Embed Size (px)
Citation preview

Malnutrition in surgical patients
Surgical Nutrition Training ModuleLevel 1
Philippine Society of General SurgeonsCommittee on Surgical Training

Objectives
• To define malnutrition and discuss its impact on the surgical patient
• To identify malnutrition in hospitalized surgical patients

MALNUTRITION IS A SYNDROME
Malnutrition syndrome: features
• Wasting / marasmus• Cachexia• Protein-energy malnutrition• Sarcopenia• Failure to thrive• Obesity
Gordon Jensen. International Guidelines: malnutrition syndrome; ASPEN Congress 2008, Chicago.

Malnutrition syndrome: features
• Wasting/marasmus– Loss of body cell mass without underlying
inflammatory condition; Pure starvation
• Cachexia– Loss of body cell mass with underlying
inflammatory condition; Cytokine mediated– Cancer: moderate to advanced stage
Gordon Jensen. International Guidelines: malnutrition syndrome; ASPEN Congress 2008, Chicago.
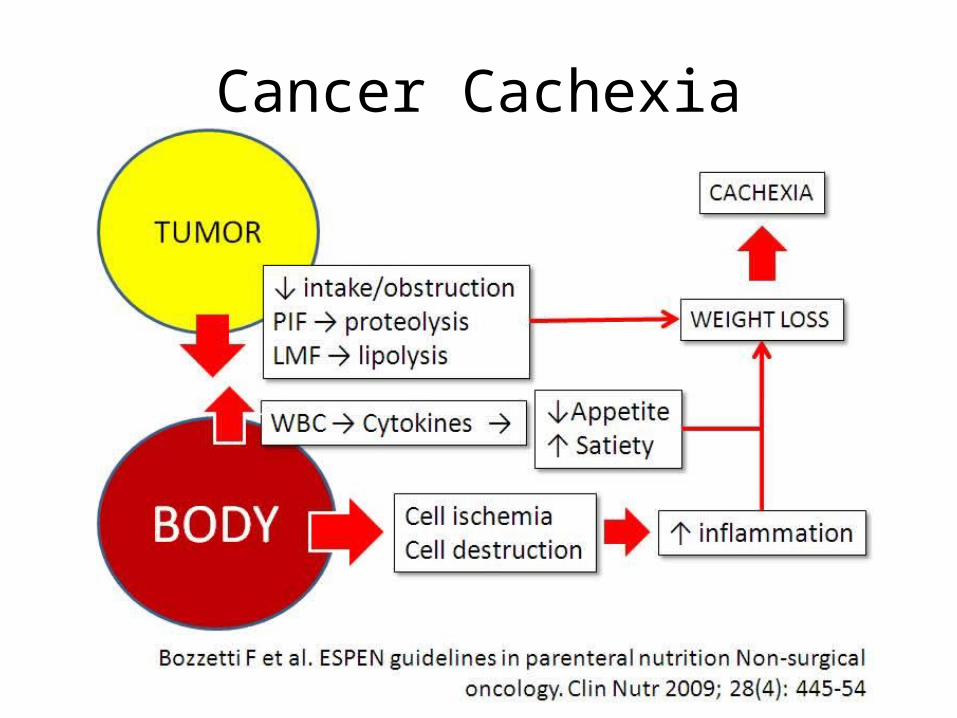
Cancer Cachexia

Inflammation in cachexia

Malnutrition syndrome: features
• Protein-energy malnutrition– In modern healthcare this is often acute metabolic
derangement driven by pro-inflammatory state; not classic PEM with clinical and metabolic evidence for reduced intake of protein and energy
Gordon Jensen. International Guidelines: malnutrition syndrome; ASPEN Congress 2008, Chicago.

Malnutrition syndrome: features
• Sarcopenia (mostly geriatric)– Age related loss of muscle; often with
inflammation / cachexia overlap
• Failure to thrive– Classic pediatric growth failure syndrome– Now also applied in clinical practice to
undernourished older persons in functional or cognitive decline (Alzheimer’s disease)
Gordon Jensen. International Guidelines: malnutrition syndrome; ASPEN Congress 2008, Chicago.

