Embed Size (px)
Citation preview

RADIOLOGY—ORIGINAL ARTICLE
Mammographic and ultrasound features of invasive lobularcarcinoma of the breastAlan J Porter,1 Elizabeth B Evans,1 Loani M Foxcroft,1 Peter T Simpson2 and Sunil R Lakhani2,3,4
1Wesley Breast Clinic, Wesley Hospital, 2UQ Centre for Clinical Research, The University of Queensland, 3The University of Queensland, School of
Medicine, and 4Pathology Queensland: The Royal Brisbane & Women’s Hospital, Brisbane, Queensland, Australia
AJ Porter MBBS, FRANZCR, FRCR; EB EvansMBBS, MFM(Clin); LM Foxcroft MBBS;
PT Simpson PhD; SR Lakhani MD, FRCPA.
CorrespondenceDr Elizabeth Evans, Wesley Breast Clinic, 451
Coronation Drive, Auchenflower, QLD 4066,
Australia.
Email: [email protected]
Conflict of interest: None.
Submitted 4 December 2012; accepted 8 April
2013.
doi:10.1111/1754-9485.12080
Abstract
Introduction: Invasive lobular cancer (ILC) is an important contributor to falsenegative mammography. This study aims to assess the value of digitalmammography and to identify imaging features that could assist the radiolo-gist to suggest the diagnosis of ILC prior to biopsy.Methods: Three hundred sixty-one cases of pure ILC diagnosed at the WesleyBreast Clinic during the period 1995–2010 were reviewed by one of theauthors (AP). Radiological features were categorized, and clinical features andneedle sampling results were recorded.Results: Mammography was negative in 29.9% of ILCs. The commonestpositive finding was a localized spiculated mass (41.8%). Thirty-four pointnine per cent of lesions were visible in only one view, usually cranio-caudal.Calcification was not a feature of ILC. The use of digital mammography in 30%of cases did not decrease the false negative rate for ILC. Breast ultrasound(BUS) showed an abnormality in 97.8%, most commonly a localized irregularhypoechoic mass with shadowing.Conclusions: Digital mammography does not reduce false negative mammog-raphy in ILC. The poor visibility of ILCs may be partly related to their lowdensity (mass/unit volume). ILCs may sometimes be poor attenuators ofX-rays but excellent attenuators of ultrasound, causing marked acousticshadowing. Bilateral whole BUS has a very low false negative rate in expe-rienced hands and is mandatory in symptomatic women. The combination ofpoor visibility on mammography with high visibility on ultrasound, as well ascertain characteristic ultrasound appearances of ILC, may enable the radiolo-gist to suggest ILC as a diagnostic possibility, prior to biopsy.
Key words: breast neoplasms; breast ultrasound; digital mammography;lobular carcinoma; mammography.
Introduction
Invasive lobular carcinoma (ILC) is the most commonlydiagnosed special subtype of invasive breast cancer,accounting for up to 15% of all cases.1 The incidence ofILC has been increasing disproportionately over recentdecades,2–4 especially in postmenopausal women. Froma screening point of view, ILC is an important cause offalse negative mammography.5–7
The Wesley Breast Clinic (WBC) examines about23 000 women per year, approximately half of whom areasymptomatic. Over 300 breast cancers (invasive and
non-invasive) are diagnosed annually. All ILCs diagnosedbetween 1995 and 2010 were reviewed in an attempt todefine features that would assist the radiologist tosuggest a diagnosis of ILC prior to biopsy.
Methods
Study population
Three hundred ninety-six pure ILCs were diagnosedduring the study period (1995–2010), comprisingapproximately 14% of all invasive cancers. In 361 of
bs_bs_banner
Journal of Medical Imaging and Radiation Oncology 58 (2014) 1–10
© 2013 The Royal Australian and New Zealand College of Radiologists 1

these, hard-copy mammogram and ultrasound imageswere available for review. Mixed ILC/invasive ductalcancers (IDC) and tubulo-lobular cancers were excludedfrom the study. This study was approved by theResearch Ethics Committees of both Uniting Health Careand the University of Queensland.
Nearly all symptomatic women attending the WBChave mammography (except very young women) andbilateral whole breast ultrasound (BUS). All womenrecalled from the screening program for a clinical ormammographic abnormality are investigated by bilateralwhole BUS.
In Australia there is a National Breast ScreeningProgram offering biennial mammography at no cost tothe participant. Their target population is 50 to 69 yearsbut women may attend from 40 years. The WBC isseparate from this and is a private clinic. There is ahealth insurance rebate for screening mammographyonly if there is a family or personal history of breastcancer. Hence our study group may have a higher pro-portion of women with a family history than in apopulation-based screening program, and a greaterproportion of women from a higher socioeconomicgroup.
