Embed Size (px)
Citation preview

MANAGING CANCER PAIN 1
Improving Nurses’ Knowledge and Comfort in Managing Pain in Cancer Patients
A Process Improvement Project
Jennifer Deneault DNPc, RN, OCN
Doctor of Nursing Practice Program Capstone
School of Nursing and Health Science
Simmons College
Boston, Massachusetts
© Jennifer Deneault 2018

2MANAGING CANCER PAIN

3MANAGING CANCER PAIN

4MANAGING CANCER PAIN
Abstract
Background: Symptom management is essential to the quality of cancer care. The goal of cancer
care is to have interventions available to ensure that the patient is as comfortable as possible
during the trajectory of their disease. Providing effective pain relief requires the use of evidence-
based interventions to prevent unnecessary suffering.
Purpose: The purpose of this process improvement project was to provide education to nurses to
address knowledge gaps that were identified through the administration of The Knowledge and
Attitudes Survey on Cancer Pain (Ferrel & McCaffery, 2014). The goal was to provide
education and resources that would allow the nurses to deliver a higher quality of patient care.
Conclusion: The use of the education intervention was designed to address the barriers of
effective pain management of cancer patients through increasing the nurses’ knowledge and
comfort when assessing pain and administering opioids. Through this process improvement
project nurses were able to identify their own knowledge deficits in the management of cancer
pain. The education and resources that was offered to the nurses increased their own knowledge
and comfort and provided the increased autonomy in managing this symptom and working
collaboratively with the physicians.
Keywords: Cancer pain, pain management, nursing education, knowledge assessment,
collaborative pain management, nursing engagement

5MANAGING CANCER PAIN
Dedication
I dedicate this project to my family. My husband Mike, I could not have made it this far
without you by my side. Your unending love, support and patience is what got me through the
endless nights of writing. My two sons Noah and Cole, I began this degree for you. To show
you that anything is possible, that learning is constant and to always reach for the stars. Every
day your love, innocence and resiliency show me that you will continue to grow into young men
that will always make me proud to be your mother. My parents, you instilled in me the yearning
for wanting more and be better than the me of yesterday. Thank you. Love you all, Jen

6MANAGING CANCER PAIN
Acknowledgements
I would like to thank my professor Dr. Eileen McGee for her guidance she provided me
through this journey, her support and words of encouragement allowed me to see the light at the
end. I would also like to thank Dr. Linda Tenofsky, who has been my mentor for the last twenty
years and it was an honor to have her guidance through this monumental achievement. I would
also like to thank Dr. Sharon Perkins; her humor, encouragement, friendship and endless
feedback was invaluable. Lastly, Kelly Fitzpatrick and Paula Lynch Ritchie I couldn’t have
imagined going through this without the two of you. The long study hours, the laughs and tears,
no words for our Boston excursions; I thank you for your friendship and love. It was an honor to
have worked on this project and influence the practice provided to a special population of
patients.

7MANAGING CANCER PAIN
Table of Contents
List of Tables..................................................................................................................................iii
List of Figures ................................................................................................................................iv
Introduction.....................................................................................................................................9
Purpose of the Project…………………………………………………………………………... 11
Significance of the Project……………….…………….………………………………………...11
Literature Review…….……………………………………………………………………….…13
Background.……….......................................................................................................................13
Prevelence of Pain……………..……………………………………………………………...….15
Barriers to Pain Management……………………………………………...……………………..16
Pain Management Interventions…...………………………………………………………...…..17
Nursing Education ….……………………...................................................................................21
Nursing Engagement…………………………………………………………………………….22
Conceptual Framework…………………………………………………………………………..23
Design.…………………………………………………………………………………………...25
Setting and Population………………………………………………………………………......27
Interventions……………...……………………………………………………………………...28
Analysis…………………………………………………………………………………….…….31
Measurement…………….…..…………………………………………………………...………32
Discussion …….…………………………………………………………………………………33
Ethics and Human Subjects…………...…………………………………………………………34

8MANAGING CANCER PAIN
Plan for Dissemination………………………………………………………………………...…34
Conclusion……...………………………………………………………………………………..35
References……………………………………………………………………………………….36
Appendix A: Knowledge and Attitude Survey…….……………………….…………………...42
Appendix B: HCAHPS Results…………………………. …………………………………...…48
Appendix C: Brief Pain Inventory ………………………………...……………………………49
Appendix D: ECOG Performance Tool ……………………………………………….….……..51
Appendix E: Equianalgesic Table Guidelines………………….………...……………….……..52
Appendix F: Narcotic Conversion Chart……………………….………………………………54
Appendix G: IRB Letter………………………………………………………………….……..55
Appendix H: Education Slides……………………………………………………………….......56
Appendix I: NCCN Guidelines…………………………………………………………………..66

9MANAGING CANCER PAIN
List of Figures
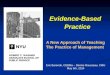
Figure 1. The WHO 3 Step Analgesic Ladder…..………………………………………………27
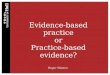
Figure 2. Deming’s PDCA Framework…………………………………………………………28
Figure 3. Kurt Lewin Change Model…………………...……………………………………….28

10MANAGING CANCER PAIN
Improving Nurses’ Knowledge and Comfort in Managing Pain in Cancer Patients
Introduction
According to Aanchal & Bhatnagar (2017), “Survival rates of cancer patients are rapidly
increasing over the last decade due to the advent of multi-modal anti-cancer treatments. The
newer treatments have shifted the disease paradigm from a serious fatal illness to a chronic
illness. During illness, survivors experience multitude of distressing symptoms such as pain,
fatigue, anxiety, depression, insomnia, lymphedema, hot flashes, and nausea/vomiting” (p 468).
Pain is experienced by one-quarter of patients newly diagnosed with cancer, one-third of the
patients who are receiving treatment, and three-quarters of those patients who have metastatic
disease (Swarm, Abernethy, Anghelescu, Bendetti, Blinderman, Boston & Weinstein, 2010).
The Oncology Nursing Society (2016) policy on cancer pain states management of each
patient’s pain must be recognized, individualized and treated accordingly. Pain is a subjective
symptom in patients and 17-70% of those diagnosed with cancer and various stages of disease
report pain as a chronic problem. Of those patients that report pain, 25-72% state that their pain
is undertreated. The undertreatment of cancer pain occurs regardless of the number of guidelines
and resources available to clinicians caring for cancer patients (Palalogos, Mocanu, Balacescu,
Nemes, Rajcsanyi, Jozsef…Burz, 2012). Pain in oncology patients can most often be attributed
to the primary tumor; however, it can also be a result of many different therapies the patient
receives (National Cancer Institute, 2017). This common symptom can be quite ambiguous to
understand and treat due to its many complexities such as the frequency and intensity of the pain,
the patients’ ability to describe the pain, and the underlying cause of the pain. Patients are
expected to quantify their pain without a comprehensive understanding in distinguishing between

11MANAGING CANCER PAIN
different types of pain, their cause, and the ability to set realistic expectations for the
management of the pain (Fourie & Nesset, 2017). The experience of pain can lead to depression,
anxiety, sleep disturbance and a physical inability to perform activities of daily living (Boveldt,
Vernooij-Dassen, Burger, Ijsseldijk, Vissers & Engels, 2013). “Due to its very nature and
complexity, coping with cancer pain requires more than information and requires knowledge,
understanding, and learning about such things as pain management and self- care” (Fourie &
Nesset, 2017, p. 6).
The healthcare team including physicians, nurses, patients and their families need to
contribute to creating an improved system of managing pain in cancer patients. The barriers that
prevent nurses from adequately managing cancer pain are varied and may include insufficient
education about cancer pain and therapeutic interventions, as well as managing side effects of
pain and pharmacologic interventions (Bartoszczyk & Gilbert-White, 2015).
Exploring nurses knowledge of cancer pain and comfort when assessing and managing
cancer pain will add to the professional development of these specialized nurses and potentially
improve nurses assessment skills ultimately improving pain management for cancer patients.
Background
A retrospective analysis of satisfaction scores of patients hospitalized on the 26 bed
inpatient medical oncology unit at a community hospital referenced as the unit participating in
this process improvement for the year June 2016-July 2017 (Appendix B) demonstrated the need
to improve how cancer pain is managed. During the time frame of June 2016 – July 2017 131
patient surveys were returned. Of the surveys returned, only 72.2% of those patients had replied
that they were ‘always’ satisfied with their pain management (Centers for Medicare & Medicaid,
2017). These findings pointed to a need to improve care related to pain but what has not been