SarcopeniaCOMPLICATIONS

Malnutrition syndrome: features
• Obesity: WHO (World Health Organization) criteria– BMI (Body Mass Index) = Weight in kg / Height in
meter / Height in meter• 30 - 34.9 Obese class 1• 35 - 39.9 Obese class 2• 40 and above Obese class 3• 40 - 50 Morbidly Obese• > 50 Super-Obese
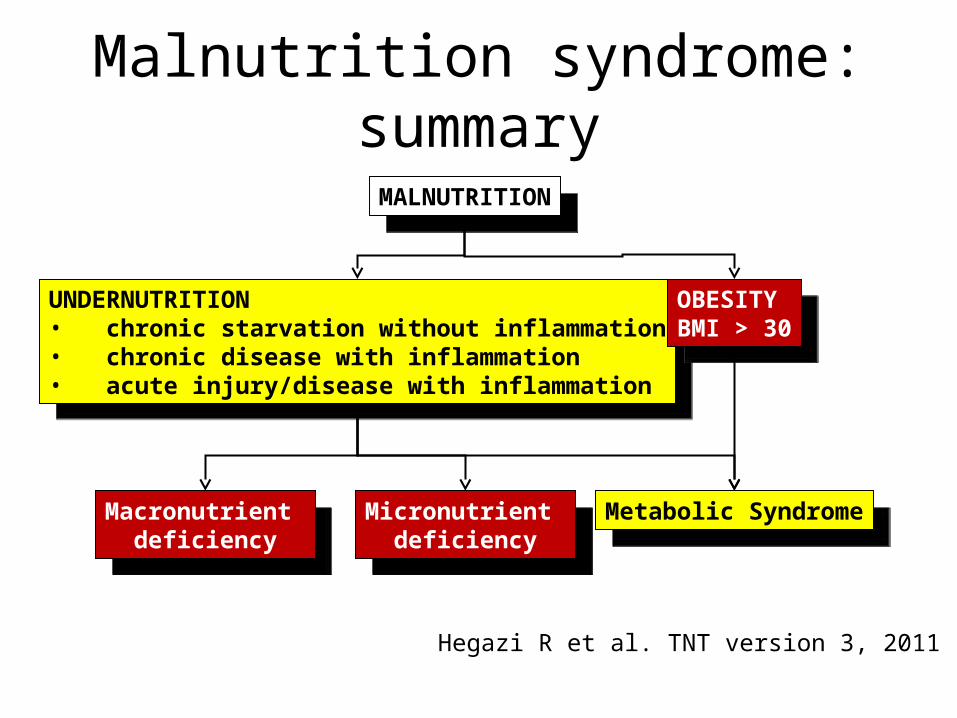
Malnutrition syndrome: summary
UNDERNUTRITION• chronic starvation without inflammation• chronic disease with inflammation• acute injury/disease with inflammation
UNDERNUTRITION• chronic starvation without inflammation• chronic disease with inflammation• acute injury/disease with inflammation
OBESITYBMI > 30
OBESITYBMI > 30
Macronutrient deficiency
Macronutrient deficiency Micronutrient
deficiency
Micronutrient deficiency Metabolic Syndrome
Metabolic Syndrome
MALNUTRITIONMALNUTRITION
Hegazi R et al. TNT version 3, 2011

Malnutrition process
• It is a continuum– Starts with poor intake– Effect of initiation and progress of the disease
process: severity of disease and adequacy of intake
– Effect of efforts to correct both body composition and disease process

Malnutrition concerns
• Lean body mass– Structure and function– Body composition capacity for healing and
recovery– Quality of life
• Energy reserves– Function– Optimal utilization of substrates and protein
synthesis

Malnutrition syndrome: features and effects
• Wasting / marasmus• Cachexia• Protein-energy
malnutrition• Sarcopenia• Failure to thrive• Obesity
• Loss of lean body mass• Structural and
functional impairment• Energy utilization
problems• Antioxidant capabilities• Increased complications
and mortality
Gordon Jensen. International Guidelines: malnutrition syndrome; ASPEN Congress 2008, Chicago.

