Embed Size (px)
Citation preview
Mantle cell Lymphoma treatment
First line
QuickTime™ and aGIF decompressor
are needed to see this picture.
Pr Olivier Hermine MD, PhD
Department of Hematology and CNRS UMR 8147
Red cell Labex
Hôpital Necker
Paris, France
4
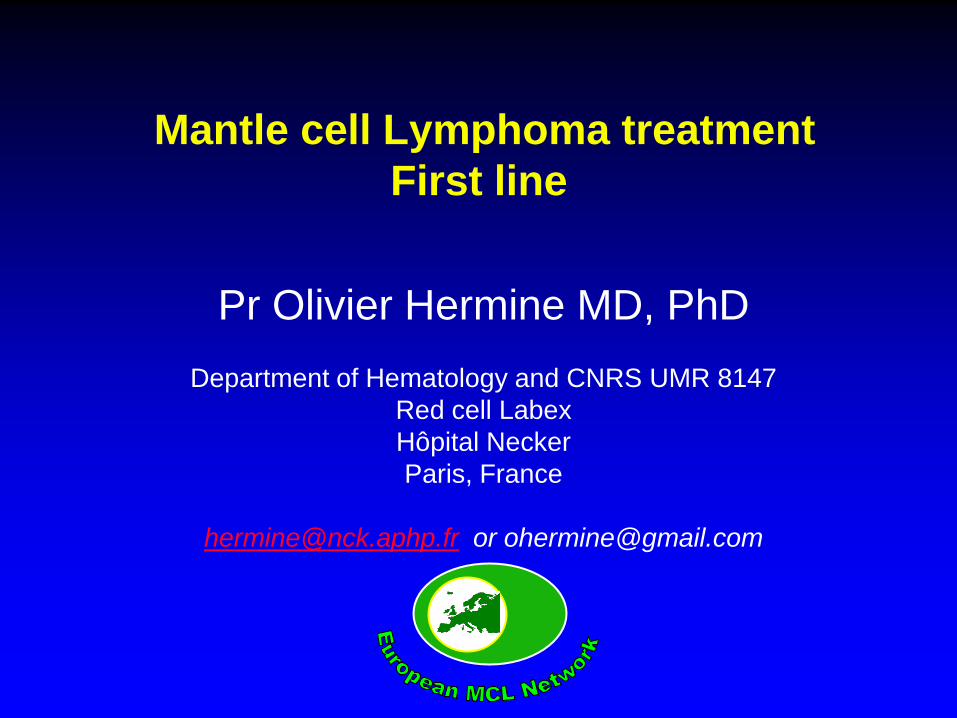
Multicenter Evaluation of MCL
Annency Criteria fulfi l led
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16
y ears
0
0,25
0,5
0,75
1
p
single agent
comb. no anthra.
comb. with anthra.
event free interval after chemotherapy in stages III + IV
Dreyling, ASCO 1999 Nickenig, Cancer 2006
CR/Cru 25%
European MCL Network Clinical course

Clinical risk factors: MIPI
Hoster, Blood 2008
Univariate risk factors
• age
• ECOG performance status
• B-symptoms
• spleen involvement
• tumor size
• leukocyte or lymphocyte count
• LDH
• hemoglobin
• albumin
• beta2-microglobulin
(PALL: PS, age, LDH, leucocyte count, Ki67)
6 ©2008 by American Society of Hematology
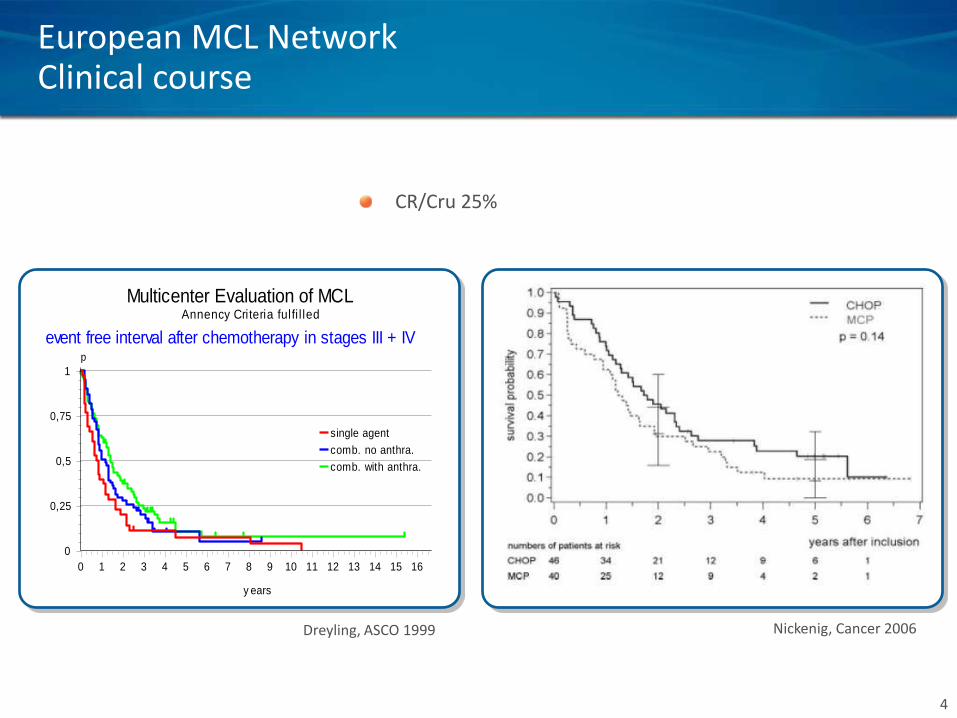
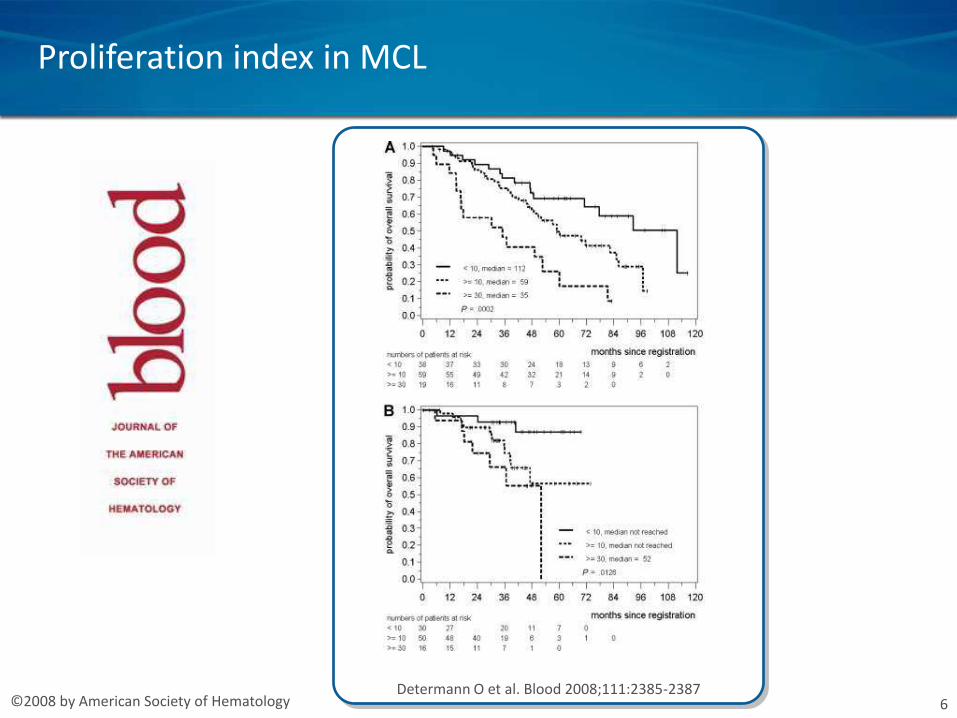
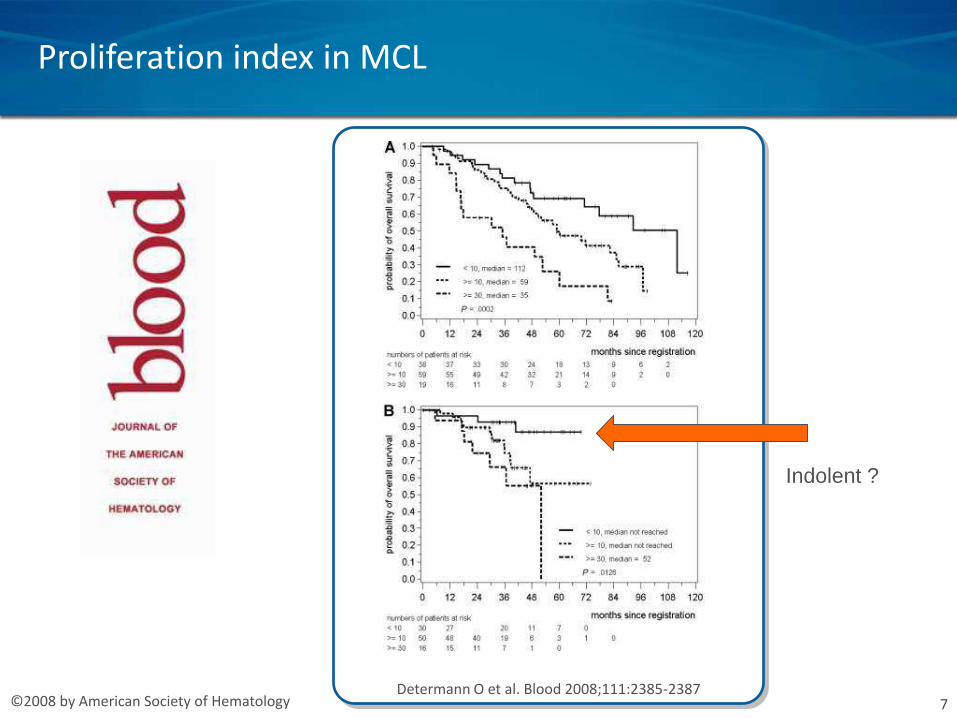
Proliferation index in MCL
Determann O et al. Blood 2008;111:2385-2387
7 ©2008 by American Society of Hematology
Proliferation index in MCL
Determann O et al. Blood 2008;111:2385-2387
Indolent ?
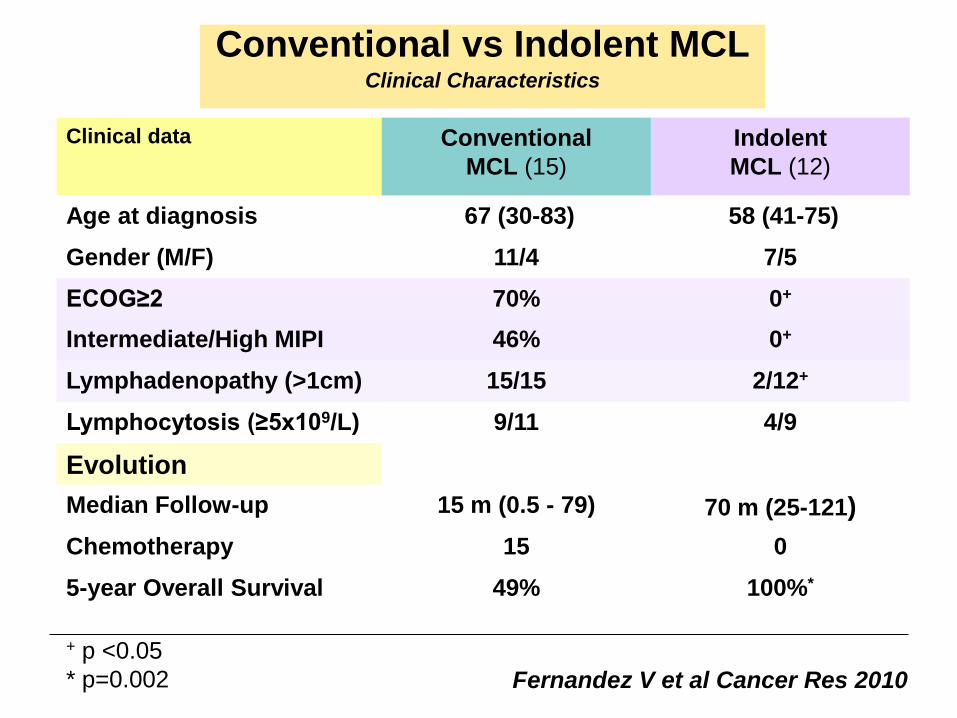
Conventional vs Indolent MCL Clinical Characteristics
Clinical data Conventional
MCL (15)
Indolent
MCL (12)
Age at diagnosis 67 (30-83) 58 (41-75)
Gender (M/F) 11/4 7/5
ECOG≥2 70% 0+
Intermediate/High MIPI 46% 0+
Lymphadenopathy (>1cm) 15/15 2/12+
Lymphocytosis (≥5x109/L) 9/11 4/9
Evolution
Median Follow-up 15 m (0.5 - 79) 70 m (25-121)
Chemotherapy 15 0
5-year Overall Survival 49% 100%*
+ p <0.05
* p=0.002 Fernandez V et al Cancer Res 2010
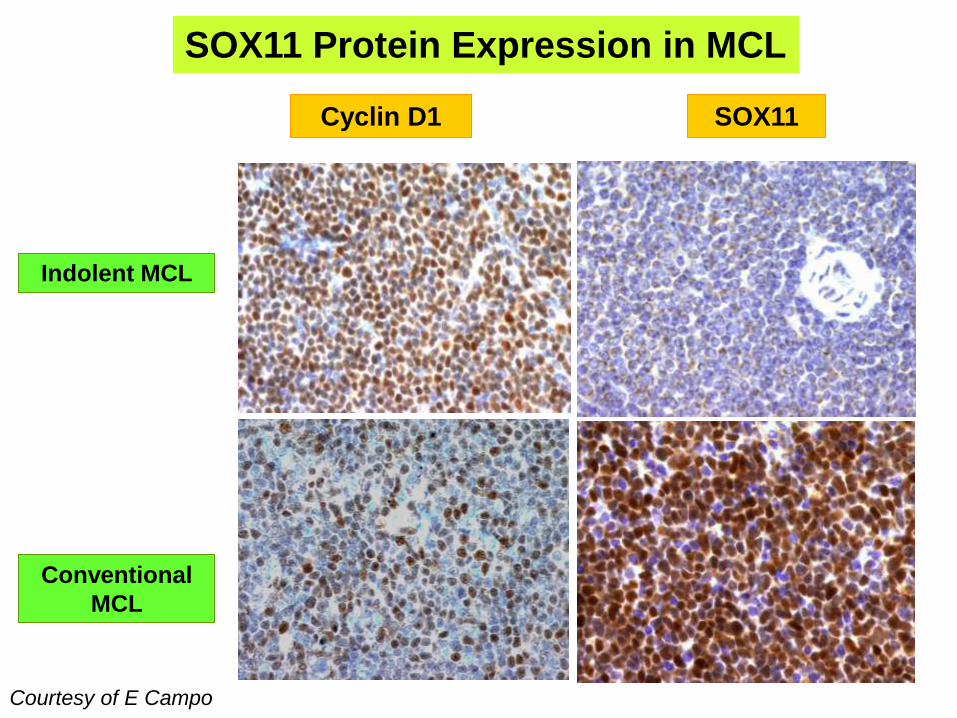
SOX11 Cyclin D1
Conventional
MCL
Indolent MCL
SOX11 Protein Expression in MCL
Courtesy of E Campo
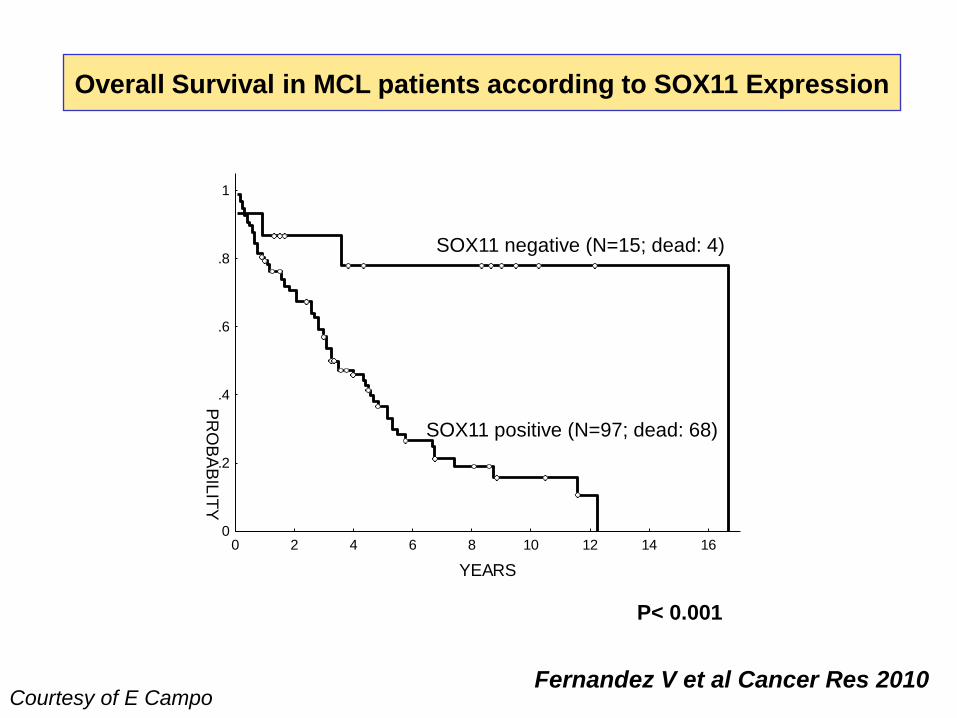
Overall Survival in MCL patients according to SOX11 Expression
Sox11 -
Sox11 +
P< 0.001
0 2 4 6 8 10 12 14 16
YEARS
0
.2
.4
.6
.8
1
PR
OB
AB
ILIT
Y
SOX11 negative (N=15; dead: 4)
SOX11 positive (N=97; dead: 68)
Fernandez V et al Cancer Res 2010 Courtesy of E Campo
11
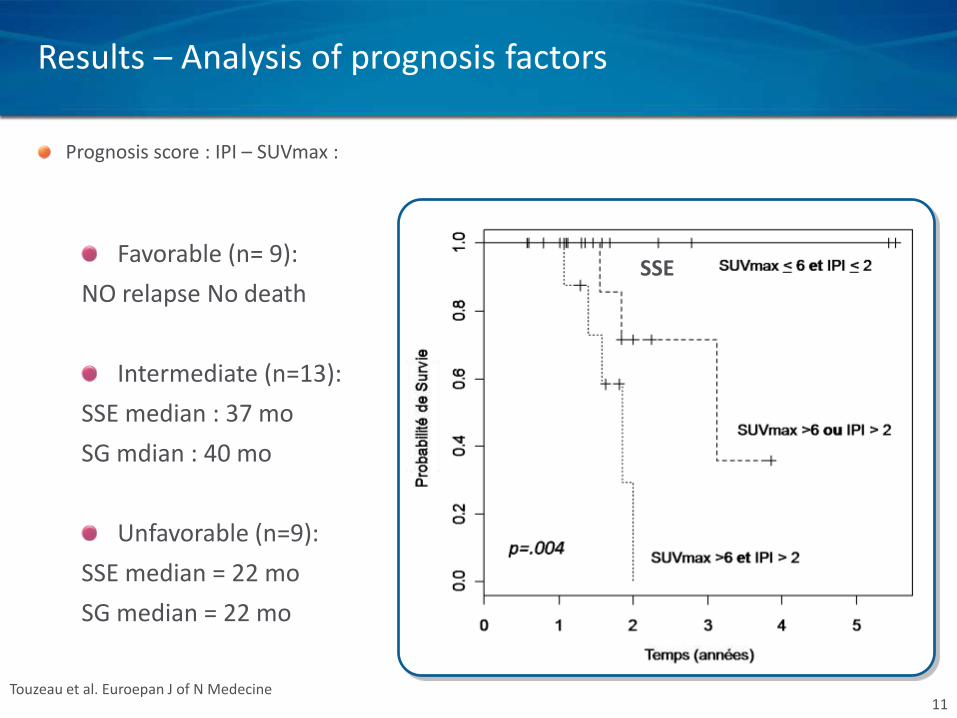
Prognosis score : IPI – SUVmax :
SSE Favorable (n= 9):
NO relapse No death
Intermediate (n=13):
SSE median : 37 mo
SG mdian : 40 mo
Unfavorable (n=9):
SSE median = 22 mo
SG median = 22 mo
Touzeau et al. Euroepan J of N Medecine
Results – Analysis of prognosis factors
12
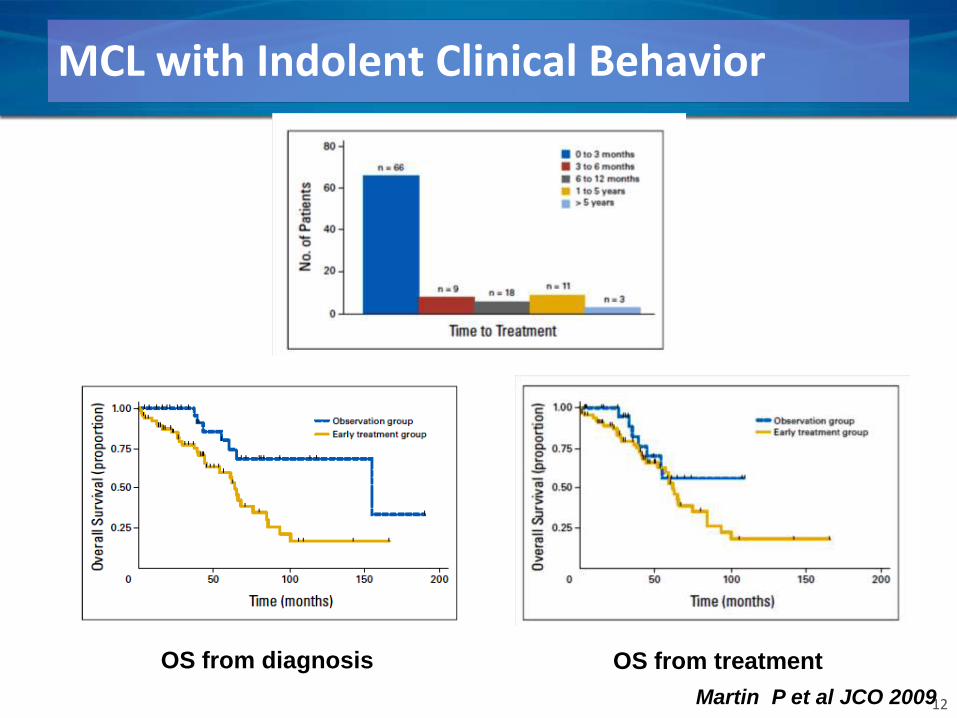
MCL with Indolent Clinical Behavior
OS from diagnosis OS from treatment
Martin P et al JCO 2009

Optimal treatment in mantle cell lymphoma ?
