Embed Size (px)
Citation preview

Dr Tha Han Consultant in Public Health Medicine, Enfield Council
Dr Tha Han, CPH, is a qualified medical doctor specialising in Public Health Medicine. His current role as a Consultant in Public Health within Enfield Council includes giving public health advice to Enfield CCG to maximise health outcomes of Enfield residents; reducing health inequalities in Enfield by influencing the Council’s partners; and ensuring health and social services are better integrated.
Miho Yoshizaki Senior Public Health Analyst, Enfield Council
Miho is part of the Council’s Health Intelligence team, which provides evidence and intelligence to support strategic decision making. She and her colleagues have developed various resources, including Locality Profiles, Ward Profiles, GP Practice Profiles and a JSNA.
Phil Gregory Public Health Associate, Enfield Council
Phil works within the Council’s Public Health team as part of the Enfield CCG support function. His work involves developing strategic solutions to reduce health inequalities and improve life expectancy; supporting the Council’s work around integrating health and social care services; and undertaking research and analysis around the wider determinants of health.
As clinicians we all know the impact hypertension can have in terms of leading to morbidity and mortality.
It is fantastic that in Enfield some 3,500 more people have their blood pressure controlled than was the case in 2008/2009.
I was particularly pleased to see the CCG commission the Hilo project and have been truly impressed by the results achieved by Eagle House and Evergreen.
I am indebted to Dr Tha Han and the team for putting this newsletter together and supporting our local clinicians, and of course to all of our local GPs, practice nurses, pharmacists and other colleagues who are making Enfield a healthier place for all of our residents.
Dr Shahed AhmadDirector of Public Health in Enfield
Enfield CCG takes hypertension seriously, especially as 2 out of 3 deaths from heart disease could be prevented and as much as 1 in 4 adults in Enfield have hypertension.
To screen for new patients and treat existing patients with hypertension, Enfield CCG has implemented a
number of evidence based initiatives. Health Kiosks measuring height, weight and blood pressure have been sited in GP Practices across Enfield, and in partnership with Enfield Council, Enfield CCG is working on the Hilo Project, an innovative way of managing hypertensive patients in areas of high need.
Dr Mo AbediChair of NHS Enfield Clinical Commissioning Group (CCG) and a local GP
EnfieldClinical Commissioning Group
www.enfield.gov.uk/bp
IntroductionMarch 2015

The Health Risks of HypertensionThe risk associated with increasing blood pressure is continuous, with each 2mmHg rise in systolic blood pressure associated with a 7% increased risk of mortality from ischaemic heart disease and a 10% increased risk of mortality from stroke1. Increased blood pressure in midlife raises the risk of dementia later on2. Public Health England (PHE) reveals that diseases caused by high blood pressure are estimated to cost the NHS over £2 billion every year. According to the World Health Organisation, the disease burden attributable to a systolic blood pressure of 115mmHg or above is:
People with hypertension are also at risk of target organ damage (kidneys, heart and brain). NICE recommends that this must be excluded within a month of every new diagnosis of hypertension3.
1 http://www.fph.org.uk/uploads/bs_hypertension.pdf 2005 accessed 13.10.142 Gottesman R. et.al. 2014. Midlife Hypertension and 20-Year Cognitive Change
The Atherosclerosis Risk in Communities Neurocognitive Study. JAMA Neurol. 2014;71(10):1218-1227. doi:10.1001/jamaneurol.2014.1646. Accessed 13.10.14
3 NICE Quality Standard for Hypertension 2013. http://www.nice.org.uk/guidance/qs28/chapter/quality-statement-2-investigations-for-target-organ-damage (accessed 13.10.14).
2 ENFIELD PubLIc HEaLtH | Newsletter for Health Professionals
Impact of Hypertension on Enfield residentsHypertension is persistently raised blood pressure, defined as 140/90mmHg or above. Treatment varies according to the nature and severity of hypertension and an individual’s ethnic background. Untreated hypertension is usually associated with a progressive rise in blood pressure, potentially causing vascular, heart and kidney damage that can culminate in a treatment-resistant state4.