12MANAGING CANCER PAIN
known from these results are exactly why the patients were dissatisfied. They were an indication
that there was a problem, but do not accurately identify the nature of the problem. What the
scores indicated is that 41% of respondents in the survey were dissatisfied with their pain
management. Despite the lack of specificity in the patient satisfactions scores, the findings did
indicate a need improve care practices related to pain management.
Purpose Statement
The purpose of this process improvement project was to identify and address knowledge
gaps related to addressing cancer pain in patients admitted to the oncology unit at the project site.
The questions addressed in this process improvement project were:
1. What are the gaps in knowledge related to the treatment of cancer pain in a group of
registered nurses working on an Oncology Unit?
2. Will the use of a targeted educational program related to the treatment of pain in
cancer patients improve practices related to cancer pain management on this unit?
3. Will providing current evidenced based assessment skills of oncology pain to nurses
improve the care delivered to oncology patients related to cancer pain management?
The specific aim of this project was to assess nurses knowledge related to the treatment
of cancer pain on an Oncology Unit and to develop and implement a targeted educational
program to address specific knowledge deficits.
Significance of the Problem
In 2012 there were a reported 14 million new diagnoses of cancer and by 2025 the
estimated increase will exceed 20 million. Regardless of the increased understanding of the
disease, and preventative screening and treatments, the progress in treating cancer pain has been
slow. Cancer pain continues to be one of the most reported side effects and one of the most

13MANAGING CANCER PAIN
feared by oncology patients. Referring to studies written within the past few years, more than
half the patients with a cancer diagnosis report the occurrence of pain (Ferlay, Soerjomataram,
Dikshit et.al, 2015).
Challenges to adequate pain assessment reflect the limitations of tools to precisely assess
the patient’s pain. There are multiple cancer pain sources in addition patients have co-
morbidities that cause pain, leaving it difficult for the patient to distinguish the type and cause of
pain they are experiencing. The current pain scales that are used do not allow for a
comprehensive pain history, which leads to physicians having decreased ability of adequately
assessing the pain. There is not an objective test for pain, such as other areas of disease
management, and lastly to adequately assess pain takes time which physicians and nurses
consistently have less of due to other constraints (Greco, Roberto, Corli, et.al, 2014).
The Joint Commission requires that hospitals educate all licensed individuals providing
patient care on the assessment and management of pain and the hospital understands the patients
right to their management of pain. Requirements that should be adhered to by healthcare
organizations are: the professional development department completes a thorough pain
assessment that meets the needs of the patient; the professional development specialists use a
method to assess the pain that is consistent with the cognitive ability of the patient; the
professional development specialists assess and respond to the patients report of pain; and, lastly
the healthcare team treats the pain accordingly or refers them for specialty treatment (Baker,
2018). The pain assessment tool used in practice at the project site is a standard assessment
nonspecific tool used for all pain, asking the patient to quantify their pain using a number analog
scale. The need for a comprehensive assessment that identifies type of pain, limiting factors and
realistic goals is vital to improve the current state.

14MANAGING CANCER PAIN
Managing cancer pain has become increasingly important to patients, families, care
providers, healthcare organizations and regulatory bodies. Various methods of assessing patient
satisfaction with pain management have been developed. One assessment tool currently utilized
for hospitalized patients is the Hospital Consumer Assessment of Healthcare Provider and
Systems (HCAHPS). This tool is the first national survey available for public viewing that
captures aspects of patients’ experiences of care received in a hospital setting. The survey has
three goals: allowing data on patients’ experience to be publicly available; allowing health care
systems to improve quality of care based on scores; and holding health care systems accountable
(Centers for Medicare & Medicaid May, 2017, Retrieved from http//www.cms.gov). The
HCAHPS survey contains questions which ask patients how well their pain was managed during
their hospital stay. The broad questions asked by HCAPHPS would be beneficial if the nursing
assessments identified the specific pain and then the patient received the right treatment
(Mahoney, 2017).
Literature Review
A thorough search of the literature was completed to identify existing research related to
pain management in cancer patients. The following databases were included: CINAHL,
PubMed, and Cochrane. Keywords included a combination of the following: cancer pain,
nursing education, barriers to cancer pain management and nursing engagement. The Oncology
Nurses Society, National Comprehensive Cancer Network and End of Life Nursing Education
Consortium were explored for resources on pain management. Inclusion criteria consisted of full
text academic literature articles published in English language within the past 5 years. The focus
on the articles was nurses knowledge and perceptions of cancer pain. The search yielded many
articles; each were examined for strength of evidence and quality to support the topic.

15MANAGING CANCER PAIN
Introduction/ Background
The diagnosis of cancer affects the patient in many ways. Subsequent to coping with the
diagnosis of cancer, patients feel uncertainty related to the disease stage and recommended
treatments, symptoms secondary to disease and treatments, body image changes and sexual well-
being (Chu, Dialla, Roignot, Bone-Lepinoy, Poillot, Coutant & Dabakuyo-Yonil, 2016). Pain is
one of the most prominent symptoms of cancer and often interferes with their ability to perform
activities of daily living (Boveldt et al., 2013). Patients are often left to manage symptoms of
their cancer pain on their own (Koller, Miaskowski, De Geest, Optiz, & Spichiger, 2012).
Anxiety, depression, and disturbances in sleep affect the patients' quality of life; each of these
can be the result of cancer pain (Boveldt et al., 2013).
Pain in cancer patients can be contributed to many different factors, including diagnostic
procedures, surgery, radiation, and chemotherapy side effects (Garcia, Whitehead, & Winter,
2015). “Comprehensive pain assessment is considered as the cornerstone of pain management,
and, consequently, assessment guidelines have been developed by different organizations”
(Garcia et al., 2015, p. 31). Garcia et al., (2015) surveyed nurses through semi structured
interviews to determine nurses' barriers in assessing and managing cancer pain. The themes that
resulted from this study were; participants had expressed that cancer pain is hard to assess
because it such a complex symptom, the expectations of relieving their patient from pain and
being unable to do so is frustrating for nurses, patients who have a fear of addiction which might
refrain from their actual reporting of pain and a lack of training and education makes it difficult
to accurately assess pain and recommend treatment options (Garcia et al., 2015).
There are different types of cancer pain. Pain can be related to the tumor or treatments the
patient receives. Pain can either be acute or chronic, and it is important to distinguish between

16MANAGING CANCER PAIN
the two when conducting an assessment. Pain has two mechanisms of pathophysiology;
nociceptive and neuropathic (Swarm et al., 2010). “Nociceptive pain results from an injury to
any of the visceral structures within the body and neuropathic pain stems from an injury to the
peripheral or central nervous system” (Swarm et al., 2010, p. 1077). Patients have a role in
cancer pain management. Not only are they expected to describe their pain but also, they must
define their pain chronic or acute, define aggravating factors and provide a history of prior
treatments. Patients often receive little education on types of pain and types of pain management
making it difficult for them to adequately assess and describe their pain (Hovind, Bredal, &
Dihle, 2013).
There are many reasons why pain is undertreated. Pain is subjective and often related to
other symptoms. The availability of proper opioids and the stigma around addiction all make
pain a complex symptom for health care professionals (Kwon, 2014). Other aspects may
influence managing pain such as the patients’ beliefs around their illness and recommended
treatment (Glattacker, Heyduck, & Meffert, 2012) as well as what patients want to know about
their disease (Grieve, Adams, & McCabe, 2016).
Prevalence of Cancer Pain
The prevalence of pain varies depending on the origin and progression of the tumor.
“Most cancer-related pain is reported by patients diagnosed with a head and neck malignancy,
with average prevalence of 70%; patients with gynecologic malignancy report 60%,
gastrointestinal at 59%, lung cancer at 55%, and 54% for patients with breast cancer” (Overcash,
Hanes, Birkhimer, & Askew, 2013, p. 365).
Boveldt et al., (2013) conducted a study to assess the prevalence of pain in cancer
patients and the intensity of pain the patient had felt. The study involved evaluating the pain of

17MANAGING CANCER PAIN
428 medical oncology patients, the Brief Pain Inventory, as well as the Pain Management Index,
were used to conduct this study. The results of study show that the prevalence of pain ranged
from 27%- 60%, with 19- 39% of those patients suffering from neuropathic pain caused by the
tumor. Inadequate pain relief was reported among 31- 65% of participants.
Barriers to Managing Cancer Pain
Kwon (2014) studied barriers to effective pain management from the physician, patient,
and a systems perspective. Common themes amongst physicians, patients, and healthcare
systems were: lack of standardized assessment tools, education focused on types of pain and
realistic goals, fear of addiction and tolerance, adherence to medication schedules and
availability of opioids. Often physicians waited until the terminal phase of a disease before
prescribing high doses of opioids because of a decreased comfort in prescribing such high doses.
Nurses often express the frustrations in managing cancer pain and find pain a complex
symptom to assess with the variances between patients. Like their physician colleagues’ nurses
have difficulty with the assessment tools that are available and find them unreliable in capturing
the patient’s pain experience. Garcia has identified a lack of education on the use of opioids
(2015). Nurses lack the understanding of identifying the different types of pain, how to manage
the pain and how to combine different types of pain medications as well as managing the side
effects that accompany some of these medications such as nausea and constipation (Bartoszczyk
& Gilbert-White, 2015).
Physicians and nurses often have a difficult time interpreting the reported pain response
of the patient and often find themselves assuming the needs of the patients. Oncologists are not
often the primary care provider in the hospital setting but rather act as consultants; thus, are not
leading the pain management care plan, despite their increased knowledge in the causes of