Review process
The study was focused on the visit where the ILC wasdiagnosed, and the accuracy of imaging at that visit. Oneof the authors (AP) independently reviewed all theimaging in the study group. The mammograms werecalled abnormal if the reviewer would have recalled thewoman based on the appearance using standard radio-graphic projections. Abnormal mammographic findingswere categorized into one of the appearances listedin Table 1. Similarly, the ultrasound films were callednormal or abnormal, and any abnormality was catego-rized into one of the appearances listed in Table 3. Thelocations of mammographic and ultrasound lesions werecompared to ensure they were the same lesion. Theofficial imaging report was then examined. Where therewere multiple abnormalities, only mammographic abnor-
malities relevant to the ILC were considered as ‘positive’findings (i.e. abnormalities in the other breast, or wellaway from the site of the ILC were not called ‘positive’for the purposes of this study). In a few cases thereviewer could identify an otherwise-undetected abnor-mality on the mammogram at the site of the ILC, withthe benefit of hindsight, once the BUS findings wereknown, but these mammograms were still recorded asnormal.
Imaging techniques
During the study period six GE DMR (Milwaukee WI,USA) mammography suites were operated, using thelatest film screen receptor systems marketed by Kodak(Rochester, NY, USA). From 2004, a computed radiog-raphy (CR) Fuji Profect CS (Tokyo, Japan) was intro-duced. By 2007 all examinations were performed usingdigital CR. BUS was undertaken in six suites (equipped atvarious times with GE, Philips (Eindhoven, the Nether-lands) and Toshiba (Otawara, Japan) units using appro-priate high frequency transducers.
Whole BUS has been the standard of care for over 20years at the WBC and is performed in the clinic bydedicated specialist breast sonographers with anaverage of about 17 years experience. In more recentyears, we have performed bilateral whole BUS on someasymptomatic, mammographically negative women whohave dense breasts and/or are at high risk due to per-sonal or family history.
Lesion sampling
The WBC policy is to perform sampling by fine needleaspiration cytology (FNAC) or core biopsy, according tothe classification of the lesion using the Breast ImagingReporting and Data System (BI-RADS®).8 FNAC is per-formed on some ultrasound lesions classified as benign(BI-RADS® 2), and especially lesions called probablybenign (BI-RADS® 3). The specimens are examined bytwo experienced cytology services. Core biopsy is per-formed on ultrasound lesions classified as either suspi-cious for malignancy or malignant (BI-RADS® 4 and 5).However, prior to the last 10 years some BI-RADS® 4and 5 lesions were initially subjected to FNAC, and someof these subsequently had a core biopsy as well. Also,some women with multiple lesions of differing BI-RADS®classifications may have FNAC of some lesions and corebiopsy of others.
Statistics
Statistical analysis of the data was performed with SASsoftware (SAS Institute Inc., Cary, NC, USA), usingt-tests and chi-squared tests. Log transformation wasperformed on ultrasound size data, whose distributionwas skewed.
Table 1. Type of mammographic abnormality in ILC
Type of mammographic
abnormality
No. cases %
Localized spiculated mass 151 41.8
Architectural distortion 50 13.8
Discrete non-spiculated mass 23 6.4
Asymmetrical density 17 4.7
Calcification 11 3.0
Nipple retraction 1 0.3
No abnormality 108 29.9
Total 361
ILC, invasive lobular carcinoma.
AJ Porter et al.
© 2013 The Royal Australian and New Zealand College of Radiologists2

Results
History and examination
The average age of the 361 women with ILC was 59years (median age 59), with an age range of 28 to 90years. Seventy-nine per cent were aged 40–69. Afamily history of breast cancer in a first degree relativewas present in 98 women with ILC (27.1%), comparedwith 26.1% for women with IDC diagnosed in theclinic. One hundred thirty of the women with ILC(36%) were having their first visit to the clinic at thetime of diagnosis.
One or more symptoms or signs of breast cancer werepresent in 255 of the 361 women with ILC. The com-monest were lump or thickening (present in 230women), followed by pain (45), skin dimpling (7), nippleretraction (6) and change in breast shape (3). For theremaining 106 women (29.4%) who had no symptomsor signs (hereafter referred to as the ‘asymptomatic’group), the cancer was detected by screening mammog-raphy and/or by ultrasound, or, in one case, was anincidental finding in breast tissue from a bilateral mas-tectomy (done for Duct Carcinoma in Situ in the otherbreast), combined with a significant family history.
