Embed Size (px)
Citation preview

Managing “Anesthesia” in Managing “Anesthesia” in RadiologyRadiology
Local anesthesia to conscious Local anesthesia to conscious sedationsedation
Collan Simmons, B.Sc., M.D.
PGY-5 Anesthesia
(Anisa’s husband)

Warm Up QuestionsWarm Up Questions
What are you typical doses of What are you typical doses of Fentanyl?Fentanyl? Midazolam?Midazolam?
What is the name of the antidote for What is the name of the antidote for benzodiazepines?benzodiazepines?
Maximum dose of lidocaine (/kg)? With Epi?Maximum dose of lidocaine (/kg)? With Epi?

ObjectivesObjectives
Basics of Sedations Basics of Sedations Monitors & SupportMonitors & Support OpioidsOpioids BenzodiazepinesBenzodiazepines
Local AnesthesiaLocal Anesthesia Toxicities & ManagementToxicities & Management

SedationSedation
What you need before you startWhat you need before you start

MonitorsMonitors
Required:Required: Oxygen Saturation/HROxygen Saturation/HR
Tells you about oxygenation (not ventilation)Tells you about oxygenation (not ventilation)
Blood pressureBlood pressure SuggestedSuggested
ECG ECG Respiratory RateRespiratory Rate

Sedation BasicsSedation Basics
IV accessIV access OxygenOxygen
Nasal prongs (Fi02 = 30% max)Nasal prongs (Fi02 = 30% max) Face mask (Fi02 = 50% max)Face mask (Fi02 = 50% max)
Backup EquipmentBackup Equipment IV fluidsIV fluids Self-inflating resuscitation bagSelf-inflating resuscitation bag
Oral/Nasal AirwaysOral/Nasal Airways AntidotesAntidotes

Fasting Guidelines:Fasting Guidelines:
Any procedure that may require IV sedation:Any procedure that may require IV sedation: 8 hours after a meal that includes meat, fried or 8 hours after a meal that includes meat, fried or
fatty foods fatty foods 6 hours after a light meal (such as toast and a clear 6 hours after a light meal (such as toast and a clear
fluid), or after ingestion of infant formula or fluid), or after ingestion of infant formula or nonhuman milk nonhuman milk
4 hours after ingestion of breast milk 4 hours after ingestion of breast milk 2 hours after clear fluids. 2 hours after clear fluids.

Sedative AgentsSedative Agents

Sedation GoalsSedation Goals
AnalgesiaAnalgesia Intra-procedural vs long actingIntra-procedural vs long acting
AnxiolysisAnxiolysis +/-Amnesia+/-Amnesia
Return to baseline shortly after procedureReturn to baseline shortly after procedure

Ideal Properties of Sedative AgentsIdeal Properties of Sedative Agents
TitratableTitratable Fast OnsetFast Onset Short durationShort duration Wide therapeutic indexWide therapeutic index
Minimal Side effectsMinimal Side effects Antidote/Reversal Agent availableAntidote/Reversal Agent available

SedationSedation
Typical Agents UsedTypical Agents Used OpioidsOpioids BenzodiazepinesBenzodiazepines PropofolPropofol

PropofolPropofol
Titratable Titratable Fast OnsetFast Onset Short durationShort duration
AmnesiaAmnesia SedationSedation No analgesiaNo analgesia

PropofolPropofol
NARROWNARROW Therapeutic indexTherapeutic index SedationSedation ApneaApnea Loss of airway reflexesLoss of airway reflexes Loss of consciousnessLoss of consciousness
Hemodynamics:Hemodynamics: Direct myocardial Direct myocardial
depressantdepressant VasodilatorVasodilator}

PropofolPropofol
Prior to usePrior to use Ready for general anesthesiaReady for general anesthesia
A/W controlA/W control Possible ventilationPossible ventilation
Ready for hemodynamic consequencesReady for hemodynamic consequences FluidsFluids Short acting vasoactive agentsShort acting vasoactive agents
= Best left to Anesthesia= Best left to Anesthesia

OpioidsOpioids

OpioidsOpioids
Common DrugsCommon Drugs FentanylFentanyl MorphineMorphine HydromorphoneHydromorphone

OpioidsOpioids
Good CharacteristicsGood Characteristics AnalgesiaAnalgesia
Bad CharacteristicsBad Characteristics Respiratory depressionRespiratory depression PruritusPruritus NauseaNausea

