Embed Size (px)
Citation preview
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 615
Management of disruptive behaviour within nursing work
environments: a comprehensive systematic review of the evidence
Catherine Rogers-Clark RN, BA, MN, PhD1,
Susanne Pearce RN, BN (with distinction),MN,PhD Candidate1
Michelle Cameron RN, BN, MEd1
1. Australian Centre for Rural and Remote Evidence Based Practice, A Collaborating Centre of the
Joanna Briggs Institute
Corresponding author: Catherine Rogers-Clark, Australian Centre for Rural
and Remote Evidence Based Practice, University of Southern Queensland.
Email : [email protected] Phone: +61(07)46998313 Fax: +61(07)46998940
Abstract
Background - In an increasingly complex health care environment, where nurses are essential to
the health system's capacity to respond to the challenges presented by an ageing population,
creating positive work environments is fundamental for nurses, their co-workers, and their
patients. Disruptive clinician behaviour, which refers to behaviours such as bullying and physical
violence, but also to more subtle behaviours such as withholding vital information or gossiping,
can be highly destructive within a work environment. The implications of such behaviours within
the nursing workforce specifically, and to the health care system more broadly, are profound.
Substantial evidence suggests that the pervasiveness of such behaviours has consequences for
recruitment and retention, staff morale, job satisfaction, and staff absenteeism, as well as intra
and inter-professional communication and teamwork which can ultimate also affect patient safety.
The extent of the problem of disruptive behaviour in the workforce is discussed widely in the
literature and nurses as a cohort have been studied extensively, however there has been no
systematic review of evidence relating to how to manage these behaviours successfully.
Objective- The objective of this systematic review was to appraise and synthesise the best
available evidence in relation to interventions which have been successful in managing disruptive
clinician behaviour in the nursing work environment.
Inclusion criteria
Types of participants - The primary participant group of interest for this systematic review
includes nurses working in any health care setting; however any other member of the health care
team such as medical practitioners or allied health were also considered.
Types of intervention(s)/phenomena of interest
Any study that explored behavioural, educational, managerial, organisational and personal
interventions to manage disruptive behaviours in the health care setting was considered.
Types of studies - Studies using quantitative and qualitative methods as well as opinion based
papers were considered for this systematic review.
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 616
Types of outcomes - Outcomes were assessed in relation to the effect of interventions on patient
safety and quality of care, quality of team work and work environment, levels of job satisfaction
and nursing staff morale as well as levels of staff retention.
Search strategy - Searches were conducted including any published and unpublished material,
including grey literature, in the English language. A search of CINAHL, Medline, Medline-in
Process, PsychINFO, Emerald and TRIP was undertaken using specifically defined terms and
synonyms. Scirus, OpenSIGLE and Google Scholar were also searched. A search of electronic
dissertations via Dissertation Abstracts was undertaken.
Methodological quality - Each paper was assessed by two independent reviewers for
methodological quality prior to inclusion in the review using an appropriate critical appraisal
instrument from the System for the Unified Management, Assessment and Review of Information'
(SUMARI) developed by JBI.
Data Collection - Data was identified as quantitative or qualitative data or opinion based and data
extraction tools developed by the Joanna Briggs Institute were used to extract the data, where
possible. Where this was not possible, findings were presented in narrative form.
Data Synthesis - Data were synthesised according to their methodological approach. Qualitative
data were pooled using the QARI instrument and a set of statements were developed that
represented a broader overview of a specific aggregation
Results - A total of 24 papers, descriptive quantitative, qualitative and textual in approach, were
included in the review. The majority of the papers were textual, with a variety of expert opinion
provided in relation to managing disruptive clinician behaviour.
Conclusions - Comprehensive review of the literature identified that there has been very little
research evaluating the effectiveness of interventions to manage disruptive clinician behaviour in
nursing, or more broadly within the health care system. A handful of studies involved localised
interventions followed by a qualitative evaluation, with useful but not generaliseable findings.
These studies emphasised personal, peer and educational approaches to assist those nurses
affected by disruptive clinician behaviour within their work teams, but none were related to specific
management strategies aimed at the person exhibiting the disruptive behaviour. Most
recommendations in the literature were expert opinion. These recommendations emphasised the
importance of a clear and consistent organisational approaches to disruptive clinician behaviour.
Keywords - disruptive, bullying, incivility, interventions, incivility, management, organisations,
nurses, clinicians, health professionals, behaviours.
Background
Safety and quality thrive in an environment that supports working in teams and respecting other
people, regardless of their position in the organisation. Disruptive behaviours that intimidate staff,
decrease morale, or increase staff turnover can threaten the safety and quality of care1. Disruptive
clinician behaviour is defined as:
"...anything a clinician does that interferes with the orderly conduct of hospital business, from patient
care to committee work. This includes behaviour that interferes with the ability of others to effectively
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 617
carry out their duties or that undermine the patient's confidence in the hospital or another member of
the health care team"2 .
Unprofessional staff behaviour was identified as one of the most common causes of staff and family
conflict in a 2001 study conducted in the United States.3 Nursing morale has also been correlated with
autonomy, workplace equipment, workplace safety, teamwork, work stress, the physical demand of
nursing work, workload, rewards for skills and experience, career prospects, status of nursing and
remuneration3,4
.
The 2005 Queensland Health Systems Review identified that 'dysfunctional behaviours including
bullying, intimidation and a reluctance to share information were frequently reported and confirmed
amongst clinical staff in 18 of the 37 Health Service Districts reviewed within Queensland Health5.
The report states that these negative behaviours interfered with the delivery of patient care in a
resource constrained environment.
Simons6
identified belittling, punishing, excessive surveillance and exclusion, as victimising
behaviours amongst 511 randomly selected registered nurses in the USA. The main finding by
Simons was that as these types of behaviours increase, so does the individuals intent to leave the
current nursing position6. Disruptive clinician behaviours have been highlighted as a risk to patient
safety by the Joint Commission on Accreditation of Healthcare Organisations (JCAHO) in the United
States. Standard LD.3.15 (Leaders create and maintain a culture of safety and quality throughout the
hospital) means that American health organisations are now required to demonstrate second yearly
completion of assessment of culture using valid and reliable tools and to provide working
interventions7. This standard specifically requires that organisations address disruptive behaviours in
the clinical environment. The Queensland Health Foster review recommendation 4.1 articulates that:
'Surveys of workplace culture and staff satisfaction need to be undertaken regularly across the
organisation so that all districts can monitor their progress with cultural change through time5.
Emotional outbursts play a negative part in organisational society and a human resource perspective
recognises that people work for social and emotional benefits as well as for money3. Understanding
how people communicate and how people are motivated is often based upon an understanding of
emotion, as are the behaviours of people. These emotions are the products of socialisation and
manipulation and can be termed the emotional climate of an organisation8,9,10
.
The Office of Public Service Merit and Equity11
refers to the organisational climate as being the
'shared perception of what an organisation is like in terms of organisational policies practices,
procedures, routines and expected behaviours'. The Office of Public Service has identified that
surveys can be employed to measure employee perceptions of a variety of management and
leadership practices including working relationships with co-workers and workgroup distress12
.
Organisational culture and climate have particular significance in health care because: organisational
climate has a strong association with organisational performance (NHS studies demonstrate a strong
association between advanced human resource practices, including staff appraisal, teamwork and
training and development with lower patient mortality)1. Staff satisfaction has a very strong positive
correlation (0.89) with patient satisfaction1. Staff satisfaction impacts strongly on absenteeism and
turnover1.
This systematic review aims to address the strategies and recommendations available to address
disruptive clinician behaviours within the nursing workforce environment. Although a number of
strategies and recommendations are already available to assess and provide solutions for disruptive
behaviour in nursing, there is a lack of summarised accessible information detailing which of these
strategies and recommendations actually work.

JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 618
Included in this review is the identification of interventions that may enhance positive nurse
behaviours. The focus here is to identify interventions and processes that might mitigate negative or
dysfunctional behaviours. Within the health care profession generally, strategies such as professional
supervision, performance review and education (audit and feedback)13
have been proposed as a
means of addressing all types of clinician behaviours. Various approaches have also been taken to
measure emotional and behavioural quotients within organisations. Effective interventions need to be
implemented in education, practice and policy to prevent or decrease dysfunctional behaviours
amongst employees14
. For example, Fellowes et al13
critically evaluated all studies that have
investigated the effectiveness of different communication skills training techniques for cancer care
health care professionals. It was found that there was some evidence that labour-intensive training
can have a beneficial impact on health care professional behaviour change13
.
As early as the year 2000 the National Summit on Medical Errors and Patient Safety identified that
'bringing about the necessary cultural changes that support team work, acceptance and integration of
decision support systems and clinical practice guidelines into health care practices, and avoidance of
a 'name and blame' response when errors occur, is vital for positive patient outcomes1.The ability to
detect the presence of disruptive behaviours amongst nursing staff and to address these may
therefore have an impact on positive patient outcomes. Patient outcomes are not a focus for this
review. The potential for improved patient outcomes as a result of improved staff behaviours should
be acknowledged as a potential benefit however.
To date, a comprehensive systematic review of the literature is yet to be completed that clarifies or
synthesises what specific interventions can enhance supportive clinical behaviours.
Inclusion criteria
Types of participants
This review considered all qualitative and quantitative research that focuses on the management of
disruptive clinician behaviours within a nursing workforce environment. Studies involving nurses and
other members of the health care team including health administrators, medical practitioners, and
allied health workers were included.
Types of intervention(s)/phenomena of interest
Interventions of interest were quantitative and qualitative nursing and other health professional
studies that addressed behavioural/educational/managerial or organisational interventions associated
with the effective management of disruptive clinician behaviour.
Types of studies
Studies that describe successful behavioural, educational or other types of management interventions
for disruptive clinician behaviours were included. Opinion-based papers were explored to extract the
opinions of respected authorities based upon consensus or experience in the absence of rigorous
quantitative and qualitative research studies. Non-English language articles were excluded.
Types of outcomes
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 619
Outcome measures included measures (quantitative studies) or descriptions (qualitative studies) of
the success or otherwise of interventions to manage disruptive clinician behaviour. Outcomes sought
included the effect of interventions on patient safety and quality of care, quality of team work, levels of
job satisfaction, retention rates of staff and perceptions of the quality of their work environment.
Search strategy
The search strategy was designed to access published and unpublished material in the English
language, including 'grey' data found within research theses and conference proceedings and
comprised of three stages:
1 A search of CINAHL, Medline, Medline-In Process, PsychINFO, Emerald and TRIP to identify any
relevant keywords contained in the title, abstract and subject descriptors, including MeSH terms.
Medline-In process was used to search articles which had not had the cataloguing process
completed.
2 Terms identified and the synonyms used by respective databases, were used in an extensive
search of the literature.
3 Reference lists and bibliographies of the articles collected from those identified in stage two were
searched.
The initial search terms were adapted to suit the requirements of each database and
terms/descriptors included:
-Disruptive
-Clinician
-Bully*
-Mobbing
-Nurs*
-Behav*
-Behavio?r
-Strateg*
-Interventions
-Communication
-Morale
-Patient Safety
-Team Work
-Retention
-Job Satisfaction
-Incivility
-Work-related anger
-Social climate
-Conflict management
-Counterproductive work behaviour
Articles published in the last 10 year (1999-2009) in English and indexed in the following data bases
were searched in order to enhance currency of any recommendations found from the search:
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 620
CINAHL
Medline
Cochrane Library
psycINFO
Emerald
Embase
Dissertation Abstracts
ERIC
Grey Literature Search
Scirus
Open SIGLE
Google Scholar
BCEOHRN
Full copies of articles identified by the search, and considered to meet the inclusion criteria, based on
their title, abstract and subject descriptors, were obtained for data synthesis/analysis. Articles
identified through reference lists and bibliographic searches were also considered for data collection
based on their title. Two reviewers independently selected articles against the inclusion criteria.
Discrepancies in reviewer selection were resolved at a meeting between reviewers prior to selected
articles being retrieved. The schema of search strategies and findings from individual databases are
detailed in Appendix I. Studies and papers identified by the search are detailed in Appendix II, with
those retrieved presented in Appendix III
Method of the review
Papers selected for retrieval were assessed by two independent reviewers for methodological validity
prior to inclusion in the review using the standardised critical appraisal instruments from the Joanna
Briggs Institute System for the Unified Management, Assessment and Review of Information package
(SUMARI). The reviewers attempted to group qualitative studies that met the publication criteria into
one of the following categories: phenomenological, ethnographic, histographic and grounded theory
methodology. However the qualitative studies selected did not typically identify their methodology, nor
was a clear methodological framework identified. The majority were simply qualitative, descriptive
studies using thematic analysis. Quantitative studies were grouped into one of the following
categories: experimental studies; quasi-experimental studies; descriptive studies; descriptive-
correlational studies. The studies were then assessed independently for methodological quality by two
reviewers, prior to inclusion in the review using the corresponding checklist from the SUMARI suite
developed by the Joanna Briggs Institute. Validity criteria used by the Joanna Briggs Institute (Qari
Software, Appendix IV) were used to determine the validity of qualitative studies relating to the
outcomes. Opinion-based papers were assessed for inclusion using the JBI Notari tool (Appendix IV).
Quantitative studies were assessed for validity using the JBI Mastari tools for experimental and
descriptive studies (Appendix IV). Disagreement between reviewers were resolved through discussion
with the assistance of a third reviewer where required. Data extraction tools appear as appendices to
all articles reviewed.
Data Collection

JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 621
Following methodological assessment, the papers were grouped according to whether they were
quantitative, qualitative or opinion-based. Data extraction tools developed by JBI were used to extract
salient information from papers within the SUMARI software suite and are detailed in Appendix V.
Data extracted from the studies included specific details about the phenomena of interest,
populations, study methods and outcomes of significance to the review question and specific
objectives.
Data Synthesis
Qualitative research findings and textual data were pooled using the Qualitative Assessment and
Review Instrument (QARI) and JBI -NOTARI. This involved the aggregation or synthesis of findings to
generate a set of statements that represent that aggregation, through assembling the findings (Level
1 findings) rated according to their quality, and categorising these findings on the basis of similarity in
meaning (Level 2 findings). These categories were then subjected to a meta-synthesis in order to
produce a single comprehensive set of synthesised findings (Level 3 findings) that can be used as a
basis for evidence-based practice. It was planned that, where possible, data from quantitative studies
would be pooled in statistical meta-analysis using the Meta-Analysis of Statistics Assessment and
Review Instrument (MAStARI). All results were to be double entered to minimise the risk of data entry
error. However, statistical pooling was not possible and hence narrative form was used to present
findings. Synthesised findings are presented and discussed in the following sections and a complete
list of the findings and conclusions from included studies is presented in Appendix VIII. The credibility
of findings was determined using JBI categories which are presented in Appendix IX.
Results
Description of studies
The literature documenting the problem of disruptive clinician behaviour is substantial. An initial
search yielded 1038 papers related to one or more aspects of disruptive clinician behaviour, such as
workplace incivility, bullying and harassment. However, comparatively few papers were found which
addressed the objective of this review, which focuses on solutions to dysfunctional clinician
behaviour. A total 87 articles were retrieved and 23 of those served as background material. Only 64
articles were viewed to be relevant to the review topic and objectives, based on the title and abstract
(Appendix VI). Of the 64 studies, 40 were expert opinion text, 18 quantitative studies and six
qualitative studies. All studies were written in English and originated in the United Kingdom, United
States of America, Canada and Australia. These papers were selected from the search strategy for
retrieval, further evaluation and methodological assessment. Of the 64 papers, 41 were excluded for a
number of reasons following critical appraisal, including lack of congruence to the review objectives.
The excluded studies, including the reason(s) for exclusion are listed in Appendix VII. Of these 64
studies, 23 were included in the review. These papers included:
Five papers reporting descriptive-correlational studies
Four qualitative, interpretive studies
Fourteen textual papers
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 622
The included papers addressed organisational as well as individual and peer approaches to
managing disruptive clinician behaviour. Of the 23 included papers, one originated in Canada, five in
Australia, five in the United Kingdom and 12 in the United States of America. The settings under
investigation included 11 hospitals and 12 health care settings from a variety of areas such as
community health, mental health or medical practices. The primary focus in the papers was on nurses
as a single group (15 papers), nurses and doctors (three papers), doctors as a single group (one
paper) and health care employees in general (four papers). As the review progressed, it became clear
that multiple terms are used to describe the range of behaviours which disrupt the healthy functioning
of a nursing team. For clarity and consistency, the term 'disruptive clinician behaviour' was
deliberately chosen as the descriptor to encompass the broad range of behaviours which were
problematic within a nursing clinical team. However, all 23 papers selected for this review identified
their focus was on solutions to workplace incivility, workplace violence, lateral violence, bullying or
harassment.
Number of studies found and retrieved
Number of studies found Number selected for retrieval
1038 87
Methodological quality
This review has found very little high quality evidence to address the review question. Of the 23
papers selected for this review, only nine were research articles. Four papers discussed the results of
qualitative research36,43,48,80
. Of these, two were descriptive36,48
and the other two involved
interventions designed to assist nurses manage disruptive clinician behaviour43,80
. The five
quantitative studies included four surveys25,38,66,71
and one study which assessed an intervention
using a quasi-experimental design30
.
Hence, of the nine, only three30,43,80
were specifically focussed on implementing and evaluating
interventions to manage disruptive clinician behaviour. The other six did address interventions to manage disruptive clinician behaviour, but their data was gathered by survey or interviews where
nurses and other health professionals were asked to discuss their experiences of disruptive clinician
behaviour and their perceptions of what worked or didn't work in managing these behaviours. Hence,
there was no evaluative component to assess the effectiveness of the strategies identified by the
survey/interview participants.
In summary, there is very little, if any, high quality evidence to address the research question for this
review, 'What interventions are successful in managing disruptive clinician behaviour in nursing
workplaces?'
Number of studies included and excluded following critical appraisal Details of included studies can be found in Appendix VI and excluded studies in Appendix VII.
QARI Number of studies included Number of studies excluded
4 2
Number of studies included and excluded
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 623
NOTARI Number of studies included Number of studies excluded
14 26
Number of studies included and excluded
MASTARI Number of studies included Number of studies excluded
5 13
Results of metasynthesis of qualitative research findings
Meta-synthesis of studies included in the review generated two synthesised findings. These
synthesised findings were derived from 11 study findings that were subsequently aggregated into four
categories. The study findings are listed in Appendix VIII and the QARI view detailing the relationships
between study findings, categories and synthesised findings are also presented. The key to the
degrees of credibility used below and in Appendix VIII can be found in Appendix IX.
Synthesised Findings
Organisational approach
Organisational approach Building
Understanding and Skills
The use of cue cards with information about how to manage laterally violent behaviour was beneficial (C)43
Newly registered nurses felt that being educated about lateral violence was helpful and should be offered to all nurses (U) 43
Building and
maintaining a
positive work
environment
Nurses look up to other professionals and value inter-disciplinary teamwork. Nurses may sometime value teamwork over advocating the needs of the patient. Inter-professional relationships with medical staff remain unequal. (C)36
The subordinate role of women and societal expectations continue to influence nursing's lack of status and recognition. (C) 36
Professional relationships were one of two main issues raised by the action research group. Professional relationships include doctor-nurse, patient-nurse and nurse-nurse. (C) 80
Staff 'indoctrinated' into the 'rules' of work, as defined by the bullies (C) 48
Comments
The included papers provided a variety of discussions about appropriate organisational interventions
to address disruptive clinician behaviour.
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 624
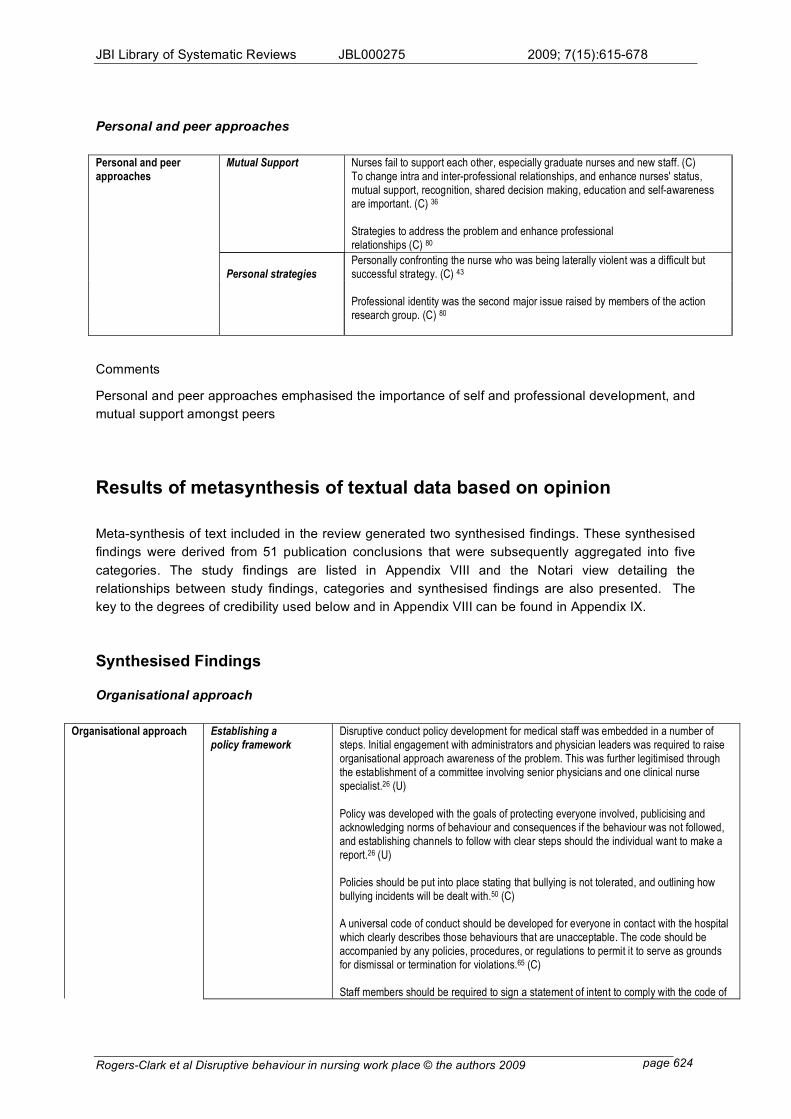
Personal and peer approaches
Mutual Support Nurses fail to support each other, especially graduate nurses and new staff. (C)
To change intra and inter-professional relationships, and enhance nurses' status, mutual support, recognition, shared decision making, education and self-awareness are important. (C) 36
Strategies to address the problem and enhance professional relationships (C) 80
Personal strategies
Personal and peer approaches
Personally confronting the nurse who was being laterally violent was a difficult but successful strategy. (C) 43
Professional identity was the second major issue raised by members of the action research group. (C) 80
Comments
Personal and peer approaches emphasised the importance of self and professional development, and
mutual support amongst peers
Results of metasynthesis of textual data based on opinion
Meta-synthesis of text included in the review generated two synthesised findings. These synthesised
findings were derived from 51 publication conclusions that were subsequently aggregated into five
categories. The study findings are listed in Appendix VIII and the Notari view detailing the
relationships between study findings, categories and synthesised findings are also presented. The
key to the degrees of credibility used below and in Appendix VIII can be found in Appendix IX.