Mammography
The radiographic findings are recorded in Table 1. Usingstandard radiographic projections, no abnormality rel-evant to the ILC was detected in 108 patients (29.9%).
Of the 361 women with pure ILC, 252 were examinedusing film screen and 109 (30.2%) with digital mam-mography. In assessing the results, women were dividedinto symptomatic and asymptomatic (Table 2). Themammographically negative ILCs in asymptomaticwomen were only diagnosed because they had bilateralwhole BUS, done either in the process of investigatingsome other breast lesion, or because of dense breastsand/or a significant family history. For symptomaticwomen, the percentages of normal mammograms with
film screen and digital mammography were similar. Forasymptomatic women, there appeared to be morenormal mammograms with digital than with film screenmammography, but this difference did not reach statis-tical significance. (chi-squared = 2.48, P = 0.115).
There was an apparent increase in the percentage ofnegative mammograms over time in both groups(namely) film-screen 27.2% negative prior to 1 January2004, 31.5% negative after 1 January 2004; digital29.4% negative prior to 1 January 2007, 36.0% after 1January 2007. However, these increases were not sta-tistically significant (P > 0.5).
In 126 cases (34.9%), the ILC was seen in only oneview, and it was the cranio-caudal view in 93 of these(73.8%). In the 33 cases where the lesion was best seenin the medio-lateral oblique view, the lesion was mostcommonly in the upper outer quadrant (22 cases,66.7%).
Breast ultrasound
Only one woman in the study had no ultrasound. Hard-copy ultrasound films of the remaining 360 women werereviewed and 8 (2.2%) showed no abnormality. In the352 with an abnormality, the commonest finding was alocalized irregular hypoechoic mass with shadowing,which was observed in 50.5% of cases (Table 3 andFig. 1, right breast). Shadowing only, without an obviousmass, was seen in 17.5% of cases (Fig. 2). Twenty pointsix per cent of cases consisted of an irregular hypoechoicmass without shadowing. Some less suspicious appear-ances included a well-circumscribed mass seen in 4.2%(Fig. 3), and an infiltrative hypoechoic pattern resem-bling fibrocystic change in 3.6% (Fig. 4). Five of the ILCswere hyperechoic (with respect to the echogenicity offat). They may sometimes have a similar appearance tothe focal areas of echogenic fat (sometimes calledlipomas), which are not uncommonly seen as an inci-dental finding in BUS. However, in all our hyperechoiccases, some acoustic shadowing was present (Fig. 5).Excellent examples were found of the classical ultra-
Table 2. False negative rates for film screen and digital mammography in symptomatic and asymptomatic
women with ILC. Size on BUS (where able to be sized)
No. of ILC No. with normal
mammogram (%)
Average size on BUS
(No. of women)
Symptomatic women
Film screen 192 58 (30.2) 18.0 mm (174)
Digital (Fuji CR) 64 21 (32.8) 20.2 mm (60)
All symptomatic 256 79 (30.9) 18.6 mm (234)
Asymptomatic women
Film screen 60 13 (21.6) 11.6 mm (58)
Digital (Fuji CR) 45 16 (35.5) 12.4 mm (39)
All asymptomatic 105 29 (27.6) 11.9 mm (97)
BUS, breast ultrasound; ILC, invasive lobular carcinoma.
ILC, mammogram and ultrasound
© 2013 The Royal Australian and New Zealand College of Radiologists 3

sound appearances of ILC, for example an appearanceresembling a suspension bridge, described by Stavros asthe ‘Golden Gate sign’10 (Fig. 6). A single umbrella-likeextension into Cooper’s ligaments is well demonstratedin Figure 7. Other examples of ILC, showing unusualpatterns such as ‘cactus’ and ‘pinnacles’, as well as amulti-locular appearance, are shown in Figure 8.
For those women where it was possible to measureultrasound size, the average size was calculated for eachgroup (Table 2). There was no significant difference inultrasound size between the women examined with filmscreen or digital mammography, but the ultrasound sizewas significantly greater for symptomatic than asymp-tomatic women (t = 5.97, P < 0.001).
Lesion sampling
Sampling results were classified according to the guide-lines of the NHS Breast Screening Pathology group.11
FNAC was performed in 214 cases, and in 173 of these(80.8%) the result was atypia (C3-C4)11 or malignantcells (C5).11 Core biopsy was performed in 216 cases,and the result showed malignancy (B5)11 or atypia (B3-B4)11 in 215 (99.5%). Seventy-six women had bothFNAC and core biopsy.