Induction ? Consolidation ?
maintenance
SCT
=> eradication => tumor reduction
Treatment Strategy
• Depend on age Old (60%) vs Young
(40%) with a 65 years old cut off
• Physiological status and comorbidity
more relevant
• High dose vs standard chemotherapy
Mantle cell lymphoma in young patients
• 40% < 60 yr
• Treatment with high dose chemotherapy and autologous SCT is possible
• Treatment with Allogeneous stem cell transplantation is feasible
Optimal treatment in mantle cell lymphoma ?
SCT
=> eradication => tumor reduction
Autologous SCT ?
Allogenous SCT ?
Optimal treatment in mantle cell lymphoma ?
SCT
=> eradication => tumor reduction
Autologous SCT ?
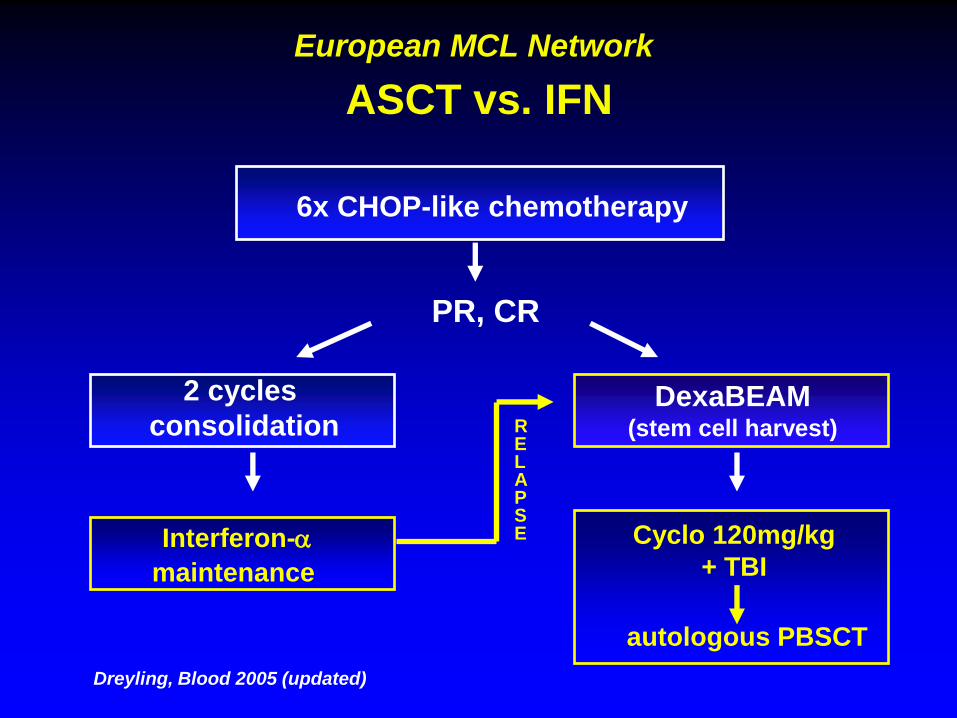
European MCL Network
ASCT vs. IFN
PR, CR
Interferon-a
maintenance
Cyclo 120mg/kg
+ TBI
autologous PBSCT
RELAPSE
DexaBEAM (stem cell harvest)
6x CHOP-like chemotherapy
2 cycles
consolidation
Dreyling, Blood 2005 (updated)
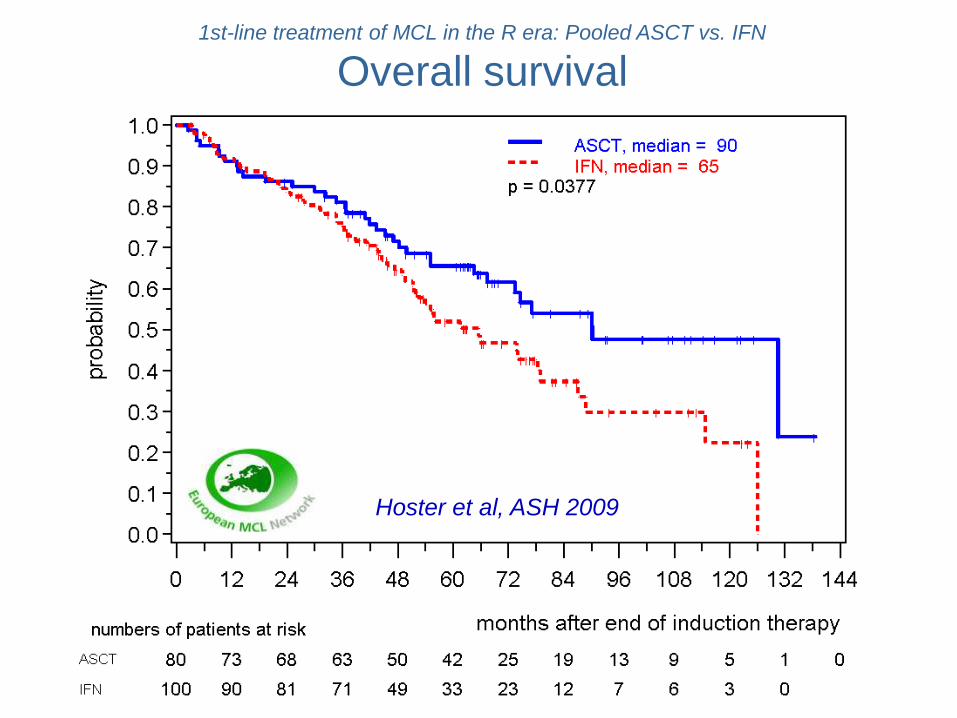
1st-line treatment of MCL in the R era: Pooled ASCT vs. IFN
Overall survival
Hoster et al, ASH 2009
Optimal treatment in mantle cell lymphoma ?
Induction ? Consolidation
SCT
=> eradication => tumor reduction
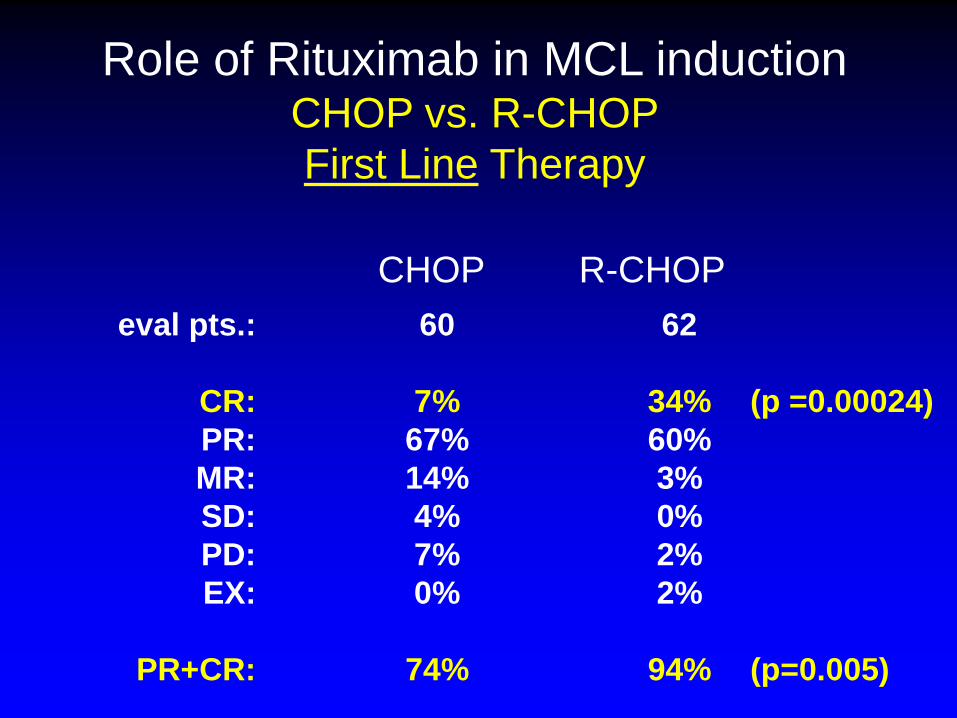
Role of Rituximab in MCL induction CHOP vs. R-CHOP
First Line Therapy
eval pts.: 60 62
CR: 7% 34% (p =0.00024)
PR: 67% 60%
MR: 14% 3%
SD: 4% 0%
PD: 7% 2%
EX: 0% 2%
PR+CR: 74% 94% (p=0.005)
CHOP R-CHOP
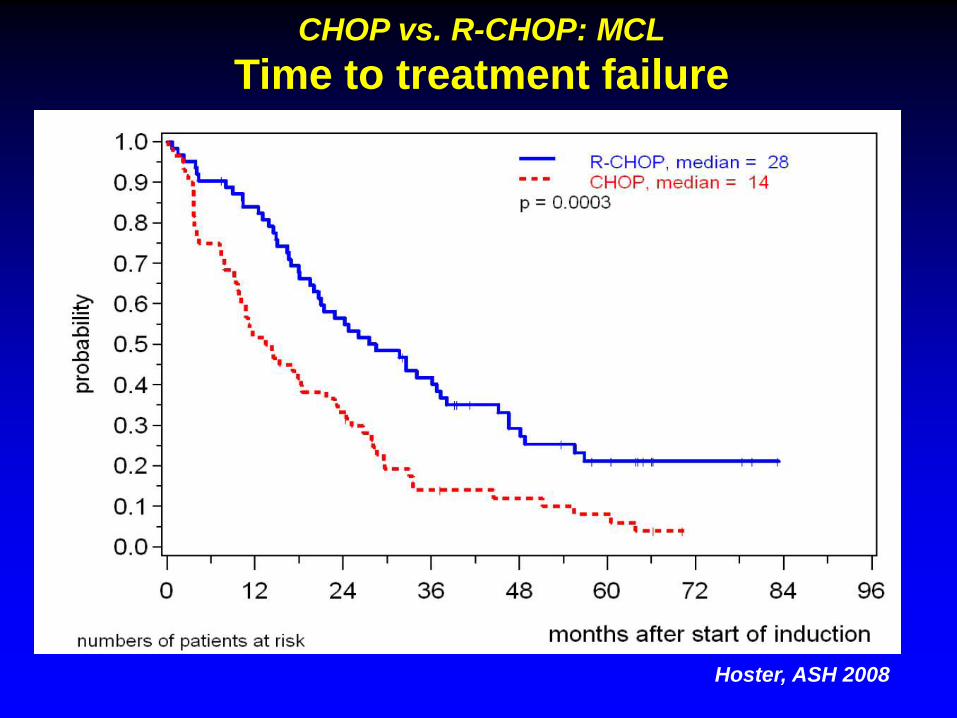
CHOP vs. R-CHOP: MCL
Time to treatment failure
Hoster, ASH 2008
Bibliography
• Tam CS, Bassett R, Ledesma C, et al. Mature results of the M.
D. Anderson Cancer Center risk-adapted transplantation
strategy in mantle cell lymphoma. Blood. 2009;113(18):4144-
52.
• Schulz H, Bohlius JF, Trelle S, et al. Immunochemotherapy
with rituximab and overall survival in patients with indolent or
mantle cell lymphoma: a systematic review and meta-analysis.
J Natl Cancer Inst. 2007;99(9):706-14.
Optimal treatment in mantle cell lymphoma ?
