Embed Size (px)
Citation preview
Malignant Lymphoma of the Thyroid GlandA Clinicopathologic Study of 108 Cases
Gregory A. Derringer, M.D., Lester D. R. Thompson, M.D.,R. Allen Frommelt, Ph.D., Karen E. Bijwaard, M.S.,Clara S. Heffess, M.D., COL, MC, USA, and Susan L. Abbondanzo, M.D.
We report a retrospective clinicopathologic study of 108 pri-mary thyroid gland lymphomas (PTLs), classified using theREAL and proposed WHO classification schemes. The patientsincluded 79 women and 29 men, with an average age of 64.3years. All patients presented with a thyroid mass. The PTLswere classified as marginal zone B-cell lymphoma of mucosa-associated lymphoid tissue (MALT) or MZBL (n � 30), dif-fuse large B-cell lymphoma (DLBCL) with MZBL (n � 36),DLBCL without MZBL (n � 41), and follicle center lym-phoma (FCL; n � 1). Excluding the FCL, features of lympho-mas of MALT-type were identified in all groups, despite afollicular architecture in 23% of cases. Lymphocytic thyroiditis(LT) was identified in 94%. Ninety-one percent of patientspresented with stage IE or IIE disease, whereas 69% had peri-thyroidal soft tissue infiltration. All patients were treated withsurgical excision followed by adjuvant therapy (76%): chemo-therapy (15%), radiation (19%), or a combination of radiationand chemotherapy (42%). Disease-specific survival was 82% atlast follow up (mean, 82.8 mos) and 79% at 5 years. Statisti-cally, stages greater than IE, presence of DLBCL, rapid clinicalgrowth, abundant apoptosis, presence of vascular invasion,high mitotic rate, and infiltration of the perithyroidal soft tissuewere significantly associated with death with disease. No pa-tients with MZBL or stage IE disease died with disease. Insummary, PTLs typically occur in middle- to older-aged indi-viduals as a thyroid mass, with a predilection for females. De-spite their histologic heterogeneity and frequent simulation ofother lymphoma subtypes, virtually all PTLs are lymphomas ofMALT-type arising in the setting of LT. Mixed DLBCL andMZBL are common. Overall, PTLs have a favorable outcome
with appropriate therapy, but prognosis depends on both clini-cal stage and histology. MZBL and stage IE tumors have anexcellent prognosis, whereas tumors with a large cell compo-nent or DLBCL or stage greater than IE have the greatestpotential for a poor outcome.Key words: Thyroid—Malignant lymphoma—Classification—Marginal zone B-cell lymphoma—Mucosa-associatedlymphoid tissue (MALT)—Immunohistochemistry—Molecular analysis—Prognosis.
Am J Surg Pathol 24(5): 623–639, 2000.
Primary thyroid gland lymphomas (PTLs) are uncom-mon tumors that have been estimated to represent ap-proximately 5% of all thyroid neoplasms73 and 2.5% to7% of all extranodal lymphomas.10,24,59 Studies haveshown that PTLs typically occur in middle- to older-agedwomen and arise in the setting of autoimmune thyroiditis(lymphocytic thyroiditis, Hashimoto’s disease). The rela-tive risk of a patient with lymphocytic thyroiditis devel-oping lymphoma has been estimated to be 40 to 80 timesgreater than in the general population29,43,59 and to take,on average, 20 to 30 years to develop after the onset oflymphocytic thyroiditis.59
In the past, PTLs have been classified using a varietyof different terms because of the use of older histologicclassifications, implying variable clinical behav-ior.3,5,9,13,19,23,24,30,41,42,45,48,51,52,54,63,64,70,71,74,75,77,80
There is a better understanding of the concept of mucosa-associated lymphoid tissue (MALT) and recognition ofthe lymphomas that can arise from MALT because of theinitial description by Isaacson and Wright.35 In light ofthe MALT concept, certain authors think PTLs representa single clinicopathologic entity: MALT lymphoma.3,36
In the Revised European-American Classification ofLymphoid Neoplasms (REAL)27 and in the proposedWorld Health Organization (WHO) Classification forNeoplastic Diseases of the Lymphoid Tissues,40 thesedistinct lymphoid tumors are included under the term
From the Departments of Hematopathology (G.A.D., S.L.A.),Endocrine and Otorhinolaryngic-Head & Neck Pathology (L.D.R.T.,C.S.H.), Cellular Pathology (K.E.B.), and Department of Epidemiol-ogy, Repository and Research Services (R.A.F.), Armed ForcesInstitute of Pathology, Washington, DC, U.S.A.
Presented at the 87th Annual Meeting of the United States andCanadian Academy of athology, Boston, MA, February 28–March 7,1998.
The opinions or assertions contained herein are the private views ofthe authors and are not to be construed as official or as reflecting theviews of the Department of the Army or the Department of Defense.
Address correspondence and reprint requests to Gregory A.Derringer, MD, Department of Hematopathology, Building 54, RoomG124a, Armed Forces Institute of Pathology, 6825 16th Street, NW,Washington, DC 20306-6000, U.S.A.
The American Journal of Surgical Pathology 24(5): 623–639, 2000 © 2000 Lippincott Williams & Wilkins, Inc., Philadelphia
623

“marginal zone B-cell lymphoma of MALT-type(MZBL).”
Whereas large cell transformation of MZBL (mixedDLBCL and MZBL) is recognized and has been reportedin the thyroid34,45,59,69 and studied in other extranodalsites,17,22,30,46,60,61,66 its characterization, frequency, andeffect on clinical behavior remains unclear in the thyroidgland. Furthermore, there are no large, long-term clini-copathologic studies of PTLs using the MALT conceptand the most recent lymphoma classification schemes(REAL and proposed WHO). Therefore, we undertook aretrospective study of 108 PTLs using current conceptsto characterize the clinical, histomorphologic, immuno-phenotypic, and molecular characteristics of PTLs.
MATERIALS AND METHODS
One hundred eight cases of PTL, seen in consultationfrom 1985 to 1993, were retrieved from the files of theEndocrine Registry at the Armed Forces Institute ofPathology, Washington, DC. They were selected from atotal of 170 cases (2.4% of 7083 benign and malignantprimary thyroid gland neoplasms seen in consultationduring the same period). The authors defined PTLs aslymphomas that presented primarily as thyroid gland tu-mors. Cases were excluded if there was inadequate clini-cal history and follow up, a lack of hematoxylin andeosin (H&E)-stained sections, insufficient material forimmunohistochemical analysis, or a history of lym-phoma. Ninety-four cases were obtained from civiliansources, including university medical centers and foreigncontributors, 11 cases from military hospitals, and threecases from Veterans Administration Medical Centers.
Materials were supplemented by a review of surgicalpathology and operative reports, cancer registry records,and written questionnaires or oral communication withthe treating physician(s). Follow-up information in-cluded patients’ demographics, symptoms at presenta-tion, radiographic studies, clinical and surgical staging ofthe lymphoma, treatment modalities, and the current sta-tus of the disease and patient.
The lymphomas were classified with the aid of estab-lished criteria, recent studies, and the REAL and pro-posed WHO classifications.27,31,40 They were evaluatedfor features of MALT or lymphomas of MALT-type,including lymphoepithelial lesions (LEL), monocytoidB-cells, centrocyte-like cells, plasma cells, abnormal cy-toplasmic immunoglobulin accumulations, Dutcher bod-ies, and reactive follicles with or without colonization bylymphoma (“follicular colonization”). Additional fea-tures assessed were presence or absence of abundant ap-optosis (more than four apoptotic cells per high-powerfield [HPF] using the 40× objective), tumor necrosis,vascular invasion (infiltration of neoplastic cells into thewall of any thyroidal vessel [artery, vein, or lymphatic]),
and extension into the perithyroidal adipose tissue and/orskeletal muscle. Fibrosis was graded semiquantitativelyas mild (thin bands or small microscopic foci of fibrosison high-power magnification [40× objective]), moderate(broad bands of fibrosis on intermediate magnification[20× objective]), and severe (large areas of sclerosis re-placing the thyroid architecture on low-power magnifi-cation [10× objective]). Mitotic activity was rated as low(less than 10 mitotic figures/10 HPF) or high (greaterthan 10 mitotic figures/10 HPF), using the 40× objective.Diffuse large cell lymphoma was defined as a lymphomaor areas within a small cell lymphoma that were com-prised of large lymphoid cells that “sheeted out” in adiffuse manner. Increased, scattered, single, large immu-noblasts or Reed-Sternberg-like cells in a small cell lym-phoma or a predominance of large atypical cells in thefollicles of a small cell lymphoma were not consideredindicative of a large cell lymphoma. All cases were in-vestigated for the presence of lymphocytic thyroiditis,defined in this study as reactive lymphocytic or lympho-plasmacytic infiltrates in the thyroid parenchyma withformation of lymphoid aggregates and fibrosis. The pres-ence of follicles with germinal center formation and oxy-philic change of the follicular epithelium was not re-quired for this designation. Other thyroid abnormalitieswere also documented.
With the aid of Musshoff’s modification of the AnnArbor staging system,16 PTLs were staged as follows:IE: PTLs with or without extension into the perithyroidalsoft tissue; IIE: PTLs with involvement of lymph nodeson the same side of the diaphragm; IIIE: PTLs withinvolvement of lymph nodes on both sides of the dia-phragm and/or spleen; and IVE: PTLs with dissemina-tion to other extranodal sites.
Formalin-fixed, paraffin-embedded tissue and un-stained sections were available for H&E and periodicacid Schiff (PAS) stains and immunohistochemicalanalysis. Immunophenotypic analysis was performed ac-cording to the standardized avidin–biotin method of Hsuet al.32 using a pertinent commercially available antibodypanel (Table 1). Predigestion was performed with eitherprotease or pepsin (as noted): 3 minutes with 0.05%Protease VIII (Sigma Chemical Co, St. Louis, MO,USA) in a 0.1 M phosphate buffer at pH of 7.8 at 37°Cor 20 minutes with 0.04% pepsin in a 0.1 M phosphatebuffer at pH 2.0 at 40°C. Antigen enhancement (recov-ery) was performed when appropriate by using formalin-fixed, paraffin-embedded tissue treated with a bufferedcitric acid solution and heated for 20 minutes in a cali-brated microwave oven. Following this, the sectionswere allowed to cool at room temperature in a citric acidbuffer solution for 15 to 45 minutes before continuingthe procedure. Standard positive and negative (serum)controls were used throughout.
G. A. DERRINGER ET AL.624
Am J Surg Pathol, Vol. 24, No. 5, 2000

Polymerase Chain Reaction
DNA was extracted from formalin-fixed, paraffin-embedded sections as previously described.65 t(11;14)and t(14;18) bcl-2/MBR-JH PCR assays were performedand analyzed as previously described.2,81 The t(14;18)bcl-2/MCR-JH assay was performed as the MBR-JH as-say using AmpliTaq Gold DNA polymerase for the “hot-start” application. Bcl-2/MCR-JH primers were derivedfrom published sequences.55,65 t(14;18) positive controlcell lines (SUDHL-6 and SUDHL-16) were obtainedfrom Alan Epstein, MD, PhD (USC, Los Angeles, CA,USA).
Statistical Analysis
Statistical analysis was performed on 107 cases, ex-cluding the single case of FCL. Mean differences be-tween groups were compared using unpaired t tests oranalysis of variance (ANOVA), respectively. Tukeymultiple comparison procedures were used to make two-way comparisons among groups in which ANOVA wasused. Differences between observed and expectedfrequencies were compared using chi-square tests orFisher’s exact test when there were fewer than five pa-tients in any subcategory. When necessary, the caseswere divided into two main groups, MZBL and DLBCL,or lymphomas with a large cell component, which in-cluded both mixed DLBCL and MZBL and DLBCLwithout MZBL groups.