Synthesised Findings
Organisational approach
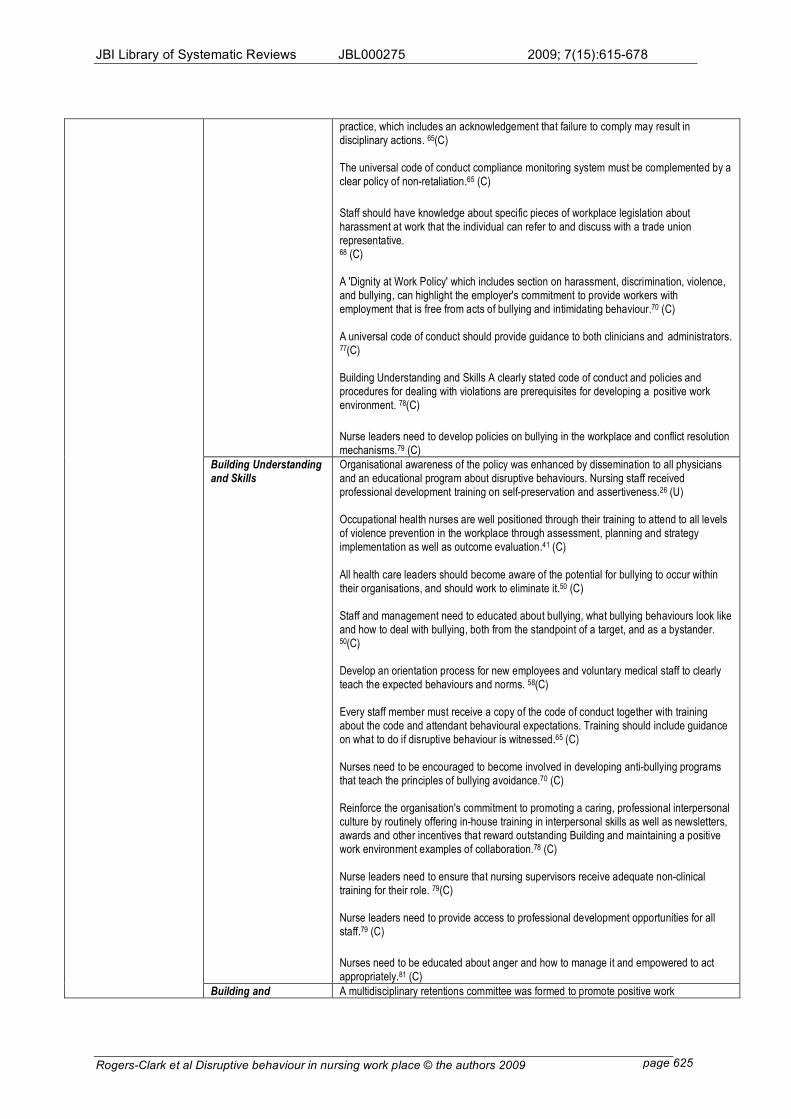
Organisational approach Establishing a
policy framework Disruptive conduct policy development for medical staff was embedded in a number of steps. Initial engagement with administrators and physician leaders was required to raise organisational approach awareness of the problem. This was further legitimised through the establishment of a committee involving senior physicians and one clinical nurse specialist.26 (U)
Policy was developed with the goals of protecting everyone involved, publicising and acknowledging norms of behaviour and consequences if the behaviour was not followed, and establishing channels to follow with clear steps should the individual want to make a report.26 (U) Policies should be put into place stating that bullying is not tolerated, and outlining how bullying incidents will be dealt with.50 (C) A universal code of conduct should be developed for everyone in contact with the hospital which clearly describes those behaviours that are unacceptable. The code should be accompanied by any policies, procedures, or regulations to permit it to serve as grounds for dismissal or termination for violations.65 (C) Staff members should be required to sign a statement of intent to comply with the code of
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 625
practice, which includes an acknowledgement that failure to comply may result in disciplinary actions. 65(C) The universal code of conduct compliance monitoring system must be complemented by a clear policy of non-retaliation.65 (C)
Staff should have knowledge about specific pieces of workplace legislation about harassment at work that the individual can refer to and discuss with a trade union representative. 68 (C) A 'Dignity at Work Policy' which includes section on harassment, discrimination, violence, and bullying, can highlight the employer's commitment to provide workers with employment that is free from acts of bullying and intimidating behaviour.70 (C) A universal code of conduct should provide guidance to both clinicians and administrators. 77(C) Building Understanding and Skills A clearly stated code of conduct and policies and procedures for dealing with violations are prerequisites for developing a positive work environment. 78(C) Nurse leaders need to develop policies on bullying in the workplace and conflict resolution mechanisms.79 (C)
Building Understanding and Skills
Organisational awareness of the policy was enhanced by dissemination to all physicians and an educational program about disruptive behaviours. Nursing staff received professional development training on self-preservation and assertiveness.26 (U) Occupational health nurses are well positioned through their training to attend to all levels of violence prevention in the workplace through assessment, planning and strategy implementation as well as outcome evaluation.41 (C)
All health care leaders should become aware of the potential for bullying to occur within their organisations, and should work to eliminate it.50 (C) Staff and management need to educated about bullying, what bullying behaviours look like and how to deal with bullying, both from the standpoint of a target, and as a bystander. 50(C) Develop an orientation process for new employees and voluntary medical staff to clearly teach the expected behaviours and norms. 58(C) Every staff member must receive a copy of the code of conduct together with training about the code and attendant behavioural expectations. Training should include guidance on what to do if disruptive behaviour is witnessed.65 (C) Nurses need to be encouraged to become involved in developing anti-bullying programs that teach the principles of bullying avoidance.70 (C) Reinforce the organisation's commitment to promoting a caring, professional interpersonal culture by routinely offering in-house training in interpersonal skills as well as newsletters, awards and other incentives that reward outstanding Building and maintaining a positive work environment examples of collaboration.78 (C) Nurse leaders need to ensure that nursing supervisors receive adequate non-clinical training for their role. 79(C) Nurse leaders need to provide access to professional development opportunities for all staff.79 (C)
Nurses need to be educated about anger and how to manage it and empowered to act appropriately.81 (C)
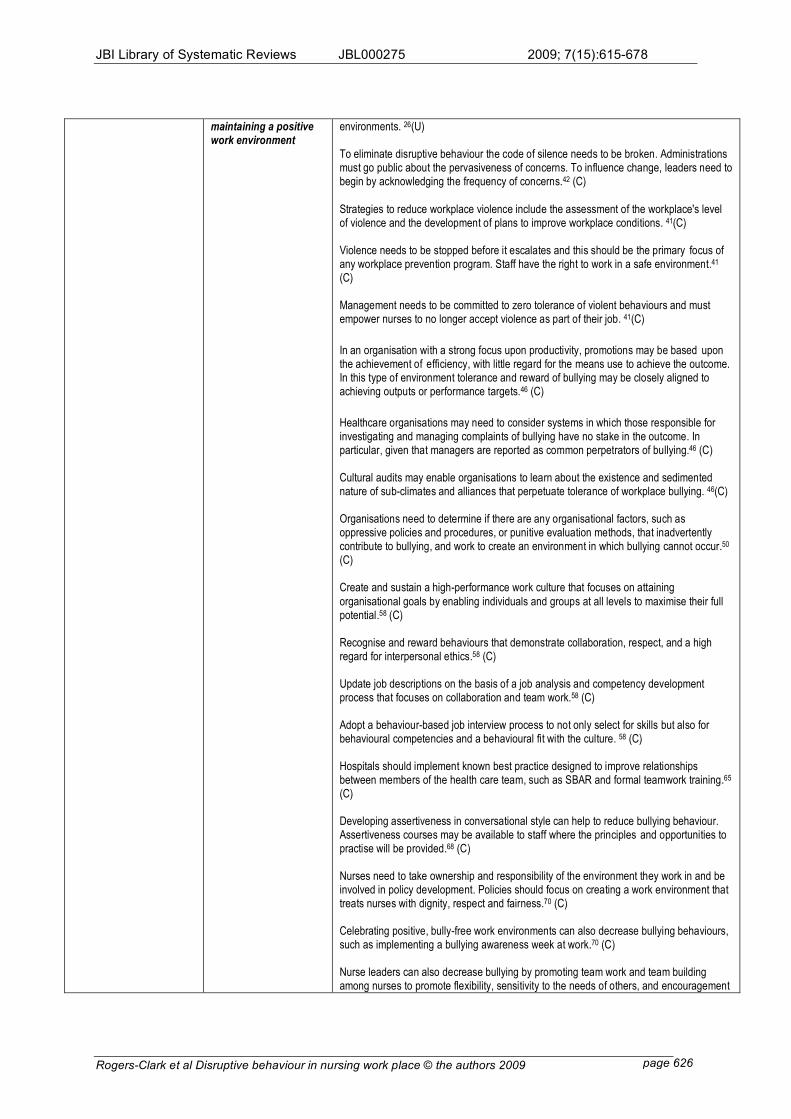
Building and A multidisciplinary retentions committee was formed to promote positive work
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 626
maintaining a positive work environment
environments. 26(U) To eliminate disruptive behaviour the code of silence needs to be broken. Administrations must go public about the pervasiveness of concerns. To influence change, leaders need to begin by acknowledging the frequency of concerns.42 (C)
Strategies to reduce workplace violence include the assessment of the workplace's level of violence and the development of plans to improve workplace conditions. 41(C) Violence needs to be stopped before it escalates and this should be the primary focus of any workplace prevention program. Staff have the right to work in a safe environment.41 (C) Management needs to be committed to zero tolerance of violent behaviours and must empower nurses to no longer accept violence as part of their job. 41(C)
In an organisation with a strong focus upon productivity, promotions may be based upon the achievement of efficiency, with little regard for the means use to achieve the outcome. In this type of environment tolerance and reward of bullying may be closely aligned to achieving outputs or performance targets.46 (C)
Healthcare organisations may need to consider systems in which those responsible for investigating and managing complaints of bullying have no stake in the outcome. In particular, given that managers are reported as common perpetrators of bullying.46 (C) Cultural audits may enable organisations to learn about the existence and sedimented nature of sub-climates and alliances that perpetuate tolerance of workplace bullying. 46(C) Organisations need to determine if there are any organisational factors, such as oppressive policies and procedures, or punitive evaluation methods, that inadvertently contribute to bullying, and work to create an environment in which bullying cannot occur.50 (C) Create and sustain a high-performance work culture that focuses on attaining
organisational goals by enabling individuals and groups at all levels to maximise their full potential.58 (C) Recognise and reward behaviours that demonstrate collaboration, respect, and a high regard for interpersonal ethics.58 (C) Update job descriptions on the basis of a job analysis and competency development process that focuses on collaboration and team work.58 (C) Adopt a behaviour-based job interview process to not only select for skills but also for behavioural competencies and a behavioural fit with the culture. 58 (C) Hospitals should implement known best practice designed to improve relationships between members of the health care team, such as SBAR and formal teamwork training.65 (C) Developing assertiveness in conversational style can help to reduce bullying behaviour. Assertiveness courses may be available to staff where the principles and opportunities to practise will be provided.68 (C) Nurses need to take ownership and responsibility of the environment they work in and be involved in policy development. Policies should focus on creating a work environment that treats nurses with dignity, respect and fairness.70 (C) Celebrating positive, bully-free work environments can also decrease bullying behaviours, such as implementing a bullying awareness week at work.70 (C) Nurse leaders can also decrease bullying by promoting team work and team building among nurses to promote flexibility, sensitivity to the needs of others, and encouragement
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 627
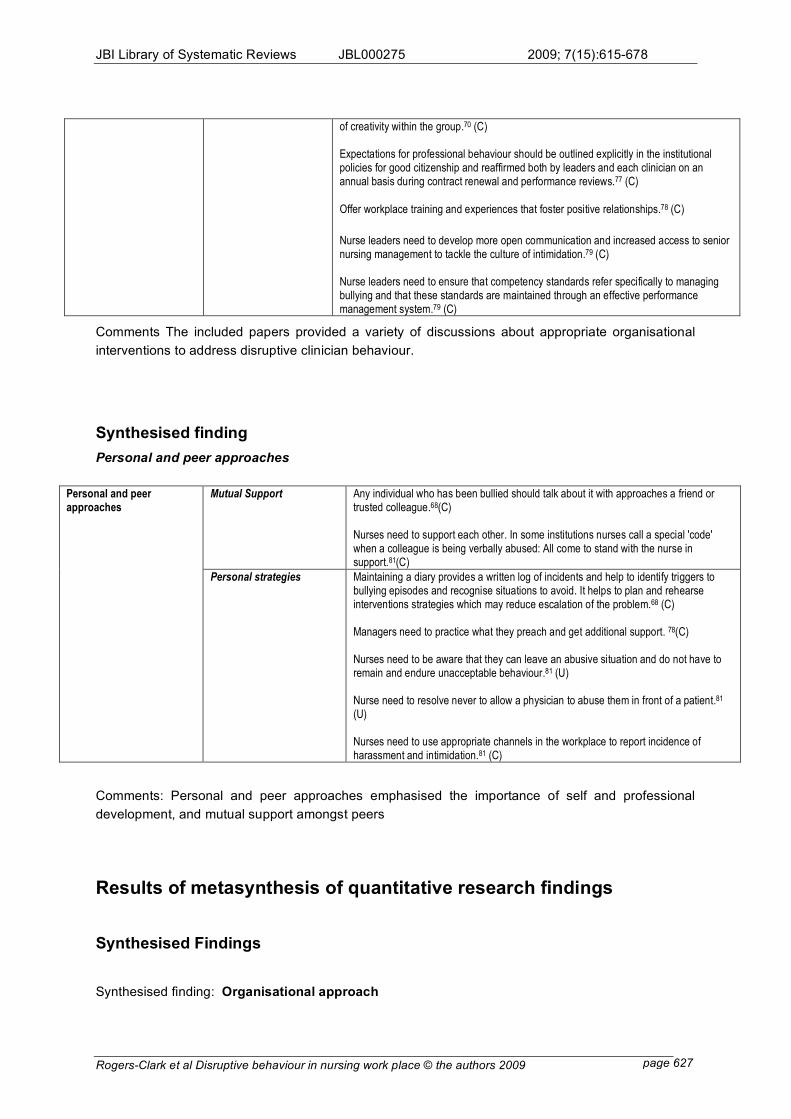
of creativity within the group.70 (C) Expectations for professional behaviour should be outlined explicitly in the institutional policies for good citizenship and reaffirmed both by leaders and each clinician on an annual basis during contract renewal and performance reviews.77 (C)
Offer workplace training and experiences that foster positive relationships.78 (C)
Nurse leaders need to develop more open communication and increased access to senior nursing management to tackle the culture of intimidation.79 (C) Nurse leaders need to ensure that competency standards refer specifically to managing bullying and that these standards are maintained through an effective performance management system.79 (C)
Comments The included papers provided a variety of discussions about appropriate organisational
interventions to address disruptive clinician behaviour.
Synthesised finding
Personal and peer approaches
Mutual Support Any individual who has been bullied should talk about it with approaches a friend or
trusted colleague.68(C) Nurses need to support each other. In some institutions nurses call a special 'code' when a colleague is being verbally abused: All come to stand with the nurse in support.81(C)
Personal and peer approaches
Personal strategies Maintaining a diary provides a written log of incidents and help to identify triggers to bullying episodes and recognise situations to avoid. It helps to plan and rehearse interventions strategies which may reduce escalation of the problem.68 (C) Managers need to practice what they preach and get additional support. 78(C) Nurses need to be aware that they can leave an abusive situation and do not have to remain and endure unacceptable behaviour.81 (U) Nurse need to resolve never to allow a physician to abuse them in front of a patient.81 (U) Nurses need to use appropriate channels in the workplace to report incidence of harassment and intimidation.81 (C)
Comments: Personal and peer approaches emphasised the importance of self and professional
development, and mutual support amongst peers
Results of metasynthesis of quantitative research findings
Synthesised Findings
Synthesised finding: Organisational approach
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 628
Comments: The included papers provided a variety of discussions about appropriate organisational
interventions to address disruptive clinician behaviour.
Synthesised finding: Personal and peer approaches
Comments: Personal and peer approaches emphasised the importance of self and professional
development, and mutual support amongst peers
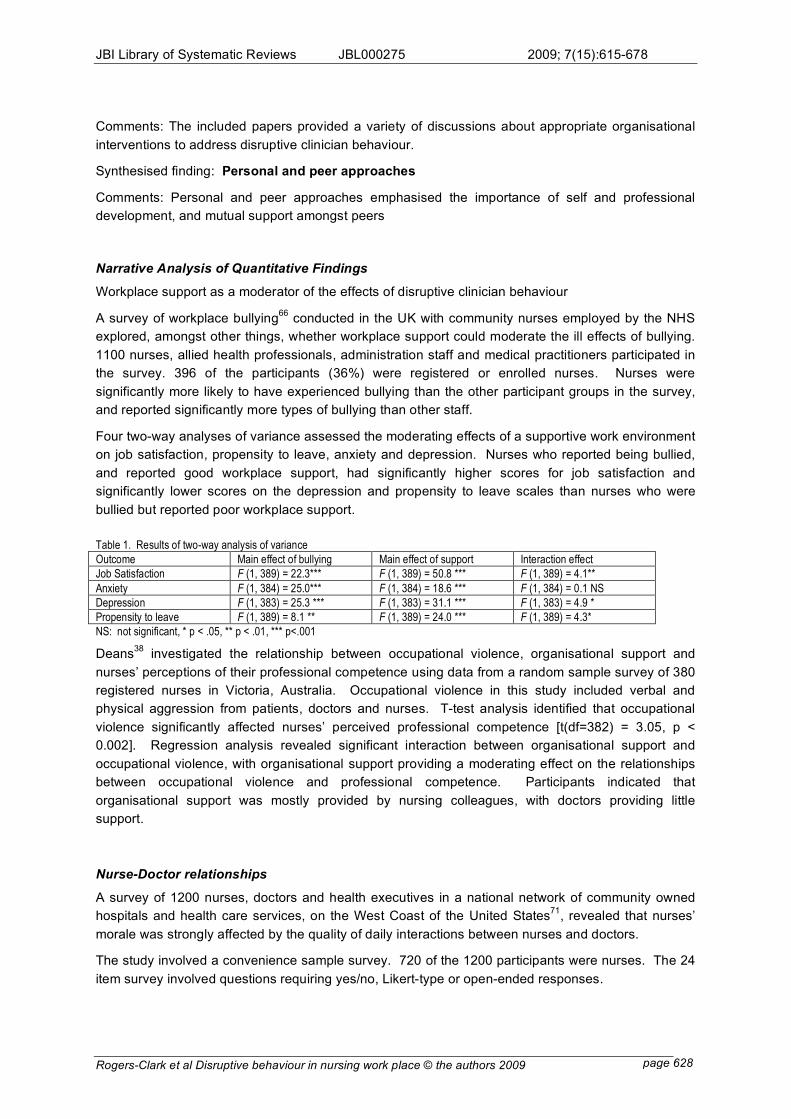
Narrative Analysis of Quantitative Findings
Workplace support as a moderator of the effects of disruptive clinician behaviour
A survey of workplace bullying66
conducted in the UK with community nurses employed by the NHS
explored, amongst other things, whether workplace support could moderate the ill effects of bullying.
1100 nurses, allied health professionals, administration staff and medical practitioners participated in
the survey. 396 of the participants (36%) were registered or enrolled nurses. Nurses were
significantly more likely to have experienced bullying than the other participant groups in the survey,
and reported significantly more types of bullying than other staff.
Four two-way analyses of variance assessed the moderating effects of a supportive work environment
on job satisfaction, propensity to leave, anxiety and depression. Nurses who reported being bullied,
and reported good workplace support, had significantly higher scores for job satisfaction and
significantly lower scores on the depression and propensity to leave scales than nurses who were
bullied but reported poor workplace support.
Table 1. Results of two-way analysis of variance
Outcome Main effect of bullying Main effect of support Interaction effect
Job Satisfaction F (1, 389) = 22.3*** F (1, 389) = 50.8 *** F (1, 389) = 4.1**
Anxiety F (1, 384) = 25.0*** F (1, 384) = 18.6 *** F (1, 384) = 0.1 NS
Depression F (1, 383) = 25.3 *** F (1, 383) = 31.1 *** F (1, 383) = 4.9 *
Propensity to leave F (1, 389) = 8.1 ** F (1, 389) = 24.0 *** F (1, 389) = 4.3*
NS: not significant, * p < .05, ** p < .01, *** p<.001
Deans38
investigated the relationship between occupational violence, organisational support and
nurses’ perceptions of their professional competence using data from a random sample survey of 380
registered nurses in Victoria, Australia. Occupational violence in this study included verbal and
physical aggression from patients, doctors and nurses. T-test analysis identified that occupational
violence significantly affected nurses’ perceived professional competence [t(df=382) = 3.05, p <
0.002]. Regression analysis revealed significant interaction between organisational support and
occupational violence, with organisational support providing a moderating effect on the relationships
between occupational violence and professional competence. Participants indicated that
organisational support was mostly provided by nursing colleagues, with doctors providing little
support.
Nurse-Doctor relationships
A survey of 1200 nurses, doctors and health executives in a national network of community owned
hospitals and health care services, on the West Coast of the United States71
, revealed that nurses’
morale was strongly affected by the quality of daily interactions between nurses and doctors.
The study involved a convenience sample survey. 720 of the 1200 participants were nurses. The 24
item survey involved questions requiring yes/no, Likert-type or open-ended responses.
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 629
One open-ended question in the survey asked participants to suggest strategies for improving nurse-
doctor relationships. 161 of the 556 nurse participants (29%) suggested that improved opportunities
for collaboration and communication would be most helpful. 131 nurses (24%) indicated that
education and training for nurses and doctors about how to build more positive working relationships
would be helpful. 38 nurses (6.8%) identified that more open forums and group discussions were
necessary, and 37 (6.7%) felt that both nurses and doctors needed to accept more accountability for
their actions.
Conflict Management Training to assist with difficulties in nurse/doctor relationships
A small study30
, using a quasi-experimental design, explored nurses’ perceptions of collaboration with
their medical colleagues before and after conflict management training. The study was set in a 372
bed private hospital in Southern California. Eighteen registered nurses were in the control group (no
conflict management training) and nine were in the experimental group. The nurses in the control
group worked on the telemetry unit within the same hospital, and had access to the same medical
practitioners as the nurses in the experimental group.
The conflict management training was based on a view that conflict begins with misunderstandings
and defensiveness. A psychodynamic approach (focus on changing thinking) underpinned the
training.
Participants in both the experimental and control groups completed the Collaborative Behaviour Scale
(CBS), a twenty item 4-point Likert-type scale, with established reliability and validity. Participants
completed the scale at baseline and at three months post-test. There were no significant differences
between the control and experimental groups on the CBS at baseline (p>.05) and at post-test, F
(1,27) = 1.47, p = .236. The intervention was not effective in enhancing nurses’ perceptions of
collaboration and conflict management with the medical practitioners working in their unit. Indeed,
scores on the CBS for the experimental group were worse at post-test than at pre-test, though not
significantly.
Of note was that only nurses were involved in the conflict management training. The medical
practitioners on the unit did not participate.