Of the 41 women with benign or unsatisfactory FNACs(C1-C2),11 22 had a malignant or atypical core biopsy.The remaining 19 did not have a core biopsy, and therewere also 7 women in whom neither FNA nor core biopsywas attempted. In these 26 women, excision was rec-ommended on the basis of the clinical and radiologicalfindings, or the ILC was an incidental finding.
Multifocal and multiple invasive cancers
In 121 of the 361 cases (33.5%), the ILC was multifocalon histology of the excised specimen. Of these 121, only73 (60.3%) were detected as multifocal on breastimaging. (MRI was introduced to the clinic during thelater years of the study, but was only performed on twowomen with ILC in the study period.) There were also 14
cases where there appeared to be multifocal lesions onimaging, but on excision, they were found to be all partof the same large lesion. There were four women withbilateral ILC, one of them also having a separate IDC onone side. Two other women also had an ipsilateral IDCseparate from the ILC. Five women had a synchronouscontralateral IDC (Fig. 1) and one had a contralateraltubular invasive cancer.
Discussion
Invasive lobular carcinoma is a special subtype type ofbreast cancer that displays morphological, biological andclinical features distinct from IDC. ‘Classical’ ILC typicallycomprises small bland cells that infiltrate along andaround ducts in single file without destroying the under-lying architecture. E-cadherin is a transmembraneprotein first described and named by Takeichi.12 Normalbreast epithelia and the vast majority of IDCs expressthis protein, but it is lost in most ILCs,13,14 althoughaberrant expression in ILCs is possible.15 This loss ofE-cadherin expression in approximately 90% of ILCs isconsidered to contribute to their lack of tumour cellcohesion and their diffuse growth pattern.
The difficulty in diagnosis of ILCs is of concern as theincidence of these tumours is increasing,2,3 and a link tothe use of combined hormone replacement therapy hasbeen suggested.4,16 ILCs, compared with IDCs, are oftendiagnosed when the tumours are larger and at a moreadvanced stage.17 Some ILCs may be clinically obviousas cancers, whereas others have only vague thickening,or may be completely normal on physical examina-tion.18,19 In our study, 29.4% of the women had nosymptoms or clinical signs, while for 6 women the onlyabnormality was nipple retraction or skin dimpling. LeGal et al. noted that nipple retraction was more commonin ILC than in other breast carcinomas.5 In the study byTan et al. of 273 women with ILC, 9 women presentedwith nipple retraction only.19
The commonest abnormal findings on mammographywere localized spiculated mass (41.8%) and architec-tural distortion (13.8%), appearances which have beennoted in ILC by other authors.18–20 Reported false nega-tive rates for ILC on mammography vary widely (e.g.19%,6 29%,21 43%,5 66%7). In our study, mammogra-phy was negative in nearly 30% of cases (Table 1). Thetrue false negative rate may be higher, as there mayhave been other mammographically negative ILCs thatwere not found at all. Only a full-scale study of intervalcancers, with Australia-wide access to cancer registries,could assess whether ILC is overrepresented amonginterval cancers.
Microcalcification is not a feature of pure ILC. It waspresent in only 3% of cases, and often not typicallymalignant-looking. Other authors have found that wheremicrocalcification led to the diagnosis of an ILC, thecalcification turned out to be in other lesions (e.g.) the
Table 3. Type of ultrasound abnormality in ILC
Type of ultrasound abnormality No. of patients %
Localised irregular hypoechoic
mass + shadowing
182 50.5
Localised irregular hypoechoic
mass, no shadowing
74 20.6
Shadowing only 63 17.5
Well circumscribed mass 15 4.2
Infiltrative pattern 13 3.6
Focal hyperechoic lesion 5 1.4
No abnormality 8 2.2
Total 360
ILC, invasive lobular carcinoma.
AJ Porter et al.
© 2013 The Royal Australian and New Zealand College of Radiologists4

ductal component of mixed ducto-lobular tumours,22 orassociated ductal carcinoma-in-situ or sclerosing adeno-sis.22 Microcalcification may be a feature of pleomorphiclobular carcinoma-in-situ,23 which may be associatedwith ILC.24 Since calcification is not a feature of ILCs, itis unlikely the difference in contrast resolution betweenCR and full field digital mammography would make anymaterial difference in ILC detection.
Variation in visibility of a mammographic lesion ondifferent views, or ‘conspicuity variation’, is known tobe a feature of radial scars, but has also been describedin association with small invasive breast cancers(<10 mm).25 In our study, 34.9% of tumours were con-spicuous in only one view, usually the cranio-caudal view(73%). In the paper by Hilleren et al. 20% of ILCs werevisible in only one view, and ILCs were twice as likely to
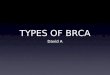
Fig 1. Bilateral cancers. An 86-year-old woman whose surgeon described a ‘clinical carcinoma’ of the left breast and a ‘clinically suspicious’ lesion in the right breast.
