Embed Size (px)
Citation preview

J. clin. Path. (1954), 7, 231.
MALIGNANT GIANT-CELL SYNOVIOMA OF PHALANXBY
C. H. G. PRICE AND J. C. VALENTINEFrom the Medical Research Laboratory, Department of Pathology, University of Bristol,
and the Department of Pathology, Bedford General Hospital
(RECEIVED FOR PUBLICATION MARCH 4, 1954)
Primary sarcoma of a phalanx is uncommon.Osteogenic sarcoma, fibrosarcoma, and chondro-sarcoma have been infrequently reported, but asearch of the literature has not revealed any previousrecord of a primary malignant synovial tumourarising endosteally, although benign synoviomataare fairly common in the digital soft tissues.The unusual site of origin of the tumour des-
cribed here is suggested both by the clinical andradiological findings. Invasion of bone by synovialtumours of digits and other sites has been reportedby Wright (1952), Fletcher and Horn (1951), andby others, but in such examples the involvementgenerally appears to be either the result of pressureatrophy or due to direct extension of a parostealgrowth. Certain primary expansive tumours ofphalanges and metacarpals have been described(vide infra), which characteristically produce a richosteoid matrix. These are usually classified withosteogenic fibroma ofbone and present a histologicalpicture which in some ways resembles the less cellularparts of the tumour reported here.
Case HistoryMrs. N. F., aged 35, a housewife (BTR/51 1), in March,
1952, fell from a chair while hanging out washing. Shefell on to the outstretched right hand, injuring the fifthfinger. Before this there was no evidence of any bonyor arthritic changes. Following the accident, the fingerbecame painful and swollen but no medical advice wassought. As the symptoms were progressive, the patientconsulted her doctor in July, 1952, who referred her forsurgical advice. On examination at that time there wasa deformity of the fifth right finger, with a tender swellingof the middle phalanx region.X-ray examination on July 19, 1952, showed an
extensive cystic swelling of the intermediate phalanx,with expansion and marked thinning of the cortex (Figs.1, 2a). There may have been a former fracture of thephalangeal shaft in the antero-medial region. Apartfrom a very slight periosteal reaction, there was no signof any new bone formation. There appeared to beperforation of the thinned cortex antero-externally. Theother two phalanges were normal, as also were radio-
graphs of the skull and other bones. The finger wasamputated at the metacarpo-phalangeal joint in Sep-tember, 1952.
FIG. '.-Radiograph of right hand on July 1!well-marked expansion and thinning of thephalanx. By September the transverse boreduced to a thin bundle of collagen fibres.
Amputation Specimen.-The finger when received hadalready been partly cut sagittally. It showed an irre-gular spheroidal mass of solid pale yellow-white tissueapproximately 1.5 x 1 cm. occupying the middle segmentof the finger in place of the intermediate phalanx (Fig.2b). This solid tissue cut easily with the knife and wasof a uniform rubbery consistency. It was fairly wellcircumscribed, more especially upon the volar aspect,and consisted of a main mass formed of a number of
on 4 May 2018 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.7.3.231 on 1 August 1954. D
ownloaded from
C. M. G. PRICE and J. C. VALENrINE
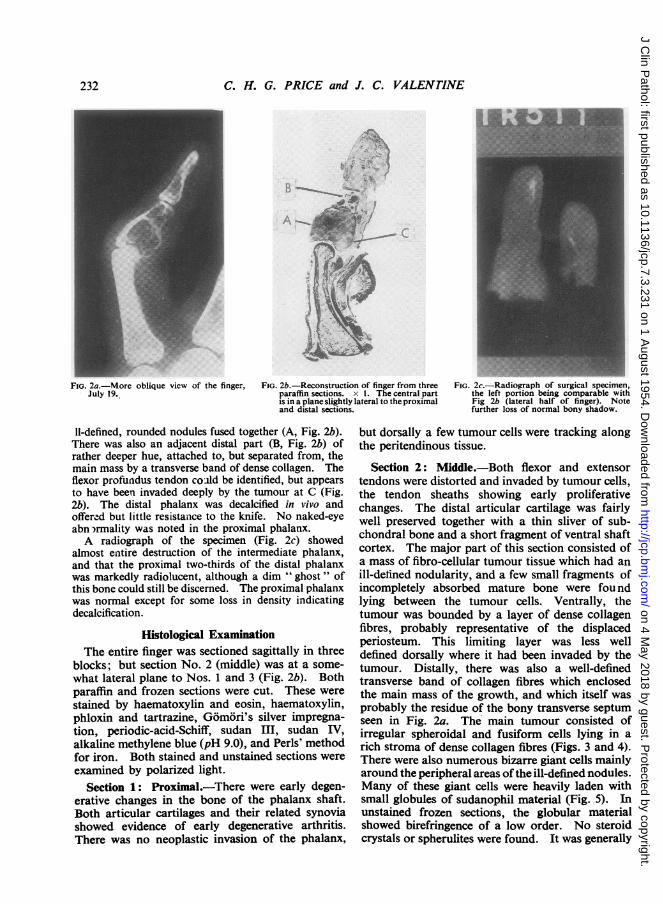
FIG. 2a.-More oblique view of the finger,July 19.
