-
Management Of Invasive Fungal Management Of Invasive Fungal
Infections In Infections In ImmunosupressedImmunosupressed
HostsHosts
Dimitrios P. Kontoyiannis, MD, MS, DSc, FACP, FIDSADimitrios P.
Kontoyiannis, MD, MS, DSc, FACP, FIDSAProfessor of
MedicineProfessor of Medicine
Director of Mycology Research ProgramDirector of Mycology
Research ProgramDepartment of Infectious Diseases and Infection
Department of Infectious Diseases and Infection
ControlControlThe University of TexasThe University of Texas
M. D. Anderson Cancer CenterM. D. Anderson Cancer Center
-
OutlineOutline
AspergillosisAspergillosis
CandidiasisCandidiasis
Emerging mycosesEmerging mycoses
-
Challenges in the Management of IAChallenges in the Management
of IA
Active underlying disease (e.g., leukemia, GVHD), Active
underlying disease (e.g., leukemia, GVHD), pleiotropicpleiotropic
immune defects following chemotherapy= poor immune defects
following chemotherapy= poor host immunityhost immunityMultiple
coMultiple co--morbidities, age=frequent drug
toxicitiesmorbidities, age=frequent drug toxicitiesSignificant
antifungal selection pressure=frequent Significant antifungal
selection pressure=frequent resistanceresistanceDiagnostic tests
lack specificity and Diagnostic tests lack specificity and
sensitivity=empiricismsensitivity=empiricismHeterogeneous
population at riskHeterogeneous population at riskMultiple
interventions, either simultaneously or Multiple interventions,
either simultaneously or sequentiallysequentially
-
Difficulties Specific to Management of Difficulties Specific to
Management of Invasive Pulmonary Invasive Pulmonary
AspergillosisAspergillosis
Multiple pathogens are not uncommonMultiple pathogens are not
uncommonCultures have suboptimal sensitivity and Cultures have
suboptimal sensitivity and specificity, timing and processing of
BAL not specificity, timing and processing of BAL not
standardizedstandardizedSurrogate markers: The vanishing Surrogate
markers: The vanishing ““gold gold standardstandard””
(autopsy)(autopsy)Not all infiltrates in Not all infiltrates in
immunosuppressedimmunosuppressedpatients with are due to
IPApatients with are due to IPADissemination is not
uncommonDissemination is not uncommon
-
1989-93 1994-98 1999-03
020
4060
8010
0
***
*P
-
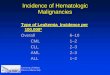
Influence of BAL Timing on Influence of BAL Timing on Diagnosis
of IPA Following HSCTDiagnosis of IPA Following HSCT
1 2 3 4 5 6 7 8 9 10 11 12 13 140
5
10
15
20
25
30
35 IPA
Day after onset of symptoms
BA
L di
agno
stic
yie
ld %
Shannon V & Kontoyiannis DP, unpublished
-
Controversies in the Management of IAControversies in the
Management of IA--11
How to deal with voriconazole failures, the preferred How to
deal with voriconazole failures, the preferred agent for IA? agent
for IA? (Walsh TJ et al. IDSA guidelines. CID 2008)(Walsh TJ et al.
IDSA guidelines. CID 2008)
Suboptimal VRC levels?Suboptimal VRC levels?Resistant
bugs?Resistant bugs?
What is the role of posaconazole as primary or salvage What is
the role of posaconazole as primary or salvage therapy?therapy?
What is the role of What is the role of azoleazole therapeutic
drug monitoring?therapeutic drug monitoring?
Is there a concern about crossIs there a concern about
cross--resistance and tolerance resistance and tolerance between
between triazolestriazoles for for AspergillusAspergillus??
-
00 1414 2828 4242 5656 7070 84840.00.0
0.20.2
0.40.4
0.60.6
0.80.8
1.01.0
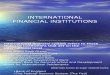
Global Comparative AspergillosisGlobal Comparative Aspergillosis
StudyStudyComparison of MortalityComparison of Mortality
Number of Days of TherapyNumber of Days of Therapy
Prob
abili
ty o
f Sur
viva
lPr
obab
ility
of S
urvi
val
Amphotericin B Amphotericin B ±± OLATOLATVoriconazole
Voriconazole ±± OLATOLAT
Hazard ratio = 0.60Hazard ratio = 0.6095% CI (0.40, 0.89)95% CI
(0.40, 0.89)
OLAT = other licensed antifungal therapyOLAT = other licensed
antifungal therapyHerbrechtHerbrecht et al. et al. N Engl J Med.N
Engl J Med. 2002;8:4082002;8:408--415415
-
OLAT = other licensed antifungal therapy.OLAT = other licensed
antifungal therapy.HerbrechtHerbrecht et al. et al. N Engl J Med.N
Engl J Med. 2002;8:4082002;8:408--415415
Global Comparative Aspergillosis StudyGlobal Comparative
Aspergillosis StudyResponses at Week 12Responses at Week 12
0
20
40
60
80
Overall Allo BMT Leuk/Lymph Pulm Extrapulm
Voriconazole ± OLAT Ampho B ± OLAT
% S
atis
fact
ory
Res
pons
e%
Sat
isfa
ctor
y R
espo
nse
-
Controversies in the Management of IAControversies in the
Management of IA--22
What is the role of the What is the role of the
echinocandinsechinocandins? ?
What is the optimal dose of lipid formulations of AMB? What is
the optimal dose of lipid formulations of AMB? Are they any PD
reasons to choose a certain lipid Are they any PD reasons to choose
a certain lipid formulations of AMB?formulations of AMB?