FentanylFentanyl
Synthetic opioidSynthetic opioid Highly lipid soluble Highly lipid soluble Minimal pruritus, nauseaMinimal pruritus, nausea
100X more potent than morphine100X more potent than morphine Fast onsetFast onset No active metabolitesNo active metabolites Clinically effective for approximately 30 Clinically effective for approximately 30
minmin dose dependentdose dependent

FentanylFentanyl
Supplied as:Supplied as: 50 mcg/ml (equivalent in potency to 5 mg morphine)50 mcg/ml (equivalent in potency to 5 mg morphine)
Dosing: (by ideal weight)Dosing: (by ideal weight) Sedation: 0.5 – 1 mcg/kg, titrated to effectSedation: 0.5 – 1 mcg/kg, titrated to effect
50kg Woman: 25 -50 mcg50kg Woman: 25 -50 mcg 80kg Man: 50-100 mcg 80kg Man: 50-100 mcg
Induction of Anesthesia:Induction of Anesthesia: Typical: 1-3 mcg/kgTypical: 1-3 mcg/kg Cardiac: 5-10 mcg/kgCardiac: 5-10 mcg/kg
OnsetOnset Subjective: 1 minSubjective: 1 min Peak effect: 5 minPeak effect: 5 min

FentanylFentanyl
Elimination half lifeElimination half life Surprisingly longSurprisingly long
T ½ = 3.1 - 6.6h T ½ = 3.1 - 6.6h Morphine = 1.7 - 3.3hMorphine = 1.7 - 3.3h
Hepatic eliminationHepatic elimination
Clinical half lifeClinical half life Short because of distribution (highly lipid soluble)Short because of distribution (highly lipid soluble)

Elimination vs. DistributionElimination vs. Distribution Rapid onset:Rapid onset:
IV injection IV injection vessel rich group –(BBB) vessel rich group –(BBB) CNS CNS Termination clinical effect is due toTermination clinical effect is due to
1.1. Washout from brainWashout from brain2.2. Distribution to clinically irrelevant tissues (muscle, fat)Distribution to clinically irrelevant tissues (muscle, fat)
Plasma concentration falls below thresholdPlasma concentration falls below threshold3.3. EliminationElimination
Exceptions to the above:Exceptions to the above: Repeat doses (fill up the inactive tissues)Repeat doses (fill up the inactive tissues) Large dosesLarge doses
Cardiac SurgeryCardiac Surgery InfusionsInfusions
ICUICU

Fentanyl & Organ FailureFentanyl & Organ Failure
Hepatic Hepatic Inactivated by hepatic metabolism Inactivated by hepatic metabolism
dependent on hepatic blood flowdependent on hepatic blood flow elderlyelderly
Reduce dose, but still safeReduce dose, but still safe RenalRenal
Inactive metabolites excreted via kidneysInactive metabolites excreted via kidneys

Side effects:Side effects:
Nausea, Vomiting, Constipation…Nausea, Vomiting, Constipation…

Side effects:Side effects:
Depressed level of consciousnessDepressed level of consciousness Airway reflexesAirway reflexes
Aspiration (Aspiration (fasted)fasted)
Respiratory DepressionRespiratory Depression Dose dependent decrease in respiratory rateDose dependent decrease in respiratory rate
HypoventilationHypoventilation1.1. Hypercarbia Hypercarbia
2.2. HypoxiaHypoxia

Side effects:Side effects:
CardiovascularCardiovascular No direct myocardial depressant effectsNo direct myocardial depressant effects No direct vasodilating effectsNo direct vasodilating effects BUT:BUT:
Does decrease patients sympathetic outflowDoes decrease patients sympathetic outflow Decr HRDecr HR Decr BPDecr BP Decr vascular toneDecr vascular tone

Patients to be WEARY of:Patients to be WEARY of: Prone to respiratory depression, desaturationProne to respiratory depression, desaturation
COPDCOPD Sleep ApneaSleep Apnea ObesityObesity
Hypovolemic/Critically IllHypovolemic/Critically Ill Limited distribution of drug = “sensitive”Limited distribution of drug = “sensitive”
More likely to experience apnea and hypotensionMore likely to experience apnea and hypotension ElderlyElderly
Decreased reserve, hepatic blood flowDecreased reserve, hepatic blood flow Slow “arm-brain” time Slow “arm-brain” time be patient in dosing be patient in dosing

Initial Treatment of (Serious) Initial Treatment of (Serious) Opioid Side EffectsOpioid Side Effects
Respiratory Depression:Respiratory Depression: Airway & BreathingAirway & Breathing
(Oxygen already on)(Oxygen already on) Upgrade to FMUpgrade to FM
Stimulate patient/check resp Stimulate patient/check resp raterate
Adjust upper airway (jaw Adjust upper airway (jaw thrust)thrust)
Look for respiratory effort (?Look for respiratory effort (?obstruction)obstruction)
Oral A/W, Jaw thrustOral A/W, Jaw thrust Bag Mask Ventilation (100% Bag Mask Ventilation (100%
O2)O2) AntidoteAntidote