Survival analysis and a survival comparison betweenthe two main groups of lymphomas, MZBL and DLBCL,could not be performed because only 20 patients diedwith disease (all with DLBCL). At least 30 cases are
needed in each group to have adequate power to detectstatistically meaningful differences.
For the purpose of this summary, strong findings weredefined as those results for which the p value was lessthan 0.05 and the confidence interval did not include thenull value. Weak findings were when either the p valueor the confidence interval was statistically significant,but not both. Stages IIIE and IVE were combined in theanalysis because of the limits of sample size.
RESULTS
Pathology
Macroscopic Findings
The lymphomas ranged in size from 0.5 to 19.5 cm inmaximum dimension with a mean size of 6.9 cm (Table2) without a statistically significant difference in tumorsize between the three groups. Tumors that presented asa rapidly enlarging mass were, on average, larger (7.2cm) than those tumors that presented as a mass only (6.4cm), but this was not statistically significant (p � 0.644).The tumors involved the right (n � 33), left (n � 23), orboth lobes (n � 48) of the thyroid gland. The specificlobe of the thyroid gland involved was unknown in fourcases.
The tumors were described grossly as firm to soft,lobulated, multinodular to diffuse, solid or cystic masses.The cut surface was smooth or slightly bulging, pale, tanto white–gray, or red with a “fish-flesh,” uniform, ho-mogeneous to mottled appearance. Foci of hemorrhageand necrosis were frequently noted. Attachment to the
TABLE 1. Immunohistochemical panel
Antibody Primary antibody Company Dilution Antigen unmasking
CD3 Rabbit polyclonal Dako Corporation,Carpinteria, CA
1:500 Protease treatment
CD5 Mouse monoclonal Vector/Novocastra Labs,Burlingame, CA
1:100 Microwave pretreatment
CD10 Mouse monoclonal Vector/Novocastra 1:100 Microwave pretreatmentCD20 (L26) Mouse monoclonal Dako 1:200 —CD23 Mouse monoclonal The Binding Site,
San Diego, CA1:200 Pepsin treatment
CD43 (MT1) Mouse monoclonal Biotest, Denville, NJ 1:50 —CD45RA (MT2) Mouse monoclonal Biotest 1:20 —CD45RB (LCA) Mouse monoclonal Dako 1:200 —CD45RO (UCHL-1) Mouse monoclonal Dako 1:200 —CD79a Mouse monoclonal Dako 1:200 Microwave pretreatmentBcl-1 (cyclin D1) Mouse monoclonal Immunotech, Marseilles, France 1:3000 Microwave pretreatmentBcl-2 Mouse monoclonal Dako 1:100 Microwave pretreatmentBeta F-1 Mouse monoclonal Endogen, Woburn, MA 1:50 Pepsin treatmentKappa Rabbit polyclonal Dako 1:25000 Protease treatmentLambda Rabbit polyclonal Dako 1:50000 Protease treatmentCytokeratin
(AE1/AE3 and CK1)Mouse monoclonal Boehringer Mannheim,
Indianapolis, IN1:50 & 1:200 Protease treatment
Thyroglobulin Mouse monoclonal Dako 1:100 —
THYROID LYMPHOMAS 625
Am J Surg Pathol, Vol. 24, No. 5, 2000
surrounding adipose tissue or skeletal muscle was de-scribed in 75 cases.
Microscopic Findings
The lymphomas were classified into four groups: 30MZBL, 36 mixed DLBCL and MZBL, 41 DLBCL with-out MZBL, and one FCL. All lymphomas were com-prised of B-lymphocytes that effaced the thyroid paren-chyma (Fig. 1). Although the lymphomas varied archi-tecturally and cytologically from case to case and withinan individual case, features of lymphomas of MALT-type were identified in almost all cases.
Infiltration by the lymphoma into the perithyroidaladipose tissue and/or skeletal muscle was detected in70% (75 of 107 cases assessable), including the case ofFCL. The frequency of soft tissue infiltration increasedas the quantity of the large cell component increased(p � 0.027), with 58 of these 75 patients having aDLBCL. Twenty-seven cases (25%) demonstrated vas-cular invasion (Fig. 2) and all were DLBCL (p �0.0001). A variable degree of background fibrosis wasdetected in all cases.
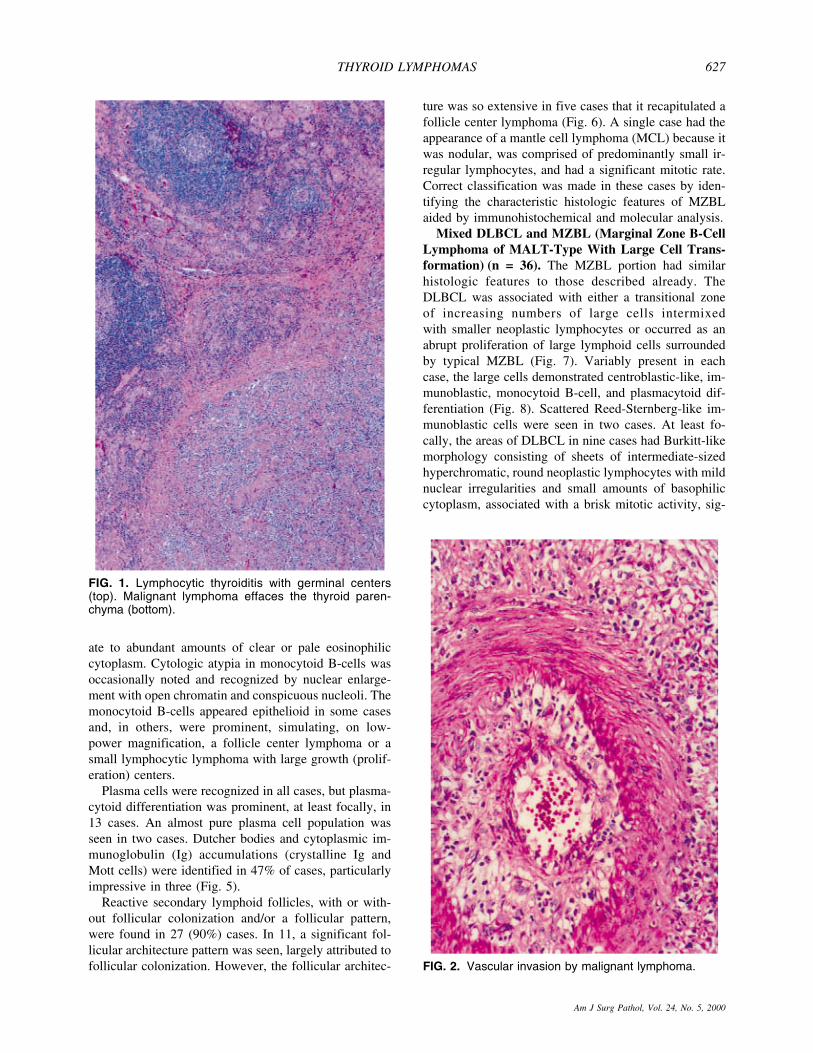
Although quantity and quality varied from case tocase, lymphoepithelial lesions (LEL) could be identifiedin most cases. LEL occurred in two forms. The first formwas more common and of the usual type, characterizedby neoplastic cells in variably sized nests or roundedgroupings infiltrating within and between the thyroid fol-
licular epithelium (Fig. 3). The second type was moreunique, characterized by variably sized, rounded massesof neoplastic cells that filled and distended the colloidalspace of the follicles, termed by us as “MALT ball” LEL(Fig. 3).
Lymphocytic thyroiditis was present in 94% (n �101), including the case of FCL. Lymphocytic thyroiditisusually contained reactive follicles with an absence of adense, sheet-like effacement of the thyroid parenchymaand demonstrated both B- and T-cells areas by immuno-histochemistry. Neoplastic cells occasionally colonizedthe germinal centers of reactive follicles in areas of lym-phocytic thyroiditis. The uninvolved thyroid parenchymacontained adenomatoid nodules which were occasionallycalcified and degenerated (n � 22), microscopic papil-lary carcinoma (n � 7), follicular adenoma (n � 1), andfollicular carcinoma (n � 1).
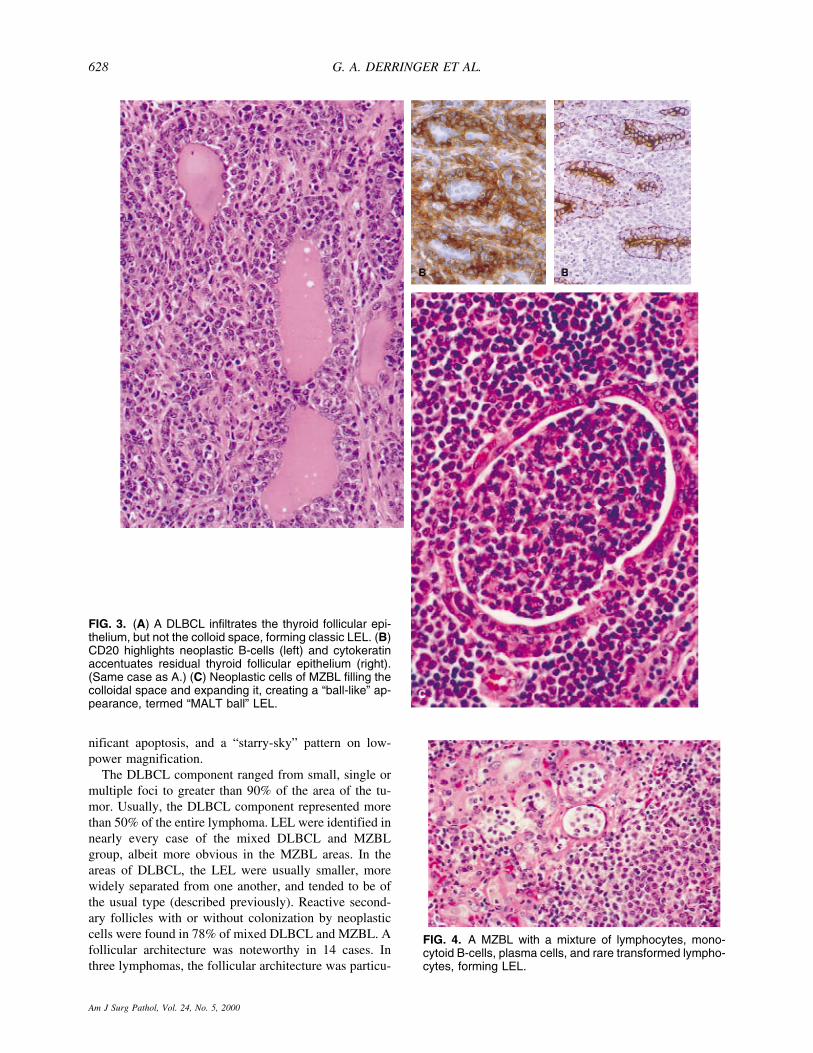
Marginal Zone B-Cell Lymphoma of MALT-Type (MZBL) (n = 30). MZBL consisted of predomi-nantly small lymphoid cells with variable proportions ofcentrocyte-like cells, plasma cells, lymphoplasmacytoidlymphocytes, monocytoid B-cells, and interspersed largetransformed lymphocytes (Fig. 4). LEL were identifiedin all cases. In a single case, a rare large transformed cellwith Reed-Sternberg-like morphology was noted, butDLBCL was not identified. The monocytoid B-cells, fre-quently arranged in cohesive groups, varied from smallto intermediate-sized cells containing round, oval, orslightly irregular nuclei with dark chromatin and moder-
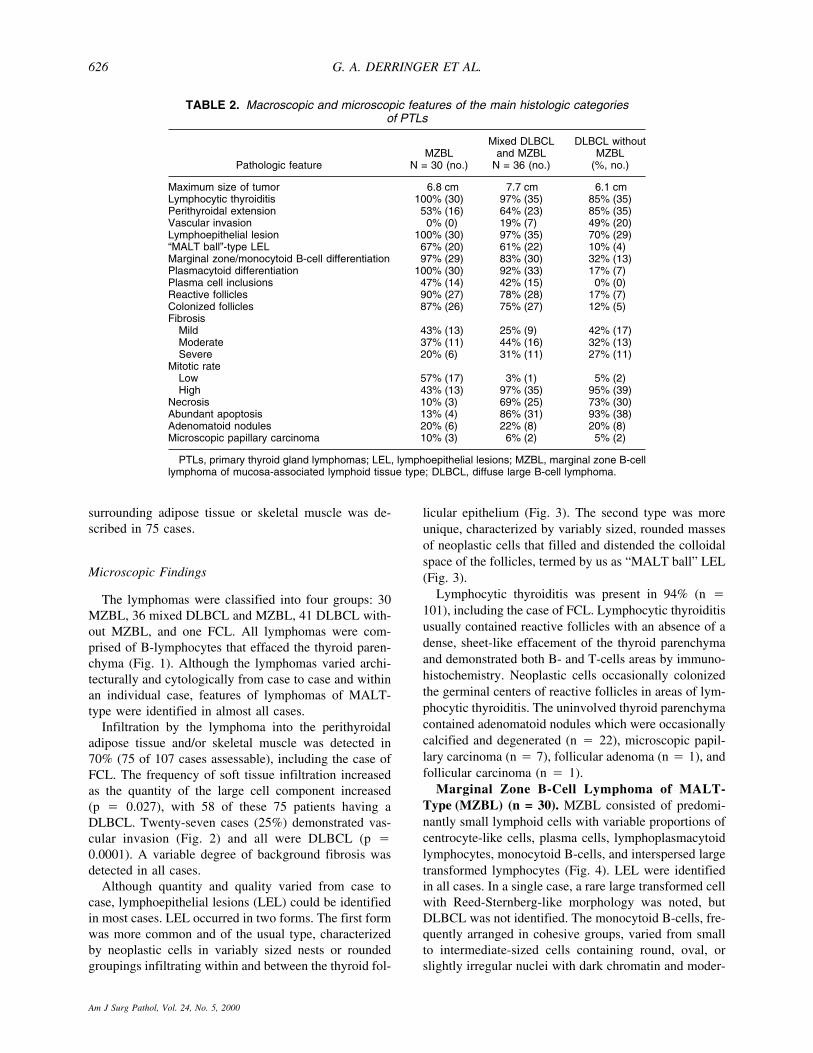
TABLE 2. Macroscopic and microscopic features of the main histologic categoriesof PTLs
Pathologic featureMZBL
N = 30 (no.)
