Embed Size (px)
Citation preview
Management of Thyroid Disease: Too much, too little, masses
1 Fitzgerald Health Education Associates, Inc.
Margaret A. Fitzgerald, DNP, FNP-BC, NP-C, FAANP, CSP, FAAN, DCC
President, Fitzgerald Health Education Associates, Inc.,
North Andover, MAFamily Nurse Practitioner,
Greater Lawrence (MA) Family Health CenterEditorial Board Member
The Nurse Practitioner Journal, The Prescribers Letter, American Nurse Today
Member, Pharmacy and Therapeutics CommitteeNeighborhood Health Plan, Boston, MA
Objectives
• Upon completion of this program, the participant will be able to:
–Discuss the pathophysiology of common thyroid disorders.
– Identify expected laboratory findings in common thyroid disorders including TSH, free T4, total T4, T3, and antithyroid antibodies.
Fitzgerald Health Education Associates, Inc. 2
Fitzgerald Health Education Associates, Inc. 3
• Upon completion of this program, the participant will be able to: (cont.)
–Discuss treatment options for the person with select thyroid disorders including thyroid masses.
Objectives (continued)
Thyroid Disorders
Fitzgerald Health Education Associates, Inc.4
References
• American Association of Clinical Endocrinologist Medical Guidelines for Clinical Practice: Hyperthyroidism and Hypothyroidism, available at https://www.aace.com/publications/guidelines
• American Thyroid Association: Topics Related to Hypothyroidism, available at
http://www.thyroid.org/thyroid-guidelines/hypothyroidism/topics/
5 Fitzgerald Health Education Associates, Inc.
Key Concepts in Thyroid Disease
• The thyroid produces two hormones, thyroxine (T4) and triiodothyronine (T3). These hormones act as cellular energy release catalysts and influence the function and health of every cell in the body.
6 Fitzgerald Health Education Associates, Inc.
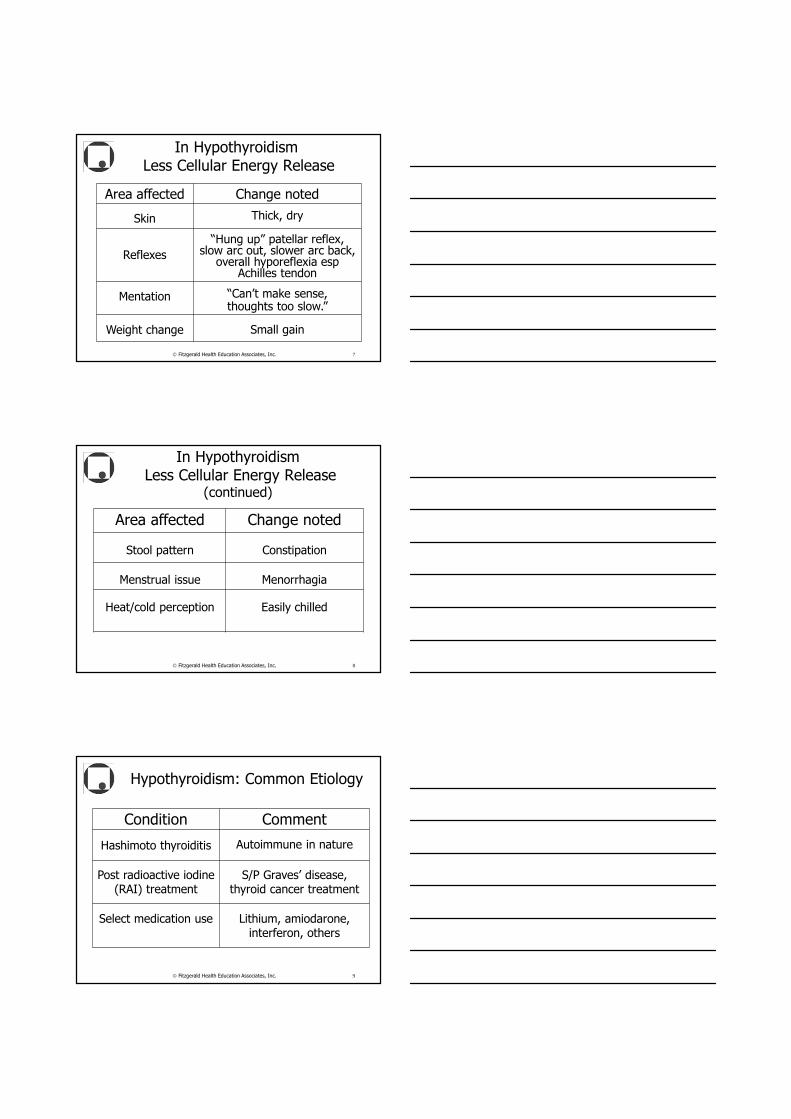
In HypothyroidismLess Cellular Energy Release
Area affected Change noted
Skin Thick, dry
Reflexes
“Hung up” patellar reflex, slow arc out, slower arc back,
overall hyporeflexia esp Achilles tendon
Mentation “Can’t make sense, thoughts too slow.”
Weight change Small gain
7 Fitzgerald Health Education Associates, Inc.
In HypothyroidismLess Cellular Energy Release
(continued)