What is the role of combination therapy (which drugs? What is
the role of combination therapy (which drugs? when?)when?)
What is the impact of What is the impact of
AspergillusAspergillus speciation (speciation (egeg A. A.
terreusterreus))in the decisionin the decision--making?making?
-
What is the role of adjunctive surgery?What is the role of
adjunctive surgery?Extent and timingExtent and timing
What is the role recovery from What is the role recovery from
immunosupressionimmunosupression in outcome?in outcome?What is the
role of immune adjunct therapy?What is the role of immune adjunct
therapy?
What is the role of local drug delivery?What is the role of
local drug delivery?
What is the best strategy for secondary prophylaxis?What is the
best strategy for secondary prophylaxis?
Do antifungals work differently based on the Do antifungals work
differently based on the immunopathologyimmunopathology of of IA
(steroids IA (steroids vsvs neutropenia?)neutropenia?)
Controversies in the Management of IAControversies in the
Management of IA--33
-
Vfend NDA Submission, www.fda.gov
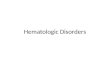
Influence of CYP2C19 Genotypeon Average Steady-State Plasma
Voriconazole Concentrations
Voriconazole Exhibits Significant Inter-Patient Pharmacokinetic
Variability
0
1
2
3
4
5
6
7
8
HomozygousExtensive
metabolizer(n=108)
HeterozygousExtensive
metabolizer(n=39)
HomozygousPoor
metabolizer(n=8)
Toxicity?
Efficacy
80% have sub-therapeutic levels with regular oralVRC dose (200mg
BID)!Bilaud et al. ISHAM 2006
-
MultiMulti--triazoletriazole (ITC, VRC, POSA, (ITC, VRC, POSA,
RAVU)RAVU)--resistant resistant AspergillusAspergillus
Netherlands survey: 0/114 pts (170 Netherlands survey: 0/114 pts
(170 A. A. fumigatusfumigatusisolates) from 1945isolates) from
1945--1998 1998 vsvs 10/81 pts (13 isolates) 10/81 pts (13
isolates) from 2002from 2002--2006 (p
-
Posaconazole for the Treatment of IA in Patients Posaconazole
for the Treatment of IA in Patients Refractory to or Intolerant of
Conventional Therapy Refractory to or Intolerant of Conventional
Therapy
(mostly AMB(mostly AMB--Based)Based)
0%5%
10%15%20%25%30%35%40%45%
Glo
bal R
espo
nse
EO
TTreatment groups:Treatment groups:–– Posaconazole
(107)Posaconazole (107)
HemeHeme maligmalig. 74%. 74%HSCT 51%HSCT 51%
–– Controls (86)Controls (86)HemeHeme maligmalig. 81%. 81%HSCT
44%HSCT 44%
PosaconazoleControl
OR 4.0695% CI 1.5-11.4P < 0.006
Walsh TJ et al. CID. 2006
-
CaspofunginCaspofungin in IAin IA
56% 56%
52%52%
42%42%
56%**56%**
44%44%
38%38%
Candoni et al. Eur J Haematol 2005*
Walsh et Al. NEJM 2004*
Betts et al. Cancer 2006*
Maertens et al. CID 2004
Kartsonis et al. J of Infection 2005
Betts et al. Cancer 2006
Monotherapy
3232
1212
1212
6666
4545
2929
% Nº Pat
Favorable Response
*First line ** >7 days of therapy
-
CaspofunginCaspofungin as First Line Therapy For as First Line
Therapy For IFIsIFIs in in Patients with Patients with
HematologicHematologic MalignancyMalignancy
Study design : OpenStudy design : Open--label, single
institution study (2004label, single institution study
(2004--2006)2006)–– Patients: Patients:
N =28, mean age = 46 yrs (18N =28, mean age = 46 yrs (18--66
yrs)66 yrs)HematologicHematologic malignancy (13 AML, 5 ALL, 2 MM,
8 lymphoma)malignancy (13 AML, 5 ALL, 2 MM, 8 lymphoma)Severe
neutropenia in all, 22/28 possible Severe neutropenia in all, 22/28
possible IFIsIFIs, Lung infection in 27/28 , Lung infection in
27/28 HSCT 36 % ( 6 HSCT 36 % ( 6 allogeneicallogeneic + 4 + 4
autologousautologous))
–– CaspofunginCaspofungin: 50 mg/day (70 mg/day loading): 50
mg/day (70 mg/day loading)Results:Results:–– Response rate: 86%
(24/28 ) w/ concomitant Response rate: 86% (24/28 ) w/ concomitant
neutrophilneutrophil recovery, 2 recovery, 2 IFIsIFIs
relapsedrelapsed–– No breakthrough InfectionNo breakthrough
Infection–– Mean duration of CAS treatment : 18 d (6Mean duration
of CAS treatment : 18 d (6--21 d)21 d)–– No dose modification
(including 6 pts receiving No dose modification (including 6 pts
receiving CsACsA))–– SafetySafety
Well tolerated, no discontinuation due to AEWell tolerated, no
discontinuation due to AE
Bonini A, et al. ASH 2006
-
ABLC vs. Liposomal Amphotericin BABLC vs. Liposomal Amphotericin
BPharmacokinetic differencesPharmacokinetic differences
ABLC
L-AMB
Rapid RES uptake
Liver, spleenlung, lymphoid organs
Avoid rapid RESuptake
XX Persistent systemiccirculation
Liver, spleenlung, lymphoid organs
-
A Randomized, Prospective Trial of a HighA Randomized,
Prospective Trial of a High--Loading Loading Regimen vs. Standard
Dosing Regimen vs. Standard Dosing
AmbiloadAmbiload TrialTrial
EOT response and Survival at 12 weeksCornely et al ASH 2005
Patients with proven or probable IFI(n=201)
blindedL-AMB 10 mg/kg X 14 days(n=94)
L-AMB 3 mg/kg X 14 days(n=107)
L-AMB 3 mg/kg Until EOT
-
SurvivalSurvivalAmbiloadAmbiload Trial Trial
Cornely et al ASH 2005
94
93
76
72
91
88
69
59
0 20 40 60 80 100
Day 14
EOT
4 weeks
12 weeks10 mg/kg3 mg/kg
% ResponseNo differences were statistically significant
-
PracticalPractical
ScientificScientific
Prospective clinical trialsAnimal studiesIn vitro studies
Mechanisms of synergy
Prospective clinical trialsAnimal studiesIn vitro studies
Mechanisms of synergy
Spectrum of therapyIntensity of therapySafety of therapy
Spectrum of therapyIntensity of therapySafety of therapy
Increasing net immunosuppressive state of patient
Pragmatism vs. Science andPragmatism vs. Science andDecisions to
Use Combination TherapyDecisions to Use Combination Therapy
Lewis REL & Kontoyiannis DP. Br J Hematology 2005
-
Combination therapy for invasive aspergillosisCombination
therapy for invasive aspergillosisAccumulating evidence for
benefit?Accumulating evidence for benefit?
