Embed Size (px)
Citation preview

Med Electron Microsc (1998) 31:207-215 �9 The Clinical Electron Microscopy Society of Japan 1998
Salma Khan �9 Hidetaka Katabuchi �9 Yoshinori Okamura Sayuri Matsnmura �9 Ryuji Nagai �9 Hideyuki Ohtake Yoshito Snenaga �9 Yukitoshi Fukumatsn �9 Yukio Ikuta Hitoshi Okamura
Malignant mesenchymal tumors of the ovary in three cases: histology, immunohistochemistry, and ultrastructural observations
Received: June 30, 1998 / Accepted: August 10, 1998
Abstract Primary ovar ian sarcoma is a rare neoplasm. The diagnosis somet imes becomes difficult by light microscopic examinat ion alone because of the rar i ty and he terogenei ty of these tumors. Immunohis tochemica l and ul t rastructural studies are very useful for diagnosis. Here , we describe two cases of ovarian sarcomas: f ibrosarcoma and le iomyosarcoma, and a case of carcinosarcoma (homolo- gous mal ignant mixed mii l ler ian tumor). In addi t ion to his- tological findings, immunohis tochemical and ul t ras t ructural observat ion was under t aken to make a final diagnosis. Clinical outcome was variable in the three cases. It was unl ikely to be re la ted to the disease stage or t rea tment , such as surgical excision or ant icancer drugs, whereas the mitot ic index may be an impor tan t prognost ic indicator in ovarian sarcomas.
Key words Ovary �9 Sarcoma �9 Immunohis tochemis t ry �9 Elec t ron microscopy
Introduction
Ovarian sarcoma must be dif ferent ia ted from pr imary ova- rian neoplasm as well as from metas ta t ic and disseminated neoplasms affecting the ovary. A m o n g all types of ovarian neoplasms, pr imary ovar ian sarcomas are very rare. Shakfeh and Woodru f f classified these tumors so as to iden-
Fibrosarcoma was presented in the 19th Annual Meeting of the Clini- cal Electron Microscopy Society of Japan, Tokyo, on September 17, 1987. Leiomyosarcoma and carcinosarcoma were presented in the 26th Annual Meeting of the Clinical Electron Microscopy Society of Japan, Kochi, on October 5, 1994
S. Khan �9 H. Katabuchi ([]) . Y. Okamura. S. Matsumura. R. Nagai. H. Ohtake. Y. Suenaga. Y. Fukumatsu �9 Y. Ikuta. H. Okamura Department of Obstetrics and Gynecology, Kumamoto University School of Medicine, 1-1-1 Honjo, Kumamoto 860-8556, Japan Tel. +81-96-373-5269; Fax +81-96-363-5164 e-mail: [email protected]
tify p robab le histogenesis and to offer some clues for be t te r therapy based on the cl inicopathological fea tures ) How- ever, histogenesis still remains controversial . Moreover , the rar i ty and heterogenei ty of these tumors may result in dif- ferent in terpre ta t ions by individual pathologists. Immuno- histochemical and ul t ras t ructural studies are very helpful techniques to elicit the histogenesis of these rare tumors in individual cases. 2'3 Here, we describe two cases of ovarian sarcomas and one case of carcinosarcoma by light micro- scopic, immunohis tochemical , and ul t rastructural analysis, and the usefulness of these techniques in his topathological diagnosis is evaluated.
Materials and methods
Patients
Case 1, a 12-year-old premenarcha l Japanese girl, was ad- mi t ted to our hospital with a complaint of ur inary retention. On physical examinat ion, a large mass extending from the pelvis to the level of the umbilicus was pa lpa ted in her lower abdomen, but there was no ascites, p leural effusion, or nevus. Plasma C A 125 level was 91.0U/ml (normal range, <37.0U/ml) , and on endocrinological examinat ion, the p lasma tes tos terone level was 98ng/dl (normal range, 15- 30ng/dl, for a 10- to 12-year-old girl). On laparo tomy, a solid mass of the size of a newborn ' s head was found to have replaced the left ovary, and a complete excision was done. The tumor mass was intact with a smooth surface measuring 14 • 10 • 7.5cm and weighing 633g. The cut surface was solid and chalky white, with some areas of cystic forma- tion. The ovarian tumor was histologically d iagnosed as f ibrosarcoma and staged as F I G O (Internat ional Federa - tion of Gynecology and Obstetr ics) IA. Dur ing the 12 years since the surgery, she has been comple te ly well with no evidence of recurrence.
