Embed Size (px)
DESCRIPTION
Managing Menstrual Abnormalities. Jan Shepherd, MD, FACOG. Objectives. Identify common causes of menstrual abnormalities and discuss their pathophysiology. Describe office, laboratory, and additional evaluation of menstrual abnormalities. - PowerPoint PPT Presentation
Citation preview

Managing Menstrual AbnormalitiesManaging Menstrual Abnormalities
Jan Shepherd, MD, FACOG

ObjectivesObjectives
• Identify common causes of menstrual abnormalities and discuss their pathophysiology.
• Describe office, laboratory, and additional evaluation of menstrual abnormalities.
• Identify management options for acute and chronic abnormal uterine bleeding.


The Normal Menstrual PeriodThe Normal Menstrual Period
• Blood loss < 80 cc (average 30-35 cc)
• Duration of flow 2-7 days (average 4 days)
• Cycle length 21-35 days (average 29 days)
• Mid-cycle spotting can occur with ovulation, but other bleeding between periods is abnormal
Consider using menstrual calendar to evaluate

Abnormal Uterine Bleeding (AUB)Abnormal Uterine Bleeding (AUB)
• Any change in menstrual period– Flow (menorrhagia)– Duration– Frequency (polymenorrhea) – Bleeding between cycles (metrorrhagia)
• 20 million office visits/year
• 25% of visits to women’s health practitioners

Causes of Abnormal Uterine BleedingCauses of Abnormal Uterine Bleeding
• Complications of Pregnancy– Miscarriage/Retained tissue– Ectopic pregnancy– Trophoblastic disease (e.g. molar pregnancy)
• Pelvic Pathology– Vaginal/Vulvar – Cervical – infection, polyp, dysplasia/Ca – Uterine – endometrial polyps, hyperplasia/Ca

Uterine Fibroids (Leiomyomata)Uterine Fibroids (Leiomyomata)
• Occur in 20-40% of reproductive-aged women
• Rule out other causes!• Diagnosis based on
physical exam• Ultrasound for
– Rule out submucous– Uncertain adnexal status– Worrisome interval growth

Coagulation DisordersCoagulation Disorders
• Inherited coagulopathy is the cause of AUB in 18% of Caucasian and 7% of African-American women
• Most commonly presents in adolescence• Von Willebrand’s disease is the #1etiology
– Occurs in ~1% of Caucasians– Order coagulation screen and Von Willebrand’s
factor (ristocetin cofactor assay) or PFA-100– Consider referral to hematologist

Common Medical Causes of AUBCommon Medical Causes of AUB
• Endocrinopathies– Thyroid most common
• Systemic diseases– Blood dyscrasias (e.g. leukemia, ITP)– Liver or kidney disease
• Medications– Hormones, including contraception, HRT, corticosteroids– Psychotropic drugs– Anticoagulants– Herbs and botanicals – esp. soy, ginseng, ginkgo

Dysfunctional Uterine Bleeding (DUB)Dysfunctional Uterine Bleeding (DUB)
• No anatomic, systemic or iatrogenic cause• Presumed disruption in normal ovarian function
– Usually anovulation (“Anovulatory bleeding”)• Continuous estrogen exposure causes excessive
endometrial proliferation; no progesterone to control and stabilize this growth uncoordinated shedding
• DUB usually irregular cycles, heavy, and long duration• Unopposed estrogen can lead to endometrial Ca

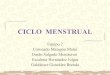
The Normal Menstrual CycleThe Normal Menstrual Cycle

Common Etiologies for DUBCommon Etiologies for DUB
• Perimenarche or perimenopause
• Obesity
• Stress (emotional or physical)
• Other hormone imbalance (esp. PCOS)


Checklist forChecklist forMaking the Diagnosis in AUBMaking the Diagnosis in AUB

Important Elements in History of AUBImportant Elements in History of AUB
• Onset– Gradual vs. sudden– Perimenarche, perimenopause– Temporal associations (postcoital, postpill, postpartum)
• Characteristics– Volume– Duration
• Is she ovulating?– Regularity? Variability?– Menstrual cramps? PMS?– History of infertility

Associated SymptomsAssociated Symptoms
• Systemic symptoms– Weight gain or loss– Fatigue, N&V– Fever
• Symptoms of endocrinopathy– Androgen Excess– Thyroid– Pituitary
• Symptoms of coagulopathy

Additional Focused HistoryAdditional Focused History
• Gynecologic history– Pap tests and annual exams– Past pelvic surgeries or problems
• Past Medical History– Medical illnesses– Surgeries– Medications
• Family History – Menstrual Abnormalities– Coagulopathies– Gynecologic cancers