Days since diagnosis of IA
0.60.6
00 2020
Prob
abilit
y of
dea
th d
ue to
IA
1.01.0
0.40.4
0.20.2
006060 70704040
0.80.8
1010 3030 5050 8080 9090
P=.02
Marr KA. Clin Infect Dis. 2004;39:797.
VariableVariable Odds Odds ratioratio
95% C.I.95% C.I. PP--valuevalue
Treatment with VRC Treatment with VRC + CAS+ CAS
0.4190.419 0.1390.139--1.2631.263
0.120.12
Renal failureRenal failure 2.8032.803 0.9460.946--8.3048.304
0.0620.062
CMV infectionCMV infection 4.3404.340
1.4431.443--13.05713.057
0.0090.009
Singh et al. Transplantation 2006;81:320-6.
When controlled for renal failure and CMV infection, patients in
the study group were 2.4 times less likely to die within 90 days
compared to the control group(O.R.=0.419, 95% CI, 0.14-1.3). The
difference however, was not statistically significant (p =
0.12).
0
10
20
30
40
50
60
70
80
Day 14 EOT
Ambi 10Ambi 3 + CAS
Favo
rabl
e O
vera
ll R
espo
nse P = 0.028
Caillot. et al. (Combistrat)ISHAM 2006; Abstract 0-0017
N= 30 patients
Voriconazole + CAS
Voriconazole
Retrospective salvage data of LipoAMB+ CAS in IA: ? benefit
(Alief et al. Cancer 2003, Kontoyiannis et al. Cancer 2003)
-
.
Maertens J et al. Cancer. 2006;107(12):2888-97
CAS-based Combination Therapy for IA
-
Not All Combinations are UsefulNot All Combinations are
Useful
Validated neutropenic rabbit model of IAValidated neutropenic
rabbit model of IASurvival rates:Survival rates:–– Control=
0%Control= 0%–– LL--AMB 1.5 mg/kg= 50%AMB 1.5 mg/kg= 50%–– RavRav 5
mg/kg= 60%5 mg/kg= 60%–– RavRav/L/L--AMB 1.5 mg/kg= 20%AMB 1.5
mg/kg= 20%–– RavRav/ L/ L--AMB 3 mg/kg= 17%AMB 3 mg/kg= 17%
Antagonism seen across all outcome markers Antagonism seen
across all outcome markers ((MeletiadisMeletiadis et alet al. . JID
2006))
Itraconazole+AMBItraconazole+AMB: ? Antagonistic in IA : ?
Antagonistic in IA ((KontoyiannisKontoyiannisDP et al. Cancer 2005,
DP et al. Cancer 2005, ChandrasekarChandrasekar& Ito, CID
2005)& Ito, CID 2005)
-
The Role of Surgery in IAThe Role of Surgery in IA
Has been associated with improved outcome in Has been associated
with improved outcome in uncontrolled seriesuncontrolled
seriesTiming, approach varies, selected group of patientsTiming,
approach varies, selected group of patientsUsually in combination
with antifungals, few patients Usually in combination with
antifungals, few patients treated with surgery alonetreated with
surgery aloneIs delay from recovery puts patient at risk for
relapse of Is delay from recovery puts patient at risk for relapse
of malignancy? malignancy? Is Is ““prepre--emptiveemptive”” surgery
important to prevent relapse surgery important to prevent relapse
of mycosis?of mycosis?Radical excision Radical excision vsvs
““debulkingdebulking”” of a dominant lesion?of a dominant
lesion?