Area affected Change noted
Stool pattern Constipation
Menstrual issue Menorrhagia
Heat/cold perception Easily chilled
8 Fitzgerald Health Education Associates, Inc.
Hypothyroidism: Common Etiology
Condition Comment
Hashimoto thyroiditis Autoimmune in nature
Post radioactive iodine (RAI) treatment
S/P Graves’ disease, thyroid cancer treatment
Select medication use Lithium, amiodarone, interferon, others
9 Fitzgerald Health Education Associates, Inc.
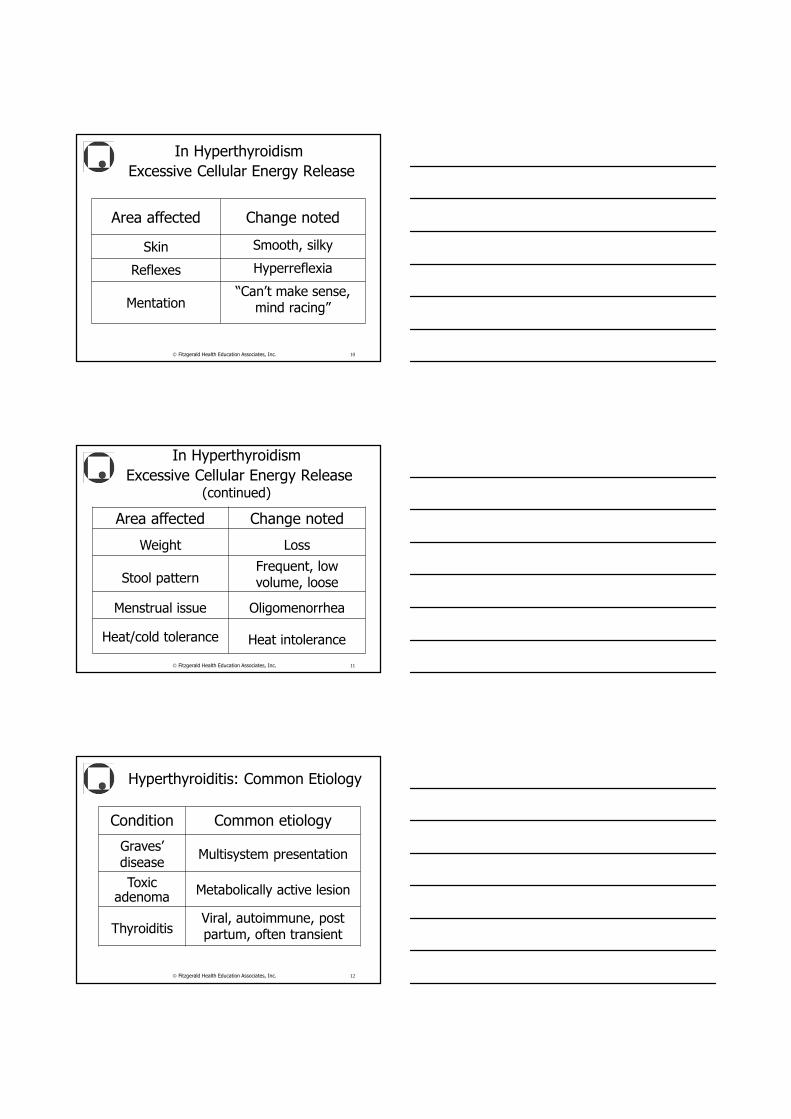
In Hyperthyroidism
Excessive Cellular Energy Release
Area affected Change noted
Skin Smooth, silky
Reflexes Hyperreflexia
Mentation“Can’t make sense,
mind racing”
10 Fitzgerald Health Education Associates, Inc.
In Hyperthyroidism
Excessive Cellular Energy Release (continued)
Area affected Change noted
Weight Loss
Stool patternFrequent, low volume, loose
Menstrual issue Oligomenorrhea
Heat/cold tolerance Heat intolerance
11 Fitzgerald Health Education Associates, Inc.
Hyperthyroiditis: Common Etiology
Condition Common etiology
Graves’ disease
Multisystem presentation
Toxic adenoma
Metabolically active lesion
ThyroiditisViral, autoimmune, post partum, often transient
12 Fitzgerald Health Education Associates, Inc.
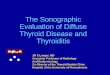
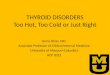
Exophthalmus in Graves' Disease
Fitzgerald Health Education Associates, Inc. 13
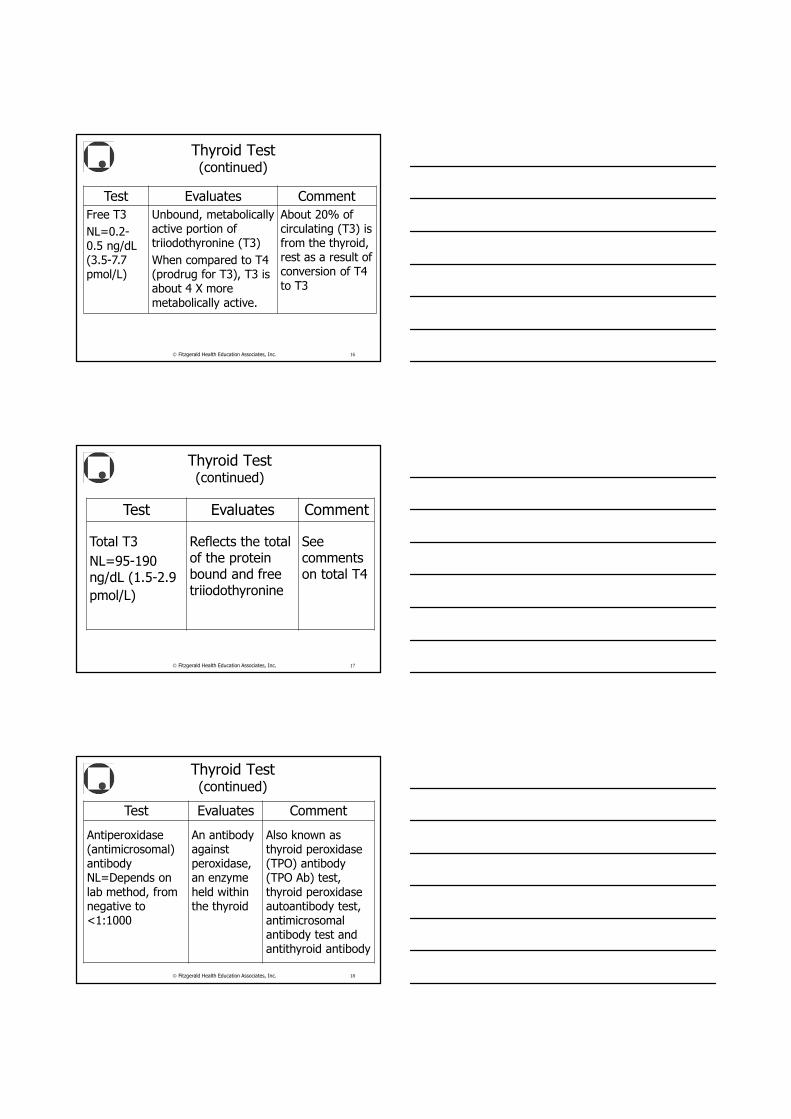
Thyroid Test
Test Evaluates Comment
Thyroid stimulating hormone (TSH)NL=0.4-4.0 mIU/L
True population distribution= 0.5-1.5 mIU/L range with M=1.18 mIU/L
Hypothalamic-pituitary-thyroid axis function, reflects
anterior pituitary lobe’s ability to detect amount of circulating free thyroxine
Per American Thyroid Association, single most reliable test to
diagnose all common forms of hypo- and hyperthyroidism, particularly in the ambulatory setting