The mammogram showed a high density discrete mass in the left breast and a lower density mass in the right breast with normal breast structures visible though
the mass. The lesions are of similar size and position in both breasts. Ultrasound of the left breast showed a lobulated sonolucent mass and on the right, a spiculated
mass with spiculations directed towards the skin. Pathology: Left breast – invasive ductal carcinoma; Right breast – invasive lobular carcinoma.
ILC, mammogram and ultrasound
© 2013 The Royal Australian and New Zealand College of Radiologists 5

be seen on the cranio-caudal view as on oblique orlateral views.18 In a screening program, ILCs may beresponsible for recalls by a single reader and this iscommonly due to the failure to detect architectural dis-tortion,26 or the presence of dense parenchyma. Poormargination, conspicuity variation and minimal disrup-tion of the normal architecture are other causes. ILC mayalso appear as focal asymmetrical fibroglandular tissueof normal density, which is sometimes difficult to inter-pret in the absence of previous mammograms.
The paper by Holland et al. on occult breast cancersstated that the loose type of fibrous tissue found in ILCsdiffers from that in IDCs, with relatively less maturecollagen and more reticulin,27 and its similarity to theloose fibrous tissue of the normal lobule makes ILCsdifficult to distinguish, especially in dense parenchyma.However, the paper by Hilleren et al. suggested that thetendency of ILCs to grow in multicentric foci with normaltissue in between contributes to their relatively lowradio-opacity.18 Figure 9 postulates how the density of abreast lesion in mass/unit volume is important in deter-mining mammographic visibility. The loss of E-cadherinin most ILCs results in fewer cancer cells and morelow-density fat per unit volume of tumour, comparedwith IDCs, which are compact, dense cancers and are
therefore relatively opaque to X-rays, and possibly moreeasily palpable. One case in our study was very informa-tive as there was an ILC in the right breast and asimilar-sized IDC in the left breast, in a mirror imagelocation, enabling an imaging comparison of the twotumours (Fig. 1). Stains for collagen, actin, elastin andsmooth muscle were performed for each tumour (notshown), and there was no demonstrable difference. Webelieve that, irrespective of the amount of desmoplasticreaction evoked, the density of the tumour is importantin determining its visibility in dense parenchyma.
We attempted to assess whether digital mammogra-phy (CR) with its improved contrast resolution wouldreduce the number of apparently normal mammogramsin ILC. The results in Table 2 appear to show the oppo-site, especially for the 105 asymptomatic women (filmscreen mammography 21.6% negative; digital mam-mography 35.5% negative). While the difference wasnot statistically significant for this sample size, such atrend is not necessarily surprising. Digital mammogra-phy was gradually phased into our clinic starting in 2004.Meanwhile, the threshold for further investigation ofasymptomatic women was changing, with increasing useof BUS if these women were considered to be at high riskor had dense breasts, resulting in the diagnosis of more
(a) (b)
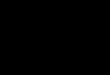
Fig 2. Shadowing only on ultrasound. (a) A 62-year-old woman with a firm, fairly mobile lump associated with some nipple retraction, and an asymmetrical density
only on mammography. Ultrasound shows marked shadowing without a visible mass. The appearance is typical of an invasive lobular carcinoma of classic type.9 (b)
A 64-year-old woman with tender thickening in the left upper outer quadrant, and asymmetrical parenchymal density on mammography. Ultrasound shows patchy
shadowing without a discrete mass. Pathology: Invasive lobular carcinoma of classic type.
(a) (b) (c)
Fig 3. Well-circumscribed mass on ultrasound. (a) A 41-year-old woman with an irregular 2 cm lump which was clinically suspicious for cancer, and an irregular mass
on mammography. Ultrasound shows a circumscribed mass. Pathology: Invasive lobular carcinoma (ILC) of pleomorphic type. (b) & (c) A 49- year-old woman with a
discrete mobile mass, and unhelpful mammography due to a prosthesis and silicone in the tissues. Ultrasound shows a circumscribed mass. Pathology: pleomorphic
ILC associated with lobular carcinoma in situ.
AJ Porter et al.
© 2013 The Royal Australian and New Zealand College of Radiologists6

cancers in mammographically negative cases. This wouldtend to make the percentage of false negatives appear toincrease over time, irrespective of which mammographicmethod was used. Indeed this appeared to be the casewith our study, although the increases over time did notreach statistical significance. For symptomatic women,the false negative rates over the study period were foundto be very similar for film screen and digital mammog-raphy. These women were usually investigated with
Fig 4. Infiltrative pattern on ultrasound. A 77-year-old woman with a rubbery
mass with skin tethering, and some increased density and distortion on mam-
mography. Ultrasound showed a poorly defined infiltrative pattern. Pathology:
Invasive lobular carcinoma.