EFFECT OF SURGERY ON THE PATIENT

Surgery = injury
SURGERY
INFLAMMATION•Metabolic response•Endocrine response
POST-SURGERY STATUS•Resolution of inflammation•Wound healing•Recovery
COMPLICATIONS•Malnutrition•Inadequate intake•Current body composition•Pre-op preparation (NPO, antibiotic, fluid balance)•Post-op management

Surgery, wound healing, and nutritional status
SURGERY
INFLAMMATION
↑WBC + ↑ENERGY
↑CELL MULTIPLICATION + ↑NUTRIENT NEEDS
WOUND HEALING
NORMAL POOR ± COMPLICATIONS
No Malnutrition Malnutrition

↑Energy needs = ↑ free radicals
Robbins Basic Pathology 7th edition. Kumar, Cotran, Robbins editors. 2003.

Role of nutrition in surgery
LIPIDS
MUSCLEMALTGALT
CARBO
Alanine
WBC, RBC, FIBROBLASTS
All WBC, RBC, FACTORSBone Marrow
MALT, GALTB-cells
T-cells
PlateletsGlutamine
Organs Affected• epithelium• connective tissue• angiogenesis• complement system
INFLAMMATIONANTIOXIDANTSWOUND HEALINGINFECTION CONTROL
Body composition
NEED TO KEEP ALL NUTRIENTS IN STEADY SUPPLY AS NEEDED

Nutrition and wound healing
Wound healing
Surgery Nutritional status
Severe malnutrition
Good Prolonged
Complications
Normal
Body reserves:• skeletal muscle – alanine and glutamine• fat reserves – energy (long term)

Malnutrition in surgical patientsSurgical patients• 9% of moderately
malnourished patients → major complications
• 42% of severely malnourished patients → major complications
• Severely malnourished patients are four times more likely to suffer postoperative complications than well-nourished patients
Detsky et al. JAMA 1994 Detsky et al. JPEN 1987
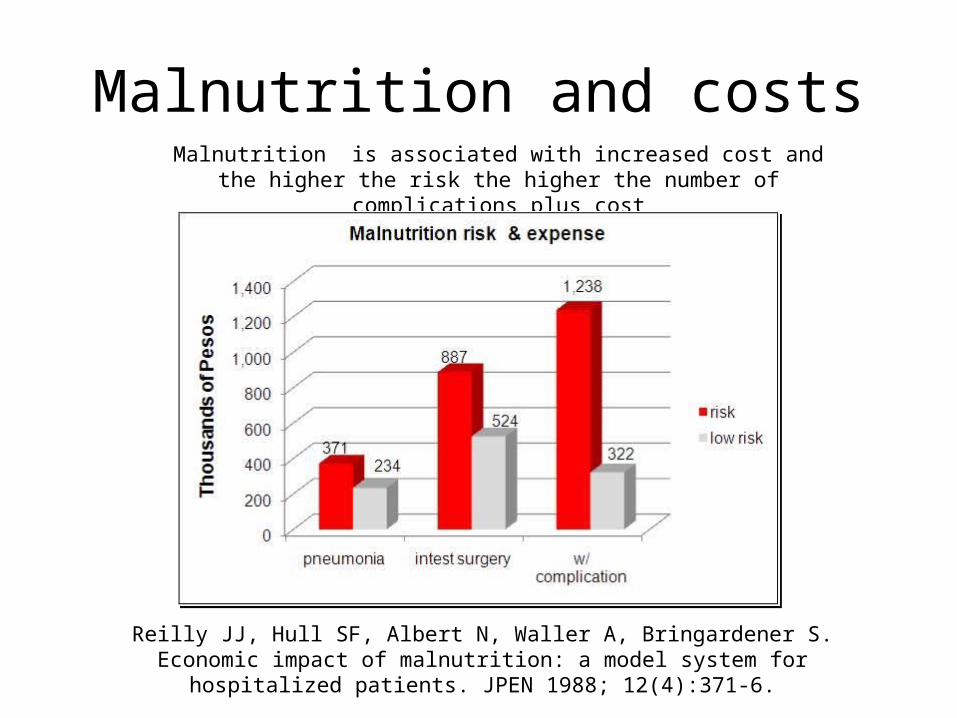
Malnutrition and costsMalnutrition is associated with increased cost and the higher the risk the
higher the number of complications plus cost
Reilly JJ, Hull SF, Albert N, Waller A, Bringardener S. Economic impact of malnutrition: a model system for hospitalized patients. JPEN 1988; 12(4):371-6.
Malnutrition: effects on surgery
• Slow wound healing.• Reduced muscle strength.• Decrease in respiratory muscle strength • Impaired cardiac function• Immune hypofunction and dysfunction• Higher morbidity and mortality• Poor quality of life