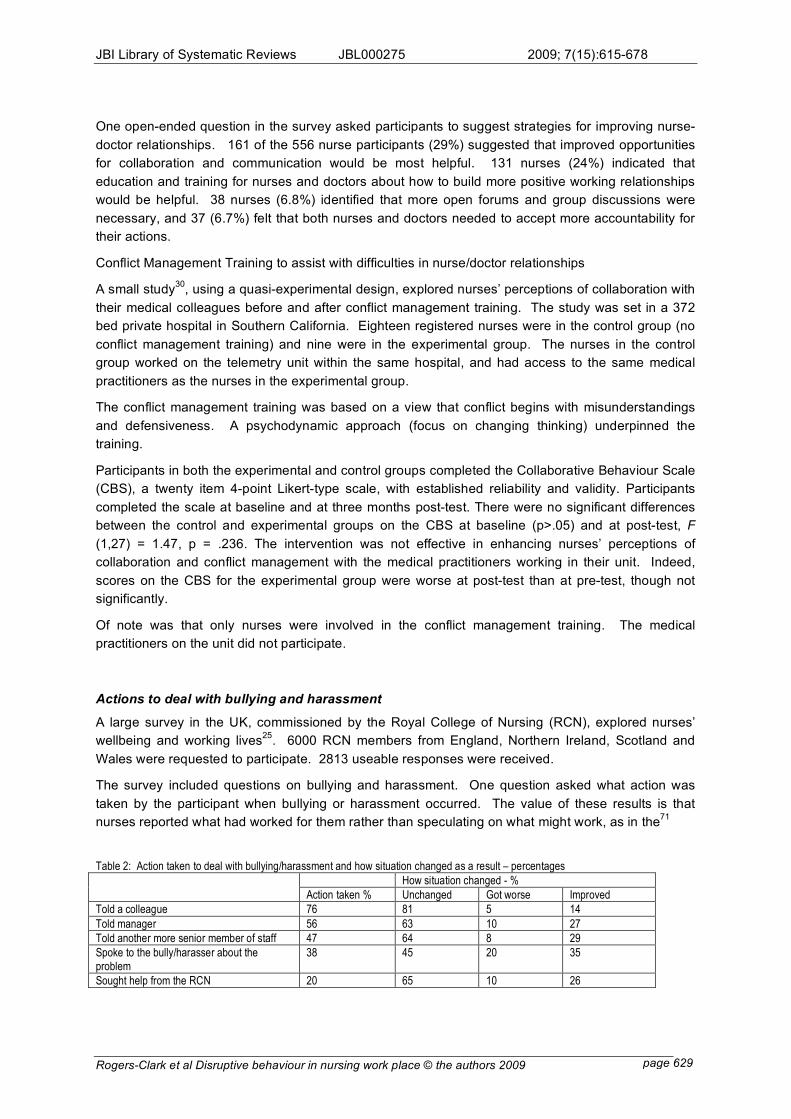
Actions to deal with bullying and harassment
A large survey in the UK, commissioned by the Royal College of Nursing (RCN), explored nurses’
wellbeing and working lives25
. 6000 RCN members from England, Northern Ireland, Scotland and
Wales were requested to participate. 2813 useable responses were received.
The survey included questions on bullying and harassment. One question asked what action was
taken by the participant when bullying or harassment occurred. The value of these results is that
nurses reported what had worked for them rather than speculating on what might work, as in the71
Table 2: Action taken to deal with bullying/harassment and how situation changed as a result – percentages
How situation changed - %
Action taken % Unchanged Got worse Improved
Told a colleague 76 81 5 14
Told manager 56 63 10 27
Told another more senior member of staff 47 64 8 29
Spoke to the bully/harasser about the problem
38 45 20 35
Sought help from the RCN 20 65 10 26
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 630
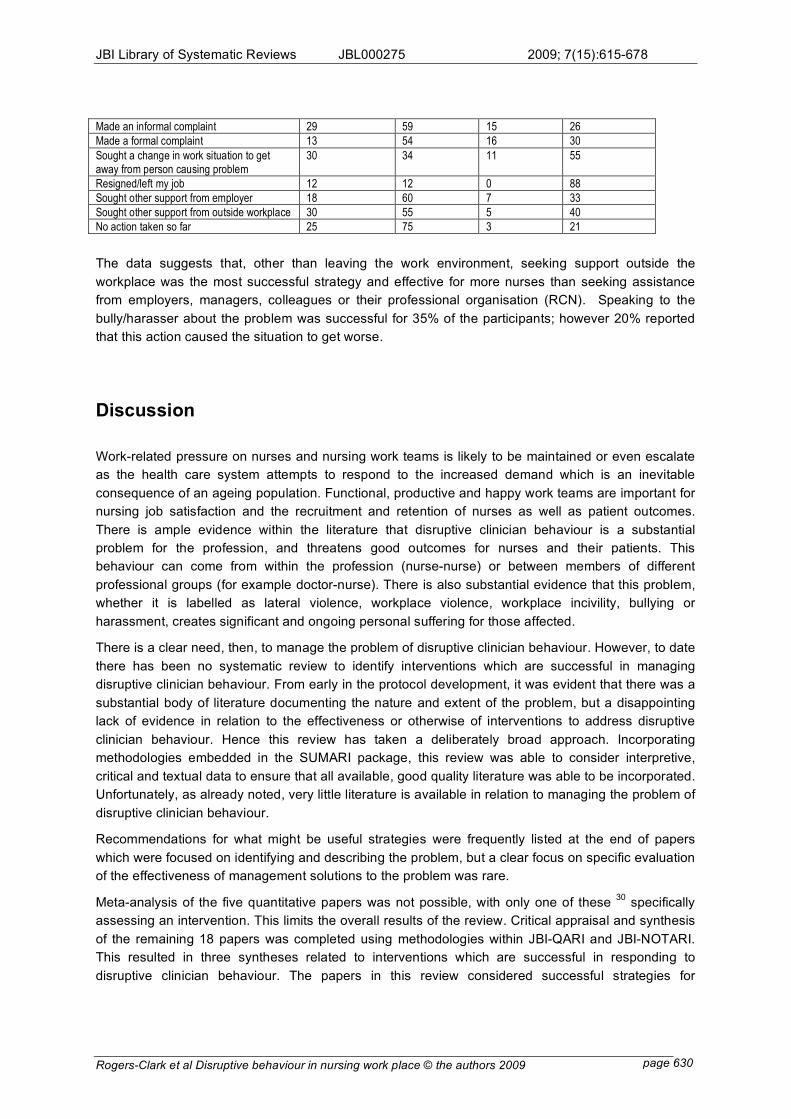
Made an informal complaint 29 59 15 26
Made a formal complaint 13 54 16 30
Sought a change in work situation to get away from person causing problem
30 34 11 55
Resigned/left my job 12 12 0 88
Sought other support from employer 18 60 7 33
Sought other support from outside workplace 30 55 5 40
No action taken so far 25 75 3 21
The data suggests that, other than leaving the work environment, seeking support outside the
workplace was the most successful strategy and effective for more nurses than seeking assistance
from employers, managers, colleagues or their professional organisation (RCN). Speaking to the
bully/harasser about the problem was successful for 35% of the participants; however 20% reported
that this action caused the situation to get worse.
Discussion
Work-related pressure on nurses and nursing work teams is likely to be maintained or even escalate
as the health care system attempts to respond to the increased demand which is an inevitable
consequence of an ageing population. Functional, productive and happy work teams are important for
nursing job satisfaction and the recruitment and retention of nurses as well as patient outcomes.
There is ample evidence within the literature that disruptive clinician behaviour is a substantial
problem for the profession, and threatens good outcomes for nurses and their patients. This
behaviour can come from within the profession (nurse-nurse) or between members of different
professional groups (for example doctor-nurse). There is also substantial evidence that this problem,
whether it is labelled as lateral violence, workplace violence, workplace incivility, bullying or
harassment, creates significant and ongoing personal suffering for those affected.
There is a clear need, then, to manage the problem of disruptive clinician behaviour. However, to date
there has been no systematic review to identify interventions which are successful in managing
disruptive clinician behaviour. From early in the protocol development, it was evident that there was a
substantial body of literature documenting the nature and extent of the problem, but a disappointing
lack of evidence in relation to the effectiveness or otherwise of interventions to address disruptive
clinician behaviour. Hence this review has taken a deliberately broad approach. Incorporating
methodologies embedded in the SUMARI package, this review was able to consider interpretive,
critical and textual data to ensure that all available, good quality literature was able to be incorporated.
Unfortunately, as already noted, very little literature is available in relation to managing the problem of
disruptive clinician behaviour.
Recommendations for what might be useful strategies were frequently listed at the end of papers
which were focused on identifying and describing the problem, but a clear focus on specific evaluation
of the effectiveness of management solutions to the problem was rare.
Meta-analysis of the five quantitative papers was not possible, with only one of these 30
specifically
assessing an intervention. This limits the overall results of the review. Critical appraisal and synthesis
of the remaining 18 papers was completed using methodologies within JBI-QARI and JBI-NOTARI.
This resulted in three syntheses related to interventions which are successful in responding to
disruptive clinician behaviour. The papers in this review considered successful strategies for
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 631
managing disruptive clinician behaviour using two main approaches. The first involved implementing
and evaluating an intervention. Only three of the nine research papers in this review took this
approach, and all involved a localised intervention and small numbers of participants. The second
approach, used in the remaining six research papers, was to survey nurses and asks them to identify
strategies which they believed had been or would be effective. These papers were not focused
specifically on an intervention focus, and hence these questions were generally part of a broader
study which looked at the problems associated with disruptive clinician behaviour.
The results of this review, limited though they are because of the limited literature addressing the
review topic, do provide some suggestions about interventions which may be of use in managing this
pervasive problem. An appropriate organisational focus on the problem is essential. Disruptive
clinician behaviour flourishes in work environments where such behaviour is ignored, tolerated or
even rewarded. Zero tolerance policies, which clearly identify what constitutes disruptive clinician
behaviour (often using the titles of bullying and harassment), are required, accompanied by clear
strategies for managing the problem and possible consequences if the behaviour does not cease. An
organisational commitment to implementing the policy is just as important and identified strategies
should be consistently adhered to. This is a critical issue in health care, where at times disruptive
behaviour is excused because the clinician is highly competent and seen as effective in his/her role,
or where different rules and/or expectations apply to different professionals. Bullying behaviours may
actually be rewarded if the perpetrator is seen as someone who can 'get results'. Dealing with
managers who are displaying disruptive behaviours is seen as crucial yet challenging. Very often,
organisations believe they have handled the problem because they have introduced a zero tolerance
policy, and charged managers with the responsibility for implementing it. However, if the disruptive
behaviour is pervasive within the management group, this is clearly an inappropriate strategy. Hence,
it is important that the organisational approach does not assume that the disruptive behaviour occurs
vertically and that managers are not engaged in such behaviour.
One paper in particular48
identified that disruptive clinician behaviour may be a group behaviour rather
than an individual response. That is, groups of clinicians may form informal alliances and operate
together to achieve their goals. These goals may include maintenance of the status quo, or of their
positions of power within a work team. This then raises issues of workplace culture, as distinct from a
perspective which sees isolated individuals as the problem. Another important aspect of an
organisational approach is to build and sustain a positive work environment. Strengthening inter-
professional relationships were seen as important for minimising disruptive clinician behaviour,
particularly in relationships traditionally marked by unequal power relationships, such as those
between nurses and medical practitioners. The creation of multidisciplinary committee to promote
positive work environments were suggested a number of times. Formal teamwork training was seen
to be important, as was identifying and rewarding positive behaviours.
Open communication between staff at different levels within the organisation makes it possible for
disruptive clinician behaviour to be reported when it occurs. A range of personal or peer responses to
disruptive behaviour were also identified. The three intervention studies fitted into this category. One
focused on teaching conflict resolution skills to nurses, to help them manage disruptive behaviour
within their interdisciplinary team30
. A second assessed the effectiveness of cognitive rehearsal as a
skill newly graduated nurses could use to help them deal with lateral violence43
. The third intervention
study involved the use of reflection on practice issues in an action research group involving registered
nurses, where the nurses chose to focus their efforts on dysfunctional nurse-nurse relationships.
None of these studies addressed the disruptive behaviour itself. Instead, their focus was on helping

JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 632
nurses manage the disruptive behaviour of their colleagues. There was, then, no focus on the
perpetrators.
Conclusion
Nurses constitute the largest group of professional in the health care arena and their contribution to
the health and wellbeing of society is well recognised and, within the community at least, highly
valued. Nursing is a profession which is intrinsically challenging. Increasing workloads, the pace of
change, more focus on budgetary control, accountability and outcomes, and a shortage of skilled staff
within the health care system create substantial levels of stress for nurses who are already fully
occupied on a daily basis in responding to the complex needs of patients and their families. In this
environment, dealing with team members who engage in disruptive behaviours is an added and
unnecessary burden. The evidence is that this burden is felt on personal, professional and systemic
levels.
Disruptive clinician behaviour is personally damaging to the nurses who have to deal with it in their
work teams, but is also damaging to the profession of nursing which seeks to improve its image,
demonstrate the positive outcomes of nursing work, and recruit and retain high quality graduates.
Finally, disruptive clinician behaviour is damaging to the effective functioning and outputs of the health
care system. It is a cause of staff dissatisfaction, higher turnover and is linked to poor outcomes in
relation to patient safety.
Despite recognition of the wide implications of this problem, to date very few studies have been
undertaken to systematically assess the effectiveness of intervention strategies. Hence, there is little
evidence to answer the research question guiding this systematic review, which asks what
interventions are successful in managing disruptive clinician behaviour.
Implications for practice
Health care organisations need to make the creation of healthy work environments a priority, as
nurses and indeed any health professionals cannot and do not work effectively in an environment that
is unsupportive and toxic. The extent of the problem is perhaps best demonstrated by the proposal
that nursing students need specific training in how to manage the horizontal violence they are bound
to encounter in their professional lives. This is a telling acknowledgement that the profession is well
aware of the problem but has not been able to address it successfully. There is clear evidence that
disruptive clinician behaviour reduces the quality of communication within a team and hence
threatens patient safety, as well as making the workplace unpleasant and at times unbearable.
Given the evidence documenting the extent of disruptive clinician behaviour, and its consequences,
effectively addressing the issue of disruptive behaviour in nursing workplaces is critically important in
achieving a healthy work environment. This is, however, a challenging task when there is little
empirical evidence to support decision-making about appropriate strategies to implement. The
evidence that is available documents some success in helping nurses to manage disruptive behaviour
from their colleagues. However, this is a reactive approach and does little if anything to address the
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 633
problem itself. The expert opinion literature suggests that a whole or organisation approach is
required, with relevant policy and process developed and implemented. Of critical importance is that
the policy must be applied to all staff regardless of their seniority within the organisation, their length
of service or their competence as clinicians.
Consideration needs to be given to how to manage managers who themselves engage in disruptive
behaviour, given that it is generally managers who are responsible for the policy implementation. In
health care settings where ongoing institutional change is the norm, rewarding managers and
significant other players for getting results at all costs, even if that is at the expense of nurses morale
and job satisfaction, encourages bullying and is ultimately unproductive. Training is important, as is
including a focus on identifying and rewarding positive behaviour which supports happy, positive work
environments.
Implications for research
This systematic review has demonstrated a clear and urgent need for research which implements and
evaluates strategies specifically designed to respond to the problem of disruptive clinician behaviour.
Due to the limited evidence currently available on what is the current best practice to manage
disruptive behaviours in the health care setting, there is an urgent need for researchers and health
care leaders to use action research and other relevant methodologies to develop implement and
evaluate strategies to manage disruptive clinician behaviour.
Conflict of Interest
No conflict of interest could be identified.
Acknowledgements
We would like to acknowledge Professor Gerry Fogarty from the University of Southern Queensland
and Ms Linda Hardy from Queensland Health for their assistance in reviewing this work.
References
1 Bennet, Margaret, Priorities for Nursing and Midwifery Research, Nursing & Nursing Education
Taskforce, 2006.
2 Brown, R.B. & Brooks, I, Emotion at work: Identifying the emotional climate of night nursing,
Journal of Management in Medicine, 16:327-344 2002.
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 634
3 Cortina, L.M. & Magley, V.J. & Hunter Williams, J. & Day Langhout, R., Incivility in the workplace:
incidence and impact, Journal of Occupational Health Psychology, 6:64-80 2001.
4 Felblinger, D. M., Incivility and bullying in the workplace and nurses' shame responses, JOGNN,
37:234-242 2008.
5 Fellowes, D. & Wilkinson, S. & Moore, P., Communication skills training for health care
professionals working with cancer patients, their families and/or carers, The Cochrane Database
of Systematic Reviews 2007-1, : 2003.
6 Fineman, S. (ed), Emotions in Organisations, Sage Publications, London, 1993.
7 Hutchinson, M. & Vickers, M. & Jackson, D. & Wilkes, L., Workplace bullying in nursing: towards a
more critical organisational perspective, Nursing Inquiry, 13:118-126 2006.
8 Hutton, S.A., Workplace incivility, JONA: The Journal of Nursing Administration, 36:22-28 2006.
9 Joint Commission on Accreditation of Healthcare Organisations, Proposed Standard for
Disruptive Behaviour-Hospital, http://www.jointcommission.org/NR/rdonlyres/@BF44E9F-6EE0-
4856-83EF-778FA47723B/0/Disruptive_Behavior_cah_stds.pdf, 2007.
10 MacIntosh, J., Tackling work place bullying, Issues in Mental Health Nursing, 27:665-679 2006.
11 McGee, D. & Shigemitsu, H. & Henig, N. & Raffin, T., Conflict over communication and
unprofessional staff behaviour: A source of dissatisfaction during the withdrawal of care? Critical
Care Medicine, 28:217-219 2001.
12 McIIduff, E. & Coghlan, D., Understanding and contending with passive-aggressive behaviour in
teams and organizations, Journal of Managerial Psychology, 15:716-736 2000.
13 Office of Public Service Merit and Equity (State of Queensland), Quality public service workplaces
information paper 8, Organisation Health: 2006.
14 Office of the Public Service, A focus on people: A workforce management strategy for the
Queensland public sector, Brisbane, Queensland, 1997.
15 Pearson A, Balancing the evidence: incorporating the synthesis of qualitative data into systematic
reviews, JBI Reports, :45-64 2004.
16 Pearson, C.M. & Andersson, L.M. & Wegner, J., When workers flout convention: A study of
workplace incivility, Human Relations, 54:1387-1419 2001.
17 Queensland Health, Workplace culture and
leadership,http://qheps.health.qld.gov.au/betterworkplaces/culture/home.htm, : 2007.
18 Queensland Health, Queensland Health Systems Review. Final
Report,http://qheps.health.qld.gov.au/health_sys_review/final/qhsr_final_report.pdf, : 2005.
19 Rayner, C. & Hoel, H. & Cooper, C.L., Workplace Bullying. What we know, who is to blame, and
what we do?, 2002.
20 Rime, B. & Mesquite, B. & Philpott, P. & Boca, S., Beyond the emotional event: six studies on the
social sharing of emotion, Journal of Cognition and Emotion, 5:435-65 1991.
21 Roberts, S.J. & Demarco, R. & Griffin, M., The effect of group behaviours on the culture of the
nursing workplace: a review of the evidence and interventions for change, Journal of Nursing
Management, 0:1-6 2008.
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 635
22 Rosenstein, A. H. & O'Daniel, M., Disruptive Behaviour & Clinical Outcomes: Perceptions of
Nurses & Physicians: Nurses, physicians, and administrators say that clinicians' disruptive
behaviour has negative effects on clinical outcomes. Nursing Management, 36:18 2005.
23 Simons, S.R., Workplace bullying experienced by nurses newly licensed in Massachusetts,
Dissertation Abstracts International: Section B: The Science and Engineering, 67:3065 2006.
Appendix I: Search Strategy
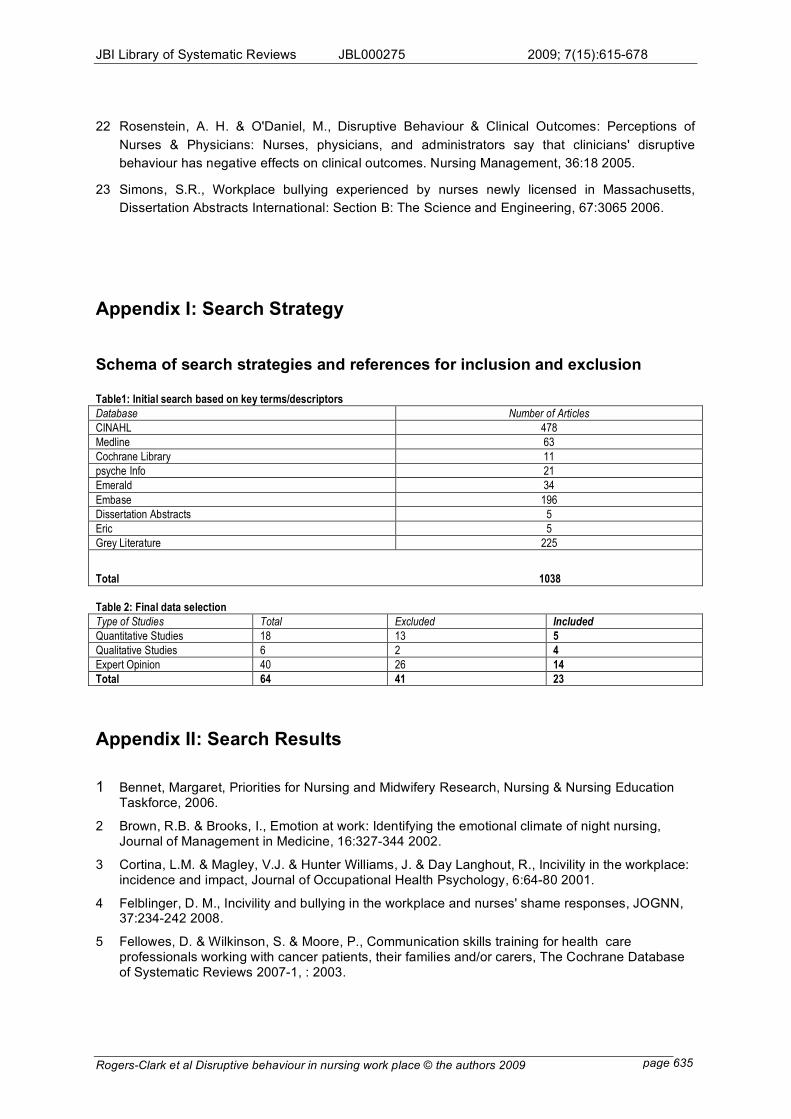
Schema of search strategies and references for inclusion and exclusion Table1: Initial search based on key terms/descriptors
Database Number of Articles
CINAHL 478
Medline 63
Cochrane Library 11
psyche Info 21
Emerald 34
Embase 196
Dissertation Abstracts 5
Eric 5
Grey Literature 225
Total 1038
Table 2: Final data selection
Type of Studies Total Excluded Included
Quantitative Studies 18 13 5
Qualitative Studies 6 2 4
Expert Opinion 40 26 14
Total 64 41 23
Appendix II: Search Results
1 Bennet, Margaret, Priorities for Nursing and Midwifery Research, Nursing & Nursing Education Taskforce, 2006.
2 Brown, R.B. & Brooks, I., Emotion at work: Identifying the emotional climate of night nursing, Journal of Management in Medicine, 16:327-344 2002.
3 Cortina, L.M. & Magley, V.J. & Hunter Williams, J. & Day Langhout, R., Incivility in the workplace: incidence and impact, Journal of Occupational Health Psychology, 6:64-80 2001.
4 Felblinger, D. M., Incivility and bullying in the workplace and nurses' shame responses, JOGNN, 37:234-242 2008.
5 Fellowes, D. & Wilkinson, S. & Moore, P., Communication skills training for health care professionals working with cancer patients, their families and/or carers, The Cochrane Database of Systematic Reviews 2007-1, : 2003.
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 636
6 Fineman, S. (ed), Emotions in Organisations, Sage Publications, London, : 1993.
7 Hutchinson, M. & Vickers, M. & Jackson, D. & Wilkes, L., Workplace bullying in nursing: towards a more critical organisational perspective, Nursing Inquiry, 13:118-126 2006.
8 Hutton, S.A., Workplace incivility, JONA: The Journal of Nursing Administration, 36:22-28 2006.
9 Joint Commission on Accreditation of Healthcare Organisations, Proposed Standard for Disruptive Behaviour-Hospital, http://www.jointcommission.org/NR/rdonlyres/@BF44E9F-6EE0-4856-83EF-778FA47723B/0/Disruptive_Behavior_cah_stds.pdf, : 2007.
