Embed Size (px)
Citation preview

March 17, 2011 NAF AMM LA CA Bringing the Ataxia World Together
Patient Registries and Participating in Clinical Trials
Susan L. Perlman M.D.Clinical Professor of NeurologyDirector, UCLA Ataxia Center
Medical Director, NAF
March 17, 2011 NAF AMM LA CA Bringing the Ataxia World Together
March 17, 2011 NAF AMM LA CA Bringing the Ataxia World Together
The Bottom Line
• Every ataxia patient must participate in clinical trials.
• Every researcher designing a clinical trial must make it accessible to all ataxia patients.
• There will be exceptions to both of these fiats, but they must be justified.

TYPES OF CLINICAL TRIALSTYPE # SUBJECTS LENGTH AIM OF STUDY
N of 1 1 Ongoing Do I get better or stop getting worse on this drug?
Pilot Up to 20
All get drug
Weeks to months
Is a larger study worth doing, will there be problems?
Phase 1 20-80 normal or patient
in groups of 3
All get drug
2 years Escalating doses to learn side effects, safety, best dose
Phase 2 20-300
Placebo and drug groups
Compassionate trials do not use placebo.
2 years To assess potential for good effects, as well as side effects.
Also designed as “futility” study—to show a drug doesn’t not work(fewer subjects, less$)
Phase 3 300-3000
Placebo and drug groups
3-5 years To prove efficacy
May include crossover design, open extension trial
Phase 4 100’s-1000’s
Open drug use
Ongoing To find out more about the effects of an approved drug.
March 17, 2011 NAF AMM LA CA Bringing the Ataxia World Together
Every Ataxia Patient Must Participate in Clinical Trials
1. Registries will enable you to be found.
These are rare diseases with very small numbers of patients who can participate. Every person counts.
2. Be knowledgeable about what makes a good clinical trial—don’t make bad investments.
3. Speak up about the roadblocks to participation. Become involved in planning the trials.
4. Be prepared to make sacrifices.

March 17, 2011 NAF AMM LA CA Bringing the Ataxia World Together
Every Researcher Designing A Clinical Trial Must Make It Accessible To All
Ataxia Patients.• Design trials that can use the fewest patients over the
shortest period of time (this usually means testing better drugs and using biomarkers).
• What is the rationale for excluding certain patients? Can those excluded be used in other ways? Parallel or compassionate studies?
But remember that a patient can participate in only one trial at a time and that participation in some trials may permanently disqualify participation in others.
• Reimbursing travel costs is essential for recruitment and compliance. Telemedicine?
• Don’t expect the patients to make unreasonable sacrifices.

March 17, 2011 NAF AMM LA CA Bringing the Ataxia World Together
Registries
• Ataxia patients are some of the most highly motivated research subjects around, but they aren’t superhuman.
• The Cooperative Ataxia Research Network and the National Ataxia Foundation are not mind-readers.
• Every ataxia patient must be in a Registry.
March 17, 2011 NAF AMM LA CA Bringing the Ataxia World Together
The National Ataxia Registryfor all ataxias, must sign a consent form and provide PHI
• National Ataxia Registry C/o Registry Coordinator Department of Neurology McKnight Brain Institute at University of Florida 100 S. Newell Dr. L1-108 PO Box 100236 Gainesville, FL 32610-0236
• Phone : 352-273-9194Fax: 352-392-8058
• Email: [email protected] • Web Site: http://www.NationalAtaxiaRegistry.org Has links to all the other registries.
