Embed Size (px)
Citation preview

Thyroid Disease During Pregnancy: What’s New in 2017?
James V. Hennessey M.D. Associate Professor of Medicine
Harvard Medical School

I have NO disclosures in regard to this presentation

Case 1 • 32 year old lawyer reads online that mild
hypothyroidism in pregnancy may have an impact on a child’s intellectual capacity.
• Asks her PCP to check her TFTs 10 weeks after her last menstrual period.
• TSH 0.22 uU/ml (0.4- 4.2) • Repeat TSH 0.15
– FT4 1.2 ng/dL (0.93 - 1.7) – TT3 230 ng/dL (80 – 200)

ARS Question 1 • Which of the following statements are
consistent with this clinical presentation?
1. This patient is likely in her 1st trimester.
2. This TSH level diagnoses hyperthyroidism.
3. A normal FT4 rules out hyperthyroidism.
4. This TT3 level diagnoses hyperthyroidism.

Thyroid Disease in Pregnancy: Impact
• All pregnancies in Denmark: 1997-2008 – Live births (n = 732,533) – Spontaneous abortions (n = 112,486) – Stillbirth (n = 2,937)
• Correlation with information on maternal: – Hypothyroidism – Hyperthyroidism – Diabetes
Andersen SL & Laurberg Clin Endo 2016 85(6):962-970

Pregnancy Outcomes
• Group 1: n = 4,951 hypothyroidism – Dx Pre-Pregnancy
• Group 2: n = 2,855 hypothyroidism – Dx within 2 years of post pregnancy
• Hyperthyroidism or DM (n = 15,841) – Dx before or within 2 years after pregnancy
• Non-exposed group (n = 824,310)
Andersen SL & Laurberg Clin Endo 2016 85(6):962-970

Freq
uenc
y (%
)
Control
* p<0.001
Andersen SL & Laurberg Clin Endo 2016 85(6):962-970

Freq
uenc
y (%
)
Control
* p<0.001
Andersen SL & Laurberg Clin Endo 2016 85(6):962-970

ATA Guidelines 2017 Recommendation 37
• When a suppressed serum TSH is detected in the first trimester (TSH less than the reference range), a medical history, PE, maternal FT4 or TT4 should be obtained.
• TSH receptor antibodies (TRAb) +/- TT3 may help in diagnosis and determination of etiology of the thyrotoxicosis.
Alexander EK et al. 2017 Thyroid doi: 10.1089/thy.2016.0457

Mandel SJ et al. 2005 Thyroid 15:44-53
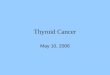
Maternal Thyroid Function: Pregnancy

TSH in 6671 Healthy Pregnant Danes TS
H m
UlL
Weeks of gestation
Laurberg P et al 2016 JCEM 101(6):2484-92

Laurberg P et al 2016 JCEM 101(6):2484-92
“Upper Normal”

Laurberg P et al 2016 JCEM 101(6):2484-92
“Lower Normal”

Trimester-Specific TSH Ranges
Negro & Stagnaro-Green BMJ 349 g4929.2014

ATA Pregnancy Guidelines 2017 Recommendation 1 A. When possible, use trimester-specific TSH ranges, defined by local population data representative of a healthcare providers practice. • Determinations should only include pregnant
women without thyroid disease, optimal iodine intake and negative TPO ab status.
Strong Recommendation, Moderate quality evidence
Alexander EK et al. 2017 Thyroid doi: 10.1089/thy.2016.0457

TSH and Miscarriage Risk
• 55,501 individuals received 1st LT4 Rx – 2001-2009 in UK General Practice Database
• 7978 women of childbearing age (18-45 yrs.) • 1031 with > 6 month LT4 Rx pre-conception • Main outcomes measured:
– TSH – Miscarriage/ Delivery Status
Taylor PN et al. JCEM 2014 99(10):3895-902

LT4 Rx Results
• 46% of LT4 treated patients 18-45 TSH > 2.5 • Among pregnant women:
– 62.8% had 1st Trimester TSH > 2.5 mIu/L • 29.1% had TSH > 4.5 mIu/L • 7.41% had TSH > 10 mIu/L
– Only 37.1% had TSH 0.2-2.5 as recommended – 6.5% had TSH <0.2
Taylor PN et al. JCEM 2014 99(10):3895-902

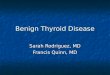
Odds of Miscarriage by 1st Trim TSH
* *
* *
Odd
s of a
Mis
carr
iage
Taylor PN et al. JCEM 2014 99(10):3895-902