R+CHOP ? Consolidation
SCT
=> eradication => tumor reduction
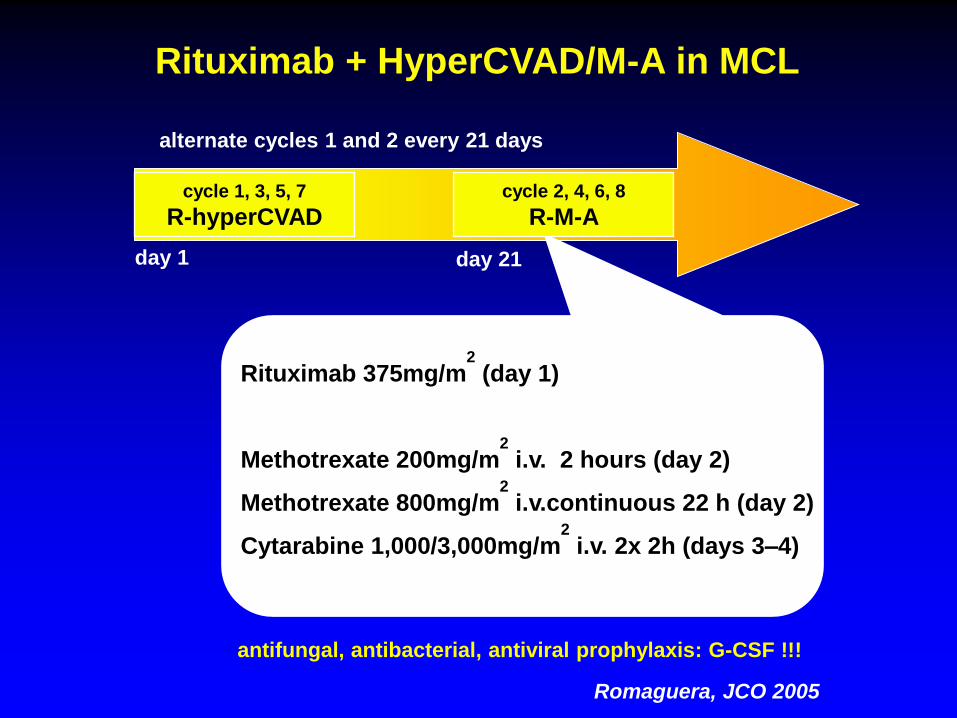
day 1 day 21
Rituximab + HyperCVAD/M-A in MCL
alternate cycles 1 and 2 every 21 days
Rituximab 375mg/m2
(day 1)
Methotrexate 200mg/m2
i.v. 2 hours (day 2)
Methotrexate 800mg/m2
i.v.continuous 22 h (day 2)
Cytarabine 1,000/3,000mg/m2
i.v. 2x 2h (days 3–4)
cycle 1, 3, 5, 7
R-hyperCVAD cycle 2, 4, 6, 8
R-M-A
antifungal, antibacterial, antiviral prophylaxis: G-CSF !!!
Romaguera, JCO 2005
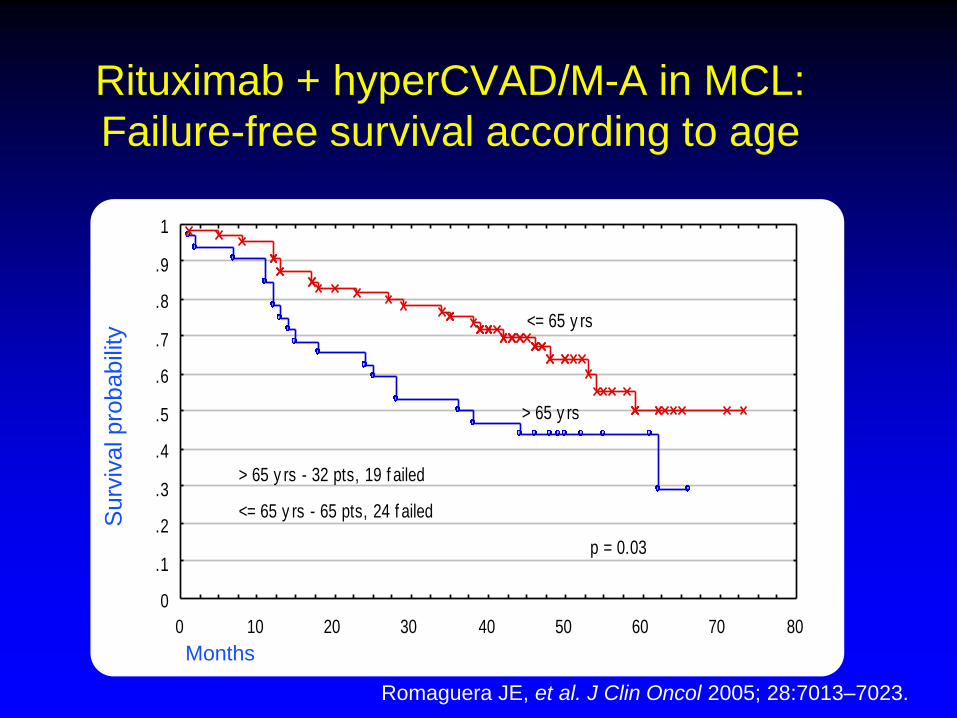
Surv
ival pro
babili
ty
Rituximab + hyperCVAD/M-A in MCL:
Failure-free survival according to age
Months
•
80706050403020100
1
.9
.8
.7
.6
.5
.4
.3
.2
.1
0
> 65 y rs - 32 pts, 19 f ailed
<= 65 y rs - 65 pts, 24 f ailed
p = 0.03
<= 65 y rs
> 65 y rs
••• •
Rituximab + HyperCVAD/M-A in MCL
Failure-Free Survival according to age
Months
Romaguera JE, et al. J Clin Oncol 2005; 28:7013–7023.
Hyper CVAD
2 year PFS 63%
40% treatment arrest
High toxicity
SWOG 0213: R-HyperCVAD/MTX-AraC in Patients
With Newly Diagnosed MCL
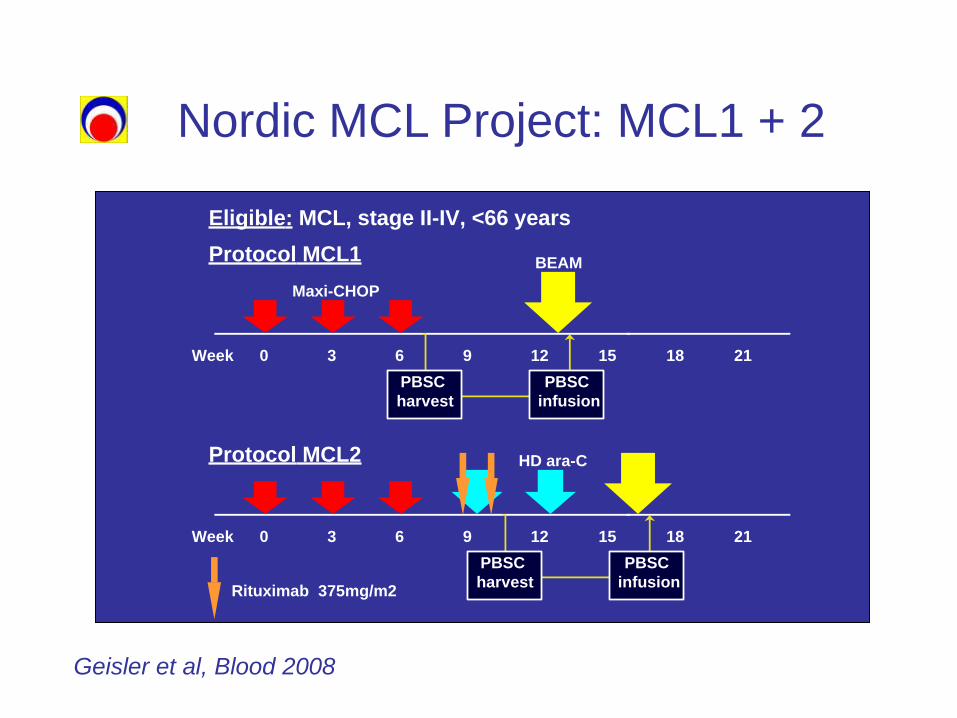
Nordic MCL Project: MCL1 + 2
Protocol MCL1
Week 0 3 6 9 12 15 18 21
Rituximab 375mg/m2
BEAM
Eligible: MCL, stage II-IV, <66 years
PBSC
harvest
PBSC
infusion
Protocol MCL2
Week 0 3 6 9 12 15 18 21
PBSC
harvest
PBSC
infusion
Maxi-CHOP
HD ara-C
Geisler et al, Blood 2008
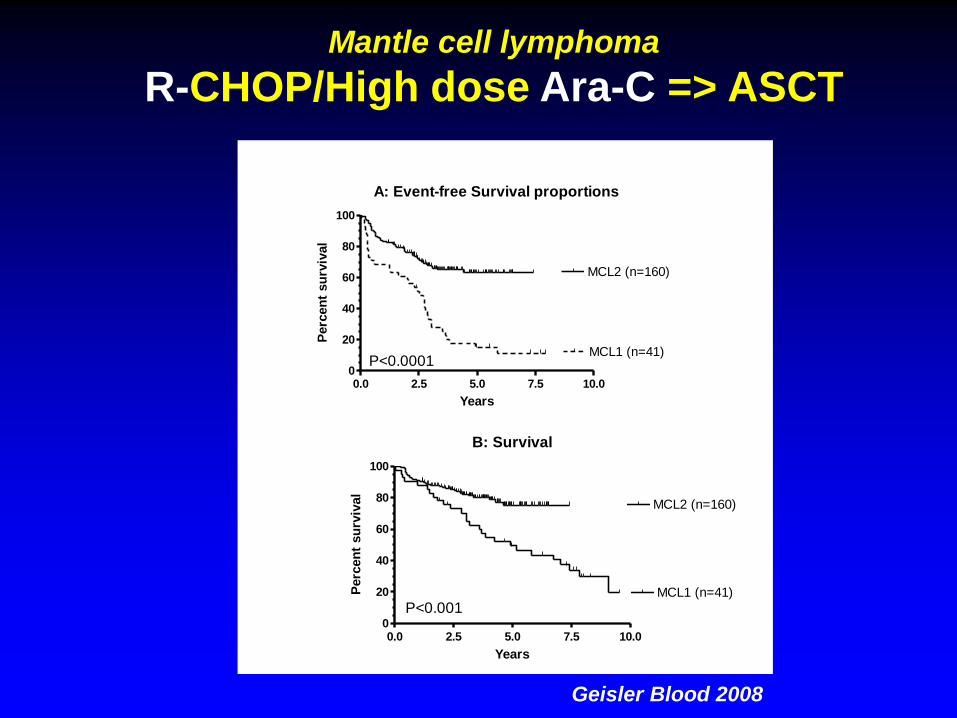
Mantle cell lymphoma
R-CHOP/High dose Ara-C => ASCT
B: Survival
0.0 2.5 5.0 7.5 10.00
20
40
60
80
100
MCL1 (n=41)
P<0.001
MCL2 (n=160)
Years
Perc
en
t su
rviv
al
A: Event-free Survival proportions
0.0 2.5 5.0 7.5 10.00
20
40
60
80
100
MCL1 (n=41)
MCL2 (n=160)
P<0.0001
Years
Perc
en
t su
rviv
al
Geisler Blood 2008
0.0 2.5 5.0 7.5 10.0 12.50.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
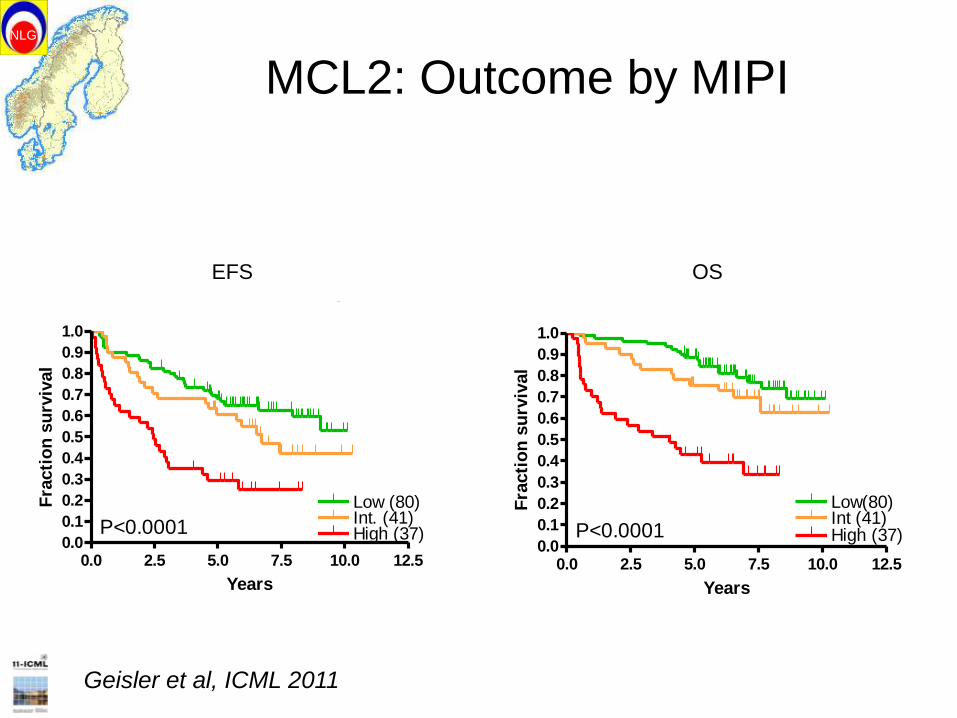
Low (80)
Event-free Survival according to MIPI