14 Fitzgerald Health Education Associates, Inc.
Thyroid Test (continued)
Test Evaluates CommentFree T4 (FT4, free thyroxine)
NL=0.5-1.3 ng/dL (6-16.7 pmol/L )
Unbound, metabolically active portion of thyroxine
About 0.025% of all T4
Total T4 (total thyroxine)
NL=4.5-12.0 mcg/dL (57.9-154.4 nmol/L)
Reflects the total of the protein-bound and free thyroxine
Often altered in the absence of thyroid disease but with the use of select medications (exogenous estrogen {HT, OC}, methadone) and presence of clinical conditions such as pregnancy, chronic hepatitis
15 Fitzgerald Health Education Associates, Inc.
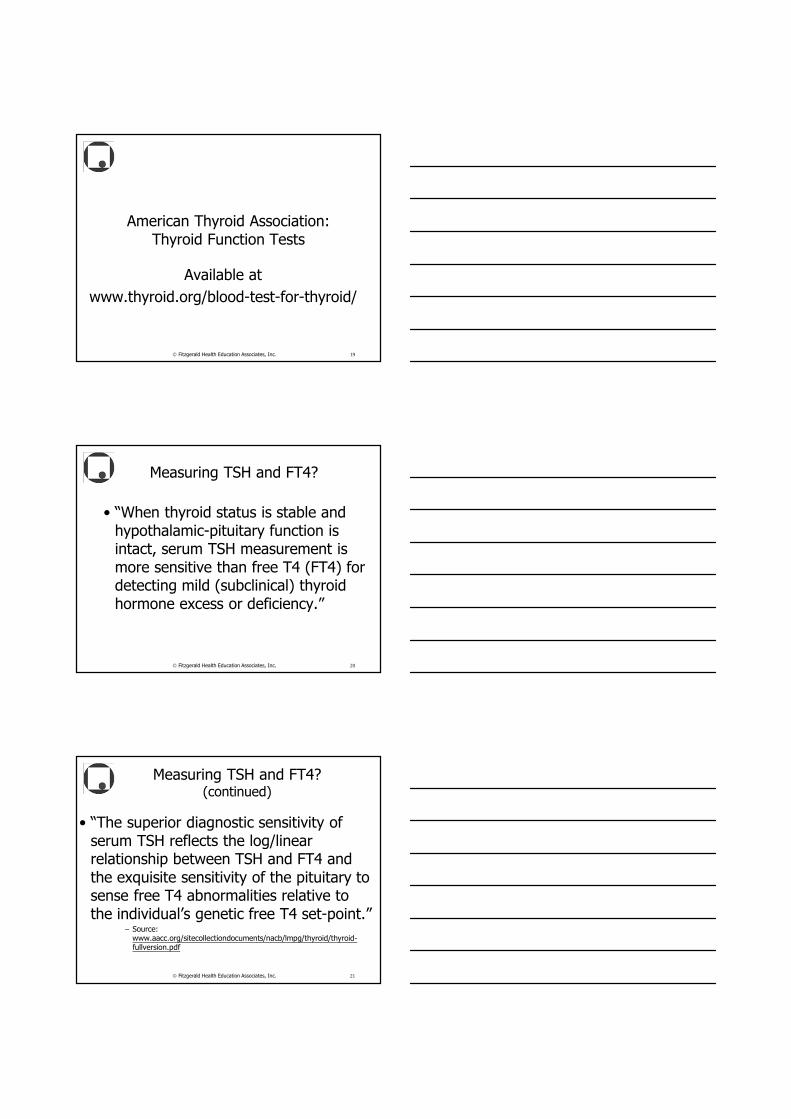
Thyroid Test (continued)
Test Evaluates Comment
Free T3
NL=0.2-0.5 ng/dL (3.5-7.7 pmol/L)
Unbound, metabolically active portion of triiodothyronine (T3)
When compared to T4 (prodrug for T3), T3 is about 4 X more
metabolically active.
About 20% of circulating (T3) is from the thyroid, rest as a result of conversion of T4
to T3
16 Fitzgerald Health Education Associates, Inc.
Thyroid Test (continued)
Test Evaluates Comment
Total T3
NL=95-190 ng/dL (1.5-2.9
pmol/L)
Reflects the total of the protein bound and free triiodothyronine
See comments on total T4
17 Fitzgerald Health Education Associates, Inc.
Thyroid Test (continued)
Test Evaluates Comment
Antiperoxidase (antimicrosomal) antibodyNL=Depends on
lab method, from negative to <1:1000
An antibody against peroxidase, an enzyme
held within the thyroid
Also known as thyroid peroxidase (TPO) antibody (TPO Ab) test,
thyroid peroxidase autoantibody test, antimicrosomal antibody test and antithyroid antibody
18 Fitzgerald Health Education Associates, Inc.
American Thyroid Association: Thyroid Function Tests
Available at
www.thyroid.org/blood-test-for-thyroid/
Fitzgerald Health Education Associates, Inc. 19
Measuring TSH and FT4?
• “When thyroid status is stable and hypothalamic-pituitary function is intact, serum TSH measurement is more sensitive than free T4 (FT4) for detecting mild (subclinical) thyroid hormone excess or deficiency.”