March 17, 2011 NAF AMM LA CA Bringing the Ataxia World Together
Rare Diseases Clinical Research Network Registryfor all ataxias
participants in the Clinical Research Consortium for SCA 1, 2, 3, and 6 are automatically registered
• http://rarediseasesnetwork.epi.usf.edu/CRC-SCA/register/registry.htm• After you have read and agreed to the authorization, the Contact Registry form will appear on your
screen. This form asks you for information such as your (or your child's) name, address, birth date, place of birth, email address, or items relevant to your (or your child's) disorders:
• Ataxia telangiectasia • Ataxia with oculomotor apraxia (AOA) type 1 • Ataxia with oculomotor apraxia (AOA) type 2 • Ataxia with vitamin E deficiency (AVED) • Ataxia, unknown cause • Autosomal recessive ataxia of Charlevoix-Saguenay (ARSACS) • Dentatorubral-pallidoluysian atrophy (DRPLA) • Fragile X tremor-ataxia syndrome (FXTAS) • Friedreich's ataxia • GAD ataxia • Gluten ataxia • Mitochondrial ataxia • Mitochondrial recessive ataxia syndrome (MIRAS; POLG mutation) • Multiple system atrophy-cerebellar type (MSA-C) • Olivopontocerebellar atrophy (OPCA) • Paraneoplastic ataxia • Spinocerebellar ataxia 1(SCA1) • Spinocerebellar ataxia 2(SCA2) • Spinocerebellar ataxia 3(SCA3/Machado Joseph disease/MJD) • Spinocerebellar ataxia 4(SCA4) • Spinocerebellar ataxia 5(SCA5) • Spinocerebellar ataxia 6(SCA6) • Spinocerebellar ataxia 7(SCA7) • Spinocerebellar ataxia 8(SCA8) • Spinocerebellar ataxia 10(SCA10) • Spinocerebellar ataxia 11(SCA11) • Spinocerebellar ataxia 12(SCA12) • Spinocerebellar ataxia 13(SCA13) • Spinocerebellar ataxia 14(SCA14) • Spinocerebellar ataxia 15(SCA15) • Spinocerebellar ataxia 16(SCA16) • Spinocerebellar ataxia 17(SCA17) • Spinocerebellar ataxia 18(SCA18) • Spinocerebellar ataxia 19(SCA19) • Spinocerebellar ataxia 20(SCA20) • Spinocerebellar ataxia 21(SCA21) • Spinocerebellar ataxia 22(SCA22) • Spinocerebellar ataxia 23(SCA23) • Spinocerebellar ataxia 24(SCA24); Spinocerebellar Ataxia, Autosomal Recessive 4; SCAR4 • Spinocerebellar ataxia 25(SCA25) • Spinocerebellar ataxia 26(SCA26) • Spinocerebellar ataxia 27(SCA27) • Spinocerebellar ataxia 28(SCA28) • Spinocerebellar ataxia 29(SCA29) • Spinocerebellar ataxia 31(SCA31) • Sporadic ataxia (onset before 20 years) • Sporadic ataxia (onset between 20-50 years) • Sporadic ataxia (onset after 50 years)
March 17, 2011 NAF AMM LA CA Bringing the Ataxia World Together
CINCHfor episodic ataxias
• http://rarediseasesnetwork.epi.usf.edu/cinch/index.htm
• CINCH • Clinical Investigation of Neurologic Channelopathies
• is a collaborative effort of doctors, patient organizations, and federal health agencies that want to learn more about these diseases so that ultimately they can offer better treatments to patients.
March 17, 2011 NAF AMM LA CA Bringing the Ataxia World Together
Friedreich’s Ataxia Registry
• http://www.curefa.org/registry.html• The FARA patient registry is the only worldwide registry of Friedreich’s ataxia patients. This
registry currently holds the demographic and clinical information on >1200 Friedreich’s ataxia patients from across the United States and internationally. This registry was created to serve the patient, physician, and research communities.
• For the Patient Community• Participation in the FARA patient registry ensures that patients are informed about opportunities
to participate in clinical research studies and kept up-to-date on the progress of clinical trials.• For the Physician• The homepage of the FARA patient registry website, www.curefa.org/registry, is a place that you
can go to find an up-to-date listing of ongoing clinical trials for FA. You can refer your FA patients to the patient registry so that he/she can consider registering. FARA can provide you with registry brochures that you can give your patients to assist with the referral process.