FIG. 2b.-Reconstruction of finger from threeparaffin sections. x 1. The central partis in a plane slightly lateral to the proximaland distal sections.
FIG. 2c.-Radiograph of surgical specimen,the left portion being comparable withFig 2b (lateral half of finger). Notefurther loss of normal bony shadow.
11-defined, rounded nodules fused together (A, Fig. 2b).There was also an adjacent distal part (B, Fig. 2b) ofrather deeper hue, attached to, but separated from, themain mass by a transverse band of dense collagen. Theflexor profundus tendon coAld be identified, but appearsto have been invaded deeply by the tumour at C (Fig.2b). The distal phalanx was decalcified in vivo andoffered but little resistance to the knife. No naked-eyeabn rmality was noted in the proximal phalanx.A radiograph of the specimen (Fig. 2c) showed
almost entire destruction of the intermediate phalanx,and that the proximal two-thirds of the distal phalanxwas markedly radiolucent, although a dim " ghost " ofthis bone could still be discerned. The proximal phalanxwas normal except for some loss in density indicatingdecalcification.
Histological ExaminationThe entire finger was sectioned sagittally in three
blocks; but section No. 2 (middle) was at a some-what lateral plane to Nos. 1 and 3 (Fig. 2b). Bothparaffin and frozen sections were cut. These werestained by haematoxylin and eosin, haematoxylin,phloxin and tartrazine, Gomori's silver impregna-tion, periodic-acid-Schiff, sudan III, sudan IV,alkaline methylene blue (pH 9.0), and Perls' methodfor iron. Both stained and unstained sections wereexamined by polarized light.
Section 1: Proximal.-There were early degen-erative changes in the bone of the phalanx shaft.Both articular cartilages and their related synoviashowed evidence of early degenerative arthritis.There was no neoplastic invasion of the phalanx,
but dorsally a few tumour cells were tracking alongthe peritendinous tissue.
Section 2: Middle.-Both flexor and extensortendons were distorted and invaded by tumour cells,the tendon sheaths showing early proliferativechanges. The distal articular cartilage was fairlywell preserved together with a thin sliver of sub-chondral bone and a short fragment of ventral shaftcortex. The major part of this section consisted ofa mass of fibro-cellular tumour tissue which had anill-defined nodularity, and a few small fragments ofincompletely absorbed mature bone were foundlying between the tumour cells. Ventrally, thetumour was bounded by a layer of dense collagenfibres, probably representative of the displacedperiosteum. This limiting layer was less welldefined dorsally where it had been invaded by thetumour. Distally, there was also a well-definedtransverse band of collagen fibres which enclosedthe main mass of the growth, and which itself wasprobably the residue of the bony transverse septumseen in Fig. 2a. The main tumour consisted ofirregular spheroidal and fusiform cells lying in arich stroma of dense collagen fibres (Figs. 3 and 4).There were also numerous bizarre giant cells mainlyaround the peripheral areas ofthe ill-defined nodules.Many of these giant cells were heavily laden withsmall globules of sudanophil material (Fig. 5). Inunstained frozen sections, the globular materialshowed birefringence of a low order. No steroidcrystals or spherulites were found. It was generally
232
on 4 May 2018 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.7.3.231 on 1 August 1954. D
ownloaded from

MALIGNANT GIANT CELL SYNOVIOMA OF PHALANX
FIG. 4.-Cellular detail of main tumour mass. The cells are mainlysmall and spheroidal or polyhedral, together with a few bizarregiant cells. There is a well-developed collagen stroma. Haema-toxylin and eosin, x 370.