10 MacIntosh, J., Tackling work place bullying, Issues in Mental Health Nursing, 27:665-679 2006.
11 McGee, D. & Shigemitsu, H. & Henig, N. & Raffin, T., Conflict over communication and unprofesional staff behaviour: A source of dissatisfaction during the withdrawal of care?, Critical Care Medicine, 28:217-219 2001.
12 McIIduff, E. & Coghlan, D., Understanding and contending with passive-aggressive behaviour in teams and organizations, Journal of Managerial Psychology, 15:716-736 2000.
13 Office of Public Service Merit and Equity (State of Queensland), Quality public service workplaces information paper 8, Organisation Health, 2006.
14 Office of the Public Service, A focus on people: A workforce management strategy for the Queensland public sector, Brisbane, Queensland,: 1997.
15 Pearson A, Balancing the evidence: incorporating the synthesis of qualitative data into systematic reviews, JBI Reports,:45-64 2004.
16 Pearson, C.M. & Andersson, L.M. & Wegner, J., When workers flout convention: A study of workplace incivility, Human Relations, 54:1387-1419 2001.
17 Queensland Health, Workplace culture and leadership, http://qheps.health.qld.gov.au/betterworkplaces/culture/home.htm, 2007.
18 Queensland Health, Queensland Health Systems Review. Final Report, http://qheps.health.qld.gov.au/health_sys_review/final/qhsr_final_report.pdf, 2005.
19 Rayner, C. & Hoel, H. & Cooper, C.L., Workplace Bullying. What we know, who is to blame, and what wer do? 2002.
20 Rime, B. & Mesquite, B. & Philpott, P. & Boca, S., Beyond the emotional event: six studies on the social sharing of emotion, Journal of Cognition and Emotion, 5:435-65 1991.
21 Roberts, S.J. & Demarco, R. & Griffin, M., The effect of group behaviours on the culture of the nursing workplace: a review of the evidence and interventions for change, Journal of Nursing Management, 0:1-6 2008.
22 Rosenstein, A. H. & O'Daniel, M., Disruptive Behaviour & Clinical Outcomes: Perceptions of Nurses & Physicians: Nurses, physicians, and administrators say that clinicians' disruptive behaviour has negative effects on clinical outcomes. Nursing Management, 36:18 2005.
23 Simons, S.R., Workplace bullying experienced by nurses newly licensed in Massachusetts, Dissertation Abstracts International: Section B: The Science and Engineering, 67:3065 2006.
24 Antecol, H. & Cobb-Clark, D., Does sexual harassment training change attitudes? A view from the Federal level, Social Science Quarterly, 84:826-842 2003.
25 Ball, J. & Pike, G., At breaking point? A survey of the wellbeing and working lives of nurses in 2005, PTRC, University of Leeds, 0:0 2006.
26 Barnsteiner, J.H. & Madigan, C., Instituting a disruptive conduct policy for medical staff,AACN Clinical Issues, 12:378-382 2001.
27 Beech, B., Beating the bullies, Emergency Nurse, 12:35 2004.
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 637
28 Befar, K.J & Peterson, R.S. & Mannix, E.A. & Trochim, M.K., The critical role of conflict resolution in teams: a close look at the links between conflict type, conflict management strategies, and team outcomes, Journal of Applied Psychology , 93:170-188 2008.
29 Beyea, Suzanne C., Intimidation in health care settings and patient safety, AORN Journal, 80:115-117 2004.
30 Boone, B. N.& King, M. L. et al. , Conflict management training and nurse-physician collaborative behaviours., Journal for Nurses in Staff Development : JNSD: Official journal of the National Nursing Staff Development Organization , 24:168-175 2008.
31 Brennan, W. I'm talking to you! Managing bullying and harassment in the workplace, Emergency nurse: the journal of the RCN Accident and Emergency Nursing Association, 7:16-20 1999.
32 Broome, B. A., Dealing with sharks and bullies in the workplace, ABNF Journal, 19:28-30 2008.
33 Cassirer, C.D. & Anderson, D. & Hanson, S., Abusive behaviour in the healthcare workplace, Creative Nursing, 8:8-9 2002.
34 Corr, Margaret, Reducing occupational stress in intensive care, Nursing in Critical Care,5:76-81 2000.
35 Crawford, N., Conundrums and confusion in organisations: the etymology of the word 'bully', International Journal of Manpower, 20:86-93 1999.
36 Daisiki, I., Changing nurses' dis-empowering relationship patterns, Journal of Advanced Nursing, 48:43-50 2004.
37 DeChurch, L. A., K. L. Hamilton, et al. , Effects of conflict management strategies on perceptions of intragroup conflict., Group Dynamics: Theory, Research and Practice ,11:66-78 2007.
38 Deans, C. , Nurses and occupational violence: the role of organisational support in moderating professional competence., Australian Journal of Advanced Nursing , 22:14-18 2004.
39 Everton, W.J. & Jolton, J. A. & Mastrangelo, P.M., Be nice and fair or else: understanding reasons for employees' deviant behaviours, Journal of Management Development, 26:117-131 2007.
40 Friesen, M.A & Hughes, R.G. & Zorn, M., Communication: patient safety and the nursing work environment, Nebraska Nurse, 40:11-12 2007.
41 Gallant-Roman, M. A., Strategies and Tools to Reduce Workplace Violence, AAOHN Journal , 56: 2008.
42 Grenny, J., Crucial conversations: the most potent force for eliminating disruptive behaviour, Critical care nursing quarterly, 32:58-61 2009.
43 Griffin, M., Teaching cognitive rehearsal as a shield for lateral violence: an intervention for newly licensed nurses, Journal of Continuing Education in Nursing, 35:257-263 2004.
44 Hegney, D. & Eley, R. & Plank, A. & Buikstra, E. & Parker, V., Workforce issues in nursing in Queensland: 2001 and 2004, Journal of Clinical Nursing, 15:1521-1530 2006.
45 Hendel, T. & Fish, M. & Galon, V., Leadership style and choices of strategy in conflict management among Israeli nurse managers in general hospitals, Journal of Nursing Management, 13:137-146 2005.
46 Hutchinson, M. & Jackson, D. & Wilkes, L. & Vickers. M.H, A new model of bullying in the nursing workplace, Advances in Nursing Science, 31:E60-E71 2008.
47 Hutchinson, M. & Vickers, M.H. & Jackson, D. & Wilkes, L., "I'm gonna do what I wanna do."Organisational change as a legitimized vehicle for bullies, Health Care Management Review, 30:331-336 2005.
48 Hutchinson, M. & Vickers, M.H. & Jackson, D. & Wilkes, L., 'They stand you in a corner, you are not to speak: nurses tell of abusive indoctrination in work teams dominated by bullies, Contemporary Nurse, 21:228-238 2006.
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 638
49 Jackson, D.,& Firtko, A. et al. , Personal resilience as a strategy for surviving and thriving in the face of workplace adversity: a literature review., Journal of Advanced Nursing , 60:1-9 2007.
50 Johnson, S.L., International perspectives on workplace bullying among nurses: a review, International ursing Review, 56:34-40 2009.
51 Judkins, S. & Reid, B. et al. , Hardiness training among nurse managers: building a healthy workplace., Journal of continuing education in nursing , 37:202 2006.
52 Kelloway, E.K. & Day, A. L, Building healthy workplaces: What we know so far, Canadian Journal of Behavioural Science, 37:223-235 2005.
53 Leiper, J., Nurse against nurse: how to stop horizontal violence, Nursing, 35:44-45 2005.
54 Lewis, M.A., Nurse bullying: organizational considerations in the maintenance and perpetration of health care bullying cultures, Journal of Nursing Management, 14:52-58 2006.
55 Lewis, T., What must we do about lateral violence?, New Mexico Nurse, 53:4 2008. ]
56 Liefooghe, A. P.D. & Olafsson, R., "Scientists" and "amateurs": mapping the bullying domain, International Journal of Manpower, 20:39-49 1999.
57 Lim, S. & Cortina, L. M & Magley, V.J., Personal and workgroup incivility: Impact on work and health outcomes, Journal of Applied Psychology, 93:95-107 2008.
58 Martin, W. F., Is your hospital safe? Disruptive behaviour and workplace bullying, Hospital Topics, 86:21-28 2008.
59 McGillis Hall, L. & Doran, D. & Pink, L., Outcomes of Interventions to improve hospital nursing work environments, JONA, 38:40-46 2008.
60 McLemore, M., Workplace aggression: beginning a dialogue, Clinical Journal of Oncology Nursing, 10:455-456 2006.
61 Olsen, B. J., D. L. Neslon, et al., Managing aggression in organizations: what leaders must know, Leadership and Organization Development Journal , 27:384-398 2006.
62 Pearson, C. M. and C. L. Porath, On the nature, consequences and remedies of workplace incivility: No time for, The Academy of Management Executive, 19:7-18 2005.
63 Pearson, C. M., & Andersson, L.M. et al. , Assessing and attacking workplace incivility., Organizational Dynamics , 29:123-137 2000.
64 Poilpot-Rocaboy, G. & Winter, R., Combating psychological harassment in the workplace: processes for management interventions, International Employment Relations Review, 13:67-83 2007.
65 Porto, G. and R. Lauve, Disruptive clinician behaviour: A persistent threat to patient safety., Patient Safety and Quality Healthcare. , 29:123-137 2006.
66 Quine, L., Workplace bullying in nurses, Journal of Health Psychology, 6:73-84 2001.
67 Ramos, M.C., Eliminate destructive behaviours through example and evidence, Nursing Management, 37:34-41 2006.
68 Randle, J. & Stevenson, K. et al, Reducing workplace bullying in healthcare organisations, Nursing Standard, 21:49-56 2007.
69 Rayner, C., From research to implementation: finding leverage for prevention, International Journal of Manpower, 20:28-38 1999.
70 Rocker, C.F., Addressing nurse-to-nurse bullying to promote nurse retention, Online Journal of Issues in Nursing, 13:1-11 2008.
71 Rosenstein, Alan H., Nurse-Physician relationships: Impact on nurse satisfaction and retention, AJN, 102:26-34 2002.
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 639
72 Rutherford, A, & Rissel, C., A survey of workplace bullying in a health sector organisation, Australian Health Review, 28:65-72 2004.
73 Salin, D. , Organisational responses to workplace harassment., Personnel Review , 38:26-44 2009.
74 Sheehan, Michael, Workplace bullying: responding with some emotional intelligence, International Journal of Manpower, 20:57-69 1999.
75 Sheehan, Michael & Barker, M. & Rayner, C., Applying strategies for dealing with workplace bullying, International Journal of Manpower, 20:50-57 1999.
76 Shuttleworth, A., Managing workplace stress: how training can help, Industrial and Commercial Training, 36:61-65 2004.
77 Simpson, K. R., Disruptive Clinician Behaviour, MCN: The American Journal of Maternal Child Nursing , 32:64 2007.
78 Sotile, W.M. & Sotile, M. O., How to shape positive relationships in medical practices and hospitals, Physician Executive, 25:51-55 1999.
79 Stevens, S. , From the field. Nursing workforce retention: challenging a bullying culture: how nurses in one Australian hospital confronted intimidation of and by nurses and took steps to remedy it., Health Affairs , 21:189-193 2002.
80 Taylor, B. , Identifying and transforming dysfunctional nurse-nurse relationships through reflective practice and action research., International journal of nursing practice , 7:406-413 2001.
81 Thomas, S. P., Anger: The mismanaged emotion, MEDSURG Nursing, 12:103-110 2003.
82 Townend, A, Understanding and addressing bullying in the workplace, Industrial and Commercial Training, 40:270-273 2008.
83 Van Fleet, D.D. & Griffin, R.W., Dysfunctional organization culture: The role of leadership in motivating dysfunctional work behaviours, Journal of Managerial Psychology, 21:698-708 2006.
84 Weiss, Barbara, Balancing act. Making it work with difficult people, RN, 68:65-68 2005.
85 Williams, R., Capturing the moment, Nursing Management, 14:10-12 2007.
86 Woelfle, C.Y. & McCaffrey, R., Nurse on Nurse, Nursing Forum, 42:123-131 2007.
87 Zwarenstein, M. B. W., Interventions to promote collaboration between nurses and doctors, Cochrane Database Systematic Reviews, :1-13 2000.
Appendix III: Studies selected for retrieval
1 Bennet, Margaret, Priorities for Nursing and Midwifery Research, Nursing & Nursing Education
Taskforce, : 2006.
2 Brown, R.B. & Brooks, I., Emotion at work: Identifying the emotional climate of night nursing, Journal of Management in Medicine, 16:327-344 2002.
3 Cortina, L.M. & Magley, V.J. & Hunter Williams, J. & Day Langhout, R., Incivility in the workplace: incidence and impact, Journal of Occupational Health Psychology, 6:64-80 2001.
4 Felblinger, D. M., Incivility and bullying in the workplace and nurses' shame responses, JOGNN, 37:234-242 2008.
5 Fellowes, D. & Wilkinson, S. & Moore, P., Communication skills training for health care professionals working with cancer patients, their families and/or carers, The Cochrane Database of Systematic Reviews 2007-1, : 2003.
6 Fineman, S. (ed), Emotions in Organisations, Sage Publications, London, : 1993.
7 Hutchinson, M. & Vickers, M. & Jackson, D. & Wilkes, L., Workplace bullying in nursing: towards a more critical organisational perspective, Nursing Inquiry, 13:118-126 2006.
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 640
8 Hutton, S.A., Workplace incivility, JONA: The Journal of Nursing Administration, 36:22-28 2006.
9 Joint Commission on Accreditation of Healthcare Organisations, Proposed Standard for Disruptive Behaviour-Hospital, http://www.jointcommission.org/NR/rdonlyres/@BF44E9F-6EE0-4856-83EF-778FA47723B/0/Disruptive_Behavior_cah_stds.pdf, : 2007.
10 MacIntosh, J., Tackling work place bullying, Issues in Mental Health Nursing, 27:665-679 2006.
11 McGee, D. & Shigemitsu, H. & Henig, N. & Raffin, T., Conflict over communication and unprofessional staff behaviour: A source of dissatisfaction during the withdrawal of care?, Critical Care Medicine, 28:217-219 2001.
12 McIIduff, E. & Coghlan, D., Understanding and contending with passive-aggressive behaviour in teams and organizations, Journal of Managerial Psychology, 15:716-736 2000.
13 Office of Public Service Merit and Equity (State of Queensland), Quality public service workplaces information paper 8, Organisation Health, : 2006.
14 Office of the Public Service, A focus on people: A workforce management strategy for the Queensland public sector, Brisbane, Queensland, : 1997.
15 Pearson A, Balancing the evidence: incorporating the synthesis of qualitative data into systematic reviews, JBI Reports, :45-64 2004.
16 Pearson, C.M. & Andersson, L.M. & Wegner, J., When workers flout convention: A study of workplace incivility, Human Relations, 54:1387-1419 2001.
17 Queensland Health, Workplace culture and leadership,
http://qheps.health.qld.gov.au/betterworkplaces/culture/home.htm, : 2007.
18 Queensland Health, Queensland Health Systems Review. Final Report, http://qheps.health.qld.gov.au/health_sys_review/final/qhsr_final_report.pdf, : 2005.
19 Rayner, C. & Hoel, H. & Cooper, C.L., Workplace Bullying. What we know, who is to blame, and what we do?, , : 2002.
20 Rime, B. & Mesquite, B. & Philpott, P. & Boca, S., Beyond the emotional event: six studies on the social sharing of emotion, Journal of Cognition and Emotion, 5:435-65 1991.
21 Roberts, S.J. & Demarco, R. & Griffin, M., The effect of group behaviours on the culture of the nursing workplace: a review of the evidence and interventions for change, Journal of Nursing Management, 0:1-6 2008.
22 Rosenstein, A. H. & O'Daniel, M., Disruptive Behaviour & Clinical Outcomes: Perceptions of Nurses & Physicians: Nurses, physicians, and administrators say that clinicians' disruptive behaviour has negative effects on clinical outcomes., Nursing Management , 36:18 2005.
23 Simons, S.R., Workplace bullying experienced by nurses newly licensed in Massachusetts, Dissertation Abstracts International: Section B: The Science and Engineering, 67:3065 2006.
24 Antecol, H. & Cobb-Clark, D., Does sexual harassment training change attitudes? A view from the Federal level, Social Science Quarterly, 84:826-842 2003.
25 Ball, J. & Pike, G., At breaking point? A survey of the wellbeing and working lives of nurses in 2005, PTRC, University of Leeds, 0:0 2006.
26 Barnsteiner, J.H. & Madigan, C., Instituting a disruptive conduct policy for medical staff,AACN Clinical Issues, 12:378-382 2001.
27 Beech, B., Beating the bullies, Emergency Nurse, 12:35 2004.
28 Befar, K.J & Peterson, R.S. & Mannix, E.A. & Trochim, M.K., The critical role of
conflict resolution in teams: a close look at the links between conflict type, conflict management strategies, and team outcomes, Journal of Applied Psychology , 93:170-188 2008.
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 641
29 Beyea, Suzanne C., Intimidation in health care settings and patient safety, AORN Journal 80:115-117 2004.
30 Boone, B. N. & King, M. L. et al. , Conflict management training and nurse-physician collaborative behaviours., Journal for Nurses in Staff Development : JNSD: Official journal of the National Nursing Staff Development Organization , 24:168-175 2008.
31 Brennan, W., I'm talking to you! Managing bullying and harassment in the workplace, Emergency nurse : the journal of the RCN Accident and Emergency Nursing Association, 7:16-20 1999.
32 Broome, B. A., Dealing with sharks and bullies in the workplace, ABNF Journal, 19:28-30 2008.
33 Cassirer, C.D. & Anderson, D. & Hanson, S., Abusive behaviour in the healthcare workplace, Creative Nursing, 8:8-9 2002.
34 Corr, Margaret, Reducing occupational stress in intensive care, Nursing in Critical Care, 5:76-81 2000.
35 Crawford, N., Conundrums and confusion in organisations: the etymology of the word 'bully', International Journal of Manpower, 20:86-93 1999.
36 Daisiki, I., Changing nurses' dis-empowering relationship patterns, Journal of Advanced Nursing, 48:43-50 2004.
37 DeChurch, L. A., K. L. Hamilton, et al. , Effects of conflict management strategies on perceptions of intra-group conflict., Group Dynamics: Theory, Research and Practice,11:66-78 2007.
38 Deans, C. , Nurses and occupational violence: the role of organisational support in moderating professional competence., Australian Journal of Advanced Nursing , 22:14-18 2004.
39 Everton, W.J. & Jolton, J. A. & Mastrangelo, P.M., Be nice and fair or else: understanding reasons for employees' deviant behaviours, Journal of Management Development, 26:117-131 2007.
40 Friesen, M.A & Hughes, R.G. & Zorn, M., Communication: patient safety and the nursing work environment, Nebraska Nurse, 40:11-12 2007.
41 Gallant-Roman, M. A. , Strategies and Tools to Reduce Workplace Violence., AAOHN Journal , 56: 2008.
42 Grenny, J., Crucial conversations: the most potent force for eliminating disruptive behaviour, Critical care nursing quarterly, 32:58-61 2009.
43 Griffin, M., Teaching cognitive rehearsal as a shield for lateral violence: an intervention for newly licensed nurses, Journal of Continuing Education in Nursing, 35:257-263 2004.
44 Hegney, D. & Eley, R. & Plank, A. & Buikstra, E. & Parker, V., Workforce issues in nursing in Queensland: 2001 and 2004, Journal of Clinical Nursing, 15:1521-1530 2006.
45 Hendel, T. & Fish, M. & Galon, V., Leadership style and choices of strategy in conflict management among Israeli nurse managers in general hospitals, Journal of Nursing Management, 13:137-146 2005.
46 Hutchinson, M. & Jackson, D. & Wilkes, L. & Vickers. M.H, A new model of bullying in the nursing workplace, Advances in Nursing Science, 31:E60-E71 2008.
47 Hutchinson, M. & Vickers, M.H. & Jackson, D. & Wilkes, L., "I'm gonna do what I wanna do. "Organisational change as a legitimized vehicle for bullies, Health Care Management Review, 30:331-336 2005.
48 Hutchinson, M. & Vickers, M.H. & Jackson, D. & Wilkes, L., 'They stand you in a corner, you are not to speak: nurses tell of abusive indoctrination in work teams dominated by bullies, Contemporary Nurse, 21:228-238 2006.
49 Jackson, D.,& Firtko, A. et al. , Personal resilience as a strategy for surviving and thriving in the face of workplace adversity: a literature review., Journal of Advanced Nursing , 60:1-9 2007.
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 642
50 Johnson, S.L., International perspectives on workplace bullying among nurses: a review, International ursing Review, 56:34-40 2009.
51 Judkins, S.& Reid, B. et al. , Hardiness training among nurse managers: building a healthy workplace., Journal of continuing education in nursing , 37:202 2006.
52 Kelloway, E.K. & Day, A. L, Building healthy workplaces: What we know so far, Canadian Journal of Behavioural Science, 37:223-235 2005.
53 Leiper, J., Nurse against nurse: how to stop horizontal violence, Nursing , 35:44-45 2005.
54 Lewis, M.A., Nurse bullying: organizational considerations in the maintenance and perpetration of health care bullying cultures, Journal of Nursing Management, 14:52-58 2006.
55 Lewis, T., What must we do about lateral violence?, New Mexico Nurse, 53:4 2008.
56 Liefooghe, A. P.D. & Olafsson, R., "Scientists" and "amateurs": mapping the bullying domain, International Journal of Manpower, 20:39-49 1999.
57 Lim, S. & Cortina, L. M & Magley, V.J., Personal and workgroup incivility: Impact on work and health outcomes, Journal of Applied Psychology, 93:95-107 2008.
58 Martin, W. F., Is your hospital safe? Disruptive behaviour and workplace bullying, Hospital Topics, 86:21-28 2008.
59 McGillis Hall, L. & Doran, D. & Pink, L., Outcomes of Interventions to improve hospital nursing work environments, JONA, 38:40-46 2008.
60 McLemore, M., Workplace aggression: beginning a dialogue, Clinical Journal of Oncology Nursing, 10:455-456 2006.
61 Olsen, B. J., D. L. Neslon, et al. , Managing aggression in organizations: what leaders must know., Leadership and Organization Development Journal , 27:384-398 2006.
62 Pearson, C. M. and C. L. Porath , On the nature, consequences and remedies of workplace incivility: No time for, The Academy of Management Executive, 19:7-18 2005.
63 Pearson, C. M., & Andersson, L.M. et al. , Assessing and attacking workplace incivility., Organizational Dynamics , 29:123-137 2000.
64 Poilpot-Rocaboy, G. & Winter, R., Combating psychological harassment in the workplace: processes for management interventions, International Employment Relations Review, 13:67-83 2007.
65 Porto, G. and R. Lauve , Disruptive clinician behaviour: A persistent threat to patient safety., Patient Safety and Quality Healthcare. , 29:123-137 2006.
66 Quine, L., Workplace bullying in nurses, Journal of Health Psychology, 6:73-84 2001.
67 Ramos, M.C., Eliminate destructive behaviours through example and evidence, Nursing Management, 37:34-41 2006.
68 Randle, J. & Stevenson, K. et al, Reducing workplace bullying in healthcare organisations, Nursing Standard, 21:49-56 2007.
69 Rayner, C. , From research to implementation: finding leverage for prevention., International Journal of Manpower , 20:28-38 1999.
70 Rocker, C.F., Addressing nurse-to-nurse bullying to promote nurse retention, Online Journal of Issues in Nursing, 13:1-11 2008.
71 Rosenstein, Alan H., Nurse-Physician relationships: Impact on nurse satisfaction and retention, AJN, 102:26-34 2002.
72 Rutherford, A, & Rissel, C., A survey of workplace bullying in a health sector organisation, Australian Health Review, 28:65-72 2004.