Mixed DLBCLand MZBL
N = 36 (no.)
DLBCL withoutMZBL
(%, no.)
Maximum size of tumor 6.8 cm 7.7 cm 6.1 cmLymphocytic thyroiditis 100% (30) 97% (35) 85% (35)Perithyroidal extension 53% (16) 64% (23) 85% (35)Vascular invasion 0% (0) 19% (7) 49% (20)Lymphoepithelial lesion 100% (30) 97% (35) 70% (29)“MALT ball”-type LEL 67% (20) 61% (22) 10% (4)Marginal zone/monocytoid B-cell differentiation 97% (29) 83% (30) 32% (13)Plasmacytoid differentiation 100% (30) 92% (33) 17% (7)Plasma cell inclusions 47% (14) 42% (15) 0% (0)Reactive follicles 90% (27) 78% (28) 17% (7)Colonized follicles 87% (26) 75% (27) 12% (5)Fibrosis
Mild 43% (13) 25% (9) 42% (17)Moderate 37% (11) 44% (16) 32% (13)Severe 20% (6) 31% (11) 27% (11)
Mitotic rateLow 57% (17) 3% (1) 5% (2)High 43% (13) 97% (35) 95% (39)
Necrosis 10% (3) 69% (25) 73% (30)Abundant apoptosis 13% (4) 86% (31) 93% (38)Adenomatoid nodules 20% (6) 22% (8) 20% (8)Microscopic papillary carcinoma 10% (3) 6% (2) 5% (2)
PTLs, primary thyroid gland lymphomas; LEL, lymphoepithelial lesions; MZBL, marginal zone B-celllymphoma of mucosa-associated lymphoid tissue type; DLBCL, diffuse large B-cell lymphoma.
G. A. DERRINGER ET AL.626
Am J Surg Pathol, Vol. 24, No. 5, 2000
ate to abundant amounts of clear or pale eosinophiliccytoplasm. Cytologic atypia in monocytoid B-cells wasoccasionally noted and recognized by nuclear enlarge-ment with open chromatin and conspicuous nucleoli. Themonocytoid B-cells appeared epithelioid in some casesand, in others, were prominent, simulating, on low-power magnification, a follicle center lymphoma or asmall lymphocytic lymphoma with large growth (prolif-eration) centers.
Plasma cells were recognized in all cases, but plasma-cytoid differentiation was prominent, at least focally, in13 cases. An almost pure plasma cell population wasseen in two cases. Dutcher bodies and cytoplasmic im-munoglobulin (Ig) accumulations (crystalline Ig andMott cells) were identified in 47% of cases, particularlyimpressive in three (Fig. 5).
Reactive secondary lymphoid follicles, with or with-out follicular colonization and/or a follicular pattern,were found in 27 (90%) cases. In 11, a significant fol-licular architecture pattern was seen, largely attributed tofollicular colonization. However, the follicular architec-
ture was so extensive in five cases that it recapitulated afollicle center lymphoma (Fig. 6). A single case had theappearance of a mantle cell lymphoma (MCL) because itwas nodular, was comprised of predominantly small ir-regular lymphocytes, and had a significant mitotic rate.Correct classification was made in these cases by iden-tifying the characteristic histologic features of MZBLaided by immunohistochemical and molecular analysis.
Mixed DLBCL and MZBL (Marginal Zone B-CellLymphoma of MALT-Type With Large Cell Trans-formation) (n = 36). The MZBL portion had similarhistologic features to those described already. TheDLBCL was associated with either a transitional zoneof increasing numbers of large cells intermixedwith smaller neoplastic lymphocytes or occurred as anabrupt proliferation of large lymphoid cells surroundedby typical MZBL (Fig. 7). Variably present in eachcase, the large cells demonstrated centroblastic-like, im-munoblastic, monocytoid B-cell, and plasmacytoid dif-ferentiation (Fig. 8). Scattered Reed-Sternberg-like im-munoblastic cells were seen in two cases. At least fo-cally, the areas of DLBCL in nine cases had Burkitt-likemorphology consisting of sheets of intermediate-sizedhyperchromatic, round neoplastic lymphocytes with mildnuclear irregularities and small amounts of basophiliccytoplasm, associated with a brisk mitotic activity, sig-
FIG. 2. Vascular invasion by malignant lymphoma.
FIG. 1. Lymphocytic thyroiditis with germinal centers(top). Malignant lymphoma effaces the thyroid paren-chyma (bottom).
THYROID LYMPHOMAS 627
Am J Surg Pathol, Vol. 24, No. 5, 2000
nificant apoptosis, and a “starry-sky” pattern on low-power magnification.
The DLBCL component ranged from small, single ormultiple foci to greater than 90% of the area of the tu-mor. Usually, the DLBCL component represented morethan 50% of the entire lymphoma. LEL were identified innearly every case of the mixed DLBCL and MZBLgroup, albeit more obvious in the MZBL areas. In theareas of DLBCL, the LEL were usually smaller, morewidely separated from one another, and tended to be ofthe usual type (described previously). Reactive second-ary follicles with or without colonization by neoplasticcells were found in 78% of mixed DLBCL and MZBL. Afollicular architecture was noteworthy in 14 cases. Inthree lymphomas, the follicular architecture was particu-
FIG. 3. (A) A DLBCL infiltrates the thyroid follicular epi-thelium, but not the colloid space, forming classic LEL. (B)CD20 highlights neoplastic B-cells (left) and cytokeratinaccentuates residual thyroid follicular epithelium (right).(Same case as A.) (C) Neoplastic cells of MZBL filling thecolloidal space and expanding it, creating a “ball-like” ap-pearance, termed “MALT ball” LEL.
FIG. 4. A MZBL with a mixture of lymphocytes, mono-cytoid B-cells, plasma cells, and rare transformed lympho-cytes, forming LEL.
G. A. DERRINGER ET AL.628
Am J Surg Pathol, Vol. 24, No. 5, 2000
larly prominent and, in conjunction with the DLBCLareas, simulated a follicle center lymphoma, large cellwith follicular and diffuse areas. However, these caseswere correctly classified by the identification of featuresof lymphomas of MALT-type and immunohistochemicaland molecular analysis.
Diffuse Large B-Cell Lymphoma Without MZBL(DLBCL Without MZBL) (n = 41). The DLBCLs werelarge cell lymphomas that lacked an associated MZBL.The large neoplastic cells of this group demonstrated the
spectrum described above for the DLBCL component ofthe mixed DLBCL and MZBL group (Fig. 9). Althoughless conspicuous than in the MZBL group, at least onemorphologic characteristic of lymphomas of MALT-typewas seen in 85% of cases (n � 35) and 85% of caseswere associated with lymphocytic thyroiditis. The pres-ence of LEL, follicular colonization, monocytoid B-celldifferentiation, and plasmacytoid differentiation variedin quantity and quality from case to case.
FIG. 6. Low-power magnification of a MZBL with a follic-ular growth pattern.
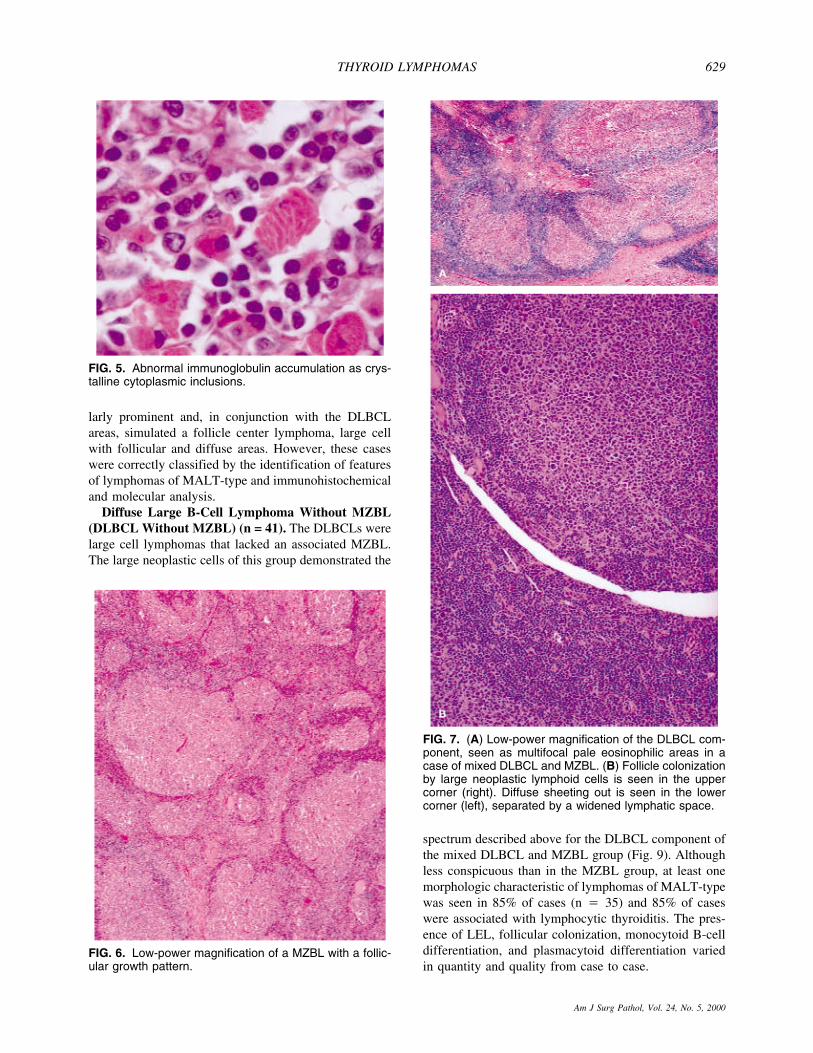
FIG. 5. Abnormal immunoglobulin accumulation as crys-talline cytoplasmic inclusions.
