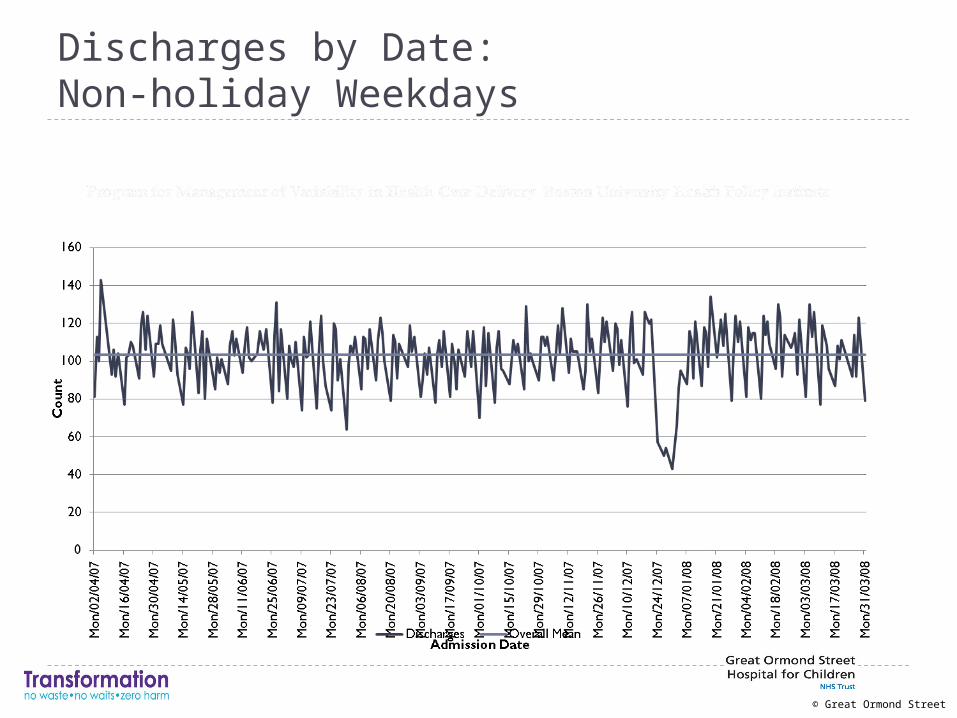
Discharges by Date: Non-holiday Weekdays
© Great Ormond Street
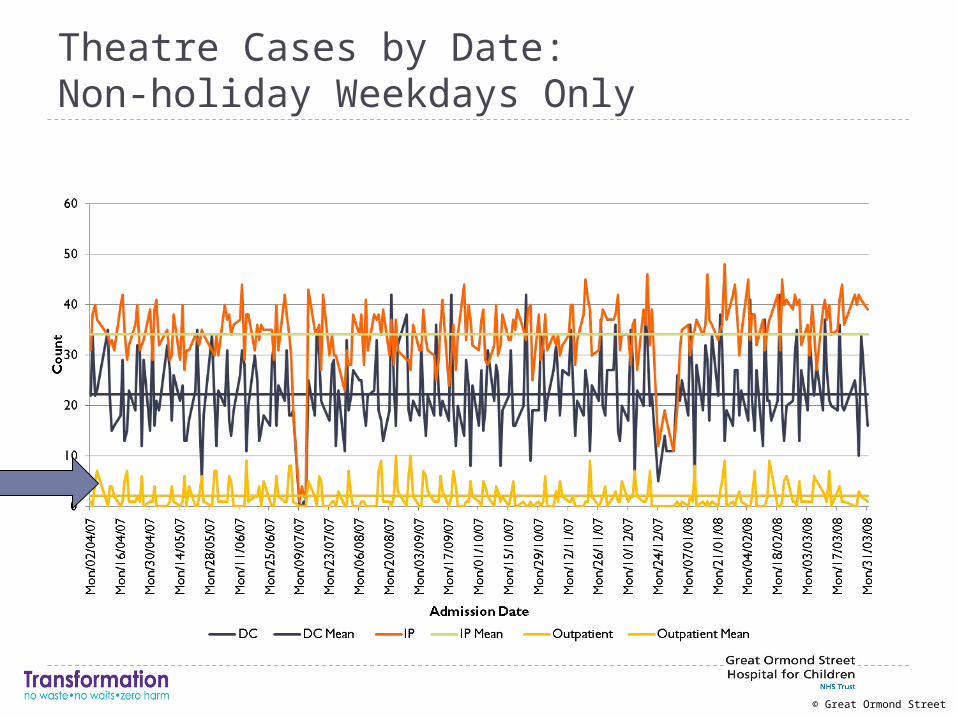
Theatre Cases by Date: Non-holiday Weekdays Only
Program for Management of Variability in Health Care Delivery Boston University Health Policy Institute
© Great Ormond Street
Summary
While day case patients comprise majority of admissions, true inpatients have most impact
Substantial variability in elective admissions Theatre cases comprise large majority
Wasted bed & theatre capacity Improved scheduling of elective admissions,
especially theatre cases, needed
© Great Ormond Street
RecommendationsRecommendations
1. Central management of admissions2. Establishment of a central ‘patient flow team’3. Central management of operationally-relevant
information systems4. Improve collection and reporting of flow data5. Separate emergency and elective beds6. Separate resources for day case and inpatients7. Determine best management strategies for ‘high
utiliser’ patients8. Reconfigure wards into larger units

And how have we responded?