)c()b()a(
(d)(e)(f)
Fig 5. Hyperechoic mass on ultrasound. Clockwise from top left: (a) A 72-year-old woman presenting for routine screening. Clinically she had some thickening in left
axillary tail, and on mammography, a new focal 1 cm density. Ultrasound shows a well-defined hyperechoic lesion. Pathology: Invasive lobular carcinoma of classic
type. (b) & (c) An 81-year-old woman with a tender lump, and a spiculated mass on mammography. Ultrasound shows a focal hyperechoic mass with marked acoustic
shadowing. Pathology: Invasive lobular carcinoma of classic type. (d) A 64-year-old woman presenting with tender swelling, and on mammography there was a focal
parenchymal density associated with non-specific microcalcification. Ultrasound shows a poorly defined hyperechoic lesion with some acoustic shadowing.
Pathology: Infiltrating lobular carcinoma of classic type. (e) & (f) A 79- year-old woman with an ill defined lump clinically, and a suspicious density on mammography.
Ultrasound shows a focal irregular hyperechoic lesion with some acoustic shadowing. Pathology: Invasive lobular carcinoma of classic type.
Fig 6. ‘Golden Gate sign’. A 90-year-old woman with a large mass and inverted
nipple, and an asymmetrical density on mammography. Ultrasound shows
invasion of Cooper’s ligaments producing the so-called ‘Golden Gate sign’.10
Pathology: Invasive lobular carcinoma of classic and solid type.
ILC, mammogram and ultrasound
© 2013 The Royal Australian and New Zealand College of Radiologists 7

BUS. An unbiased evaluation of the efficacy of digitalmammography for the diagnosis of ILC would require allpatients to be investigated in the same way (i.e. to haveconcurrent BUS), regardless of the presence or absenceof symptoms or signs.
The sensitivity of BUS was 97.8% in our series. Thishigh figure is due in part to the quality and considerableexperience of our dedicated breast sonographers. Sig-nificant shadowing was apparent in 68% of our tumours.Other authors have reported posterior shadowing in75%9 and 84%28 of ILCs. Shadowing only, without anobvious mass, was seen in 17.5% of our cases, anappearance which has been described as typical of ILC ofclassic type.9 The ‘Golden Gate sign’ described byStavros, results from extension of ILC into Cooper’sligaments.10 These ligaments, including their bases, arethree-dimensional structures which are invaded by theILC, and open up in the atrophic breast like an umbrella(Fig. 7). Invasion of Cooper’s ligaments probably causes
the skin changes and nipple retraction, which are fea-tures of ILC. Cooper’s ligaments may be a potentialsource of blood supply, providing nutrition to ILCs.29
Multifocality was present in 33.5% of women in ourstudy. In 13 women (3.6%) there was bilateral ILC, or aseparate IDC in the ipsilateral breast, or an IDC ortubular cancer in the contralateral breast. This illustratesthe importance of bilateral whole BUS.
FNAC may yield a benign result or produce a non-diagnostic sample due to the sparse cellularity of thesetumours and the presence of small relatively normal-appearing cells. Classical ILC may yield a pauci-cellularsmear with subtle atypia, and a certain percentage ofinconclusive aspirates may be unavoidable.30 FNAC in
Fig 7. Invasion of Cooper’s ligament. A 59-year-old woman recalled for archi-
tectural distortion on screening mammography. Ultrasound shows invasion of
a Cooper’s ligament. Pathology: Multifocal invasive lobular carcinoma of pleo-
morphic type.
(a) (b) (c) (d)
Fig 8. Unusual appearances on ultrasound. (a) & (b) A 32-year-old woman who presented, with a large 6 cm breast mass, skin dimpling and nipple retraction, with
distortion and a lobulated density on mammography. Ultrasound shows projections upwards towards the skin with probable involvement of Cooper’s ligaments
producing a bizarre pattern, which could be described as ‘gloved hand’ or ‘ cactus’. There is a marked hyperechoic rim around the projections. Pathology: Invasive
lobular carcinoma of pleomorphic type. (c) A 38-year-old woman whose screening mammogram showed 2 irregularly shaped densities in the upper outer quadrant.
