Embed Size (px)
Citation preview

Malaria
Anne McCarthy, MD, MSc, FRCPC, DTM&H Professor of Medicine University Ottawa Director Tropical Medicine and International Health Clinic Ottawa Hospital General Campus

Objectives – to review Geographic risk of travelers’ malaria Malaria lifecycle/transmission Methods of prevention – incorporating
Canadian Guidelines Chemoprophylaxis Personal Protection Measures
Symptoms and appropriate triage/referral Self-treatment of malaria

What’s really different for upcoming guidelines??
New format to country of risk Statements about length of time of
exposure in lower risk areas Giving providers latitude to make
individualized recommendations

WHO World Malaria Report 2011
Global Malaria Situation:
Millennium Development Goal – some progress…
3.3 billion at risk ● 106 countries ● 45 within Africa
Cases 81% in tropical Africa
91% deaths SSA
Most severe effects ● Children less 5 years ● Pregnant women

What in the world been happening with Malaria?
● Worldwide there has been a push to control malaria ● Improved access to bed nets ● Improved diagnostics ● Improved therapy
● However we do see resurgence of malaria ● civil unrest, natural disasters and global warming
● Epidemics in areas of previous low endemicity ● increasing falciparum (DR, Jamaica, Bahamas)
● Increasing malaria resistance ● especially in chloroquine resistant falciparum

Malaria in Travelers # 1 life-threatening infection > 20 million at risk Approx. 30,000 acquire malaria/yr
Canadian travelers ● 1 million potentially at risk ● 350-500 cases per year
US travelers ● 1500 cases per year
Mortality (PF): overall 1-4% > 40 yrs 6% > 70 yrs 30% severe >20%

So do we really have to worry about malaria in our travellers? 29 year old lady 3 week journey to Togo and Ghana
No malaria prophylaxis Minimal mosquito prevention measures
Ill on day of return – in bed ? Temp Day 3 at home brother could not get sense
from her on the phone – called a friend... sent RN friend to check things out… called 911

So do we really have to worry about malaria in our travellers?
When she arrives at ER – confused Hgb 78; platlets 32 Parasitemia 30%
Exchange transfusion x 3 days Total 18 units PRBC

Increasing numbers of risk travelers
Young children Pregnant women HIV and other Immune suppressed Long-term expatriate VFR travelers
Risk of malaria in VFR traveler estimated to be 8 x tourists

Malaria management Canadian Malaria Prevention and
Treatment Guidelines www.travelhealth.gc.ca Malaria Branch CDC www.cdc.gov Malaria Hotline 770-488-7788 or 770-488-7100 (after hours) World Health Organization
Treatment Guidelines http://www.who.int/malaria/publications/
atoz/9241546948/en/index.html

US Malaria cases and deaths 1985 – 2008*
Average of 1400 case per year and 5 deaths

2009 data summary USA 1,484 cases of malaria
3 congenital, 3 transplant/transfusion related Region acquisition; n = 987
• 74% AFR (81% W AFR) • 14% Asia (85% SAsia; 46% India) • 10% Americas:
– 61% Caribbean (56% Haiti); 21% S Am (59% Guyana); 17% Cam (67% Honduras)
Species available in 927 (63%) PF 74%; PV 18% PF geographical distribution
• 88% African cases; 73% Americas; 12% Asia; 14% Oceania PV geographic distribution
• 4% AFR cases, 24% Americas, 78% Asia, 86% Oceania
MMWR April 22, 2011 / 60(SS03);1-15

2009 data summary USA
1,484 cases of malaria Time to symptoms
• 16% pre arrival • 84% after arrival • <1 month PF; <1 mo 56% PV
Severity of illness Uncomplicated 85% Severe 10%
Cases Children (< 18 years) 16% > 65 years 5%overall - PF 74%; PV 18% Pregnant women – 19 cases– 2 severe
MMWR April 22, 2011 / 60(SS03);1-15

2009 data summary USA
Use of chemoprophylaxis 25% of US citizens took prophylaxis 66% “appropriate” but 55% non adherent
Reason for travel - for US citizens 70% VFR – visiting friends and relatives 11% missionaries 7% business
MMWR April 22, 2011 / 60(SS03);1-15