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 643
73 Salin, D. , Organisational responses to workplace harassment., Personnel Review , 38:26-44 2009.
74 Sheehan, Michael, Workplace bullying: responding with some emotional intelligence, International Journal of Manpower, 20:57-69 1999.
75 Sheehan, Michael & Barker, M. & Rayner, C., Applying strategies for dealing with workplace bullying, International Journal of Manpower, 20:50-57 1999.
76 Shuttleworth, A., Managing workplace stress: how training can help, Industrial and Commercial Training, 36:61-65 2004.
77 Simpson, K. R. , Disruptive Clinician Behaviour., MCN: The American Journal of Maternal Child Nursing , 32:64 2007.
78 Sotile, W.M. & Sotile, M. O., How to shape positive relationships in medical practices and hospitals, Physician Executive, 25:51-55 1999.
79 Stevens, S., From the field. Nursing workforce retention: challenging a bullying culture: how nurses in one Australian hospital confronted intimidation of and by nurses and took steps to remedy it., Health Affairs , 21:189-193 2002.
80 Taylor, B. , Identifying and transforming dysfunctional nurse-nurse relationships through reflective practice and action research., International journal of nursing practice , 7:406-413 2001.
81 Thomas, S. P., Anger: The mismanaged emotion, MEDSURG Nursing, 12:103-110 2003.
82 Townend, A, Understanding and addressing bullying in the workplace, Industrial and Commercial Training, 40:270-273 2008.
83 Van Fleet, D.D. & Griffin, R.W., Dysfunctional organization culture: The role of leadership in motivating dysfunctional work behaviours, Journal of Managerial Psychology, 21:698-708 2006.
84 Weiss, Barbara, Balancing act. Making it work with difficult people, RN, 68:65-68 2005.
85 Williams, R., Capturing the moment, Nursing Management, 14:10-12 2007.
86 Woelfle, C.Y. & McCaffrey, R., Nurse on Nurse, Nursing Forum, 42:123-131 2007.
87 Zwarenstein, M. B. W., Interventions to promote collaboration between nurses and doctors , Cochrane Database Systematic Reviews, :1-13 2000.
Appendix IV: Critical Appraisal instruments
QARI Appraisal instrument
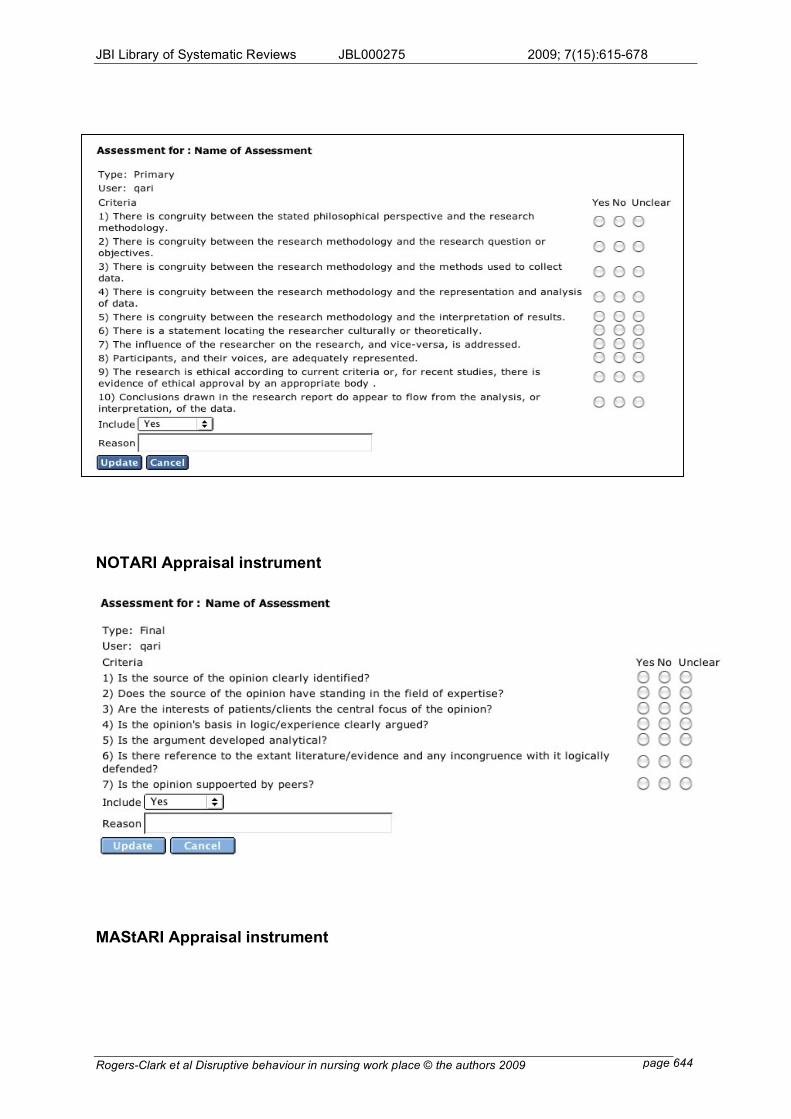
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 644
NOTARI Appraisal instrument
MAStARI Appraisal instrument
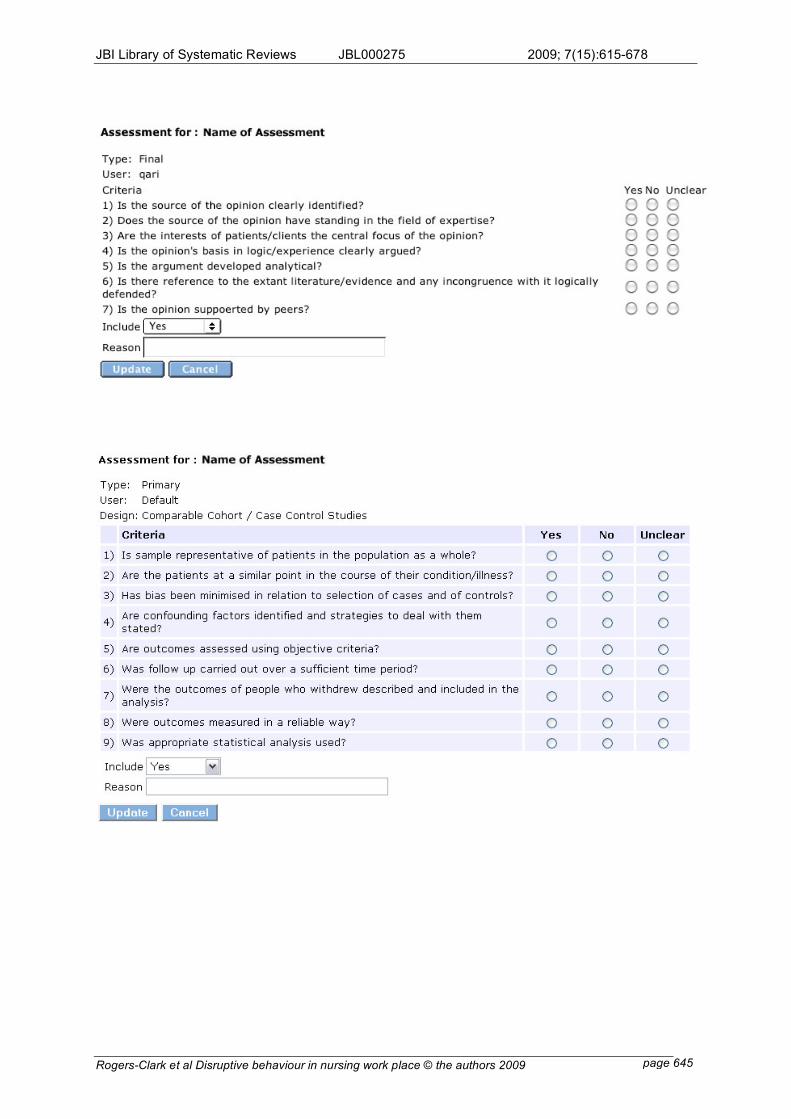
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 645
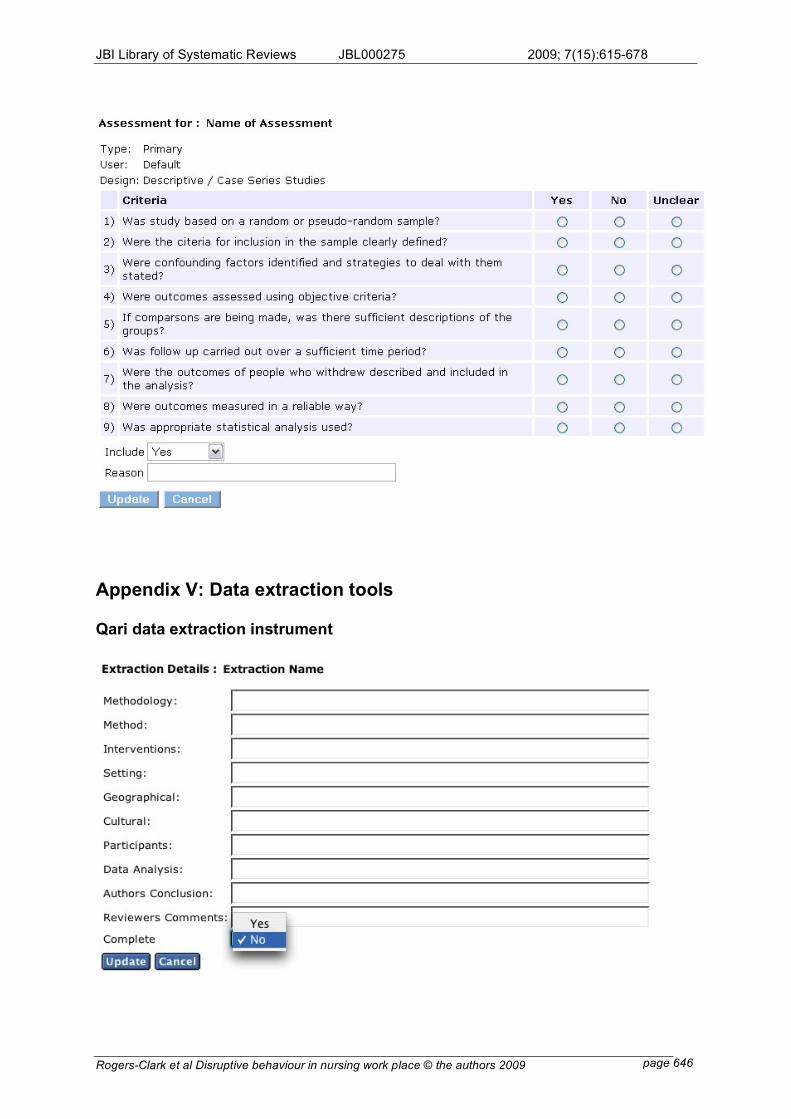
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 646
Appendix V: Data extraction tools
Qari data extraction instrument
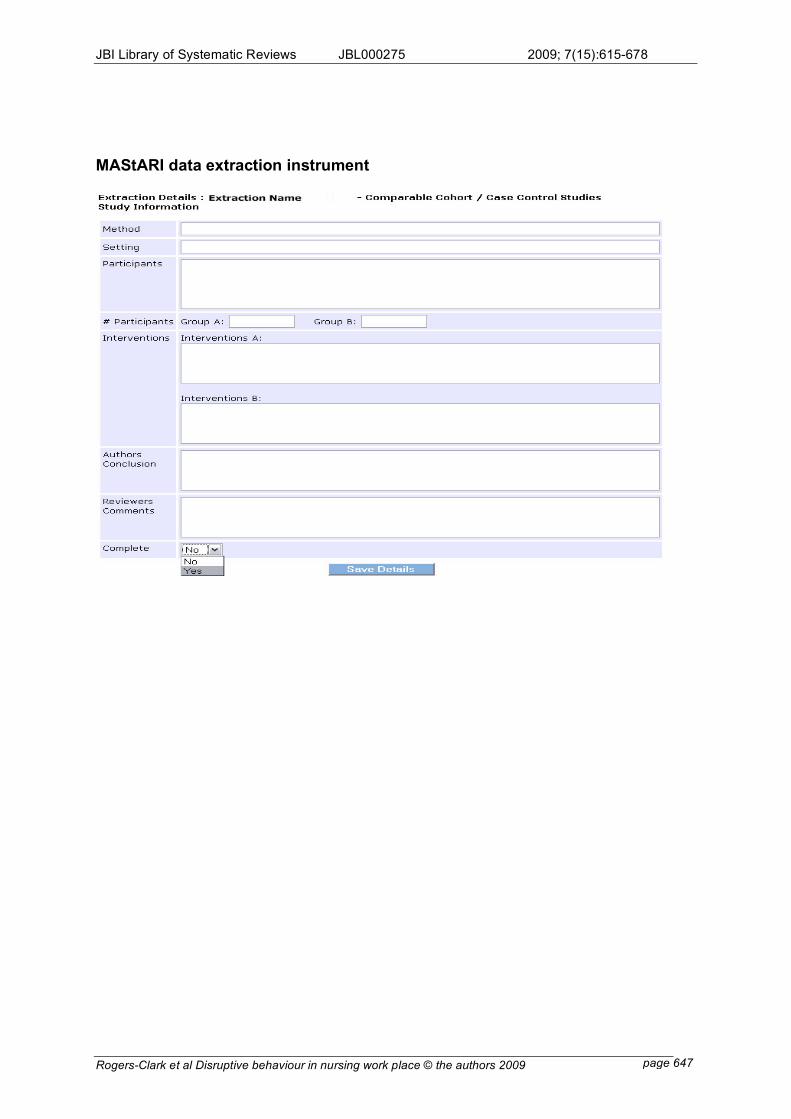
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 647
MAStARI data extraction instrument
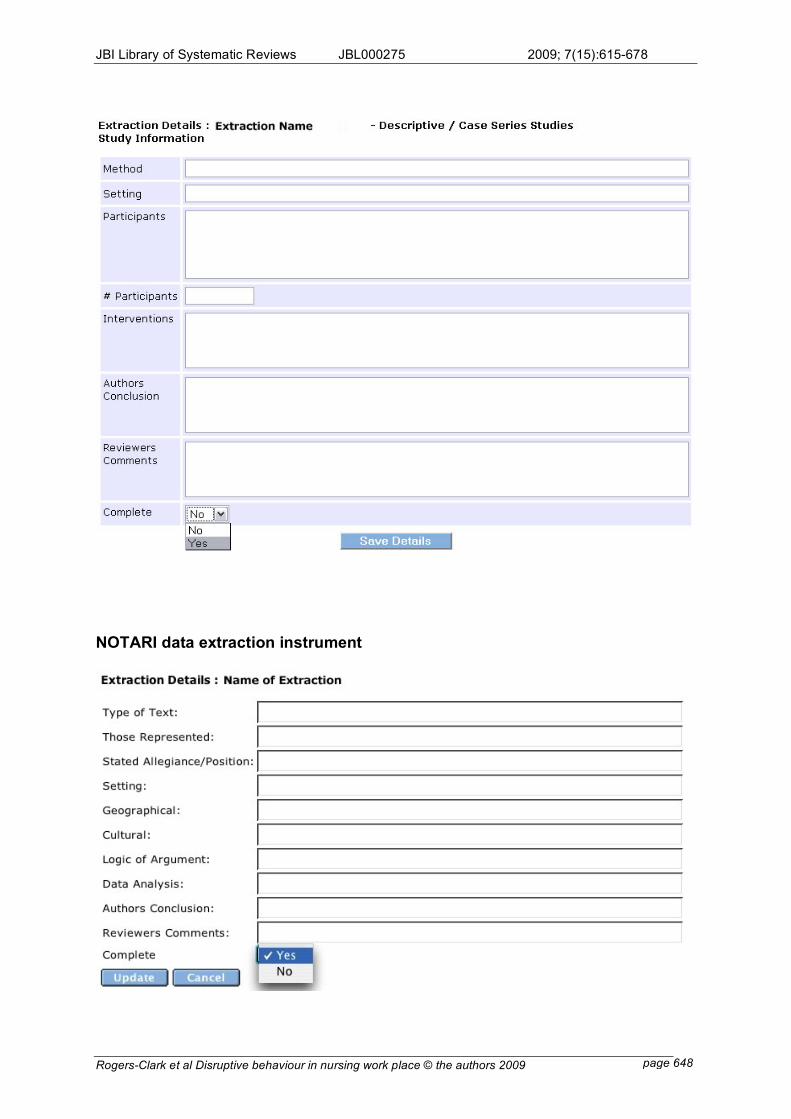
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 648
NOTARI data extraction instrument
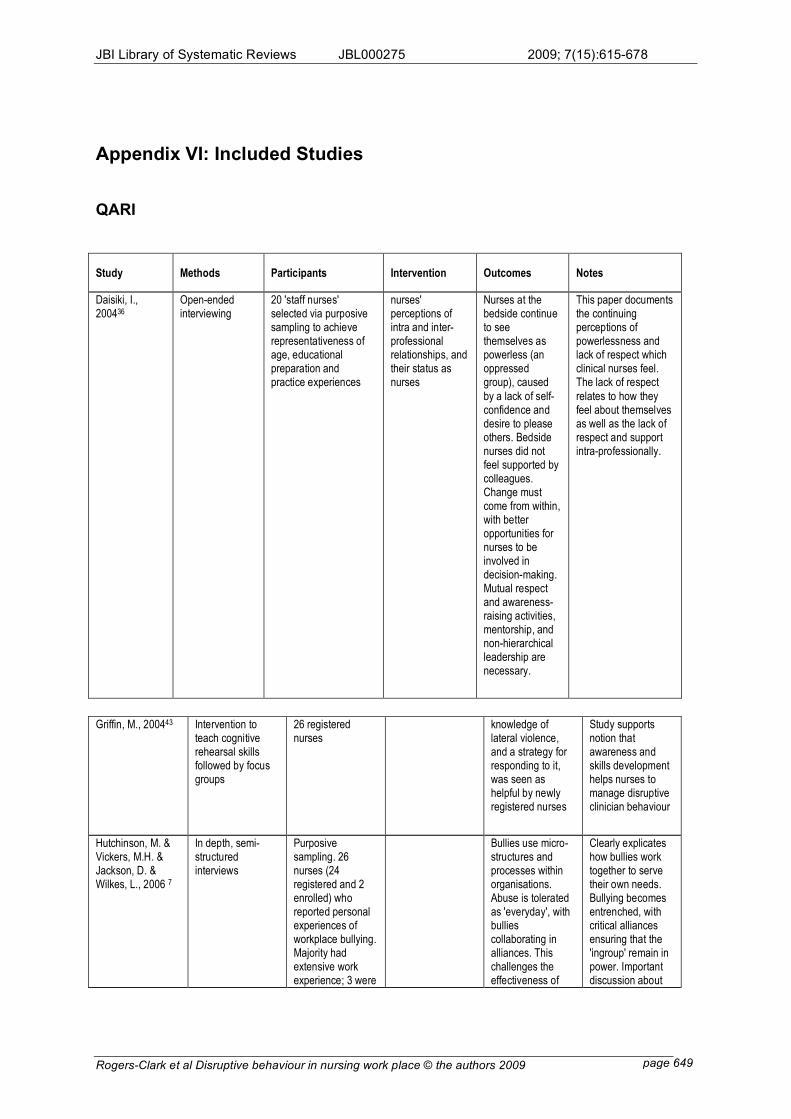
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
!
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 649
Appendix VI: Included Studies
QARI
Study Methods Participants Intervention Outcomes Notes
Daisiki, I., 200436
Open-ended interviewing
20 'staff nurses' selected via purposive sampling to achieve representativeness of age, educational preparation and practice experiences
nurses' perceptions of intra and inter-professional relationships, and their status as nurses
Nurses at the bedside continue to see themselves as powerless (an oppressed group), caused
by a lack of self-confidence and desire to please others. Bedside nurses did not feel supported by colleagues. Change must come from within, with better opportunities for nurses to be involved in decision-making. Mutual respect and awareness-raising activities, mentorship, and non-hierarchical leadership are necessary.
This paper documents the continuing perceptions of powerlessness and lack of respect which clinical nurses feel. The lack of respect
relates to how they feel about themselves as well as the lack of respect and support intra-professionally.
Griffin, M., 200443 Intervention to
teach cognitive rehearsal skills followed by focus groups
26 registered nurses
knowledge of lateral violence, and a strategy for responding to it, was seen as helpful by newly registered nurses
Study supports notion that awareness and skills development helps nurses to manage disruptive clinician behaviour
Hutchinson, M. & Vickers, M.H. & Jackson, D. & Wilkes, L., 2006 7
In depth, semi-structured interviews
Purposive sampling. 26 nurses (24 registered and 2 enrolled) who reported personal experiences of workplace bullying. Majority had extensive work experience; 3 were
Bullies use micro-structures and processes within organisations. Abuse is tolerated as 'everyday', with bullies collaborating in alliances. This challenges the effectiveness of
Clearly explicates how bullies work together to serve their own needs. Bullying becomes entrenched, with critical alliances ensuring that the 'ingroup' remain in power. Important discussion about
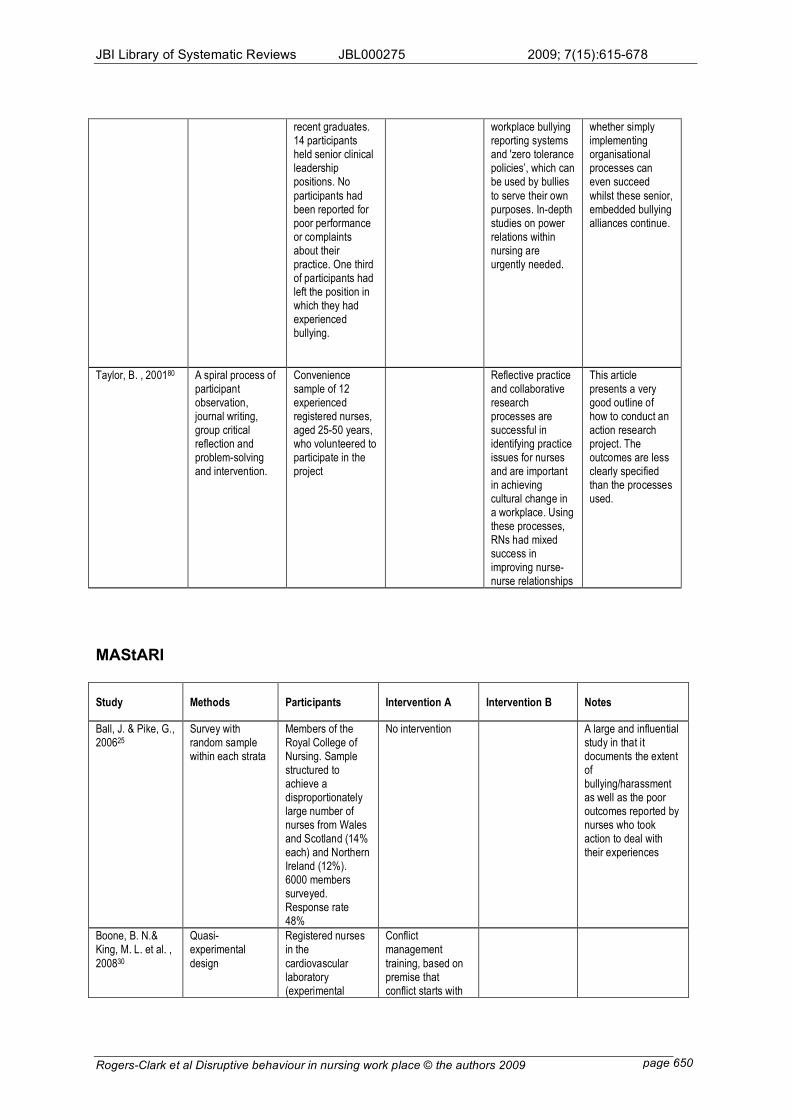
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
!
