Embed Size (px)
Citation preview
MANAGEMENT OF LUNG TUMORS; IMAGE-GUIDED ABLATION vs. SBRT
Servet Tatli MDAssociate Professor Radiology
Harvard Medical School
Department of RadiologyBrigham and Women’s Hospital
Objectives
• Review current status of image-guided tumor ablation techniques to treat lung neoplasms
• Discuss advantages and disadvantages of image-guided ablation to treat lung neoplasms in comparison to radiation therapy
• Nothing to disclose
Image-Guided Ablation• In last decades, a rapid advancement in image-guided
tumor ablative methods (i.e., RF ablation)– effective
– safe (no late complications)
– preserves normal lung parenchyma
– successful regardless of tumor histology
– minimally invasive• feasible to inoperable patient with other co-morbidities• requires minimal hospital stay; can be performed as outpatient• can be performed under conscious sedation
– can be combined with other methods (or when others fail)– serves for various goals (cure, local control, symptom palliation)
–
Image-Guided Ablation– widely available– fast– practical
• can be done in a session• requires no prior procedures such as fiducial placement or biopsy• can be done at the time of biopsy
– easily tolerated by patients– does not usually require patient cooperation– repeatable– easy to learn – less expensive than other alternatives
• 4.25 times higher cost of SBRT

Patient Selection
• Early stage (stage I&II) NSCLC– non-surgical candidate– failed other treatments
• Solitary or small number of lung metastases– without extrapulmonary disease– non-surgical candidate– failed other treatments
• Advanced (stage IIIB/IV) NSCLC & lung metastases– failed other treatments– local tumor control– symptom palliation (chest pain, cough, dyspnea, hemoptysis)
(Wagner TD, Curr Drug Targets 2010)
Tumor Selection• Size
– < 3 cm (ideal), up to 5 cm
• Number– <3-5– exceptions (very slow growing tumors such as adenoid
cystic carcinoma of salivary glands)
• Location– pleural-based– intraparenchymal (surrounded by lung parenchyma)
• >1 cm from bronchus, hilum, mediastinum (heart, trachea)
– safe access route
Complications• Pneumothorax: (~30%), majority is mild, and asymptomatic
– central tumors, patients with no prior history of surgery– ~1/3 requires pig tail catheter insertion; next day removal
• Hemoptysis: (~3%), may last 1-2 weeks– no intervention required
• Infection: (~2%)– requiring IV antibiotic
• Hydro/hemothorax, pulmonary hemorrhage: self-limited• Cavitation and bronchial fistula formation: very rare
– ablation of large tumors near large bronchi
• Issue related to low lung reserve and other co-morbidities– ~2.5 % (4/153) procedure related death (Simon
CJ, Radiology 2007)
Lung Ablation, effectiveness
• Variable reported outcome – depending on case selection and the method to measure – heterogeneous populations (~50% NSCLC and ~50% mets)
• Over all post ablation complete tumor necrosis rate – (38% to 91% ; ~63.5 %) (Ambrogi MC, E J of Cardiothoracic Surg 2006)
• Local recurrence of 43% with median disease free survival of 23 months (Beland MD, Radiology 2010)
• Local tumor control at 1year: 88% (Lencioni RR, Clin Oncology 2008)
– overall survival: 1 year (92%), 2 years (73%)
• Overall survival: (Simon JS, Radiology 2007)
• NSCLC at 1, 2, 3, 4, 5 y: 78%, 57%, 36%, 27% & 27%• colorectal mets at 1, 2, 3, 4, 5 y: 87%, 78%, 57%, 57% & 57%
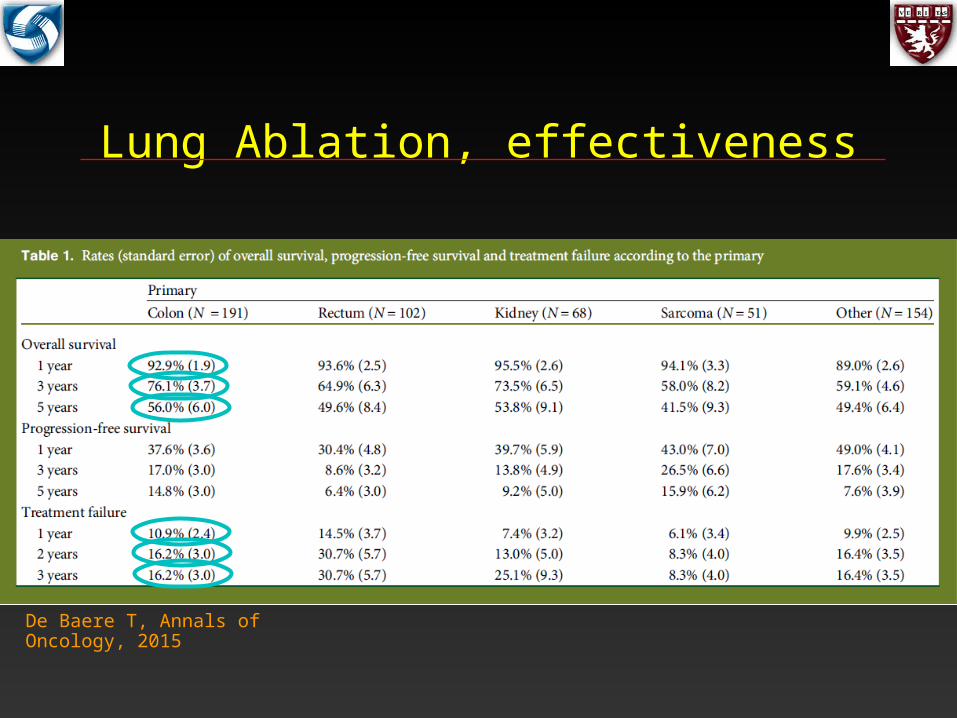
Lung Ablation, effectiveness
De Baere T, Annals of Oncology, 2015
Lung Ablation vs. SBRT
• External beam XRT– 5-year overall survival rates; 0% to 42% (Rowel NP, Thorax 2001)
• SBRT– local control rate at 3 years: ~90 (Onishi H, Cancer 2004)
– 3 year overall survival: 58% (Timmerman R, JAMA 2010)
• 5 year lung cancer specific survival rate– XRT: 46%– SBRT:73%– RFA: 77% (Tramontano AC, AJR 2012)
RFA vs. SBRT
• Decision should be depend on – tumor size
– location
– comorbidities
– individual patient preference
– availability
RFA vs. SBRT
• Patients with cardiopulmonary compromise may find it difficult to stay still during SBRT
• RFA– require no prior biopsy or fiducial placement
– can be done in a single session
– repeatable
– can be combined with other techniques
RFA vs. SBRT
• RFA is not appropriate:– central tumors
• blood vessels (heat sink)• central airways, nerves, esophagus (injury)
– large tumors (>3cm), decreased effectiveness
• Microwave may be proven more effective• better energy deposition (higher intratumoral heat)• less effected by thermal sink
• Cryoablation may be better– central tumor– large tumors
• IRE may be better for central tumors
Conclusion
• Image-guided RF ablation is promising treatment option for selected patients with primary or metastatic neoplasm of lungs that are not amenable to surgery
• It is not only safe and minimally invasive but also associated with improve long term survival given the patient population treated
• Careful patient selection and appropriate preablation work up and post ablation surveillance are important for satisfactory results

Thank you