observed that the sudanophil material was minimalor absent from those giant cells showing mitosis orcytoplasmic vacuolation. The dense stromal col-lagen showed typical birefringence and its formmainly suggested new fibre formation by the tumourcells rather than residual collagen matrix from
FIG. 6.-Predominantly giant celled area from edge of main tumourmass. The cytoplasm of the paler cells is stained mainly withtartrazine, and shows marked vacuolation. Haematoxylinphloxin, and tartrazine, x 210.
destroyed bone, cartilage, or tendon. In certainareas there was a suggestion of a trabeculararrangement.
Lying between the collagen fibres were numerousround or oval " clefts," in some instances forminglarger spaces by confluence. It had originally beenthought that many of these were fat cells, but infrozen sections these spaces were again empty and
233
on 4 May 2018 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.7.3.231 on 1 August 1954. D
ownloaded from

C. H. G. PRICE and J. C. VALENTINE
devoid of sudanophil material. Neithernor frozen sections stained with methylenby the periodic-acid-Schiff method was axfound of a mucinous content in theseone can only conclude that they must
*l'5YxO Aj
)
e~ e; ;,tt+
FIG. 7.-Tumour tissue from distal outlying nodule shous giant cells, some simulating atypical osteoclasa few small spindle cells present, but only scanty strntoxylin and eosin, x 370.
*.. Xs .1
_ .* :^o.t_ s s.Yi __ w ssdi_ wOIIF allS _ 4 *
se . #
w *Rew'sbt {Xj,a
.s is,pr
FIG. 8.-Bizaffe vacuolated giant cells which are theponent of the distal outlying nodule. Haematoand tartrazine, x 240.
in paraffin tained a water-miscible fluid which had been lostie blue and into the formol fixative.ay evidence It was possible to observe the manner in whichclefts, and these small clefts were formed. The earliesthave con- evidence was to be found in the foamy cytoplasm of
the larger multinucleated giant cells. Small vacuolesappear to form which grow, and a number of clefts
* of moderate size were noted in which there was stilla thin rim of granular cell cytoplasm, with thedeeply stained pyknotic nuclei compressed andaggregated to one side (Figs. 4 and 6). Occasion-ally, such clefts or vacuolated giant cells weresurrounded by a thin phloxinophil rim of materialwhich showed feeble birefringence. This latterfeature is probably due to protein crystallization ata gel/fluid interface, and is essentially similar to theearly radial zone of osteoid which may be seen
R ' around the periphery of the mature cartilage cells ofan orderly column of epiphyseal chondrocytes, andmay represent the earliest sign of endochondral
* -% ossification. It was generally noted that the giantcells which showed this cytoplasmic vacuolationstained metachromatically a pale mahogany colour
v^ with the phloxin-tartrazine staining, whereas thosegiant cells in which there were no vacuoles weretypically phloxinophil. (These tissue clefts aregenerally typical of synovioma, and may be numer-ous and large even in the absence of any giant cells.
iowing numer-sts. There are Obviously, the manner of cleft formation indicatedoma. Haema- here may not be the only one; on the contrary, the
modified cell structure seen in the central fibrousareas of this tumour suggests that maturation of thegiant cells, with concomitant morphological changes,is associated with a well-marked collagen stromaand numerous clefts. Hence, in certain synovio-mata these latter features may be the more
W* ^ prominent.)There were also quite a number of larger spaces
* ^^- lined with flattened cells whose appearance sug-gested dilated lymphatics. There was little or nosudanophil material lying between the stromalcollagen fibres, nor yet between the fibres of thelimiting collagen bundles and the adjacent tendons.This latter feature is usually well marked in giant-cell tumours of tendon sheaths.
In the cells of the main tumour mass, mitoses*tv4. were numerous and often abnormal. The mitotic
ratio (Price, 1952) was 97 to 1, and in many high-power fields 3% or more of the cell nuclei were in
* ;^ mitosis. No necrosis was seen, and no evidence> ;*" found of any new bone formation in the collagen
matrix, even in the denser areas where it resembledosteoid. Many of the giant cells were multi-
main cell com- nucleated, and transitional forms were noted to be)xylin, phloxin, fairly typical osteoclasts (Figs. 6 and 7).