Case 2, a 49-year-old, gravida 4, pa ra 3, Japanese woman came to our hospital with a complain t of a mass in her lower abdomen. On physical examinat ion, it was suspected to be a

208
left ovarian tumor. Plasma carcinoembryonic antigen (CEA), CA 19-9, and CA 125 were all within normal limits. On laparotomy, a left ovarian solid mass, the size of a man's fist, was seen. It had loose adhesion to lateral peritoneum and omentum with fibrous tissue but no capsular adhesion. The uterus and right ovary were grossly normal. A total abdominal hysterectomy with bilateral salpingo- oophorectomy was performed. The left ovarian mass was 11.5 • 11 • 8cm in size and weighed 475g. The cut surface was firm and pearly white, showing whirled intersecting fascicles; moreover, a focal, small variegated hemorrhage and necrosis was admixed. A well-circumscribed soybean- sized node was present in the myometrium. Peritoneal sur- faces were free of disseminated tumors. A FIGO stage IA ovarian leiomyosarcoma was diagnosed, and subsequently she received intravenous combination chemotherapy (cy- clophosphamide, adriamycin, and cis-platinum). At 35 months after surgery, she developed recurrence with mul- tiple lung tumors. The patient died of recurrent disease 4.5 years following initial diagnosis.
Case 3, a 44-year-old, gravida 4, para 2, Japanese woman complained of a lower abdominal mass and was referred to our hospital. On physical examination, a large solid mass was found to occupy the entire lower abdomen. Tumor markers were measured as CEA, 8.2ng/ml (normal range, <2.0ng/ml); CA 19-9, 60.5U/ml (normal range, <37.0U/ ml); and CA 125, 141.2U/ml. Routine hemogram showed marked anemia (hemoglobin, 7.5g/dl). She was given a blood transfusion and underwent laparotomy. A large solid and cystic mass was found that arose from the left ovary and occupied the whole lower abdomen. The surface of the cystic part was smooth but the solid counterpart was ad- hered to the pelvic wall. Uterus and right adenexa were apparently normal.
Radical hysterectomy, pelvic and paraaortic lymph node dissection, and omentectomy were performed. The left ova- rian mass measured 21 x 16 • 14cm and weighed 4550g. The cut surface was tan/brown with focal hemorrhage. Cysts were filled with chocolate-colored material. The his- tological diagnosis of the ovarian tumor was carcino- sarcoma (homologous malignant mixed mtillerian tumor). The clinical stage was FIGO IIIA because there was evi- dence of dissemination of the tumor cells to the posterior pelvic wall, but no metastasis of lymph nodes or omentum was detected. Three courses of combination chemotherapy (cyclophosphamide, adriamycin, cis-platinum) were admin- istered following surgical excision. Unfortunately, she was readmitted 2 months later with extensive metastasis all over the body and died immediately.
Immunohistochemistry
Paraffin sections for immunohistochemistry were cut at 4 b~m and incubated with eight antibodies: mouse antihuman cytokeratin gp 56-kDa monoclonal antibody (Immunotech, Marseilles, France) diluted 1 : 20, mouse antihuman epithe- lial membrane antigen (EMA) monoclonal antibody (Dakopatts, Glostrup, Denmark) diluted 1:200, mouse an- tihuman CEA monoclonal antibody (Dakopatts) diluted 1:100, mouse antihuman vimentin monoclonal antibody (Dakopatts) diluted 1 : 10, mouse antihuman desmin mono- clonal antibody (Dakopatts) diluted 1:100, mouse anti- human (,-smooth muscle actin monoclonal antibody (Dakopatts) diluted 1:50, rabbit antihuman myoglobin polyclonal antibody (Dakopatts) diluted 1:100, and rabbit antihuman a-fetoprotein polyclonal antibody (Dakopatts) diluted 1 : 100.