• For the Researcher• The FARA patient registry is a patient recruitment and communications tool for both academic
and industry sponsored clinical research studies and trials. The registry coordinator can perform queries based on the inclusion/ exclusion criteria of a study and send patients information about a study for which they qualify. Patients can be contacted by the registry coordinator via e-mail, mail, or by telephone. Informational postings can also be added to the registry homepage as well as the FARA website and in the FARA newsletter. FARA is committed to assisting researchers with study recruitment and participation.
March 17, 2011 NAF AMM LA CA Bringing the Ataxia World Together
Becoming A Knowledgeable Consumer
• General trial info:
• • Determining dosage maximum – is it safe?
• • How will my confidentiality be maintained? Identity disclosure issues
• • Explain need for exclusionary and placebo process
• • How to choose a trial and where to go
• • Telemedicine for trials?
• • Face to face presentation of each trial’s process/benefit and communicate to potential participants: Why do we have to discontinue our current meds? What are the measures of confidentiality required or available? Type of contact?
•
• In terms of ongoing trials:
• • Why is this trial being done?
• • What’s the long term benefit?
• • Explain what you’ll do in the trial—why will these measures show change?
• • Present info in clear format for FAQs, ex.: travel expenses, risks, disclosure
• • What are the side effects, benefits
• • How will participation affect or be affected by my current medications?
• • Concealment/placebo affects
March 17, 2011 NAF AMM LA CA Bringing the Ataxia World Together
Roadblocks
March 17, 2011 NAF AMM LA CA Bringing the Ataxia World Together
Sacrifices
• Time
• Money
• Confidentiality
• Ultimately, choosing and giving up one drug trial for another.

March 17, 2011 NAF AMM LA CA Bringing the Ataxia World Together
Roadblocks for Clinical Researchers
• Picking the right drugs.• Designing the trial properly—number of patients,
measures/biomarkers, length of study, placebo, how many sites.
• Getting the FDA to agree.• Getting funding.• Finding sites and getting them approved.• Finding subjects.• Doing the work in a timely fashion.
March 17, 2011 NAF AMM LA CA Bringing the Ataxia World Together
PRO’S AND CON’S OF CANDIDATE DRUGS FOR HUMAN TRIALS
• Rationale--do we expect it to work? Basic Science
• Efficacy-has it worked in well-designed animal or pilot human trials?
• Safety-has safety been proven?• Do the anticipated benefits outweigh the
possible risks? • Availability--designer drugs vs. already
available ones. What’s in it for the drug company?
• Cost (and where to get the money from)
March 17, 2011 NAF AMM LA CA Bringing the Ataxia World Together
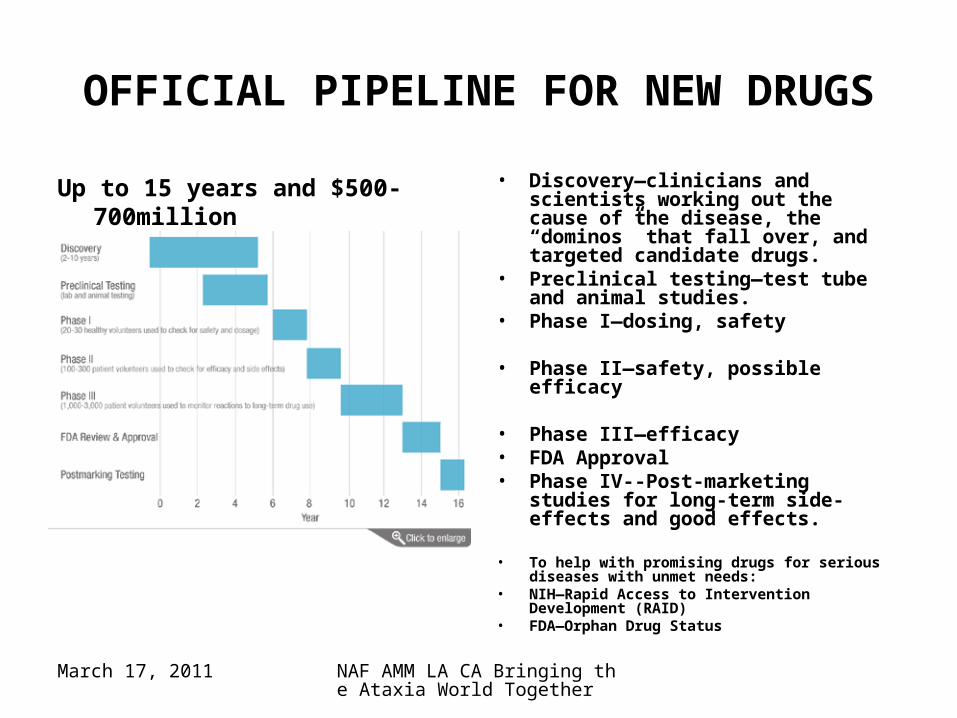
OFFICIAL PIPELINE FOR NEW DRUGS
Up to 15 years and $500-700million to get to market
• Discovery—clinicians and scientists working out the cause of the disease, the “dominos” that fall over, and targeted candidate drugs.