Naloxone (Narcan)Naloxone (Narcan) Narcotic antagonistNarcotic antagonist Supplied as 0.4 mg in 1 ccSupplied as 0.4 mg in 1 cc Route: IV, SC, IM, (ETT)Route: IV, SC, IM, (ETT) Onset: <2 minOnset: <2 min Dose:Dose:
ER: 0.4mg IV, double every 2-3min until desired LOC/RR ER: 0.4mg IV, double every 2-3min until desired LOC/RR achievedachieved
Reserve for RR = 0. ACUTE REVERSAL OF ANALGESIAReserve for RR = 0. ACUTE REVERSAL OF ANALGESIA Selective reversal: dilute 0.4 mg to total of 10cc = 0.04 mg/ccSelective reversal: dilute 0.4 mg to total of 10cc = 0.04 mg/cc
11stst dose = 0.04mg IV, double q 2min until desired LOC/RR dose = 0.04mg IV, double q 2min until desired LOC/RR achievedachieved
Rarely need to give more than 2-3 dosesRarely need to give more than 2-3 doses Elimination half-life: 60-90minElimination half-life: 60-90min
Shorter that most opioid elimination half-livesShorter that most opioid elimination half-lives May need repeat doses or infusionMay need repeat doses or infusion

Fentanyl SummaryFentanyl Summary
Short-acting, potent analgesicShort-acting, potent analgesic Termination of effect by distributionTermination of effect by distribution Only redose after enough time for peak effect Only redose after enough time for peak effect
5 min5 min Dose dependent respiratory depressionDose dependent respiratory depression
Oxygen for all patientsOxygen for all patients Keep an eye on the RRKeep an eye on the RR
Simple A&B’s will get you out of most troubleSimple A&B’s will get you out of most trouble NarcanNarcan

Be patient in your Be patient in your dosing:dosing:
You can always give some more, but You can always give some more, but you can’t take a big dose back you can’t take a big dose back

BenzodiazepinesBenzodiazepines

BenzodiazepinesBenzodiazepines
Anterograde AmnesiaAnterograde Amnesia AnxiolysisAnxiolysis Anticonvulsant properties Anticonvulsant properties Somnolence/HypnoticSomnolence/Hypnotic No analgesiaNo analgesia

Typical BenzosTypical Benzos
MidazolamMidazolam DiazepamDiazepam LorazepamLorazepam

MidazolamMidazolam
Water solubleWater soluble 2x more potent than diazepam2x more potent than diazepam Amnesia > SedationAmnesia > Sedation Route: IV, IM, PO, INRoute: IV, IM, PO, IN Supplied as:Supplied as:
1 mg/ml1 mg/ml 5 mg/ml5 mg/ml Oral preparation (facility dependent, 2mg/ml)Oral preparation (facility dependent, 2mg/ml)
Onset: Onset: IV: 30 - 60s IV: 30 - 60s
Peak: 3 - 5 minPeak: 3 - 5 min

MidazolamMidazolam
Dosing:Dosing: IVIV
0.5 – 2.5 mg aliquots0.5 – 2.5 mg aliquots 5 min between doses (allow peak effect)5 min between doses (allow peak effect) Duration: 15 - 85 minDuration: 15 - 85 min

MidazolamMidazolam
DurationDuration Distribution to/from brainDistribution to/from brain Rapid hepatic clearanceRapid hepatic clearance
EliminationElimination Half-time 1-4 hHalf-time 1-4 h Doubled in elderlyDoubled in elderly
MetabolitesMetabolites Partially active (50%), rapidly cleared via kidneysPartially active (50%), rapidly cleared via kidneys

Midazolam & Organ FailureMidazolam & Organ Failure
Hepatic Hepatic Metabolism dependent on hepatic blood flow and enzyme Metabolism dependent on hepatic blood flow and enzyme
activityactivity Elderly, liver failureElderly, liver failure
Reduce dose, but still safeReduce dose, but still safe Faster metabolism than other benzosFaster metabolism than other benzos
RenalRenal Not affected by renal failureNot affected by renal failure
Caveat: renal failure + infusion (ICU setting)Caveat: renal failure + infusion (ICU setting)