Immunoperoxidase staining of cytokeratin, EMA, CEA, vimentin, desmin, and a-smooth muscle actin was per- formed by the avidin-biotin peroxidase complex (ABC) method with a Vectastain ABC kit (Vector, Burlingame, CA, USA). For the detection of myoglobin and c,- fetoprotein, the peroxidase and antiperoxidase method was performed with a Dako Pap kit (Dako, Carpenteria, CA, USA). Peroxidase activity was visualized with 3,3'- diaminobenzidine (Sigma, St. Louis, MO, USA) as a sub- strate in Tris-HCL buffer (0.5mg/ml, pH 7.6) containing 0.01% H202. Nuclear staining was performed with 1% me- thyl green in water. Appropriate positive controls were used for each immunoprotein, and negative controls were used by omitting the primary antibody.
Electron microscopy
In case 1, several small pieces of ovarian tumor were fixed in chilled 2.5% glutaraldehyde in 0.1M cacodylate buffer (pH 7.4). For cases 2 and 3, formalin-fixed, paraffin-embedded tissue specimens were dewaxed and fixed in cacodylate- buffered glutaraldehyde. They were postfixed in osmium tetroxide dissolved in cacodylate buffer, dehydrated in a graded series of ethanol and propylene oxide, and embed- ded in epoxy resin. Tissue blocks were cut into ultrathin sections with a microtome (Ultrotome Nova, LKB, Uppsala, Sweden) and stained with 1% toluidin blue. Ultrathin sections were stained with lead citrate and uranyl acetate and observed with a 12-A electron microscope (Hitachi, Tokyo, Japan).
Light microscopy
Tissue specimens obtained at the initial operation were fixed in 10% buffered formalin for preparation of routine paraffin sections and stained with hematoxylin and eosin. Selected sections were stained with periodic acid-Schiff (PAS) reaction, alcian blue, oil red-O, and phosphotungstic acid-hematoxylin (PTAH) stains.
Results
Fibrosarcoma
The ovarian tumor showed dense cellularity with spindle cells arranged in a herringbone pattern and with small to moderate amounts of collagen fibers (Fig. la) and with poorly defined eosinophilic cytoplasm; the tumor cells

209
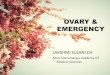
Fig. la,b. Photomicrograph of the ovarian fibrosarcoma in case 1. a Densely packed spindle cells are arranged with a small amount of collagen fibers. These tumor cells showed nuclear pleomorphism, and
mitotic figures are relatively frequent, b Numerous small round gran- ules are distributed intracetlularly or extracellularly (hematoxylin and eosin stain). • (a), • (h)
showed a large nucleocytoplasmic ratio. Although cellular pleomorphism was mild, mitotic figures were 5 per 10 high- power fields (HPF). In oil red-O stain, lipid droplets were found in the cytoplasm of the tumor cells. Numerous small round granules were observed in the cytoplasm of the tu- mor cells or extracellularly around the cysts (Fig. lb). These granules were histochemically negative for a-fetoprotein. Tumor cells showed negative reactivity to desmin, c~- smooth muscle actin, and myoglobin but were positive for vimentin. An electron microscopy study revealed the ma- jority of the tumor cells were spindle shaped and had scanty cytoplasm, while some polygonal or stellate tumor cells pos- sessed abundant cytoplasm (Fig. 2). Their nuclei were large and irregular in outline without marked peripheral con- densation of chromatin, and one or two large nucleoli were present. Besides lipid droplets of variable electron density, a bundle of their filaments exhibiting focal con- densation was observed in the cytoplasm (Fig. 3a). Numer- ous cytoplasmic granules lacked limiting membranes, showed marked homogeneous osmiophilia (Fig. 3b), and differed in ultrastructure from hyaline globules frequently observed as multivesicular bodies in an endodermal sinus tumor.