In Enfield, just over 13% of the population know they have high blood pressure whilst the actual prevalence is estimated to be nearer 25%. This means that there could be more than 26,000 people in the borough who have hypertension without knowing it and therefore are not treated.
Improving the management of hypertension across the borough would make an important contribution to tackling local health inequalities and reducing burden on health and social care. Mortality from circulatory diseases is one of the largest contributors to the life expectancy gap between the most and least deprived areas in Enfield. Public Health England estimates that 179 deaths (100 men and 79 women) from circulatory diseases would have been prevented if the most deprived fifth had the same mortality rate as the least deprived fifth5.
Evidence suggests that one of the most effective interventions to improve blood pressure control in primary care settings is an organised system of regular population review6.
4 NICE CG127. 2011. Hypertension: Clinical management of hypertension in adults. http://www.nice.org.uk/guidance/cg127/chapter/introduction
5 Public Health England Segment Tool 2015. http://www.lho.org.uk/LHO_Topics/Analytic_Tools/Segment/Documents/LA_E09000010.pdf (Accessed: 16.04.2015)
6 Glynn LG, Murphy AW, Smith SM, Schroeder K, Fahey T. Interventions used to improve control of blood pressure in patients with hypertension. Cochrane Database of Systematic Reviews 2010, Issue 3. Art. No.: CD005182. DOI: 10.1002/14651858.CD005182.pub4
20% of all deaths
in men
24% of all deaths
in women
49%of coronary heart
disease
62% of strokes

Know your blood pressure‘Know your blood pressure’ is one of LB Enfield’s most recent campaigns, launched in October 2014. Posters were displayed at GP practices, on the sides of buses, and at other prominent places in the community.
This campaign will help the GPs in explaining patients the importance of blood pressure self-monitoring and control.
The NHS Health Checks Programme is another good way for Enfield residents with higher cardiovascular disease (CVD) risk to get their blood pressure and other risks checked. Over 8,000 health checks took place in Enfield between 2013 and 2014.
NHS Health ChecksEnfield residents who have not already been diagnosed with high blood pressure, diabetes, heart disease or other vascular disease, are aged between 40 and 74 years old and have not had an NHS health check in the past 5 years are entitled to a free NHS Health Check. They will be asked some questions about their health, and have their cholesterol, blood pressure, pulse and BMI (body mass index) checked.
In Enfield, NHS Health Checks take place mainly at GP surgeries. On some occasions, it is available at pharmacies, and community events at supermarkets, leisure centres and schools. Please ask your GP surgery whether you are eligible for a NHS Healthcheck.
3March 2015

4 ENFIELD PubLIc HEaLtH | Newsletter for Health Professionals
Gauging the stages of hypertensionNICE (CG127) recommended that people with treated hypertension should have a clinic blood pressure target set to below 140/90mmHg if they are aged under 80 years, or below 150/90mmHg if 80 years and over7.
The Guidance recommends ambulatory blood pressure measurements, taken whilst walking around with a blood pressure cuff strapped to the arm for 24 hours to confirm whether a person has hypertension. This reduces the risk of unnecessary treatment in people who do not have true hypertension (for example, those who test high due to a ‘white coat’ effect). One economic evaluation study found that ambulatory blood pressure monitoring (ABPM) is significantly more cost-effective than conventional measurement of blood pressure, reduces the cost of follow-up, and improves patients’ quality of life8.
Scale of the problemThe Quality and Outcomes Framework (QOF) has indicators for recording patients with blood pressure of 150/90 or less (systolic/diastolic) on the hypertension, diabetes, stroke and coronary heart disease registers9.
7 NICE CG127. 2011. Hypertension: Clinical management of hypertension in adults. http://www.nice.org.uk/guidance/cg127/chapter/introduction
8 Roca R. et.al. 2006. Cost-effectiveness of ambulatory blood pressure monitoring in the follow-up of hypertension. Blood Press 26(1); 27-36 http://www.ncbi.nlm.nih.gov/pubmed/16492613 (accessed 13.10.14).