P<0.0001Int. (41)High (37)
Years
Fra
cti
on
su
rviv
al
0.0 2.5 5.0 7.5 10.0 12.50.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Low(80)
Survival according to MIPI
Int (41)High (37)P<0.0001
Years
Fra
cti
on
su
rviv
al
NLG
MCL2: Outcome by MIPI
EFS OS
Geisler et al, ICML 2011
32
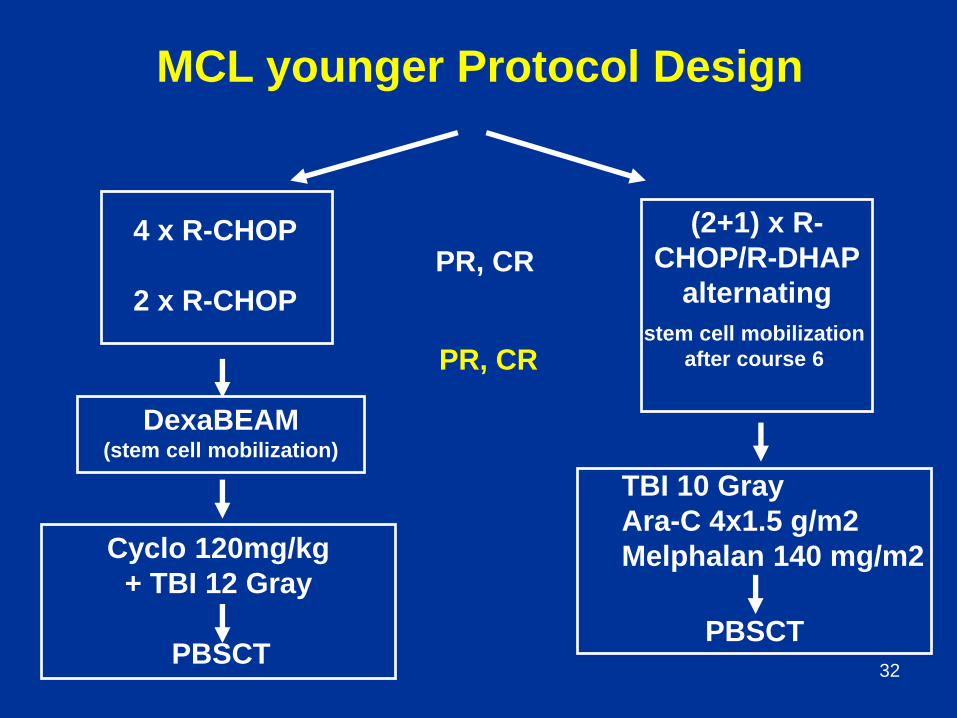
PR, CR
Cyclo 120mg/kg
+ TBI 12 Gray
PBSCT
PR, CR
(2+1) x R-
CHOP/R-DHAP
alternating
stem cell mobilization
after course 6
PBSCT
TBI 10 Gray
Ara-C 4x1.5 g/m2
Melphalan 140 mg/m2
4 x R-CHOP
2 x R-CHOP
DexaBEAM (stem cell mobilization)
MCL younger Protocol Design
33
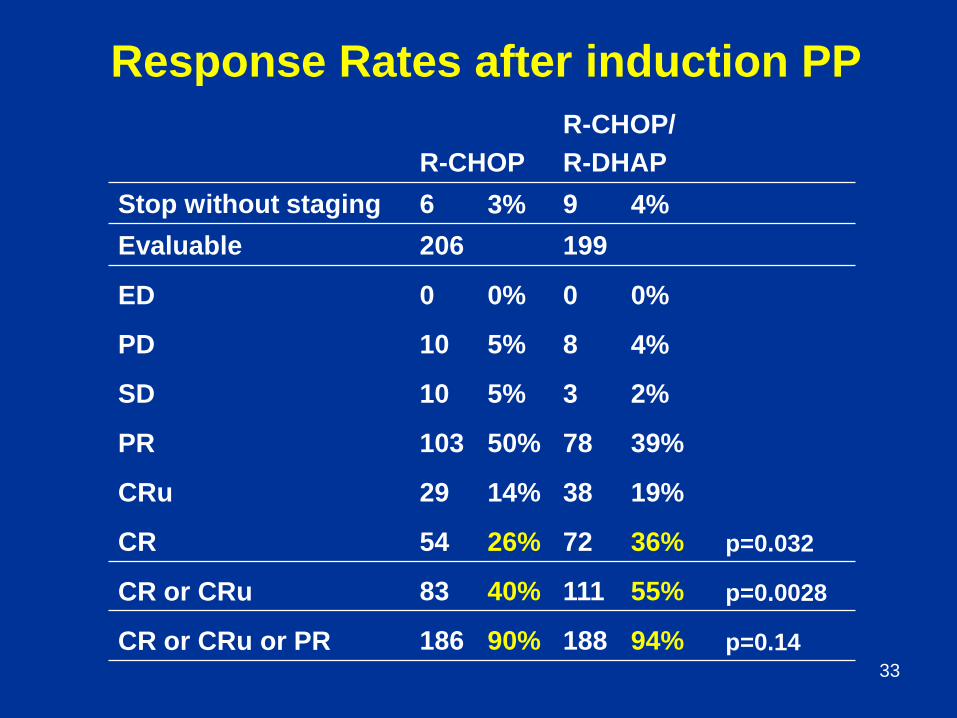
Response Rates after induction PP
R-CHOP
R-CHOP/
R-DHAP
Stop without staging 6 3% 9 4%
Evaluable 206 199
ED 0 0% 0 0%
PD 10 5% 8 4%
SD 10 5% 3 2%
PR 103 50% 78 39%
CRu 29 14% 38 19%
CR 54 26% 72 36% p=0.032
CR or CRu 83 40% 111 55% p=0.0028
CR or CRu or PR 186 90% 188 94% p=0.14
Update November 19, 2010, European MCL Network, V0.3 26.11.2010
34
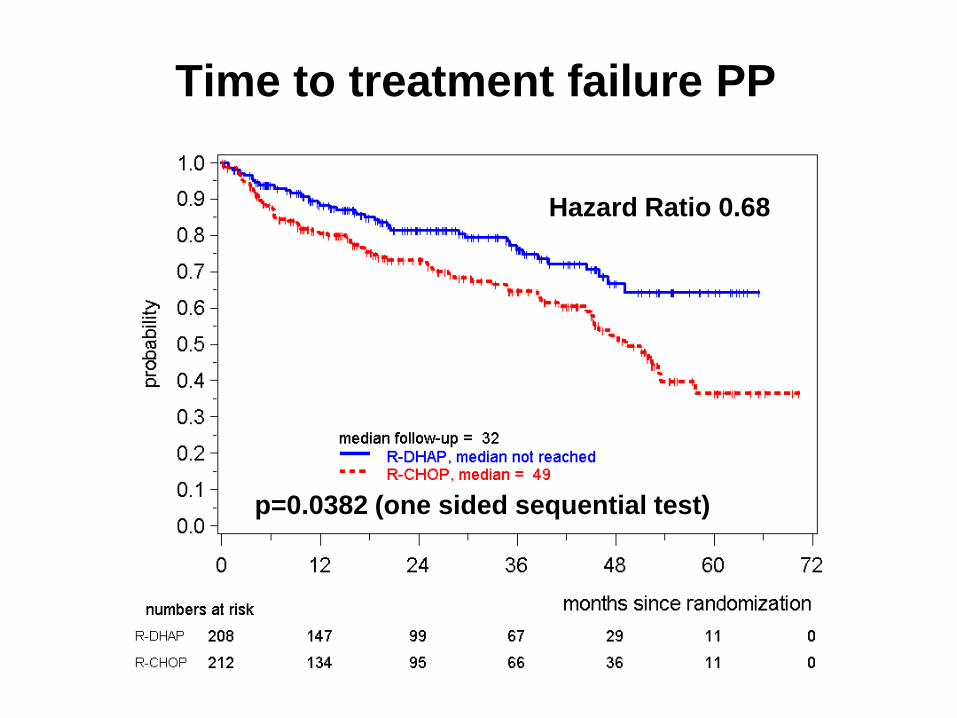
Time to treatment failure PP
p=0.0382 (one sided sequential test)
Hazard Ratio 0.68
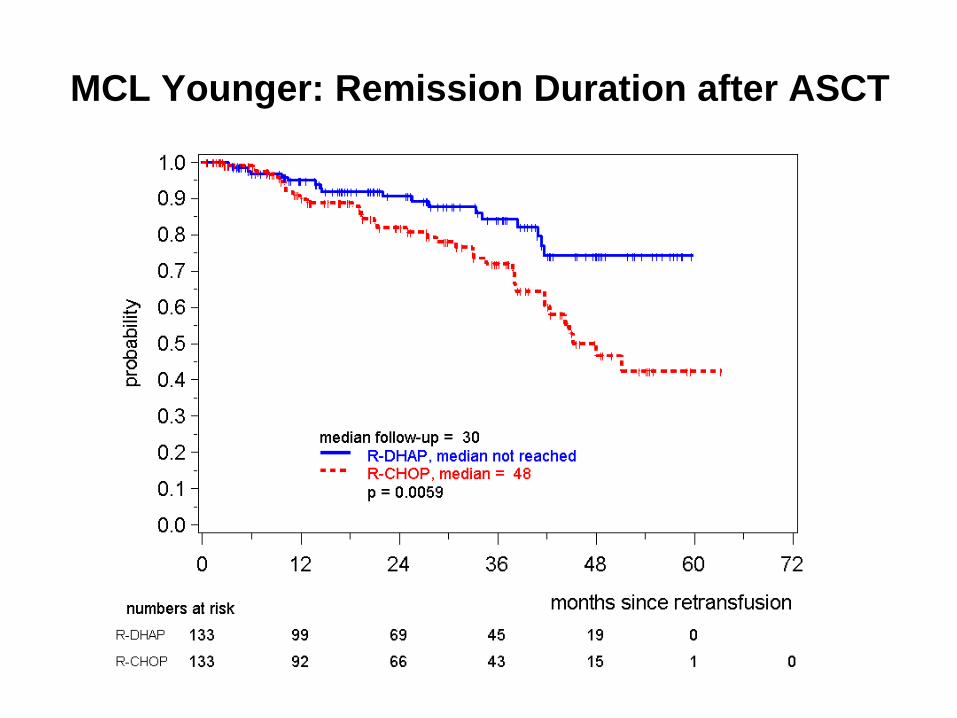
MCL Younger: Remission Duration after ASCT
Update April 7, 2013, European MCL Network, V1.0 22.05.2013
36
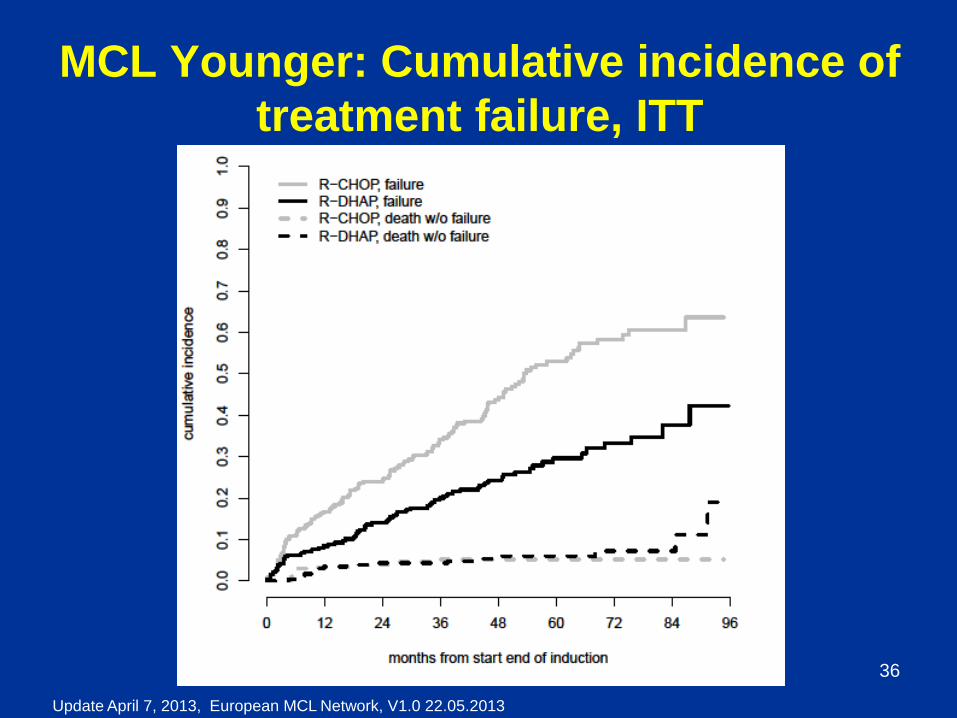
MCL Younger: Cumulative incidence of
treatment failure, ITT
Update April 7, 2013, European MCL Network, V1.0 22.05.2013
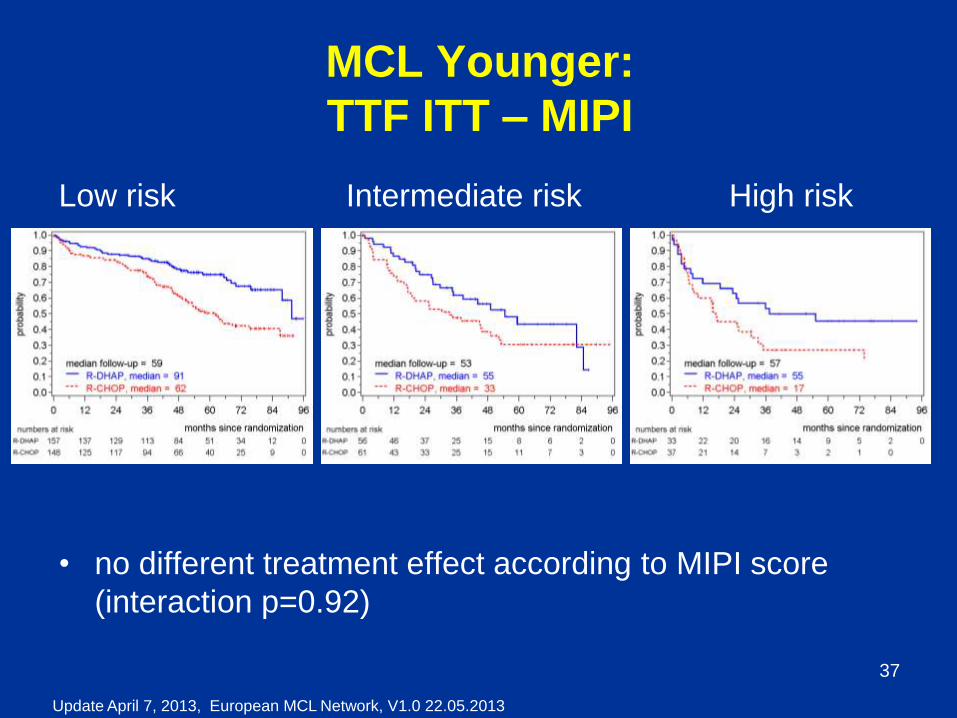
37
MCL Younger:
TTF ITT – MIPI
Low risk Intermediate risk High risk
• no different treatment effect according to MIPI score
(interaction p=0.92)
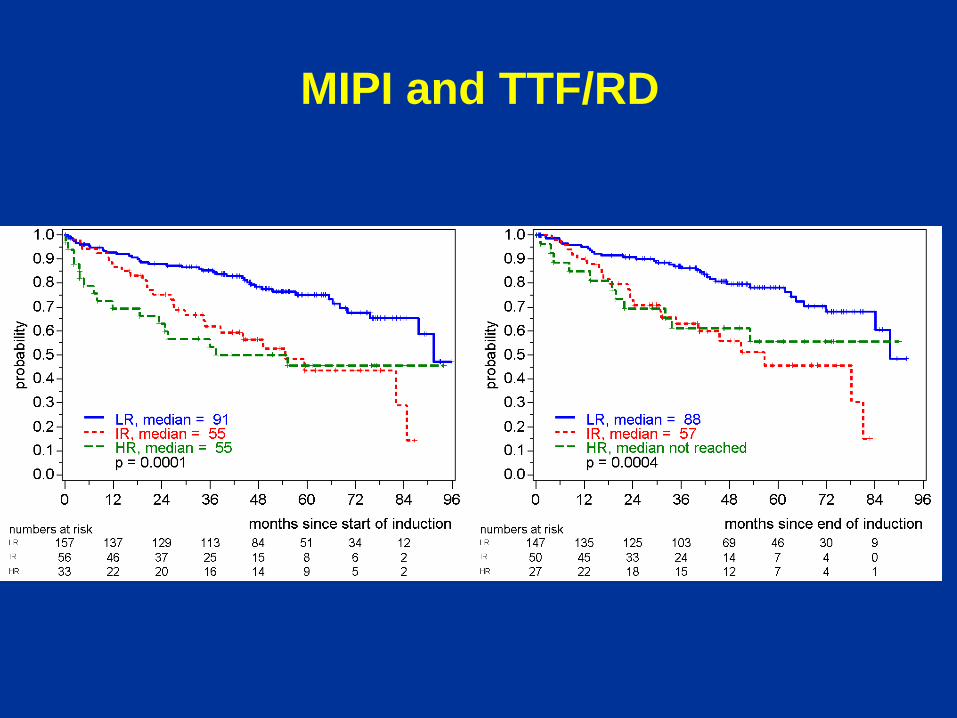
MIPI and TTF/RD
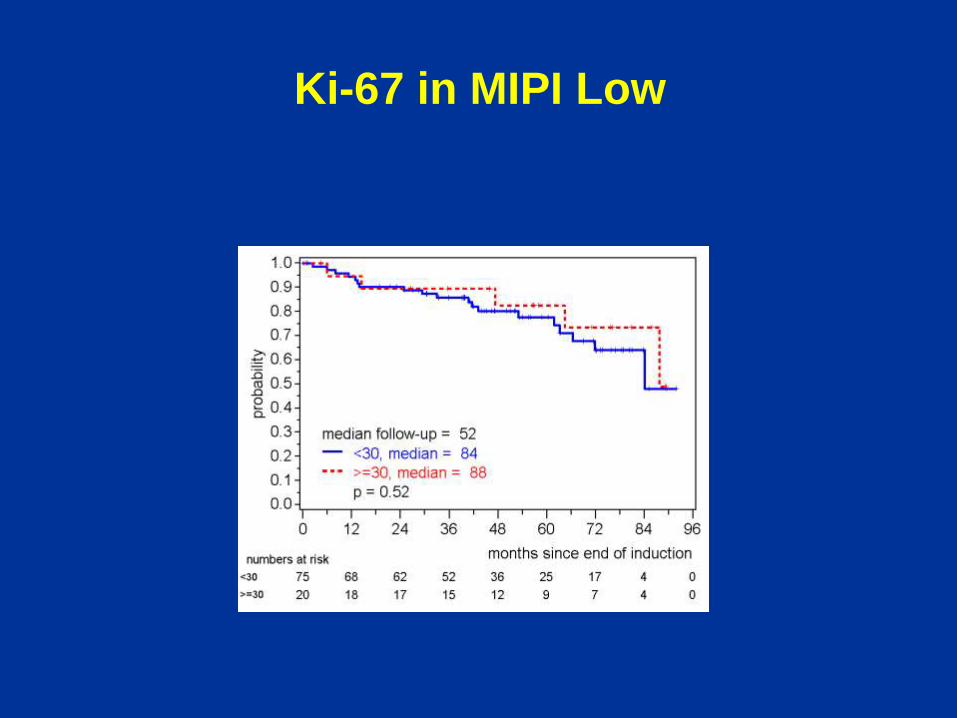
Ki-67 in MIPI Low
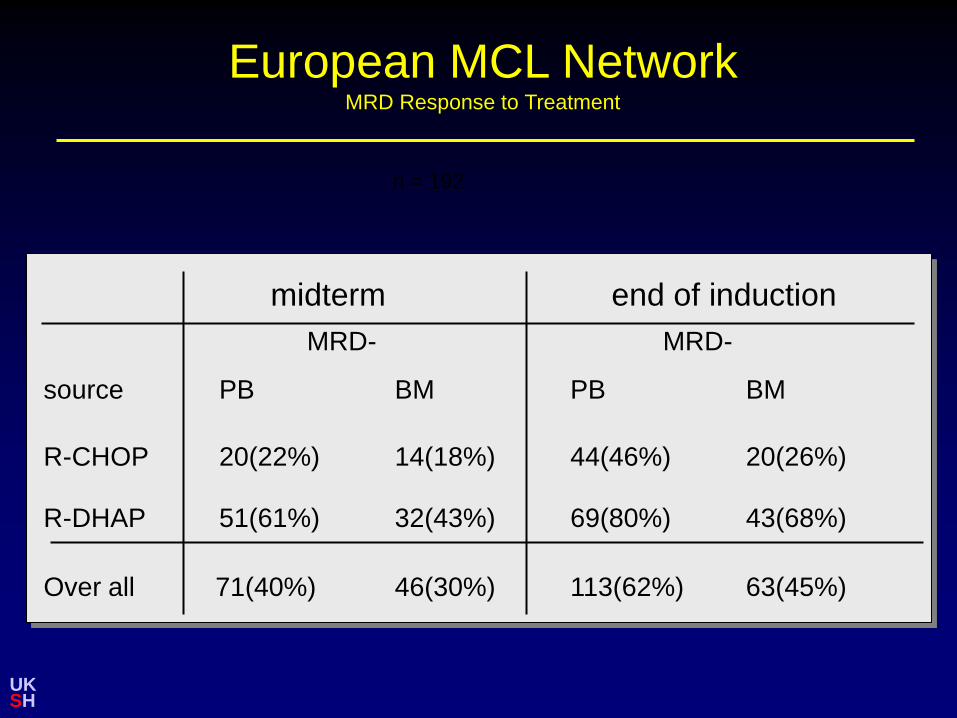
European MCL Network
MRD Response to Treatment
UK SH
midterm end of induction
MRD- MRD-
source PB BM PB BM