Leiomyosarcoma
Intersecting fascicles of large spindle cells formed the ova- rian tumor and also the loci of the hemorrhage, and necrosis was prominent (Fig. 4a). Significant nuclear atypia was ob- served, and mitotic counts were 23 per 10 HPF (Fig. 4b). A myometrial node constituted uniform smooth muscle cells without nuclear atypia and mitosis, presenting typical leiomyoma. Immunohistochemical staining revealed the presence of desmin and a-smooth muscle actin (Fig. 5a) in the cytoplasm, whereas myoglobin was negative in the tu- mor cells. On electron microscopy, the spindle-shaped cells possessed an elongated nucleus with prominent nuclear cleft, and dense bodies existing as a close bundle of thin to intermediate filaments were observed in the cyto- plasm (Fig. 5b).
Carcinosarcoma
The ovarian tumor was composed histologically of malig- nant epithelium and sarcomatous stroma. The epithelial component was characterized by glandular formation (Fig.

210
Fig. 2. Electron photomicrograph of the ovarian fibrosarcoma. Polygonal or stellate tumor cells have abundant cytoplasm with marked irregular nuclear profiles. Intervening collagen fibers (Co) are present (uranyl acetate and lead citrate stain)
Fig. 3a,b. Electron photomicrograph of the ovarian fibrosarcoma, a The tumor cell possesses a bundle of thin filaments (arrow) in the cytoplasm, b Cytoplasmic granules show homogeneous osmiophilia
without a limiting membrane (uranyl acetate and lead citrate stain). N, nucleus

211
Fig. 4a,b. Photomicrograph of the ovarian leiomyosarcoma in case 2. a Highly dense spindle cells arc seen in the lower-l@ side and extensive necrosis is located at the upper right, b Tumor cells are arranged in an
orderly fascicular pattern, and their nuclei show mild to moderate atypia with many mitotic figures (hematoxylin and eosin stain). • (a), xS0 (b)
6). Irregularly shaped glands were embedded in dense stroma and surrounded by extracellular mucin. The cells lining the glands were stratified and possessed hyper- chromatic nuclei with coarse chromatin, mitosis, and intracytoplasmic mucin (Fig. 6). Immunohistochemically, C E A as well as cytokeratin and E M A were expressed in nearly all the epithelial component. Sarcomatous areas were admixed with spindle or polygonal cells accom- panied with fewer collagen fibers (Fig. 7a). The polygonal cells had a large amount of bright eosinophilic cytoplasm (Fig. 7b). Nuclei were oval to round, with prominent nucleoli, and were sometimes multinucleated. The mitotic count was 23 per 10 HPF. By P T A H stain, cross-striations were not .shown in the cytoplasm. The tumor cells immunohistochemically showed strong reactivity with c~- smooth muscle actin (Fig. 8a), as well as desmin, but no reactivity was seen with myoglobin. On electron microscopy, nuclei were notched, and the cytoplasm contained parallel bundles of intermediate filaments with focal densities (Fig. 8b). The presence of Z-bands or their precursors was not demonstrable in these tumor cells.
Discussion
Ovarian sarcomas are rare neoplasms. They may be classi- fied into four different groups such as pure sarcoma, mixed sarcomas, malignant mixed m011erian tumor, and unclassi- fied. I Fibroma/fibrosarcoma is generally believed to be de- rived from differentiated mesenchymal cells of ovarian stroma, i.e., fibroblasts. Ovarian fibrosarcoma occurring in adolescents or young adults is found to be associated with nevoid basal carcinoma syndrome, 4 but other diseases concerning the syndrome were not evident in our 12-year- old premenarchal girl with fibrosarcoma. Differential diagnosis may be spindle cell tumors including cellular fibroma, thecoma, leiomyoma, and leiomyosarcoma. Fi- broma/fibrosarcoma lacks bundles of cytoplasmic smooth muscle-type filaments and does not express c~-smooth muscle actin. Ovarian fibroma or cellular fibroma shows cellular atypia but lacks mitotic activity; in contrast, great mitotic activity is characteristic of fibrosarcoma. In our present case, cellular atypia was not prominent, but accord- ing to the histopathological classification by Prat and

212
Fig. 5a,b. Immunohistochemistry and electron photomicrograph of the leiomyosarcoma in case 2. a a-Smooth muscle actin is immuno- histochemically positive in the tumor cells (methyl green stain) • 100,