• Preclinical testing—test tube and animal studies.
• Phase I—dosing, safety
• Phase II—safety, possible efficacy
• Phase III—efficacy• FDA Approval• Phase IV--Post-marketing studies
for long-term side-effects and good effects.
• To help with promising drugs for serious diseases with unmet needs:
• NIH—Rapid Access to Intervention Development (RAID)
• FDA—Orphan Drug Status
March 17, 2011 NAF AMM LA CA Bringing the Ataxia World Together
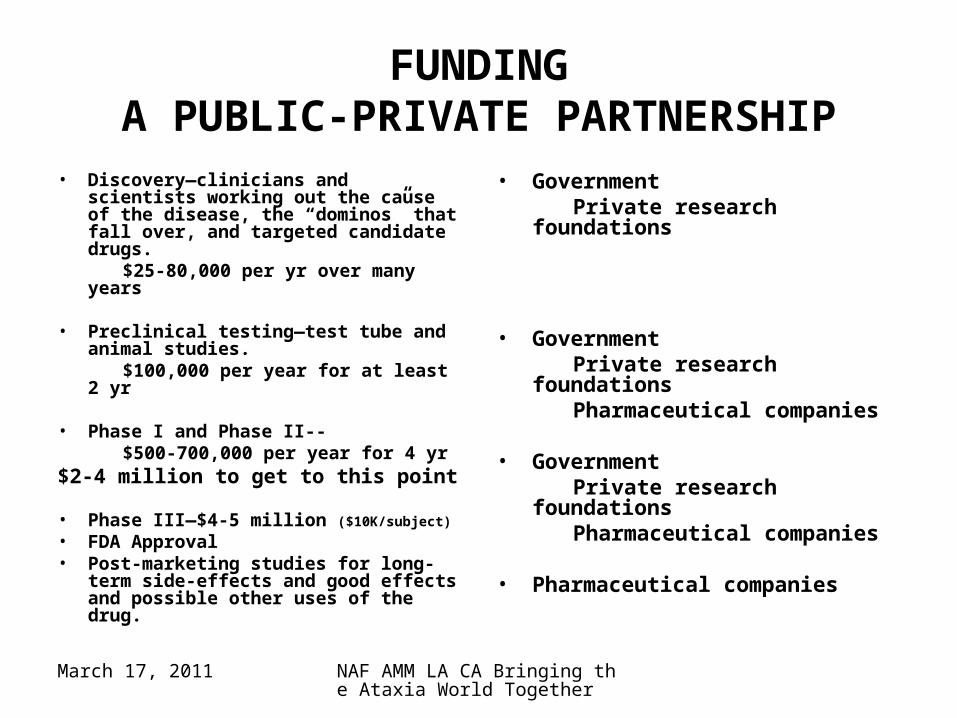
FUNDINGA PUBLIC-PRIVATE PARTNERSHIP
• Discovery—clinicians and scientists working out the cause of the disease, the “dominos” that fall over, and targeted candidate drugs.