-
Emergent Surgery for Emergent Surgery for Pulmonary
BleedingPulmonary Bleeding
Active ALL, diabetes, neutropenia, pancytopenia, Aspergillus
flavus+ Rhizopusspp
-
Lesions Suggestive of Lesions Suggestive of Aspergillosis
(LISA)Aspergillosis (LISA)
Lung sequestrum, Lung sequestrum, ““halo signhalo sign””, ,
““airair--crescent signcrescent sign””, , cavitationcavitationLISA
have 90% positive predictive value for IPA LISA have 90% positive
predictive value for IPA (25/39)(25/39)Resected LISA carry a
relatively good prognosisResected LISA carry a relatively good
prognosis
2 year2 year--survivalsurvivalResected LISA :Resected LISA :
36%36%Unresected LISA, culture negativeUnresected LISA, culture
negative 20%20%No LISA, culture positiveNo LISA, culture positive
5%5%
YeghenYeghen, et al: CID 2000;31:859, et al: CID
2000;31:859--6868
-
Role of Immune EnhancementRole of Immune EnhancementNeutrophils,
MC/macrophages are key effector immune cells againsNeutrophils,
MC/macrophages are key effector immune cells against t molds molds
((RomaniRomani et al. Nat Rev et al. Nat Rev ImmunImmun
2004)2004)Abundant preclinical data (healthy volunteers, high
infecting fuAbundant preclinical data (healthy volunteers, high
infecting fungal ngal inoculum, suprainoculum, supra--physiologic
doses of cytokines): ? relevancephysiologic doses of cytokines): ?
relevance
Local ecology of bugs, plasticity of interactions between
innateLocal ecology of bugs, plasticity of interactions between
innate and and adaptive immunity, cytokine circuitry in lung
environment, adaptive immunity, cytokine circuitry in lung
environment,
chemokineschemokinesImmunopathogenesisImmunopathogenesis is complex
and dependent of underlying immune is complex and dependent of
underlying immune defect (steroids Vs neutropenia, defect (steroids
Vs neutropenia, BalloyBalloy et al. et al. InfInf & &
ImmunImmun 2004, 2004, ChamilosChamilos et al. et al.
HematologiaHematologia 20062006))FungusFungus--related immune
dysfunction (related immune dysfunction (StanzaniStanzani et al.
Blood 2004et al. Blood 2004))
Timing, approach varies, selected group of patientsTiming,
approach varies, selected group of patients
Usually in combination with antifungals, no patients treated
witUsually in combination with antifungals, no patients treated
with h immune enhancement aloneimmune enhancement alone
Anecdotal evidence of beneficial adjunct use of GMAnecdotal
evidence of beneficial adjunct use of GM--CSF or INFCSF or
INF--gamma and or WBC transfusions in neutropenic and nongamma and
or WBC transfusions in neutropenic and non--neutropenic neutropenic
patients with patients with IMIsIMIs ((Segal et al. CID 2006)Segal
et al. CID 2006), appears safe , appears safe ((SafdarSafdar et al.
et al. Cancer 2006)Cancer 2006)
-
Strategies for Secondary Prevention of Strategies for Secondary
Prevention of Fungal PneumoniaFungal Pneumonia
Secondary antifungal prophylaxis (new triazoles)Secondary
antifungal prophylaxis (new triazoles)
GMGM--CSF elicited WBC transfusionsCSF elicited WBC
transfusions
SurgerySurgery
Role of nonRole of non--culture based methods (e.g., GM) to
prevent culture based methods (e.g., GM) to prevent
relapse?relapse?
Adoptive ImmunotherapyAdoptive Immunotherapy ((PerrucioPerrucio
et al. Blood 2005, et al. Blood 2005, ShaoShao C et al. Genes C et
al. Genes ImmunImmun 20052005) ?) ?
Sipsas & Kontoyiannis. CID 2006
-
Local Antifungal Delivery For The Local Antifungal Delivery For
The Treatment Of IPATreatment Of IPA
Aerosols, Aerosols, percutaneouspercutaneous catheter
deliverycatheter deliveryPolyenesPolyenes (AMB(AMB--d, lipid AMB)d,
lipid AMB)Case reports, concomitant systemic Case reports,
concomitant systemic antifungals, different end points of efficacy
antifungals, different end points of efficacy and safetyand
safetyDrug distribution, stability, delivery devise, Drug
distribution, stability, delivery devise, frequency:
unclearfrequency: unclear
Arthur R et al. Expert Opin Investig Drugs 2004
-
Needs in Management of IANeeds in Management of IA
Improvements in Improvements in diagnosticsdiagnostics a)
Culture yield, b) nona) Culture yield, b)
non--cultureculture--based based early early diagnosisdiagnosis
((--> pre> pre--emptive combination therapy) and c)
scorecards that emptive combination therapy) and c) scorecards that
differentiate early lung infection by different mycoses, d)
Studdifferentiate early lung infection by different mycoses, d)
Study of y of immunopathogenesisimmunopathogenesis
Understand the specific reasons why patients with fail
antifungaUnderstand the specific reasons why patients with fail
antifungalsls–– Resistance, PK/PD, toxicity, host issuesResistance,
PK/PD, toxicity, host issues
New antifungal drug developmentNew antifungal drug
development
Innovative Innovative combinationscombinations–– Local+systemic
antifungalsLocal+systemic antifungals–– Antifungals and
immunotherapy (? local, e.g, inhaled GMAntifungals and
immunotherapy (? local, e.g, inhaled GM--CSF)CSF)–– Antifungals
+surgeryAntifungals +surgery
-
CandidiasisCandidiasis
-
Delaying the Empiric Treatment of CandidaBloodstream InfectionA
Risk Factor for Hospital Mortality
0
5
10
15
20
25
30
35
24 >48
% H
ospi
tal M
orta
lity
Delay in Start of Antifungal Therapy (days)
Variable OR 95% CI P
APACHE II 1.24 (1.18-1.31)
-
TimeTime toto InitiationInitiation ofof FluconazoleFluconazole
TherapyTherapy ImpactsImpactsMortalityMortality inin
PatientsPatients withwith CandidemiaCandidemia
AA MultiMulti--InstitutionalInstitutional StudyStudy
Garey et al Clin Infect Dis 2006; 43:25-31.