PREVALENCE OF MALNUTRITION
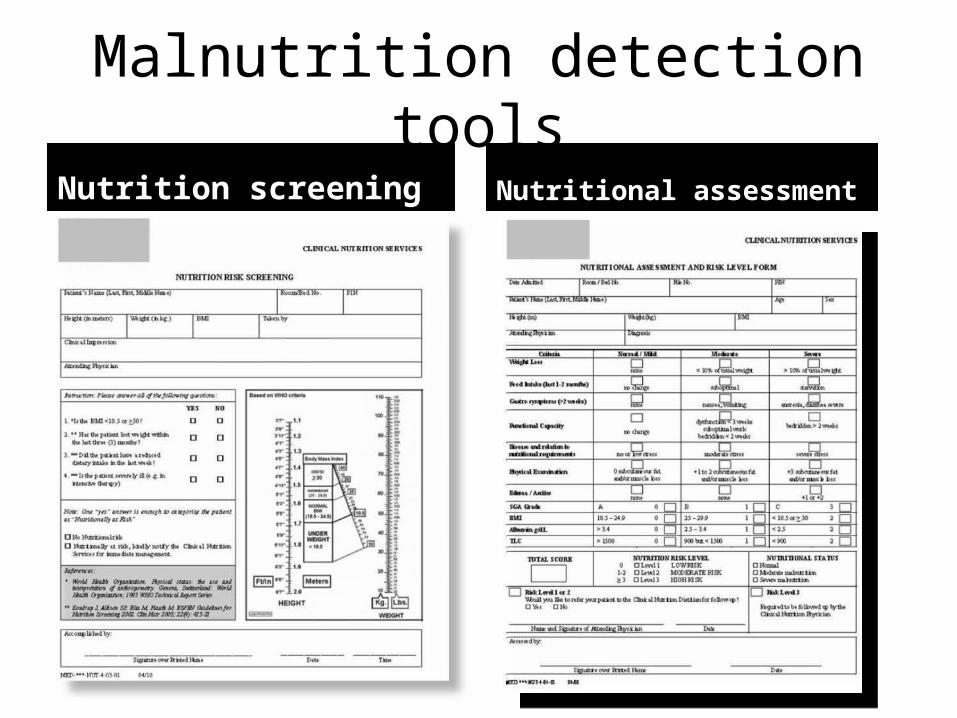
Malnutrition detection toolsNutrition screening Nutritional assessment