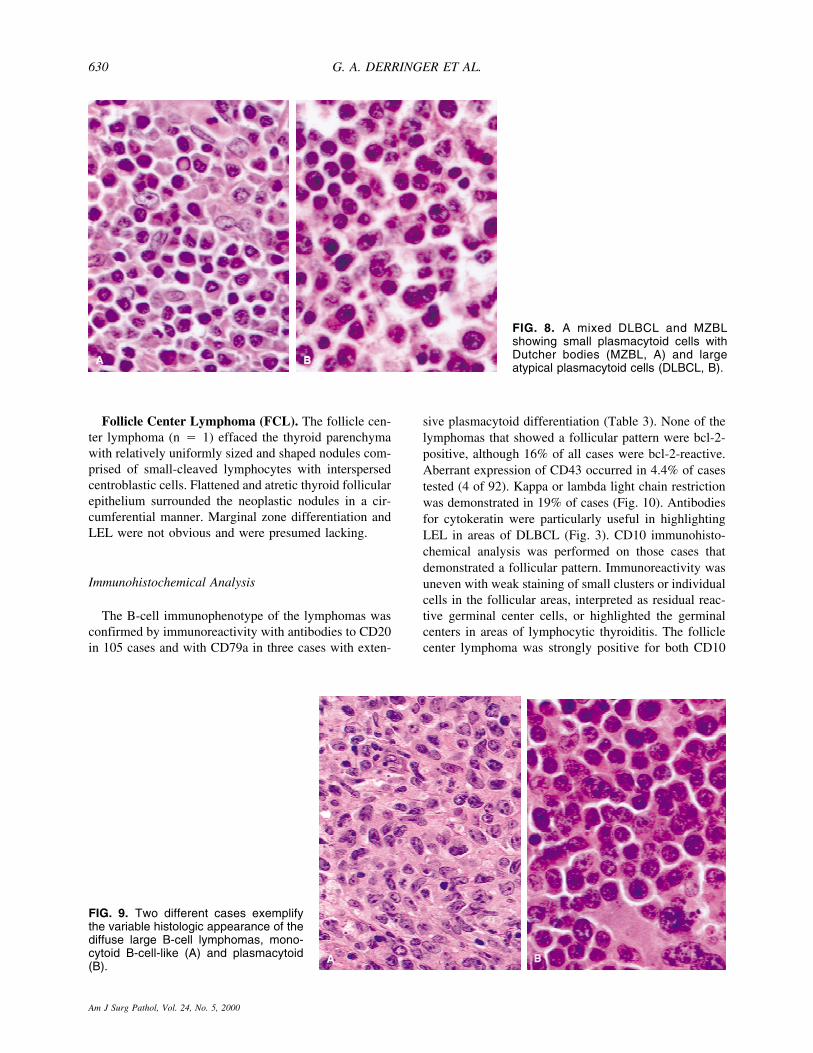
FIG. 7. (A) Low-power magnification of the DLBCL com-ponent, seen as multifocal pale eosinophilic areas in acase of mixed DLBCL and MZBL. (B) Follicle colonizationby large neoplastic lymphoid cells is seen in the uppercorner (right). Diffuse sheeting out is seen in the lowercorner (left), separated by a widened lymphatic space.
THYROID LYMPHOMAS 629
Am J Surg Pathol, Vol. 24, No. 5, 2000
Follicle Center Lymphoma (FCL). The follicle cen-ter lymphoma (n � 1) effaced the thyroid parenchymawith relatively uniformly sized and shaped nodules com-prised of small-cleaved lymphocytes with interspersedcentroblastic cells. Flattened and atretic thyroid follicularepithelium surrounded the neoplastic nodules in a cir-cumferential manner. Marginal zone differentiation andLEL were not obvious and were presumed lacking.
Immunohistochemical Analysis
The B-cell immunophenotype of the lymphomas wasconfirmed by immunoreactivity with antibodies to CD20in 105 cases and with CD79a in three cases with exten-
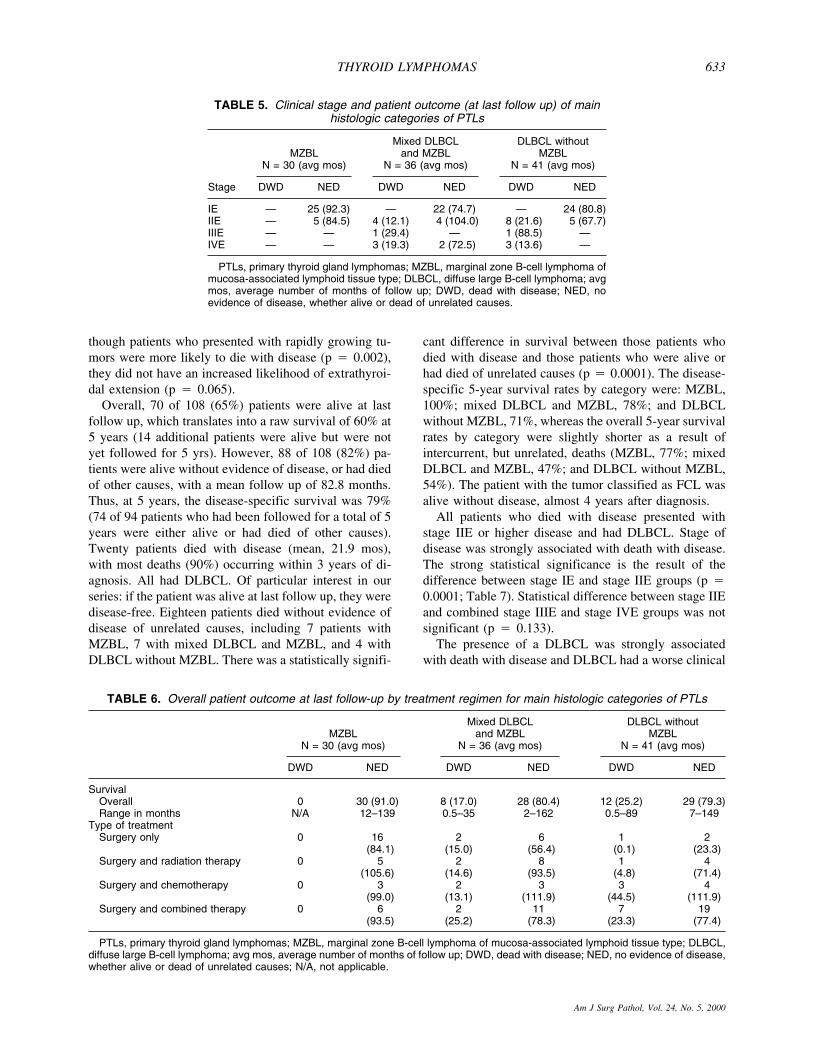
sive plasmacytoid differentiation (Table 3). None of thelymphomas that showed a follicular pattern were bcl-2-positive, although 16% of all cases were bcl-2-reactive.Aberrant expression of CD43 occurred in 4.4% of casestested (4 of 92). Kappa or lambda light chain restrictionwas demonstrated in 19% of cases (Fig. 10). Antibodiesfor cytokeratin were particularly useful in highlightingLEL in areas of DLBCL (Fig. 3). CD10 immunohisto-chemical analysis was performed on those cases thatdemonstrated a follicular pattern. Immunoreactivity wasuneven with weak staining of small clusters or individualcells in the follicular areas, interpreted as residual reac-tive germinal center cells, or highlighted the germinalcenters in areas of lymphocytic thyroiditis. The folliclecenter lymphoma was strongly positive for both CD10
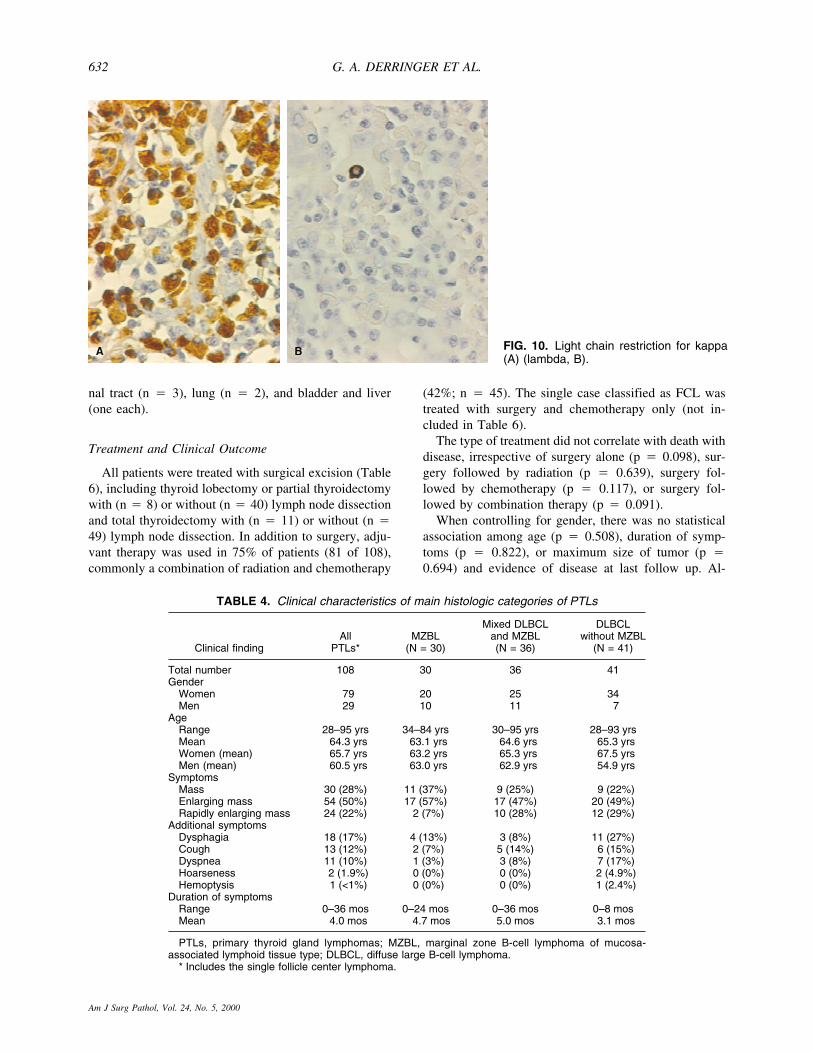
FIG. 9. Two different cases exemplifythe variable histologic appearance of thediffuse large B-cell lymphomas, mono-cytoid B-cell-like (A) and plasmacytoid(B).
FIG. 8. A mixed DLBCL and MZBLshowing small plasmacytoid cells withDutcher bodies (MZBL, A) and largeatypical plasmacytoid cells (DLBCL, B).
G. A. DERRINGER ET AL.630
Am J Surg Pathol, Vol. 24, No. 5, 2000

and bcl-2. The case that simulated mantle cell lymphomaand the case that had the appearance of small lympho-cytic lymphoma were negative for antibodies to CD5,CD23, CD43, and bcl-1.
Molecular Analysis
In molecular analysis, amplifiable DNA was obtainedin 17 of the 25 lymphomas that demonstrated a follicularpattern, at least focally, including seven of eightcases with an extensive follicular pattern that simulatedFCL. None were positive for either the t(14;18)bcl-2/MBR-JH (major break point/MBR) or the t(14;18)bcl-2/MCR-JH (minor cluster region/MCR) assays. Thesingle case classified as follicle center lymphoma wasalso negative for both assays. The single case that simu-lated a mantle cell lymphoma was negative for thet(11;14) assay.