18MANAGING CANCER PAIN
cancer pain and treatment options. The emphasis of goal setting is important in managing pain,
rather than focusing on eradicating the pain. It would be best to determine what level of pain is
acceptable and allow the patient to participate in activities of daily living (Bhatia, Gibbins &
Forbes, 2014).
Patient-reported barriers are often contributed to adequate pain control. A type of
patient- reported barrier is the perspective of the patient in regards to pain medication. Pain
medication perspectives that are often concerning for the patient are the fear of addiction, the
side effects of the medication, developing a drug tolerance. These barriers are many times
deterrence to physicians prescribing efficient therapies to control the pain the patient is having
(Hye Kwon et al., 2013).
Kwon et al., (2013), distinguishes a correlation of identifying barriers through the use of
the pain management index (PMI). The PMI is a suitable tool to determine if the patient is
prescribed therapies that meet their needs, however with patients that are prescribed strong
opioids they will always have a positive PMI. With that being said it is imperative for other
variables to be considered when evaluating the efficacy of treatments prescribed. Kwon et al.,
(2013) conducted a study on other variables that effect pain management, results of their study
show that depression was a prognosticator of high barrier score to pain management. This
indicated that physicians need to be mindful of this concept and manage both symptoms.
“Barriers should be explored among patients with a high level of depression, and depression
should be explored among patients with a high level of barriers (Hye Kwon et al., 2013, p. 1181).
Pain Management Interventions
The World Health Organization (2016) states that about 90% of cancer pain can be
managed with basic interventions. Regardless of the number of interventions that have been

19MANAGING CANCER PAIN
implemented patients continue to suffer from uncontrolled pain because the evidence-based
interventions are rarely incorporated into daily practice (Brant, Potter, Tavernier, & Beck, 2012).
Smith & Saiki, (2015) summarize a series of steps guiding an improved system of cancer
pain management;
1. Assessment of pain: ensuring the clinician can define the type of pain,
understand the cause of the pain and interpret the characteristics of the pain and
provide the patient with examples.
2. Management of the pain: ensuring the nurses can identify an appropriate
method to treat the pain, understand the current uses and its effectiveness and
characteristics of each medication.
3. Prevention and management of adverse effects: ensuring the clinician
understands the mechanism of action of each medication and preemptively
treating and monitoring for expected side effects (pages 1430-1433)
The World Health Organization Pain Ladder (see Appendix F) provides guidelines for
managing cancer pain based on the intensity of the pain. The ladder is used by many physicians
and nurses in a variety of settings to assist in managing cancer pain effectively. The ladder
recommends immediate administration of oral medications. If the patient reports mild pain then
start with non-opioid drugs such as Tylenol with or without adjuvant non-steroidal anti-
inflammatory drugs. If complete pain relief is not achieved then a weak opioid such as codeine
or tramadol can be initiated. If this becomes insufficient then a stronger opioid should be
started such as morphine, fentanyl, oxycodone or hydromorphone, while continuing on the non-
opioid therapy. The opioid dose is escalated until the patient is free of pain or at maximum
relief without unbearable side effects (World Health Organization, 2016).

20MANAGING CANCER PAIN
A thorough pain assessment should identify the location of the pain, type of pain, pain
history, pain intensity, temporality, referral pattern, and radiation of pain to other parts of the
body. An understanding of what currently relieves the pain and what prior therapies have been
prescribed and determining the patient’s goals of comfort. The location of the pain must be
described by the patient and often having them point to identify the exact area of discomfort is
helpful, this can be essential to determining the cause of the pain. The intensity of the pain is
subjective and is often quantified by using a number of different pain scales and having an
understanding of the type of pain whether it be neuropathic, somatic or visceral is an important
part of an extensive pain assessment. Temporality defines the patients’ experience of pain,
determining if the pain is chronic or breakthrough (Gallagher, Rogers, & Brant, 2017).
There are three tools that are commonly used in assessing levels of pain and
recommended therapies. The first tool is the pain-management index which was developed to
compare the strongest form of analgesic prescribed for the patient to the patients’ level of
reported pain. This tool was developed in 1994 and has been modified over the years to reflect
current practice (Cleeland et al., 1994). The pain management index score indicates how the
patients reported pain is managed by the analgesics that have been prescribed. A pain score of
zero is when there is no pain reported, 1 would be mild pain, 2 moderate pain and 3 severe pain.
The analgesic score on the pain management index was reached by the analgesic prescribed. If
there is no analgesic prescribed it would be scored as 0, a nonopioid medication would be 1,
weak opioid such as codeine would be 2, and strong opioids such as morphine would be 3. The
index score is calculated by subtracting the worst pain score from analgesic score. If a patient
calculates a negative score they were determined as having inadequate pain control (Singh,
Banpal, & Singh, 2017). The World Health Organization’s (WHO) guidelines were referenced in

21MANAGING CANCER PAIN
developing the pain index. The WHO created a three-step ladder for the relief of pain in cancer
patients. If a patient reports pain then there should be an immediate oral administration of
analgesics in the order of non-opioids, then mild opioids, then strong opioids until the patient
reports relief of pain (World Health Organization, 2016). Boveldt et al., (2013) showed that 39%
of the patients that participated reported pain and 20% had moderate to severe pain. Half the
patients that participated in this study had pain that was inadequately treated, and the high pain
intensity that was reported inter fered with activities of daily living (Boveldt et al., 2013).
Figure 1. The WHO 3 Step Analgesic Ladder.
The National Comprehensive Cancer Network (NCCN) recognizes the efficacy of the
WHO guidelines but also; posit that the management of cancer pain is much more complicated
than the three-tiered approach. The NCCN guideline is different in how it approaches to pain
management. The patient must validate the pain intensity; a comprehensive pain assessment
must be completed and reassessing the pain is vital along with social support and patient
education. The NCCN guidelines provide dosing guidelines for NSAIDs, opioids, and co-

22MANAGING CANCER PAIN
analgesics; they also provide guidance on the titration and rotation of opiates. To adequately
assess pain, it must be determined if the pain is associated with the tumor, treatment or neither.
Once the origin of the pain is determined an individualized pain care plan can be created for the
patient to reach a level that maximizes their functional status (Swarm et al., 2010).
Nursing Education
The Oncology Nursing Society (ONS) strives to incorporate evidence-based practice to
improve patient outcomes. The Putting Evidence into Practice (PEP) initiative began in 2006.
The main focus of this initiative was to recognize the best scientific evidence to improve patient
care and the education of patients. Twenty topics were identified and of those twenty a
supplement was dedicated just as a resource for pain. The initial pain resource was created in
2007 and was last updated in 2013 to include multiple opioid preparations for pain, and to review
guidelines for standard opioids, ultimately creating clear recommendations for practice (Irwin,
Brant, & Eaton, 2011).
"Evidence-based pain management implementation involves a comprehensive assessment
of pain with a reliable and valid patient-report instrument, delivery of pharmacologic and non-
pharmacologic interventions based on the evaluation of findings, frequent reassessment of pain,
and repeated delivery of interventions" (Eaton, Meins, Mitchell, Voxx, & Doorenbos, 2015, p.
166). Nurses are vital members of the health care team regarding pain management, relying on
best practice and using a holistic style along with the patient in understanding the disease process
(Morales-Fernandez, Morales-Asencio, Canca-Sanchez, Moreno-Martin, & Vergara-Romero,
2016). Education programs focus on providing a foundation in defining the multidimensional
aspects of pain and provide a basic understanding of pain including the experience of the patient
and its impact on their daily living. The other domains of pain education focus on the

23MANAGING CANCER PAIN
assessment and measurement of pain, the management of pain and the nurse’s role in applying
these competencies while caring for patients (Fisherman et al., 2013). Gustafsson & Borglin
(2013), state the importance of incorporating the elements of various beliefs that may affect the
management of cancer pain and understanding the expectations of the patient.
Nursing Engagement
Nurses are expected to engage in efforts to provide quality care at a lower cost. “Among
the 3 million registered nurses in the United States, frontline nurses, positioned at the point of
care, are pivotal to the success of new payer models and outcome measures” (Riley, Dearmon,
Mestas, & Buckner, 2016, p. 325). Cziraki (2015) highlights the importance of retaining nurses
and enticing new nurses through the culture of the work environment. In this study Cziraki
suggests that managers who demonstrate the behavior of leadership empowerment provide
nurses with information, support and opportunity for growth. An organization that has a strong
sense of shared purpose fosters an environment where nurses are engaged in change initiatives.
Developing the resilient environment provide an outlet for nurses to emerge from the negativity
and increase positive outcomes (Scott, 2015).
Improving the meaningfulness of work and providing an opportunity to accomplish goals
had the greatest impact on the engagement of nurses. Unit structure around huddles, staff
meetings and professional development opportunities strengthen the importance of the nurses
work and foster a sense of autonomy (Cziraki & Laschinger, 2015). A definitive method for
improvement nurse engagement at work is to provide professional development opportunities to
promote knowledge and ultimately improve patient outcomes (Koppel, Virkstis, Strumwasser,
Katz, & Boston-Fleischhauer, 2016). Engaging nurses in the better understanding of pain