Ultrasound shows invasion of multiple Cooper’s ligaments resembling the Pinnacles (a landmark in Western Australia). Pathology: Invasive lobular carcinoma of
pleomorphic type. (d) A 63-year-old woman with a palpable mass, and a large lobulated mass on mammography, containing a small focus of calcification. Ultrasound
shows a discrete lesion with a multilocular appearance Pathology: Invasive lobular carcinoma of pleomorphic type.
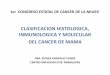
densityg / cm3
FibroglandularTissue
cysts
fibroadenomas
Conspicuity on Mammogram
ILC
ductalcancer
Fig 9. Conspicuity and density. Against a background of dense fibroglandular
tissue, the visiblilty or conspicuity of a lesion is determined by its physical
density (mass/unit volume). Invasive ductal carcinoma is more likely to be
visible in dense fibroglandular tissue than invasive lobular carcinoma.
AJ Porter et al.
© 2013 The Royal Australian and New Zealand College of Radiologists8

our series demonstrated atypia or malignant cells in80.8% of cases, but other series have demonstratedFNAC positivity around 60%.5,19 Core biopsy has beenreported as more reliable (e.g. 90.8%).19 In our study,99.5% (186/187) of core biopsies performed (usuallywith ultrasound guidance) showed atypia or malignancy.
Conclusion
The incidence of ILC is rising, and knowledge of itsspecial features is therefore relevant. The fact that ILC isa low density malignancy (mass/unit volume), maydiminish both its palpability and its visibility on mam-mography (even digital mammography). This, plus thelack of calcification as a feature of ILCs, creates diag-nostic difficulty in some cases. However, while someILCs are poor attenuators of X-rays, they may be excel-lent absorbers and attenuators of ultrasound, causingsignificant shadowing in a high percentage of cases. Therole of whole BUS in the detection of ILC may be espe-cially important in women with dense breasts or otherrisk factors, and its use can result in the earlier diagnosisof smaller ILCs, as well as detection of multifocality.When there is a combination of poor visibility on themammogram and a conspicuous lesion on the ultra-sound, the possibility of an ILC can be suggested bythe radiologist prior to biopsy, thus enabling considera-tion of other investigations (including MRI and immuno-histochemistry of core samples) and treatment planning.On BUS, a growth pattern peculiar to ILC may give theradiologist additional clues that the lesion is an ILC.
Acknowledgements
We wish to thank the following: This study was sup-ported by the Wesley Research Institute. Dr PeterSimpson is funded by a Fellowship from the NationalBreast Cancer Foundation, Australia. Dr John Heggieassisted with the physics of density and radio-opacity oftumours. Sullivan Nicolaides Pathology performed thecomparative stains on the tumours in Figure 1. Mr TobySimm prepared the art work for Figure 9. Mrs JoNewman prepared the radiological images for publica-tion. Mrs Sandra Govenlock and Mrs Debra Brownassisted with data collection.
References
1. Rakha EA, Sayed ME, Powe DG et al. Invasive lobularcarcinoma of the breast: response to hormonaltherapy and outcomes. Eur J Cancer 2008; 44:73–83.
2. Li CI, Anderson BO, Porter P, Holt SK, Daling JR, MoeRE. Changing incidence rate of invasive lobular breastcarcinoma among older women. Cancer 2000; 88:2561–9.
3. Verkooijen HM, Fioretta G, Vlastos G et al. Importantincrease of invasive lobular breast cancer incidencein Geneva, Switzerland. Int J Cancer 2003; 104:778–81.
4. Chikman B, Lavy R, Davidson T et al. Factorsaffecting rise in the incidence of infiltrating lobularcarcinoma of the breast. IMAJ 2010; 12: 697–700.
5. Le Gal M, Ollivier L, Asselain B et al. Mammographicfeatures of 455 invasive lobular carcinomas.Radiology 1992; 185: 705–8.
6. Krecke KN, Gisvold JJ. Invasive lobular carcinoma ofthe breast: mammographic findings and extent ofdisease at diagnosis in 184 patients. AJR Am JRoentgenol 1993; 161: 957–60.
7. Berg WA, Gutierrez L, NessAiver MS et al. Diagnosticaccuracy of mammography, clinical examination, US,and MR imaging in preoperative assessment of breastcancer. Radiology 2004; 233: 830–49.
8. D’Orsi CJ. Breast Imaging Reporting and DataSystem: Breast Imaging Atlas. American College ofRadiology, Reston, VA, 2003.
9. Butler RS, Venta LA, Wiley EL, Ellis RL, Dempsey PJ,Rubin E. Sonographic evaluation of infiltrating lobularcarcinoma. AJR Am J Roentgenol 1999; 172: 3–25.