Fitzgerald Health Education Associates, Inc. 20
Measuring TSH and FT4? (continued)
• “The superior diagnostic sensitivity of serum TSH reflects the log/linear relationship between TSH and FT4 and the exquisite sensitivity of the pituitary to sense free T4 abnormalities relative to the individual’s genetic free T4 set-point.”
– Source: www.aacc.org/sitecollectiondocuments/nacb/lmpg/thyroid/thyroid-fullversion.pdf
Fitzgerald Health Education Associates, Inc. 21
Measuring TSH and FT4? (continued)
• “Serum FT4 measurement is a more reliable indicator of thyroid status than TSH when thyroid status is unstable, such as during the first 2-3 months of treatment for hypo- or hyperthyroidism.”
– Source: www.aacc.org/sitecollectiondocuments/nacb/lmpg/thyroid/thyroid-fullversion.pdf
Fitzgerald Health Education Associates, Inc. 22
True or false?
• TSH levels peak in the evening and are lowest in the afternoon.
• TSH varies with physiologic conditions such as illness, psychiatric disorders and low energy intake.
Fitzgerald Health Education Associates, Inc. 23
Thyroid Test ResultsLow Thyroxine (FT4)=High TSH
• Example–TSH=84 mIU/L (0.4-4.0 mIU/L)
–Free T4=3 pmol/L (10-27 pmol/L)
• Etiology–Untreated hypothyroidism
– Inadequate thyroxine dose
24 Fitzgerald Health Education Associates, Inc.
From Levothyroxine PI
• “Synthetic T4 is identical to that produced in the human thyroid gland. Levothyroxine (T4) sodium has an empirical formula of C15H10I4N NaO4 • H2O, molecular weight of 798.86 g/mol (anhydrous)…” – Source-www.rxabbvie.com/pdf/synthroid.pdf
Fitzgerald Health Education Associates, Inc. 25
From Levothyroxine PI(continued)
• T ½
– In hypothyroid state=9-10 d
– In euthyroid state=7 d
– In hyperthyroid state=3-4 d
• How many T ½ to reach steady state? Eliminate drug from the body?
Fitzgerald Health Education Associates, Inc. 26
Intervention in Hypothyroidism
• Calculating anticipated levothyroxine dose
–1.6 mcg/kg/day in adults
–1.0 mcg/kg/day in elderly
–4.0 mcg/kg/day in children
–=>50% increase during pregnancy
• Increase levothyroxine dose by =>33% as soon as pregnancy is confirmed.
27 Fitzgerald Health Education Associates, Inc.
True or false?
• When calculating the levothyroxine dose for a patient, ideal body weight (IBW) should be used for the person who is obese.
• For the person who is underweight, actual body weight should be used.
Fitzgerald Health Education Associates, Inc. 28
Therapy is usually initiated in patients under the age of 50 years with full replacement.
• For those patients who are older than 50 years, or in younger patients with a history of cardiac disease, a lower initial dosage is indicated, starting with 0.025 to 0.05 mg of levothyroxine daily, with clinical and biochemical reevaluations at 6- to 8-week intervals until the serum TSH concentration is normalized.
Fitzgerald Health Education Associates, Inc. 29
What about desiccated porcine thyroid preparations?
Source: American Thyroid Association Treatment Guidelines for Patients with Hypothyroidism,
available at http://thyroidguidelines.net
Fitzgerald Health Education Associates, Inc. 30
T4/T3 Combinations
• Desiccated thyroid preparations (T4/T3 combination, porcine origin such as Armour® Thyroid, Nature-Throid®, Bio-Throid®, Westhroid®)
–1 grain=60-65 mg thyroid USP=100 mcg levothyroxine
–Thyroid USP 60-120 mg per day for typical adult daily dose
Fitzgerald Health Education Associates, Inc. 31
Per American Thyroid Association (ATA)
• “Biological and synthetic thyroid hormone preparations containing both T4 and T3 are also not currently recommended for therapy since they produce fluctuating and often elevated T3 concentrations, although their use is not necessarily contraindicated.”
Fitzgerald Health Education Associates, Inc. 32
Monitoring Thyroxine Therapy
• TSH
–No sooner than 6-8 (AACE) or 8-12 (ATA) weeks
• Long T ½
• TSH too high
–Dose too low
–Adherence
–Drug interaction
• TSH too low
–Excessive use
–Dose too high
33 Fitzgerald Health Education Associates, Inc.
Thyroid Test ResultsHigh Thyroxine (FT4)=Low TSH
• Example
–TSH<0.15 mIU/L (0.4-4.0 mIU/L)
–Free T4=79 pmol/L (10-27 pmol/L)
• Etiology
–Hyperthyroidism
–Excessive thyroxine dose
34 Fitzgerald Health Education Associates, Inc.
Intervention in Hyperthyroidism at the Time of Diagnosis
• Beta adrenergic antagonist
–B1, B2 blockade if possible
• Propranolol, nadolol
• Antithyroid medication
–PTU, methimazole
• Radioactive iodine (RAI)
–Thyroid ablation
35 Fitzgerald Health Education Associates, Inc.
From PTU PI
• “PTU inhibits synthesis of thyroid hormone by interfering with the incorporation of iodine into thyroglobulin; it also inhibits the formation of iodothyronine. Besides blocking hormone synthesis, it also inhibits the peripheral deiodination of thyroxine to triiodothyronine (liothyronine).”
Fitzgerald Health Education Associates, Inc. 36
FDA Advisory on PTU
• FDA is notifying healthcare professionals of the risk of serious liver injury, including liver failure and death, with the use of propylthiouracil in adult and pediatric patients.
– Source: http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/DrugSafetyInformationforHeathcareProfessionals/ucm162701.htm
Fitzgerald Health Education Associates, Inc. 37
From Methimazole PI
• “Methimazole inhibits synthesis of thyroid hormone by interfering with the incorporation of iodide into tyrosyl. Methimazole also inhibits the formation of iodothyronine.”