24MANAGING CANCER PAIN
management and how improving pain scores will improve patient satisfaction thus being
reimbursed at the local level.
Conceptual Framework
Lewin’s Change Theory was utilized as the framework for this improvement project.
Kurt Lewin’s Change Theory (1947) is a widely used model for implementing change. Lewin
believed (1947), that there are two forces to consider when implementing a change: driving
forces and restraining forces. Driving forces promote the implementation of change by
motivating the participants toward the determined goal (Kritsonis, 2004; Lewin, 1947).
Restraining forces counter the driving forces by delaying progress. The driving force in this
project was to address the urgent need to improve cancer pain management in a specific patient
population through the use of a targeted intervention with nursing staff. The restraining forces in
this project were the lack of education and limited resources to adequately assess pain. Lewin’s
theory offers suggestions and guidance about how to implement a change process within an
organization. Nurses must identify the barriers to managing the pain adequately and achieve the
knowledge and confidence to meet the goal.
Figure 2. Kurt Lewin Change Model. Retrieved from http://www.change-management-coach.com/kurt_lewin.html
Lewin’s Change Theory articulates three stages of the change process: Unfreezing,
Change and Re-freezing (Well, Manuel, & Cunning, 2011). The first stage of the change

25MANAGING CANCER PAIN
process is “Unfreezing”. Unfreezing occurs when participants realize that there is a need for
change around a process (Well et al., 2011). Using this process, the organization is obligated to
evaluate the current state and investigate a new standard work that could improve how care is
delivered. The unfreezing process requires a recognition of the need for change and a gradual
melting away of old practices and behaviors. Anecdotal evidence, supported by patient
satisfaction data provided the impetus for iniating a change in practices around pain management
on this unit. The nurses caring for the oncology patients realized that their current practice
reflected a lack of knowledge in assessing and managing pain and this reality helped the nurses
accept the need for change. It was important for the nurses to realize the importance of this
change and how it would benefit the patients and improve the care that was delivered. This stage
of the change process required attention to the restraining forces which might impede the desired
change.
The second stage in Lewin’s Change Model is “Transitioning” or “Change”.
Transitioning is when the change is implemented. This stage can be difficult for those involved,
leaving behind an old process and implementing a changed model of care. Continuous support
and education are vital reinforcements for the nurses as they embark on this stage in the theory
(Well et al., 2011).
The first goal of Lewin’s Change Theory was to provide the right climate to make this
change successful by involving the nurses in the discussions leading up to the education. Nurses
from the unit-based education council were involved in discussing the identified gap and offered
feedback on realistic improvements and what education would benefit their practice. These
nurses helped facilitate the buy-in from the other staff nurses on the unit and assisted in
developing this small test of change (Well et.al, 2011).

26MANAGING CANCER PAIN
Lewin’s final stage, “Refreezing” this stage is about establishing stability once the
changes have been made. The changes are accepted and become the new norm. People form new
relationships and become comfortable with their routines. This final phase can take time. During
this stage questions that complement the “ACT” phase would focus on what needs to be changed
and is there more to learn on the topic. Auditing of the process is instrumental to ensure that the
change is sustainable. Planning around this change would include educating new nurses on this
model of care and ensure that the interventions are used by everyone going forward (Well et al.,
2011). Once the outcomes of this process improvement are reached, the results will be shared
with other units and the entire oncology service line.
Methods
Timeline
This process improvement project began in January of 2017 after the results of a three
month period of patient satisfaction scores were reviewed. The results of the surveys
demonstrated that the pain management in the population of patients cared for on the inpatient
oncology unit could be improved. This information was shared with the leaders of the oncology
program and the nurses on the unit.
The next step in this process improvement project was to arrange a meeting with the unit
based education council. This council was formed three years ago; the members include six staff
nurses that helped in creating and dessiminating education to the rest of the staff. The education
council reviewed The Knowledge and Attitudes Survey on Cancer Pain and assisted to
modifying it to better reflect the population of patients that are cared for on this inpatient unit.
The survey was available to all staff via Survey Monkey© to provide an easy and anonymous
venue for the nursing staff to participate in a pre and post survey.

27MANAGING CANCER PAIN
The pre survey was sent out on October 23rd, 2017 and remained open for 3 weeks, after
which the results were analyzed. The data analysis of completed surveys identified knowledge
gaps that supported the intent of this process improvement project. Five educational training
sessions were offered to the nursing staff. In addition to educational sessions nurses were also
provided the Brief Pain Inventory (see Appendix C) and a narcotc conversion chart (see
Appendix F) to help improve their assessment and management of cancer pain. Nurses provided
patient care using the new resources during the months of December and January. The modified
Knowledge and Attitudes Survey was distributed again to determine if the resources were
beneficial in improving their overall knowledge. During the month of February the results were
analyzed and compared to the pre survey.
Design
The design of this project was process improvement with the intent of improving
nursing knowledge in managing cancer pain. This was completed with education, pre and post
data from surveys and anecdotal feedback from the nurses that participated in this project. The
PDCA Cycle Model was used to guide this process improvement project. According to Deming
(2016), PDCA, also known as the Deming Cycle, uses four cyclical steps for continuous quality
improvement. The initial step, ‘Plan’, begins by identifying the problem, defining the targeted
outcome, developing a process for the desired change as well as a method for evaluation or
monitoring the change. The next step, ‘Do’, involves implementing the change process and
collecting the data. The ‘Check’ step involves completing data analysis, reviewing results and
comparing the actual outcome. Finally, ‘Act’ entails identifying any needed modifications and
acting.

28MANAGING CANCER PAIN
Figure #3 Deming’s PDCA Framework Image retrieved from The W. Edwards Deming Institute®
In August of 2017, the planning for this practice improvement began on the inpatient
oncology unit. The oncology unit was selected based on the specialized care delivered to meet
the needs of cancer patients that receive inpatient care. An anonymous staff survey to assess
baseline knowledge the nurses had in managing cancer pain. In October of 2017 education
sessions began with the bedside nursing staff. Training was conducted by a select group of
content experts. The curriculum was developed utilizing materials from End of Life Nursing
Education Cirriculum (ELNEC) and National Comprehensive Cancer Network (NCCN) clinical
practice guidelines for nurses on adult cancer pain management. The Brief Pain Inventory and
medication conversion chart were also shared with the nurses as additional resources.
The goal of the cirriculum was to help the nurses identify barriers to adequately relieving
pain across the trajectory of their disease. The other objectives of the cirrculum were that the
nurses would describe the components of an extensive pain assessment as well as list
pharmacologica and nonpharmacological therapies used in the relief of pain. Lastly, nurses

29MANAGING CANCER PAIN
would be able to describe the role of the nurse in managing cancer pain. For each session 1.0
ANCC continuing education credit was provided for each education session.
The change began after a pre-survey was distributed to all the nurses using Survey
Monkey© to identify the gaps in knowledge amongst the nursing staff. The results of the survey
were utilized to develop the curriculum for the educational intervention which was the “Plan
phase”. The educational program took place over a rolling three-month cycle which was the
“Do” phase with a re-evaluation (“Check phase”) at the end to determine and improvement in
knowledge and success of the change.
Training offered by End of Life Nursing Education Consortium (ELNEC) became a
framework for the curriculum that would be used to educate the nurses and identify potential
barriers to the education that was planned. Prior to the proposed intervention other content
experts were contacted to discuss the project and invite them to participate in the education. A
medical oncologist, two palliative care nurse practitioners and a hospice nurse were part of the
project faculty. The educational material was reviewed and the content was taken from the
ELNEC core curriculum as well as the NCCN (see appendix I). An agenda was completed and a
tentative schedule of education was created. The unit-based education council, faculty, unit
manager and this author met to ensure the education met the facility’s objectives for the growth
of the cancer program. Five weekdays were scheduled to conduct hour long in-service sessions
that would be available to nurses working various shifts.
Setting and Population
This process improvement project included all registered nurses, working on a 26-bed
medical oncology unit in a not-for-profit, 375 bed acute care hospital. This oncology unit
provides care to an average of 2200 patients per year. The South Shore Health System provides

30MANAGING CANCER PAIN
acute, ambulatory and home care to southeastern Massachusetts (www.southshorehospital.org).
This project was shared with the chief nurse as well as the associate chief nurse to obtain senior
leadership support.
The key stakeholders included the staff nurses, unit manager and the director of nursing.
The process improvement was supported by administration. The participant sample consisted of
45 registered nurses working on the oncology unit. Demographics collected consisted of years
of experience as an oncology nurse and if they were certified or belonged to any professional
organizations. All surveys were anonymous, and staff were made aware of anonymity.
Interventions
The first step of this process improvement involved the administration of the “The
Knowledge and Attitude Survey Regarding Pain” tool (see Attachment A) to all registered nurses
currently working on the SSH oncology unit through the use of Survey Monkey©. “Knowledge
and Attitudes Survey Regarding Pain” is a 39 item, validated tool that was developed by Ferrell
and McCaffery in 1987 and revised in 2014. This tool assesses the nurses knowledge of cancer
pain aspects which include; assessing pain, the patients response to pain and effective therapies.
Results of the survey provided insight into the specific educational needs of the staff (Ferrel &
McCaffery, 2014).
After completing the survey, a targeted educational program was developed and
implemented to registered nurses on the unit. The education intervention utilized materials from
the ELNEC curriculum and The NCCN. The core curriculum was utilized to meet the specific
knowledge gaps identified in the survey. Specific attention was given to the ELNEC module on
pain management, which defined the basic principles of pain assessment and management.