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 650
recent graduates. 14 participants held senior clinical leadership positions. No
participants had been reported for poor performance or complaints about their practice. One third of participants had left the position in which they had experienced bullying.
workplace bullying reporting systems and 'zero tolerance policies’, which can be used by bullies
to serve their own purposes. In-depth studies on power relations within nursing are urgently needed.
whether simply implementing organisational processes can even succeed
whilst these senior, embedded bullying alliances continue.
Taylor, B. , 200180 A spiral process of participant observation, journal writing, group critical reflection and problem-solving and intervention.
Convenience sample of 12 experienced registered nurses, aged 25-50 years, who volunteered to participate in the project
Reflective practice and collaborative research processes are successful in identifying practice issues for nurses and are important in achieving cultural change in a workplace. Using these processes, RNs had mixed success in improving nurse-nurse relationships
This article presents a very good outline of how to conduct an action research project. The outcomes are less clearly specified than the processes used.
MAStARI
Study Methods Participants Intervention A Intervention B Notes
Ball, J. & Pike, G., 200625
Survey with random sample within each strata
Members of the Royal College of Nursing. Sample structured to achieve a disproportionately large number of nurses from Wales and Scotland (14% each) and Northern Ireland (12%). 6000 members surveyed. Response rate 48%
No intervention A large and influential study in that it documents the extent of bullying/harassment as well as the poor outcomes reported by nurses who took action to deal with their experiences
Boone, B. N.& King, M. L. et al. ,
200830
Quasi-experimental
design
Registered nurses in the
cardiovascular laboratory (experimental
Conflict management
training, based on premise that conflict starts with
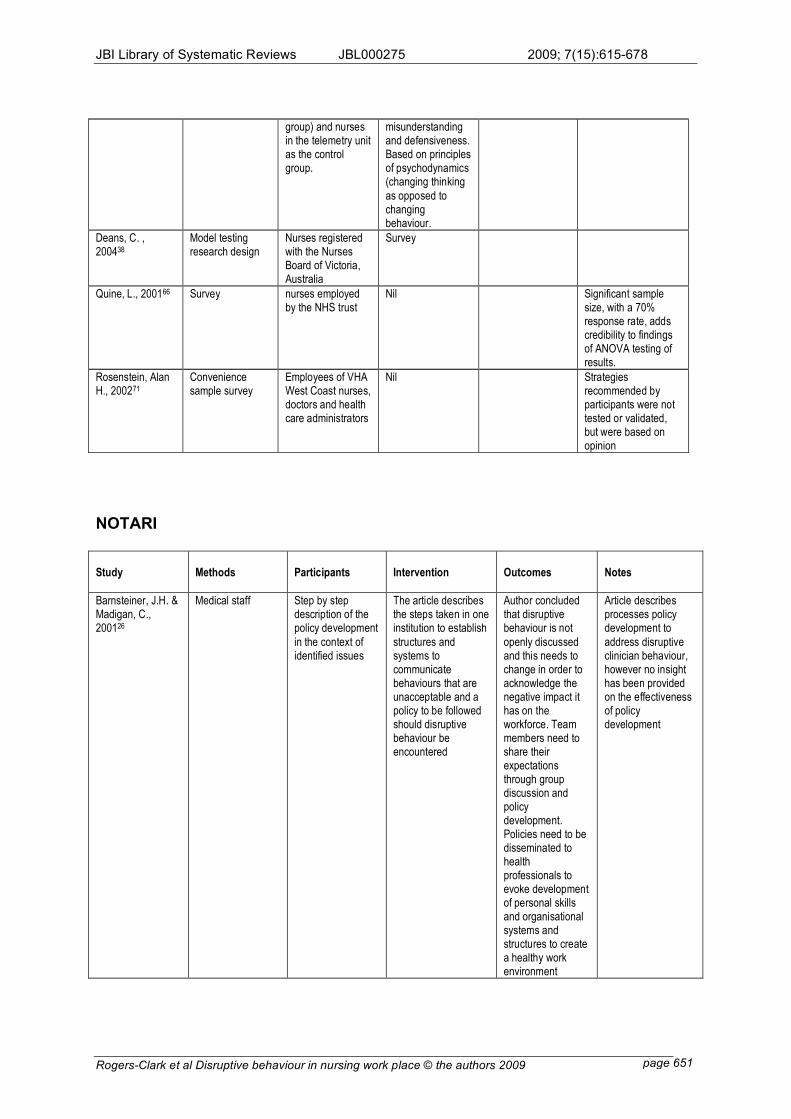
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
!
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 651
group) and nurses in the telemetry unit as the control group.
misunderstanding and defensiveness. Based on principles of psychodynamics (changing thinking
as opposed to changing behaviour.
Deans, C. , 200438
Model testing research design
Nurses registered with the Nurses Board of Victoria, Australia
Survey
Quine, L., 200166 Survey nurses employed by the NHS trust
Nil Significant sample size, with a 70% response rate, adds credibility to findings of ANOVA testing of results.
Rosenstein, Alan H., 200271
Convenience sample survey
Employees of VHA West Coast nurses, doctors and health care administrators
Nil Strategies recommended by participants were not tested or validated, but were based on opinion
NOTARI
Study Methods Participants Intervention Outcomes Notes
Barnsteiner, J.H. & Madigan, C., 200126
Medical staff Step by step description of the policy development
in the context of identified issues
The article describes the steps taken in one institution to establish
structures and systems to communicate behaviours that are unacceptable and a policy to be followed should disruptive behaviour be encountered
Author concluded that disruptive behaviour is not
openly discussed and this needs to change in order to acknowledge the negative impact it has on the workforce. Team members need to share their expectations through group discussion and policy development. Policies need to be disseminated to health professionals to evoke development of personal skills and organisational systems and structures to create a healthy work environment
Article describes processes policy development to
address disruptive clinician behaviour, however no insight has been provided on the effectiveness of policy development
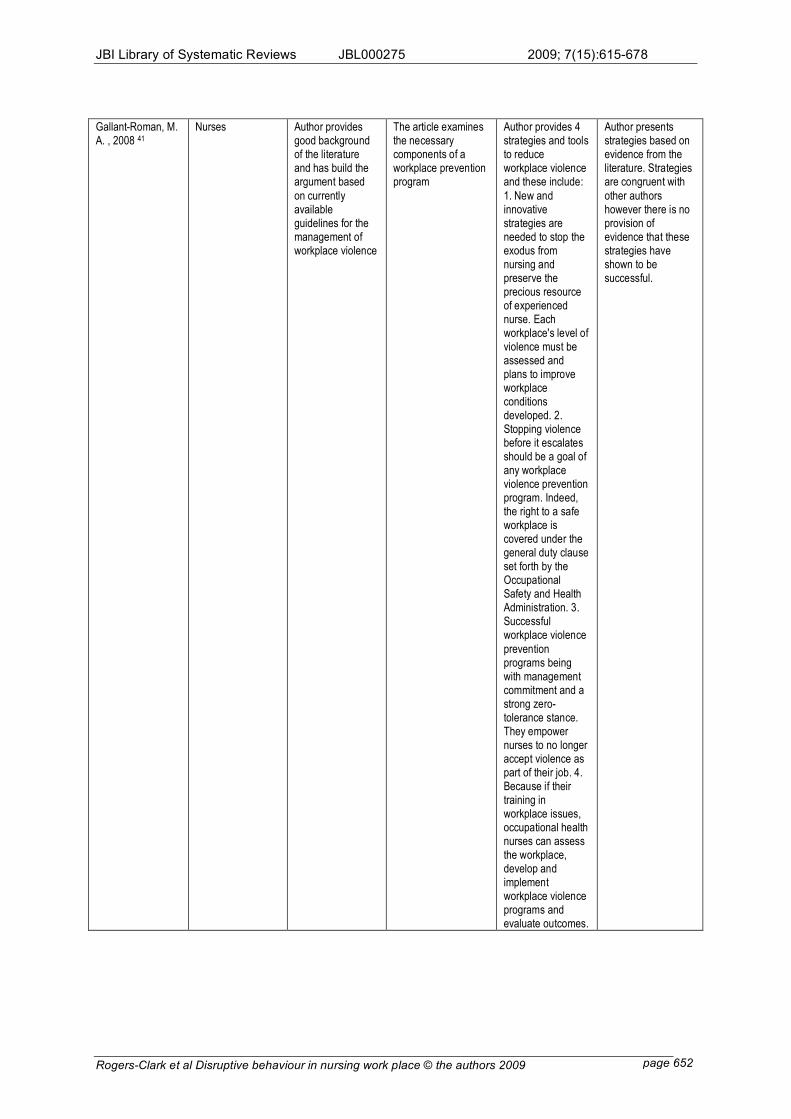
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
!
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 652
Gallant-Roman, M. A. , 2008 41
Nurses Author provides good background of the literature and has build the argument based
on currently available guidelines for the management of workplace violence
The article examines the necessary components of a workplace prevention program
Author provides 4 strategies and tools to reduce workplace violence and these include:
1. New and innovative strategies are needed to stop the exodus from nursing and preserve the precious resource of experienced nurse. Each workplace's level of violence must be assessed and plans to improve workplace conditions developed. 2. Stopping violence before it escalates should be a goal of any workplace violence prevention program. Indeed, the right to a safe workplace is covered under the general duty clause set forth by the Occupational Safety and Health Administration. 3. Successful workplace violence
prevention programs being with management commitment and a strong zero-tolerance stance. They empower nurses to no longer accept violence as part of their job. 4. Because if their training in workplace issues, occupational health nurses can assess the workplace, develop and implement workplace violence programs and evaluate outcomes.
Author presents strategies based on evidence from the literature. Strategies are congruent with
other authors however there is no provision of evidence that these strategies have shown to be successful.
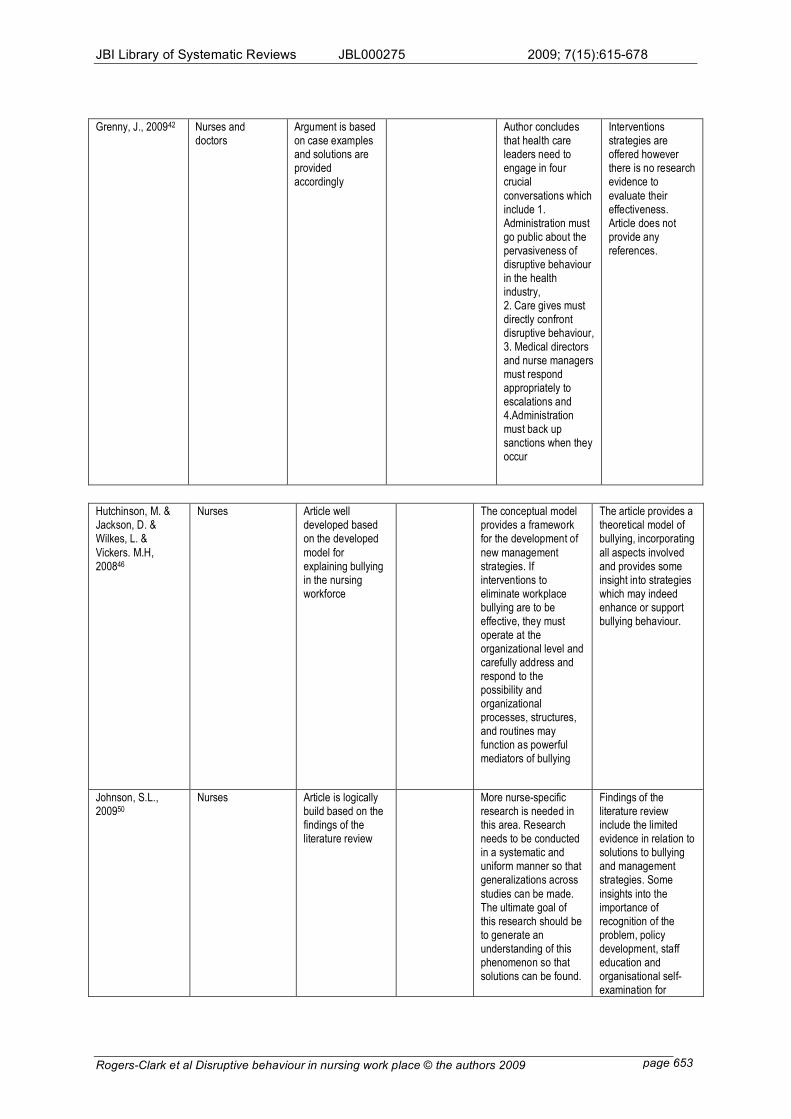
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
!
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 653
Grenny, J., 200942 Nurses and doctors
Argument is based on case examples and solutions are provided accordingly
Author concludes that health care leaders need to engage in four crucial
conversations which include 1. Administration must go public about the pervasiveness of disruptive behaviour in the health industry, 2. Care gives must directly confront disruptive behaviour, 3. Medical directors and nurse managers must respond appropriately to escalations and 4.Administration must back up sanctions when they occur
Interventions strategies are offered however there is no research evidence to
evaluate their effectiveness. Article does not provide any references.
Hutchinson, M. & Jackson, D. & Wilkes, L. &
Vickers. M.H, 200846
Nurses Article well developed based on the developed
model for explaining bullying in the nursing workforce
The conceptual model provides a framework for the development of
new management strategies. If interventions to eliminate workplace bullying are to be effective, they must operate at the organizational level and carefully address and respond to the possibility and organizational processes, structures, and routines may function as powerful mediators of bullying
The article provides a theoretical model of bullying, incorporating
all aspects involved and provides some insight into strategies which may indeed enhance or support bullying behaviour.
Johnson, S.L., 200950
Nurses Article is logically build based on the findings of the literature review
More nurse-specific research is needed in this area. Research needs to be conducted in a systematic and uniform manner so that generalizations across
studies can be made. The ultimate goal of this research should be to generate an understanding of this phenomenon so that solutions can be found.
Findings of the literature review include the limited evidence in relation to solutions to bullying and management strategies. Some
insights into the importance of recognition of the problem, policy development, staff education and organisational self-examination for
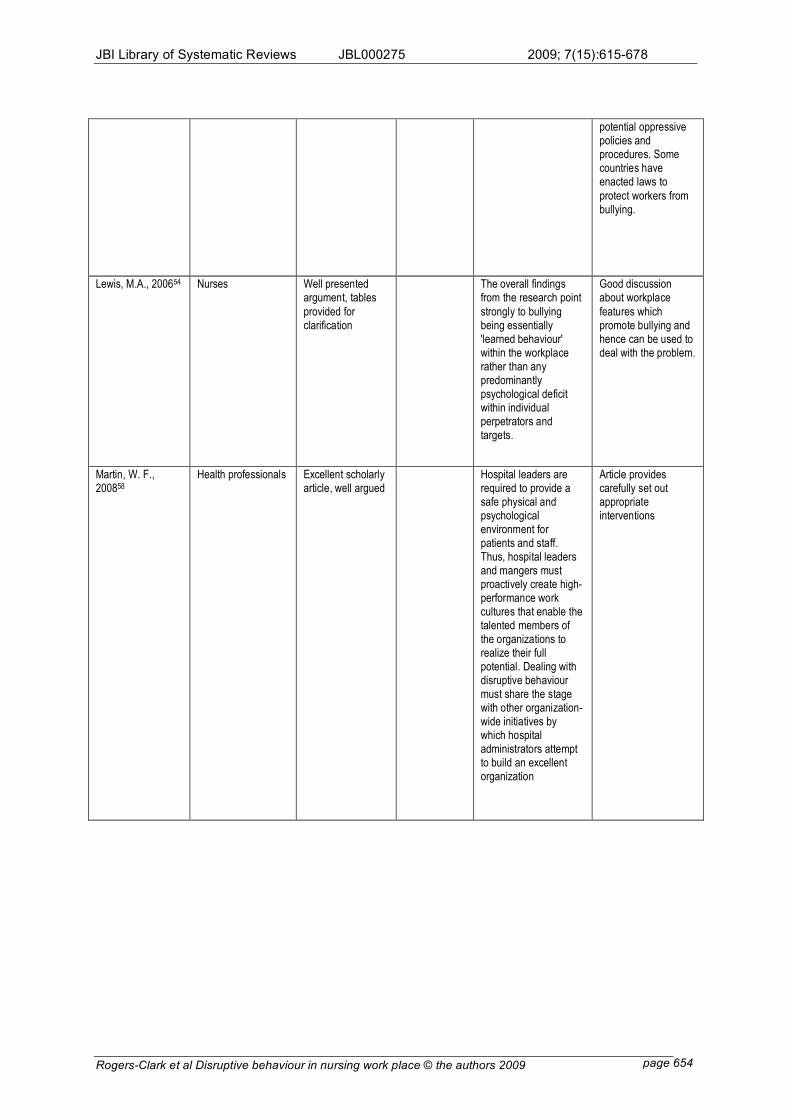
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
!
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 654
potential oppressive policies and procedures. Some countries have enacted laws to
protect workers from bullying.
Lewis, M.A., 200654 Nurses Well presented argument, tables
provided for clarification
The overall findings from the research point
strongly to bullying being essentially 'learned behaviour' within the workplace rather than any predominantly psychological deficit within individual perpetrators and targets.
Good discussion about workplace
features which promote bullying and hence can be used to deal with the problem.
Martin, W. F., 200858
Health professionals Excellent scholarly article, well argued
Hospital leaders are required to provide a safe physical and psychological environment for patients and staff. Thus, hospital leaders and mangers must proactively create high-performance work cultures that enable the talented members of the organizations to realize their full potential. Dealing with disruptive behaviour must share the stage with other organization-wide initiatives by which hospital administrators attempt to build an excellent organization
Article provides carefully set out appropriate interventions
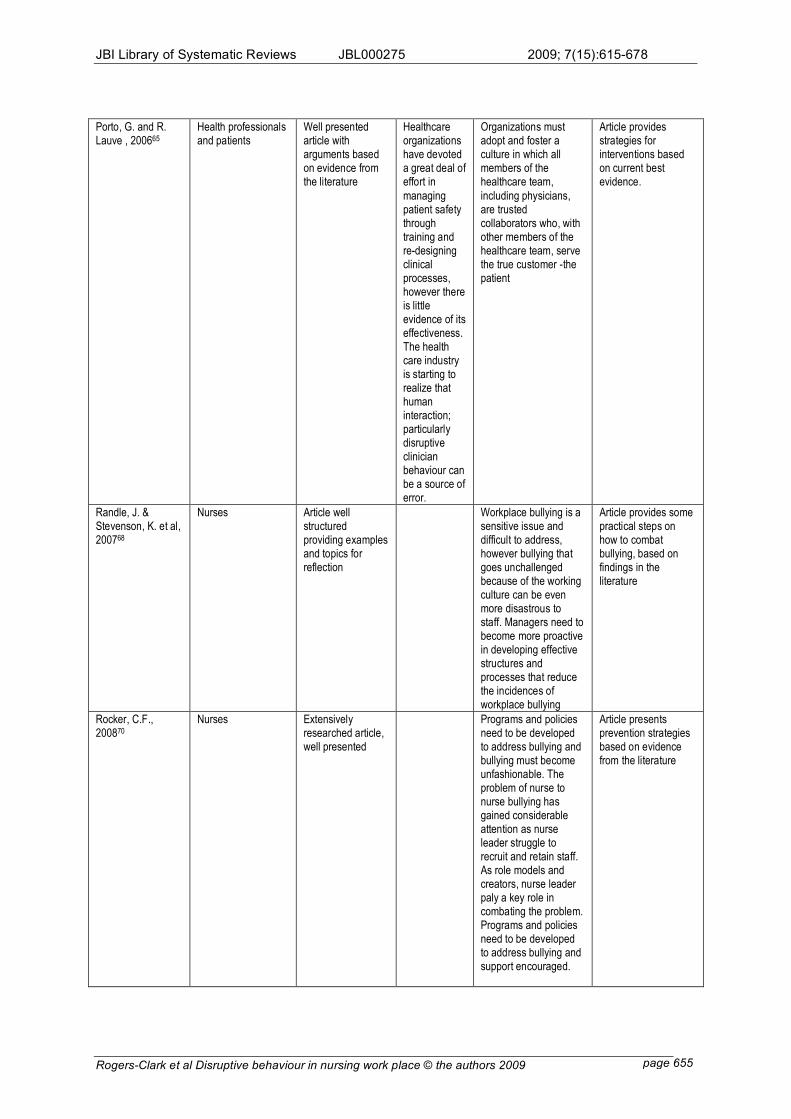
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
!
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 655
Porto, G. and R. Lauve , 200665
Health professionals and patients
Well presented article with arguments based on evidence from the literature
Healthcare organizations have devoted a great deal of effort in
managing patient safety through training and re-designing clinical processes, however there is little evidence of its effectiveness. The health care industry is starting to realize that human interaction; particularly disruptive clinician behaviour can be a source of error.
Organizations must adopt and foster a culture in which all members of the healthcare team,
including physicians, are trusted collaborators who, with other members of the healthcare team, serve the true customer -the patient
Article provides strategies for interventions based on current best evidence.
Randle, J. & Stevenson, K. et al, 200768
Nurses Article well structured providing examples and topics for reflection
Workplace bullying is a sensitive issue and difficult to address, however bullying that goes unchallenged because of the working culture can be even more disastrous to staff. Managers need to become more proactive in developing effective structures and processes that reduce the incidences of workplace bullying
Article provides some practical steps on how to combat bullying, based on findings in the literature
Rocker, C.F., 200870
Nurses Extensively researched article, well presented
Programs and policies need to be developed to address bullying and bullying must become unfashionable. The problem of nurse to nurse bullying has gained considerable attention as nurse leader struggle to recruit and retain staff. As role models and creators, nurse leader paly a key role in combating the problem. Programs and policies need to be developed to address bullying and support encouraged.
Article presents prevention strategies based on evidence from the literature
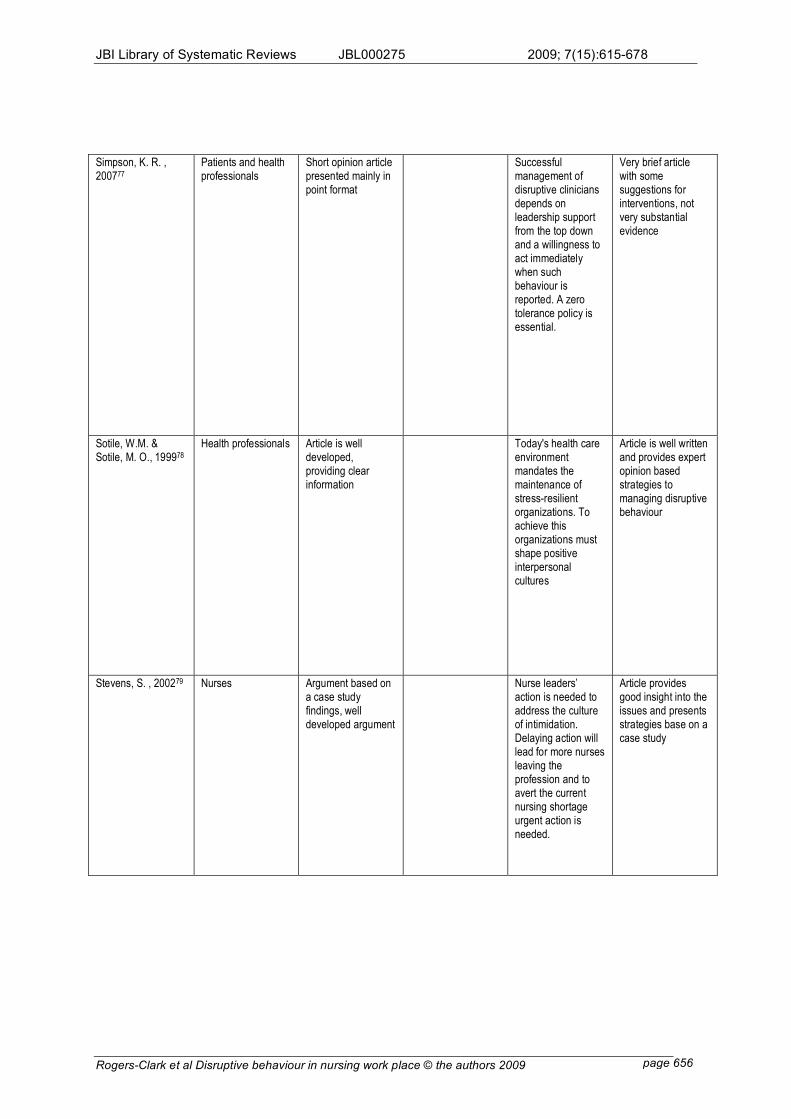
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
!