Hypothyroidism Diagnosis Timing H
azar
d R
atio
Dx Pre-pregnancy Dx Post-pregnancy
* *
* *
Andersen SL & Laurberg Clin Endo 2016 85(6):962-970

Conclusions
• Increased risk of SA when hypothyroidism diagnosed prior to pregnancy. – Likely due to undertreated hypothyroidism – Not seen when hypothyroidism diagnosed after
the pregnancy when antibodies common bond. • Stillbirth association with disease diagnosed
after pregnancy most consistent with undetected maternal disease in pregnancy?
Andersen SL & Laurberg Clin Endo 2016 85(6):962-970

ATA Pregnancy Guidelines 2017 Recommendation 1 • B. When this is not feasible, reference ranges
obtained from similar patient populations and performed using similar TSH assays can be substituted.
• C. If internal or transferable reference ranges are not available, the upper limit of TSH in non-pregnant patients (≈ 4.0 mU/l) should be used. Strong recommendation, moderate quality evidence
Alexander EK et al. 2017 Thyroid doi: 10.1089/thy.2016.0457

ATA Pregnancy Guidelines 2017 Recommendation 2 • The accuracy of serum Free T4 measurement
by the indirect analog immunoassays is influenced by pregnancy and also varies significantly by manufacturer.
• If measured in pregnant women, assay method specific and trimester-specific pregnancy reference ranges should be applied.
Strong recommendation, Moderate quality evidence
Alexander EK et al. 2017 Thyroid doi: 10.1089/thy.2016.0457

ATA Pregnancy Guidelines 2017
Recommendation 3 • In lieu of measuring FT4, total T4 measurement
(with a pregnancy adjusted reference range), is a highly reliable means of estimating hormone concentration during pregnancy.
• Accurate estimation of the free T4 concentration can be done by calculating a free thyroxine index. Strong recommendation, Moderate quality evidence
Alexander EK et al. 2017 Thyroid doi: 10.1089/thy.2016.0457

• Recommendation 3 – Optimal method to assess FT4 is in dialysate or
ultrafiltrate of serum by LC/MS/MS • Level A – USPSTF
• Recommendation 4 – If LC/MS/MS not available, estimate FT4 by
whatever method available (limitations) – TSH more accurate indication of thyroid
status than any of the alternatives. • Level A - USPSTF
ATA Pregnancy Guidelines 2011
Brent GA ATA Guideline Symposium ENDO 2016

Case 1 Continued
• Follow up TFT’s @ 14 weeks • TSH 0.62 uU/ml (0.4- 4.2) • FT4 1.1 ng/dL (0.93 - 1.7) • TT3 232 ng/dL (80 – 200)
– FT3I wnl • Probable Diagnosis:
– Gestational Transient Thyrotoxicosis or – Hyperemesis gravidarum

ATA Guidelines 2017 Recommendation 39
• The appropriate management of abnormal maternal thyroid function tests attributable to Gestational Transient Thyrotoxicosis and/or hyperemesis gravidarum includes supportive therapy, management of dehydration, and hospitalization if needed.
• Antithyroid drugs are not recommended, but beta-blockers may be used.
Strong recommendation, Moderate quality evidence
Alexander EK et al. 2017 Thyroid doi: 10.1089/thy.2016.0457

Case 2
• A 28 year old woman consults with her PCP prior to starting her family.
• PMHx: S/P total thyroidectomy @ 14 years – Stage 1 (T1a[0.5 cm], N0, Mx) FV-PTC (NI) – Post operative hypothyroidism (LT4 100 mcg/d)
• Most recent neck US negative – TSH 4.8 – Tg < 0.1 ng/Ml – Tg-ab < 20 IU/mL

ARS Question 2 What recommendations would you make to this patient as she prepares for pregnancy?
1. Restaging of the thyroid cancer is the priority.
2. Increase the LT4 dose to 125/d, recheck TSH prior to encouraging this patient to conceive.
3. Once cleared, no dose adjustments expected.
4. Stop LT4 as it not recommended in pregnancy.