9 QOF HYP indicator 006 England QOF guidance 7th revision 2014-2015 Accessed 13.10.14
The Public Health Intelligence team in Enfield assimilates this data and publishes locality profiles and general practice profile. Excluding exceptions, 81.02% (32,814 out of 40,499) of patients with hypertension were reported to have had their blood pressure under 150/90mmHg (HYP002) in 2013/14 in Enfield. This is lower than both the London average of 82.3%, and England average of 83.1%. However among GP practices the proportion of registered patients achieving blood pressure control ranges from 39.4% to 96.8%.
Case StudyMark Tickner, a non-smoker and vegetarian, only knew about his high blood pressure after he suffered a heart attack. Feeling fit at 49, his heart attack happened suddenly.
He explained, “I had a multiple by-pass operation, was in hospital for five weeks and although I recovered, I am not quite the same person. Post-operative pain has lasted quite a while and now I must take medications every day.
“It has also been a strain on my family. But, of course I am glad to be alive. I want people to know that I was a knowledgeable nurse and this still happened to me. My condition arose through high blood pressure and I did not know about it – so I implore people to get their blood pressure checked.”

Everybody Active EnfieldEverybody Active is Enfield Borough Council’s physical activity strategy for all of Enfield’s residents. The programme includes:
� Activities at youth centres and leisure centres � An extensive walks programme � An outreach estates programme � Coach and instructor development � Competitive pathways and events � Dance classes such as ballet, jazz, zumba and
street danceDisability sport programmes � Family sport sessions � Healthy weight projects � Holiday and term programmes for young people � Volunteer development � Women and girls programme
For more information go to www.enfield.gov.uk/sport
5March 2015
Prevention and Public HealthReducing prevalence of hypertension would have important health effects. People with hypertension develop cardiovascular disease 5 years earlier10 than those with normal blood pressure. An economic study11 also estimated that a prevention programme reducing blood pressure levels by 5% across the whole population of England and Wales would result in annual savings worth at least £80m to £100m. A retrospective case note analysis is being undertaken in Enfield to strengthen our understanding of the proportions of each risk factor that contribute to cardiovascular disease.
Smoking, physical inactivity, high sodium intake, being overweight and low fruit and vegetable intake are the main modifiable lifestyle contributors to hypertension in Western societies12. A local prevention strategy that addresses moving, eating, drinking and smoking (mnemonics MEDS) will make a major contribution to the prevention of hypertension in Enfield.
A diet high in salt can contribute to high blood pressure. Nationally, salt consumption has reduced by about 15% over the past ten years, but the average intake is still around 8.1g/day – much higher than the recommended intake of 6g/day (3g for children aged 4-6 years)13.
Pre-prepared foods can be high in salt. Some food, such as bacon, ham, hard cheeses, ketchup and pickles are almost always high in salt. Using spices and herbs instead of salt can provide a healthier and often tastier alternative.
Supporting our residents with lifestyle change requires concerted action across agencies, and it includes consideration of the way we design our spatial environment – for example, through access to green spaces and active transport infrastructure. Enfield Borough Council’s Everybody Active programme aims to support physical activity across the borough by facilitating activities in schools, the workplace and in the community. We are delighted that in 2014, Enfield Borough Council won £27m funding to increase cycling in the borough – an initiative that should significantly impact on levels of physical activity among our residents.
10 Rapsomaniki E, Timmis A, George J, Pujades-Rodriguez M, Shah AD, Denaxas S, et al. Blood pressure and incidence of twelve cardiovascular diseases: lifetime risks, healthy life-years lost, and age-specific associations in 1·25 million people. Lancet [Internet]. 2014 May 31;383(9932):1899–911. Available from: http://www.sciencedirect.com/science/article/pii/S0140673614606851
11 Barton P, Andronis L, Briggs A, Lindsay WR, McPherson K, Capewell S (2011) Effectiveness and costeffectiveness of cardiovascular disease prevention in whole populations: modelling study. BMJ, 343, d4044. http://www.ncbi.nlm.nih.gov/pmc/articles/
12 Geleunse J. et.al. 2004. Impact of dietary and lifestyle factors on the prevalence of hypertension in Western Populations. European Journal of Public Health 14(3); 235-239.