31MANAGING CANCER PAIN
In addition to the use of the ELNEC curriculum, other educational opportunities were
provided. These included:
1. A round table discussion for nursing staff with a panel of speakers from the Oncology
and Palliative Care Services. Discussion related to pain management, assessment and
medication dosing.
2. Individual educational opportunities specifically designed to meet the individual
educational needs of the nurses.
3. The use of “Skills Days” for all Oncology unit nursing staff which provided opportunities
for simulation, didactic content and discussion.
A series of five educational programs were offered to the nursing staff and clinical
educators. The Core Curriculum for ELNEC was referenced and tailored to meet the needs
identified through assessing current nurses knowledge and comfort in cancer pain. The module
on pain management defines the basic principles of pain assessment and management. ELNEC
(2014) recognizes that a comprehensive pain assessment is vital in adequately relieving the pain
reported by the patient. The objectives of this course were:
1. Identify barriers to adequate pain relief at the end of life for patients across the life
span.
2. List components of a thorough pain assessment.
3. Describe pharmacological and nonpharmacological therapies used to relieve pain.
4. Discuss the role of the nurse involved with pain assessment and management
The series of five education sessions offered to the nurses incorporated the NCCN
guidelines and ELNEC core curriculum on pain management and an educational framework.
These in-services reviewed pain assessment techniques, medication management and narcotic

32MANAGING CANCER PAIN
conversions. Sessions were didactic in nature and presented material through the use of case
studies and discussions (Appendix H).
In addition to the educational programs, nurses were provided a medication conversion
tool which provided recommended doses of medications when converting from intravenous to
oral and when considering conversion from one type of opiate to another. (see Appendix G).
This resources was instrumental in elevating nursing practice and enabled the nurse to be active
care providers in recognizing appropriate narcotic dosing.
The nurses were provided an additional assessment tool (see Appendix E) that was
intended to quantify the patients’ pain. This was another resource to improve the nurse -patient
relationship around managing pain. Previously nurses had used a numerical pain score tool, in
which the patient quantified their pain with a number from 1-10. The new tool that was
introduced was the Brief Pain Inventory, which was a part of the ELNEC core curriculum. The
Brief Pain Inventory is a seminal tool that assures the validity, reliability, and sensitivity of
patient reported pain to help determine the patient's Eastern Cooperative Oncology Group
(ECOG) performance status and attribute to care plans (Cleeland, Gonin, Hatfield, Edmonson,
Blum, Stewart & Pandya, 1994, p. 592).
Post educational intervention included “The Knowledge and Attitudes Survey
Regarding Pain” tool which was administered to the nursing staff on the oncology unit using
Survey Monkey© to assess improvement.
Data Analysis
Forty-five nurses are employed and work day, evening or night shifts, 26 nurses
participated in the pre-survey. The average score on these surveys was 78%. The lowest score
was 62% with the highest score 94%. The questions that scored less than 80 % were used to

33MANAGING CANCER PAIN
provide guidance in creating the educational content. The lowest scoring questions reflected a
gap in knowledge pertaining to medication conversions, appropriate medication use and
assessment of pain.
Pre-test ResultsMean: 78%Standard Deviation: 7%N: 26
The post survey was completed by seventeen nurses with an increase in the total score of
12 %. The lowest score for the post survey was a 71% with the highest being 100%.

34MANAGING CANCER PAIN
Post- Test ResultsMean: 90%Standard Deviation: 9%N: 17
Measurement
Survey results were analyzed following the guidelines established by Ferrell and
McCaffery (2014) who have recommended the following in terms of analysis of the “The
Knowledge and Attitudes Survey Regarding Pain” tool,
“Regarding analysis of data: We have found that it is most helpful to avoid
distinguishing items as measuring either knowledge or attitudes. Many items
such as one measuring the incidence of addiction really measures both knowledge
of addiction and attitude about addiction. Therefore, we have found the most
benefit to be gained from analyzing the data in terms of the percentage of
complete scores as well as in analyzing individual items. For example, we have
found it very helpful to isolate those items with the least number of correct

35MANAGING CANCER PAIN
responses and those items with the best scores to guide your educational needs”
(Ferrell & McCaffery, 2014, p. 1).
The educational intervention had met the goal of addressing some initial gaps in nursing
knowledge and attitudes of cancer pain management. Those that participated in the project
indicated improved knowledge when assessing and managing the pain reported by the patient.
Discussion
The results demonstrate that the education provided to registered nurses working on the
oncology unit improved nurses’ knowledge of how to treat cancer pain using a standardized tool
to help assess the patients’ perception of pain. As not all the staff attended the education
sessions it will be difficult to identify any changes in the HCAPHS scores that can be directly
correlated to the intervention implemented with this process improvement project.
The nurse is a vital member in providing care specific to the comfort of the patient,
which involves assessing the patient's pain and relieving their symptoms. Nurses conduct
routine evaluations of the patient's pain and use pharmacologic and nonpharmacological
interventions to alleviate the pain experience of the patient. The nurse's knowledge and attitudes
around pain have been demonstrated to be important considerations in increased patient
satisfaction regarding the management of their cancer pain. It would be helpful to implement
this intervention across the oncology service line and then send out the survey to measure nurses
understanding of how to assess pain. The lack of knowledge around the different types of pain
may be preventing better control and standardizing the education for nurses, regarding the
management of cancer pain, has the potential to improve patients’ experiences of care provided
in the acute care setting (Gustafsson & Borglin, 2013).
Limitations

36MANAGING CANCER PAIN
The initial goal of this project was to complete a series of educational in-services on
cancer pain, five sessions were offered. The education was voluntary and participation consisted
of 26 nurses for the pre-test and 17 for the post-test. A potential barrier could have been that an
education session was not offered during the night shift. Due to the increase in patient volume
the staff morale and engagement level on the unit was extremely low. Support to care for the
increased number of patients was not always available and left the nurses little time to attend
anything additional. Another barrier was that the patient satisfaction scores that were analyzed
didn’t narrow it down specifically to cancer pain, the questions assess general pain.
Ethics and Human Subject
The project was process improvement and had been approved as such by the Simmons
and South Shore Hospital IRB’s.
Plan for Dissemination
The results of this project will be shared at local and national conferences through poster
submission. An executive summary will be disseminated to all leaders and nursing staff at the
project site. This process improvement will be shared with other organizations through
publication. The gap in patient care is oncology and pain specialists are not assigned providers,
but instead consulting providers in managing cancer as a disease and its accompanying
symptoms. This model of care does not allow for those specialized in cancer and symptom
management to consistently support the care of these patients. Hospital and service line leaders
have been meeting to discuss how this model can be changed to improve patient care. This
improved symptom management program would ultimately decrease length of stay and
readmission rates.
Conclusion

37MANAGING CANCER PAIN
Cancer pain is a common symptom related to this devastating diagnosis. Based on its
complexity, clinicians are faced with a difficult task of assessing this symptom and providing
relief allowing the patient to have improved quality of life. Through this comprehensive process
improvement project, it is evident that the standardization in the nurses knowledge about cancer
pain and their responsiveness to patients must be improved. Learning the nurses’ perceptions
about caring for cancer patients in pain and their ability to address the needs of those patients is a
significant step in improving the quality of care provided.
Pain management depends on the relationship between the nurse and patient and how
they interact. Patients who were involved in their care had reported fewer barriers to reaching a
preset goal and having adequate pain relief. Nurses need to have a comprehensive understanding
of the patient’s illness and the patient needs to be involved in the decision making process where
an alliance in addressing this devastating symptom is formed. The end goal being that the nurses
care about the new tools that were introduced into their practice and the improved knowledge
ultimately improves the care provided.
The intent of this project was to provide nurses with an advanced understanding of the
many facets of cancer pain management and the importance of their role in managing this
complex symptom. Goals were met in involving the nurses in the development of the education
and bridging the gap in nursing practice and patient outcomes. Future plans for the
implementation of this education will lead to an improvement of patient pain management
outcomes.