ATA Pregnancy Guidelines 2017 Recommendation 65
• ATA 2015 DTC Excellent Response to treatment – No clinical, biochemical (LT4 Tg <0.2, Stim Tg <1),
nor structural evidence of disease. • US and Tg monitoring during pregnancy not
required.
Strong recommendation, Moderate quality evidence
Alexander EK et al. 2017 Thyroid doi: 10.1089/thy.2016.0457

ATA Guidelines 2017 Recommendation 93 • All patients seeking pregnancy, or newly
pregnant should undergo clinical evaluation. • If any of the following risk factors are
identified, testing TSH is recommended.
Alexander EK et al. 2017 Thyroid doi: 10.1089/thy.2016.0457

ATA Guidelines 2017 • Women at high risk of thyroid dysfunction
– Hx or Sx of hyper or hypothyroidism – Thyroid antibody positivity or goiter – Hx H/N irradiation or prior thyroid surgery – Age > 30 years – Personal or FHx of DM 1 or other AI disease – Hx miscarriage, preterm delivery or infertility – Multiple prior pregnancies (> 2) – Morbid obesity (BMI > 40 kg/m2) – Amiodarone, Lithium or IV Contrast exposure – Residence in area of moderate to severe iodine deficiency
Alexander EK et al. 2017 Thyroid doi: 10.1089/thy.2016.0457

SCHypo & Thyroid Autoimmunity • 3315 low risk women followed prospectively • Initial TFTs drawn at 4-8 weeks gestation • Clinical Classification based on TSH results:
– Euthyroid (0.29 < TSH <2.5) – Isolated SCHypo
• SCHypo 1 (> 2.5 TSH <5.22 mIu/L) • SCHypo 2 (5.22 < TSH < 10 mIu/L)
– Isolated AITD (TPO &/or Tg-ab +) – SCHypo + AITD
Liu H et al. 2014 Thyroid 24(11):1642-1649

Miscarriage (Preg. loss < 20 weeks)
Liu H et al. 2014 Thyroid 24(11):1642-1649
Freq
uenc
y of
Occ
urre
nce
**
*
% % % % % % Wee
ks
*
*
* * p < 0.05 vs. EuT
** ** ** **
** p < 0.05 vs. EuT W
eeks
Wee
ks
Wee
ks
Wee
ks
Wee
ks

LT4 & Outcomes in SCHypo
• Pregnant women with SC Hypothyroidism – TSH < 10 > 2.5 first trimester, > 3.0 2nd or 3rd
• Pregnancy loss or adverse outcomes assessed • Divided by treatment:
– Group A received LT4 treatment – Group B did NOT receive LT4
• 82 in Group A, 284 in Group B
Maraka S et al. 2016 Thyroid 25(7):980-986

LT4 Rx Impact on Outcomes • Group A
– Higher BMI* – Higher TSH* – * = p < 0.05
• Limitations – Retrospective – No randomization – Selection bias possible
• Higher risk got LT4
Maraka S et al. 2016 Thyroid 25(7):980-986
Perc
enta
ge *
*
*

ATA Pregnancy Guidelines 2017 Recommendation 3 • Subclinical hypothyroidism in pregnancy should
be approached as follows: A. Levothyroxine therapy is recommended for:
– TPO ab positive women with TSH greater than the reference range (See recommendation 1)
Strong recommendation, Moderate quality evidence – TPO ab negative with a TSH greater than 10.0 mIu/L.
Strong recommendation, Low quality evidence
Alexander EK et al. 2017 Thyroid doi: 10.1089/thy.2016.0457

Euthyroid AITD & LT4 Outcomes (1st Trimester TSH < 2.5)
• 8530 women in 1st Trimester screened – TSH and Antithyroid antibodies
• Group A: 198 ATA+ with LT4 prospective Rx – LT4 Rx adjustments for TSH > 3.0 or <0.5
• Group B: 195 ATA+ without routine LT4 Rx – LT4 Rx if TSH >3.0 in 2nd or 3rd trimester
• Group C: 197 euthyroid ATA(-) women • Outcomes: Miscarriage, preterm delivery
Negro R et al. JCEM 2016 101(10):3685-3690

LT4 Rx in AITD in Pregnancy T
SH (
mIU
/L)
*
*p < 0.05 vs. A&B
* *
Rou
tine
LT4
Rx
PRN
LT
4 R
x
Negro R et al. JCEM 2016 101(10):3685-3690

LT4 Rx in AITD in Pregnancy Pe
rcen
tage
*
*p = 0.01 R
outin
e LT
4 R
x
PRN
LT
4 R
x
Negro R et al. JCEM 2016 101(10):3685-3690

ATA Pregnancy Guidelines 2017
Recommendation 3 B. Levothyroxine therapy may be considered for:
– TPO ab positive women with TSH concentration > 2.5 mIu/L and the upper limit of the reference range.
Weak recommendation, Low quality evidence
– TPO ab negative women with TSH concentrations greater than the reference range though < 10 mIu/L.
Weak recommendation, Low quality evidence
Alexander EK et al. 2017 Thyroid doi: 10.1089/thy.2016.0457