R-CHOP 20(22%) 14(18%) 44(46%) 20(26%)
R-DHAP 51(61%) 32(43%) 69(80%) 43(68%)
Over all 71(40%) 46(30%) 113(62%) 63(45%)
n = 192
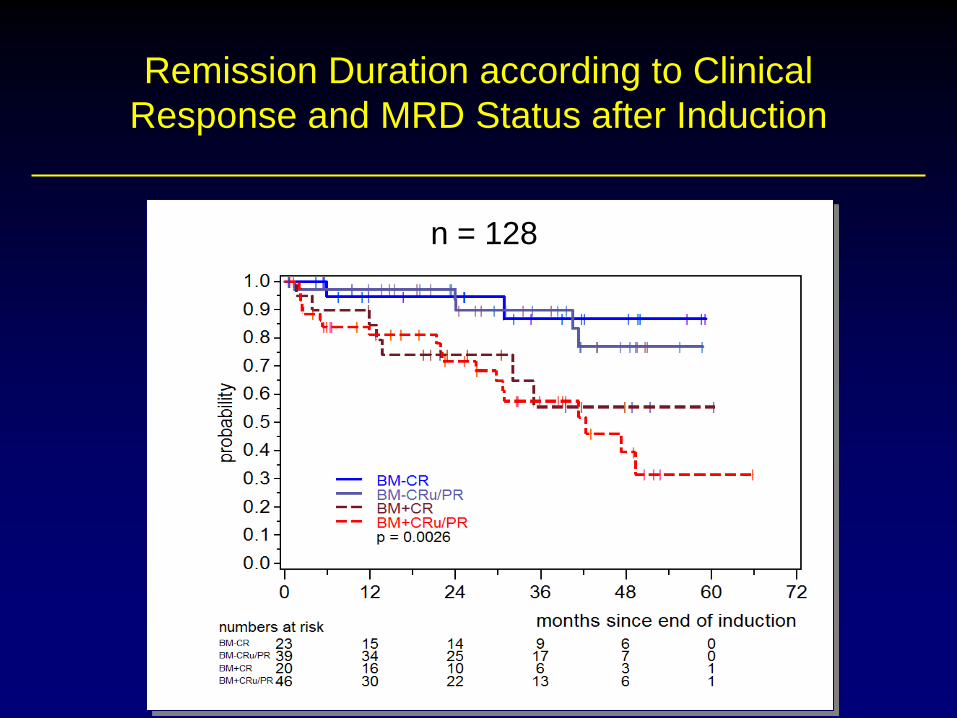
Remission Duration according to Clinical
Response and MRD Status after Induction
CR BM+
PR BM-
PR BM+
CR; MRD-
Cru/PR; MRD-
Cru/PR; MRD+
CR; MRD+
CR BM- CR BM+
PR BM-
PR BM+
p=0.0013
n = 128
42
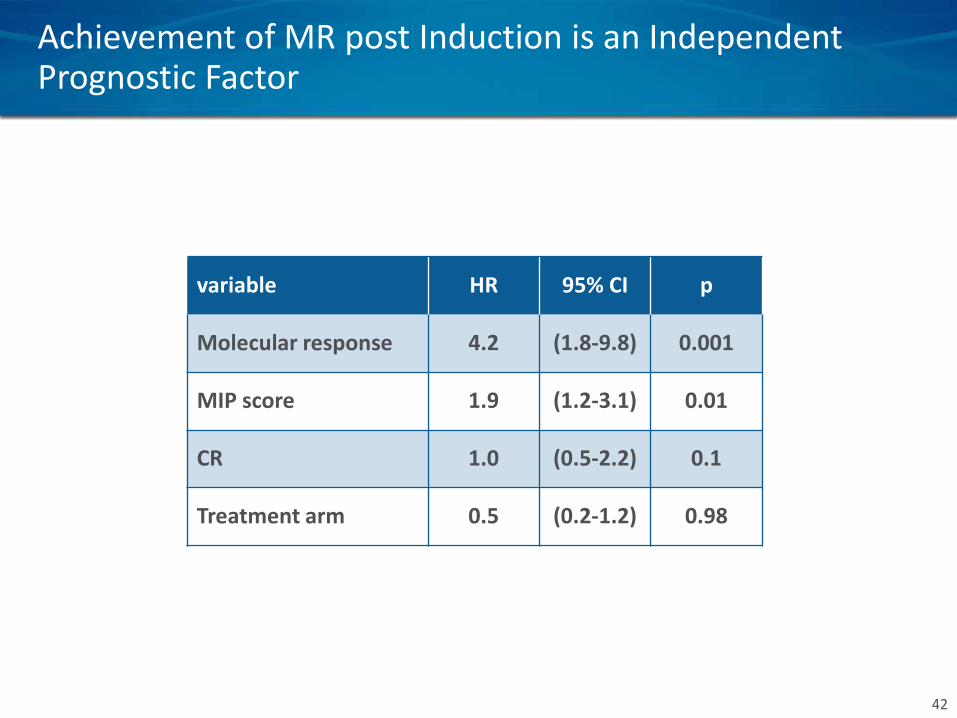
Achievement of MR post Induction is an Independent Prognostic Factor
variable HR 95% CI p
Molecular response 4.2 (1.8-9.8) 0.001
MIP score 1.9 (1.2-3.1) 0.01
CR 1.0 (0.5-2.2) 0.1
Treatment arm 0.5 (0.2-1.2) 0.98
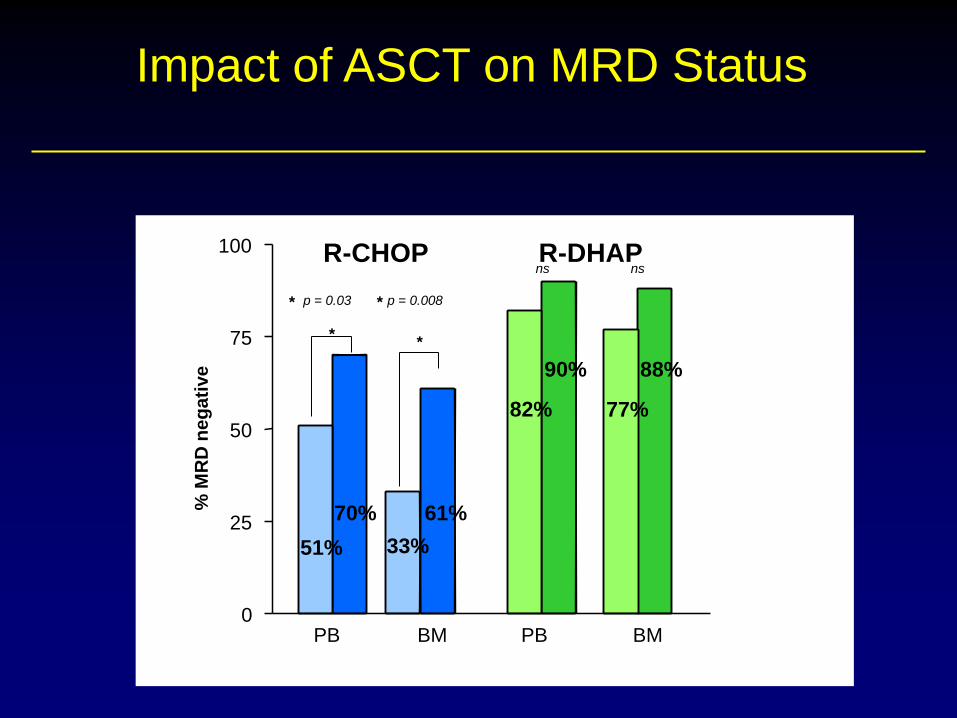
R-CHOP R-DHAP
Impact of ASCT on MRD Status
PB BM PB BM 0
25
50
75
100
% M
RD
ne
ga
tive
51%
70%
p = 0.03 p = 0.008
33%
61%
82%
90%
77%
88%
ns ns
* *
* *
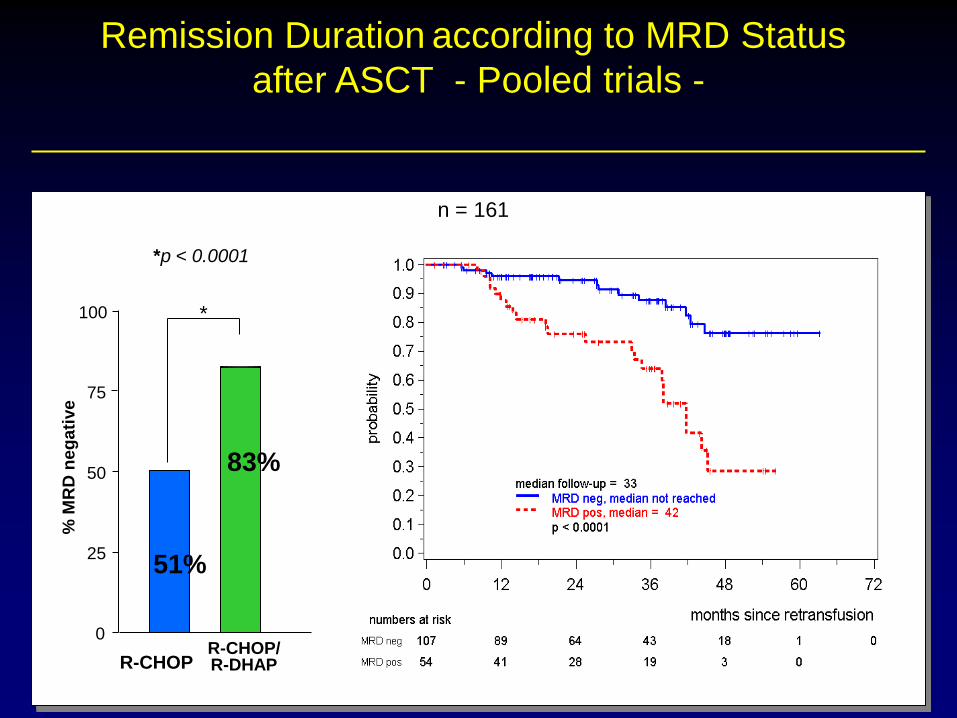
Remission Duration according to MRD Status
after ASCT - Pooled trials -
n = 161
*
% M
RD
ne
ga
tive
*p < 0.0001
R-CHOP R-CHOP/ R-DHAP
0
25
50
75
100
51%
83%
*

Update April 7, 2013, European MCL Network, V1.0 22.05.2013
45
MCL Younger: Overall Survival
PP population
ARM 24 36 48
R-DHAP 88% 83% 80%
R-CHOP 83% 76% 74%

Optimal treatment in mantle cell lymphoma ?
R+high dose ARAC
RCHOP/RDHAP ?
Consolidation
SCT
=> eradication => tumor reduction
Optimal treatment in mantle cell lymphoma ?
R+high dose ARAC
RCHOP/RDHAP ? Maintenance ?
SCT
=> eradication => tumor reduction
TBI ? MCL2 vs EMCL (ASH 2013)
>PR (EBMT)
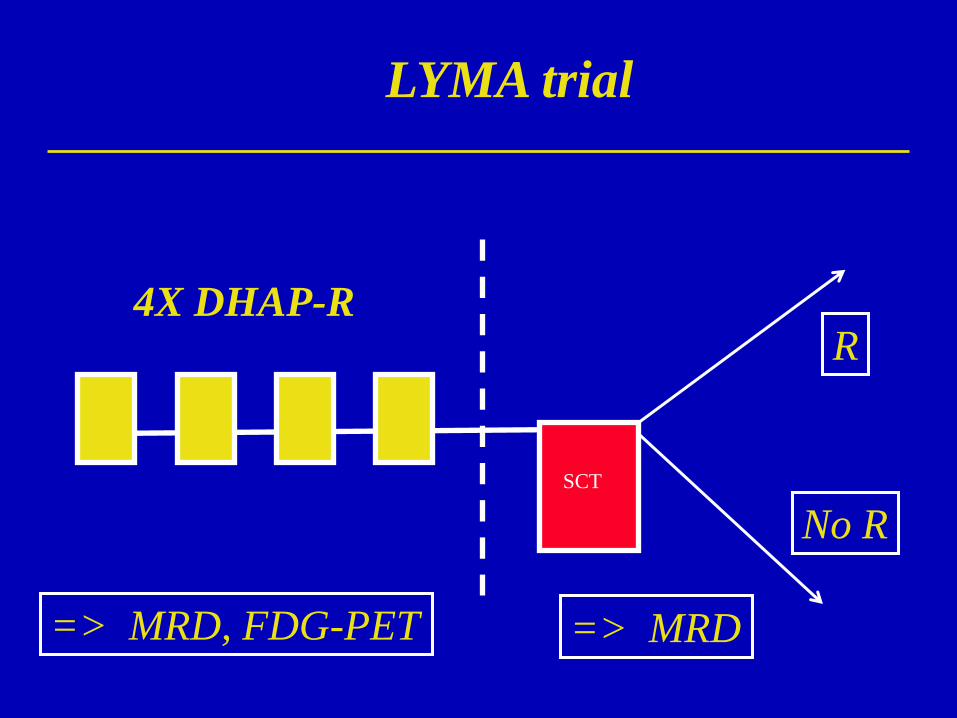
LYMA trial
SCT
=> MRD => MRD, FDG-PET
4X DHAP-R R
No R
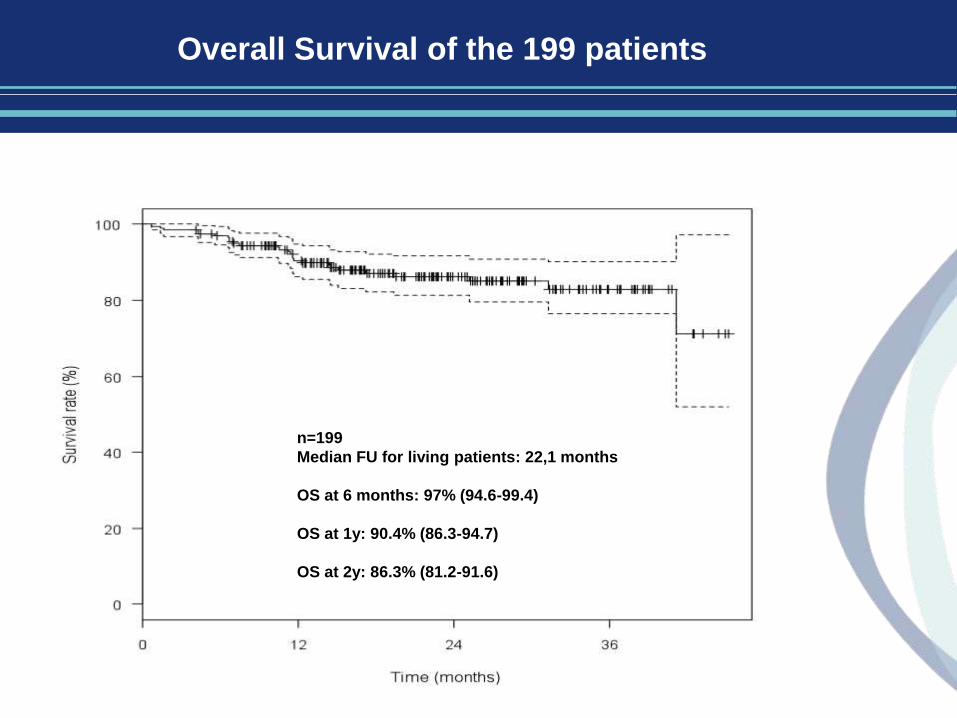
n=199
Median FU for living patients: 22,1 months
OS at 6 months: 97% (94.6-99.4)
OS at 1y: 90.4% (86.3-94.7)
OS at 2y: 86.3% (81.2-91.6)
Overall Survival of the 199 patients
Optimal treatment in mantle cell lymphoma ?
SCT
=> eradication => tumor reduction
Allogeneous SCT ?