234
0 W.., ..
0 It
'o. :4^#-.- ... - A-.::.
on 4 May 2018 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.7.3.231 on 1 August 1954. D
ownloaded from

MALIGNANT GIANT CELL SYNOVIOMA OF PHALANX
FIG. 9.-Scanty reticulin network of distal outlying nodule of tumour.This appearance was also characteristic of the peripheral partsof the main tumour mass which were predominantly giant celled.Gomori silver method, x 190.
\ ...-.. - 9 *..
FIG. 10.-Area of degeneration of cartilage matrix at the edge offragment of proximal articular cartilage of intermediate phalanx.toxylin and eosin, x 46.
The distal part of the tumour (Fig. 2b) lay inthe concavity formed by the residue of the head ofthe phalanx. It consisted almost entirely of atypicalmulti-nucleated giant cells similar to those of theperi-nodular areas described above (Fig. 8). Thesecells mainly showed marked cytoplasmic phloxino-philia, with five to 10 irregular pyknotic or vesicular
Fie. 11.-Area of tumour near residue base of intermediate phalanx.There are a number of large complex spaces lined by flattenedcells suggesting a synovial structure. Haematoxvlin and eosin,x 180.
nuclei. In many cells the deeply stainingirregular nuclei were indistinct and con-joined, an appearance suggesting eitherincomplete separation, atypical nuclearlobation, or fusion of an aggregated massof the smaller nuclei observed in othercells. Nucleoli were, in general, indistinct.Many of the cells resembled atypicalosteoclasts and showed coarsely granularcytoplasm, a few having small vacuoles.Mingled with these cells were smallernumbers of spheroidal and fusiformcells mostly related to the small bloodcapillaries. The intercellular stroma wasscanty, consisting of a few reticulin andcollagen fibres, together with a smallamount of amorphous collagen (Fig. 9).Occasional mitoses were seen but werefar fewer than in the main tumour mass.Three main residual fragments repre-
sented the proximal articular cartilageof the intermediate phalanx. Theseshowed a thinned shell of old sub-
chondral bone. The cartilage was degenerate,and there were areas of amorphous granularmaterial apparently derived from the disintegratedjuxta-osseous zone of the articular cartilage (Fig. 10).The granular debris was isotropic, strongly phloxino-phil, did not stain metachromatically with methyleneblue, but showed a strongly positive reaction with
235
, -- ..k .I %,-1
1.
on 4 May 2018 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.7.3.231 on 1 August 1954. D
ownloaded from

C. H. G. PRICE and J. C. VALENTINE
the periodic-acid-Schiff method. Surrounding thismaterial was reactive tissue, including a few cells ofosteoclastic type. No neoplastic cartilage was foundanywhere in the tumour. The synovium of theproximal interphalangeal joint showed early villo-nodular changes but no iron-containing or otherpigment was found. In the vicinity of these car-tilaginous fragments were a number of largebranched tissue spaces lined with a layer of cellssimulating normal synovium (Fig. 11). Deep tothis surface cell layer were numerous tumour giantcells. It is difficult to be certain whether this repre-sented invasion of displaced joint synovium by thetumour, or whether the structure was proper to thenew growth. A close examination of the branchedspaces suggested a relationship to the larger onesmentioned above, which had been regarded asdilated lymph spaces.
Section 3: Distal.-The bone and cartilage of thedistal phalanx showed degenerative changes butwere not invaded by tumour cells.