ATA Pregnancy Guidelines 2017
Recommendation 3 C. Levothyroxine is not recommended for:
– TPO ab negative women with normal TSH
• TSH within the pregnancy specific reference range, or • TSH < 4.0 mIu/L if unavailable
Strong recommendation, Good quality evidence
Alexander EK et al. 2017 Thyroid doi: 10.1089/thy.2016.0457

ATA pregnancy Guidelines 2017
• TPO ab positive – TSH > reference range LT4 recommended – TSH > 2.5 < upper reference LT4 considered – TSH < 2.5 mIu/L NO LT4
• TPO ab negative – TSH > 10 mIU/L LT4 recommended – TSH > reference < 10 LT4 considered – TSH in reference range NO LT4
Alexander EK et al. 2017 Thyroid doi: 10.1089/thy.2016.0457

Case 3
• 28 year old woman diagnosed with Graves’ disease, now euthyroid with MMI 30 mg/day after 9 months of treatment.
• Reports last menstrual period 8 weeks previously, morning sickness and a home pregnancy test is positive.
• Physical exam includes active Graves’ ophthalmopathy, tachycardia and TSH <0.1

ARS Question 3 What do you recommend to this patient who is likely in the first trimester of pregnancy?
1. She is well controlled with MMI, no concerns are present nor would MMI adjustments be necessary. 2. She should increase her MMI dose to assure a normal TSH during the first trimester. 3. Her MMI will be continued and the dose will need to be decreased as the pregnancy progresses. 4. Stop the MMI, consider observation or switch to PTU during the first trimester.

Hyperthyroidism in Pregnancy • Diagnosis: (Recommendation 78)
– TSH – TT4 and TT3 (adjust to 1.5 X normal) or – Trimester specific FT4 and TT3
Strong recommendation, low evidence • Pregnancy physiology TFT changes! (Rec. 79)
• hCG-mediated TSH suppression not to be treated
Strong recommendation, low evidence
Ross DS, et al. Thyroid. 2016;26(10):1343-1421.

Hyperthyroidism in Pregnancy • Diagnosis: (Recommendation 78)
– TSH – TT4 and TT3 (adjust to 1.5 X normal) or – Trimester specific FT4 and TT3 Strong recommendation, low evidence
• TRab levels should be measured when etiology of hyperthyroidism uncertain (Recomm. 92) Strong recommendation, low evidence Ross DS, et al. Thyroid. 2016;26(10):1343-1421.

Freq
uenc
y (%
)
Control
* p<0.001
Andersen SL & Laurberg Clin Endo 2016 85(6):962-970

Consequences of ATD Treatment Actual number of women exposed to ATDs during
pregnancy unknown (This is an Overestimate)
% o
f Exp
osed
repo
rted
Clementi et al. 2010 JCEM 95(11):E337-E341

Specific Birth Defect Associations • MMI/CMZ: (Combined OR 21.8 (13.4-35.4)
– Aplasia Cutis, Eye and Circulatory abnormalities – Choanal & Esophageal Atresia – Omphalocele, Omphalo-mesenteric duct anomalies
• PTU – Face/Neck sinus, fistulae, cysts
• Both – Urinary Tract
Andersen & Laurberg 2013 JCEM 98(11):4373-81

Hyperthyroidism Before Pregnancy • Risks of hyperthyroid state and treatment
on maternal and fetal outcomes. (Rec 81) – Postpone pregnancy until euthyroid Strong recommendation, low evidence
• GD requiring higher (> 10 mg/d MMI) dose ATD should consider definitive therapy prior to conception. (Rec 82)
Weak recommendation, low evidence
Ross DS, et al. Thyroid. 2016;26(10):1343-1421.

Recommendation 84
• We suggest that women who are treated with ATD and who may potentially become pregnant should be instructed to perform a pregnancy test within the first days after a missed or unusually light menstrual period.
Weak recommendation, Low-quality evidence
Ross DS, et al. Thyroid. 2016;26(10):1343-1421.

Recommendation 85 • We suggest that a woman who tests positive
for pregnancy contact the physician responsible for the Anti Thyroid Drug therapy within 24 hours to discuss future treatment options.
Weak recommendation, low-quality evidence
Ross DS, et al. Thyroid. 2016;26(10):1343-1421.