Nutritional Assessment
and Risk Level Form
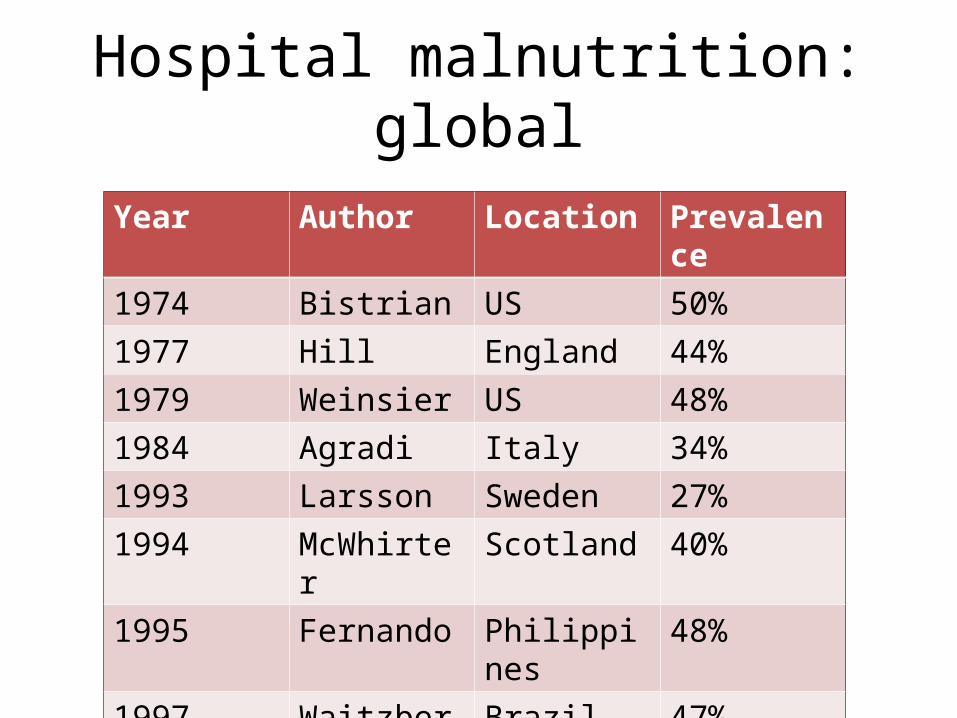
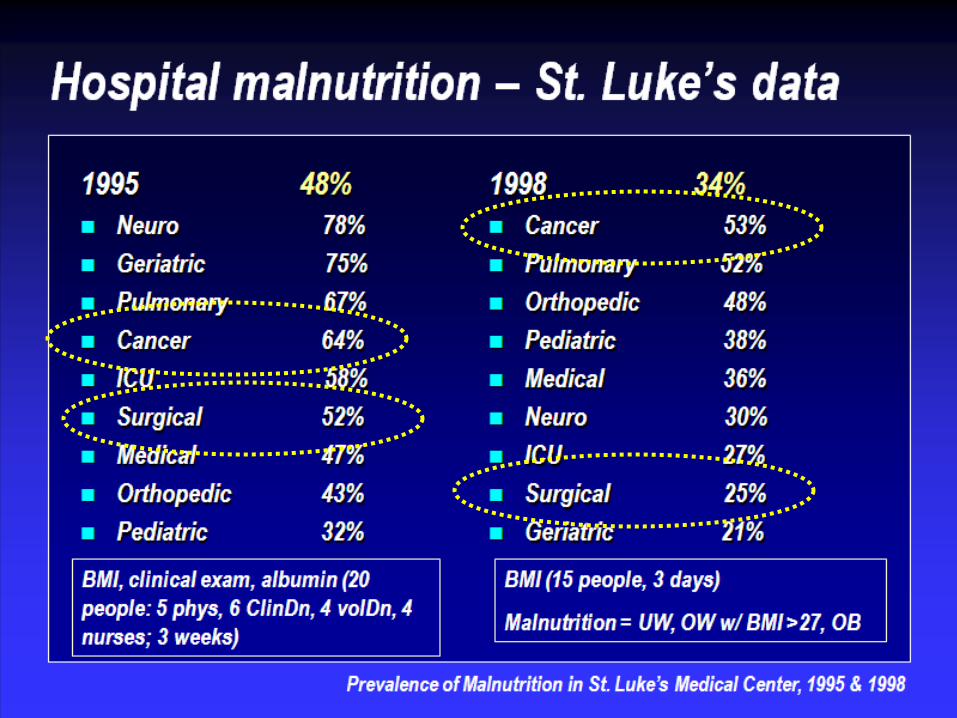
Hospital malnutrition: global
Year Author Location Prevalence1974 Bistrian US 50%1977 Hill England 44%1979 Weinsier US 48%1984 Agradi Italy 34%1993 Larsson Sweden 27%1994 McWhirter Scotland 40%1995 Fernando Philippines 48%1997 Waitzberg Brazil 47%
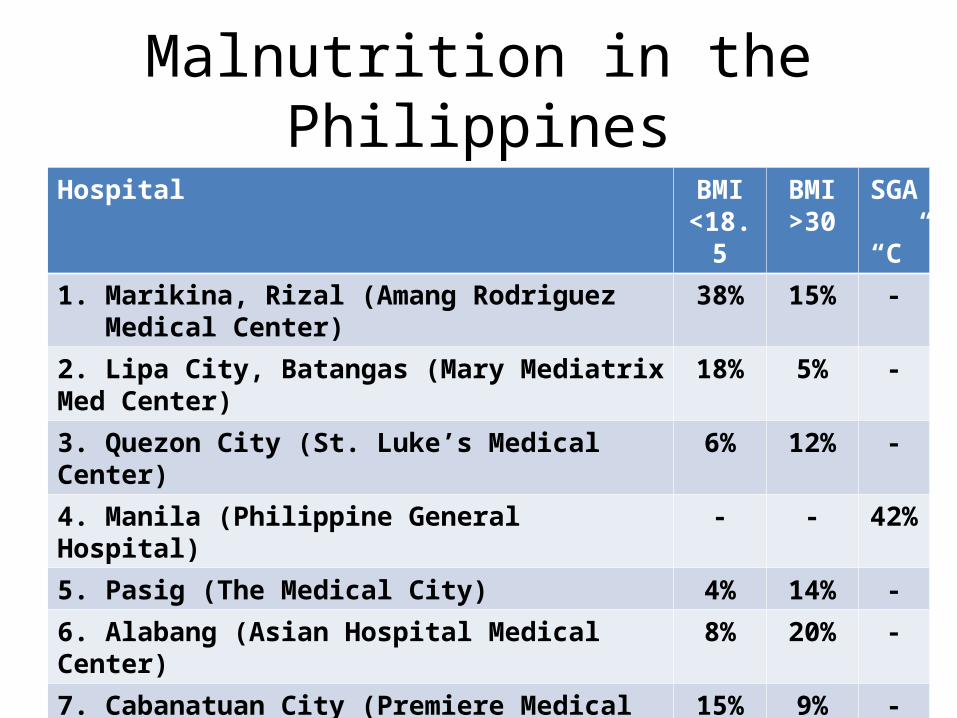
Malnutrition in the PhilippinesHospital BMI
<18.5BMI>30
SGA “C”
1. Marikina, Rizal (Amang Rodriguez Medical Center) 38% 15% -
2. Lipa City, Batangas (Mary Mediatrix Med Center) 18% 5% -
3. Quezon City (St. Luke’s Medical Center) 6% 12% -
4. Manila (Philippine General Hospital) - - 42%
5. Pasig (The Medical City) 4% 14% -
6. Alabang (Asian Hospital Medical Center) 8% 20% -
7. Cabanatuan City (Premiere Medical Center) 15% 9% -
8. Mandaluyong (St. Martin De Porres Hospital 12% 8% -
Mean 14.4% 11.8%

Malnutrition in the units

Nutritionally at risk patients
Llido L. The impact of computerization of the nutrition support process in the nutrition support program in a tertiary care hospital in the Philippines: report
for the years 2000-2003. Clin Nutr 2006; 25(1):91-101 .

WHAT IS THE PREVALENCE OF MALNUTRITION AMONG SURGICAL
PATIENTS IN YOUR CENTER?

CONCLUSION
Malnutrition
• Is a syndrome• Its presence in surgical patients influences
outcome• Detection and management is a priority in
surgical patients• Is prevalent in the surgical patient population





