MidazolamMidazolam
Side EffectsSide Effects Depressed level of consciousnessDepressed level of consciousness
Depressed airway reflexesDepressed airway reflexes VentilationVentilation
Decrease hypoxic drive (COPD)Decrease hypoxic drive (COPD) Midazolam as sole agentMidazolam as sole agent
Minimal respiratory depression (unless COPD or elderly)Minimal respiratory depression (unless COPD or elderly)
Synergism with other agentsSynergism with other agents Worsen respiratory depression of fentanylWorsen respiratory depression of fentanyl
More significant than diazepam/lorazepamMore significant than diazepam/lorazepam

MidazolamMidazolam
Side EffectsSide Effects CardiovascularCardiovascular
Decr BPDecr BP Incr HRIncr HR CO maintainedCO maintained

DiazepamDiazepam
““Valium”Valium” ½ as potent as midazolam½ as potent as midazolam Long elimination timeLong elimination time
21-37h21-37h Directly proportional with ageDirectly proportional with age
Active metabolitesActive metabolites Renal excretion:Renal excretion:
even longer elimination half-life even longer elimination half-life
Organ failureOrgan failure Hepatic: prolonged eliminationHepatic: prolonged elimination Renal: prolonged eliminationRenal: prolonged elimination

LorazepamLorazepam 3x as potent as midazolam3x as potent as midazolam PO, SL, IV, IMPO, SL, IV, IM Slow peak effects (20-30 minutes)Slow peak effects (20-30 minutes) Long clinical effects (6-10 hours)Long clinical effects (6-10 hours) More potent sedative and amnesticMore potent sedative and amnestic Long elimination timeLong elimination time
10-20 hours10-20 hours Non-active metabolites, no adjustments for Non-active metabolites, no adjustments for
organ failureorgan failure

BenzodiazepinesBenzodiazepines
Most common side effects:Most common side effects: Prolonged sedationProlonged sedation Respiratory depressionRespiratory depression
COPDCOPD ElderlyElderly
... synergistic with other CNS depressants... synergistic with other CNS depressants Opioids etc.Opioids etc.

Initial Treatment of (Serious) Initial Treatment of (Serious) BenzoBenzo Side Effects Side Effects
Respiratory Depression:Respiratory Depression: Airway & BreathingAirway & Breathing
(Oxygen already on)(Oxygen already on) Upgrade to FMUpgrade to FM
Stimulate patient/check resp Stimulate patient/check resp raterate
Adjust upper airway (jaw Adjust upper airway (jaw thrust)thrust)
Look for respiratory effort (?Look for respiratory effort (?obstruction)obstruction)
Oral A/W, Jaw thrustOral A/W, Jaw thrust Bag Mask Ventilation (100% Bag Mask Ventilation (100%
O2)O2) AntidoteAntidote

FlumazenilFlumazenil
Specific and exclusive benzodiazepine Specific and exclusive benzodiazepine antagonistantagonist Dose dependent reversal of Dose dependent reversal of
SedationSedation Respiratory DepressionRespiratory Depression

FlumazenilFlumazenil
Dosage:Dosage: Titration to desired level consciousnessTitration to desired level consciousness
0.1 mg IV q 1 min0.1 mg IV q 1 min Typical dose 0.3 – 0.6mg to reverse side effectsTypical dose 0.3 – 0.6mg to reverse side effects
0.5- 1 mg to abolish any benzo effect0.5- 1 mg to abolish any benzo effect In overdose: 0.1 -0.4 mg/hr to maintain LOCIn overdose: 0.1 -0.4 mg/hr to maintain LOC
Duration of actionDuration of action 30 to 60 min30 to 60 min May require redosingMay require redosing

FlumazenilFlumazenil
Side effects Side effects Nausea/VomitingNausea/Vomiting Possible seizures Possible seizures
Chronic benzo userChronic benzo user On anti-epileptic drugsOn anti-epileptic drugs

Local AnestheticsLocal Anesthetics

ClassificationClassification
AmidesAmides LidocaineLidocaine BupivacaineBupivacaine RopivacaineRopivacaine
......
EstersEsters ChloroprocaineChloroprocaine ProcaineProcaine
......