05
1015202530354045
Culture day Day 1 Day 2 Day >= 3
Mor
talit
y (%
)
-
Difficulties in Establishing a Difficulties in Establishing a
Diagnosis for CandidemiaDiagnosis for Candidemia
No disease Cultures/AntigenSigns andsymptoms
Cultures/histopathology
Sequelae
Prophylaxis Preemptive Empirical
Crude Mortality40%
Dise
ase
burd
enTreatment Morbidity/
Mortality
Mortality doubles if antifungals are not started within 12 hrs
of a positive blood culture*
* Morrell et al. Antimicrob Agent Chemother 2005;49:3640.
Antigentest orPCR?
-
(1(1→→3) 3) ßß--DD--Glucan as a Marker for Glucan as a Marker
for Invasive MycosesInvasive Mycoses
Cell wall component of yeast and filamentous Cell wall component
of yeast and filamentous fungifungi
AmebocyteAmebocyte lysate assay lysate assay
Does detect:Does detect:–– Aspergillus, Candida,
FusariumAspergillus, Candida, Fusarium, , TrichosporonTrichosporon,
, SaccharomycesSaccharomyces, ,
and and AcremoniumAcremonium
Does not detect:Does not detect:–– Cryptococcus, Cryptococcus,
ZygomycetesZygomycetes
1. Yoshida M, et al. J Med Vet Mycol. 1997;35:371-374; 2.
Obayashi T, et al. Lancet.1995;345:17-20; 3. Mori T, et al. EJCCCB.
1997;35:553-560.
-
Wilson DA, et al. J Clin Microbiol. 2005;43:2909-2912.
Diagnostic MethodsDiagnostic MethodsRapid
Culture/IdentificationRapid Culture/Identification
Peptide nucleic acid fluorescence in situ hybridization assay
Peptide nucleic acid fluorescence in situ hybridization assay (PNA
(PNA FISH)FISH)–– Utilizes fluorescentUtilizes
fluorescent--labeledlabeled peptide nucleic acid probes targeting
the peptide nucleic acid probes targeting the
specific specific rRNArRNA sequencessequences of of Candida
albicansCandida albicans
Can reduce the medianCan reduce the median time required for the
identification of time required for the identification of C. C.
albicansalbicans to 9.5 hto 9.5 h (range, 3 to 17 h) vs. standard
culture median(range, 3 to 17 h) vs. standard culture median time
time of 44 h (range, 36 to 92 h) (of 44 h (range, 36 to 92 h) (PP
< 0.001)< 0.001)–– Non C. albicansNon C. albicans by culture
was even longer (61 h; range, 36 to 124by culture was even longer
(61 h; range, 36 to 124 h).h).
-
EchinocandinsEchinocandins: The preferred Drugs in The : The
preferred Drugs in The Treatment of Invasive CandidiasisTreatment
of Invasive Candidiasis
End of IV Therapy (ITT/MITT Analysis)End of IV Therapy (ITT/MITT
Analysis)
0102030405060708090
100
Ampho-d 0.6 mg/kg
Fluconazole 800/400
Vori 6mg/3mgCaspo 70/50Mica 100Mica 150Anid 200/100
% R
espo
nse
Mora-Duarte et al. N Eng J Med 2002;347:2020.Kullberg et al.
Lancet 2005;366:1435.Reboli et al. ICAAC 2005; LB Abstract
M-718.Betts et al ICAAC 2006; LB Abstract M-1308a
73.4% 73.9% 75.6%70.3%
-
CandidemiaCandidemia--Initial TherapyInitial Therapy
AI-Recommendation
• Caspofungin 70 mg d#1, 50 mg/d• Fluconazole 400-800 mg/day•
Amphotericin B 0.7 mg/kg/d• Amphotericin B (5-6 days) +
Fluconazole 800 mg/day
C-III
Liposomal AMB 3 mg/kg/dAmphotericin B + 5-FC
IDSA Guidelines for Treatment of Candidiasis. Clin Infect Dis
2004;38:161-189.