Fitzgerald Health Education Associates, Inc. 38
From Methimazole PI(continued)
• There have been rare reports of fulminant hepatitis, hepatic necrosis, encephalopathy, and death. Symptoms suggestive of hepatic dysfunction (anorexia, pruritus, right upper quadrant pain, etc.) should prompt evaluation of liver function.
Fitzgerald Health Education Associates, Inc. 39
Subclinical HypothyroidismElevated TSH, NL Free T4
• Example
–TSH=8.9 mIU/L (0.4-4.0 mIU/L)
–Free T4=15 pmol/L (10-27 pmol/L)
–Antithyroid antibodies=1:1,800 (<1:1,000)
40 Fitzgerald Health Education Associates, Inc.
Per AACE GuidelinesSubclinical Hypothyroidism
• AACE guidelines recommend treatment of patients with TSH>5 mIU/L if the patient has a goiter or if thyroid antibodies are present.
• The presence of symptoms compatible with hypothyroidism, infertility, pregnancy or imminent pregnancy would also favor treatment.
– Source: https://www.aace.com/publications/position-statements
41 Fitzgerald Health Education Associates, Inc.
Samantha, 47 YO Woman
• Last year’s results
–TSH=1.2 mIU/L
• 0.35-4.0 mIU/L
–FT4=14 pmol/L
• 10-27 pmol/L
• This year’s results
–TSH=6.4 mIU/L
–FT4=6 pmol/L
• Long-standing hypothyroidism
• States continues to take her levothyroxine “every day, just like clockwork”
42 Fitzgerald Health Education Associates, Inc.
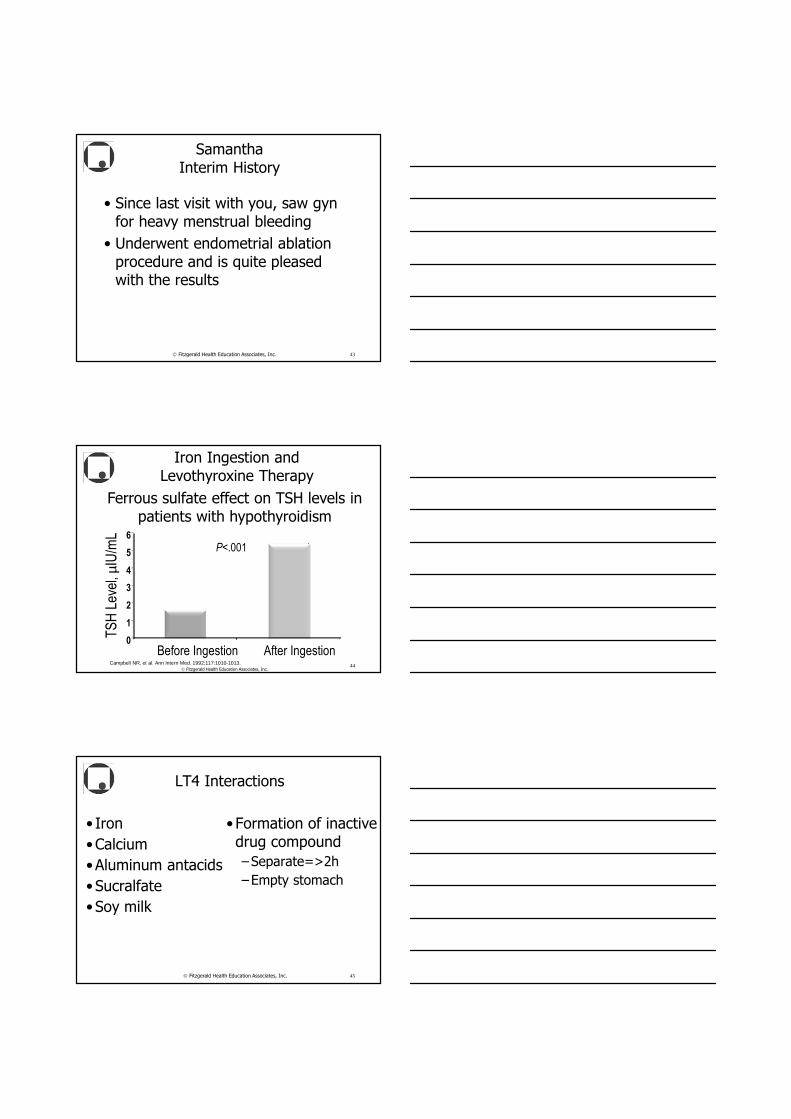
SamanthaInterim History
• Since last visit with you, saw gyn for heavy menstrual bleeding
• Underwent endometrial ablation procedure and is quite pleased with the results
43 Fitzgerald Health Education Associates, Inc.
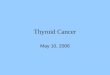
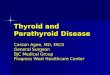
Iron Ingestion and Levothyroxine Therapy
Campbell NR, et al. Ann Intern Med. 1992;117:1010-1013.
Ferrous sulfate effect on TSH levels in patients with hypothyroidism
P<.001
0
1
2
3
4
5
6
TS
H L
evel
, µI
U/m
L
Before Ingestion After Ingestion44
Fitzgerald Health Education Associates, Inc.
LT4 Interactions
• Iron
•Calcium
•Aluminum antacids
•Sucralfate
•Soy milk
• Formation of inactive drug compound
–Separate=>2h
–Empty stomach
45 Fitzgerald Health Education Associates, Inc.
Medications Increasing Metabolism of Thyroid Hormone
• Phenytoin
• Phenobarbital
• Carbamazepine
• Rifampin
46 Fitzgerald Health Education Associates, Inc.
NTI with Many Drug-drug, Drug-nutrient Interactions
• Take your levothyroxine
–Always at the same time of day
–Empty stomach, =>½ h before or =>2 h after meal
–Separate from other meds including OTC, minerals, vitamins by =>2 h
47 Fitzgerald Health Education Associates, Inc.
Generic or brand?Per AACE Statement
• "Patients should be maintained on the same brand name levothyroxine product. If the brand of levothyroxine medication is changed, either from one brand to another brand, from a brand to a generic product, or from a generic product to another generic product, patients should be retested by measuring serum TSH in six (6) weeks, and the drug reiterated as needed.