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 656
Simpson, K. R. , 200777
Patients and health professionals
Short opinion article presented mainly in point format
Successful management of disruptive clinicians depends on leadership support from the top down and a willingness to act immediately when such behaviour is reported. A zero tolerance policy is essential.
Very brief article with some suggestions for interventions, not very substantial evidence
Sotile, W.M. & Sotile, M. O., 199978
Health professionals Article is well developed, providing clear information
Today's health care environment mandates the maintenance of stress-resilient organizations. To achieve this organizations must shape positive interpersonal cultures
Article is well written and provides expert opinion based strategies to managing disruptive behaviour
Stevens, S. , 200279 Nurses Argument based on a case study findings, well developed argument
Nurse leaders’ action is needed to address the culture of intimidation. Delaying action will lead for more nurses leaving the profession and to avert the current nursing shortage urgent action is needed.
Article provides good insight into the issues and presents strategies base on a case study
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
!
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 657
Thomas, S. P., 200381
Nurses Well structured and logically presented
Nurses have a vital obligation to play a part in creating a more humane and satisfying workplace
and ultimately a more powerful profession.
Well researched article which presents some research based strategies for
managing anger in the workplace.
Appendix VII: Excluded Studies
QARI
Hutchinson, M. & Vickers, M.H. & Jackson, D. & Wilkes, L., "I'm gonna do what I wanna do."
Organisational change as a legitimized vehicle for bullies
Reason for Exclusion Does not adequately address objectives of this review
Liefooghe, A. P.D. & Olafsson, R., "Scientists" and "amateurs": mapping the bullying domain
Reason for Exclusion Does not address review objective, no focus on interventions
MAStARI
Antecol, H. & Cobb-Clark, D., Does sexual harassment training change attitudes? A view from the
Federal level
Reason for Exclusion Does not meet inclusion criteria
Befar, K.J & Peterson, R.S. & Mannix, E.A. & Trochim, M.K., The critical role of conflict resolution in
teams: a close look at the links between conflict type, conflict management strategies, and
team outcomes
Reason for Exclusion Does not meet inclusion criteria
DeChurch, L. A., K. L. Hamilton, et al. , Effects of conflict management strategies on perceptions of
intragroup conflict.
Reason for Exclusion Not congruent with review objectives
Hegney, D. & Eley, R. & Plank, A. & Buikstra, E. & Parker, V., Workforce issues in nursing in
Queensland: 2001 and 2004
Reason for Exclusion Does not meet review objectives
Hendel, T. & Fish, M. & Galon, V., Leadership style and choices of strategy in conflict management
among Israeli nurse managers in general hospitals
Reason for Exclusion Does not meet review objectives
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
!
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 658
Judkins, S.& Reid, B. et al. , Hardiness training among nurse managers: building a healthy workplace.
Reason for Exclusion Very small sample size, study not congruent with review objectives
Lim, S. & Cortina, L. M & Magley, V.J., Personal and workgroup incivility: Impact on work and health
outcomes
Reason for Exclusion Does not meet inclusion criteria, no focus on interventions
McGillis Hall, L. & Doran, D. & Pink, L., Outcomes of Interventions to improve hospital nursing work
environments
Reason for Exclusion Does not address review objectives
McLemore, M., Workplace aggression: beginning a dialogue
Reason for Exclusion No focus on successful interventions
Poilpot-Rocaboy, G. & Winter, R., Combating psychological harassment in the workplace: processes
for management interventions
Reason for Exclusion A single case study, does not meet inclusion criteria
Rutherford, A, & Rissel, C., A survey of workplace bullying in a health sector organisation
Reason for Exclusion Does not meet review objectives, no focus on interventions
Salin, D. , Organisational responses to workplace harassment.
Reason for Exclusion Does not meet inclusion criteria
Williams, R., Capturing the moment
Reason for Exclusion Does not address study objectives
NOTARI
Beech, B., Beating the bullies
Reason for Exclusion Poor quality, does not meet review objective
Beyea, Suzanne C., Intimidation in health care settings and patient safety
Reason for Exclusion Does not address review objective
Brennan, W. , I'm talking to you! Managing bullying and harassment in the workplace.
Reason for Exclusion Little reference to previous research, opinion not well justified
Broome, B. A., Dealing with sharks and bullies in the workplace
Reason for Exclusion Poorly written and unprofessional analogies used
Cassirer, C.D. & Anderson, D. & Hanson, S., Abusive behaviour in the healthcare workplace
Reason for Exclusion Opinion article, interventions suggested but no supportive evidence
Corr, Margaret, Reducing occupational stress in intensive care
Reason for Exclusion Does not meet review objective
Crawford, N., Conundrums and confusion in organisations: the etymology of the word 'bully'
Reason for Exclusion A loose discussion of the problem, no interventions presented
Everton, W.J. & Jolton, J. A. & Mastrangelo, P.M., Be nice and fair or else: understanding reasons for
employees' deviant behaviours
Reason for Exclusion Does not meet inclusion criteria
Friesen, M.A & Hughes, R.G. & Zorn, M., Communication: patient safety and the nursing work
environment
Reason for Exclusion Does not provide information on interventions
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
!
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 659
Jackson, D.,& Firtko, A. et al. , Personal resilience as a strategy for surviving and thriving in the face
of workplace adversity: a literature review.
Reason for Exclusion Not congruent with review objective
Kelloway, E.K. & Day, A. L, Building healthy workplaces: What we know so far
Reason for Exclusion Does not meet inclusion criteria
Leiper, J., Nurse against nurse: how to stop horizontal violence
Reason for Exclusion Short article that does not add anything to review, based on brief review
of the literature
Lewis, T., What must we do about lateral violence?
Reason for Exclusion Brief opinion piece, does not meet study objective
Olsen, B. J., D. L. Neslon, et al. , Managing aggression in organizations: what leaders must know.
Reason for Exclusion Does not meet inclusion criteria
Pearson, C. M. and C. L. Porath , On the nature, consequences and remedies of workplace incivility:
No time for
Reason for Exclusion An interesting commentary article but does not meet inclusion criteria
Pearson, C. M., & Andersson, L.M. et al. , Assessing and attacking workplace incivility.
Reason for Exclusion Studies poorly reported, does not meet inclusion criteria
Ramos, M.C., Eliminate destructive behaviours through example and evidence
Reason for Exclusion Does not offer anything new, just commentary on what should be done
Rayner, C. , From research to implementation: finding leverage for prevention.
Reason for Exclusion Interesting findings but insufficient detail about study methodology
Sheehan, Michael, Workplace bullying: responding with some emotional intelligence
Reason for Exclusion Does not meet inclusion criteria
Sheehan, Michael & Barker, M. & Rayner, C., Applying strategies for dealing with workplace bullying
Reason for Exclusion Does not meet inclusion criteria
Shuttleworth, A., Managing workplace stress: how training can help
Reason for Exclusion Does not address objective of review
Townend, A, Understanding and addressing bullying in the workplace
Reason for Exclusion Does not meet inclusion criteria
Van Fleet, D.D. & Griffin, R.W., Dysfunctional organization culture: The role of leadership in
motivating dysfunctional work behaviours
Reason for Exclusion Does not meet inclusion criteria
Weiss, Barbara, Balancing act. Making it work with difficult people
Reason for Exclusion Commentary only, does not address review objective
Woelfle, C.Y. & McCaffrey, R., Nurse on Nurse
Reason for Exclusion Does not adequately address objectives of the review
Zwarenstein, M. B. W., Interventions to promote collaboration between nurses and doctors
Reason for Exclusion Does not meet review objective
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
!
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 660
Appendix VIII: List of study findings / conclusions
Changing nurses' disempowering relationship patterns 36
Finding1
Nurses look up to other professionals and value inter-disciplinary teamwork. Nurses may sometime value teamwork over advocating the needs of the patient. Inter-professional relationships with medical staff remain unequal.36
Illustration
'Because the nurse is part of the team, it is good...but that he or she aligns herself with the client and not the team, which we initially thought that would happen, but it has not' 36 (p.45).
Finding2
Nurses fail to support each other, especially graduate nurses and new staff. 36
Illustration 'Nurses get on each others' cases....The nice thing would be if there was no pettiness, of this holding back...I will not tell others this, it is my own little, personal pool of knowledge...because so and so will steal the glory or whatever...like sometimes the pettiness interferes from one shift to another, or one person to another' 36 (P.46)
Finding3 The subordinate role of women and societal expectations continue to influence nursing's lack of status and recognition.36
Illustration 'Nurses are still considered handmaidens to medicine...we like to think otherwise, but you just have to watch people in action and they still kowtow [bow] to them, they still have the power'. 36
Finding4
To change intra and inter-professional relationships, and enhance nurses' status, mutual support, recognition, shared decision making, education and self-awareness are important. 36
Illustration
'You have to be prepared to help each other and listen to each other' 36
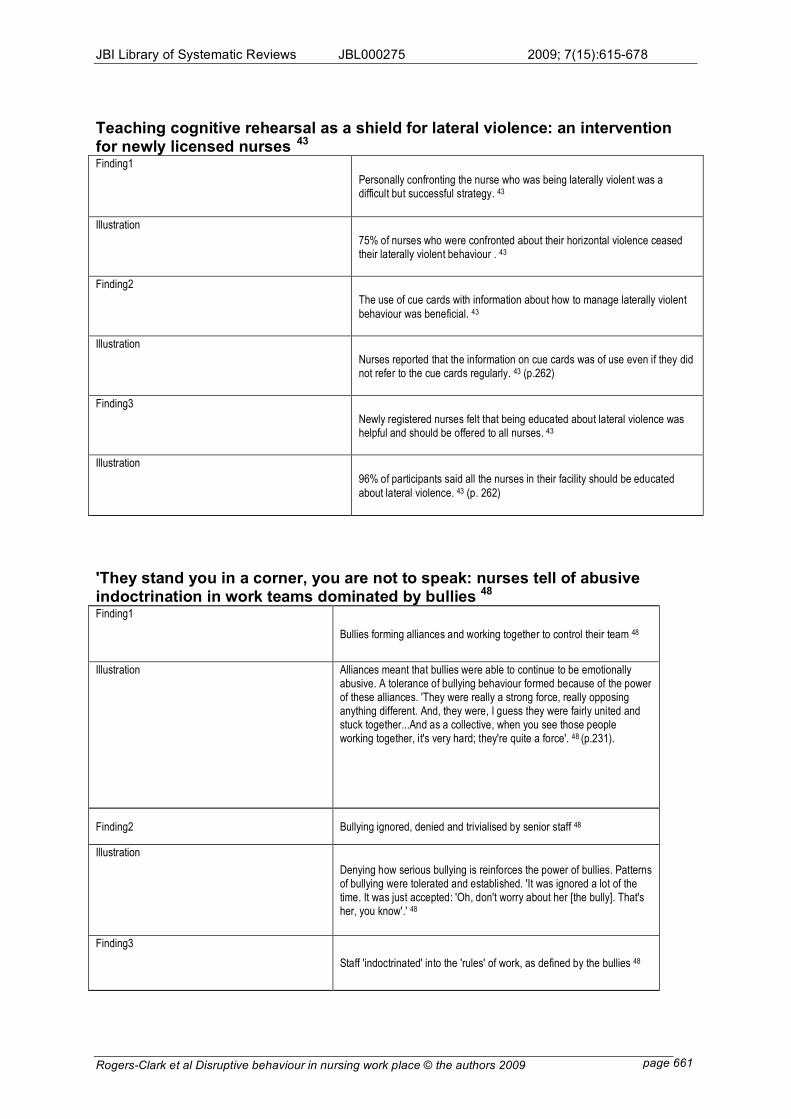
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
!
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 661
Teaching cognitive rehearsal as a shield for lateral violence: an intervention for newly licensed nurses 43
Finding1
Personally confronting the nurse who was being laterally violent was a difficult but successful strategy. 43
Illustration
75% of nurses who were confronted about their horizontal violence ceased their laterally violent behaviour . 43
Finding2
The use of cue cards with information about how to manage laterally violent
behaviour was beneficial. 43
Illustration
Nurses reported that the information on cue cards was of use even if they did not refer to the cue cards regularly. 43 (p.262)
Finding3
Newly registered nurses felt that being educated about lateral violence was helpful and should be offered to all nurses. 43
Illustration
96% of participants said all the nurses in their facility should be educated
about lateral violence. 43 (p. 262)
'They stand you in a corner, you are not to speak: nurses tell of abusive indoctrination in work teams dominated by bullies 48 Finding1
Bullies forming alliances and working together to control their team 48
Illustration Alliances meant that bullies were able to continue to be emotionally abusive. A tolerance of bullying behaviour formed because of the power of these alliances. 'They were really a strong force, really opposing anything different. And, they were, I guess they were fairly united and stuck together...And as a collective, when you see those people working together, it's very hard; they're quite a force'. 48 (p.231).
Finding2 Bullying ignored, denied and trivialised by senior staff 48
Illustration
Denying how serious bullying is reinforces the power of bullies. Patterns of bullying were tolerated and established. 'It was ignored a lot of the time. It was just accepted: 'Oh, don't worry about her [the bully]. That's her, you know'.' 48
Finding3
Staff 'indoctrinated' into the 'rules' of work, as defined by the bullies 48
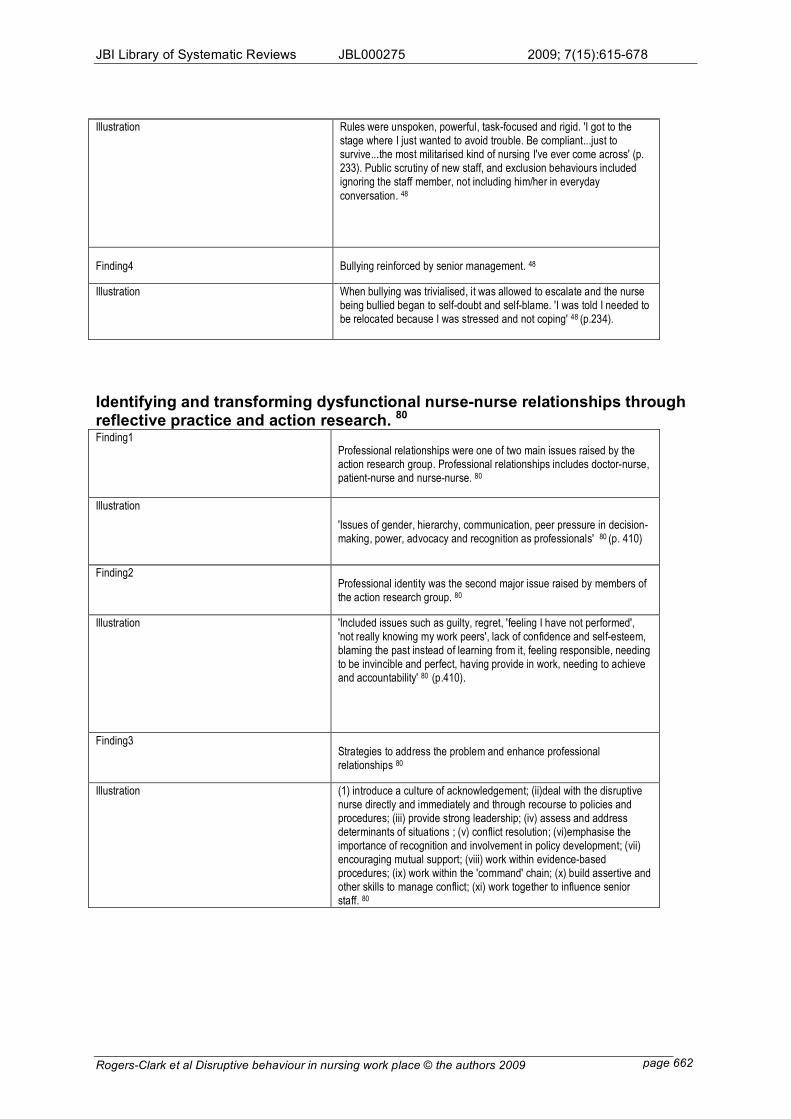
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
!
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 662
Illustration Rules were unspoken, powerful, task-focused and rigid. 'I got to the stage where I just wanted to avoid trouble. Be compliant...just to survive...the most militarised kind of nursing I've ever come across' (p. 233). Public scrutiny of new staff, and exclusion behaviours included ignoring the staff member, not including him/her in everyday
conversation. 48
Finding4 Bullying reinforced by senior management. 48
Illustration When bullying was trivialised, it was allowed to escalate and the nurse being bullied began to self-doubt and self-blame. 'I was told I needed to be relocated because I was stressed and not coping' 48 (p.234).
Identifying and transforming dysfunctional nurse-nurse relationships through reflective practice and action research. 80
Finding1 Professional relationships were one of two main issues raised by the action research group. Professional relationships includes doctor-nurse, patient-nurse and nurse-nurse. 80
Illustration
'Issues of gender, hierarchy, communication, peer pressure in decision-making, power, advocacy and recognition as professionals' 80 (p. 410)
Finding2 Professional identity was the second major issue raised by members of the action research group. 80
Illustration 'Included issues such as guilty, regret, 'feeling I have not performed', 'not really knowing my work peers', lack of confidence and self-esteem, blaming the past instead of learning from it, feeling responsible, needing to be invincible and perfect, having provide in work, needing to achieve and accountability' 80 (p.410).
Finding3 Strategies to address the problem and enhance professional relationships 80
Illustration (1) introduce a culture of acknowledgement; (ii)deal with the disruptive nurse directly and immediately and through recourse to policies and procedures; (iii) provide strong leadership; (iv) assess and address determinants of situations ; (v) conflict resolution; (vi)emphasise the importance of recognition and involvement in policy development; (vii) encouraging mutual support; (viii) work within evidence-based procedures; (ix) work within the 'command' chain; (x) build assertive and other skills to manage conflict; (xi) work together to influence senior staff. 80
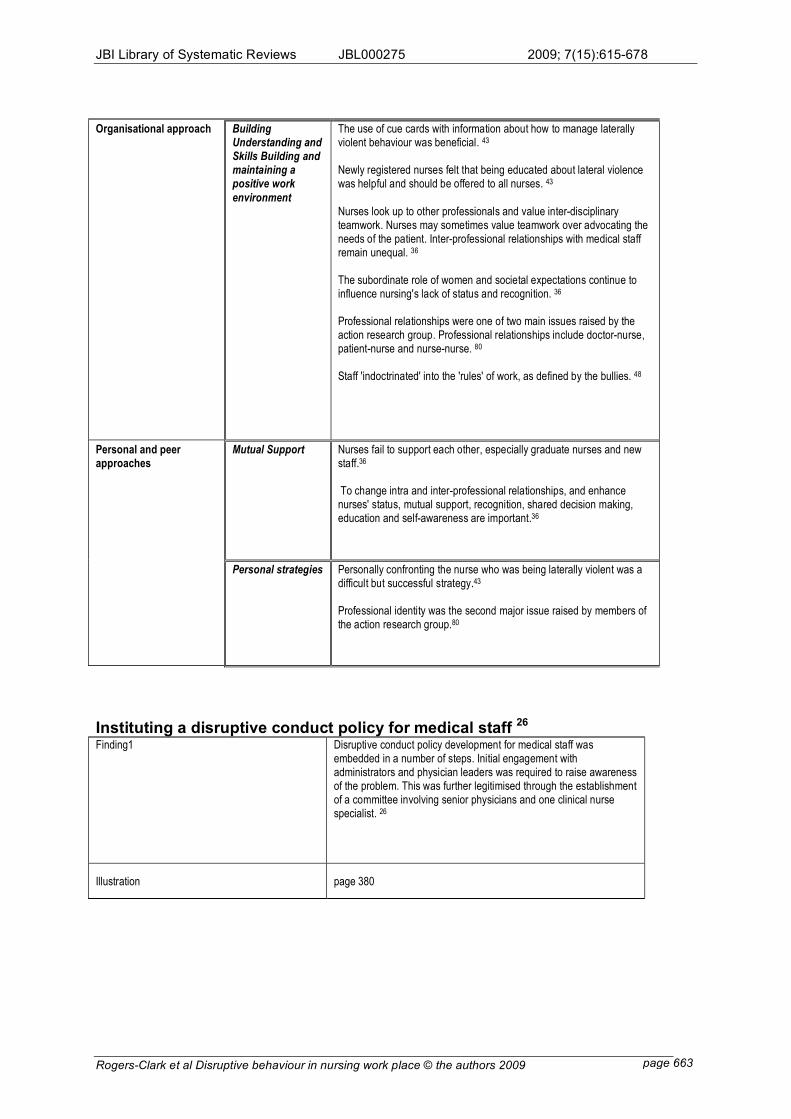
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
!
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 663
Organisational approach Building Understanding and Skills Building and maintaining a positive work
environment
The use of cue cards with information about how to manage laterally violent behaviour was beneficial. 43
Newly registered nurses felt that being educated about lateral violence was helpful and should be offered to all nurses. 43
Nurses look up to other professionals and value inter-disciplinary teamwork. Nurses may sometimes value teamwork over advocating the needs of the patient. Inter-professional relationships with medical staff remain unequal. 36
The subordinate role of women and societal expectations continue to influence nursing's lack of status and recognition. 36 Professional relationships were one of two main issues raised by the action research group. Professional relationships include doctor-nurse, patient-nurse and nurse-nurse. 80
Staff 'indoctrinated' into the 'rules' of work, as defined by the bullies. 48
Mutual Support Nurses fail to support each other, especially graduate nurses and new staff.36
To change intra and inter-professional relationships, and enhance nurses' status, mutual support, recognition, shared decision making, education and self-awareness are important.36
Personal and peer approaches
Personal strategies
Personally confronting the nurse who was being laterally violent was a difficult but successful strategy.43
Professional identity was the second major issue raised by members of the action research group.80
Instituting a disruptive conduct policy for medical staff 26
Finding1 Disruptive conduct policy development for medical staff was embedded in a number of steps. Initial engagement with administrators and physician leaders was required to raise awareness of the problem. This was further legitimised through the establishment of a committee involving senior physicians and one clinical nurse specialist. 26
Illustration page 380
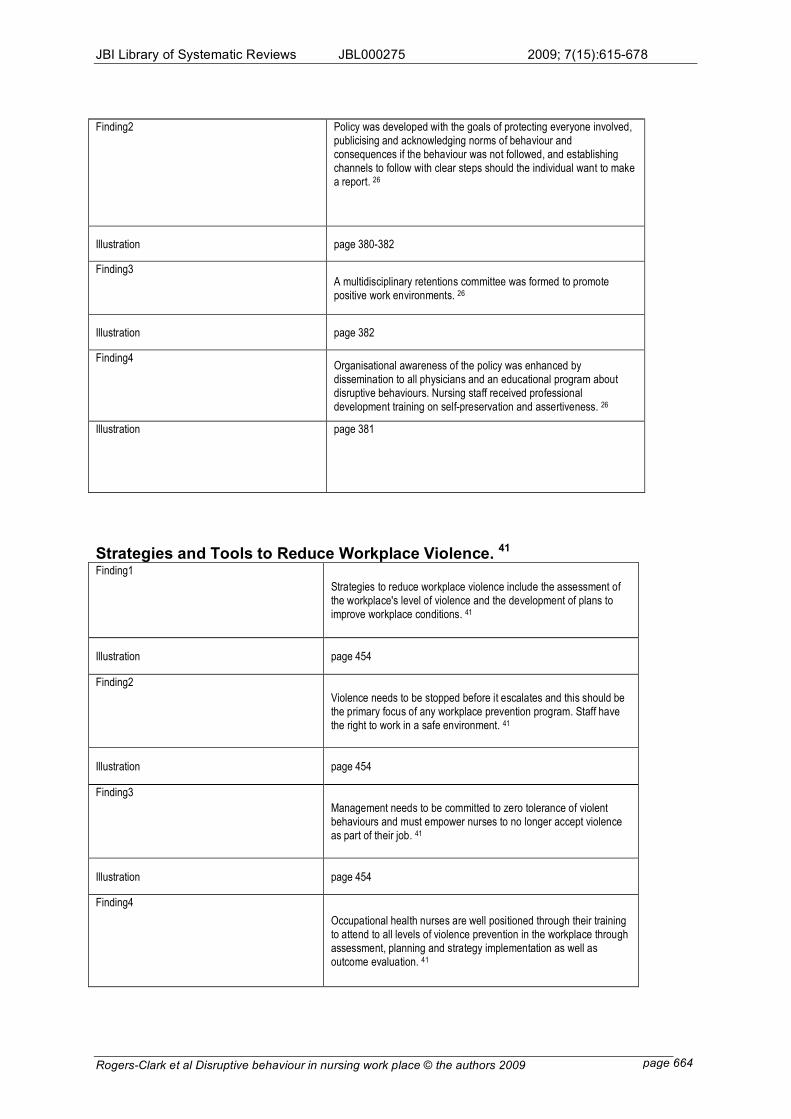
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
!