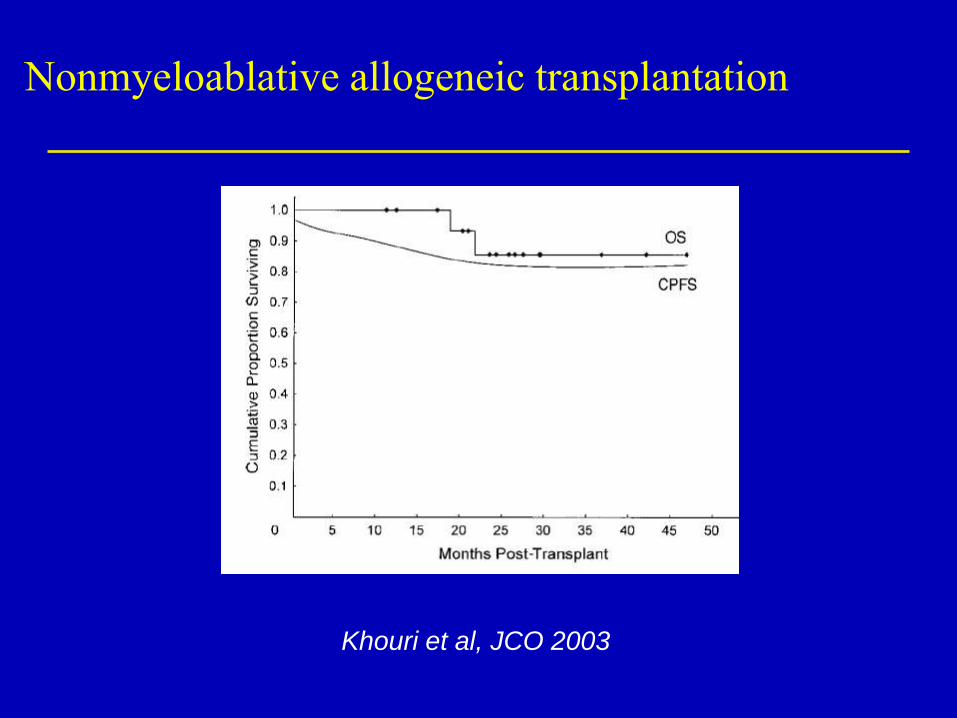
Nonmyeloablative allogeneic transplantation
Khouri et al, JCO 2003
60 48 36 24 12 0
Months after SCT
1,0
0,8
0,6
0,4
0,2
0,0
Cu
m S
urv
iva
l
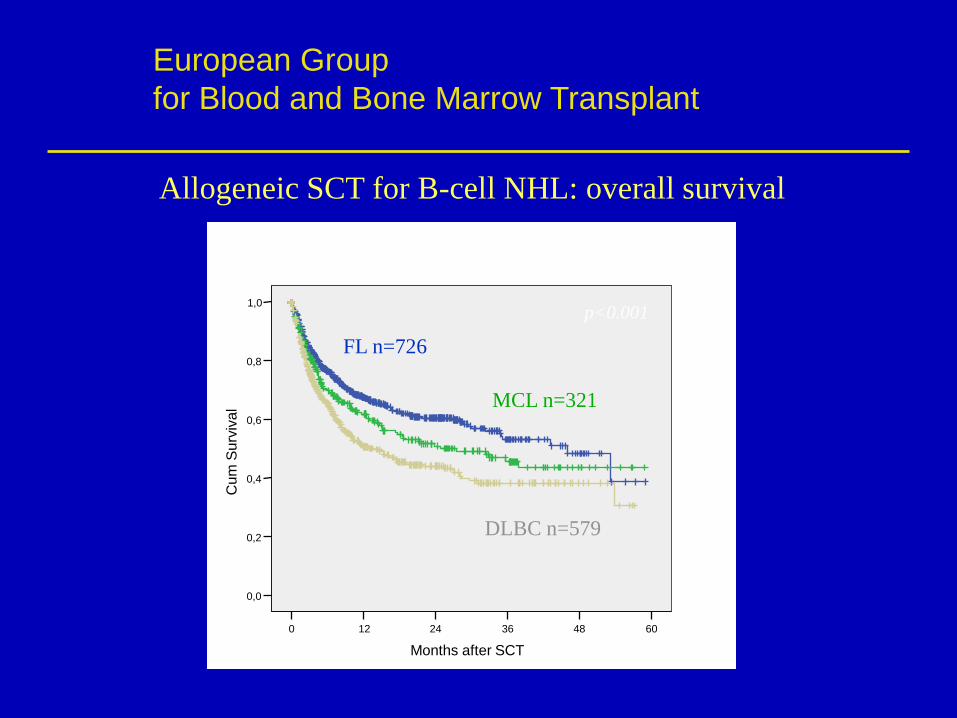
FL n=726
MCL n=321
DLBC n=579
p<0.001
Allogeneic SCT for B-cell NHL: overall survival
European Group
for Blood and Bone Marrow Transplant
Months
60 48 36 24 12 0
1,0
0,8
0,6
0,4
0,2
0,0
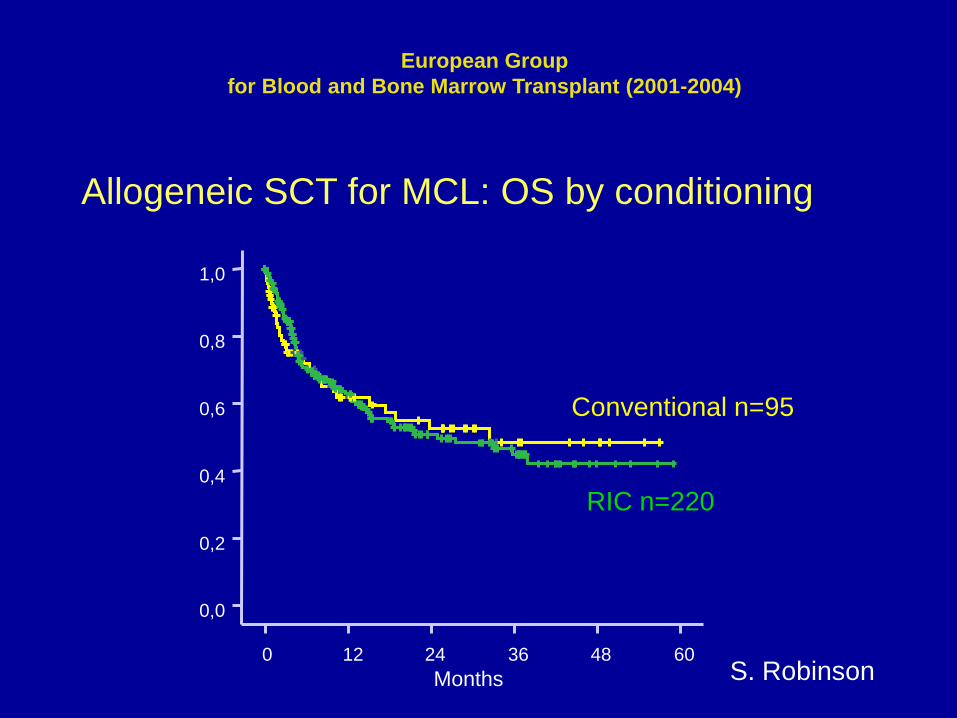
Allogeneic SCT for MCL: OS by conditioning
RIC n=220
Conventional n=95
European Group
for Blood and Bone Marrow Transplant (2001-2004)
S. Robinson
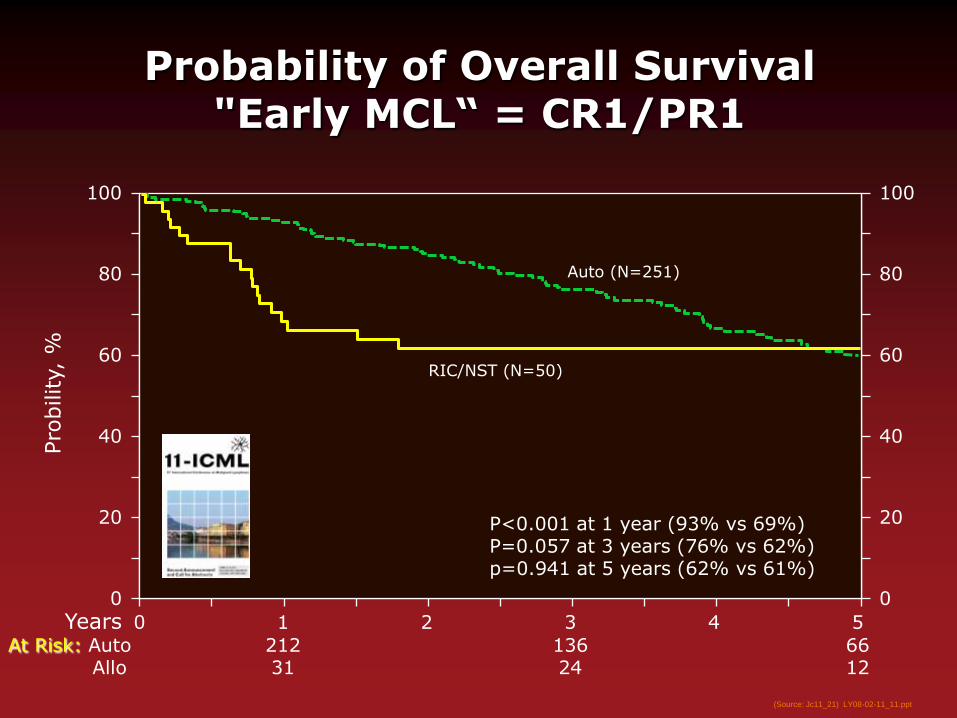
Years 1 2 3 4 5
At Risk: Auto 212 136 66 Allo 31 24 12
0
Pro
bility,
%
100
0
20
40
60
80
100
0
20
40
60
80 Auto (N=251)
Probability of Overall Survival "Early MCL“ = CR1/PR1
P<0.001 at 1 year (93% vs 69%) P=0.057 at 3 years (76% vs 62%) p=0.941 at 5 years (62% vs 61%)
(Source: Jc11_21) LY08-02-11_11.ppt
RIC/NST (N=50)

Allogeneic SCT for MCL: OS by disease status
60 48 36 24 12 0
Months
1,0
0,8
0,6
0,4
0,2
0,0
CR1 n=56
Others n=133
Refrac / Relapse / Progr n=140
European Group
Blood and Bone Marrow Transplant (2001-2004)
Allogeneous Stem
Transplantation in MCL
• GVL effect occurs
• Curative procedure
• Not in first line except in patients
with poor prognosis that remain to
be determined (hıgh MIPI,
MRD+,blastoıd ?)
• In relapsing setting in responding
patients (CR or PR)
Mantle cell lymphoma is also a
disease of the ederly patients or unfit
patients
• 60% >40 yr
• Treatment with high dose chemotherapy and autologous/allo SCT is not possible (70 y)
Update April 7, 2013, European MCL Network, V1.0, 23.05.2013
Update April 7, 2013, European MCL Network, V1.0, 23.05.2013
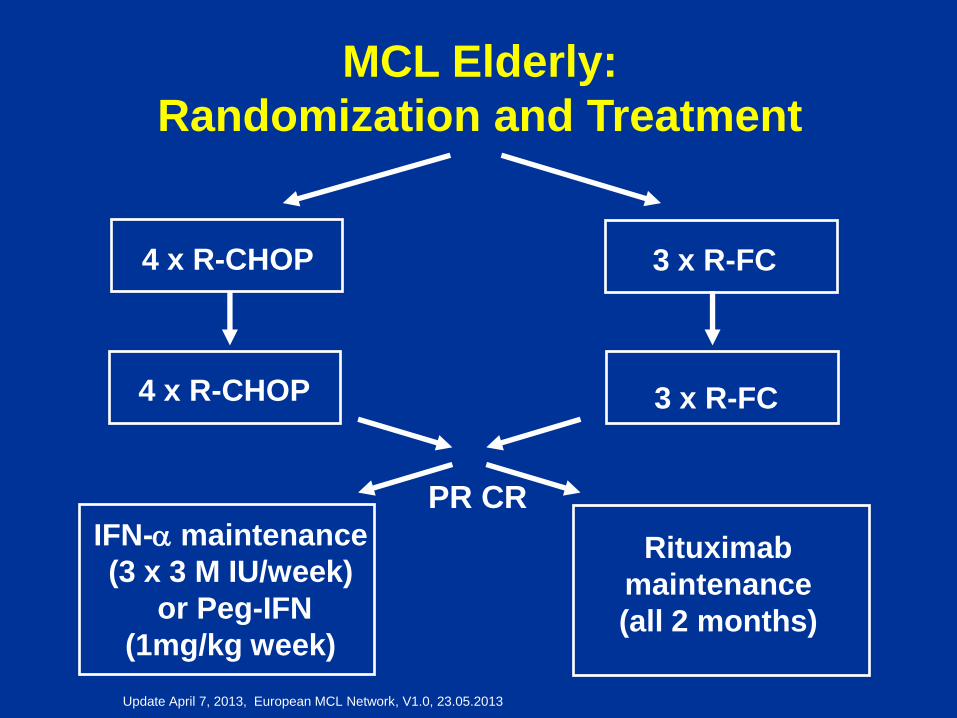
4 x R-CHOP
IFN-a maintenance
(3 x 3 M IU/week)
or Peg-IFN
(1mg/kg week)
4 x R-CHOP
PR CR
3 x R-FC
Rituximab
maintenance
(all 2 months)
3 x R-FC
MCL Elderly:
Randomization and Treatment
Update April 7, 2013, European MCL Network, V1.0, 23.05.2013