Comment
The tumour described here appears to have adouble morphology: (1) areas, mainly giant celled,with very scanty stroma (Figs. 6 and 8); (2) otherparts, usually central, showing fewer giant cells butwith fairly numerous smaller spheroidal and fusi-form cells associated with numerous small tissueclefts and much tumour collagen or osteoid (Figs. 3and 4).The cell pleomorphism, the degree of mitotic
activity, and the invasiveness indicate malignancy,and although apparently of endosteal origin, thetumour should be regarded as a synovial sarcomaof giant-cell type.The osteoid-forming expansive tumour of a
metacarpal bone reported by Jaffe and Mayer (1932)may have had a similar origin and be closely relatedto the one reported here. The former, however,consisted mainly of spindle and spheroidal cellsproducing much trabecular osteoid (" coarse, irre-gular decussating, fibres which stained like colla-gen"). This osteoid was partly calcified, partlyossified. These authors mention the completeabsence of tumour giant cells and relate theirtumour to the " osteoid chondroma" of Virchow(1863) also reported by others, mainly in theGerman literature. By virtue of the ability of sucha tumour to form osteoid and/or bone the malignantcounterpart would naturally fall within the broadclass of osteogenic sarcoma. Jaffe and Mayerexpress the opinion, moreover, that had surgicalremoval of this growth and the metacarpal bone
been long delayed it would have undergone malig-nant changes and have developed into true osteo-genic sarcoma. Such a view is conjecture basedupon experience and judgment, but nevertheless itimplies that the osteoid-producing tumour was tobe regarded as a presarcomatous lesion. Lichten-stein (1952), who mentions this particular tumour inhis chapter on " Osteogenic Fibroma of Bone,"comments further upon the rarity of this type, andrelates such neoplasms to the bones of the handand foot in particular. He also points out theirslow rate of growth and characteristic bone expan-sion.
Irrespective of its malignancy, the present tumourappears to be able both to produce and destroyosteoid, the change in function being accompaniedby modified cell morphology as seen in the twoforms noted above. It is of interest to note thatthe intracellular sudanophil material appears in thecollagen-destroying giant cell areas, while, on thecontrary, it is generally absent in the more centralareas of dense collagen stroma, smaller cell size,cytoplasmic metachromasia, and tissue cleft forma-tion. It seems probable that with further matura-tion of the stromal collagen of these central areassome degree of ossification would have taken place.The nodular appearance of the tumour (Fig. 2b),while not well defined, is very similar to that depictedin synoviomata by Wright (1951); in fact, thisauthor's low-power photomicrograph (Fig. 376,Wright, 1951) is a very close image. In Wright'sseries of 57 benign giant-cell synoviomata of fingersand toes there is no mention, however, of invasionand expansion of the adjacent bones. His paperdoes illustrate the typical pressure atrophy ofadjacent bone which may be caused by a benigngiant cell synovioma especially when occurring inthe foot, but is unusual in the finger growths. Thislatter point is also made by Coley (1949), and others.Nevertheless, malignant synoviomata, of whichabout one half occur around the knee, not infre-quently erode and destroy adjacent bone but donot usually cause cortical expansion.The recurrent synovioma of the finger described
by Wright (1949) shows some histological featuresin common with the present tumour, but in itsrecurrent malignant form seems to have been amore cellular growth, predominantly of spheroidalcells with relatively scanty stroma. This latterform has been seen in two other cases in the BristolBone Tumour Register collection (BTR/7 andBTR/426). The latter recurred eight months aftersurgical excision.The case reported by Berger (1938) is of great
interest, since it was essentially a fibrosarcoma with
236
on 4 May 2018 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.7.3.231 on 1 August 1954. D
ownloaded from

MALIGNANT GIANT CELL SYNOVIOMA OF PHALANX
areas suggesting typical synovioma. The reverseof these conditions has also recently been seen in atumour from the knee region by one of us in a managed 31 (BTR/597). The tumours reported by DeSanto, Tennant, and Rosahn (1941) are describedas of mixed cellular structure, showing polyhedraland spindle cells with foci of numerous giant cells.Their patient (No. 1 1) died with terminal pulmonarymetastases.
Fletcher and Horn, in describing the features ofbone involvement by giant cell synovioma, mentiondestruction of bone by erosion with subsequenttumour growth within the marrow cavity. Theradiographs illustrated by these authors certainlyshow well marked focal osteolysis with corticalperforation, but only very questionable evidence ofcortical expansion (Case No. 1). In their reportedcases there was an extra-osseous soft tissue tumourin three instances (Nos. 1, 7, and 8), the radiologicalappearances clearly suggesting invasion of bonefrom without. Erosion of adjacent bone ends iswell shown in the radiograph of their Case 2described in this series.Vermooten (1925) has reported a benign central
osteolytic phalangeal tumour under the term" xanthosarcoma." This was described as havingbeen of a bright yellow cast, and contained numbersof " foamy" cells together with a few giant cellsintermingled with the fibrous stroma. In additionto the central area of marked bone destructionthere were a number of small cortical erosions, anda soft tissue tumour. These findings, in the lightof the relevant case history, suggest bone invasionfrom without, the tumour being probably a giantcell synovioma with an unusually large "foamy "
cell component.Clark (1952) reported an osteogenic sarcoma of
phalanx, which appears to have been primarily afibrosarcoma with evidence of both osteolytic andosteoblastic activity. It appears to have invadedthe distal and intermediate phalanges from without,and the history and published skiagrams suggest aparosteal origin.