13 https://responsibilitydeal.dh.gov.uk/salt-targets-review/ Accessed 13.10.14
As part of Making Every Contact Count strategy, NHS Bedfordshire introduced an initiative for reviewing medicines adherence with patients. The initiative, reported in the Health Service Journal used two simple questions: Can you take your medicines? And ‘Do you take your medicines?19
19 http://www.hsj.co.uk/home/commissioning/how-to-implement-medicines-optimisation/5061419.article (accessed 13.10.14)
6 ENFIELD PubLIc HEaLtH | Newsletter for Health Professionals
A 20mmHg reduction in systolic blood pressure is associated with less than half the risk of dying from a stroke, and half the risk of dying from coronary heart disease14.
According to one meta-analysis, compared with placebo, anti-hypertensive medication reduces the relative risk of mortality by 11% (effect size 0.89), of stroke by 35% (effect size 0.65), and hospitalisations by 5% (effect size 0.95).
Yet nationally, the proportion of patients taking medication for blood pressure with uncontrolled hypertension has changed little since 200315.
Enfield CCG is piloting a programme called ‘Hilo’ to help manage those patients whose blood pressure control is a problem. The pilot is supported by UCL partners and NIHR Pragmatic Clinical Trials Unit at QMUL. 2008 patients with uncontrolled hypertension or uncontrolled cholesterol from Evergreen Primary care Centre and Eagle House Surgery are included in the pilot. The preliminary results are promising at 9 months. Systolic blood pressure is reduced by 10.1 mmHg in those with hypertension and 9.7 mmHg in those with both hypertension and high cholesterol. To succeed further, national and local partners need to take action together16.
One element of the problem is poor medication adherence. The Royal Pharmaceutical Society reports that only 16% of patients prescribed a new medicine for a chronic illness take it as prescribed. Just ten days after starting a new medicine almost a third of patients are already non-compliant? adherent17. A Cochrane review found that patient reinforcement and reminding was the most promising category of interventions for increasing medication adherence18.
14 Prospective Studies Collaboration. 2002. Age-specific relevance of usual blood pressure to vascular mortality: a metaanalysis of individual data for one million adults in 61 prospective studies. Lancet; 360: 1903-12
15 Optimising hypertension treatment: NICE/BHS guideline implementation and audit for best practice | The British Journal of Cardiology [Internet]. [cited 2015 Mar 16]. Available from: http://bjcardio.co.uk/2013/03/optimising-hypertension-treatment-nicebhs-guideline-implementation-and-audit-for-best-practice/#
16 https://www.gov.uk/government/case-studies/tower-hamlets-managed-practice-networks-to-improve-rates-of-cardiovascular-disease
17 Royal Pharmaceutical Society. Medicines Optimisation: Helping patients to make the most of medicines. Good practice guidance for healthcare professionals in England. May 2013.
18 Schedlbauer A, Davies P, Fahey T. Interventions to improve adherence to lipid lowering medication. Cochrane Database of Systematic Reviews 2010, Issue 3. Art. No.: CD004371. DOI: 10.1002/14651858.CD004371.pub3. Assessed as up to date Sept 2008.
Gaining control
“Very helpful, practical advice. Even available on the phone. Excellent!”
Eagle House Surgery
HiLo Pilot
MECC (Making Every Contact Count) for Medicine AdherenceNHS Bedfordshire CCG introduced a strategy for implementing medicines management as part of Making Every Contact Count. The initiative, reported in the Health Service Journal used two simple questions:
‘Can you take your medicines?’ This opens a dialogue in which patients can highlight any practical problems such as inability to remove small tablets from foil strips or any misunderstanding about the role of their medicines.
‘Do you take your medicines?’This encourages patients to be honest about adherence problems so they can be fully supported by their community pharmacist or GP practice.
Source: http://www.hsj.co.uk/home/commissioning/how-to-implement-medicines-optimisation/5061419.article (accessed 13.10.14)
7March 2015
Based on evidence that calls for stepped care approach20, the NICE hypertension guideline recommends a four-step pathway approach to treatment. Nurse or pharmacist-led interventions guided by a structured care algorithm directed by a family doctor have shown promising results in the implementation of stepped treatment for hypertension21.