Clinical
Age, Gender, Signs, and Symptoms
The patients included 79 women and 29 men, with afemale to male ratio of 2.7:1 (Table 4). Their ages rangedfrom 28 to 95 years with a mean of 64.3 years at initialpresentation. The difference in mean age at presentationfor women (65.7 yrs) and men (60.5 yrs) was not statis-tically significant (p � 0.135). Curiously, men withDLBCL without MZBL presented a decade earlier (54.9yrs) compared with women (67.5 yrs), but this differencewas also not statistically significant (p � 0.508).
Clinically, all patients presented with a mass in thethyroid gland that was noticeably enlarging in 72% (n �78) of cases (Table 4). Rapidly enlarging masses werereported more frequently in DLBCL (29% of DLBCLwithout MZBL, 28% of mixed DLBCL and MZBL) thanin the MZBL (6.6%), yielding a statistically significantresult (p � 0.042). Symptoms resulting from compres-sion/infiltration of the neck organs such as dyspnea, dys-phagia, choking and/or coughing, and hemoptysis werereported in 31% of cases (n � 33). Pain was also expe-rienced. Additional symptoms were reported more fre-quently in enlarging tumors (37%) or rapidly enlargingtumors (33%) than in tumors that presented as a massonly (17%) and were significantly more common inDLBCL (p � 0.048). As the percentage of large cellcomponent increased, there was a greater frequency ofassociated symptoms resulting from compression/infiltration of the neck structures (17% of MZBL, 25% ofmixed DLBCL and MZBL, and 46% of DLBCL withoutMZBL).
Overall, the duration of symptoms ranged from a fewdays to 36 months (mean, 4 mos; Table 4). Whereaspatients in the DLBCL without MZBL category had a
slightly shorter duration of symptoms than the othergroups, this difference was not statistically significant(p � 0.241).
Diagnostic Investigations
Radioactive iodine uptake roentgenographic proce-dures were performed in the majority of patients, al-though a detailed radiographic narrative was available inonly 52. The scans were reported to show “cold” nodulesin 21 cases, diffuse low-uptake in 19 cases, and no sig-nificant abnormalities in 12 cases. Serum antibody re-sults were available in too few cases to be meaningfullyreported.
Stage
The majority of patients presented with stage IE dis-ease (n � 71, 66%; Table 5). An additional 27 patientspresented with stage IIE (including the one follicularlymphoma), with the remaining patients presenting withstage IIIE (n � 2) and stage IVE (n � 8) disease. Nopatients with stage IE died with disease, irrespective ofthe histologic grade of the tumor (mean, 82.2 mos),whereas 44% of stage IIE, 100% of stage IIIE, and 75%of stage IVE patients died of their disease. MZBL pa-tients presented with stage IE (83%) or IIE (17%) dis-ease. All patients who presented with stage IIIE or IVEhad DLBCL. When dissemination was present, either atpresentation or subsequently, the most common site ofinvolvement was lymph nodes. Cervical/perithyroidallymph nodes were the most common nodal sites in-volved, usually identified at, or shortly after initial sur-gery, followed by mediastinal and abdominal lymphnodes. Extranodal involvement was found in 8.3% of allcases and included bone marrow (n � 4), gastrointesti-
TABLE 3. Immunohistochemical findings of mainhistologic categories of PTLs
AntibodyMZBL
(N = 30)
Mixed DLBCLand MZBL(N = 36)
DLBCL withoutMZBL
CD45RB 100% (29/29) 97% (33/34) 95% (35/37)CD20 93% (28/30) 97% (35/36) 100% (41/41)CD3 0% (0/30) 0% (0/35) 0% (0/36)CD45RO 4% (1/26) 9% (3/33) 9% (3/35)CD43 7% (2/28) 6% (2/34) 0% (0/31)CD45RA 40% (10/25) 16% (5/31) 14% (4/29)Bcl-2 18% (5/28) 28% (5/18) 22% (6/27)Kappa r 10% (3/29) 9% (3/33) 3% (1/29)Lambda r 14% (4/29) 15% (5/33) 3% (1/29)
MZBL, marginal zone B-cell lymphoma of mucosa-associatedlymphoid tissue type; DLBCL, diffuse large B-cell lymphoma; r,light chain restriction.
THYROID LYMPHOMAS 631
Am J Surg Pathol, Vol. 24, No. 5, 2000
nal tract (n � 3), lung (n � 2), and bladder and liver(one each).
Treatment and Clinical Outcome
All patients were treated with surgical excision (Table6), including thyroid lobectomy or partial thyroidectomywith (n � 8) or without (n � 40) lymph node dissectionand total thyroidectomy with (n � 11) or without (n �49) lymph node dissection. In addition to surgery, adju-vant therapy was used in 75% of patients (81 of 108),commonly a combination of radiation and chemotherapy
(42%; n � 45). The single case classified as FCL wastreated with surgery and chemotherapy only (not in-cluded in Table 6).
The type of treatment did not correlate with death withdisease, irrespective of surgery alone (p � 0.098), sur-gery followed by radiation (p � 0.639), surgery fol-lowed by chemotherapy (p � 0.117), or surgery fol-lowed by combination therapy (p � 0.091).
When controlling for gender, there was no statisticalassociation among age (p � 0.508), duration of symp-toms (p � 0.822), or maximum size of tumor (p �0.694) and evidence of disease at last follow up. Al-
TABLE 4. Clinical characteristics of main histologic categories of PTLs
Clinical findingAll
PTLs*MZBL
(N = 30)
Mixed DLBCLand MZBL(N = 36)
DLBCLwithout MZBL
(N = 41)
Total number 108 30 36 41Gender
Women 79 20 25 34Men 29 10 11 7
AgeRange 28–95 yrs 34–84 yrs 30–95 yrs 28–93 yrsMean 64.3 yrs 63.1 yrs 64.6 yrs 65.3 yrsWomen (mean) 65.7 yrs 63.2 yrs 65.3 yrs 67.5 yrsMen (mean) 60.5 yrs 63.0 yrs 62.9 yrs 54.9 yrs
SymptomsMass 30 (28%) 11 (37%) 9 (25%) 9 (22%)Enlarging mass 54 (50%) 17 (57%) 17 (47%) 20 (49%)Rapidly enlarging mass 24 (22%) 2 (7%) 10 (28%) 12 (29%)
Additional symptomsDysphagia 18 (17%) 4 (13%) 3 (8%) 11 (27%)Cough 13 (12%) 2 (7%) 5 (14%) 6 (15%)Dyspnea 11 (10%) 1 (3%) 3 (8%) 7 (17%)Hoarseness 2 (1.9%) 0 (0%) 0 (0%) 2 (4.9%)Hemoptysis 1 (<1%) 0 (0%) 0 (0%) 1 (2.4%)
Duration of symptomsRange 0–36 mos 0–24 mos 0–36 mos 0–8 mosMean 4.0 mos 4.7 mos 5.0 mos 3.1 mos
PTLs, primary thyroid gland lymphomas; MZBL, marginal zone B-cell lymphoma of mucosa-associated lymphoid tissue type; DLBCL, diffuse large B-cell lymphoma.
* Includes the single follicle center lymphoma.
FIG. 10. Light chain restriction for kappa(A) (lambda, B).
G. A. DERRINGER ET AL.632
Am J Surg Pathol, Vol. 24, No. 5, 2000
though patients who presented with rapidly growing tu-mors were more likely to die with disease (p � 0.002),they did not have an increased likelihood of extrathyroi-dal extension (p � 0.065).
Overall, 70 of 108 (65%) patients were alive at lastfollow up, which translates into a raw survival of 60% at5 years (14 additional patients were alive but were notyet followed for 5 yrs). However, 88 of 108 (82%) pa-tients were alive without evidence of disease, or had diedof other causes, with a mean follow up of 82.8 months.Thus, at 5 years, the disease-specific survival was 79%(74 of 94 patients who had been followed for a total of 5years were either alive or had died of other causes).Twenty patients died with disease (mean, 21.9 mos),with most deaths (90%) occurring within 3 years of di-agnosis. All had DLBCL. Of particular interest in ourseries: if the patient was alive at last follow up, they weredisease-free. Eighteen patients died without evidence ofdisease of unrelated causes, including 7 patients withMZBL, 7 with mixed DLBCL and MZBL, and 4 withDLBCL without MZBL. There was a statistically signifi-
cant difference in survival between those patients whodied with disease and those patients who were alive orhad died of unrelated causes (p � 0.0001). The disease-specific 5-year survival rates by category were: MZBL,100%; mixed DLBCL and MZBL, 78%; and DLBCLwithout MZBL, 71%, whereas the overall 5-year survivalrates by category were slightly shorter as a result ofintercurrent, but unrelated, deaths (MZBL, 77%; mixedDLBCL and MZBL, 47%; and DLBCL without MZBL,54%). The patient with the tumor classified as FCL wasalive without disease, almost 4 years after diagnosis.
All patients who died with disease presented withstage IIE or higher disease and had DLBCL. Stage ofdisease was strongly associated with death with disease.The strong statistical significance is the result of thedifference between stage IE and stage IIE groups (p �0.0001; Table 7). Statistical difference between stage IIEand combined stage IIIE and stage IVE groups was notsignificant (p � 0.133).
The presence of a DLBCL was strongly associatedwith death with disease and DLBCL had a worse clinical
TABLE 5. Clinical stage and patient outcome (at last follow up) of mainhistologic categories of PTLs
Stage
MZBLN = 30 (avg mos)
Mixed DLBCLand MZBL
N = 36 (avg mos)
DLBCL withoutMZBL
N = 41 (avg mos)
DWD NED DWD NED DWD NED
IE — 25 (92.3) — 22 (74.7) — 24 (80.8)IIE — 5 (84.5) 4 (12.1) 4 (104.0) 8 (21.6) 5 (67.7)IIIE — — 1 (29.4) — 1 (88.5) —IVE — — 3 (19.3) 2 (72.5) 3 (13.6) —
PTLs, primary thyroid gland lymphomas; MZBL, marginal zone B-cell lymphoma ofmucosa-associated lymphoid tissue type; DLBCL, diffuse large B-cell lymphoma; avgmos, average number of months of follow up; DWD, dead with disease; NED, noevidence of disease, whether alive or dead of unrelated causes.
TABLE 6. Overall patient outcome at last follow-up by treatment regimen for main histologic categories of PTLs
MZBLN = 30 (avg mos)
Mixed DLBCLand MZBL
N = 36 (avg mos)
DLBCL withoutMZBL
N = 41 (avg mos)
DWD NED DWD NED DWD NED
SurvivalOverall 0 30 (91.0) 8 (17.0) 28 (80.4) 12 (25.2) 29 (79.3)Range in months N/A 12–139 0.5–35 2–162 0.5–89 7–149
Type of treatmentSurgery only 0 16 2 6 1 2
(84.1) (15.0) (56.4) (0.1) (23.3)Surgery and radiation therapy 0 5 2 8 1 4
(105.6) (14.6) (93.5) (4.8) (71.4)Surgery and chemotherapy 0 3 2 3 3 4
(99.0) (13.1) (111.9) (44.5) (111.9)Surgery and combined therapy 0 6 2 11 7 19
(93.5) (25.2) (78.3) (23.3) (77.4)
PTLs, primary thyroid gland lymphomas; MZBL, marginal zone B-cell lymphoma of mucosa-associated lymphoid tissue type; DLBCL,diffuse large B-cell lymphoma; avg mos, average number of months of follow up; DWD, dead with disease; NED, no evidence of disease,whether alive or dead of unrelated causes; N/A, not applicable.
THYROID LYMPHOMAS 633
Am J Surg Pathol, Vol. 24, No. 5, 2000

outcome (p � 0.002; Table 7). No patients with MZBLdied with disease (mean, 91.0 mos). All 20 patients whodied with disease had DLBCL (eight patients with mixedDLBCL and MZBL, mean, 17.0 mos; 12 patients withDLBCL without MZBL, mean, 25.2 mos) with no dif-ference between mixed DLBCL and MZBL and DLBCLwithout MZBL groups (p � 0.604).