48 Fitzgerald Health Education Associates, Inc.
Generic or brand?Per AACE Statement
(continued)
• Since small changes in levothyroxine administration can cause significant changes in TSH serum concentrations, precise and accurate TSH control is necessary to avoid potential adverse iatrogenic effects.”– Source: http://dig.pharm.uic.edu/faq/levothyroxine.aspx
49 Fitzgerald Health Education Associates, Inc.
Continued Fatigue
• With NL TSH and free T4
–Consider checking T3
• T4
–~40% converted in peripheral tissue to T3
50 Fitzgerald Health Education Associates, Inc.
Should we also give T3?
• Triiodothyronine (T3) –About 4 X as active
as T4
–Can be important to brain function
51 Fitzgerald Health Education Associates, Inc.
T4 and Liothyronine Sodium (Cytomel®)?
• Add to T4?
– Liothyronine sodium, LT3 (Cytomel®) usual dose=12.5 mcg
• Short T ½
• Usual daily dose 25-75 mcg per day
–Reduce T4 dose by 50 mcg
• Inconclusive study in effectiveness but anecdotal, patient-by-patient reports
52 Fitzgerald Health Education Associates, Inc.
T3 Replacement Per ATA
• “After taking a tablet of Cytomel® there are very high levels of T3 for a short time, and then the levels fall off very rapidly. This means that T3 has to be taken several times each day, and even doing this does not smooth out the T3 levels properly.”– Source:
http://www.thyroid.org/patients/patient_brochures/hormonetreatment.html
Fitzgerald Health Education Associates, Inc. 53
Fitzgerald Health Education Associates, Inc. 54
Sonia35-year-old Woman
• Afebrile
• Pharynx and TM benign
• Hyperreflexia
• Tender, slightly enlarged thyroid
Fitzgerald Health Education Associates, Inc.55
Sonia describes where her throat and ears hurt.
Fitzgerald Health Education Associates, Inc.56
Sonia35-year-old Woman
(continued)
• TSH<0.15 mIU/L (0.15–4.0)
• Free T4=33 pmol/L (10–27)
• ESR=66 mm/hr (<15 mm/hr)
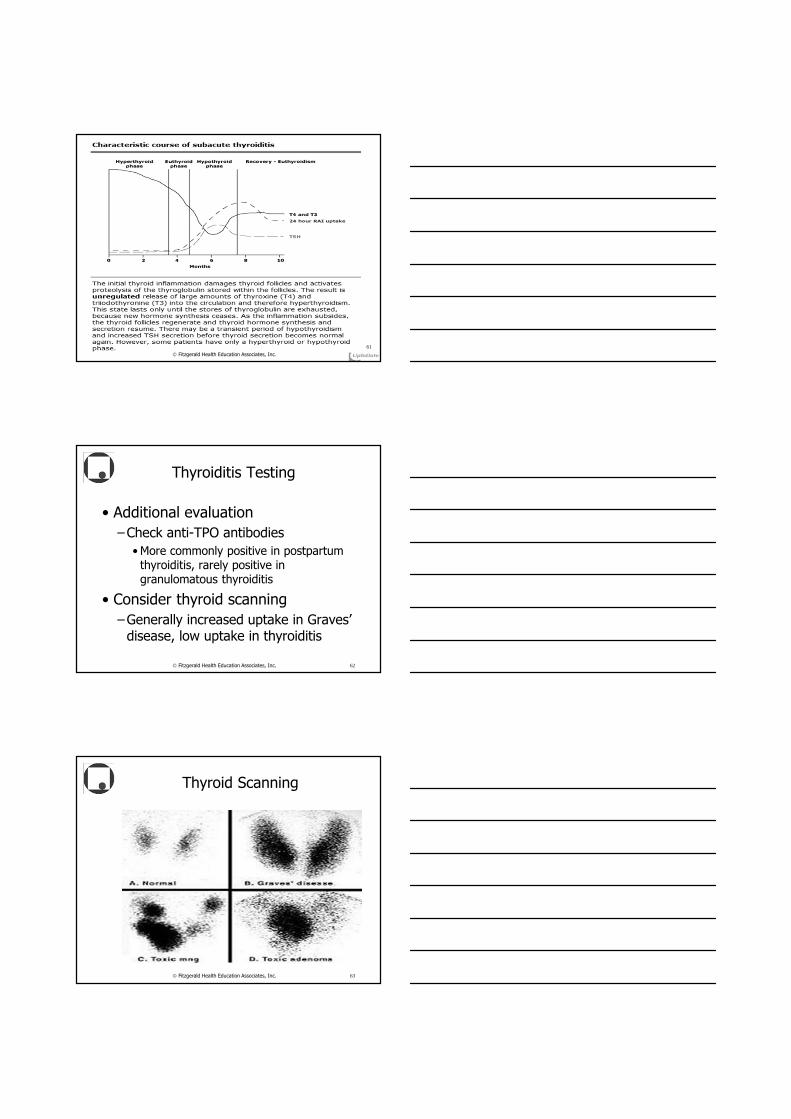
Thyroiditis: Subacute (Granulomatous) Thyroiditis
• In hyperthyroid phase
–Neck pain, a tender diffuse goiter, and elevated T4 and/or T3
• Caused by damage to thyroid follicular cells
and breakdown of stored thyroglobulin, leading to unregulated release of thyroxine (T4) and triiodothyronine (T3)
Fitzgerald Health Education Associates, Inc. 57
Thyroiditis: Subacute (Granulomatous) Thyroiditis
(continued)
• Duration of hyperthyroid phase
–Lasts 2–6 weeks until T4 and T3 stores are depleted• Low TSH minimizes thyroid
follicular stimulation
–Hypothyroidism often follows,
usually transient
Fitzgerald Health Education Associates, Inc. 58
Thyroiditis: Subacute (Granulomatous) Thyroiditis
(continued)
• Etiology
–Likely viral infection trigger
• Common report of recent URI symptoms
• Multiple case reports post
Coxsackievirus outbreaks
–Also strong association with HLA-B35
• ?Viral trigger with genetic basis
Fitzgerald Health Education Associates, Inc. 59
Additional More Common Thyroiditis Forms
• Subacute lymphocytic thyroiditis–Most common form of
postpartum thyroiditis
• Often presents with nervousness, poor sleep, painless thyroid, in first year postpartum, most often around month 3 after birth
–Lasts 1–2 months with self-resolution
Fitzgerald Health Education Associates, Inc. 60
Fitzgerald Health Education Associates, Inc.