In addition to anti-hypertensives, statins should be used in those patients with hypertension who also have 10% ten-year CVD risk as assessed by QRisk222. The recommendation is for atorvastatin 20mg as the first line primary prevention at these risk levels is linked to their assessment that higher intensity statins are cost-effective down to risk thresholds of 6.8%. NICE cites evidence that for every 49 people (95% CI 40 to 66) in England and Wales treated with statins as primary prevention as per the NICE guidance, one CVD event would be avoided23. Locally ‘Hilo’ pilot is facilitating the control of cholesterol to those patients with hypertension and high cholesterol.
20 Stewart S.et.al. Effect of intensive structured care on individual blood pressure targets in primary care: multicentre randomised controlled trial. BMJ 2012; 345 doi: http://dx.doi.org/10.1136/bmj.e7156 (Published 20 November 2012) Cite this as: BMJ 2012;345:e7156
21 Clark CE, Smith LF, Taylor RS, Campbell JL. Nurse led interventions to improve control of blood pressure in people with hypertension: systematic review and meta-analysis. BMJ2010;341:c3995.
22 CG181 published July 2014. Lipid modification: cardiovascular risk assessment and the modification of blood lipids for the primary and secondary prevention of cardiovascular disease. https://www.nice.org.uk/Guidance/CG181. Accessed 13.10.14.
23 Lipid modification Cardiovascular risk assessment and the modification of blood lipids for the primary and secondary prevention of cardiovascular disease Clinical guideline Appendices July 2014 http://www.nice.org.uk/guidance/cg181/resources/cg181-lipid-modification-update-appendices2
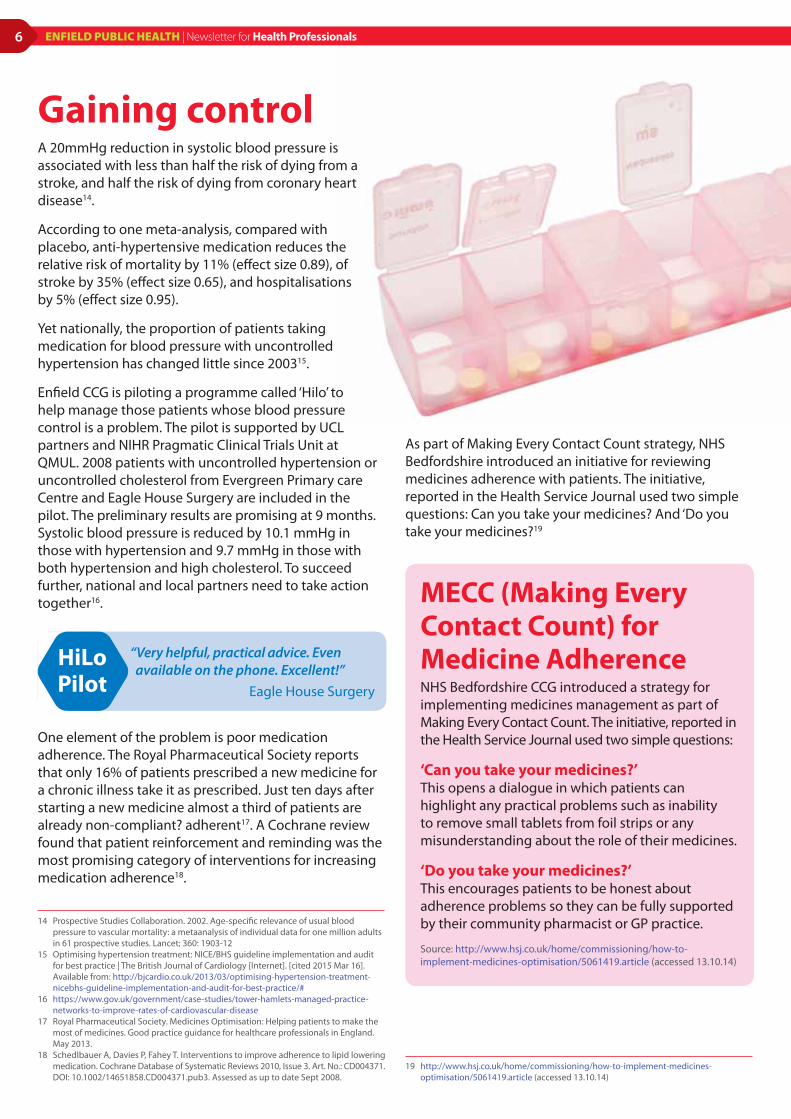
STEP 1Either ACE inhibitors or low-cost ARBs (for people who do not tolerate ACEi) for people age 55 years or under.