Recommendation 83 • Women with hyperthyroidism due to GD well
controlled on MMI have options: – A. Consider definitive treatment before conception – B. Switch to PTU before conception – C. Switch to PTU when pregnancy confirmed – D. Selected patients may be withdrawn from ATD
therapy when pregnancy diagnosed. • If withdrawn, TFTs weekly then monthly if acceptable
Weak recommendation, low quality evidence
Ross DS, et al. Thyroid. 2016;26(10):1343-1421.

A. Definitive Rx before pregnancy
• Advantage: – Free of worry about Anti Thyroid Drugs – Allows treatment of hypothyroidism with LT4 – Substantial experience with LT4 in pregnancy
• Disadvantage: – Delays pregnancy until euthyroid on LT4 – Potential complications of 131-I or surgery
Ross DS, et al. Thyroid. 2016;26(10):1343-1421.

B. MMI to PTU Pre-Pregnancy • Advantages:
– Avoids early exposure to MMI • 2-4% incidence of birth defects with MMI
• Disadvantage: – PTU exposure early in pregnancy
• 2-3% incidence of less severe birth defects • 1:10,000 risk of maternal hepatic failure
• May be considered in younger women, with regular menses expected to conceive within 3 months of PTU exposure.
Ross DS, et al. Thyroid. 2016;26(10):1343-1421.

Switching from MMI to PTU
• Dosage ratio of MMI to PTU of 1:20 is recommended when changing.
• Difference in duration of action considered – MMI longer ½ life than PTU
• Examples: – 15 mg of MMI is roughly 300 mg of PTU – 15 mg MMI 1X/day to 100 mg PTU 3X/day
Ross DS, et al. Thyroid. 2016;26(10):1343-1421.

Recommendation 87 • We suggest that women in early pregnancy
(1st trimester), on MMI who have a high risk of recurrent or worsening hyperthyroidism if ATDs are withdrawn be shifted from MMI to PTU immediately after diagnosing pregnancy.
Weak recommendation, low-quality evidence
Ross DS, et al. Thyroid. 2016;26(10):1343-1421.

C. MMI to PTU After Conception • Requirement:
– Must detect pregnancy VERY early • Period of risk from ATDs Gestational weeks 6-10 • Urine pregnancy tests NOT positive until week 5! • Positive test MUST contact MD in < 24 hours
• Advantage: euthyroidism until conception – Prevents prolonged PTU exposure
• Disadvantage: MMI exposure in early pregnancy • May be preferred in:
– Older women and with delayed conception
Ross DS, et al. Thyroid. 2016;26(10):1343-1421.

Recommendation 88
• Women taking PTU during the first trimester of pregnancy, may be switched to MMI at the beginning of the second trimester, OR they may continue PTU therapy for the remaining part of pregnancy if ATDs are needed.
No recommendation, insufficient evidence
Ross DS, et al. Thyroid. 2016;26(10):1343-1421.

D. Withdraw ATDs after Conception • Requirement:
– Stable euthyroidism, LOW DOSE MMI (5-10 mg/d) – Falling to negative TSH Receptor antibody (Trab)
• Risk of relapse about 10%
• Advantage: – Minimizes exposure to ATDs
• Disadvantages: – Early fetal ATD exposure – Requires close monitoring (Q week to Q month TFTs) – May require reintroduction of PTU (1st) or MMI (2nd-3rd)
Ross DS, et al. Thyroid. 2016;26(10):1343-1421.

Hyperthyroidism First Diagnosed During Pregnancy
• Treatment of GD with ATD (Rec 80) – For overt hyperthyroidism – PTU during the first trimester – MMI started after the first trimester
Strong recommendation, low evidence • Surgery only when medical treatment unsuccessful
or ATDs can not be used. (Rec 90) – Second trimester surgery as required (Rec 91)
Ross DS, et al. Thyroid. 2016;26(10):1343-1421.

Recommendation 89 • Graves’ disease in pregnancy should be
treated with the lowest dose of ATD possible. • Maintain maternal thyroid hormone levels at
or slightly above the reference range for TT4 and TT3 in pregnancy (1.5 X upper normal).
• TSH values should be below normal. • Assess thyroid function monthly Strong recommendation, low-quality evidence
Ross DS, et al. Thyroid. 2016;26(10):1343-1421.

Conclusions
• The physiology of pregnancy may result in abnormalities of thyroid function testing that must be differentiated from hyperthyroidism.
• Subclinical hypothyroidism has adverse impact on pregnancy outcomes and may require Rx.
• Hyperthyroidism during pregnancy has negative impact on outcomes and requires accurate diagnosis and a nuanced approach to Rx.

Thank You for Your Attention