b The cytoplasm contains numerous elongated intermediate filaments. They are aligned longitudinally and have associated dense bodies (DB) (uranyl acetate and lead citrate stain). N, nucleus
Fig. 6, Photomicrograph of the carcinosarcoma in case 3. The carcinomatous element is characteristic of irregularly shaped glands, surrounded by mucin. Epithelial cells are Iining the glands and papiI-
lary proliferation is seen. These cells are stratified with moderate nuclear atypia (hematoxylin and eosin stain). •

213
Fig. 7a,b. Photomicrograph of the carcinosarcoma, a Spindle and polygonal cells appear dense in the sarcomatous element, b The cytoplasm of the polygonal cells is abundant with eosinophilic and numerous mitotic figures (hematoxylin and eosin). • (a), • 100 (b)
Scully, ~ her neoplasm was diagnosed as fibrosarcoma with its mitotic index (5 mitotic figures per 10 HPF). Primary ovarian leiomyosarcoma is a very rare subset of ovarian sarcoma with only 27 well-documented cases in the litera- ture. 6 Ovarian leiomyoma/leiomyosarcoma probably arises from the smooth muscle cells of the walls of blood vessels in the ovary or smooth muscle cells in the ovary itself] In our case, by using immunohistochemistry and electron micros- copy, the demonstrat ion of expression of c~-smooth muscle actin and desmin, and the existence of dense bodies as bundles of thin to intermediate filaments in the cytoplasm, were conclusive of a smooth muscle tumor.
The malignant mixed mtillerian tumor is a biphasic tumor containing both a malignant epithelial and a sarcomatous component. Most ovarian malignant mixed mtillerian tumors were thought to arise from the ovarian surface epithelium or the immediately subjacent stroma. Recently, tumor of the female genital tract, including ova- rian carcinosarcoma, has been shown to be closely related to carcinoma. Sreenan and Hart described that these should no longer be regarded as a subtype of sarcoma, s On the other hand, some authors have discussed that the stromal component of endometriosis is also their precursor, 2'9 but we found no endometriotic loci in any of our resected ma- terials. In our case of malignant mixed mtillerian tumor, the
epithelial component was diagnosed as mucinous adeno- carcinoma. The sarcomatous area consisted of spindle or polygonal cells. In particular, the polygonal cells were char- acterized by abundant pale eosinophilic cytoplasm. How- ever, such tumor cells did not possess cross-striation in their cytoplasm. Immunohistochemistry demonstrated that both desmin and c~-smooth muscle actin were positive in their cytoplasm, but myoglobin was negative. Ultrastructural ob- servations detected only the dense bodies in their cytoplasm without cross-striation, providing that the sarcomatous component was leiomyosarcoma. In cases 2 and 3, electron microscopy proved to be a suitable method for identifying smooth muscle cells, even though paraffin-embedded tis- sues were used as the sample sources.
The clinical outcome of ovarian sarcomas is variable without relation to the treatment. Ovarian fibrosarcoma is likely to have a better prognosis, compared to the same tumor occurring in sites other than the ovary, when its surgical excision is complete, 5'~~ and this is also observed as in our case of fibrosarcoma. The prognosis of ovarian leiomyosarcoma remains greatly variable. The present case of leiomyosarcoma reflected distant metastasis even though she was treated with chemotherapy followed by complete surgical excision. Malignant mixed mtillerian tumor of the ovary is usually associated with poor prognosis. Some au-

214
Fig. 8a,b. Immunohistochemistry and electron photomicrograph of the carcinosarcoma, a The tumor cells in the sarcomatous component are partly stained with a-smooth muscle actin (methyl green stain). • 100. b The nuclear (N) contour is irregular. Dense bodies (DB) are located
as a close bundle of intermediate filaments in the cytoplasm, but no intracytoplasmic cross-striation is visible (uranyl acetate and lead cit- rate stain)
thors pointed out that the homologous tumors have a better prognosis than the heterologous tumors such as rhabdomyosarcoma or chondrosarcoma. ~1-13 On the con- trary, others commented that there was probably no differ- ence in mortality between heterologous and homologous tumors. 14 Our case of homologous malignant mixed maller ian tumor showed very poor prognosis.