People aged over 55years and people of black African or Caribbean descent at any age should be offered a calcium channel blocker (CCB), or if that is not suitable they should be offered a thiazide-like diuretic.
STEP 2If step 1 does not successfully control hypertension, offer a CCB in combination with either an ACE inhibitor or an ARB.
People for whom a CCB is not suitable should be offered a thiazide-like diuretic, and people of black African or Caribbean descent can be offered an ARB in preference to an ACE inhibitor or in combination with a CCB.
STEP 3After review, if treatment with three drugs is required, the combination of ACE inhibitor or angiotensin II receptor blocker, calcium-channel blocker and thiazide-like diuretic should be used.
STEP 4(Resistant hypertension). People with blood potassium levels of 4.5 mmol/l or lower can be offered further diuretic therapy with low-dose spironolactone (25mg once daily). Caution is needed with people who have a reduced e-glomerular filtration rate.
For those with blood potassium higher than 4.5 mmol/l consider higher dose thiazide-like diuretic treatment.
Blood sodium and potassium, and renal function should be monitored in all patients at step 4.
Stepping up to hypertension management
“Evergreen has a very large patient population, disproportionately young compared with the rest of the Borough.
However, many of the older patients have particularly poor health with multiple
complex problems, coupled with poor compliance with medication and limited interest in preventative care. We have found working with the HiLo team to be particularly rewarding because it has enabled us to make tightly focussed healthcare interventions addressing multiple problems simultaneously. This is particularly important as we find patients reluctant to make return visits to deal with chronic illness as opposed to simple, acute problems.”
Evergreen Surgery/Edmonton Walk-In Centre, Edmonton Green
HiLo Pilot
8 ENFIELD PubLIc HEaLtH | Newsletter for Health Professionals
At National level, the Blood Pressure System Leadership Board was set up to oversee the collective programme of work on blood pressure including development of this action plan. Chaired by Public Health England, its wider members include the Royal College of General Practitioners, NHS England, NHS Improving Quality, Pharmacy Voice, British Heart Foundation, British Hypertension Society, Department of Health, Faculty of Public Health, Local Government Association, Association of Directors of Public Health, and Blood Pressure UK.
On 18th November 2014, the Board published an action plan for the prevention, early detection and management of high blood pressure. It shows the roles that different partners can play to tackle this important issue. Local voluntary organisations in our neighbourhood make an important contribution to hypertension management. Heart Throbs is one of the leading cardiac support groups in North London. It is an independent voluntary group affiliated to the British Heart Foundation. Heart Throbs offers support to patients after a heart procedure, including exercises and monthly meetings.
Working togetherHigh blood pressure is a hidden problem. There are around 36,000 people with uncontrolled blood pressure, of whom 26,000 do not even know they have hypertension. Although hypertension is a hidden problem, there is clear evidence around the benefits of prevention and treatment. Guidance is also available for effective management of the disease to prevent end organ damage.
Support is also made available by the CCG for the areas of high need. A joint effort between patients, professionals, public health and commissioners will improve the health of Enfield citizens by better understanding and better control of hypertension – thus preventing hypertension and the burden from its complications.
Useful resources l The NICE Quality Standard for hypertension was
published in 2013. http://tinyurl.com/peo6kq3 (accessed 13.10.14)
l The British Journal of Cardiology has published an education resource that can be used to contribute towards re-validation. http://tinyurl.com/p79skn6 (accessed 13.10.14)
l Residents can find information about hypertension from NHS Choices, http://tinyurl.com/6aqmccf, and a NHS shared decision making aid for hypertension, http://tinyurl.com/bshkds6 (accessed 13.10.14)
l NHS Choices provides a useful guide to salt reduction, http://tinyurl.com/o9a5ckc (accessed 13.10.14)
l The Heart Throbs website can be found here: http://heart-throbs.org.uk/
Sharing the care