Histogenesis.-King (1952) rightly draws attentionto the insecure basis of the presumed origin ofsynovioma. Tumours showing the structure ofsynovioma but unrelated to anatomical synoviumhave also been reported by Fisher (1942), Briggs(1942), and by Haagensen and Stout (1944). Thehistogenesis of these atypical growths can be opento only two explanations: (1) origin from heterotopicsynovium, or (2) origin from pluripotential mesen-chymal cells.
Appearances suggest that the giant cells of thepresent tumour are associated with destruction of
collagen, being related functionally and morphologi-cally to osteoclasts. In a paper on the StrangewaysCollection, Lawford Knaggs (1932) briefly describedthe formation of osteoclasts from cells of degeneratebone and cartilage, changes which have also beenseen by one of us. Furthermore, in the articularcartilage of a rat, which was invaded by a methyl-cholanthrene-induced fibrosarcoma, the chondro-cytes were greatly enlarged and granular, closelysimulating many of the giant cells seen in thisphalangeal tumour. Moreover, in view of themutations of cell form which may be seen in activecallus, it is not surprising that wide variation mayoccur in cell differentiation in mesenchymal tumoursof a similar origin. From these considerations, thesecond alternative of an origin in pluripotentialcells would seem preferable. There were no featuresin the present tumour to support the assertion ofFoster (1947), who suggested a vascular origin forgiant-cell synovioma.As a corollary to King's morphological classifica-
tion of synoviomata, one may perhaps borrow byanalogy the classification applied by Meyerdingand Jackson (1950) to giant-cell tumours of bone,with reference to the whole group of synovialtumours (the term " synovial " is here used in adescriptive rather than a histogenetic sense), namelybenign, malignant (a) malignant ab initio and(b) showing delayed malignancy, which maypossibly be associated with such factors as trauma,sepsis, surgical intervention, and/or irradiation.
Subdivision in this manner overlaps the classifica-tion suggested by Stevenson (1950), who separatedgiant-cell synovial tumours into two groups on thebasis of presence or absence of concomitant generalmetabolic changes.The more slowly growing benign synoviomata not
infrequently show some atypical mesenchymaldifferentiation, often in the form of dense collagen(simulating osteoid), myxoid tissue, or occasionallyislets of cartilage. The in vitro tissue culturemethods applied to three synovial sarcomata byMurray, Stout, and Pogogeff (1944) yielded resultsinterpreted as representing two main tissue forms,synovial and fibroblastic, but it was uncertainwhether the latter may not have arisen from reactive,vascular, or other mesenchyme included in thetumour tissue taken for culture. Whatever may bethe true explanation, the fibroblast element may atleast be considered as having a potential ability todifferentiate in many ways under a suitable stimulus.With the disordered metabolism ofmore aggressive
growth, as in malignancy, a wider stromal differen-tiation may be expected and appears as sarcoma,which morphologically may take any of the forms of
237
on 4 May 2018 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.7.3.231 on 1 August 1954. D
ownloaded from

C. H. G. PRICE and J. C. VALENTINE
synovial sarcoma of the more usual classic pattern,reticulo-sarcoma, fibrosarcoma, osteogenic sarcoma,chondrosarcoma, malignant giant-cell tumour, ormixed tumours in which the various cell and stromaltypes are intermingled.One may from this assertion then perhaps pose
the question, If sarcoma is related to the existenceof a preceding benign tumour, why the very markeddisproportion of the malignant and benign forms ofneoplasia in the digits where the former are veryrare and the latter relatively common ? Oneobvious feature with tumours of the hand and footis the urgency of symptoms, which lead to earlytreatment. In other anatomical sites, the propor-tion of malignant forms of synovioma would bemuch higher, and more closely follow the groupincidence of malignant forms of other mesenchymaltumours, e.g., giant-cell tumours of bone or chon-droid growths of major bones.