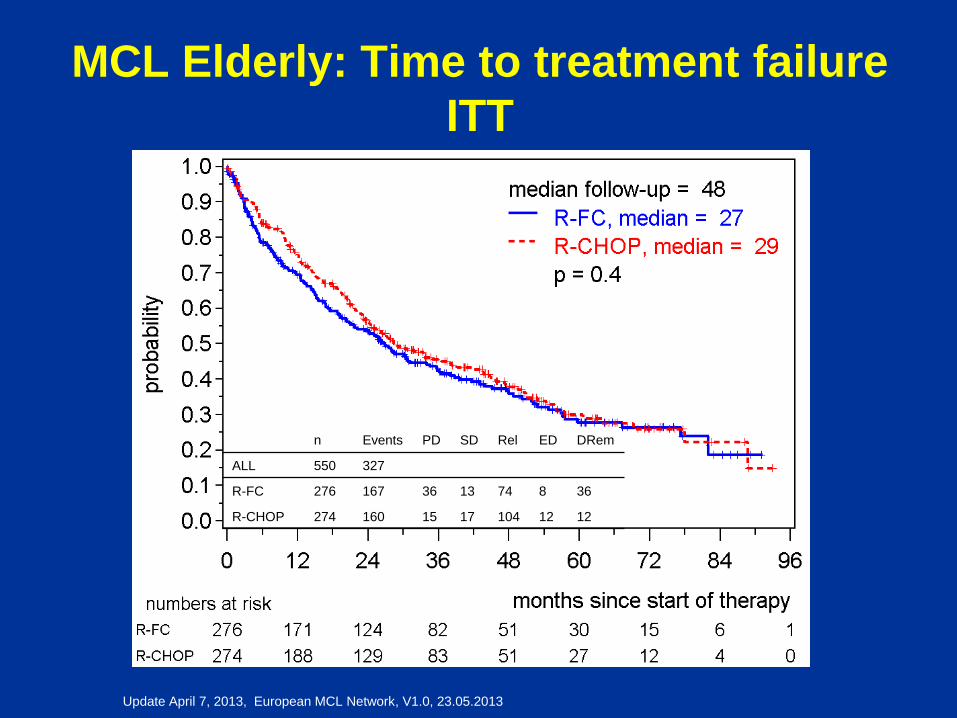
MCL Elderly: Time to treatment failure
ITT
n Events PD SD Rel ED DRem
ALL 550 327
R-FC 276 167 36 13 74 8 36
R-CHOP 274 160 15 17 104 12 12
Update April 7, 2013, European MCL Network, V1.0, 23.05.2013
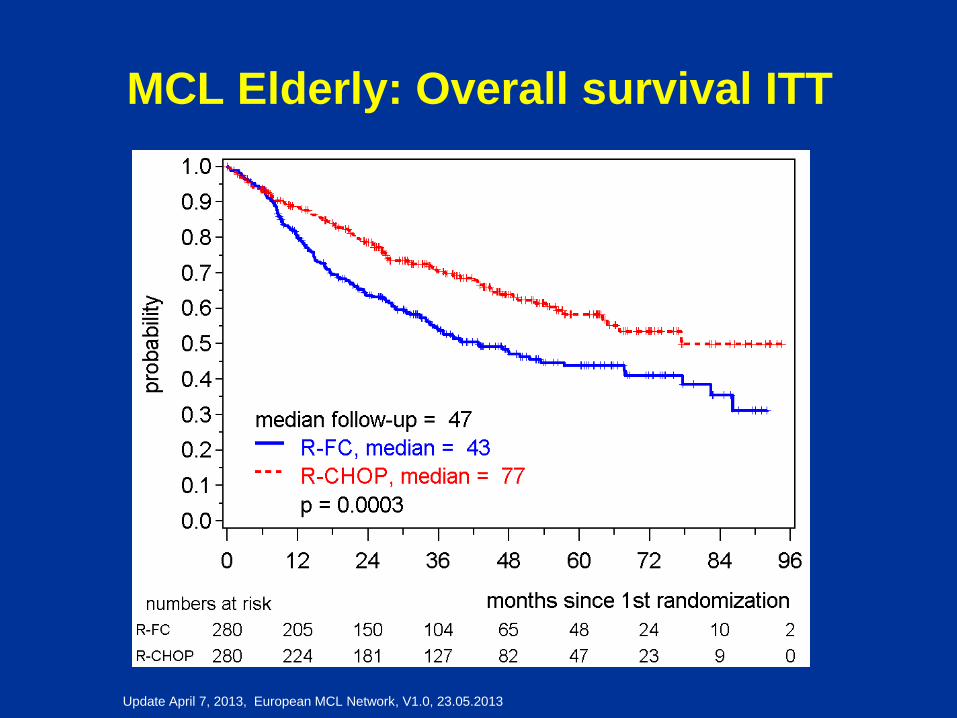
MCL Elderly: Overall survival ITT
Update April 7, 2013, European MCL Network, V1.0, 23.05.2013
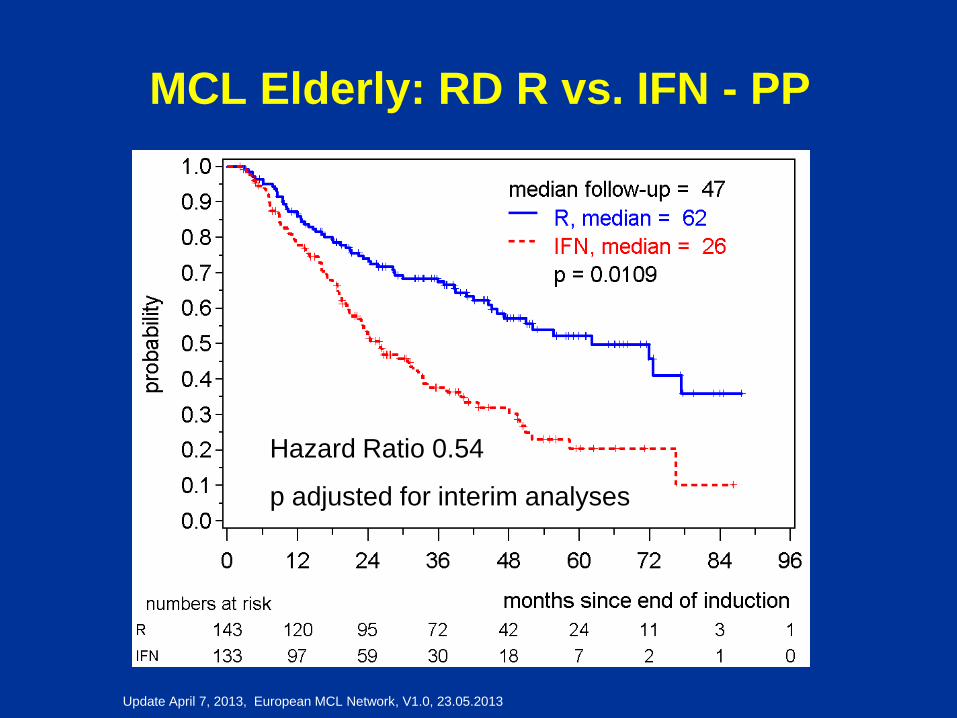
MCL Elderly: RD R vs. IFN - PP
Hazard Ratio 0.54
p adjusted for interim analyses
Update April 7, 2013, European MCL Network, V1.0, 23.05.2013
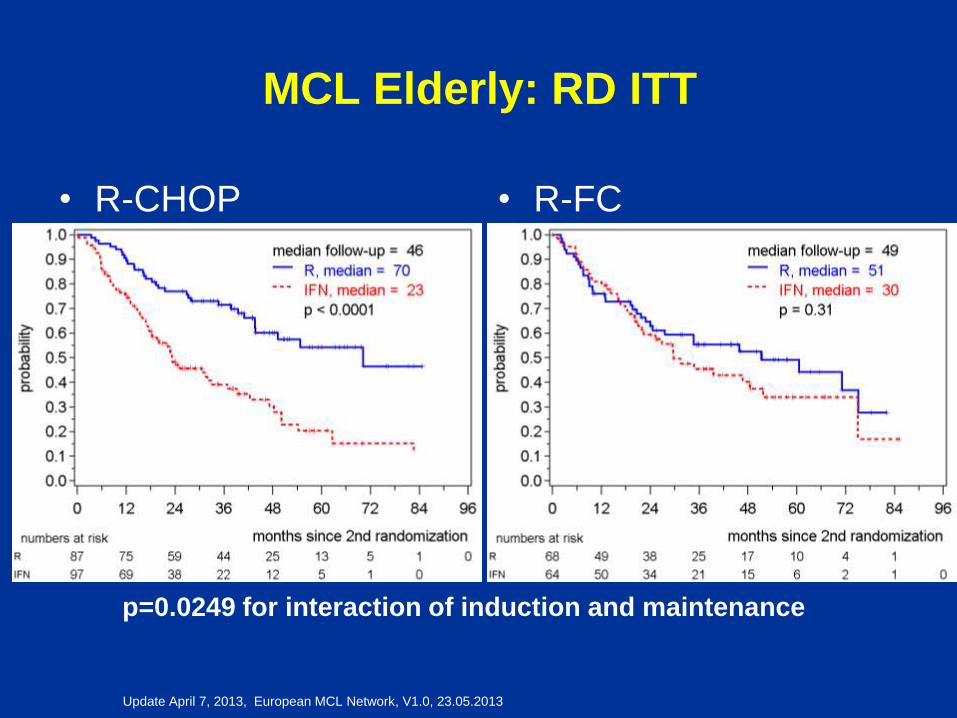
MCL Elderly: RD ITT
• R-CHOP • R-FC
p=0.0249 for interaction of induction and maintenance
Update April 7, 2013, European MCL Network, V1.0, 23.05.2013
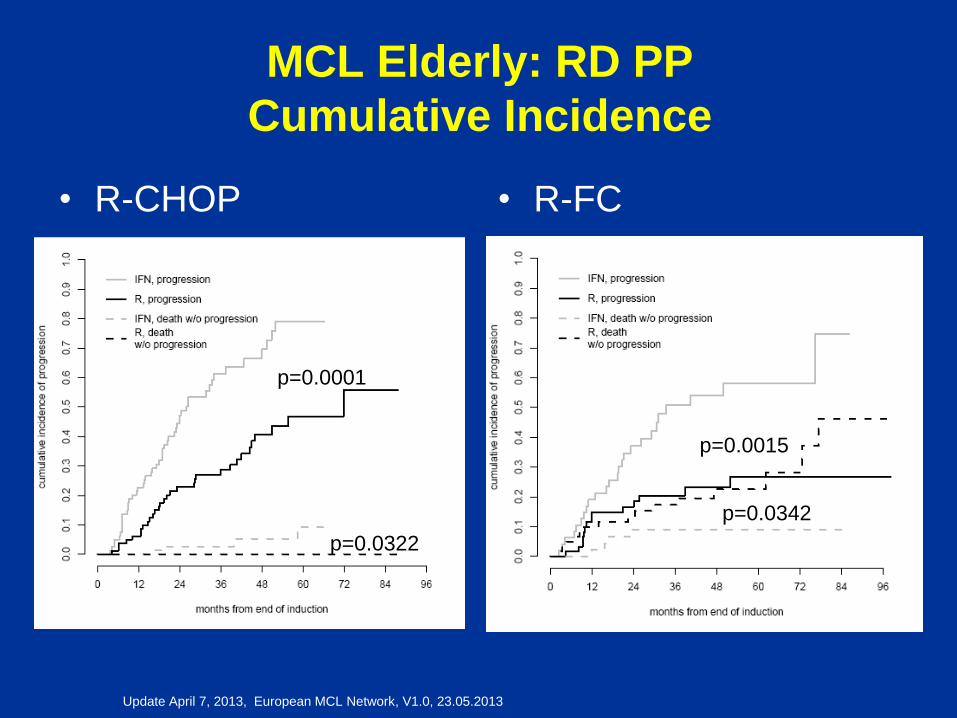
MCL Elderly: RD PP
Cumulative Incidence
• R-CHOP • R-FC
p=0.0015
p=0.0342
p=0.0001
p=0.0322
Update April 7, 2013, European MCL Network, V1.0, 23.05.2013
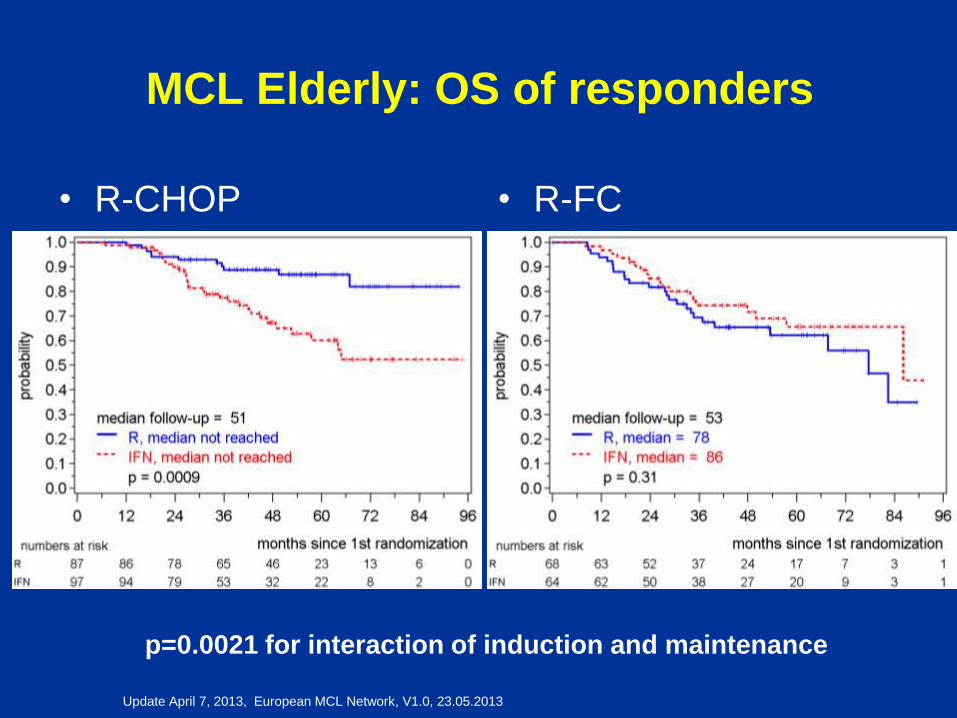
MCL Elderly: OS of responders
• R-CHOP • R-FC
p=0.0021 for interaction of induction and maintenance
MCL in Ederly
• RCHOP + R is the new standard
• However room to improve prognosis
(increase CR)
• Chemotherapy of induction ?
• Improve maintenance
• New drugs ?
New Drugs to improve response
before Allogeneous Stem cell
transplantation ?
Bendamustine
Bortezomib (FDA approval)
Thalidomide/Lenalidomide
Temsirolimus (EMEA approval)
Others new compounds
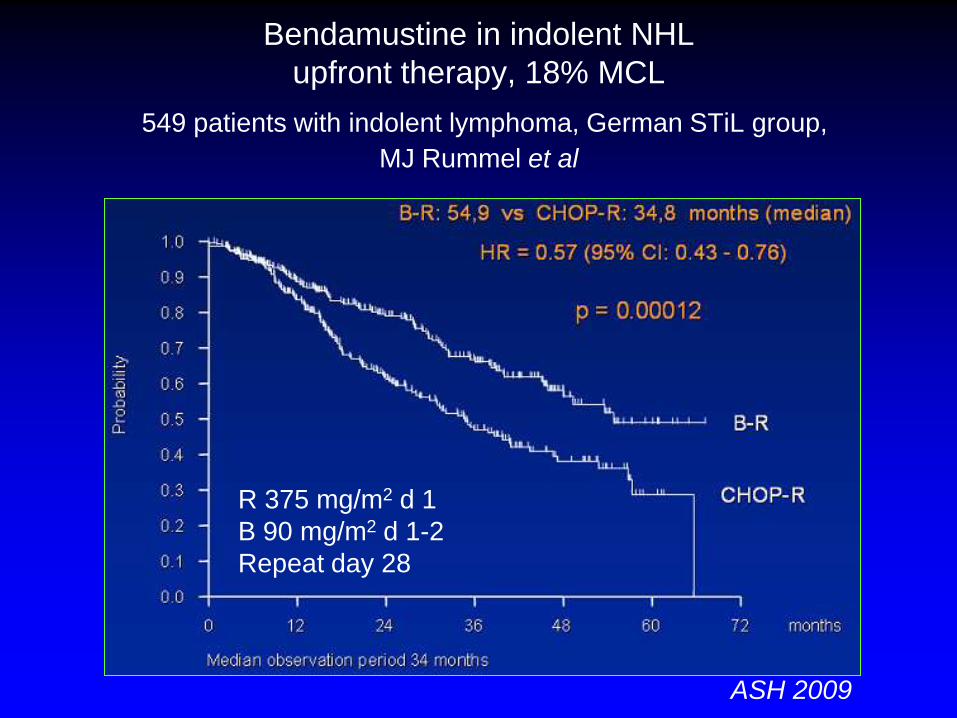
Bendamustine in indolent NHL
upfront therapy, 18% MCL
549 patients with indolent lymphoma, German STiL group,
MJ Rummel et al
R 375 mg/m2 d 1
B 90 mg/m2 d 1-2
Repeat day 28
ASH 2009
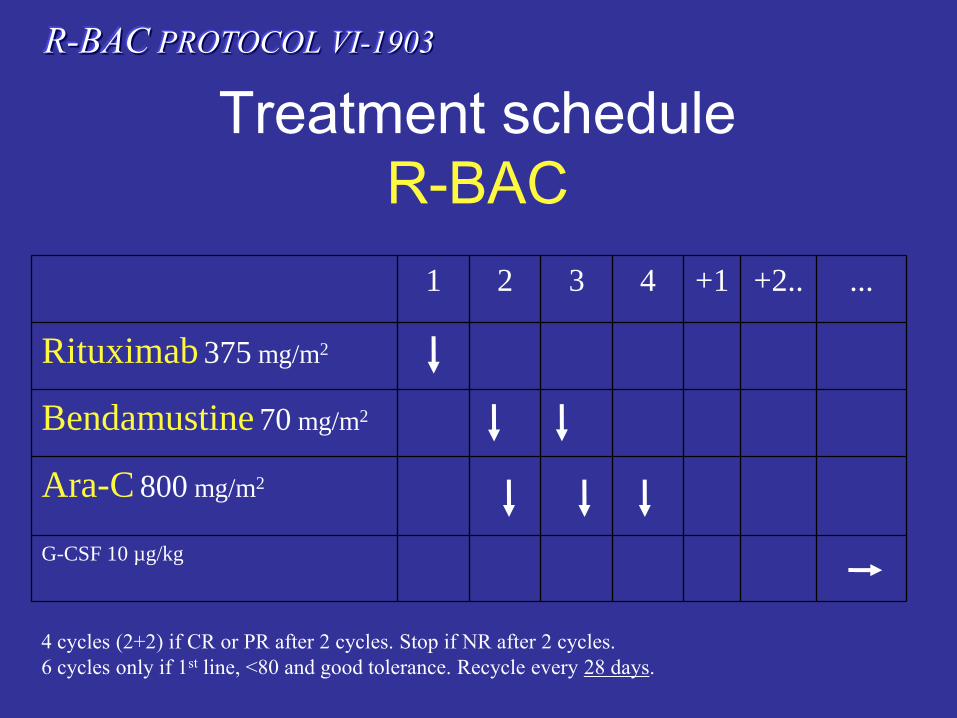
Treatment schedule
R-BAC
R-BAC PROTOCOL VI-1903
1 2 3 4 +1 +2.. ...
Rituximab 375 mg/m2
Bendamustine 70 mg/m2
Ara-C 800 mg/m2
G-CSF 10 µg/kg
4 cycles (2+2) if CR or PR after 2 cycles. Stop if NR after 2 cycles.
6 cycles only if 1st line, <80 and good tolerance. Recycle every 28 days.