Perithyroidal soft tissue invasion was significantly as-sociated with death with disease (p � 0.025), as 18 of 20patients (90%) who died of disease had lymphomas thatdemonstrated perithyroidal extension. Likewise, thepresence of vascular invasion was significantly associ-ated with death with disease (p � 0.005). Furthermore,vascular invasion was only identified in DLBCL, andthose who died with disease had stage IIE or higherdisease. Patients with lymphomas that demonstratedabundant apoptosis (p � 0.003) and high mitotic rates(p � 0.022), histologic features more often found in theDLBCL (p � 0.0001), were significantly more likely todie with disease (Table 7). Although tumor necrosis wassignificantly more likely to be present in the DLBCL(p � 0.0001), this histologic finding was not associatedwith death with disease (p � 0.138). Similarly, grade offibrosis was not associated with death with disease (p �0.123). There was no significant difference in the num-ber of sections examined per case between the tumorcategories (p � 0.664).
DISCUSSION
PTLs typically occur in middle- to older-aged indi-viduals in the setting of lymphocytic thyroiditis with apredilection for females. Patients present with a mass inthe thyroid, usually noticeably enlarging, and commonlyhave symptoms related to compression of neck structures
by the tumor. With radioisotopic 131I scanning, a coldnodule or areas of decreased uptake are common.
PTLs demonstrate considerable diversity in architec-ture and cytology, not only from case to case, but withinthe same case. Although isolated T-cell PTLs have beenreported,1,54,59,69,82 all cases in this study were B-celllymphomas. Barring the single FCL, they fell into threegroups: MZBL, mixed DLBCL and MZBL, and DLBCLwithout MZBL. Many of our cases (71%) contained aDLBCL element, paralleling the findings in the litera-ture.9,11,13,14,23–25,34,36,41,42,51,52,54,59,64,69–71,75–78 Con-versely, almost half (47%) of our tumors that containeda DLBCL contained a MZBL, to which the term mixedDLBCL and MZBL was applied (in keeping with termi-nology of the REAL and proposed WHO classifications).The small and large cell components varied in proportionfrom case to case, requiring evaluation of several slidesto recognize the mixture. Random microscopic foci ofDLBCL or small areas of MZBL could be easily missedon cursory examination or with limited sampling. MixedDLBCL and MZBL, previously reported in other extra-nodal sites17,22,30,46,60,61,66 as well as in the thyroidgland,34,45,59,69 seem to represent approximately onethird of all thyroid lymphomas, similar to our findings(33% of all cases). Could the mixed DLBCL and MZBLcases represent de novo mixed small and large cell pre-sentations? Absolutely, but the occasional focal nature ofthe components, areas of transition between the two his-tologies, and the clinical presentation of a rapidly enlarg-ing mass lend support to the transformation theory (largecell transformation). Furthermore, many patients withPTLs have a history of sustained thyroid enlargement orgoiter before the presentation of a mass or rapid enlarge-ment of the gland, suggesting that there may have been apre-existing MZBL before the development of DLBCL(large cell transformation).3,5,6,9,11,19,23,42,71,78 In fact, astudy of a few patients with a history of persistent goiterretrospectively had MZBL that went undetected.34 More-over, immunohistochemical and molecular studies char-acterizing mixed DLBCL and MZBL in the thyroid andstomach lend further support to the transformationtheory.17,22,30,60,61
Although characteristics of lymphomas of MALT-type were more obvious in MZBL, they were also foundin the areas of DLBCL. Barring lymphocytic thyroiditis,LEL were the most common characteristic identified inthe DLBCL, accentuated with CD20 and cytokeratinstains. Although there were notable exceptions, the neo-plastic large lymphocytes were more destructive and in-vasive. Consequently, the LEL were typically fewer,smaller, and more inconspicuous than in the MZBL areasand were most often of the usual type. In our series, the“MALT ball” type of LEL, seen most often in MZBL,were unique and seemed specific for malignancy, a fea-ture that has been suggested by others.3,5,9,19,31,56 We
TABLE 7. Statistical significance of clinical andhistologic parameters for patient outcome using dead
with disease as the end point of PTLs
Variable p value
Stage greater than IE 0.0001Diffuse large cell lymphomas 0.002Rapid clinical growth 0.002Abundant apoptosis 0.003Presence of vascular invasion 0.005High mitotic rate 0.022Presence of perithyroidal extension 0.025Symptoms of compression/infiltration
of neck organs by tumor mass 0.040Modalities of treatment 0.05*Degree of fibrosis 0.123*Presence of necrosis 0.138*Duration of symptoms 0.265*Maximum tumor size 0.346*Age 0.61*
PTLs, primary thyroid gland lymphomas.* Not statistically significant.
G. A. DERRINGER ET AL.634
Am J Surg Pathol, Vol. 24, No. 5, 2000

attribute the differences in quality and quantity of LELbetween the MZBL and DLBCL components to the tu-mor’s degree of differentiation.38 In a large cell lym-phoma, the presence of a MZBL and/or LEL has beenused by some authors to classify a lymphoma as a lym-phoma of MALT-type.30,59 While LEL of the usual typeare not specific and can be seen in benign lymphoidproliferations involving the thyroid such as Hashimoto’s(lymphocytic) thyroiditis,31,47,50 LEL formed by eithersmall or large B-lymphocytes which diffusely efface thethyroid parenchyma support a lymphoma of MALT-typein the thyroid. In other words, a DLBCL in the thyroidgland that demonstrates LEL, whether or not there is anaccompanying MZBL, supports that it is a lymphoma ofMALT-type. However, because we think the ability of alymphoma of MALT-type to form LEL in the thyroid isaffected by its degree of differentiation, a lack of promi-nent LEL should not preclude the same designation.
Lymphocytic thyroiditis is almost certainly a requisitefor the development of lymphoma in the thyroid. Thefew cases (<7%) that did not have documented lympho-cytic thyroiditis may have been either inadequatelysampled or the lymphoma may have completely obliter-ated any residual thyroid tissue. Furthermore, the chro-nicity of the disease process was supported by the pres-ence of atrophy of the thyroid parenchyma and the pres-ence of fibrosis, often of a moderate to severe degree, inall cases.
In this study, FCL, as a PTL, is uncommon whendefined by the clinicopathologic features typical of thosearising in nodal sites. Of 108 cases, we made this diag-nosis in only one case, based on histologic and im-munohistochemical findings. The FCL in our series dem-onstrated a prominent follicular architecture, lacked de-finitive features of a MZBL (although there was lym-phocytic thyroiditis), and was immunoreactive for CD10.Before the understanding of the MALT concept, a sig-nificant proportion of PTLs was thought to be of folli-cle center origin.3–5,8,9,11,19,23,28,48,50,52,54,56,70 It is wellknown that extensive colonization of the germinal cen-ters of reactive follicles by neoplastic marginal zonecells in MZBL can resemble follicle center lym-phoma.34,36–38,46 The follicular pattern seen in 25 of ourcases could be attributed to this phenomenon, a findingsimilar to that of other authors.3 In many of these (n �17), features of MZBL were easily identified, raisinglittle question as to their subclassification. However, wewere impressed how eight cases closely resembled FCL.On closer observation, despite a prominent nodular ar-chitecture, marginal zone differentiation and LEL couldbe distinguished. Additionally, all were negative forbcl-2 and CD10 by immunohistochemical analysis andwere negative for t(14;18) molecular assays. A studyspecifically addressing this issue analyzed nine MZBL ofthe thyroid that demonstrated a prominent follicular pat-
tern. None of these cases were immunoreactive for CD10(on frozen instead of paraffin-embedded, formalin-fixedtissue) or showed evidence of a t(14;18) using polymer-ase chain reaction on DNA from fresh and/or paraffin-embedded tissue.37 Similar findings, using immunohis-tochemical and molecular techniques, have been reportedin gastrointestinal tract MZBL which demonstrated a fol-licular pattern.39,58 From a clinical perspective, the tu-mors in our study were not characteristic for FCL, almostalways presenting with low-stage disease without bonemarrow involvement. Only one patient presented withhigh-stage disease (IVE), with the lymphoma identifiedin the bladder and gastrointestinal tract, organs that canbe considered part of the “MALT axis.” Furthermore, theoutcomes were not characteristic of FCL. Of the patientswith a follicular pattern, only two patients died with dis-ease less than a year after presentation (mixed DLBCLand MZBL, initially stage IE disease). The remainingpatients were either alive (n � 21) or had died (n � 2)of other causes with no evidence of disease at last followup. Our only case of FCL did not yield positive t(14;18)assays. However, the negative t(14;18) assay could beexplained by a false-negative result. On the other hand,there is room for doubt about our classification of thiscase, because the patient presented with stage IIE dis-ease, had lymphocytic thyroiditis, and is alive withoutevidence of disease at last follow up, 46.5 months afterpresentation.
It is our supposition that most PTL are lymphomas ofMALT-type that have a highly variable cytomorphologicappearance and range from MZBL to “DLBCL ofMALT-type.” However, they can simulate “non-MALT-type” lymphomas.6 The architectural heterogeneity oflymphomas in the thyroid may depend on the mutationalevents leading to the development of the neoplasticclone. It is well known that centrocyte-like lymphocytesare common components of the typically cytologicallyheterogeneous MZBL. Is it possible that the neoplasticclone of some lymphomas that develop out of MALTfavors follicle center or mantle zone-like differentiationover monocytoid B-cell or plasma cell lines? This theoryis supported by the recent description of a nodular vari-ant of marginal zone B-cell lymphoma that can simulatefollicle center or even a mantle cell lymphoma.15 Al-though further study is necessary, we think, in the thy-roid, FCLs are uncommon and MCLs are exceptional.Because appropriate treatment and prognostic implica-tions depend on accurate classification, we recommendthat the diagnosis of a primary FCL or MCL in the thy-roid be made only when the tumor arises primarily in thethyroid and there is supportive immunohistochemicaland/or molecular evidence.
Plasma cells and plasmacytic differentiationwere common in our PTL. It is not difficult to sug-gest as others have3,33,36 that cases previously report-
THYROID LYMPHOMAS 635
Am J Surg Pathol, Vol. 24, No. 5, 2000

ed as extramedullary plasmacytomas of the thy-roid4,7,9,12,18,19,23,44,54,57,68,80 represent MZBL with ex-treme plasma cell differentiation. Although a few of ourMZBL cases could have been called extramedullaryplasmacytomas (EMP) by some pathologists, studiessupport that EMP are different entities from solitary plas-macytomas of the bone (SPB) and multiple myeloma(MM) (neoplasms arising from marrow cells) and thatEMP are probably MZBL with extensive plasma celldifferentiation with origin from MALT.20,33,53,79 Thistheory is based on the numerous clinicopathologic simi-larities that exist between EMP and MZBL. In our study,we found that the quantity of the plasma cell componentvaried greatly, as did other histologic characteristics ofMZBL, from one case to the next, thus indicating a dis-ease with a wide histologic spectrum. Although not allcharacteristics of MZBL were seen in our plasma cell-predominant MZBL cases, many features could be iden-tified. These findings are similar to a recent study ad-dressing this issue in which features of MZBL could beidentified in five cases from various non-thyroidal extra-medullary sites that were diagnosed as EMP originallybut thought to represent MZBL with extensive plasmacell differentiation.33 Although EMP in the thyroid couldrepresent different entities from plasma cell predominantMZBL, mounting evidence appears to support otherwise.Lastly, plasma cell dyscrasias such as MM could involvethe thyroid secondarily, but clear-cut evidence fulfillingestablished diagnostic criteria to support this unusualevent (that is, atypical plasma cell infiltrate of the mar-row, lytic bone lesions, monoclonal gammopathy) wouldbe required to support this interpretation.