C. glabrata
• Caspofungin 70d#1, 50mg/d (A-I)• Amphotericin B 0.7mg/kg/d
(B-III)• Fluconazole 12mg/kg/d(C-III)
C. krusei
• Caspofungin 70d#1, 50mg/d(A-I)• Voriconazole 4 mg/kg
q12h(B-III) • Amphotericin B 1mg/kg/d(C-III)
-
Limitations of modern Limitations of modern
candidiasiscandidiasistrialstrials
No No neutropenicneutropenic patientspatientsRelatively stable,
most with Relatively stable, most with APACHEII
-
Caspofungin Use in a “Real-World”Setting
Caspofungin Use in aCaspofungin Use in a
““RealReal--WorldWorld””SettingSetting
Clinical Cure rates 55/66 (83%)– 23/26 (88%) intra-
abdominal infections
Attributable mortality to candidiasis (13%)Adverse events
(rare)
Clinical Cure rates Clinical Cure rates 55/66 (83%)55/66 (83%)––
23/26 (88%) intra23/26 (88%) intra--
abdominal abdominal infectionsinfections
Attributable Attributable mortality to mortality to candidiasis
(13%)candidiasis (13%)Adverse events Adverse events
(rare)(rare)
0
5
10
15
20
25
30
2001 2002 2003
Invasive candidiasis failure rates
Zaas E et al. AJM 2006
-
10
20
30
40
5060
70
80
90
100
Day 7 Day 14 Clinical Mycological
Caspofungin monotherapyCaspofungin monotherapytreatment outcome
at MDACC, 2001treatment outcome at MDACC, 2001--2006 2006
(n=64 patients)(n=64 patients)
% R
espo
nse
5
10
15
20
25
30
Day 7 Day 14 AttributableDay 30
% M
orta
lity
Sipsas & Kontoyiannis. ECCMID 2007
Day 30
-
CaspofunginCaspofungin For For Other Invasive Other Invasive
Candida Candida InfectionsInfectionsNoncomparative study to
evaluate caspofungin in Noncomparative study to evaluate
caspofungin in less common cases of invasive candidiasis:less
common cases of invasive candidiasis:–– Osteomyelitis, meningitis,
& endocarditisOsteomyelitis, meningitis, & endocarditis––
Chronic disseminated candidiasis (CDC)Chronic disseminated
candidiasis (CDC)–– Candida Candida intraintra--abdominal
infections (peritonitis & abdominal infections (peritonitis
&
abscesses) abscesses)
Diagnostic criteria: Clinical & microbiological Diagnostic
criteria: Clinical & microbiological evidence of
infectionevidence of infection
Caspofungin dosing at 50 or 100 mg/day Caspofungin dosing at 50
or 100 mg/day –– UpdosingUpdosing of caspofungin (to 100 or 150 mg
daily) of caspofungin (to 100 or 150 mg daily)
allowed in patients not responding allowed in patients not
responding Cornely O et al, ICAAC 2006
-
CaspofunginCaspofungin For Other Invasive For Other Invasive
Candida Candida Infections (cont.)Infections (cont.)
Total of 40+ sites in 13 countriesTotal of 40+ sites in 13
countries–– Enrollment at 17 sites in 10 countries, including US
(4), Enrollment at 17 sites in 10 countries, including US (4),
Central or Latin America (6), Europe (5), & Australia
(2)Central or Latin America (6), Europe (5), & Australia
(2)
Target enrollment ~50 patientsTarget enrollment ~50 patients
Enrollment August 2004 to February 2006Enrollment August 2004 to
February 2006–– Since June 2005, enrollment limited to certain
types of Since June 2005, enrollment limited to certain types
of
infections (i.e., endocarditis, meningitis, osteomyelitis,
infections (i.e., endocarditis, meningitis, osteomyelitis, septic
arthritis, endophthalmitis)septic arthritis, endophthalmitis)
–– Final data available on all 48 patientsFinal data available
on all 48 patients
Cornely O et al, ICAAC 2006
-
n/mEndpoint
Success at the End of Caspofungin Therapy (MITT)
Relapse out to 12 weeks posttherapy in patients with a favorable
response
Mortality (to 12 weeks posttherapy)
39/48 (81)
2/39 (5)
(%)
Efficacy Results Efficacy Results
MITT defined as any patient with a confirmed diagnosis of
invasive candidiasis who received at least 1 dose of
caspofungin
11/48 (23)
Cornely O et al, ICAAC 2006
-
Efficacy by Site of Efficacy by Site of Candida Candida
InfectionInfection
0102030405060708090
100
Peritonitis Endocarditis, Osteomyelitis, or Septic Arthritis
50%
Suc
cess
(%)
10/13
77%
Abscess CDC Multiple/Other
Success at the End of Caspofungin Therapy
9/10
90%
7/888%
5/771% 8/10
80%
Cornely et al, Cancer 2007
-
Controversies about treatment of Controversies about treatment
of candidiasiscandidiasis
Antifungal activity in Antifungal activity in
biofilmbiofilm--associated associated CandidaCandidaCatheter
managementCatheter managementActivity in Activity in
neutropenicneutropenic and critically ill patientsand critically
ill patientsIs there any role of in vitro Is there any role of in
vitro echinocandinechinocandin MICsMICs??What is the potential of
What is the potential of echinocandinechinocandin resistance in
resistance in CandidaCandida? ? Value of short term Value of short
term echinocandinechinocandin therapy followed by therapy followed
by
azolesazolesAre they any meaningful differences among the Are
they any meaningful differences among the
echinocandinsechinocandins??
-
Echinocandins are fungicidal versus Echinocandins are fungicidal
versus CandidaCandida species and exhibit activity species and
exhibit activity against against biofilmbiofilm--embedded
organismsembedded organisms
FIG. 3. CSLM of planktonic C. albicans cells treated with
antifungal agents. Images utilize CAAF and FUN-1 staining, a 63x
oil immersion objective, and 2xmagnification. Green CAAF staining
highlights blastospore cell walls.
Control CAS
Kuhn et al. Antimicrob Agent Chemother. 2002;46:1773-80
-
Echinocandin Activity vs. Echinocandin Activity vs.
BiofilmBiofilm--Embedded Embedded CandidaCandida
Ramage et al. Antimicrob Agent Chemother 2002;46:3634
Antifungal Killing vs. Biofilm-EmbeddedCandida spp.
Echinocandin response in azole-refractory esophagitis
10 days after echinocandin therapy10 days after echinocandin
therapy
0.5 2 160
25
50
75
100CASAMBFLU
Drug Conc (µg/mL)
% V
iabi
lity
(XTT
Ass
ay)
-
Removal of Infected CathetersRemoval of Infected Catheters
Rex et al Clin Infect Dis 1995:21;994-6.