Typical UseTypical Use
InfiltrationInfiltration
?Blocks?Blocks

+/- Epinephrine+/- Epinephrine
VasoconstrictorVasoconstrictor Decrease systemic absorptionDecrease systemic absorption
Decrease risk of toxicityDecrease risk of toxicity Increase duration of blockIncrease duration of block
Greatest effect with lidocaineGreatest effect with lidocaine Less so with bupivacaineLess so with bupivacaine

+/- Epinephrine+/- Epinephrine
Contraindications:Contraindications: Anything that could fall off:Anything that could fall off:
Fingers/ToesFingers/Toes EarsEars NoseNose Ankle Ankle foot foot Male genitaliaMale genitalia
Unstable Cardiac conditionUnstable Cardiac condition CAD etcCAD etc ArrhythmiaArrhythmia

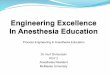
InfiltrationInfiltration
AgentAgent
LidocaineLidocaine
BupivacaineBupivacaine
RopivacaineRopivacaine
Max Dose+
350/500*
175/225*
200
Duration (min)
30-120
120-240
60-360
mg/kg
5/7*
2.5/3.2*
3
* = with epinephrine
+ Assumes 70 kg patient

Systemic ToxicitySystemic Toxicity
Due to excess Due to excess plasma concentrationplasma concentration of any local of any local anesthetic druganesthetic drug Different agents have different thresholds for major Different agents have different thresholds for major
effects, but all can cause toxicityeffects, but all can cause toxicity Main concernsMain concerns
NeurologicNeurologic CardiovascularCardiovascular

Neurologic Toxicity:Neurologic Toxicity:
Dose dependent effects Dose dependent effects (with increasing plasma (with increasing plasma concentrations):concentrations): (Cardiovascular depression) (Cardiovascular depression) Coma, Respiratory arrestComa, Respiratory arrest Seizures, UnconsciousnessSeizures, Unconsciousness Lightheadedness, Tinnitus, Numbness of Lightheadedness, Tinnitus, Numbness of
tonguetongue AnalgesiaAnalgesia

Cardiovascular Toxicity:Cardiovascular Toxicity:
Progression to Progression to (with increasing plasma concentrations):(with increasing plasma concentrations):
Sinus bradycardia, ventricular dysrhythmias, Sinus bradycardia, ventricular dysrhythmias, ARRESTARREST
Decreased cardiac output, hypotensionDecreased cardiac output, hypotension Hypertension, tachycardiaHypertension, tachycardia

Toxicity IndexToxicity Index
Ratio of the dose required to produce eachRatio of the dose required to produce each Cardiovascular Collapse Cardiovascular Collapse :: CNS toxicity CNS toxicity
Lidocaine: ~ 7Lidocaine: ~ 7 Bupivacaine: ~ 3.7Bupivacaine: ~ 3.7

Avoiding LA Toxicity:Avoiding LA Toxicity:
Avoid:Avoid: Overdoses (absorption)Overdoses (absorption) Intravascular injection (short lived, high plasma concentration)Intravascular injection (short lived, high plasma concentration)
Good practice:Good practice: Give less than maximum doseGive less than maximum dose Avoid intravascular injectionAvoid intravascular injection
Aspirate prior to injectionAspirate prior to injection Incremental dosingIncremental dosing Use of epinephrine (where appropriate)Use of epinephrine (where appropriate)
Signs of intravascular injection (tachycardia, hypertension)Signs of intravascular injection (tachycardia, hypertension) Decrease rate of absorptionDecrease rate of absorption

Treatment of LA ToxicityTreatment of LA Toxicity
AvoidanceAvoidance Neurologic symptoms (i.e. Seizures)Neurologic symptoms (i.e. Seizures)
SupportiveSupportive ABC’sABC’s
Acidosis/hypoxia worsens effects of toxicity Acidosis/hypoxia worsens effects of toxicity OxygenOxygen +/- Ventilate+/- Ventilate +/- ETT+/- ETT
Increase seizure thresholdIncrease seizure threshold MidazolamMidazolam
Thankfully briefThankfully brief

Treatment of LA ToxicityTreatment of LA Toxicity Cardiovascular symptomsCardiovascular symptoms
SupportiveSupportive Call for HELP (Call for HELP (CODECODE)) ABC’sABC’s
Control a/w Control a/w OxygenOxygen Ventilate +/- intubateVentilate +/- intubate FluidsFluids Cardiopulmonary bypass (bupivacaine)Cardiopulmonary bypass (bupivacaine)
Intralipid (bupivacaine)Intralipid (bupivacaine) Lipid emulsion (similar to propofol carrier)Lipid emulsion (similar to propofol carrier)












![Welcome [weillcornellbrainandspine.org] · Maricruz Rivera, MD, PhD PGY-3. Neurological Surgery Residents. Evan Bander, MD PGY-5 Alexander D. Ramos, MD, PhD PGY-5 Joseph Carnevale,](https://img.pdfslide.net/doc/110x75/5f7167444c714e55d46f024a/welcome-weill-maricruz-rivera-md-phd-pgy-3-neurological-surgery-residents.jpg)