38MANAGING CANCER PAIN
References
Baker, D. (2018). Statement on pain management. Retrieved from
http://www.jointcommission.org/joint_commission_statement_on_pain_management/
Bartoszczyk, D., & Gilbert-White, S. (November 2015). Interventions for nurse-related barriers
in cancer pain management. Oncology Nursing Forum, 6, 634-641. https://doi.org/
Bhatnagar, A. (October 2017). Complementary therapies for symptom management in cancer
patients. Journal of Palliative Care, 23,468-479.
Bhatia, R., Gibbins, J., & Forbes, K. (March 2, 2014). “We talk about it as though we’re thinking
about the same thing.” healthcare professionals’ goals in the management of pain due to
advanced cancer: a qualitative study. Support Cancer Care, 22, 2067-2073.
http://dx.doi.org/DOI 10.1007/s00520-014-191-6
Boveldt, N., Vernooij-Dassen, M., Burger, N., IJsseldijk, M., Vissers, K., & Engels, Y. (2013).
Pain and its interference with daily activities in medical oncology patients. Pain
Physician Journal, 16, 379-389.
Brant, J., Potter, C., Tavernier, S., & Beck, S. ( November 2012). Pain care quality and outcomes
in U.S. inpatient oncology units. Oncology Nursing Society Connections: Advancing
Care Through Science, https://doi.org/Retrieved from
Brown, C. (2014, April 1, 2014). The iowa model of evidence-based practice to promote quality
care: an illustrated example in oncology nursing. Clinical Journal of Oncology Nursing,
18, 157-159. https://doi.org/Retrieved from

39MANAGING CANCER PAIN
Canivet, D., Delvaux, N., Gibon, A., Brancart, C., Slachmuylder, J., & Razavi, D. ( April 9,
2014). Improving communication in cancer pain management nursing: a randomized
controlled study assessing the efficacy of a communication skills training program.
Support Cancer Care, 3311-3320. https://doi.org/Retrieved from
Centers for Medicare & Medicaid. (2017). http://www.cms.gov
Chu, W., Dialla, P., Roignot, P., Bone-Lepinoy, M., Poillot, M., Coutant, C., ... Dabakuyo-Yonil,
T. (2016, February 9, 2016). Determinants of quality of life among long-term breast
cancer survivors. Quality of Life Research, 1981-1990. https://doi.org/DOI
10.1007/s11136-016-1248-z
Cleeland, C. (2009). The Brief Pain Inventory User Guide. Houston, Texas
Cleeland, C., Gonin, R., Hatfield, A., Edmonson, J., Blum, R., Stewart, J., & Pandya, K. ( March
3, 1994). Pain and its treatment in outpatients with metastatic cancer. New England
Journal of Medicine, 592-596. http://dx.doi.org/DOI:10.1056/NEJM199403033300902
Cziraki, K., & Laschinger, H. (2015). Leader empowering behaviors and work engagement: the
mediating role of structural empowerment. Nursing Leadership, 28, 10-22.
Doody, C., & Doody, O. ( June 7, 2011). Introducing evidence into nursing practice using the
iowa model. British Journal of Nursing, 20(), 661-664. https://doi.org/Retrieved from
Drake, G., & Williams, A. (February 2017). Nursing education interventions for managing acute
pain in hospital settings: a systematic review of clinical outcomes and teaching methods.
Pain Management Nursing, 18, 3-15. https://doi.org/Retrieved from
Eaton, L., Meins, A., Mitchell, P., Voxx, J., & Doorenbos, A. (March 2015). Evidence-based
practice beliefs and behaviors of nurses providing cancer pain management: a mixed-
methods approach. Oncology Nursing Forum, 42, 165-173.

40MANAGING CANCER PAIN
ECOG-ACRIN Cancer Research Group. (2016). ecog-acrin.org/resources/ecog-performance-
status
Ferlay J, Soerjomataram I, Dikshit R, et al.: Cancer incidence and mortality worldwide: sources,
methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136(5): E359–86.
Ferrell, B., & McCaffery, M. (2014). The knowledge and attitudes survey regarding pain
(KASRP). Retrieved from prc.coh.org
Fisherman, S., Arwood, E., Chou, R., Herr, K., Murinson, B., Watt-Watson, J., ... Strassels, S.
(2013). Core competencies for pain management: results of an interprofessional
consensus summit. Pain Medicine, 14, 971-981.
Fourie, I., & Nesset, V. (2017). An exploratory review of research on cancer pain and
information-related needs: what (little) we know in proceedings of ISIC, the information
behavior conference. Information Research, 22(1-30), 1-30. Retrieved from http:
InformationR.net/ir/22-1/isic/isic1621.html
Gallagher, E., Rogers, B., & Brant, J. (2017). Cancer-related pain assessment: monitoring the
effectiveness of interventions. Clinical Journal of Oncology Nursing, 21(3), 1-11.
https://doi.org/Retrieved from
Garcia, A., Whitehead, D., & Winter, H. (2015). Oncology nurses’ perception of cancer pain: a
qualitative exploratory study. Nursing Praxis of New Zealand, 31, 27-32.
http://dx.doi.org/Retrieved from
Glattacker, M., Heyduck, K., & Meffert, C. (2012). Illness beliefs, treatment beliefs and
information need as starting points for patient information- Evaluation of an intervention
for patients with chronic back pain. Patient Education & Counseling, 86, 378-389.

41MANAGING CANCER PAIN
Greco MT, Roberto A, Corli O, et al.: Quality of cancer pain management: an update of a
systematic review of under treatment of patients with cancer. J Clin
Oncol. 2014;32(36):4149–54. 10.1200/JCO.2014.56.0383
Grieve, S., Adams, J., & McCabe, C. (2016). ’What i really needed was the truth’: exploring the
information needs of people with complex regional pain syndrome. Musculoskeletal
Care, 14, 15-25. https://doi.org/Retrieved from
Gustafsson, M., & Borglin, G. (2013). Can a theory-based educational intervention change
nurses’ knowledge and attitudes concerning cancer pain management? a quasi-
experimental design. BMC Health Services Research, 13(328), 1-11.
http://dx.doi.org/Retrieved from
Hovind, I., Bredal, I., & Dihle, A. (2013). Women’s experience of acute and chronic pain
following breast cancer surgery. Journal of Pain and Symptom Management, 26, 1044-
1052. https://doi.org/Retrieved from
Hye Kwon, J., Yong Oh, S., Chisholm, G., Lee, J., Jin Lee, J., Woo Park, K., ... Ho Song, H.
(2013). Predictors of high score patient-reported barriers to controlling cancer pain: a
preliminary report. Support Cancer Care, 1175-1183. https://doi.org/Retrieved from
Koller, A., Miaskowski, C., De Geest, S., Optiz, O., & Spichiger, E. (August 2, 2012). A
systematic evaluation of content, structure, and efficacy of interventions to improve
patients’ self-management of cancer pain. Journal of Pain and Symptom Management,
44, 264-285. https://doi.org/Retrieved from
Koppel, J., Virkstis, K., Strumwasser, S., Katz, M., & Boston-Fleischhauer, C. (2016).
Broadening access to nontraditional development opportunities to drive frontline

42MANAGING CANCER PAIN
engagement. Journal of Nursing Administration, 46, 61-62. https://doi.org/Retrieved
from
Kritsonis, A. (2005). Comparison of change theories. International Journal of Scholarly
Academic Intellectual Diversity, 8(1).
Kwon, J. (2014). Overcoming barriers in cancer pain management. Journal of Clinical
Oncology, 32, 1727-1733. https://doi.org/Retrieved from
Lewin, K. (1947). Frontiers in group dynamics. In Cartwright, D. (Ed.), Field theory in social
science. London, England: Social Science Paperbacks.
Mahoney, D. (2017). Revised HCAHPS pain management questions: what you need to know.
Industry Edge A Press Ganey Publication, 1-2. Retrieved from
www.pressganey.com/resources/industry-edge
Morales-Fernandez, A., Morales-Asencio, J., Canca-Sanchez, J., Moreno-Martin, G., & Vergara-
Romero, M. (2016). November 19, 2016. Journal of Advanced Nursing, 72, 1182-1190.
https://doi.org/Doi:10.1186/ISRCTN95299159
Olsen, L., Goolsby, A., & McGinnis, M. (2009). IOM roundtable on evidence-based medicine:
leadership commitments to improve value in health care. Retrieved from
ncbi.nlm.nih.gov
Overcash, J., Hanes, D., Birkhimer, D., & Askew, T. (August 2013). Pain intensity and pain
management of hospitalized patients with cancer: an opportunity for improvement.
Clinical Journal of Oncology Nursing, 17, 365-368. https://doi.org/Retrieved from
Palalogos, R., Mocanu, A., Balacescu, L., Nemes, A., Rajcsanyi, R., Jozsef, T., ... Burz, C.
(December,2012). The assessment of cancer pain treatment using the pain management

43MANAGING CANCER PAIN
index in hospitalized patients with cancer: a pilot study. Journal of Radiotherapy and
Medical Oncology, 17, 64-68.
Riley, B., Dearmon, V., Mestas, L., & Buckner, E. (2016). Frontline nurse engagement and
empowerment characteristics and processes for building leadership capacity. Nursing
Administration, 40, 325-333. Retrieved from
Scott, J. (2015, November 3, 2015). Creating engagement through purpose and meaning. Nursing
Leadership, 28, 53-55. https://doi.org/Retrieved from
Singh, H., Banpal, R., & Singh, B. (2017). Assessment of adequacy of pain management and
analgesic use in patients with advanced cancer using the brief pain inventroy and pain
management index calculation. Journal of Global Oncology, 235-241.
Smith, T., & Saiki, C. ( October 2015). Cancer Pain Management. Cancer Pain Management,
1428-1438. https://doi.org/Retrieved from
Swarm, R., Abernethy, A., Anghelescu, D., Benedetti, C., Blinderman, C., Boston, B., ...
Weinstein, S. (September, 2010). Adult cancer pain clinical practice guidelines in
oncology. Journal of the National Comprehensive Cancer Network, 8, 1046-1086.
The W. Edwards Deming Institute. (2016). Retrieved from https://deming.org/management-system/pdsacycle
Well, K., Manuel, M., & Cunning, G. (2011). Changing the model of care deliver: nurses’
perceptions of job satisfaction and care effectiveness. Journal of Nursing Management, 6,
777-785.
World Health Organization. (n.d.). www.who.int/cancer/palliative/painladder/en/
World Health Organization. (2016). http://www.who.int/cancer/palliative/painladder/en
(http://www.who.int/cancer/palliative/painladder/en)