So who/what should we be focusing our malaria prevention efforts on??? VFR travellers
but how are you going to reach them??
Education of travellers for proper management of fever illness after return
Children that means their parents

Malaria Cases by species US, 1985-2008

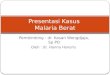
Distribution of Canadian Severe Cases Acquired in Africa 92/108 (85%)
Ghana 14 Nigeria 14 Ivory Coast 6 Congo 6 Mali 4 Uganda 4 Burkina Faso 4 Senegal 4 Tanzania 4 Sierra Leone 4 Guinea 4 Cameroon 3 Burundi 3 Kenya 3
Benin 2 Ethiopia 2 Liberia 2 Mozambique 2 Malawi 1 Gabon 1 DRC 1 Zambia 1 Eritrea 1 Sudan 1 “Africa” 1
* * *
*
*
*
*
*
*
* * *
* *
* * *
* *
* *
*
* *

Malaria No perfect prophylaxis
may alter how and when you present Widespread in the tropics, widespread (R) 3/4 falciparum present in the first month
almost never > 6 months Other malarias - 45% first month
but, 25% have symptoms > 6 months

5 species infect humans: ● Plasmodium falciparum ● Plasmodium vivax ● Plasmodium ovale ● Plasmodium malariae ● Plasmodium knowlesi


Malaria clinical spectrum ● Most fever or flu-like illness ● Fatalities with P falciparum (Pf)
● occasionally with Pvivax - splenic rupture ● Cerebral malaria (Pf) - focal or generalized symptoms ● Hypoglycemia - from disease and treatment
● quinine leads to insulin release ● Risk Acute Respiratory Distress Syndrome (Pf)
● due to capillary leak - need to limit fluids ● Acute renal failure (Pf)
● Not uncommon complication of severe malaria

Malaria diagnosis Smear microscopy
Malaria is present Species Parasitemia Results available within hours
Rapid diagnostic test Malaria is present Results available within minutes
PCR – confirmation only

Malaria diagnosis: issues Average lab does not see many malaria
cases and may not maintain proficiency Choose to batch malaria testing Provide limited services
• Not report species or parasitemia • RDT only
Sends out all malaria tests • Results available days too late
Negative impacts Patient care Surveillance data

Malaria: Problems for North American health care providers ◆ Not seriously considering the diagnosis ◆ Not recognizing fever in a returning
traveler /recent immigrant as a MEDICAL EMERGENCY
◆ Not recognizing malaria as a medical emergency
◆ Not appreciating how quickly a patient can become gravely ill

Multiple Guidelines WHO European UK Australian US CDC CATMAT - Canada

Goals of Malaria Chemosuppression Overall prevention of symptomatic malaria
Main goal - prevention of falciparum malaria, specifically, prevention of falciparum deaths
Requires an Individual Risk Assessment Benefits must outweigh the risks

MMWR 2001;Eurosurveillance 1998;Kain et al CID 1998
Malaria pills don’t work if you don’t take them Shanks
Px US UK Canada None/wrong 84.2% 81% 97% Recommended 15.8% 4% 3%

CATMAT Guidlines 2009
Four (five) components of malaria prevention should be discussed with the traveller (ABCDE):
a. the risk of acquiring malaria b. personal protective measures to prevent mosquito
bites c. chemoprophylactic drugs (where appropriate) d. the need to seek early diagnosis and treatment for
a febrile illness e. educate providers about appropriate management
of febrile traveler

ATV/PG PQ
MQ DOXY CHLOROQUINE ATV/PG
PQ

Mefloquine Cochrane Library 2001; BMJ 1997;315:1412 In RCTs versus placebo 3.6 (1.6-7.6) x chance stop drug <50% for neuropsychiatric AEs
In RCTs versus other active drugs 0.95 (.9-2.6) – not a lot more on mefloquine stop