$25-80,000 per yr over many years
• Preclinical testing—test tube and animal studies.
$100,000 per year for at least 2 yr
• Phase I and Phase II-- $500-700,000 per year for 4 yr$2-4 million to get to this point
• Phase III—$4-5 million ($10K/subject)
• FDA Approval• Post-marketing studies for long-
term side-effects and good effects and possible other uses of the drug.
• Government Private research foundations
• Government Private research foundations Pharmaceutical companies
• Government Private research foundations Pharmaceutical companies
• Pharmaceutical companies

March 17, 2011 NAF AMM LA CA Bringing the Ataxia World Together
EFFICACY--CAN WE SHOW THAT THE DRUG ACTUALLY MAKES A DIFFERENCE?
• Symptomatic benefit vs. disease-modifying• Is the candidate drug strong and specific?• How much does the disease change over
how much time? Natural history.• How accurately can this change be
measured? Rating scales, QOL measures.• Can biomarkers show clinically meaningful
change quicker? 1° vs. 2° outcome measure.• Can enough researchers and patients be
found? Research centers and registries.
March 17, 2011 NAF AMM LA CA Bringing the Ataxia World Together
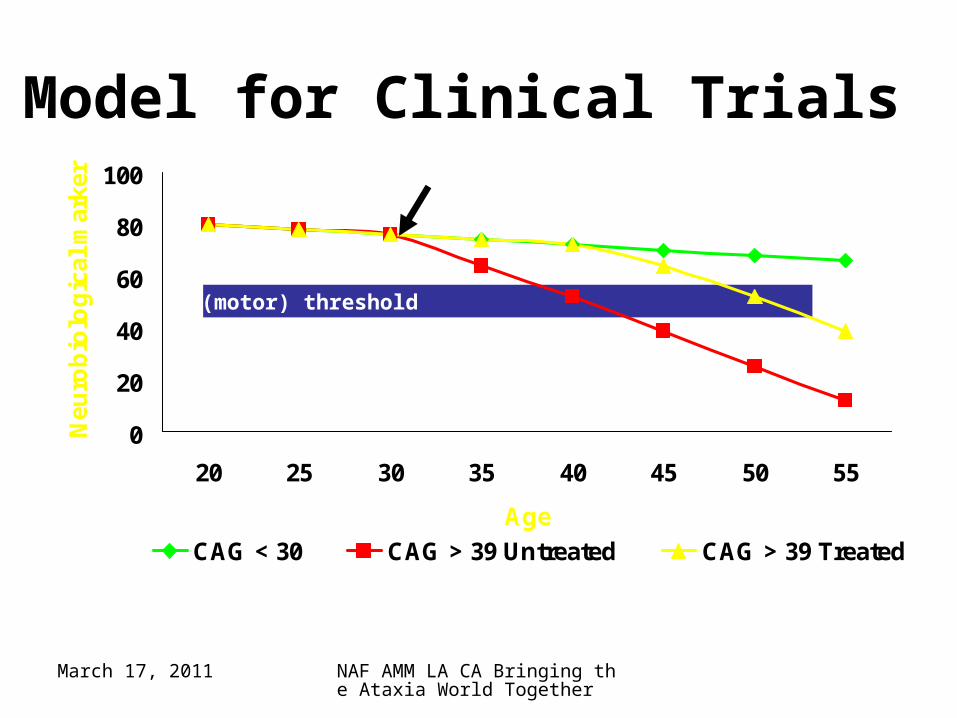
Diagnostic (motor) threshold
0
20
40
60
80
100
20 25 30 35 40 45 50 55
Age
Neu
rob
iolo
gic
al m
arke
r
CAG < 30 CAG > 39 Untreated CAG > 39 Treated
Model for Clinical Trials





