61
Thyroiditis Testing
• Additional evaluation
–Check anti-TPO antibodies
• More commonly positive in postpartum thyroiditis, rarely positive in granulomatous thyroiditis
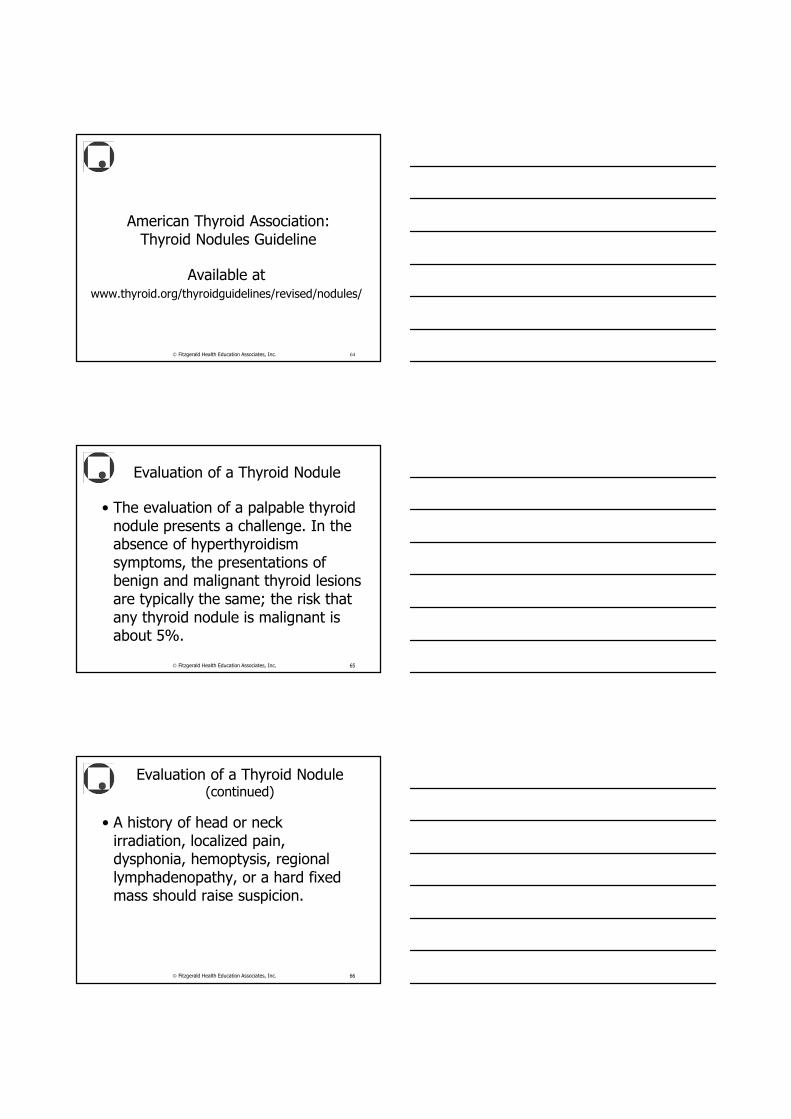
• Consider thyroid scanning
–Generally increased uptake in Graves’ disease, low uptake in thyroiditis
Fitzgerald Health Education Associates, Inc. 62
Thyroid Scanning
Fitzgerald Health Education Associates, Inc. 63
American Thyroid Association: Thyroid Nodules Guideline
Available at www.thyroid.org/thyroidguidelines/revised/nodules/
Fitzgerald Health Education Associates, Inc. 64
Evaluation of a Thyroid Nodule
• The evaluation of a palpable thyroid nodule presents a challenge. In the absence of hyperthyroidism symptoms, the presentations of benign and malignant thyroid lesions are typically the same; the risk that any thyroid nodule is malignant is about 5%.
Fitzgerald Health Education Associates, Inc. 65
Evaluation of a Thyroid Nodule (continued)
• A history of head or neck irradiation, localized pain, dysphonia, hemoptysis, regional lymphadenopathy, or a hard fixed mass should raise suspicion.