The plasma cells in a MZBL of the thyroid may bereactive and part of the lymphocytic thyroiditis. Thismay account for our inability to demonstrate mono-clonality with immunohistochemistry in a number ofour cases. However, CD79a immunoreactivity washelpful in confirming the B-cell immunophenotype ofcases that were negative for L26 because of plasmacy-toid differentiation. While there may be true T-cell lym-phomas of MALT origin of the thyroid,38 becauseUCHL-1 can be expressed by some B-cell lymphomas,as observed in our study, it should not be used alone. Theuse of more specific T-cell markers such as CD3 andCD5 is recommended.
Reed-Sternberg-like cells are known to occur in awide variety of lymphoma subtypes and in reactive lym-phoid proliferations, so it is not surprising that a few ofour cases, like those in the literature,14,52,80 containedthese cells. However, we could not verify the claims ofothers that report primary thyroid Hodgkin’s lymphomain our series.19,26,42,49,76
It is difficult to compare our 5-year disease-specific survivalof 79% to the wide range of 35% to 79% reported in theliterature3,5,11,13,14,19,24,41,42,45,48,51,52,54,59,62,64,69–72,74–77,80
because of differences in population size, study design,lymphoma classification used, treatment modalities used,and statistical analyses used. As expected,14,19,76,80 anumber of clinical and histologic findings were pre-dictive of patient outcome (Table 7), although the rela-tionship of stage of disease and histologic grade arecertainly interrelated. Patients who presented with en-larging tumors or symptoms of compression of neckorgans were more likely to die with disease, as ex-pected.13,41,48,69,71,76 However, age at presentation, gen-der, and size of the tumor were not prognostic markers,contrary to other studies.5,41,43,48,71,75,76
The majority (91%) of our patients presented withstage IE or IIE disease, analogous to other re-ports.5,9,13,14,23,41,45,48,51,54,59,62,69,71,74,75 As noted inother studies,3,14,19,23,42,45,48,54,56,59,63,69,71 cervicallymph nodes were the most frequently involved site, fol-lowed by a variety of other nodal and extranodal sites,including mediastinal lymph nodes, gastrointestinal tract,bone marrow, lung, bladder, liver, and spleen. Stage ofdisease is an important prognostic indicator, with stage IEyielding an excellent clinical outcome. Stage is an im-portant prognostic indicator,13,14,19,41,48,52,54,59,71 althoughothers have not found this to be the case.5,62,74–76,80 Werealize that differences in staging modalities and vari-ability in treatment regimens can affect findings. How-ever, none of the patients with stage IE, irrespective ofhistologic grade, died with disease. Therefore, because ofprognostic implications, accurate staging is important.
It is difficult to separate clinical stage and histologicfindings as prognostic indicators, because these param-eters are intimately interrelated. In our study, only pa-tients with DLBCL (mixed DLBCL and MZBL andDLBCL without MZBL) presented with advanced stage(stage IIIE or IVE) and/or had a poor outcome. AllMZBL presented with lower stage disease (most stageIE) and none died with disease. Although evidence tosupport histology as a prognostic indicator varies in theliterature, in our study, the lymphomas, when dividedinto two main subgroups MZBL and DLBCL, demon-strated a strong statistical association with death withdisease (p � 0.002). Therefore, the distinction betweenMZBL and DLBCL in the thyroid is important and clini-cally significant. Distinction between mixed DLBCL andMZBL and DLBCL without MZBL categories appearsnot to be important. However, analysis of a larger seriesof cases may be necessary to confirm this conclusion.
Because the majority (71%) of our patients withDLBCL had a favorable outcome, we studied additionalhistologic factors to see if they had an influence on clini-cal behavior. In our series, presence of vascular invasion,abundant apoptosis, high mitotic rate, and perithyroidalsoft tissue invasion were significant histologic prognos-tic indicators. Vascular invasion5,19,56 and perithyroidal
G. A. DERRINGER ET AL.636
Am J Surg Pathol, Vol. 24, No. 5, 2000

invasion11,14,19,42,56,76,78,80 have been demonstrated to beindicators of poor clinical outcome in the past. There isno study, to our knowledge, that has demonstrated ap-optosis as a significant prognostic factor. Although all ofthese histologic features were significantly more charac-teristic of DLBCL (high mitotic activity, frank necrosis,and abundant apoptosis; p � 0.0001), with the exceptionof vascular invasion, these histologic features could beidentified without adverse effects on clinical outcome inthe MZBL group. However, there may be use in seekingthese histologic features, particularly in DLBCL, be-cause their presence may portend a greater risk of recur-rence and/or dying of disease.
As expected, chemotherapy was used in a greater per-centage of the DLBCL, but it is difficult to accuratelydetermine the impact of a single therapeutic modality onpatient survival when a wide variety of different treat-ment modalities were applied in an uncontrolled manner.Therefore, we cannot extrapolate our findings to clinicalapplication. However, authors have documented a sig-nificant relapse rate of PTLs at distant sites, attributed totreatment failure.13,21,36,41,63,75–77 Whereas a number ofstudies have reported improved survival with tumor de-bulking and local control of the tumor,13,41,67,75,76 a morefavorable patient outcome seems to follow the use ofcombined adjuvant therapy,51,63,71,75 even without tumordebulking. Our excellent overall survival rates may berelated to a combination of good local control of thetumor through the use of surgery and radiation therapyand control of disseminated disease, undetected at pre-sentation, with chemotherapy (57% of patients), despitea lower stage of disease at presentation. Chemotherapymay have treated undetected occult disseminated diseasein our patients and protected against recurrence, particu-larly for those patients with DLBCL. Further, recent im-provements in radiotherapeutic techniques and betterchemotherapy regimens may account for the better sur-vival in our patients compared with patients in earlierstudies.
In conclusion, we studied 108 PTL using recent con-cepts. PTLs typically occur in middle- to older-aged per-sons and have a predilection for females. Virtually allPTLs are lymphomas of MALT-type, arising as neoplas-tic transformations from MALT in the form of lympho-cytic thyroiditis. In keeping with the current terminol-ogy, most PTLs can be classified as MZBL or DLBCL(DLBCL of MALT-type). Mixed DLBCL and MZBL arecommon. Because the histology of PTL varies tremen-dously and can sometimes simulate other “non-MALT-type lymphomas,” specifically FCL, familiarity with thevarious patterns of PTL will prevent misclassificationand clinical confusion. The overall clinical outcome forPTL is favorable with appropriate management, but re-currence and death from disease do occur. The prognosisof PTL is dependent on both histologic findings and
clinical stage, with patients having MZBL and stageIE disease yielding the best prognosis and those withDLBCL or greater than stage IE disease having the great-est potential for a poor outcome. Further study is neededto determine the occurrence and frequency of PTLs of“non-MALT-type.” �
AcknowledgmentsThe authors thank Robin-Anne Ferris and Luther Duckett for
their expert photography, Ian W. McLean and Allen Burke fortheir statistical analysis, and Pamela Thompson for her researchassistance.
REFERENCES
1. Abdul-Rahman ZH, Gogas HJ, Tooze JA, et al. T-cell lymphomain Hashimoto’s thyroiditis. Histopathology 1996;29:455–9.
2. Aguilera NS, Bijwaard KE, Duncan B, et al. Differential expres-sion of cyclin D1 in mantle cell lymphoma and other non-Hodgkin’s lymphomas. Am J Pathol 1998;153:1969–76.
3. Anscombe AM, Wright DH. Primary malignant lymphoma of thethyroid—a tumour of mucosa-associated lymphoid tissue: reviewof seventy-six cases. Histopathology 1985;9:81–97.
4. Aozasa K, Inoue A, Katagiri S, et al. Plasmacytoma and follicularlymphoma in a case of Hashimoto’s thyroiditis. Histopathology1986;10:735–40.
5. Aozasa K, Inoue A, Tajima K, et al. Malignant lymphomas of thethyroid gland. Analysis of 79 patients with emphasis on histologicprognostic factors. Cancer 1986;58:100–4.
6. Aozasa K, Inoue A, Yoshimura H, et al. Intermediate lymphocyticlymphoma of the thyroid. An immunologic and immunohistologicstudy. Cancer 1986;57:1762–7.
7. Aozasa K, Inoue A, Yoshimura H, et al. Plasmacytoma of thethyroid gland. Cancer 1986;58:105–10.
8. Aozasa K, Nara H, Ikeda H, et al. The influence of histologic typeon survival in early extranodal non-Hodgkin’s lymphoma in headand neck. Oncology 1984;41:164–9.
9. Aozasa K, Tajima K, Tominaga N, et al. Immunologic and immu-nohistochemical studies on chronic lymphocytic thyroiditis with orwithout thyroid lymphoma. Oncology 1991;48:65–71.
10. Aozasa K, Tsujimoto M, Sakurai M, et al. Non-Hodgkin’s lym-phomas in Osaka, Japan. Eur J Cancer Clin Oncol 1985;21:487–92.
11. Aozasa K, Ueda T, Katagiri S, et al. Immunologic and immuno-histologic analysis of 27 cases with thyroid lymphomas. Cancer1987;60:969–73.
12. Beguin Y, Boniver J, Bury J, et al. Plasmacytoma of the thyroid:a case report, a study with use of the immunoperoxidase technique,and a review of the literature. Surgery 1987;101:496–500.
13. Blair TJ, Evans RG, Buskirk SJ, Banks PM, Earle JD. Radiothera-peutic management of primary thyroid lymphoma. Int J RadiatOncol Biol Phys 1985;11:365–70.
14. Burke JS, Butler JJ, Fuller LM. Malignant lymphomas of the thy-roid: a clinical pathologic study of 35 patients including ultrastruc-tural observations. Cancer 1977;39:1587–602.
15. Campo E, Miquel R, Krenacs L, et al. Primary nodal marginal zonelymphomas of splenic and MALT type. Am J Surg Pathol 1999;23:59–68.
16. Carbone PP, Kaplan HS, Musshoff K, Smithers DW, Tubiana M.Report of the Committee on Hodgkin’s Disease Staging Classifi-cation. Cancer Res 1971;31:1860–1.
17. Chan JK, Ng CS, Isaacson PG. Relationship between high-gradelymphoma and low-grade B-cell mucosa-associated lymphoid tis-sue lymphoma (MALToma) of the stomach. Am J Pathol 1990;136:1153–64.
18. Chesyln-Curtis S, Akosa AB. Primary plasmacytoma of the thy-roid. Postgrad Med J 1990;66:477–8.
19. Compagno J, Oertel JE. Malignant lymphoma and other lympho-proliferative disorders of the thyroid gland. A clinicopathologicstudy of 245 cases. Am J Clin Pathol 1980;74:1–11.
THYROID LYMPHOMAS 637
Am J Surg Pathol, Vol. 24, No. 5, 2000
20. Corwin J, Lindberg RD. Solitary plasmacytoma of bone vs. extra-medullary plasmacytoma and their relationship to multiple my-eloma. Cancer 1979;43:1007–13.
21. Doria R, Jekel JF, Cooper DL. Thyroid lymphoma. The case forcombined modality therapy. Cancer 1994;73:200–6.
22. Du M, Peng H, Singh N, Isaacson PG, Pan L. The accumulation ofp53 abnormalities is associated with progression of mucosa-associated lymphoid tissue lymphoma. Blood 1995;86:4587–93.
23. Faure P, Chittal S, Woodman-Memeteau F, et al. Diagnostic fea-tures of primary malignant lymphomas of the thyroid with mono-clonal antibodies. Cancer 1988;61:1852–61.
24. Freeman C, Berg JW, Cutler SJ. Occurrence and prognosis ofextranodal lymphomas. Cancer 1972;29:252–60.
25. Hamburger JI, Miller JM, Kini SR. Lymphoma of the thyroid. AnnIntern Med 1983;99:685–93.
26. Hardoff R, Bar-Shalom R, Dharan M, Luboshitsky R. Hodgkin’sdisease presenting as a solitary thyroid nodule. Clin Nucl Med1995;20:37–41.