Mefloquine Efficacy PF, PV >90%
except Thai borders Adverse Events
GI upset Neuropsychiatric adverse events
• severe 1/10,000, mod 1/200 Discontinuation rate 1-5% Longterm safety data available (Lobel)

Mefloquine Lot of publicity – including recent documentary Suicides reported – not related to drug dosing Contraindicated if history of psychiatric illness
Any symptoms of anxiety, poor sleep etc may be harbinger to worse neuropsychiatric adverse events – advise to change
Conclusions still useful, in selected individuals trial of therapy pre-departure

Mefloquine Lot of publicity – including recent documentary Suicides reported – not related to drug dosing Contraindicated if history of psychiatric illness
Any symptoms of anxiety, poor sleep etc may be warning of future worse neuropsychiatric adverse events – advise to change

Mefloquine
Conclusions still useful, in selected individuals trial of therapy pre-departure

Doxycycline Protective efficacy > 90% Contraindicated – pregnancy and kids <8y Adverse events:
GI upset frequent esophogeal ulceration sun sensitivity candida vaginitis
Daily dosing – concern re effectiveness

Doxycycline – long term use Extracted from data on minocycline (Gough BMJ 1996; Gotlieb Lancet 1997)
Have been rare reports of Serum sickness, drug induced lupus, autoimmune hepatitis and fulminant hepatic necrosis

Atovaquone/proguanil Malarone ®
Causal prophylaxis – take 7 days post Daily dosing Expensive Safe in children
CDC and PHAC say safe to use down to 5 kg – adapted from data on safety for treatment

ATV/PG vs MQ Overbosch et al CID 2001
Non- immune travellers; N=1013 (~80% SSA) PE 100% for both (secondary endpoint) AEs ATV/PG MQ Any 71% 76% Rx rel 30% 42%* Neuropsych 14% 29%*
Dreams 7 14 Insomnia 3 13 Dizzy 2 9
D/C rate 1.2% 5%* D/C neuro 0.6% 3.9%

ATV/PG vs Doxy vs MQ vs CQ/PG Schlagenaugh et al BMJ Nov 2003
RCT non-immune travellers < 4 wks N = 623 Endpoints – AEs QoL POMs CQ/PG worst tolerated MQ moderate tolerated, most
neuropsychiatric effects Best tolerated ATV/PG

ATV/PG and underlying disease No adjustment needed for: Elderly Mild to moderate renal impairment Mild to moderate hepatic impairment
Contraindicated in those with severe renal impairment (CrCl < 30 ml/min)

Primaquine (off label use) Efficacy 85-95% for PF and PV Causal prophylaxis Adverse effects - GI upset Contraindicated – G6PD deficiency,
pregnancy Alternative for CRPF areas Possibly for areas with PV

Malaria Chemopophylaxis Summary Chloroquine sensitive areas (very few areas)
CQ Alternative first line agents CRPF areas
Chloroquine resistant areas ATVPG (Malarone) > 5 kg Doxycycline > 8 years Mefloquine – > 5 kg (alternative Primaquine)
Areas with predominantly PV consider (NOTE G6PD) Primaquine
CQ and MQ resistant areas Doxycycline (alternatvie ATVPG/Malarone)

Standby Treatment/ Reliable Supply Medicine Means different things in different
countries EU recommendations many places no Px,
instead carry SBT New term from CDC – reliable supply medicine North America usually reserved for those who
will not take prophylaxis or else will be far from medical care • can self-initiate therapy on way to getting care
Consider for longer trips or those not taking Px • safe and effective therapy in case Dx with malaria

Artemether-lumefantrine*
Not licenced or available in Canada
In US approved for the treatment of uncomplicated P. falciparum – not for severe infections Not approved for use during pregnancy CDC: Prescribed as a reliable supply medicine

Reliable supply/ standby therapy* Higher risk of malaria - may be prescribed a full
malaria treatment course to carry with them HOWEVER need to understand
If ill, seek immediate medical attention for diagnosis Can then treat with the full treatment course they are
carrying with them
Avoids the risk of inappropriate drug-drug interactions
Avoids counterfeit medicines Does not deplete local supplies of medicines
Malarone and Coartem are now options