Fitzgerald Health Education Associates, Inc. 66
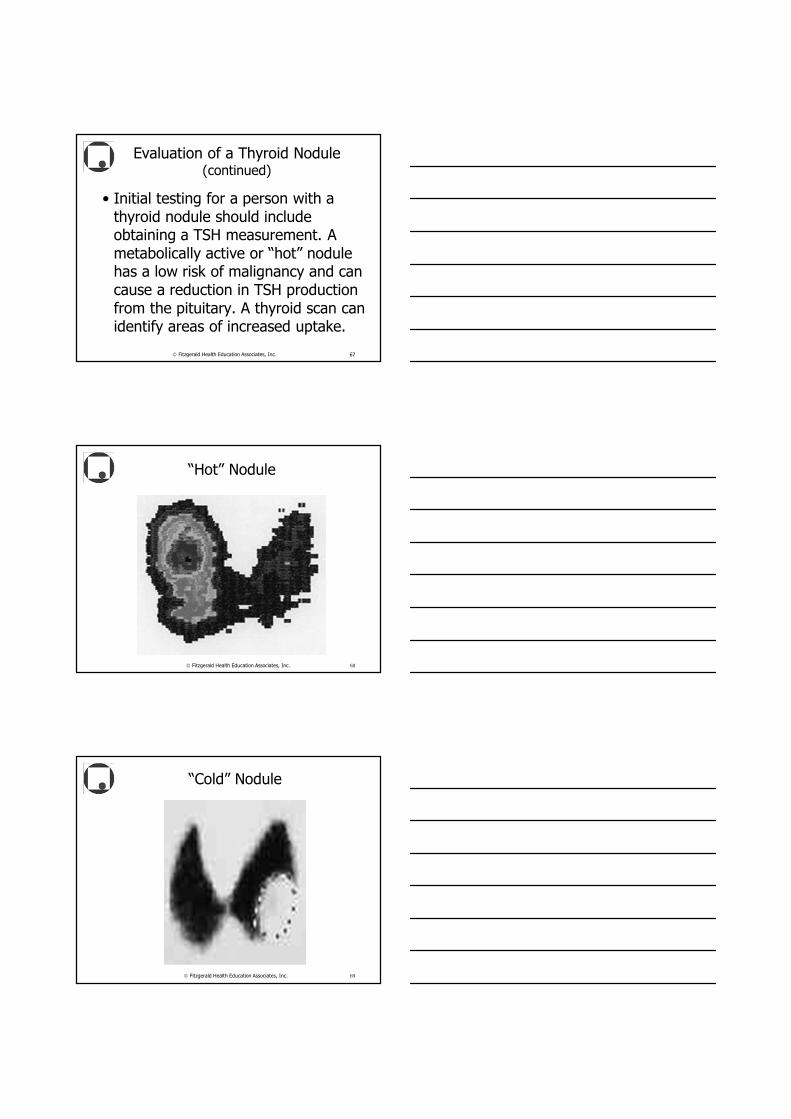
Evaluation of a Thyroid Nodule (continued)
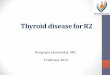
• Initial testing for a person with a thyroid nodule should include obtaining a TSH measurement. A metabolically active or “hot” nodule has a low risk of malignancy and can cause a reduction in TSH production from the pituitary. A thyroid scan can identify areas of increased uptake.
Fitzgerald Health Education Associates, Inc. 67
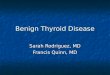
“Hot” Nodule
Fitzgerald Health Education Associates, Inc. 68
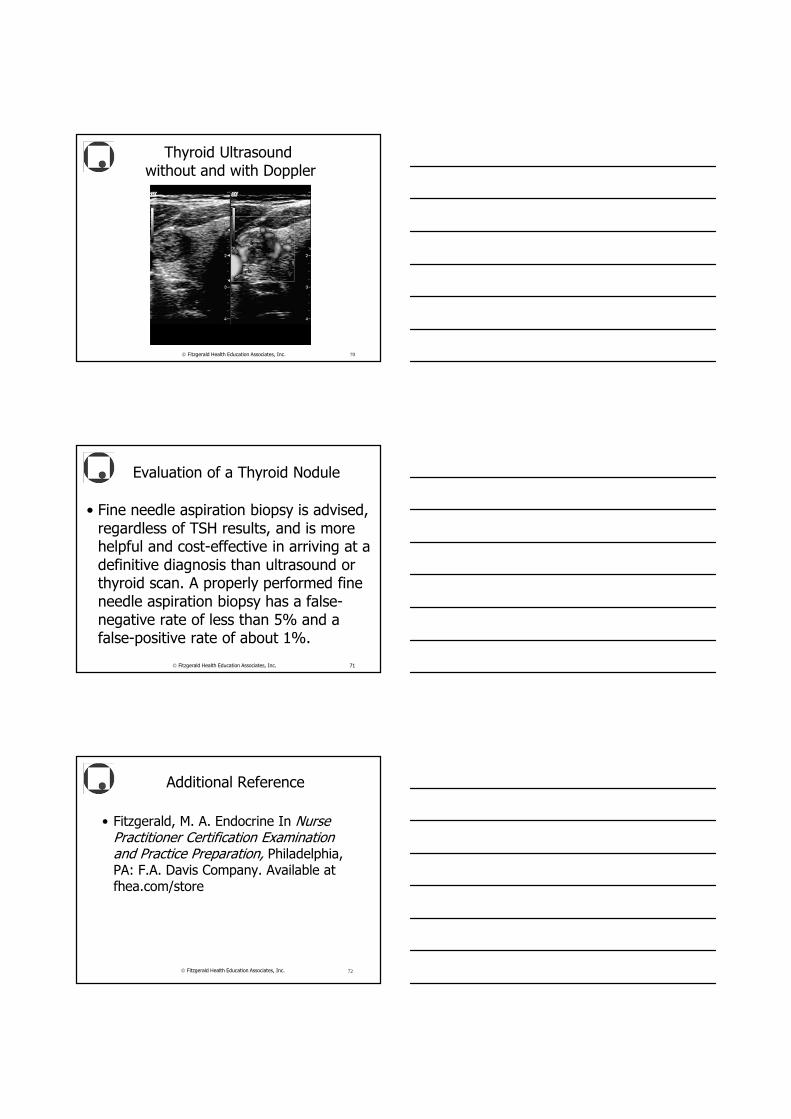
“Cold” Nodule
Fitzgerald Health Education Associates, Inc. 69
Thyroid Ultrasoundwithout and with Doppler
Fitzgerald Health Education Associates, Inc. 70
Evaluation of a Thyroid Nodule
• Fine needle aspiration biopsy is advised, regardless of TSH results, and is more helpful and cost-effective in arriving at a definitive diagnosis than ultrasound or thyroid scan. A properly performed fine needle aspiration biopsy has a false-negative rate of less than 5% and a false-positive rate of about 1%.
Fitzgerald Health Education Associates, Inc. 71
• Fitzgerald, M. A. Endocrine In Nurse Practitioner Certification Examination and Practice Preparation, Philadelphia, PA: F.A. Davis Company. Available at fhea.com/store
Fitzgerald Health Education Associates, Inc. 72
Additional Reference
End of Presentation
Thank you for your time and attention.
Margaret A. Fitzgerald,
DNP, FNP-BC, NP-C, FAANP, CSP, FAAN, DCC
www.fhea.com, e-mail: [email protected]
Fitzgerald Health Education Associates, Inc. 73
Fitzgerald Health Education Associates, Inc. 74
All websites listed active at the time of publication.