Therapy started
0255075
100
% C
andi
dem
ic
-5 5 15Day of Last +BC
25
Changed
Not changed
-
Mortality 3 months after the initial positive blood cultureamong
adults with candidemia, according to Candida species
and APACHE II score
Pappas et al. Clin Infect Dis. 2003;37:634-643
-
Does CAS Work in NeutropenicPatients?
Does CAS Work in Does CAS Work in
NeutropenicNeutropenicPatients?Patients?
Casn/
pofungm (%
in)
L-An/m (
MB%)
Overall* 14/27 (51.9) 7/27 (25.9)
Aspergillus spp. 5/12 (41.7) 1/12 (8.3)
Candida spp. 8/12 (66.7) 5/12 (41.7)
Other 1/3 (33.3) 1/3 (33.3)
* p = 0.043
Walsh et al. N Eng J Med 2004;351:1391-1402
-
C. C. glabrataglabrata FungemiaFungemia in Patients in
Patients
With CancerWith Cancer
0102030405060708090
AMB (n=35) FLU (n=72)
C. albicansC. glabrata
0102030405060708090
AMB (n=16) FLU(n=3)
% R
espo
nded
Not neutropenic Persistently neutropenic
Bodey et al. Am J Med 2002;112:380-386.
-
Comparing tComparing thehe echinechinocandinsocandinsAre MIC
differences clinically important? Are MIC differences clinically
important?
MIC data MIC data ((unstandardizedunstandardized, mixed results,
differences not consistent , mixed results, differences not
consistent with with animal data)animal data)–– Pharmacokinetics
Pharmacokinetics (Serum (Serum eexposures xposures MICA, CAS, >
MICA, CAS, > AnidulAnidul))–– Clinical outcome Clinical outcome
(no correlation with outcomes in (no correlation with outcomes in
candidemiacandidemia))
Is there a difference in the potential to select or treat
echinoIs there a difference in the potential to select or treat
echinocandin candin resistant resistant CandidaCandida species?
species? NoNo
PPharmacokinetic differences, drug interactions, and hepatic
harmacokinetic differences, drug interactions, and hepatic
toxicity? toxicity? Some, uSome, unclear clinical
significancenclear clinical significance
Important differences in pivotal clinical trials and
indicationsImportant differences in pivotal clinical trials and
indications? ? Probably notProbably not
Formulary considerations: Formulary considerations: Complex,
costComplex, cost
-
Comparison of Comparison of MicafunginMicafungin and and
CaspofunginCaspofungin for for CandidemiaCandidemia or Invasive or
Invasive CandidiasisCandidiasis
Phase 3, 1:1:1 randomized doublePhase 3, 1:1:1 randomized
double--blind nonblind non--inferiority study in adults:inferiority
study in adults:–– MicafunginMicafungin 150 mg/day150 mg/day––
MicafunginMicafungin 100 mg/day100 mg/day–– CaspofunginCaspofungin
70/50 mg/day70/50 mg/day
Primary endpoint:Primary endpoint:–– Clinical and mycological
response at end of IV Clinical and mycological response at end of
IV
therapy with a pretherapy with a pre--specified specified ΔΔ --
15%15%
Betts et al. ICAAC 2006. Abstract M-1308a
-
C. albicans C. glabrata C. tropicalis C. krusei C.
parapsilosis0
102030405060708090
MICA 100 CAS 70/50
Comparison of Comparison of MicafunginMicafungin and and
CaspofunginCaspofungin for for CandidemiaCandidemia or Invasive or
Invasive CandidiasisCandidiasis
MICA 100 MICA 150 CAS 70/500
25
50
75
100
Per
cent
N=199 202 192
71/93 62/84
24/28
22/33 21/31 24/32 6/8 3/4 23/30
27/42
Overall Success Success by Baseline Pathogen
Betts et al. ICAAC 2006. Abstract M-1308a
-
Invasive candidiasisInvasive candidiasisWhere weWhere we’’ve
been, where weve been, where we’’re goingre going……..
SuccessesSuccesses–– Improved prevention/treatment of Improved
prevention/treatment of seriousserious CandidaCandida
infectionsinfections–– Less toxic alternatives to Less toxic
alternatives to AmBAmB--based therapybased therapy–– Resistance
remains relatively uncommon overallResistance remains relatively
uncommon overall
ChallengesChallenges: F: Further reductions in mortality!urther
reductions in mortality!–– Improved prevention strategies for high
risk ptsImproved prevention strategies for high risk pts–– Early
initiation of therapy with the best drug, at an effective Early
initiation of therapy with the best drug, at an effective
dosedose–– Improved nonImproved non--culture based
diagnosisculture based diagnosis–– Better laboratory support for
management and detection of Better laboratory support for
management and detection of
antifungal resistanceantifungal resistance
-
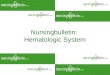
Changing Epidemiology of Invasive Changing Epidemiology of
Invasive Moulds Era of Voriconazole?Moulds Era of Voriconazole?