Considering these three cases of primary ovarian sar- coma, the mitotic index is likely to be the most significant prognostic indicator, as observed by othersJ 'a The high mi- totic index (23 per 10 HPF) in our case of leiomyosarcoma in case 2 reflected a poor prognosis, even though the tumor was localized in the unilateral ovary. In contrast, the low mitotic count (5 per 10 HPF) in the case of fibrosarcoma in case 1 at stage Ia showed low malignant potential, without any long- term evidence of recurrence after the initial treatment.
In conclusion, we emphasize that in addition to light microscopic findings, immunohistochemical and ultrastruc- tural criteria should be included in the diagnosis of all cases of primary ovarian sarcomas. Although the mitotic index may be a significant prognostic indicator in these tumors, the subsequent t reatment after surgery remained inconclu- sive. Further studies should be tried to find efficacious treatments.
References
1. Shakfeh SM, Woodruff JD (1987) Primary ovarian sarcomas: re- port of 46 cases and review of the literature. Obstet Gynecol Surv 42:331-349
2. Friedman HD, Mazur MT (1991) Primary ovarian leiomyo- sarcoma: an immunohistochemical and ultrastructural study. Arch Pathol Lab Med 115:941-945
3. Geisinger KR, Dabbs D J, Marshal RB (1987) Malignant mixed mesodermal tumors: an ultrastructural and immunohis- tochemical analysis with histologenetic considerations. Cancer (Phila) 59:1781-1790
4. Kraemer BB, Silva GE, Sneige N (1984) Fibrosarcoma of ovary. A new component in the nevoid basal cell carcinoma syndrome. Am J Surg Pathol 8:231-236
5. Prat J, Scully RE (1981) Cellular fibromas and fibrosarcomas of the ovary. A comparative clinicopathologic analysis of seventeen cases. Cancer (Phila) 47:2663-2670
6. Rasmussen CC, Skilling JS, Sorosky JI, Lager D J, Buller RE (1997) Stage IIIC ovarian leiomyosarcoma in a premenopausal woman with multiple recurrences: prolonged survival with surgical therapy. Gynecol Oncol 66:519-525
7. Okamura H, Virutamasen P, Wright KH, Wallach EE (1972) Ova- rian smooth muscle in the human being, rabbit, and cat. Am J Obstet Gynecol 112:183-191
8. Sreenan JJ, Hart WR (1995) Carcinosarcomas of the female genital tract. A pathologic study of 29 metastatic tumors: further evidence for the dominant role of the epithelial component and the conver- sion of the theory of histogenesis. Am J Surg Pathol 19:666-674

9. Balaton A, Vaury P, Imbert M, Mussy M (1987) Primary leiomyosarcoma of ovary: a histological and immunohistochemical study. Gynecol Oncol 28:116-120
10. Stellato G, Di Bontio M, Tramontana S (1995) Primary fibrosarcoma of the ovary. Acta Obstet GynecoI Scand 74:649- 652
11. Dictor M (1985) Malignant mixed mesodermal tumor of the ovary: a report of 22 cases. Obstet Gynecoi 65:720-724
12. Costa MJ, Khan R, Judd R (1991) Carcinosarcoma (malignant mixed mullerian [mesodermal] tumor) of the uterus and ovary:
215
correlation of clinical, pathologic, and immunohistochemical fea- tures in 29 cases. Arch Pathol Lab Med 115:583-590
13. de Brito PA, Silverberg SG, Orenstein JM (1993) Carcinosarcoma (malignant mixed mullerian tumors) of the female genital tract: immunohistochemicat and ultrastructuraI analysis of 28 cases. Hum Pathol 24:132-142
14. Morrow CP, d'Ablang G, Brady LW, Blessing JA, Hreshchyshyn MM (1984) A clinical and pathologic study of 30 cases of malignant mixed mullerian epithelial and mesenchymal ovarian tumors: a gynecologic oncology group study. Gynecol Oncol 18:278-292