10. Stavros A. Breast Ultrasound, 1st edn. LippincottWilliams and Wilkins, Philadelphia, PA, 2004;488–94.
11. NHS Cancer Screening Programmes. Guidelines forNon-Operative Diagnostic Procedures and Reportingin Breast Cancer Screening: Non-operative DiagnosisSubgroup of the National Coordinating Group forBreast Screening Pathology. NHS Cancer ScreeningProgrammes, Sheffield, NHSBSP publication no. 50,2001.
12. Takeichi M. Functional correlation between celladhesive properties and some cell surface proteins.J Cell Biol 1977; 75: 463–74.
13. Berx G, Cleton-Jansen A-M, Nollet F et al. E-cadherinis a tumour/invasion suppressor gene mutated inhuman lobular breast cancers. EMBO J 1995; 14:6107–15.
14. Moll R, Mitze M, Frixen UH, Birchmeier W. Differentialloss of E-cadherin expression in infiltrating ductal andlobular breast carcinomas. Am J Pathol 1993; 143:1731–42.
15. Da Silva L, Parry S, Reid L et al. Aberrant expressionof E-cadherin in lobular carcinomas of the breast. AmJ Surg Pathol 2008; 32: 773–83.
16. Li CI, Malone KE, Porter PL et al. Relationshipbetween long durations and different regimens ofhormone therapy and risk of breast cancer. JAMA2003; 289: 3254–63.
17. Li CI, Uribe DJ, Daling JR. Clinical characteristics ofdifferent histologic types of breast cancer. Br JCancer 2005; 93: 1046–52.
18. Hilleren DJ, Andersson IT, Lindholm K, Linnell FS.Invasive lobular carcinoma: mammographic findingsin a 10-year experience. Radiology 1991; 178:149–54.
ILC, mammogram and ultrasound
© 2013 The Royal Australian and New Zealand College of Radiologists 9

19. Tan SM, Behranwala KA, Trott PA et al. Aretrospective study comparing the individualmodalities of triple assessment in the pre-operativediagnosis of invasive lobular breast carcinoma. Eur JSurg Oncol 2002; 28: 203–8.
20. Evans WP, Burhenne LJ, Laurie L, O’Shaughnessy KF,Castellino RA. Invasive lobular carcinoma of thebreast: mammographic characteristics andcomputer-aided detection. Radiology 2002; 225:182–9.
21. Albayrak ZK, Onay HK, Karatag GV, Karatag O.Invasive lobular cancer of the breast: mammographicand sonographic evaluation. Diagn Interv Radiol2011; 17: 232–8.
22. Cawson JN, Law E-M, Kavanagh AM. Invasive lobularcarcinoma: sonographic features of cancers detectedin a BreastScreen Program. Australas Radiol 2001;45: 25–30.
23. Georgian-Smith D, Lawton TJ. Calcifications of lobularcarcinoma in situ of the breast: radiologic-pathologiccorrelation. AJR 2001; 176: 1255–9.
24. Carder PJ, Shaaban A, Alizadeh Y, KumarasuwamyV, Liston JC, Sharma N. Screen-detectedpleomorphic lobular carcinoma in situ (PLCIS):risk of concurrent invasive malignancy following acore biopsy diagnosis. Histopathology 2010; 57:472–8.
25. Cawson JN, Nickson C, Evans J, Kavanagh AM.Variation in mammographic appearance betweenprojections of small breast cancers compared withradial scars. J Med Imaging Radiat Oncol 2012; 54:415–20.
26. Veltman J, Boetes C, van Die L, Bult P, Blickman JG,Barentsz JO. Mammographic detection and staging ofinvasive lobular carcinoma. J Clin Imaging 2006; 30:94–8.
27. Holland R, Hendriks JH, Mravunac M.Mammographically occult breast cancer. A pathologicand radiologic study. Cancer 1983; 52: 1810–19.
28. Watermann DO, Tempfer C, Hefler LA, Parat C,Stickeler E. Ultrasound morphology of invasivelobular breast cancer is different compared with othertypes of breast cancer. Ultrasound Med Biol 2005;31: 167–74.
29. Zeng H, Zhao Y-L, Huang Y, Lin X, Chen X-Y LA-H.Values of color doppler flow imaging and imagingchanges of breast fascia and ligament in differentialdiagnosis of small breast neoplasms. Chin J Cancer2006; 25: 339–42.
30. Hwang S, Ioffe O, Lee I, Waisman J, Cangiarella J,Simsir A. Cytologic diagnosis of invasive lobularcarcinoma: factors associated with negative andequivocal diagnoses. Diagn Cytopathol 2004; 31:87–93.
AJ Porter et al.
© 2013 The Royal Australian and New Zealand College of Radiologists10