In untreated patients, In untreated patients, currently
considered firstcurrently considered first--line therapy for
invasive line therapy for invasive aspergillosisaspergillosisHas
activity against many Has activity against many AMBAMB--resistant
speciesresistant species–– Aspergillus terreusAspergillus terreus––
Aspergillus flavusAspergillus flavus–– FusariumFusarium sppspp..––
ScedosporiumScedosporium apiospermumapiospermum
2000 2001 2002 20030.0
0.10.2
0.3
0.40.5
0.60.7
Aspergillus
Zygomycetes
0.00
0.030.06
0.09
0.120.15
0.180.21
Year
Kontoyiannis et al. J Infect Dis 2005: 191:1350
Inci
denc
e /1
000
pt d
ay
-
0
2
4
6
8
10
12
14
16
19891990199119921993199419951996199719981999200020012002200320042005
All inpatientsAllo-HSCT
Zygomycosis at MDACC (1989-2005)A review of 100 cases
Cas
es P
er 1
00,0
00 In
patie
nt D
ays
Chamilos G, et al. ICAAC 2006 Abstract A-2156
-
Case 1Case 1
Persistent fever on day 4 of neutropenia in a patient with
leukemia during remission induction chemotherapy on
fluconazoleprophylaxis
All are false but one:A. Empiric antifungal therapy is not
justified B. Fluconazole is appropriateC. Viruses are common cause
of fever in that settingD. Caspofungin, lipid AMB formulations,
voriconazole are appropriate choices
-
Case 2Case 2
Development of fever, positive cultures for yeasts in a febrile
critically patient with in ICU while on fluconazole
prophylaxis.
The most common yeasts in that setting is:
A. C. glabrataB. C. parapsilosisC. C. albicansD. C.
tropicalis
-
Case 3Case 3
Development of fever, increased alkaline phosphatase, and
multiple lucent lesions in liver and spleen on CT scan after
engraftment post-HSCT is most likely due to:
A. Fusarium sppB. Aspergillus fumigatusC. Candida sppD.
Staphylococcus sppE. Zygomycetes
-
Case 4Case 4
In the late postengraftment period after HSCT a pulmonary
cavitary nodule seen on chest CT would most likely be due to:
A. Candida tropicalisB. Invasive moulds, most likely Aspergillus
sppC. Candida glabrataD. Pseudomonas aeruginosaE. Staphylococcus
aureus
-
Case 5Case 5
A non-neutropenic patient with AML developed postnasal drainage
and left maxillary sinus pain 52 days after allogeneic BMT while
receiving voriconazole prophylaxis (400 mg/day) since
transplantation. The patient had been receiving high-dose
methylprednisolone (total dose> 600 mg in the month prior) for
GvHD
What is a major consideration here?A) CandidaB) FusariumC)
AspergillusD) Zygomycetes
-
Case 6Case 6
A profoundly neutropenic patient with refractory AML develops
sepsis, acute pneumonia and multiple necrotic skin lesions
What is a major consideration here?A) CandidaB) FusariumC)
AspergillusD) Zygomycetes
-
Thank you!Thank you!
Management Of Invasive Fungal Infections In Immunosupressed
HostsOutlineChallenges in the Management of IADifficulties Specific
to Management of Invasive Pulmonary AspergillosisWe increasingly do
not know the cause �of death in patients with IA �Autopsy Rate
(Autopsies/deaths) at MDAAC (1015 Autopsies,Influence of BAL Timing
on Diagnosis of IPA Following HSCT Global Comparative Aspergillosis
Study �Comparison of MortalityGlobal Comparative Aspergillosis
Study Responses at Week 12Controversies in the Management of
IA-3Multi-triazole (ITC, VRC, POSA, RAVU)-resistant
AspergillusPosaconazole for the Treatment of IA in Patients
Refractory to or Intolerant of Conventional Therapy (mostly
AMB-Based)Caspofungin in IACaspofungin as First Line Therapy For
IFIs in Patients with Hematologic MalignancyABLC vs. Liposomal
Amphotericin B�Pharmacokinetic differencesA Randomized, Prospective
Trial of a High-Loading Regimen vs. Standard Dosing �Ambiload Trial
Survival�Ambiload Trial Pragmatism vs. Science and�Decisions to Use
Combination TherapyCombination therapy for invasive
aspergillosis�Accumulating evidence for benefit?Not All
Combinations are UsefulThe Role of Surgery in IALesions Suggestive
of �Aspergillosis (LISA)Role of Immune EnhancementStrategies for
Secondary Prevention of Fungal PneumoniaLocal Antifungal Delivery
For The Treatment Of IPANeeds in Management of
IACandidiasisDifficulties in Establishing a �Diagnosis for
Candidemia(13) ß-D-Glucan as a Marker for �Invasive
MycosesDiagnostic Methods�Rapid
Culture/IdentificationEchinocandins: The preferred Drugs in The
Treatment of Invasive Candidiasis�End of IV Therapy (ITT/MITT
Analysis)Candidemia-Initial TherapyLimitations of modern
candidiasis trialsCaspofungin Use in a “Real-World”
SettingCaspofungin monotherapy� treatment outcome at MDACC,
2001-2006 �(n=64 patients)Caspofungin For �Other Invasive Candida
InfectionsCaspofungin For Other Invasive Candida Infections
(cont.)Efficacy Results Efficacy by Site of Candida
InfectionControversies about treatment of candidiasis Echinocandins
are fungicidal versus Candida species and exhibit activity against
biofilm-embedded organismsEchinocandin Activity vs.
�Biofilm-Embedded CandidaRemoval of Infected CathetersDoes CAS Work
in Neutropenic Patients?�C. glabrata Fungemia in Patients �With
Cancer Comparing the echinocandinsComparison of Micafungin and
Caspofungin for Candidemia or Invasive CandidiasisComparison of
Micafungin and Caspofungin for Candidemia or Invasive
CandidiasisInvasive candidiasis�Where we’ve been, where we’re
going….Changing Epidemiology of Invasive Moulds Era of
Voriconazole?