44MANAGING CANCER PAIN
Appendix A
July 2014 The “Knowledge and Attitudes Survey Regarding Pain” tool can be used to assess nurses and
other professionals in your setting and as a pre and post test evaluation measure for educational programs. The tool was developed in 1987 and has been used extensively from 1987 - present. The tool has been revised over the years to reflect changes in pain management practice.
Regarding issues of reliability and validity: This tool has been developed over several years. Content validity has been established by review of pain experts. The content of the tool is
derived from current standards of pain management such as the American Pain Society, the World Health Organization, and the National Comprehensive Cancer Network Pain Guidelines. Construct validity has been established by comparing scores of nurses at various levels of expertise such as students, new graduates, oncology nurses, graduate students, and senior pain experts. The tool was identified as discriminating between levels of expertise. Test-retest reliability was established (r>.80) by repeat testing in a continuing education class of staff nurses (N=60). Internal consistency reliability was established (alpha r>.70) with items reflecting both knowledge and attitude domains.
Regarding analysis of data: We have found that it is most helpful to avoid distinguishing items
as measuring either knowledge or attitudes. Many items such as one measuring the incidence of addiction really measures both knowledge of addiction and attitude about addiction. Therefore, we have found the most benefit to be gained from analyzing the data in terms of the percentage of complete scores as well as in analyzing individual items. For example, we have found it very helpful to isolate those items with the least number of correct responses and those items with the best scores to guide your educational needs.
Enclosed for your use is a copy of our instrument and an answer key. You may use and
duplicate the tool for any purpose you desire in whole or in part. References to some of our studies which have included this tool or similar versions are included below. We have received hundreds of

45MANAGING CANCER PAIN
requests for the tool and additional use of the tool can be found in other published literature. We also acknowledge the assistance of several of our pain colleagues including Judy Paice, Chris Pasero, and Nessa Coyle in the revisions over the years. If using or publishing the tool results please cite the reference as “Knowledge and Attitudes Survey Regarding Pain” developed by Betty Ferrell, RN, PhD, FAAN and Margo McCaffery, RN, MS, FAAN, (http://prc.coh.org), revised 2014.
We hope that our tool will be a useful aid in your efforts to improve pain management in your
setting. Sincerely,
Betty R. Ferrell, RN, PhD, FAAN Margo McCaffery, RN, MS, FAAN Research Scientist Lecturer and Consultant
7/14 References:
Ferrell BR, McCaffery M, Rhiner M. (1992). "Pain and addiction: An urgent need for changing nursing education." Journal of Pain and Symptom Management, 7(2): 117-124.
Ferrell BR, Grant M, Ritchey KJ, Ropchan R, Rivera LM (1993). "The Pain Resource Nurse Training program: A unique approach to pain management." Journal of Pain and Symptom Management, 8(8):
549-556
McCaffery M, Ferrell BR (1994). "Understanding opioids & addiction." Nursing 94, 24(8): 56-59.
Ferrell BR, McCaffery M (1997). "Nurses' knowledge about Equianalgesic and opioid dosing." Cancer Nursing, 20(3): 201-212
McCaffery M, Ferrell BR (1997). "Nurses' knowledge of pain assessment and management: How much progress have we made?" Journal of Pain and Symptom Management, 14(3): 175-188
McCaffery M, Ferrell BR (1997). "Influence of professional vs. personal role on pain assessment and use of opioids." The Journal of Continuing Education in Nursing, 28(2): 69-77
Ferrell BR, Virani R (1998). "Institutional commitment to improved pain management: Sustaining the effort." Journal of Pharmaceutical Care in Pain and Symptom Control, 6(2): 43-55
McCaffery M, Ferrell BR (1999). "Opioids and pain management - What do nurses know?" Nursing 99, 29(3): 48-52

46MANAGING CANCER PAIN
McCaffery M, Ferrell BR, Pasero C (2000). "Nurses' personal opinions about patients' pain and their effect on recorded assessments and titration of opioid doses." Pain Management Nursing, 1(3): 79-87
Borneman T, Sun V, Ferrell BR, Koczywas M, Piper B, & Uman G. (2006). Educating patients about pain management. Oncology Nurse Edition, 20(10), 41-49.
Ferrell BR. (2007). Reducing barriers to pain assessment and management: An institutional perspective. Journal of Palliative Medicine, 10(1S), S15-S18. DOI: 10.1089/jpm.2007.9828. (Pages 15-18 in Optimizing Opioid Management in Palliative Care article).
American Pain Society. (2008). Principles of Analgesic Use in the Treatment of Acute Pain and Cancer Pain Guidelines, 6th Edition.
Borneman T, Koczywas M, Chih-Yi Sun V, Piper BF, Uman G, & Ferrell BR. (2010). Reducing patient barriers to pain and fatigue management. Journal of Pain and Symptom Management, 39(3), 486.501. DOI: 10.1016/j.jpainsymman.2009.08.007.
BornemanT, Koczywas M, Sun V, Piper B, Smith-Idell C, Laroya B, Uman G, & Ferrell BR.
(2011). Effectiveness of a clinical intervention to eliminate barriers to pain and fatigue management in
oncology. Journal of Palliative Medicine, 14(2), 197-205. DOI: 10.1089/jpm.2010.0268. National Comprehensive Cancer Network. (2014). NCCN Clinical Practice Guidelines®
National Comprehensive Cancer Network, Inc, All Rights Reserved.
Knowledge and Attitudes Survey Regarding Pain
True/False – Circle the correct answer.
T F 1. Vital signs are always reliable indicators of the intensity of a patient’s pain.
T F 2. Patients who can be distracted from pain usually do not have severe pain.
T F 3. Patients may sleep in spite of severe pain.
T F 4. Aspirin and other nonsteroidal anti-inflammatory agents are NOT effective analgesics for painful bone metastases.
T F 5. Respiratory depression rarely occurs in patients who have been receiving stable doses of opioids over a
period of months.
T F 6. Combining analgesics that work by different mechanisms (e.g., combining an NSAID with an opioid) may result in better pain control with fewer side effects than using a single analgesic agent.
T F 7. The usual duration of analgesia of 1-2 mg morphine IV is 4-5 hours.
T F 8. Opioids should not be used in patients with a history of substance abuse.

47MANAGING CANCER PAIN
T F 9. Elderly patients cannot tolerate opioids for pain relief.
T F 10. Patients should be encouraged to endure as much pain as possible before using an opioid.
T F 11. Patients’ spiritual beliefs may lead them to think pain and suffering are necessary.
T F 12. After an initial dose of opioid analgesic is given, subsequent doses should be adjusted in accordance with the individual patient’s response.
T F 13. Vicodin (hydrocodone 5 mg + acetaminophen 300 mg) PO is approximately equal to 5-10 mg of morphine
PO.
T F 14. If the source of the patient’s pain is unknown, opioids should not be used during the pain evaluation period, as this could mask the ability to correctly diagnose the cause of pain.
T F 15. Anticonvulsant drugs such as gabapentin (Neurontin) produce optimal pain relief after a single dose.
T F 16. Benzodiazepines are not effective pain relievers and are rarely recommended as part of an
analgesic regiment.
T F 17. Narcotic/opioid addiction is defined as a chronic neurobiologic disease, characterized by behaviors that include one or more of the following: impaired control over drug use, compulsive use, continued use despite harm, and craving.
T F 18. The term ‘equianalgesia’ means approximately equal analgesia and is used when referring to the doses of
various analgesics that provide approximately the same amount of pain relief.
T F 19. Sedation assessment is recommended during opioid pain management because excessive sedation precedes opioid-induced respiratory depression.
Multiple Choice – Place a check by the correct answer.
20. The recommended route of administration of opioid analgesics for patients with persistent cancer-related pain is
a. intravenous b.intramuscular c.subcutaneous
d.oral e.rectal
21.The recommended route administration of opioid analgesics for patients with brief, severe pain
of sudden onset such as trauma or postoperative pain is a. intravenous
b. intramuscular c. subcutaneous d. oral e. rectal
22.Which of the following analgesic medications is considered the drug of choice for the treatment
of prolonged moderate to severe pain for cancer patients? a. codeine b. morphine