Personal Protection Measures
● Insecticides ● Insecticide impregnated bednets save more than a half
million lives annually ● Safe in pregnancy and for small children ● Insecticide treatment of clothing
● DEET ● Remarkably safe profile, with more than 200,000,000
utilizations annually ● Concerns about DEET formulations leading to
encephalitis NOTsubstantiated in prospective cohorts

Clinical Cases

*Visiting Friends and Relatives
Family trip to Ghana VFR* traveller – 2nd generation Canadian
parents in Canada 14 years 7 month old girl
19 May – 8 June 2006 Saw Travel Medicine Provider, “Too young for Px” No chemoprophylaxis No Bednet Did use DEET/OFF

What would you advise???

Family trip to Ghana Well in Ghana Fever onset 1-2 days after return Temps to 394, lethargy, poor oral
intake, decreased urinary input Saw pediatrician in office – “viral” Next day to walk in clinic then ER


Hospital management Hyperasitemia (26% to 35%) Consideration of exchange transfusion Marked anemia – Hgb 81 -> 65; required
transfusion Admitted to ICU for observation

So what can we learn? Prevention is key
Malarone (atovaquone/proguanil) – down to 5 kg Mefloquine – down to 5 kg Doxycycline - contraindicated DEET Insecticide treated bed nets/clothing

What else? Early diagnosis and treatment
Parents/travellers need to be advocates for their own and their children’s health
Fever or flu-like illness especially within 3 months of travel • need to seek medical attention • need to have blood smears to rule out
malaria Preferable to go to hospital where lab
tests are available and reported

Take Home Messages Malaria is an important risk for many
travelers Prevention is key
Assessment of risk of exposure Prevention of anophelene bites Assessment of appropriate prophylaxis *** Fast and appropriate medical care in
event of malaria

Now you can prevent some cases…

Mr D is a 28-year-old male. He will be travelling for 12 weeks, backpacking with a friend to Kenya, Tanzania, Uganda and Zambia. He is in good health, has no allergies, and is not on any medications. He will be travelling during the months of February, March, and April.

What would you recommend for malaria prevention?

What would you recommend for malaria prevention?

Africa WHO: Canada/CDC: EU:
Actually in agreement – this is a high risk area for CRPF.
All advise ATV/PG; Doxycycline; Mefloquine (Primaquine)

Would you give him stand-by treatment/ reliable supply?

Would you give him stand-by treatment (SBT) – reliable therapy?
Will he be able to get to medical attention if ill? Will he be able to get safe drugs for treatment? Will drug other than his prophylaxis be available? What would you recommend for him to do about
malaria prevention after he is treated for an episode of malaria??

His “friend” is actually his wife and figures that this will be a good, relaxed time to try to get pregnant.
What would you advise her about malaria prevention?

Recommendations for Pregnancy
Travel to malaria risk area during pregnancy not recommended
Risk for Mom and Babe Limited to CQ (no use in Africa) and
MQ (some recommend only after the first trimester)


The Jones family are off to the Dominican Republic to visit a resort for a two week well deserved vacation. (Marg 33, Joe 34, Sally 5, Mikey 3)
What are you going to recommend about malaria prevention?

The Jones family …

John and Tim are about to embark on an adventure through South East Asia. They have already blown the bankroll and plan to take in Cambodia, Vietnam, Thailand, and Loas over 12 weeks.
what are you going to recommend??

South East Asia – Malaria Recommendations

South East Asia – Malaria Recommendations

South East Asia – Malaria Recommendations

Bed nets?
What do you do for individuals in and out of risk areas?
South East Asia – Malaria Recommendations


34 year old man on eco-adventure in Borneo
What would you recommend for malaria prevention?

Area of CRPF
BUT ALSO Potential risk of leptospirosis with flooding and also risk for rickettsiosis

? IMPORTANT RESOURCES:
• Health Canada (www.travelhealth.gc.ca) [CATMAT] • US CDC (www.cdc.gov) • World Health Organization (www.who.int) • International Society of Travel Medicine (www.istm.org)