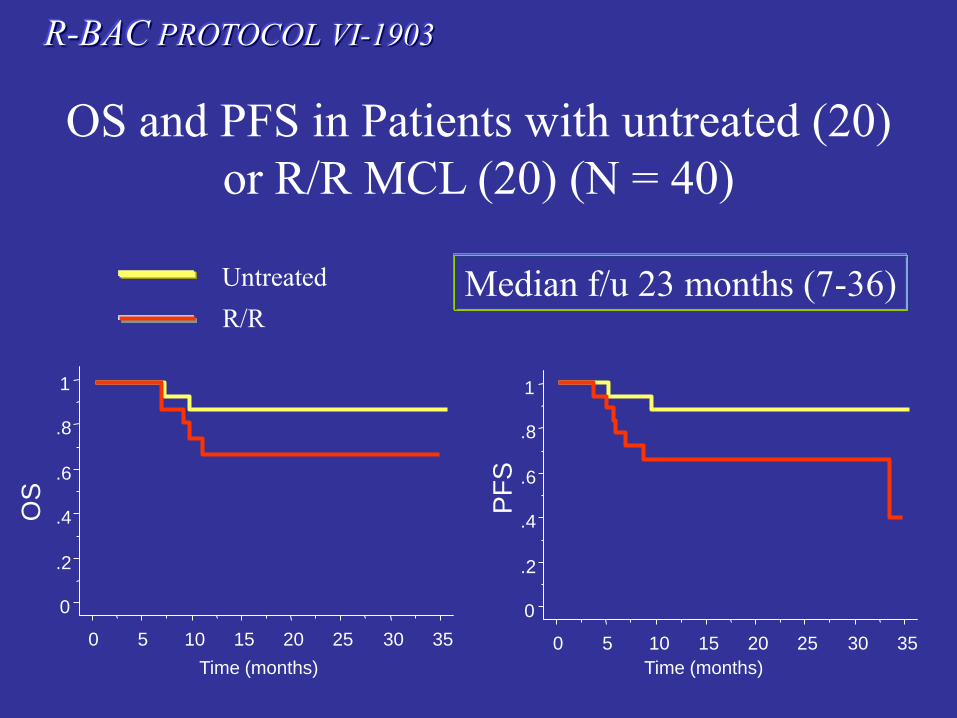
R-BAC PROTOCOL VI-1903
Untreated
R/R
OS and PFS in Patients with untreated (20)
or R/R MCL (20) (N = 40)
Median f/u 23 months (7-36)
0
.2
.4
.6
.8
1
0 5 10 15 20 25 30 35
Time (months)
0
.2
.4
.6
.8
1
0 5 10 15 20 25 30 35
Time (months)
OS
PF
S
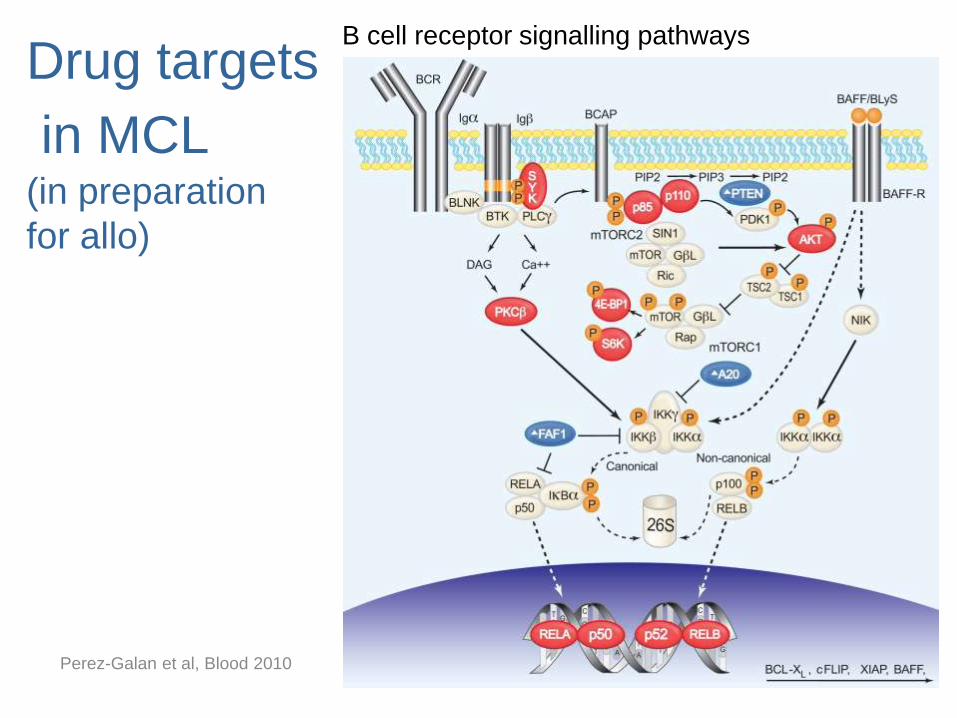
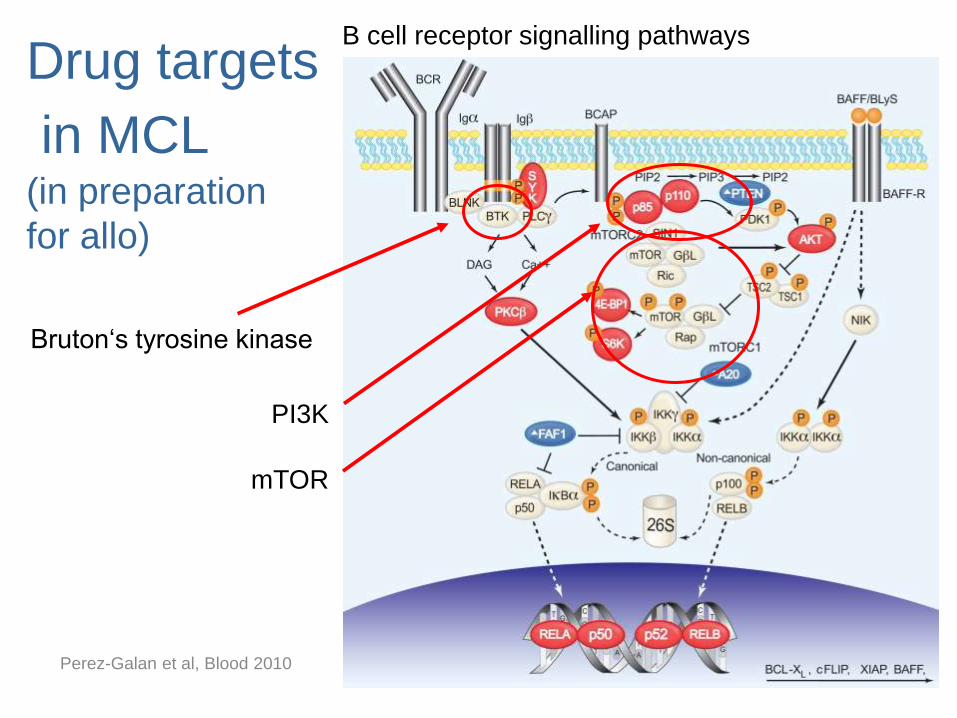
Drug targets
in MCL (in preparation
for allo)
B cell receptor signalling pathways
Perez-Galan et al, Blood 2010
Drug targets
in MCL (in preparation
for allo)
B cell receptor signalling pathways
Bruton‘s tyrosine kinase
Perez-Galan et al, Blood 2010
PI3K
mTOR
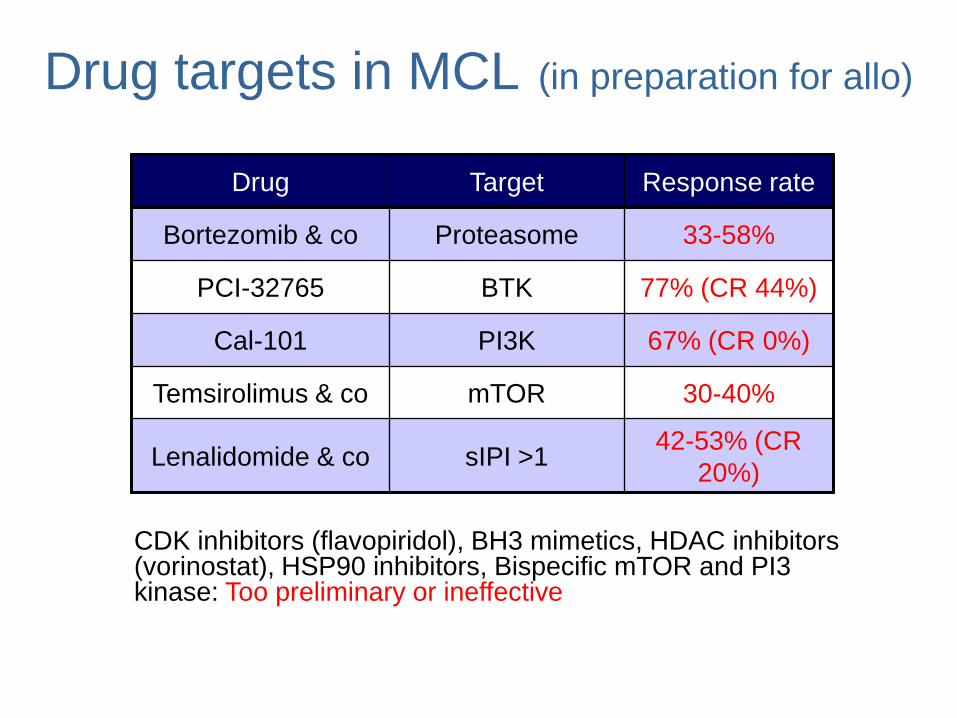
Drug Target Response rate
Bortezomib & co Proteasome 33-58%
PCI-32765 BTK 77% (CR 44%)
Cal-101 PI3K 67% (CR 0%)
Temsirolimus & co mTOR 30-40%
Lenalidomide & co sIPI >1 42-53% (CR
20%)
Drug targets in MCL (in preparation for allo)
CDK inhibitors (flavopiridol), BH3 mimetics, HDAC inhibitors (vorinostat), HSP90 inhibitors, Bispecific mTOR and PI3 kinase: Too preliminary or ineffective
CCI 779 +Rituximab Ansell et al ASH 2009 (abs 1665)
• 71 pts atleast two prior therapies
• 30% Rituximab refractory
• ORR 47% CR 20% PR 28%
• PFS 9.5 m
• Use of combination T3 (RFC,
RCHOP, RDHAP)
77
0
0.2
0.4
0.6
0.8
1
0 100 200 300
PFS (days)
Su
rviv
al
pro
ba
bil
ity
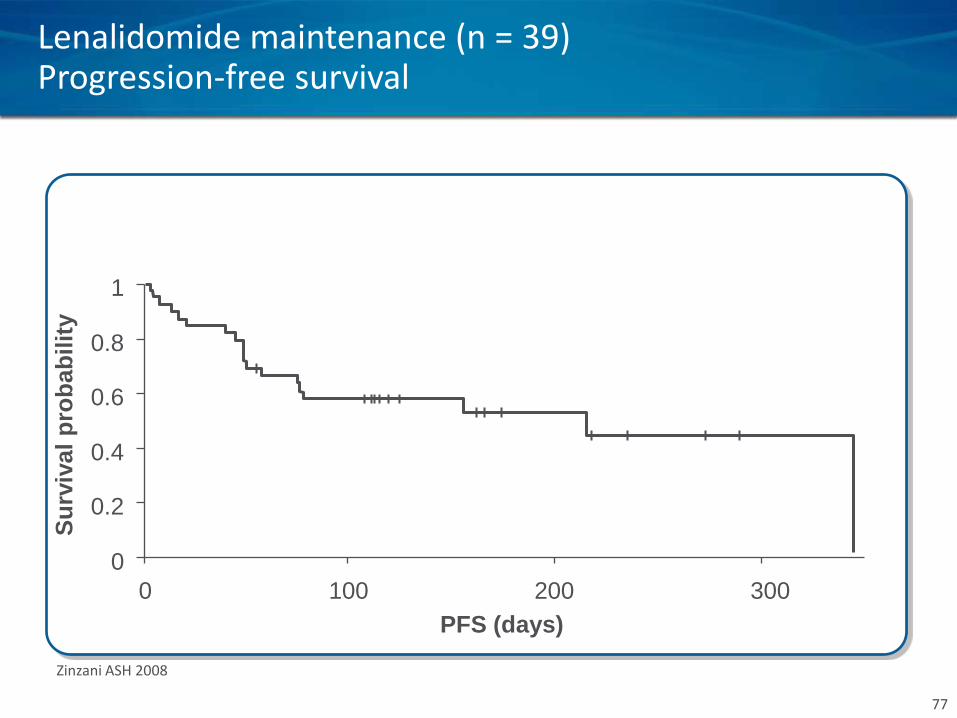
Zinzani ASH 2008
Lenalidomide maintenance (n = 39) Progression-free survival
78
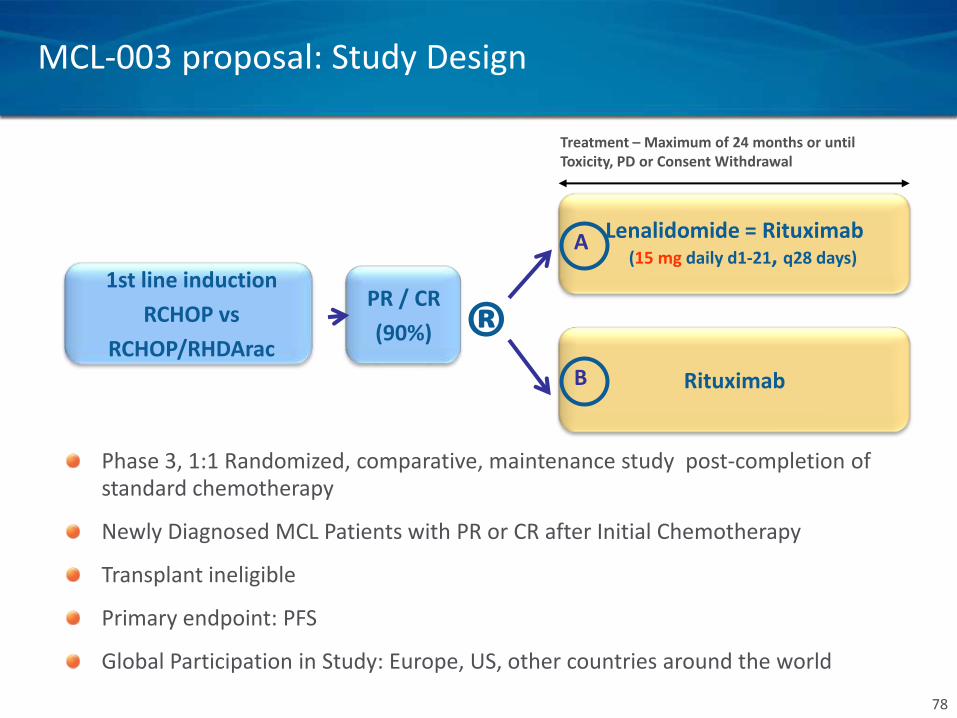
Treatment – Maximum of 24 months or until Toxicity, PD or Consent Withdrawal
1st line induction
RCHOP vs
RCHOP/RHDArac
Lenalidomide = Rituximab (15 mg daily d1-21, q28 days)
Rituximab
PR / CR
(90%) ® B
A
MCL-003 proposal: Study Design
Phase 3, 1:1 Randomized, comparative, maintenance study post-completion of standard chemotherapy
Newly Diagnosed MCL Patients with PR or CR after Initial Chemotherapy
Transplant ineligible
Primary endpoint: PFS
Global Participation in Study: Europe, US, other countries around the world
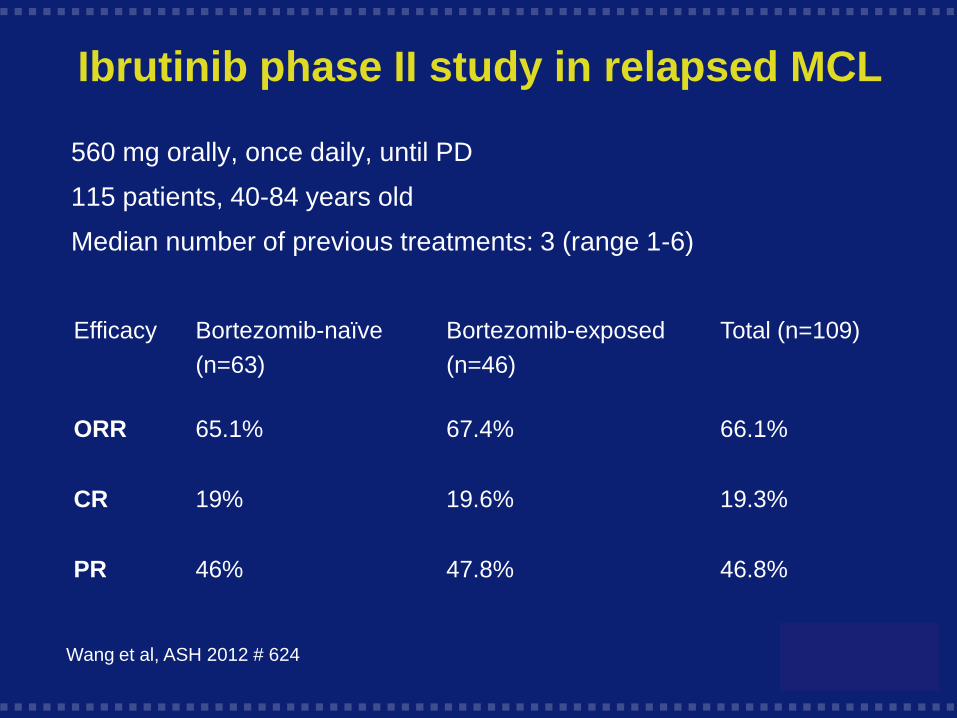
Ibrutinib phase II study in relapsed MCL
560 mg orally, once daily, until PD
115 patients, 40-84 years old
Median number of previous treatments: 3 (range 1-6)
Efficacy Bortezomib-naïve
(n=63)
Bortezomib-exposed
(n=46)
Total (n=109)
ORR 65.1% 67.4% 66.1%
CR 19% 19.6% 19.3%
PR 46% 47.8% 46.8%
Wang et al, ASH 2012 # 624
First line Elderly MCL
International trial (Jand J)
MCL
BR
BR-I
Conclusıon
• MCL prognosıs has ımproved and cure ıs
now a goal to achıeve
• Hıgh dose Arac/Rıtuxımab contaınıng
regımen
• Stem cell transplantatıon ın young
• Maıntenance ın ederly
• New drugs, probably best ıf used ın
combınatıon, are now avaılable that may
change these paradıgms
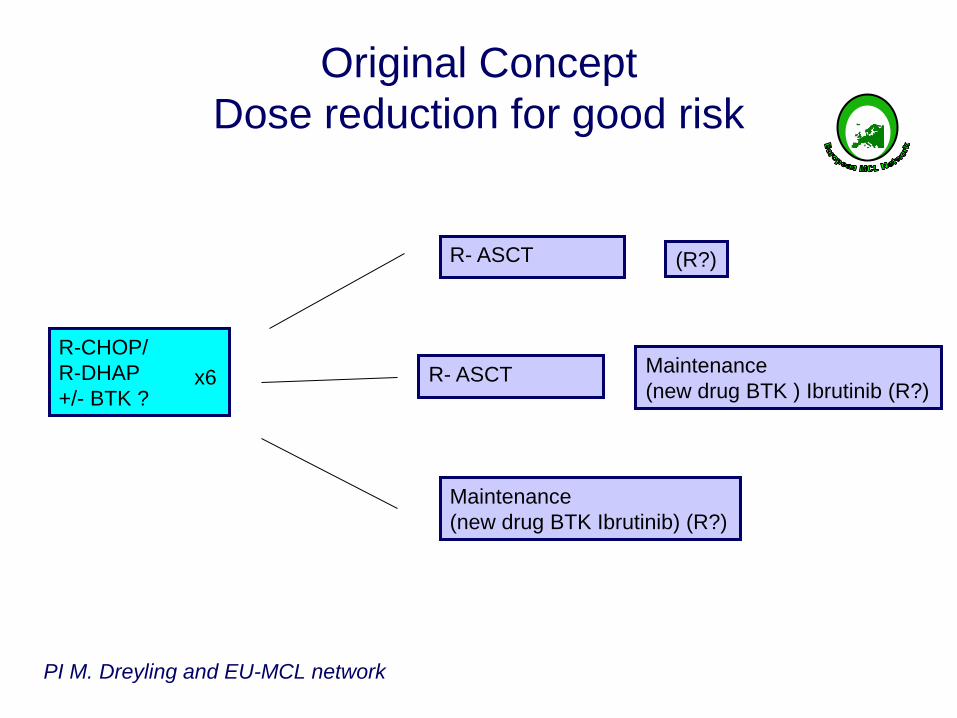
Original Concept
Dose reduction for good risk
R-CHOP/
R-DHAP
+/- BTK ? x6
R- ASCT
Maintenance
(new drug BTK ) Ibrutinib (R?)
PI M. Dreyling and EU-MCL network
R- ASCT
Maintenance
(new drug BTK Ibrutinib) (R?)
(R?)
Thank you Med V
Heidelberg
M Rieger
U Hegenbart
S Dietrich
AD Ho
Nordic LG
C Geisler
E Kimby
LWP
P Dreger
A Sureda
JJ Luan
H Finel
O Hermine
S Montoto
J Robinson
N Schmitz
H Schouten
A Boumendil
Slides
M Dreyling
T Fenske
C Geisler
B Glass
P Hari
O Hermine
S Montoto
S Robinson
N Schmitz
A Sureda
R Storb

Update November 19, 2010, European MCL Network, V0.3 26.11.2010
84
Aknowledgments
M Dreyling EMCL coordinator
• The support of the EMCL network including the
GELA , GLSG, and Polish lymphoma group.
• All the investigators and their staff from 129
centers in 4 countries (Germany 82 , France
35, Belgium 11 and Poland 1)
• The EMCL pathology review Panel (W Klapper,
N Brousse)
• The MRD group (C Pott, EA Macintyre, K
Beldjord, MH Delfau)
• The Data Center of Munich (E Hoster, M
Unterhalt) for data processing and statistics
• The GELA and GELA-RC, GLSG and PLSG
teams for organization, monitoring, data
cleaning
Treatment frail elderly MCL
patients
• Aim at optimal palliative treatment:
– Rituximab + chloorambucil
– Rituximab alone: not effective
– R-CVP
– (low dose) radiotherapy
– Small molecules (Lenalidomide,
Temsirolimus)?