Checklist for Physical Exam for AUBChecklist for Physical Exam for AUB
• Bruising, petechiae
• Low or high BMI
• Hirsutism or acne (Hyperandrogenism)
• Acanthosis nigricans
• Enlarged thyroid or thyroid nodule
• Galactorrhea
• Complete pelvic exam

Checklist for Laboratory Evaluation of AUBChecklist for Laboratory Evaluation of AUB
• Rule Out Pregnancy
• CBC
• TSH
• Coagulation profile if indicated (esp teenager)
• Chem screen if indicated
• 17OHP, Testosterone, and DHEAS if indicated

Additional TestingAdditional Testing
• Endometrial Biopsy (esp if DUB suspected)– > 35 years old– obese, diabetic, hypertensive – PCOS
• Findings– Proliferative vs secretory endometrium (is she ovulating?)– Simple or complex hyperplasia +/- atypia, endometrial ca– Chronic endometritis– Atrophic endometrium– Insufficient for diagnosis needs further testing

Additional TestingAdditional Testing
• Transvaginal Ultrasonography– Measure endometrial stripe (< 5 mm reassuring)– Rule out endometrial pathology, fibroids, ovarian
pathology • Saline Installation - Sonohysterography – Useful in further evaluating intracavitary abnormalities– Superior to TVS alone

Saline Installation Sonography

Additional TestingAdditional Testing
• Hysteroscopy with directed biopsy– Definitive diagnosis– Excision of endometrial polyps, submucous fibroids
• MRI– Can further characterize pelvic and intrauterine
lesions, e.g. adenomyosis vs fibroids, penetration depth of fibroids

Endometrial PolypsEndometrial Polyps
Slide courtesy of Linda Darlene Bradley, MD.

Am Fam Physician 2004;69:1915-26.Am Fam Physician 2004;69:1915-26.


Management of AUBManagement of AUB

Management of Acute AUB/DUBManagement of Acute AUB/DUB
• Can be a life-threatening emergency– Monitor Vital signs– IV fluids– Type and Crossmatch
• Estrogen - 25 mg IV q 4-6 hrs x 24 hrs or 10-20 mg po in 4 divided doses over 24 hrs
• 30-35 μg OCP, Norethindrone acetate 5 mg, or Medroxyprogesterone acetate 20 mg tid x 7, tapering to qd x 3-6 weeks

Management of Chronic AUB/DUBManagement of Chronic AUB/DUB
• General Health Measures– weight control– stress reduction– iron supplements
• NSAIDS (Antiprostaglandins) – blood loss 50-80%• NEW – Tranexamic acid – superior to NSAIDS
– Blocks plasminogen/plasmin prevents breakdown of fibrinogen preserves fibrin matrix stabilizes clots
– Two 650 mg tabs tid x 5 days per cycle– Contraindicated with thrombophilia and with OCPs

Management of Chronic AUB/DUBManagement of Chronic AUB/DUB
• Progestins (control bleeding & prevent endometrial Ca) – Oral contraceptives, if not contraindicated– Cyclic progestins (days 5-26)
• Norethindrone acetate• Medroxyprogesterone acetate
– Progestin-only contraception• Progestin-only pills• Depo Provera
– Levonorgestrel IUC
• Endometrial Ablation

LNG IUS vs Endometrial AblationLNG IUS vs Endometrial Ablation
Recent Meta-analysis Efficacy of LNG IUS Endometrial Ablation
up to 2 years after
treatment
YearYear 1
Year 3
Year 1Year 1
Year 1
Year 2
Obstet Gynecol 2009;113:1104-16.Obstet Gynecol 2009;113:1104-16.

Global Endometrial AblationGlobal Endometrial Ablation
• Indication – Idiopathic menorrhagia (pathology ruled out) in
premenopausal woman who has completed childbearing and failed hormonal therapy
• Contraindications– Pregnancy or desire for future pregnancy– Premalignant endometrial changes or endometrial carcinoma– History of classical C-section or transmural myomectomy– Uterine anomaly– Untreated PID, hydrosalpinx

Considerations for Endometrial AblationConsiderations for Endometrial Ablation
• Patient expectations– Does she understand she will still need contraception?– Will she be satisfied with reduced flow?
• 23% amenorrhea1
– 16% will need further treatment within 5 years1
• 20-40% in other series– Highest failure rate1
• Age < 45• Parity > 5
1. Obstet Gynecol 2009;113:97-106.1. Obstet Gynecol 2009;113:97-106.

Comparison of MethodsComparison of Methods
Obstet Gynecol 2006;108:990-1003.Obstet Gynecol 2006;108:990-1003.