27. Harris NL, Jaffe ES, Stein H, et al. A revised European-Americanclassification of lymphoid neoplasms: a proposal from the Inter-national Lymphoma Study Group. Blood 1994;84:1361–92.
28. Heimann R, Vannineuse A, De Sloover C, Dor P. Malignant lym-phomas and undifferentiated small cell carcinoma of the thyroid: aclinicopathological review in the light of the Kiel classification formalignant lymphomas. Histopathology 1978;2:201–13.
29. Holm LE, Blomgren H, Lowhagen T. Cancer risks in patients withchronic lymphocytic thyroiditis. N Engl J Med 1985;312:601–4.
30. Hsi ED, Eisbruch A, Greenson JK, et al. Classification of primarygastric lymphomas according to histologic features. Am J SurgPathol 1998;22:17–27.
31. Hsi ED, Singleton TP, Svoboda SM, Schnitzer B, Ross CW. Char-acterization of the lymphoid infiltrate in Hashimoto thyroiditis byimmunohistochemistry and polymerase chain reaction for immu-noglobulin heavy chain gene rearrangement. Am J Clin Pathol1998;110:327–33.
32. Hsu SM, Raine L, Fanger H. Use of avidin-biotin-peroxidase com-plex (ABC) in immunoperoxidase techniques: a comparison be-tween ABC and unlabeled antibody (PAP) procedures. J Histo-chem Cytochem 1981;29:577–80.
33. Hussong JW, Perkins SL, Schnitzer B, Hargreaves H, Frizzera G.Extramedullary plasmacytoma. A form of marginal zone cell lym-phoma? Am J Clin Pathol 1999;111:111–6.
34. Hyjek E, Isaacson PG. Primary B cell lymphoma of the thyroid andits relationship to Hashimoto’s thyroiditis. Hum Pathol 1988;19:1315–26.
35. Isaacson P, Wright DH. Malignant lymphoma of mucosa-associated lymphoid tissue. A distinctive type of B-cell lymphoma.Cancer 1983;52:1410–6.
36. Isaacson PG. Lymphoma of the thyroid gland. Curr Top Pathol1997;91:1–14.
37. Isaacson PG, Androulakis-Papachristou A, Diss TC, Pan L, WrightDH. Follicular colonization in thyroid lymphoma. Am J Pathol1992;141:43–52.
38. Isaacson PG, Spencer J. Malignant lymphoma of mucosa-associated lymphoid tissue. Histopathology 1987;11:445–62.
39. Isaacson PG, Wotherspoon AC, Diss T, Pan LX. Follicular colo-nization in B-cell lymphoma of mucosa-associated lymphoid tis-sue. Am J Surg Pathol 1991;15:819–28.
40. Jaffe ES, Harris NL, Diebold J, Muller-Hermelink HK. WorldHealth Organization classification of neoplastic diseases of thehematopoietic and lymphoid tissues. A progress report. Am J ClinPathol 1999;111:S8–12.
41. Junor EJ, Paul J, Reed NS. Primary non-Hodgkin’s lymphoma ofthe thyroid. Eur J Surg Oncol 1992;18:313–21.
42. Kapadia SB, Dekker A, Cheng VS, Desai U, Watson CG. Malig-nant lymphoma of the thyroid gland: a clinicopathologic study.Head Neck Surg 1982;4:270–80.
43. Kato I, Tajima K, Suchi T, et al. Chronic thyroiditis as a risk factorof B-cell lymphoma in the thyroid gland. Jpn J Cancer Res 1985;76:1085–90.
44. Kovacs CS, Mant MJ, Nguyen GK, Ginsberg J. Plasma cell lesions
of the thyroid: report of a case of solitary plasmacytoma and areview of the literature. Thyroid 1994;4:65–71.
45. Laing RW, Hoskin P, Hudson BV, et al. The significance ofMALT histology in thyroid lymphoma: a review of patients fromthe BNLI and Royal Marsden Hospital. Clin Oncol (R Coll Radiol)1994;6:300–4.
46. Li G, Hansmann ML, Zwingers T, Lennert K. Primary lymphomasof the lung: morphological, immunohistochemical and clinical fea-tures. Histopathology 1990;16:519–31.
47. Li VV. The pathology of autoimmune thyroid disease: a review.Thyroid 1994;4:333–9.
48. Logue JP, Hale RJ, Stewart AL, Duthie MB, Banerjee SS. Primarymalignant lymphoma of the thyroid: a clinicopathological analysis.Int J Radiat Oncol Biol Phys 1992;22:929–33.
49. Luboshitzky R, Dharan M, Nachtigal D, Rosen G, Honigman J.Syncytial variant of nodular sclerosing Hodgkin’s disease present-ing as a thyroid nodule. A case report. Acta Cytol 1995;39:543–6.
50. Matias-Guiu X, Esquius J. Lymphoepithelial lesion in the thyroid.A non-specific histological finding. Pathol Res Pract 1991;187:296–300.
51. Matsuzuka F, Miyauchi A, Katayama S, et al. Clinical aspects ofprimary thyroid lymphoma: diagnosis and treatment based on ourexperience of 119 cases. Thyroid 1993;3:93–9.
52. Maurer R, Taylor CR, Terry R, Lukes RJ. Non-Hodgkin lympho-mas of the thyroid. A clinico-pathological review of 29 cases ap-plying the Lukes-Collins classification and an immunoperoxidasemethod. Virchows Arch 1979;383:293–317.
53. Meis JM, Butler JJ, Osborne BM, Ordonez NG. Solitary plasma-cytomas of bone and extramedullary plasmacytomas. A clinico-pathologic and immunohistochemical study. Cancer 1987;59:1475–85.
54. Mizukami Y, Michigishi T, Nonomura A, et al. Primary lymphomaof the thyroid: a clinical, histological and immunohistochemicalstudy of 20 cases. Histopathology 1990;17:201–9.
55. Ngan BY, Nourse J, Cleary ML. Detection of chromosomal trans-location t(14; 18) within the minor cluster region of bcl-2 by poly-merase chain reaction and direct genomic sequencing of the enzy-matically amplified DNA in follicular lymphomas. Blood 1989;73:1759–62.
56. Oertel JE, Heffess CS. Lymphoma of the thyroid and related dis-orders. Semin Oncol 1987;14:333–42.
57. Ohshima M, Momiyama T, Souda S, et al. Primary plasmacytomaof the thyroid: a case report and comparative literature study be-tween Western nations and Japan. Pathol Int 1994;44:645–51.
58. Pan L, Diss TC, Cunningham D, Isaacson PG. The bcl-2 gene inprimary B cell lymphoma of mucosa-associated lymphoid tissue(MALT). Am J Pathol 1989;135:7–11.
59. Pedersen RK, Pedersen NT. Primary non-Hodgkin’s lymphoma ofthe thyroid gland: a population based study. Histopathology 1996;28:25–32.
60. Peng H, Chen G, Du M, et al. Replication error phenotype and p53gene mutation in lymphomas of mucosa-associated lymphoid tis-sue. Am J Pathol 1996;148:643–8.
61. Peng H, Du M, Diss TC, Isaacson PG, Pan L. Genetic evidence fora clonal link between low and high-grade components in gastricMALT B-cell lymphoma. Histopathology 1997;30:425–9.
62. Pledge S, Bessell EM, Leach IH, et al. Non-Hodgkin’s lymphomaof the thyroid: a retrospective review of all patients diagnosed inNottinghamshire from 1973 to 1992. Clin Oncol (R Coll Radiol)1996;8:371–5.
63. Pyke CM, Grant CS, Habermann TM, et al. Non-Hodgkin’s lym-phoma of the thyroid: is more than biopsy necessary? World J Surg1992;16:604–9.
64. Rasbach DA, Mondschein MS, Harris NL, Kaufman DS, WangCA. Malignant lymphoma of the thyroid gland: a clinical andpathologic study of twenty cases. Surgery 1985;98:1166–70.
65. Reid AH, Cunningham RE, Frizzera G, O’Leary TJ. bcl-2 rear-rangement in Hodgkin’s disease. Results of polymerase chain re-action, flow cytometry, and sequencing on formalin-fixed, paraf-fin-embedded tissue. Am J Pathol 1993;142:395–402.
66. Rivas C, Echezarreta G, Garcia R, et al. A multiparametric study
G. A. DERRINGER ET AL.638
Am J Surg Pathol, Vol. 24, No. 5, 2000

of malignant lymphoma of mucosa associated lymphoid tissue(MALT). Leuk Lymphoma 1992;8:87–96.
67. Rosen IB, Sutcliffe SB, Gospodarowicz MK, Chua T, SimpsonWJ. The role of surgery in the management of thyroid lymphoma.Surgery 1988;104:1095–9.
68. Rubin J, Johnson JT, Killeen R, Barnes L. Extramedullary plas-macytoma of the thyroid associated with a serum monoclonal gam-mopathy. Arch Otolaryngol Head Neck Surg 1990;116:855–9.
69. Sasai K, Yamabe H, Haga H, et al. Non-Hodgkin’s lymphoma ofthe thyroid. A clinical study of twenty-two cases. Acta Oncol 1996;35:457–62.
70. Sirota DK, Segal RL. Primary lymphomas of the thyroid gland.JAMA 1979;242:1743–6.
71. Skarsgard ED, Connors JM, Robins RE. A current analysis ofprimary lymphoma of the thyroid. Arch Surg 1991;126:1199–203.
72. Souhami L, Simpson WJ, Carruthers JS. Malignant lymphoma ofthe thyroid gland. Int J Radiat Oncol Biol Phys 1980;6:1143–7.
73. Staunton MD, Greening WP. Clinical diagnosis of thyroid cancer.BMJ 1973;4:532–5.
74. Tennvall J, Cavallin-Stahl E, Akerman M. Primary localized non-Hodgkin’s lymphoma of the thyroid: a retrospective clinicopatho-logical review. Eur J Surg Oncol 1987;13:297–302.
75. Tsang RW, Gospodarowicz MK, Sutcliffe SB, et al. Non-
Hodgkin’s lymphoma of the thyroid gland: prognostic factors andtreatment outcome. The Princess Margaret Hospital LymphomaGroup. Int J Radiat Oncol Biol Phys 1993;27:599–604.
76. Tupchong L, Hughes F, Harmer CL. Primary lymphoma of thethyroid: clinical features, prognostic factors, and results of treat-ment. Int J Radiat Oncol Biol Phys 1986;12:1813–21.
77. Vigliotti A, Kong JS, Fuller LM, Velasquez WS. Thyroid lympho-mas stages IE and IIE: comparative results for radiotherapy only,combination chemotherapy only, and multimodality treatment. IntJ Radiat Oncol Biol Phys 1986;12:1807–12.
78. Walt AJ, Woolner LB, Black BM. Primary malignant lymphomaof the thyroid. Cancer 1957;10:663–77.
79. Wiltshaw E. The natural history of extramedullary plasmacytomaand its relation to solitary myeloma of bone and myelomatosis.Medicine (Baltimore) 1976;55:217–38.
80. Woolner LB, McConahey WM, Beahrs OH, Black BM. Primarymalignant lymphoma of the thyroid. Review of forty-six cases. AmJ Surg 1966;111:502–23.
81. Wright CF, Reid AH, Tsai MM, et al. Detection of Epstein-Barrvirus sequences in Hodgkin’s disease by the polymerase chainreaction. Am J Pathol 1991;139:393–8.
82. Yamaguchi M, Ohno T, Kita K. Gamma/delta T-cell lymphoma ofthe thyroid gland [Letter]. N Engl J Med 1997;336:1391–2.
THYROID LYMPHOMAS 639
Am J Surg Pathol, Vol. 24, No. 5, 2000





