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 664
Finding2 Policy was developed with the goals of protecting everyone involved, publicising and acknowledging norms of behaviour and consequences if the behaviour was not followed, and establishing channels to follow with clear steps should the individual want to make a report. 26
Illustration page 380-382
Finding3 A multidisciplinary retentions committee was formed to promote positive work environments. 26
Illustration page 382
Finding4 Organisational awareness of the policy was enhanced by dissemination to all physicians and an educational program about disruptive behaviours. Nursing staff received professional development training on self-preservation and assertiveness. 26
Illustration page 381
Strategies and Tools to Reduce Workplace Violence. 41
Finding1
Strategies to reduce workplace violence include the assessment of the workplace's level of violence and the development of plans to improve workplace conditions. 41
Illustration page 454
Finding2
Violence needs to be stopped before it escalates and this should be the primary focus of any workplace prevention program. Staff have the right to work in a safe environment. 41
Illustration page 454
Finding3
Management needs to be committed to zero tolerance of violent behaviours and must empower nurses to no longer accept violence as part of their job. 41
Illustration page 454
Finding4
Occupational health nurses are well positioned through their training to attend to all levels of violence prevention in the workplace through assessment, planning and strategy implementation as well as outcome evaluation. 41
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
!
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 665
Illustration page 454
Crucial conversations: the most potent force for eliminating disruptive behaviour 42
Finding1
To eliminate disruptive behaviour the code of silence needs to be broken. Administrations must go public about the pervasiveness of concerns. To influence change, leaders need to begin by acknowledging the frequency of concerns. 42
Illustration page 60
Finding2
Caregivers must directly confront disruptive behaviour and nursing leaders need to invest substantially in increasing the will and skill of every employee to speak up when they see problems. 42
Illustration page 60
Finding3
Medical directors and nurse managers must respond appropriately to escalations as nurses fail to speak to their peers when they have concerns and managers fail to confront direct reports. 42
Illustration page 60
Finding4
Administration must back up sanctions when they occur. It must be clear that if code-of conduct violations occur, that administration will back up those who take appropriate action. 42
Illustration page 61
A new model of bullying in the nursing workplace 46
Finding1 In an organisation with a strong focus upon productivity, promotions may be based upon the achievement of efficiency, with little regard for the means use to achieve the outcome. In this type of environment tolerance and reward of bullying may be closely aligned to achieving outputs or performance targets. 46
Illustration page E67
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
!
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 666
Finding2 Although organisations may have well developed and high profile policies and procedures in place to respond to bullying, the authors suggest that informal organisational alliances may serve to counteract these policies and ensure reports are minimised, ignored or denied. 46
Illustration page E67
Finding3 Healthcare organisations may need to consider systems in which those responsible for investigating and managing complaints of bullying have no stake in the outcome. In particular, given that managers are reported as common perpetrators of bullying. 46
Illustration page E68
Finding4
The authors suggest that conflict-based mediation strategies risk further increasing the vulnerability of those targeted by failing to address the organisational features that enable bullying. 46
Illustration page E68
Finding5
Cultural audits may enable organisations to learn about the existence and sedimented nature of sub-climates and alliances that perpetuate tolerance of workplace bullying. 46
Illustration page E68
International perspectives on workplace bullying among nurses: a review 50
Finding1
All health care leaders should become aware of the potential for bullying to occur within their organisations, and should work to eliminate it. 50
Illustration page 38
Finding2
Policies should be put into place stating that bullying is not tolerated, and outlining how bullying incidents will be dealt with. 50
Illustration page 38
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
!
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 667
Finding3
Staff and management need to educated about bullying, what bullying behaviours look like and how to deal with bullying, both from the standpoint of a target, and as a bystander. 50
Illustration page 38
Finding4 Organisations need to determine if there are any organisational factors, such as oppressive policies and procedures, or punitive evaluation methods, that inadvertently contribute to bullying, and work to create an environment in which bullying cannot occur. 50
Illustration page 38
Nurse bullying: organizational considerations in the maintenance and perpetration of health care bullying cultures 54
Finding1 Author concludes that elements conducive to effective bullying negotiations include the avoidance of trouble, illness, litigation, damage to reputation, poor working practices and the avoidance of being called a trouble maker or labelled and rocking the boat. 54
Illustration page 57
Is your hospital safe? Disruptive behaviour and workplace bullying 58
Finding1
Adopt a zero tolerance for disruptive practitioner behaviour and enforce the policy consistently throughout the organisation. 58
Illustration page 24
Finding2
Create and sustain a high-performance work culture that focuses on attaining organisational goals by enabling individuals and groups at all levels to maximise their full potential. 58
Illustration page 24
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
!
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 668
Finding3
Recognise and reward behaviours that demonstrate collaboration, respect, and a high regard for interpersonal ethics. 58
Illustration page 24
Finding4
For any policies and procedures to be perceived as just, it is essential that reporting a complaint has no repercussions. 58
Illustration page 25
Finding5
Develop an orientation process for new employees and voluntary medical staff to clearly teach the expected behaviours and norms. 58
Illustration page 26
Finding6
Update job descriptions on the basis of a job analysis and competency development process that focuses on collaboration and team work. 58
Illustration page 26
Finding7
Adopt a behaviour-based job interview process to not only select for skills but also for behavioural competencies and a behavioural fit with the culture 58
Illustration page 26
Disruptive clinician behaviour: A persistent threat to patient safety 65
Finding1 A universal code of conduct should be developed for everyone in contact with the hospital which clearly describes those behaviours that are unacceptable. The code should be accompanied by any policies, procedures, or regulations to permit it to serve as grounds for dismissal or termination for violations 65
Illustration page 7
Finding2
Every staff member must receive a copy of the code of conduct together with training about the code and attendant behavioural expectations. Training should include guidance on what to do if disruptive behaviour is witnessed. 65
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
!
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 669
Illustration page 7
Finding3
Staff members should be required to sign a statement of intent to comply with the code of practice, which includes an acknowledgement that failure to comply may result in disciplinary actions. 65
Illustration page 7
Finding4
Organisations must have a well developed plan for monitoring compliance of the code of practice by addressing the inadequacies of voluntary reporting systems and peer monitoring. 65
Illustration page 8
Finding5
The universal code of conduct compliance monitoring system must be complemented by a clear policy of non-retaliation. 65
Illustration page 8
Finding6
Hospitals must counteract the corrosive effects of a past history of tolerance and indifference to disruptive behaviour, with consistent,
unfailing, timely, yet just responses to code violations. 65
Illustration page 8
Finding7
A multidisciplinary oversight committee must be appointed to monitor the progress of code implementation as well as code violations. 65
Illustration page 9
Finding8
Hospitals should implement known best practice designed to improve relationships between members of the health care team, such as SBAR and formal teamwork training. 65
Illustration page 9
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
!
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 670
Reducing workplace bullying in healthcare organisations 68
Finding1
Any individual who has been bullied should talk about it with a friend or trusted colleague. 68
Illustration page 55
Finding2
Staff should have knowledge about specific pieces of workplace legislation about harassment at work that the individual can refer to and discuss with a trade union representative. 68
Illustration page 55
Finding3
Maintaining a diary provides a written log of incidents and help to identify triggers to bullying episodes and recognise situations to avoid. It helps to plan and rehearse interventions strategies which may reduce escalation of the problem. 68
Illustration page 55
Finding4
Developing assertiveness in conversational style can help to reduce bullying behaviour. Assertiveness courses may be available to staff where the principles and opportunities to practise will be provided. 68
Illustration page 55-56
Addressing nurse-to-nurse bullying to promote nurse retention 70
Finding1
Nurses need to be encouraged to become involved in developing anti-bullying programs that teach the principles of bullying avoidance. 70
Illustration page 6
Finding2 Nurses need to take ownership and responsibility of the environment they work in and be involved in policy development. Policies should focus on
creating a work environment that treats nurses with dignity, respect and fairness. 70
Illustration page6-7
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
!
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 671
Finding3
Celebrating positive, bully-free work environments can also decrease bullying behaviours, such as implementing a bullying awareness week at work. 70
Illustration page 7
Finding4
Nurse leaders can also decrease bullying by promoting team work and team building among nurses to promote flexibility, sensitivity to the needs of others, and encouragement of creativity within the group. 70
Illustration page 7
Finding5 A 'Dignity at Work Policy' which includes section on harassment, discrimination, violence, and bullying, can highlight the employer's commitment to provide workers with employment that is free from acts of bullying and intimidating behaviour. 70
Illustration page 7
Disruptive Clinician Behaviour 77
Finding1 A universal code of conduct should provide guidance to both clinicians and administrators. 77
Illustration page 1
Finding2
Expectations for professional behaviour should be outlined explicitly in the institutional policies for good citizenship and reaffirmed both by leaders and each clinician on an annual basis during contract renewal and performance reviews. 77
Illustration page 1
Finding3
Behaviour should not be qualified by discipline and exceptions should not be made because he or she is 'a good doctor or nurse' otherwise. 77
Illustration page 2
Finding4
Process of reporting disruptive behaviour should be widely disseminated. There should be accountability, meaningful follow up ad actionable implications handled in a timely manner. 77
Illustration page 2
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
!
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 672
How to shape positive relationships in medical practices and hospitals 78
Finding1
A clearly stated code of conduct and policies and procedures for dealing with violations are prerequisites for developing a positive work
environment. 78
Illustration page 51
Finding2
Specific procedures for reporting inappropriate behaviours include an easy and confidential reporting system, timely and regular feedback system and development of a special committee to oversee interpersonal relationships. 78
Illustration page 52
Finding3
Managers need to listen, empathise and communication triangles when responding to complaints. 78
Illustration page 52
Finding4
Managers need to confront offenders with data, authority and compassion.78
Illustration page
Finding5
Outside help may be required for disruptive individuals or the organisation.78
Illustration page 54
Finding6
Offer workplace training and experiences that foster positive relationships.78
Illustration page 54
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
!
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 673
Finding7 Reinforce the organisation's commitment to promoting a caring, professional interpersonal culture by routinely offering in-house training in interpersonal skills as well as newsletters, awards and other incentives that reward outstanding examples of collaboration. 78
Illustration page 54
Finding8
Managers need to practice what they preach and get additional support. 78
Illustration page 55
From the field. Nursing workforce retention: challenging a bullying culture: how nurses in one Australian hospital confronted intimidation of and by nurses and took steps to remedy it. 79
Finding1
Nurse leaders need to develop more open communication and increased access to senior nursing management to tackle the culture of intimidation. 79
Illustration page 192
Finding2 Nurse leaders need to ensure that nursing supervisors receive adequate non-clinical training for their role. 79
Illustration page 192
Finding3
Nurse leaders need to ensure that competency standards refer specifically to managing bullying and that these standards are maintained through an effective performance management system. 79
Illustration page 192
Finding4 Nurse leaders need to provide access to professional development opportunities for all staff. 79
Illustration page 192
Finding5 Nurse leaders need to develop policies on bullying in the workplace and conflict resolution mechanisms. 79
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
!
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 674
Illustration page 192
Anger: The mismanaged emotion 81
Finding1
Nurses need to be educated about anger and how to manage it and empowered to act appropriately. 81
Illustration page 108
Finding2
Nurses need to support each other. In some institutions, nurses call a special 'code' when a colleague is being verbally abused: All come to stand with the nurse in support. 81
Illustration page 108
Finding3
Nurses need to be aware that they can leave an abusive situation and do not have to remain and endure unacceptable behaviour. 81
Illustration page 108
Finding4 Nurse need to resolve never to allow a physician to abuse them in front of a patient. 81
Illustration page 108
Finding5 Nurses need to use appropriate channels in the workplace to report incidence of harassment and intimidation. 81
Illustration page 108
Organisational approach Establishing a policy framework
Disruptive conduct policy development for medical staff was embedded in a number of steps. Initial engagement with administrators and physician leaders was required to raise awareness of the problem. This was further legitimised through the establishment of a committee involving senior physicians and one clinical nurse specialist. 26
Policy was developed with the goals of protecting everyone involved, publicising and acknowledging norms of behaviour and consequences if the
behaviour was not followed, and establishing channels to follow with clear steps should the individual want to make a report. 26
Policies should be put into place stating that bullying is not tolerated, and outlining how bullying incidents will be dealt with. 50
A universal code of conduct should be developed for everyone in contact with the hospital which clearly describes those behaviours that are unacceptable. The code should be accompanied by any policies, procedures, or regulations to permit it to serve as grounds for dismissal or termination for violations 65
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
!
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 675
Staff members should be required to sign a statement of intent to comply with the code of practice, which includes an acknowledgement that failure to comply may result in disciplinary actions. 65
The universal code of conduct compliance monitoring system must be
complemented by a clear policy of non-retaliation. 65
Staff should have knowledge about specific pieces of workplace legislation about harassment at work that the individual can refer to and discuss with a trade union representative. 68 A 'Dignity at Work Policy' which includes section on harassment, discrimination, violence, and bullying, can highlight the employer's commitment to provide workers with employment that is free from acts of bullying and intimidating behaviour. 70
A universal code of conduct should provide guidance to both clinicians and administrators. 77
A clearly stated code of conduct and policies and procedures for dealing with violations are prerequisites for developing a positive work environment. 78
Nurse leaders need to develop policies on bullying in the workplace and conflict resolution mechanisms. 79
Building Understanding and Skills
Organisational awareness of the policy was enhanced by dissemination to all physicians and an educational program about disruptive behaviours. Nursing staff received professional development training on self-preservation and assertiveness. 26
Occupational health nurses are well positioned through their training to attend to all levels of violence prevention in the workplace through assessment, planning and strategy implementation as well as outcome evaluation. 41
All health care leaders should become aware of the potential for bullying to
occur within their organisations, and should work to eliminate it. 50
Staff and management need to educated about bullying, what bullying behaviours look like and how to deal with bullying, both from the standpoint of a target, and as a bystander. 50 Develop an orientation process for new employees and voluntary medical staff to clearly teach the expected behaviours and norms. 58
Every staff member must receive a copy of the code of conduct together with training about the code and attendant behavioural expectations. Training should include guidance on what to do if disruptive behaviour is witnessed. 65
Nurses need to be encouraged to become involved in developing anti-bullying programs that teach the principles of bullying avoidance. 70
Reinforce the organisation's commitment to promoting a caring, professional interpersonal culture by routinely offering in-house training in interpersonal skills as well as newsletters, awards and other incentives that reward outstanding examples of collaboration. 78
Nurse leaders need to ensure that nursing supervisors receive adequate non-clinical training for their role. 79
Nurse leaders need to provide access to professional development opportunities for all staff. 79
Nurses need to be educated about anger and how to manage it and empowered to act appropriately. 81
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
!
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 676
Building and maintaining a positive work environment
A multidisciplinary retentions committee was formed to promote positive work environments. 26
To eliminate disruptive behaviour the code of silence needs to be broken. Administrations must go public about the pervasiveness of concerns. To
influence change, leaders need to begin by acknowledging the frequency of concerns. 42
Strategies to reduce workplace violence include the assessment of the workplace's level of violence and the development of plans to improve workplace conditions. 41
Violence needs to be stopped before it escalates and this should be the primary focus of any workplace prevention program. Staff have the right to work in a safe environment. 41
Management needs to be committed to zero tolerance of violent behaviours and must empower nurses to no longer accept violence as part of their job. 41
In an organisation with a strong focus upon productivity, promotions may be based upon the achievement of efficiency, with little regard for the means use to achieve the outcome. In this type of environment tolerance and reward of bullying may be closely aligned to achieving outputs or performance targets. 46
Healthcare organisations may need to consider systems in which those responsible for investigating and managing complaints of bullying have no stake in the outcome. In particular, given that managers are reported as common perpetrators of bullying. 46
Cultural audits may enable organisations to learn about the existence and sedimented nature of sub-climates and alliances that perpetuate tolerance of workplace bullying. 46
Organisations need to determine if there are any organisational factors, such as oppressive policies and procedures, or punitive evaluation methods, that inadvertently contribute to bullying, and work to create an environment in which bullying cannot occur. 50
Create and sustain a high-performance work culture that focuses on attaining organisational goals by enabling individuals and groups at all levels to maximise their full potential. 58
Recognise and reward behaviours that demonstrate collaboration, respect, and a high regard for interpersonal ethics. 58
Update job descriptions on the basis of a job analysis and competency development process that focuses on collaboration and team work. 58
Adopt a behaviour-based job interview process to not only select for skills but also for behavioural competencies and a behavioural fit with the culture.58 Hospitals should implement known best practice designed to improve relationships between members of the health care team, such as SBAR and formal teamwork training. 65
Developing assertiveness in conversational style can help to reduce bullying behaviour. Assertiveness courses may be available to staff where the principles and opportunities to practise will be provided. 68
Nurses need to take ownership and responsibility of the environment they work in and be involved in policy development. Policies should focus on creating a work environment that treats nurses with dignity, respect and
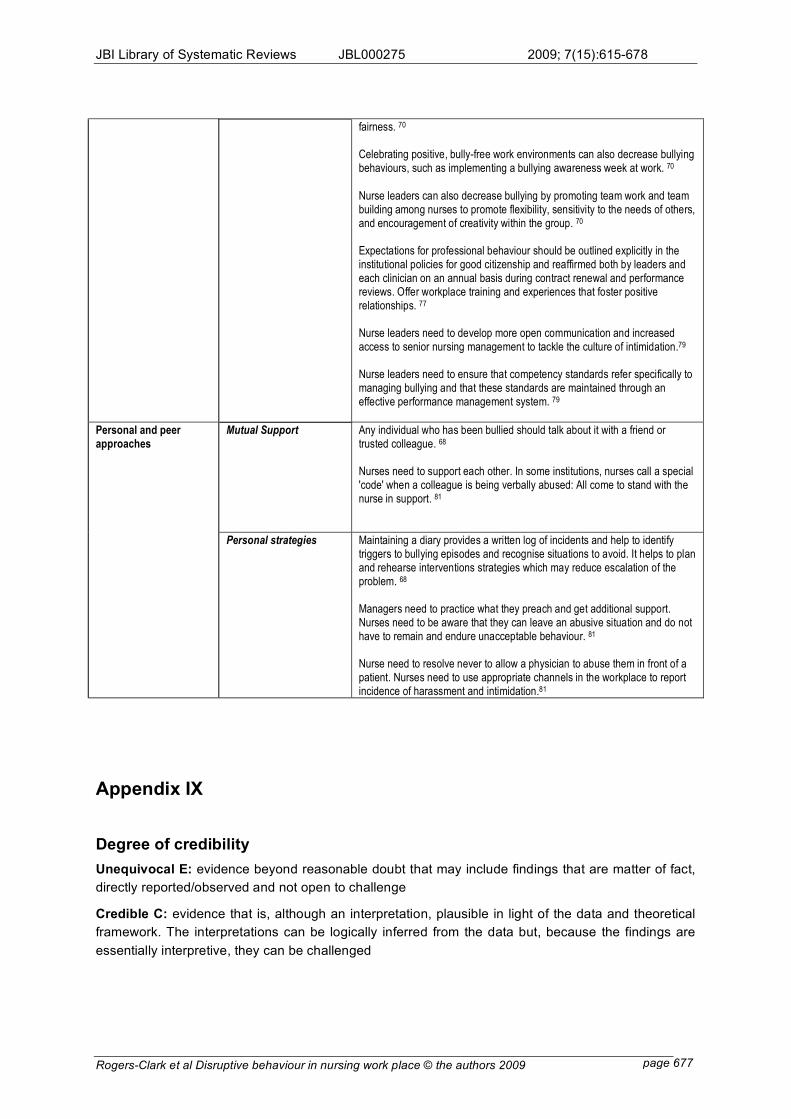
JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
!
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 677
fairness. 70
Celebrating positive, bully-free work environments can also decrease bullying behaviours, such as implementing a bullying awareness week at work. 70
Nurse leaders can also decrease bullying by promoting team work and team building among nurses to promote flexibility, sensitivity to the needs of others, and encouragement of creativity within the group. 70
Expectations for professional behaviour should be outlined explicitly in the institutional policies for good citizenship and reaffirmed both by leaders and each clinician on an annual basis during contract renewal and performance reviews. Offer workplace training and experiences that foster positive relationships. 77
Nurse leaders need to develop more open communication and increased access to senior nursing management to tackle the culture of intimidation.79 Nurse leaders need to ensure that competency standards refer specifically to managing bullying and that these standards are maintained through an effective performance management system. 79
Mutual Support Any individual who has been bullied should talk about it with a friend or trusted colleague. 68
Nurses need to support each other. In some institutions, nurses call a special 'code' when a colleague is being verbally abused: All come to stand with the nurse in support. 81
Personal and peer approaches
Personal strategies Maintaining a diary provides a written log of incidents and help to identify triggers to bullying episodes and recognise situations to avoid. It helps to plan and rehearse interventions strategies which may reduce escalation of the problem. 68
Managers need to practice what they preach and get additional support. Nurses need to be aware that they can leave an abusive situation and do not have to remain and endure unacceptable behaviour. 81
Nurse need to resolve never to allow a physician to abuse them in front of a patient. Nurses need to use appropriate channels in the workplace to report incidence of harassment and intimidation.81
Appendix IX
Degree of credibility
Unequivocal E: evidence beyond reasonable doubt that may include findings that are matter of fact,
directly reported/observed and not open to challenge
Credible C: evidence that is, although an interpretation, plausible in light of the data and theoretical
framework. The interpretations can be logically inferred from the data but, because the findings are
essentially interpretive, they can be challenged

JBI Library of Systematic Reviews JBL000275 2009; 7(15):615-678
!
Rogers-Clark et al Disruptive behaviour in nursing work place © the authors 2009 page 678
Unsupported U: when none of the other level descriptors apply and when, most 0notably, findings
are not supported by the data These three levels of evidence are incorporated into the System for the
Unified Management, Assessment and Review of Information (SUMARI) software. The Joanna Briggs
Institute, Adelaide, 2003. Used with the permission of the Joanna Briggs Institute.

Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.