© Great Ormond Street
© Great Ormond Street
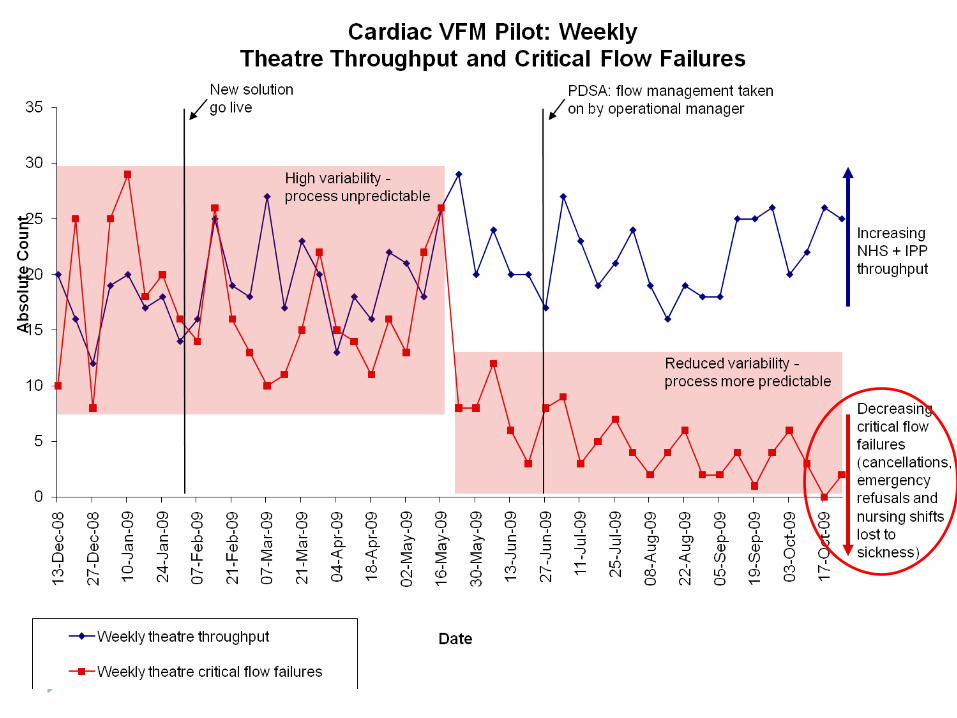
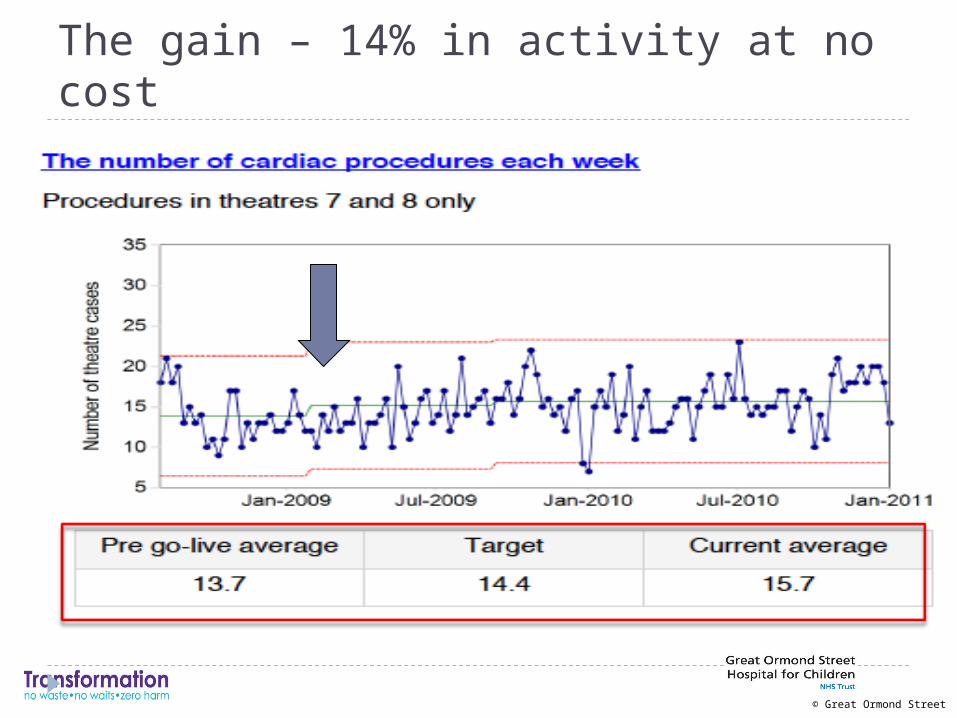
The gain – 14% in activity at no cost
© Great Ormond Street
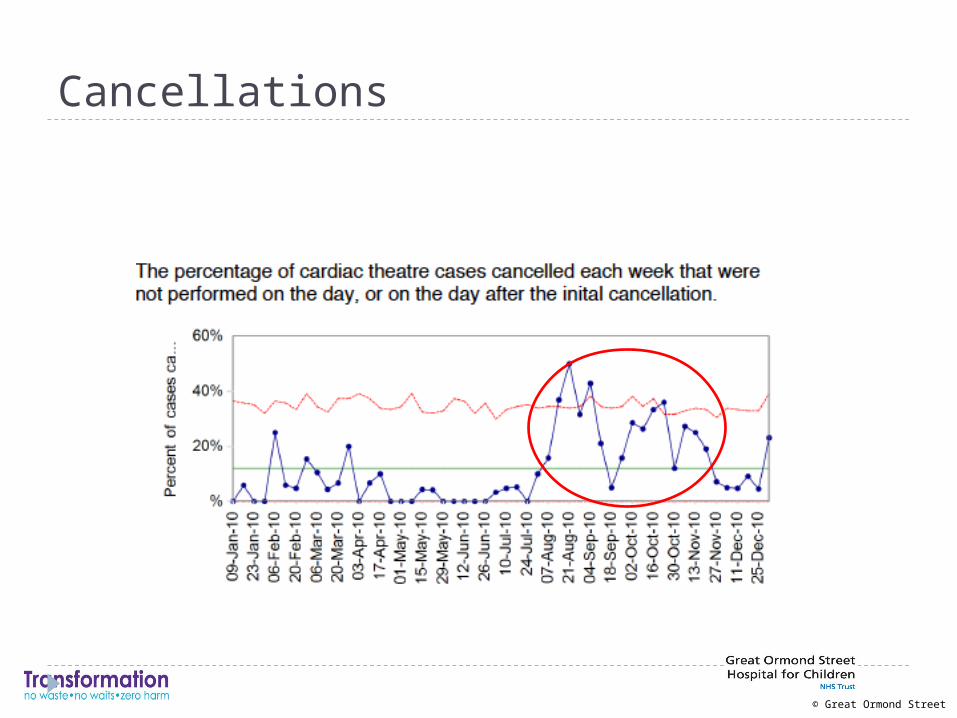
Cancellations
© Great Ormond Street
Patients:
• Reduced waiting time and improved access to care
• Reduced mortality and medical errors
Nurses:
• Reduced overtime
• Reduced workload
Outcomes
© Great Ormond Street
What do we need to do?
Decrease harm – adds value and decreases waste
Eliminate variation – redesign services to do more for less Consider areas where you do not know how to solve the
blocks in the system Emergency room Inpatient beds Diagnostic procedures Operating room Outpatients