48MANAGING CANCER PAIN
c. meperidine d. tramadol
23. A 30 mg dose of oral morphine is approximately equivalent to:
a. Morphine 5 mg IV b. Morphine 10 mg IV c. Morphine 30 mg IV d. Morphine 60 mg IV
24. Analgesics for post-operative pain should initially be given
a. around the clock on a fixed schedule b. only when the patient asks for the medication c. only when the nurse determines that the patient has moderate or greater discomfort
25. A patient with persistent cancer pain has been receiving daily opioid analgesics for 2 months. Yesterday the
patient was receiving morphine 200 mg/hour intravenously. Today he has been receiving 250 mg/hour intravenously. The likelihood of the patient developing clinically significant respiratory depression in the absence of new comorbidity is
a. less than 1% b. 1-10% c. 11-20% d. 21-40% e. > 41%
26. The most likely reason a patient with pain would request increased doses of pain medication is
a. The patient is experiencing increased pain. b. The patient is experiencing increased anxiety or depression. c. The patient is requesting more staff attention. d. The patient’s requests are related to addiction.
27. Which of the following is useful for treatment of cancer pain?
a. Ibuprofen (Motrin) b. Hydromorphone (Dilaudid) c. Gabapentin (Neurontin) d. All of the above
28. The most accurate judge of the intensity of the patient’s pain is
a. the treating physician b. the patient’s primary nurse c. the patient d. the pharmacist e. the patient’s spouse or family
29. Which of the following describes the best approach for cultural considerations in caring for patients in pain: a. There are no longer cultural influences in the U.S. due to the diversity of the population. b. Cultural influences can be determined by an individual’s ethnicity (e.g., Asians are stoic, Italians are
expressive, etc). c. Patients should be individually assessed to determine cultural influences. d. Cultural influences can be determined by an individual’s socioeconomic status (e.g., blue collar workers
report more pain than white collar workers).
30. How likely is it that patients who develop pain already have an alcohol and/or drug abuse problem?
< 1% 5 – 15% 25 - 50% 75 - 100%

49MANAGING CANCER PAIN
31. The time to peak effect for morphine given IV is _____a. 15 min.
_____b. 45 min. _____c. 1 hour _____d. 2 hours
32. The time to peak effect for morphine given orally is _____a. 5 min.
_____b. 30 min. _____c. 1 – 2 hours _____d. 3 hours
33. Following abrupt discontinuation of an opioid, physical dependence is manifested by the following: _____ a. sweating, yawning, diarrhea and agitation with patients when the opioid is abruptly discontinued.
_____ b. Impaired control over drug use, compulsive use, and craving. _____ c. The need for higher doses to achieve the same
effect. _____ d. a and b
34. Which statement is true regarding opioid induced respiratory depression: _____ a. More common several nights after surgery due to accumulation of opioid.
_____ b. Obstructive sleep apnea is an important risk factor. _____ c. Occurs more frequently in those already on higher doses of opioids before
surgery. _____ d. Can be easily assessed using intermittent pulse oximetry.

Appendix B
South Shore Hospital, Inc. infoEDGE
INPATIENT REPORTGlobalDOMAIN Question n %
AllDB
N = 2279
LargePG DB
N = 1619
300-449Bed GrpN = 248
SSHSCompariN = 12
PAIN MANAGEMENT
Never 0.8 1.0 1.1 1.1 0.7
Sometimes 6.6 5.6 6.0 5.9 5.6
Usually 20.4 21.9 21.8 23.1 21.9
Always 72.2 70.9 70.3 69.8 71.8
Total 131 Top Box
%ile rank 59 63 68 61
Pain well controlledNever 2 1.5 1.2 1.3 1.2 1.0
Sometimes 8 6.2 6.9 7.3 7.1 7.0
Usually 38 29.2 28.5 28.1 29.4 28.4
Always Total
82130
63.1 62.8 62.5 62.0 63.7 34
Top Box%ile rank 53 54 54
Staff do everything help with pain
Never 0 0 0.8 0.9 0.9 0.5
Sometimes 9 7.0 4.3 4.6 4.6 4.3
Usually 15 11.6 15.3 15.6 16.9 15.4
Always Total
105129
81.4 78.9 78.2 77.5 79.9 55
Top Box%ile rank 65 72 76

51MANAGING CANCER PAIN
Appendix C
Date:Study Name: ________________________________
___________________________________________1903 (month) (day) (year)
Protocol #: _________________________________Subject's Initials : ________________
PI:
________________________________________
Study Subject #:Revision: 07/01/05PLEASE USEBLACK INK PEN
Brief Pain Inventory (Short Form)1. Throughout our lives, most of us have had pain from time to time (such as minor headaches,
sprains, and toothaches). Have you had pain other than these everyday kinds of pain today?
Yes No
2. On the diagram, shade in the areas where you feel pain. Put an X on the area that hurts the most.
3. Please rate your pain by marking the box beside the number that best describes your pain at its worst in the last 24 hours.
0 1 2 3 4 5 6 7 8 9 10No Pain As Bad AsPain You Can Imagine
4. Please rate your pain by marking the box beside the number that best describes your pain at its
Front Back
/ /

52MANAGING CANCER PAIN
least in the last 24 hours.0 1 2 3 4 5 6 7 8 9 10
No Pain As Bad AsPain You Can Imagine
5. Please rate your pain by marking the box beside the number that best describes your pain on the
average.
0 1 2 3 4 5 6 7 8 9 10No Pain As Bad AsPain You Can Imagine
6. Please rate your pain by marking the box beside the number that tells how much pain you have right now.
0 1 2 3 4 5 6 7 8 9 10No Pain As Bad AsPain You Can Imagine
Copyright 1991 Charles S. Cleeland, PhD
Page 1 of 2 Pain Research Group All rights reserved
Date:Study Name: ________________________________
___________________________________________1903 (month) (day) (year)
Protocol #: _________________________________Subject's Initials : ________________
PI: ________________________________________
Study Subject #:Revision: 07/01/05PLEASE USE
BLACK INK PEN
8. In the last 24 hours, how much relief have pain treatments or medications provided? Please mark the box below the percentage that most shows how much relief you have received.
7. What treatments or medications are you receiving for your pain?
0% 10%
20% 30% 40% 50% 60% 70% 80% 90% 100%
No Complete Relief Relief
9. Mark the box beside the number that describes how, during the past 24 hours, pain has interfered
/ /

MANAGING CANCER PAIN 53
with your:
A. General ActivityDoes Not Interfere
Completely Interferes
0 1 2 345678910
0 1 2 3 4 5 6 7 8 9 10Does Not Interfere
Completely Interferes
B. Mood
C. Walking ability
0 1 2 3 4 5 6 7 8 9 10Does Not Interfere
Completely Interferes
D. Normal Work (includes both work outside the home and housework)5 6 7 8 9 10
CompletelyInterferes
5 6 7 8 9 10
CompletelyInterferes
5 6 7 8 9 10
CompletelyInterferes
5 6 7 8 9 10CompletelyInterferes
Copyright 1991 Charles S. Cleeland, PhD
Page 2 of 2 Pain Research Group All rights reserved
InterfereDoes Not
InterfereDoes Not
InterfereDoes Not
InterfereDoes Not
Enjoyment of lifeG.
43210
43210
43210
43210
SleepF.
E. Relations with other people

MANAGING CANCER PAIN 54
Appendix D
Oken M., Creech, R., Tormey, D, et al. Toxicity and response criteria of the Eastern Cooperative
Oncology Group. Am J Clin Oncol. 1982; 5:649-655

MANAGING CANCER PAIN 55
Appendix E

MANAGING CANCER PAIN 56
Appendix F
(DFCI/Brigham & Women’s Pain Management Guide 2010)

MANAGING CANCER PAIN 57
Appendix G
Simmons CollegeInstitutional Review Board
Worksheet to determine if the project is research or performance improvement (aka Quality Improvement)
Researcher's Name: Jennifer Deneault MSN, RN, OCN
DepartmenJProgram: DNP
E-Mail:[email protected] Phone:
Project Title: Managing Cancer Pain
508-813-2318
Is the project's purpose SOLELY to evaluate whether putting research evidence into practice improves quality measures? No C] Yes
Will the data you gather be sensitive in nature? (i.e. have the ability to cause emotional distress, potentially put someone in finmcial, legal, physical or other harm)?No Yes (please explain)
Do you intend the data that will be collected to be of widespread interest or usefulness to a larger audience than the subjects you collect data from, or widespread interest beyond your deparünent? No Yes (please explain)
Will you be publishing or presenting the results outside of Simmons College?No Yes [3 If yes: as a PI project or as a research study? perhaps, if so then it would be as a PI project
Will subjects to be used in the project come from a vulnerable population including minors under the age of 18, economically and/or educationally disadvantaged persons, prisoners, pregnant women, fetuses, the seriously ill, persons with mental disabilities, or incompetent individuals?No Yes
PROJECT DESCRIPTION: Please attach the description ofyour PI/QI project to this form. Sufficient detail should be provided so that we can determine the level of risk involved as well as the purpose of the project.
Student Signature:
Faculty/Staff Signature:
Accepted research) or Denied [3 (this is resemx;h)

MANAGING CANCER PAIN 58
Next action to be taken: Submit
separate IRB
Authorized Signature:

MANAGING CANCER PAIN 59
Appendix H

MANAGING CANCER PAIN 60

MANAGING CANCER PAIN 61

MANAGING CANCER PAIN 62

MANAGING CANCER PAIN 63

MANAGING CANCER PAIN 64

MANAGING CANCER PAIN 65

MANAGING CANCER PAIN 66
Appendix I
NCCN Guidelines