Considered in this light, it becomes apparent thatthe histological picture of giant-cell synovioma maybe shown by a mesenchymal growth potentiallycapable of further tissue differentiation in severaldirections. This parallels in most respects thebehaviour of giant-cell bone tumours. The litera-ture relating to the latter growths records acceptableexamples of supervening or associated malignancytaking the form offibrosarcoma, osteogenic sarcoma,and malignant giant-cell tumours of mainly osteo-lytic form. There are also reported cases of giant-cell bone tumours which have been malignant fromthe time of initial examination, although, in suchcases (e.g., that reported by Cameron and Marsden,1952), the history may be atypical in symptomsequence or timing, either for benign giant-celltumour or primary sarcoma.The most tenable view is surely that giant-cell
tumours, whether of bone or otherwise, grade fromthe so-called " benign " to the obviously malignant;and that the features, both clinical and histological,which typify the latter may appear either at an earlyor late stage, and may possibly be provoked by thefactors mentioned above.
While any attempted sub-division of a tumourtype may add unwanted fuel to the conflagrationwhich burns around the differentiation of benignand malignant forms, it yet may be of some prac-tical value. The useful application of this would
seem to be the rational basis for treatment andprognosis, founded upon careful consideration ofat least five major features in each instance, viz., thetumour type, histological grading, site, stage, andpotential ability for further aggressive development.
SummaryA detailed description is given of a malignant
giant-cell synovioma of the phalanx apparently ofintraosseous origin.The structure of this tumour has been interpreted
in the light of other closely related growths, and ahistogenesis from pluripotential mesenchymal cellsis suggested.The relationship and similarity of behaviour of
this tumour to other giant-cell mesenchymal growthsis discussed.
The authors wish to record their thanks to Mr. G. S.Storrs for permission to publish this case. The personalexamination of this tumour made by one of us formspart of a wider programme of investigation into thecausation of giant-cell tumours and their relationship toosteogenic sarcoma. This more extensive research isgenerously supported by the British Empire CancerCampaign. The reproductions of the radiographs andphotomicrographs are the work of Mr. J. E. Hancock,of the Medical Research Laboratory, Department ofPathology, University of Bristol.
REFERENCESBerger, L. (1938). Amer. J. Cancer, 34, 501.Briggs, C. D. (1942). Ann. Surg., 115, 413.Cameron, J. A. P., and Marsden, A. T. H. (1952). 1. Bone It Surg.,
34B, 93.Clark, C. E. (1952). Amer. J. Surg., 83, 112.Coley, B. L. (1949). Neoplasms of Bone, p. 472. Hoeber, New
York.De Santo, D. A., Tennant, R., and Rosahn, P. D. (1941). Surg.
Gt'nec. Obstet., 72, 951.Fisher, H. R. (1942). Amer. J. Path. 18, 529.Fletcher, A. G., Jr., and Horn, R. C., Jr. (1951). Ann. Surg., 133, 374.Foster, L. N. (1947). Amer. J. Path., 23, 567.Haagensen, C. D., and Stout, A. P. (1944). Ann. Surg., 120, 826.Jaffe, H. L., and Mayer, L. (1932). Arch. Surg., Chicago, 24, 550.King, E. S. J. (1952). J. Bone Jt Surg., 34B, 97.Knaggs, R. Lawford (1932). Brit. J. Surg., 20, 309.Lichtenstein, L. (1952). Bone Tumours, p. 83. Kimpton. London.Meverding. H. W., and Jackson, A. E. (1950). Surg. Clin. N. Amier.,
30, 1201.Murray, M. R., Stout, A. P., and Pogogeff, I. A. (1944). Ann. Surg.
120, 843.Price, C. H. G. (1952). Brit. J. Cancer, 6, 46.Stevenson, T. W. (1950). P/ast. reconstr. Surg., 5, 75.Vermooten, V. (1925). Ann. Surg., 81, 851.Virchow, R. (1863). Die Krankhaften Geschwulste, vol. 1, p. 527.
Hirschwald, Berlin. Quoted by Jaffe, H. L., and Mayer, L.Wright, C. J. E. (1949). J. Path. Bact., 61, 271.- (195 1). Brit. J. Surg., 38, 257.
(1952). J. Path. Bact., 64, 585.
238
on 4 May 2018 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.7.3.231 on 1 August 1954. D
ownloaded from





