CaseCase
• A 14-year-old Caucasian female is brought in by her mother because she has been having periods every 2 weeks for the past 3 months. Currently she has been bleeding for 2 days, is filling a pad every 3 hours, and flooding the bed overnight. Periods began at age 13 but were initially 3 months apart and not as heavy. Patient and her mother deny any past medical problems and state she is not sexually active.

AdolescentAdolescent
• Pregnancy test!
• Rule out coagulation disorder– Order CBC,coag screen and Von Willebrand’s
panel (vWF, ristocetin cofactor, PFA-100, etc.)
• OCP or Norethindrone acetate 5 mg tid x 7, tapering to qd x 3 weeks
• Consider maintenance OCP

CaseCase
• A 36-year-old Caucasian female g2p2 presents c/o bleeding constantly for over a month. The flow has varied but now fills about 5 pads per day. Her periods have been increasingly irregular, heavy, and long for the past few years. PE reveals BMI of 36, bp 140/86, pelvic exam difficult to evaluate but no gross abnormalities noted. Bright red blood seen flowing from cervical os. How will you manage this patient?

Obesity-Related AUBObesity-Related AUB
• Pregnancy test!
• Estrogen excess Consider endometrial biopsy
• Norethindrone acetate 5 mg tid x 7, tapering to qd x 3 weeks
• Consider Mirena IUC
• Consider maintenance progestin therapy: medroxyprogesterone acetate 5-10 mg or norethindrone acetate 5 mg cycle days 5-26

CaseCase
• A 49-year-old AA woman g2p2 presents c/o almost continuous bleeding for the past month. Her menses have been becoming further apart (LMP 3 months ago), heavier, and longer, but this is the worst so far. She has been having some hot flashes lately but otherwise feels well. She was told in the past that she had uterine fibroids and is currently taking medication for hypertension. Her BMI is 28.

Perimenopausal WomanPerimenopausal Woman
• Pregnancy test!
• Consider endometrial biopsy
• Norethindrone acetate 5 mg tid x 7, tapering to qd x 3 weeks
• Consider – Maintenance OCP, if not contraindicated– Maintenance progestin therapy– Levonorgestrel IUC

COCPs for PerimenopauseCOCPs for Perimenopause
• Benefits– Regulation of menses– Symptom relief– Maintenance of bone density
• Risks– Safe for nonsmokers with no CV risk factors– Incidence of VTE increases at age 40
• Exercise caution with high risk, esp. obesity

IUCs for Perimenopausal WomenIUCs for Perimenopausal Women
• Among perimenopausal women who are bleeding normally or less frequently, either the Copper IUC or the levonorgestrel IUC is acceptable
• Among women who are bleeding abnormally– Preinsertion endometrial evaluation is recommended– If no intrauterine pathology, hormone-releasing IUDs
may help control bleeding and prevent endometrial hyperplasia

Innovative Management of FibroidsInnovative Management of Fibroids
• Medical – GnRH agonists/antagonists– Aromatase inhibitors (anastrozole, letrozole)– Anti-progesterone (mifepristone)
• Interventional– Endometrial Ablation– Endoscopic myomectomy
• Hysteroscopy• Laparoscopy
– Radiologic management• Uterine artery embolization• MRI-guided focused ultrasound (ExAblate)

Amenorrhea/OligomenorrheaAmenorrhea/Oligomenorrhea

DefinitionsDefinitions
• Primary Amenorrhea – no spontaneous uterine bleeding by the age of 16
• Secondary Amenorrhea – absence of menses for 6 months or more
• Oligomenorrhea – menstrual cycle > 35 days

Causes of Primary AmenorrheaCauses of Primary Amenorrhea
• Hypothalamic/Pituitary– Constitutional– Systemic Illness– Extreme physical, nutritional, or emotional stress– PCOS
• Ovarian– Gonadal dysgenesis (esp Turner’s Syndrome)
• Anatomic– Mullerian anamolies or agenesis (e.g. absent vagina)– Imperforate hymen

Causes of Secondary AmenorrheaCauses of Secondary Amenorrhea• Pregnancy or Breast-Feeding• Hypothalamic
– Extreme physical, emotional, or nutritional stress– Systemic illness– PCOS– Obesity– Perimenarche, perimenopause
• Pituitary– Hyperprolactinemia
• Ovarian– Premature ovarian failure
• Uterine– Iatrogenic

Evaluation of Evaluation of Amenorrhea/OligomenorrheaAmenorrhea/Oligomenorrhea
• Rule Out Pregnancy• Complete H and P with focus on Weight,
Hirsutism, Galactorrhea• TSH, Prolactin• FSH, LH • Testosterone, DHEAS (if indicated)
* Treat based on etiology